")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 15
Role of Surgery in Metastatic Breast Cancer: Insights from a Narrative Review
Authors Alghamdi MAA, Esam Mahmood S
Received 24 January 2023
Accepted for publication 27 April 2023
Published 9 May 2023 Volume 2023:15 Pages 349—358
DOI https://doi.org/10.2147/BCTT.S405864
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert Clarke
Maha Ahmed Alamodi Alghamdi,1 Syed Esam Mahmood2
1Department of General Surgery, College of Medicine, King Khalid University, Abha, Saudi Arabia; 2Department of Family and Community Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia
Correspondence: Syed Esam Mahmood, Abha, 62529, Saudi Arabia, Tel +966550484344, Email [email protected]
Abstract: Metastatic breast cancer is difficult to cure and has a worse prognosis with higher rates of mortality. Recently, breast surgery is believed to improve the survival rates among these women, but due to limited evidence, definite conclusions cannot be made. Therefore, we undertook this narrative review to synthesize the evidence from existing studies to assess the effectiveness of locoregional surgery and surgery of metastatic sites in improving the outcomes among women diagnosed with metastatic cancer disease along with the summary of current treatment guidelines. We reviewed PubMed and Embase and included both observational studies and randomized controlled trials (RCTs) that were published in English between 2000 and 2021. Outcomes were either survival, quality of life, toxicity related to local treatment assessed by mortality at the end of one month, progression-free survival, and breast cancer-specific survival. The main effect size assessed was hazard ratio with their 95% CIs. After literature search, we found 8 observational studies and 3 RCTs. The findings of the observational studies revealed that breast cancer surgery improves survival from 30% to 50% among women. However, findings from RCTs were mixed for local and distant progression survival. Surgery improved the local progression-free survival but worsened the distant progression-free survival. Besides, there was no effect of breast surgery on quality of life. Regarding the surgery of metastatic site, studies are complex with mixed findings and variation in survival depending upon the type of metastatic site and response to initial systematic therapy and other factors. Based on the existing mixed evidence, it is not possible to make firm and definite conclusions about the effectiveness of breast surgery in improving the survival or quality of life among women with metastatic breast cancer. In future, more RCTs are required with a larger sample size to confirm the findings of observational studies.
Keywords: breast surgery, metastatic breast cancer, women, narrative review
Introduction
Breast cancer is a highly prevalent cancer in women across the world as it contributes to 25% of all diagnosed cancers.1 It is the second most common cause of cancer-related mortality in the United States.2 It is estimated that one out of every eight women will be diagnosed with breast cancer in their lifetime and the most commonly affected age group is 55 to 64 years.3 Each year, approximately 1.67 million cases of breast cancer are identified globally.4 Of the total breast cancer cases, 20% to 30% end up having metastatic breast cancer, which eventually causes 400, 000 to 50,000 deaths annually across the world.5 At the time of initial diagnosis, around 3.5% of women with breast cancer had already developed distant metastasis in the United States and this proportion is even higher in resource-poor settings.6 This implies that annually around 50,000 women will be diagnosed with metastatic breast cancer.7
While it may be challenging to have a complete cure for metastatic breast cancer, women can now live relatively longer than before due to various treatment modalities. This has increased the survival rate of five years from 10% in 1970 to approximately 40% after 1995.8 Also, the existing evidence reveals that median survival has improved from 20 to 26 months over the last two decades.9 However, this increased life expectancy may enhance the risk of symptoms among those women who have not undergone surgical removal of the breast. Although it is necessary to treat breast cancer, sometimes treatment can negatively affect the women’s quality of life.10 This is perhaps due to fear of developing the disease again, decrease sexuality, and loss of job.
Since metastatic breast cancer is considered an incurable disease with a worse prognosis, usually patients are provided with palliation and systematic therapy.11 Typically, breast surgery is performed if a woman presents with symptoms. Over the last many decades, it was believed that after metastasis, aggressive local treatment is not beneficial and therefore should not be considered as the treatment of choice.12 However, evidence from retrospective observational studies and few intervention studies suggest that patients with metastatic breast cancer may benefit from surgery and removal of the breast tumor.12 This evidence-primarily comes from observational studies, which are subject to confounding and selection bias issues.13 Therefore, it is important to review the evidence both from observational and interventional studies before making any conclusions about the role of breast surgery in metastatic breast cancer. Further, the evidence generally considers systematic therapy as the main treatment modality in case of metastasis. However, locoregional surgery by removing the breast and axillary tissues along with treating or doing surgery of meta-static site may reduce the symptoms and prevent cancer-related adverse outcomes. To provide up-to-date evidence, we performed a narrative review of both observational and interventional studies carried out to synthesize the findings regarding the efficacy of breast surgery in treating metastatic breast cancer. In addition, we also reviewed the evidence regarding the role of surgery of metastatic sites in preventing cancer-related complications followed by providing a summary of current guidelines in managing metastatic breast cancer.
Methods
This narrative review addresses the research question of what is the benefit of breast surgery (mastectomy: removal of the complete breast along with lymph nodes, nipple and areola or lumpectomy: removing breast tissue and tumor but preserving nipple and areola) among women diagnosed with metastatic breast cancer. Any study either observational or intervention study that assessed the effectiveness of breast surgery in improving the survival or quality of life among women with metastatic breast cancer, published in the English language between 2000 and 2021 was included. We searched the databases such as PubMed and Embase by using appropriate search terms such as “Breast surgery” OR” mastectomy” OR “lumpectomy” AND “Metastatic disease” AND “Survival” AND “observational studies” OR” intervention studies” AND “Quality of Life”. The randomized controlled trials that compared breast surgery with systematic therapy including endocrine therapy, chemotherapy, radiotherapy, biologic therapy, and supportive care against only systematic therapy were included. Outcomes were either survival, quality of life, toxicity related to local treatment assessed by mortality at the end of one month, progression-free survival, and breast cancer-specific survival (Table 1).
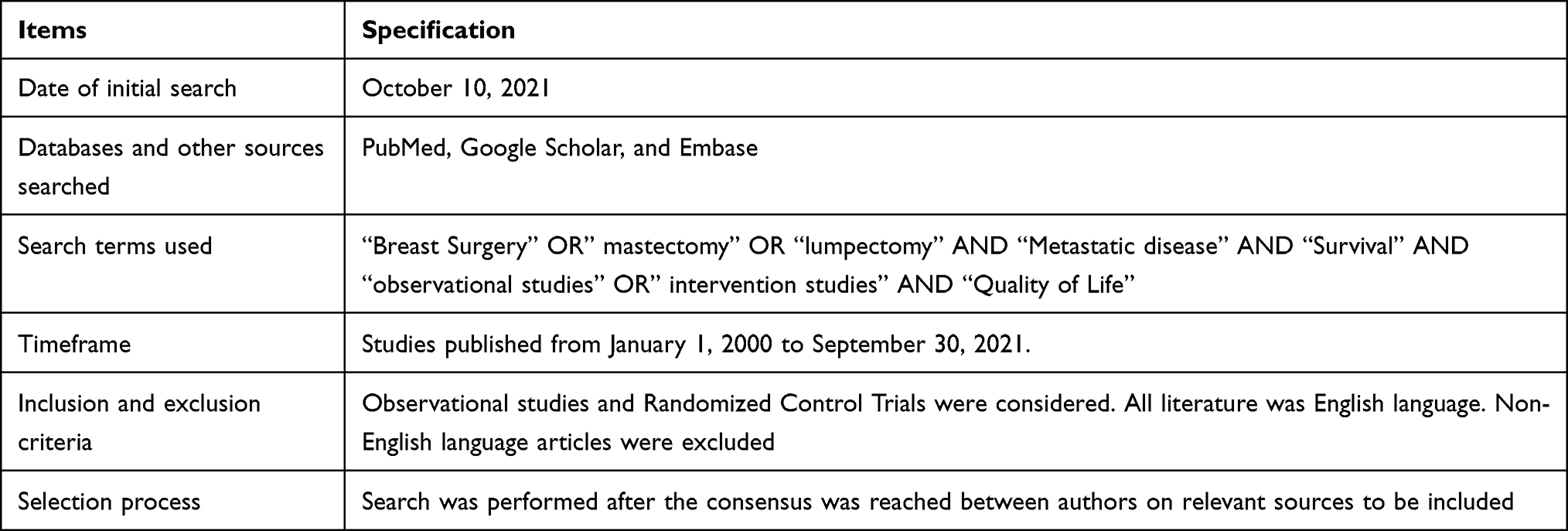 |
Table 1 Methodology Applied for the Development of This Narrative Review |
Study Results
Indication of Locoregional Surgery (Breast and Axilla) in Metastatic Breast Cancer: Evidence from Observational Studies
Overall, the existing evidence from retrospective observational studies reveals a beneficial effect of breast surgery in improving the survival of women (Table 2). For instance, a study by Khan et al in 2002 on 16,023 patients found that breast surgery improved the survival of women by almost 40% (HR: 0.61, 95% CI: 0.58 to 0.65) with statistically significant results.6 In 2006, Babiera et al conducted a retrospective analysis of 224 patients and 37% of those underwent surgery.14 The findings of the study demonstrated that breast surgery improved survival by 50% (HR: 0.51, 95% CI: 0.21 to 1.19); however, the results were not statistically significant.14 These findings were in agreement with a study by Rapiti et al who performed the study in the same year (2006) on 300 patients.15 Around 42% of the women underwent surgery and authors found surgical treatment reduces the mortality by 40% (HR: 0.60, 95% CI: 0.4 to 1.0) with statistically non-significant results as shown in Table 2.15
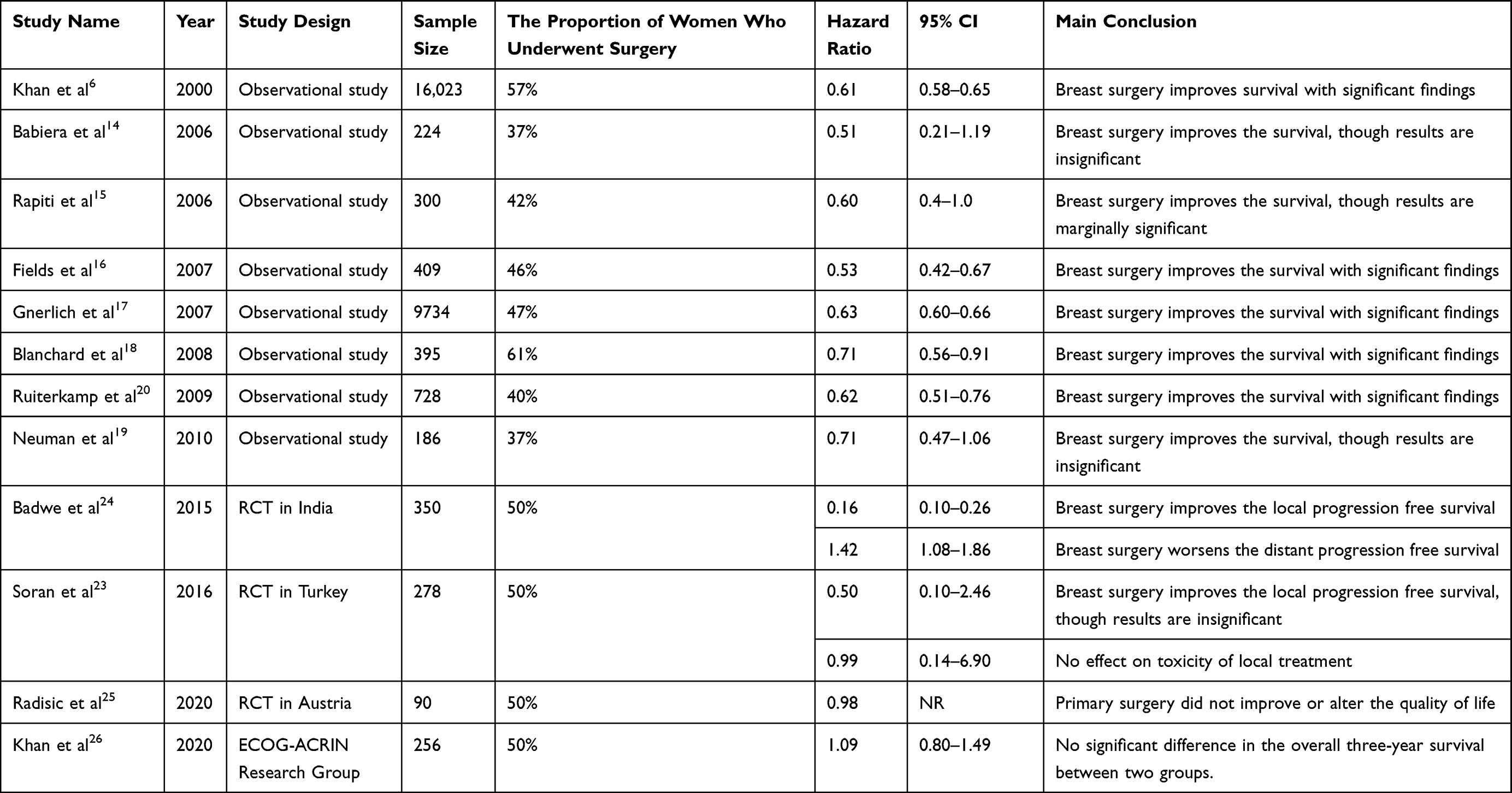 |
Table 2 Summary of Findings Regarding the Effectiveness of Locoregional Breast Surgery in Women Diagnosed with Metastatic Breast Cancer |
Likewise, in 2007, Fields et al undertook a study on 409 patients and 46% of women underwent surgery.16 Authors found that surgery improved survival by almost 50% with statistically significant results (HR: 0.53, 95% CI: 0.42 to 0.67). These findings were analogous to the study by Babiera et al, which provided evidence for the protective effect of breast surgery against mortality.14 This series of observational studies were followed by subsequent studies from 2006 to 2010 with almost consistent findings for the effect size of the hazard ratio. For instance, in 2007, Gnerlich et al undertook a huge study on 9734 women and 47% of them underwent surgery.17 Findings revealed that breast surgery reduces mortality by almost 40% with significant and reasonably precise results as indicated by narrow confidence intervals (HR: 0.63, 95% CI: 0.60 to 0.66).17 In the next year (2008), Blanchard found similar results, however, with wide 95% CIs most likely due to the small sample size of 395 (HR: 0.71, 95% CI: 0.56 to 0.91).18 These findings were confirmed by Ruiterkam et al and Neuman et al, where surgery was found to reduce mortality by almost 30% to 40%. However, as opposed to Ruiterkam et al (HR: 0.62, 95% CI: 0.51 to 0.76), Neuman et al did not find statistically significant results (HR: 0.71, 95% CI: 0.47 to 1.06).19,20 These results are analogous to subsequent retrospective studies conducted during the same decade, which provide similar conclusions about the role of breast surgery in improving the survival of women diagnosed with metastatic cancer.21,22
Indication of Locoregional Surgery (Breast and Axilla) in Metastatic Breast Cancer: Findings from Interventional Studies
While the observational studies suggest the protective role of surgery in metastatic cancer, these studies are not free of limitations. Due to limitations of internal threats to validity resulting from selection and information bias, and unmeasured confounding, it is crucial to review the evidence from interventional studies before making any firm conclusions. This is because randomized controlled trials (RCTs) control for known and unknown confounders and such designs are considered the ideal and gold standard to address the issues of unmeasured confounding. Recently, only four RCTs are conducted to compare the locoregional surgery plus systematic treatment against only systematic treatment in improving the survival, quality of life, local progression-free survival, distant progression-free survival, breast cancer-specific mortality, and toxicity due to local treatment among women diagnosed with metastatic breast cancer.23,24 If we apply the PICOS framework to such RCTs, the population would be women diagnosed with breast cancer, intervention would be breast surgery plus systematic treatment, the comparison would be systematic treatment, the outcome is the survival or mortality, and setting would be inpatient or outpatient departments. For example, Badwe et al and Soran et al undertook two RCTs on 624 women in 2015 and 2016, respectively, to compare the breast surgery plus systematic treatment with only systematic treatment (Table 2).
Badwe et al conducted a study in India on women who responded to systematic therapy initially,24 whereas Soran et al carried out a study on women without any previous systematic treatment.23 Authors found that overall survival at two years improved by almost 20% in the intervention group; however, results were not statistically significant (HR: 0.83, 95% CI: 0.53 to 1.31).23,24 The risk of death was 511 per 1000 in the comparison group, whereas it was 448 per 1000 in the intervention group with a range of 318 to 608 per 1000.23,24 However, the authors did not report the quality of life as an outcome of interest.23,24 Regarding local progression-free survival at two years, findings were statistically significant (HR: 0.22, 95% CI: 0.08 to 0.57), which reveals that breast surgery improved the local progression-free survival by almost 80%.23,24 However, the results were inverse for the distant progression-free survival (HR: 1.42, 95% CI: 1.08 to 1.86), which indicate that surgery may worsen the distant progression-free survival.24 On the other hand, Radisic et al published an RCT in 2020 to compare the effect of primary surgery on patient-reported quality of life versus no surgery among women with metastatic breast cancer.25 Authors randomized 90 women to either surgery or a systematic therapy without surgery.25 The study demonstrated no statistically significant difference in the quality of life as reported by the patients between the intervention and control group.25 The authors concluded that primary surgery neither improves nor deteriorates the quality of life (Table 2). In 2020, a multi-center trial was conducted on 256 patients diagnosed with stage IV breast cancer who already had undergone systematic therapy for 4 to 8 weeks and were randomized to either systemic therapy or local surgery with or without radiation followed by resuming the systematic therapy.26 The authors did not find any difference in the three-year survival between the two groups (HR: 1.09, 95% CI: 0.80 to 1.49). Although women receiving only systematic therapy were at a higher risk of locoregional progression, they experienced almost equal or even better quality of life-related outcomes when compared with women receiving local surgery.26 Another trial by Eastern Cooperative Oncology Group ‐ USA is not completed yet and probably will end by 2025. This trial compares early surgery against standard palliative therapy to treat women with advanced breast cancer. Based on the findings from limited RCTs with inconsistent findings, it is unclear whether breast surgery is effective for metastatic breast cancer until evidence is drawn from more well-designed and well-executed RCTs in the future on the larger sample size.
Sites of Metastasis in Breast Cancer and Evidence for the Indication of Surgery of Metastatic Site
There could be various sites where breast cancer can spread such as the brain, eyes, bones, lungs, liver, ovaries, and gastrointestinal tract. Metastasis to these sites is sometimes considered an emergency, leading to making decisions about surgically removing the metastatic site. However, the evidence to perform surgery or provide any other treatment differ by the site of metastasis. For example, for patients with metastasis to the brain, surgical resection, stereotactic radiosurgery, or radiotherapy of the whole brain should be considered regardless of the patient is having symptoms or not.27 However, this should be done either before or concurrently with systematic treatment. However, there are some exceptions to this for selected patients with restricted intracranial disease due to HER2-positive breast cancer, where only systematic therapy may be considered an option in some cases. Meanwhile, radiation therapy is used for patients with multiple metastatic deposits or extensive leptomeningeal disease. However, for patients with the limited intracranial disease, stereotactic radiosurgery is used whenever possible rather than the radiation of the whole brain to reduce the risk of toxicity.28
On the other hand, metastasis involving ophthalmic structures ranges from 5% to 38%, with the commonly involved site in metastatic breast cancer being choroid followed by iris, optic nerve, orbital bone, retina, extraocular muscles, vitreous body, ciliary body, an optical disc.29,30 There should be multidisciplinary decisions for local therapy when metastasis involves choroid.31 In case of metastasis involving ophthalmic structures, a brain CT scan and MRI are also recommended to figure out any concurrent brain metastasis. As far as treatment options for choroidal metastasis are concerned, there are various options. For example, among asymptomatic patients, systematic therapy with careful follow-up and observation is recommended. Whereas, in symptomatic patients, palliative external-beam radiation therapy after sparing the lens and the anterior chamber is considered a safe and effective therapy. For instance, evidence from a prospective study conducted in Germany revealed that visual function improved in 36% of the patients and stabilized in 50% among those who were treated with external-beam radiation therapy (40 Gy) after being diagnosed with choroidal metastasis.32 On the follow-up of these patients, complete and partial regression was documented in 38% and 44% of the patients, respectively. Likewise, short courses of external-beam radiation therapy may also be useful and improve the visual symptoms and visual acuity as found in one observational study on 123 patients. Other local treatment alternatives could be plaque brachytherapy, proton therapy, or intravitreal injection of anti-vascular endothelial growth factors.33 However, the data on these therapies are limited and based on case reports or case series.33
In case of metastasis to bone, indications for local treatment include any bone disease or pathologic fracture, compression of the spinal cord, decreased movement or pain, and disability. Bony metastasis usually responds well to systematic therapy and for asymptomatic patients without evidence of impending fracture, there is no clear evidence and role for resection. However, in the case of painful metastasis, a large body of literature supports the use of the short course, local-fixed external-beam radiation therapy in single or multiple fractions.34,35 Similarly, metastasis to the lungs typically does not need to be intervened locally until patients develop some life-threatening symptoms due to internal or external obstruction to superior vena cava where local treatments may benefit.36–38 In some cases, pulmonary resection can be done for diagnostic as well as palliative purposes because solitary pulmonary nodules may not be actually breast cancer metastasis. There is no valid and robust data suggestive of resecting the pulmonary tissues in case of metastatic breast cancer except date from case series suggest that it may improve 5-year survival from 30% to 80%, and median survival duration may increase from 40 to 100 months among selective breast cancer patients.39–42 Findings from a meta-analysis on 2000 patients documented a 5-year survival rate of 46% after resecting isolated metastasis of lung tissue.43
In case of metastasis to the liver, where more than 50% of the breast cancer can metastasize and most likely present with the disseminated disease with poor prognosis than metastasis to bones or soft tissues with 5% to 10% have isolated involvement of liver.44,45 Usually, local management of liver metastasis is done in case symptoms such as pain, bleeding not treated by medical therapy, or in case of biliary obstruction. However, sometimes local resection is done in symptomless patients, despite the absence of any prospective data comparing systematic treatment with the local treatment. Typically, the local treatment includes hepatic resection and stereotactic body radiation therapy to ablate liver metastasis after evaluating the patient carefully. For peripheral lesions more than 5 cm, surgery can be sometimes useful in preserving the liver function than stereotactic body radiation therapy. However, for central lesions, stereotactic body radiation therapy may work better. Further, the retrospective studies suggest local efficacy of radiofrequency ablation, mainly for hepatic lesions that are solitary and smaller than 3cm, not close to the diaphragm, biliary structure, and major vessels.46–48 The findings of the systematic review of 19 retrospective studies (n = 535 patients) where hepatectomy was performed for metastatic breast cancer.49 The results showed that median overall survival was 40 months, five-year survival was 40%, and postoperative mortality was 0% to 6%.49 However, in a subsequent case-control study of 167 patients, overall survival between those who received surgery and/or ablation was not different from those who were treated medically. The findings indicated that local treatment may offer a significant time of disease-free survival and time from systematic chemotherapy among patients with favorable risk-disease.50
Lastly, the gastrointestinal tract is usually less likely affected by metastasis, and organs such as the stomach and colon are involved followed by the esophagus and small intestine.51 The choice of local procedure in case of gastrointestinal tract metastasis should be done with the multidisciplinary approach after reviewing the patient’s symptoms, clinical indications, and ruling out other conditions such as primary tumor of the gastrointestinal tract, lymphoma, or any other benign disease. Similarly, ovaries are also a rare site for breast cancer metastasis.52 Oophorectomy may provide a beneficial therapeutic effect for premenopausal patients with hormone receptor-positive breast cancer irrespective of metastatic disease to the ovaries is present or not. There are limited data available regarding the local management of ovarian metastasis. In a series of 147 patients with ovarian metastasis, overall median survival was 41 months following ovarian metastasectomy.53
Discussion
This narrative review provides insights into the role of breast surgery in metastatic breast cancer by synthesizing findings from both observational and interventional studies. The findings from the review of observational studies the beneficial effects of breast surgery in improving the survival of women diagnosed with metastatic breast cancer. These findings are consistent across all retrospective studies included in the narrative review with variation in statistical significance, which may be due to differences in the sample size. Despite the consistent evidence from observational studies, critics consider this as low quality of evidence because of substantial bias associated with observational studies. Regardless of this criticism, a possible explanation for such findings or mechanism by which breast surgery may work is because the primary breast tumor is perhaps a reservoir of tumor cells and can be a source of more cells that can grow and dislodge to other tissues.54 Therefore, removal of primary breast tumor may reduce the probability of generating new metastasis, thereby improving survival. Besides, the tumor cells may produce growth factors, which can trigger signals that may help the growth of metastatic sites.55 The evidence from animal studies suggests that resection of the primary tumor may result in a decline in the growth of metastatic tumors.56
Contrary to this, the evidence from very few RCTs is limited and inconclusive. The findings of the RCTs reveal that breast surgery may improve the two-year survival, local progression-free survival but may not improve the distant progression-free survival and quality of life. Thus, without robust evidence drawn from several RCTs, it is hard to make definite conclusions on the benefits and risks of breast cancer surgery for metastatic breast cancer. Also, the existing evidence is clueless about the breast-specific survival and evidence for toxicity from local treatment does not differ across two groups that only comes from one RCT. Further, women diagnosed with metastatic breast cancer are not a homogenous group of patients rather they differ from each other based on prognoses. It is possible that women with minimal metastasis may have better survival than women whose multiple organs are affected by metastasis.24 This suggests that RCTs need to be conducted from different countries rather than relying on data from one or a few countries. This is because women in developed countries may be diagnosed at an earlier stage with minimal metastasis, whereas women from developing countries may be diagnosed with multiple organ metastasis. This may affect the results of surgery in two groups of women, therefore, generalizing findings from a few RCTs to all women may not be warranted.
Summary of the Current Guidelines (National Comprehensive Cancer Network (NCCN) and European Society for Medical Oncology (ESMO) in Metastatic Breast Cancer
Survival of patients diagnosed with metastatic breast cancer is increasing as a result of new treatment modalities; therefore, patients should be given optimal treatment to control their symptoms and provide spiritual and psychological support.57 Typically, such patients are treated with systematic therapy, but this can be given along with locoregional surgery after evaluating the disease status of the patients. Generally, the guidelines recommend taking a multidisciplinary approach for the adequate management of metastatic breast cancer. According to ESMO clinical practice guidelines, treatment decisions of these patients should not depend upon the patient’s age; however, patients’ comorbid, and preferences need to be taken into account by taking a joint multidisciplinary approach.58 Besides, supportive care should be considered in the overall treatment plan of ABC along with palliative care to control the symptoms of patients.58 Therapeutic decisions need to be made in a multidisciplinary context for patients who are newly diagnosed with stage IV breast cancer with intact primary tumor. In the absence of symptomatic local disease, locoregional treatment of the primary tumor is not beneficial to improve overall survival and therefore is not recommended in routine.58 Among patients experiencing local symptoms due to primary tumor or metastasis, there is a need to evaluate the use of local treatment approaches.58 The resection of the primary tumor may be considered for those patients who are diagnosed with metastasis to bones only, HER2-negative tumors, patients younger than 55 years of age, patients who are diagnosed with HR-positive tumors, patients with oligometastatic disease, and those who respond well to initial systematic therapy.58 Further, for patients diagnosed with advanced breast cancer (ABC), this includes both inoperable locally advanced breast cancer and metastatic breast cancer.59 The ABC guidelines, jointly developed by ESMO and The European School of Oncology (ESO), are endorsed by multiple international organizations and have been recently updated with the details of treatment modalities after assessing the symptoms, pathology reports, and other workups of the patient.59 These guidelines are based on the principle of equal access to multidisciplinary and specialized care including anticancer care, palliative and end-of-life care with full implementation of guidelines tailored to the needs of the patients.59
Conclusion and Implications for Future Research
The observational studies suggest the beneficial effect of breast surgery in metastatic breast cancer; however, the evidence from RCTs is very limited and inconclusive. Without having firm evidence from RCTs, it is hard to make any conclusions about the benefits of breast surgery because observational studies are usually affected by issues of selection bias and unmeasured confounding. Until the data from large ongoing RCTs is obtained, the decision to perform surgery on a woman diagnosed with metastatic breast cancer should be individualized. Both patient and physician need to decide together about the treatment keeping the risks, benefits, and costs of each intervention in mind. Due to a dearth of robust evidence, future RCTs with larger sample sizes should be carried out both in developing and developed countries, and these RCTs should separately analyze the group of women who are symptomatic versus non-symptomatic or they are provided with systematic therapy or not before the surgery. Also, one needs to consider HER2-positive breast cancer with metastasis and compare the outcomes separately for those who either did or did not obtain anti-HER2 treatment.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to it not directly involving human subjects (secondary research study).
Informed Consent Statement
The study itself was a review article and did not involve human subjects and hence patient consent was waived.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University for funding this work through large group Research Project under grant number RGP2/263/44.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Parks R, Derks M, Bastiaannet E, Cheung K. Breast cancer epidemiology. In: Breast Cancer Management for Surgeons. Springer; 2018:19–29.
2. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. doi:10.3322/caac.21208
3. DeSantis CE, Fedewa SA, Goding Sauer A, Kramer JL, Smith RA, Jemal A. Breast cancer statistics, 2015: convergence of incidence rates between black and white women. CA Cancer J Clin. 2016;66(1):31–42. doi:10.3322/caac.21320
4. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E86. doi:10.1002/ijc.29210
5. Robb GL, Hortobagyi GN. Advanced therapy of breast disease: PMPH-USA; 2004.
6. Khan SA, Stewart AK, Morrow M. Does aggressive local therapy improve survival in metastatic breast cancer? Surgery. 2002;132(4):620–6; discussion 6–7. doi:10.1067/msy.2002.127544
7. Ly BH, Nguyen NP, Vinh-Hung V, Rapiti E, Vlastos G. Loco-regional treatment in metastatic breast cancer patients: is there a survival benefit? Breast Cancer Res Treat. 2010;119(3):537–545. doi:10.1007/s10549-009-0610-z
8. Giordano SH, Buzdar AU, Smith TL, Kau SW, Yang Y, Hortobagyi GN. Is breast cancer survival improving? Cancer. 2004;100(1):44–52. doi:10.1002/cncr.11859
9. Thomas A, Khan SA, Chrischilles EA, Schroeder MC. Initial surgery and survival in stage IV breast cancer in the United States, 1988–2011. JAMA Surg. 2016;151(5):424–431. doi:10.1001/jamasurg.2015.4539
10. Sales C, Paiva L, Scandiuzzi D, Anjos AC. Quality of life of breast cancer survivors: social functioning. Rev Bras Cancerol. 2011;47(3):263–272. doi:10.32635/2176-9745.RBC.2001v47n3.2304
11. Wang R, Zhu Y, Liu X, Liao X, He J, Niu L. The clinicopathological features and survival outcomes of patients with different metastatic sites in stage IV breast cancer. BMC Cancer. 2019;19(1):1091. doi:10.1186/s12885-019-6311-z
12. Ruiterkamp J, Ernst MFJ. The role of surgery in metastatic breast cancer. Eur J Cancer. 2011;47:S6–S22. doi:10.1016/S0959-8049(11)70142-3
13. Poscia A, Collamati A, Milovanovic S, et al. Methodological issues in the observational studies conducted in older population: a narrative review. Epidemiol Biostat Public Health. 2017;14(2):e12627–e.
14. Babiera GV, Rao R, Feng L, et al. Effect of primary tumor extirpation in breast cancer patients who present with stage IV disease and an intact primary tumor. Ann Surg Oncol. 2006;13(6):776–782. doi:10.1245/ASO.2006.03.033
15. Rapiti E, Verkooijen HM, Vlastos G, et al. Complete excision of primary breast tumor improves survival of patients with metastatic breast cancer at diagnosis. J Clin Oncol. 2006;24(18):2743–2749. doi:10.1200/JCO.2005.04.2226
16. Fields RC, Jeffe DB, Trinkaus K, et al. Surgical resection of the primary tumor is associated with increased long-term survival in patients with stage IV breast cancer after controlling for site of metastasis. Ann Surg Oncol. 2007;14(12):3345–3351. doi:10.1245/s10434-007-9527-0
17. Gnerlich J, Jeffe DB, Deshpande AD, Beers C, Zander C, Margenthaler JA. Surgical removal of the primary tumor increases overall survival in patients with metastatic breast cancer: analysis of the 1988–2003 SEER data. Ann Surg Oncol. 2007;14(8):2187–2194. doi:10.1245/s10434-007-9438-0
18. Blanchard DK, Shetty PB, Hilsenbeck SG, Elledge RM. Association of surgery with improved survival in stage IV breast cancer patients. Ann Surg. 2008;247(5):732–738. doi:10.1097/SLA.0b013e3181656d32
19. Neuman HB, Morrogh M, Gonen M, Van ZKJ, Morrow M, King TA. Stage IV breast cancer in the era of targeted therapy: does surgery of the primary tumor matter? Cancer. 2010;116(5):1226–1233. doi:10.1002/cncr.24873
20. Ruiterkamp J, Ernst M, Van de Poll-Franse L, Bosscha K, Tjan-Heijnen V, Voogd A. Surgical resection of the primary tumour is associated with improved survival in patients with distant metastatic breast cancer at diagnosis. Eur J Surg Oncol. 2009;35(11):1146–1151. doi:10.1016/j.ejso.2009.03.012
21. Cady B, Nathan N, Michaelson J, Golshan M, Smith B. Matched pair analyses of stage IV breast cancer with or without resection of primary breast site. Ann Surg Oncol. 2008;15(12):3384–3395. doi:10.1245/s10434-008-0085-x
22. Leung AM, Vu HN, Nguyen K-A, Thacker LR, Bear HD. Effects of surgical excision on survival of patients with stage IV breast cancer. J Surg Res. 2010;161(1):83–88. doi:10.1016/j.jss.2008.12.030
23. Soran A, Ozmen V, Ozbas S, et al. A randomized controlled trial evaluating resection of the primary breast tumor in women presenting with de novo stage IV breast cancer: Turkish Study (protocol MF07-01). Am J Clin Oncol. 2016;34:1005. doi:10.1200/JCO.2016.34.15_suppl.1005
24. Badwe R, Hawaldar R, Nair N, et al. Locoregional treatment versus no treatment of the primary tumour in metastatic breast cancer: an open-label randomised controlled trial. Lancet Oncol. 2015;16(13):1380–1388. doi:10.1016/s1470-2045(15)00135-7
25. Bjelic-Radisic V, Fitzal F, Knauer M, et al. Primary surgery versus no surgery in synchronous metastatic breast cancer: patient-reported quality-of-life outcomes of the prospective randomized multicenter ABCSG-28 positive trial. BMC Cancer. 2020;20(1):392. doi:10.1186/s12885-020-06894-2
26. Khan SA, Zhao F, Solin LJ, et al. A randomized Phase III trial of systemic therapy plus early local therapy versus systemic therapy alone in women with de novo stage IV breast cancer: a trial of the ECOG-ACRIN research group (E2108). Am J Clin Oncol. 2020;38:LBA2–LBA2. doi:10.1200/JCO.2020.38.18_suppl.LBA2
27. Loeffler JS, Wen P. Epidemiology, Clinical Manifestations, and Diagnosis of Brain Metastases. Waltham, MA: Google Scholar; 2018.
28. Loeffler JS, Wen P. Overview of the Treatment of Brain Metastases. Waltham, MA: Wolters Kluwer; 2020.
29. Wiegel T, Kreusel KM, Bornfeld N, et al. Frequency of asymptomatic choroidal metastasis in patients with disseminated breast cancer: results of a prospective screening programme. Br J Ophthalmol. 1998;82(10):1159–1161. doi:10.1136/bjo.82.10.1159
30. Mewis L, Young SE. Breast carcinoma metastatic to the choroid. Analysis of 67 patients. Ophthalmology. 1982;89(2):147–151. doi:10.1016/s0161-6420(82)34838-1
31. Georgalas I, Paraskevopoulos T, Koutsandrea C, et al. Ophthalmic metastasis of breast cancer and ocular side effects from breast cancer treatment and management: mini review. Biomed Res Int. 2015;2015:574086. doi:10.1155/2015/574086
32. Wiegel T, Bottke D, Kreusel KM, et al. External beam radiotherapy of choroidal metastases--final results of a prospective study of the German Cancer Society (ARO 95-08). Radiother Oncol. 2002;64(1):13–18. doi:10.1016/s0167-8140(02)00134-2
33. Mathis T, Jardel P, Loria O, et al. New concepts in the diagnosis and management of choroidal metastases. Prog Retin Eye Res. 2019;68:144–176. doi:10.1016/j.preteyeres.2018.09.003
34. Lutz S, Balboni T, Jones J, et al. Palliative radiation therapy for bone metastases: update of an ASTRO evidence-based guideline. Pract Radiat Oncol. 2017;7(1):4–12. doi:10.1016/j.prro.2016.08.001
35. Chow R, Hoskin P, Schild SE, et al. Single vs multiple fraction palliative radiation therapy for bone metastases: cumulative meta-analysis. Radiother Oncol. 2019;141:56–61. doi:10.1016/j.radonc.2019.06.037
36. Staren ED, Salerno C, Rongione A, Witt TR, Faber LP. Pulmonary resection for metastatic breast cancer. Arch Surg. 1992;127(11):1282–1284. doi:10.1001/archsurg.1992.01420110024006
37. Cahan WG, Castro EB. Significance of a solitary lung shadow in patients with breast cancer. Ann Surg. 1975;181(2):137–143. doi:10.1097/00000658-197502000-00002
38. Casey JJ, Stempel BG, Scanlon EF, Fry WA. The solitary pulmonary nodule in the patient with breast cancer. Surgery. 1984;96(4):801–805.
39. Friedel G, Pastorino U, Ginsberg RJ, et al. Results of lung metastasectomy from breast cancer: prognostic criteria on the basis of 467 cases of the international registry of lung metastases. Eur J Cardiothorac Surg. 2002;22(3):335–344. doi:10.1016/s1010-7940(02)00331-7
40. Planchard D, Soria JC, Michiels S, et al. Uncertain benefit from surgery in patients with lung metastases from breast carcinoma. Cancer. 2004;100(1):28–35. doi:10.1002/cncr.11881
41. Yoshimoto M, Tada K, Nishimura S, et al. Favourable long-term results after surgical removal of lung metastases of breast cancer. Breast Cancer Res Treat. 2008;110(3):485–491. doi:10.1007/s10549-007-9747-9
42. Meimarakis G, Rüttinger D, Stemmler J, et al. Prolonged overall survival after pulmonary metastasectomy in patients with breast cancer. Ann Thorac Surg. 2013;95(4):1170–1180. doi:10.1016/j.athoracsur.2012.11.043
43. Fan J, Chen D, Du H, Shen C, Che G. Prognostic factors for resection of isolated pulmonary metastases in breast cancer patients: a systematic review and meta-analysis. J Thorac Dis. 2015;7(8):1441–1451. doi:10.3978/j.issn.2072-1439.2015.08.10
44. Hoe AL, Royle GT, Taylor I. Breast liver metastases--incidence, diagnosis and outcome. J R Soc Med. 1991;84(12):714–716. doi:10.1177/014107689108401207
45. Atalay G, Biganzoli L, Renard F, et al. Clinical outcome of breast cancer patients with liver metastases alone in the anthracycline-taxane era: a retrospective analysis of two prospective, randomised metastatic breast cancer trials. Eur J Cancer. 2003;39(17):2439–2449. doi:10.1016/s0959-8049(03)00601-4
46. Veltri A, Gazzera C, Barrera M, et al. Radiofrequency thermal ablation (RFA) of hepatic metastases (METS) from breast cancer (BC): an adjunctive tool in the multimodal treatment of advanced disease. Radiol Med. 2014;119(5):327–333. doi:10.1007/s11547-013-0354-z
47. Pawlik TM, Izzo F, Cohen DS, Morris JS, Curley SA. Combined resection and radiofrequency ablation for advanced hepatic malignancies: results in 172 patients. Ann Surg Oncol. 2003;10(9):1059–1069. doi:10.1245/aso.2003.03.026
48. Livraghi T, Goldberg SN, Solbiati L, Meloni F, Ierace T, Gazelle GS. Percutaneous radio-frequency ablation of liver metastases from breast cancer: initial experience in 24 patients. Radiology. 2001;220(1):145–149. doi:10.1148/radiology.220.1.r01jl01145
49. Chua TC, Saxena A, Liauw W, Chu F, Morris DL. Hepatic resection for metastatic breast cancer: a systematic review. Eur J Cancer. 2011;47(15):2282–2290. doi:10.1016/j.ejca.2011.06.024
50. Sadot E, Lee SY, Sofocleous CT, et al. Hepatic resection or ablation for isolated breast cancer liver metastasis: a case-control study with comparison to medically treated patients. Ann Surg. 2016;264(1):147–154. doi:10.1097/sla.0000000000001371
51. Washington K, McDonagh D. Secondary tumors of the gastrointestinal tract: surgical pathologic findings and comparison with autopsy survey. Mod Pathol. 1995;8(4):427–433.
52. Quan ML, Fey J, Eitan R, et al. Role of laparoscopy in the evaluation of the adnexa in patients with stage IV breast cancer. Gynecol Oncol. 2004;92(1):327–330. doi:10.1016/j.ygyno.2003.10.026
53. Li W, Wang H, Wang J, L VF, Zhu X, Wang Z. Ovarian metastases resection from extragenital primary sites: outcome and prognostic factor analysis of 147 patients. BMC Cancer. 2012;12:278. doi:10.1186/1471-2407-12-278
54. Bland KI, Copeland EM, Klimberg VS, Gradishar WJ. The Breast E-Book: Comprehensive Management of Benign and Malignant Diseases. Elsevier Health Sciences; 2017.
55. Karnoub AE, Dash AB, Vo AP, et al. Mesenchymal stem cells within tumour stroma promote breast cancer metastasis. Nature. 2007;449(7162):557–563. doi:10.1038/nature06188
56. Danna EA, Sinha P, Gilbert M, Clements VK, Pulaski BA, Ostrand-Rosenberg S. Surgical removal of primary tumor reverses tumor-induced immunosuppression despite the presence of metastatic disease. Cancer Res. 2004;64(6):2205–2211. doi:10.1158/0008-5472.can-03-2646
57. Caswell-Jin JL, Plevritis SK, Tian L, et al. Change in survival in metastatic breast cancer with treatment advances: meta-analysis and systematic review. JNCI Cancer Spectr. 2018;2(4):pky062. doi:10.1093/jncics/pky062
58. Gennari A, André F, Barrios CH, et al. ESMO clinical practice guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol. 2021;32(12):1475–1495. doi:10.1016/j.annonc.2021.09.019
59. Cardoso F, Paluch-Shimon S, Senkus E, et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann Oncol. 2020;31(12):1623–1649. doi:10.1016/j.annonc.2020.09.010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.