")
Back to Journals » International Journal of General Medicine » Volume 12
Role of nurses and nurse practitioners in the recognition, diagnosis, and management of neurogenic orthostatic hypotension: a narrative review
Authors Biswas D, Karabin B, Turner D
Received 22 September 2018
Accepted for publication 11 February 2019
Published 1 May 2019 Volume 2019:12 Pages 173—184
DOI https://doi.org/10.2147/IJGM.S170655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Debashis Biswas,1 Beverly Karabin,2 Debra Turner3
1Neurology, Baptist Memorial Hospital-Memphis, Memphis, TN, USA; 2Cardiovascular Medicine, University of Toledo, Toledo, OH, USA; 3Autonomic Services, Semmes Murphey Clinic, Memphis, TN, USA
Abstract: Neurogenic orthostatic hypotension (nOH) is a sustained reduction in blood pressure (BP) upon standing that is caused by autonomic dysfunction and is common among patients with a variety of neurodegenerative disorders (eg, Parkinson’s disease, multiple system atrophy, pure autonomic failure). A systolic BP drop of ≥20 mmHg (or ≥10 mmHg diastolic) upon standing with little or no compensatory increase in heart rate is consistent with nOH. Symptoms of nOH include light-headedness, dizziness, presyncope, and syncope; these symptoms can severely impact patients’ activities of daily living and increase the likelihood of potentially dangerous falls. Because of their patient contact, nurses and nurse practitioners can play a key role in identifying and evaluating patients at risk for nOH. It is advisable to screen for nOH in patients presenting with one or more of the following characteristics: those who have disorders associated with autonomic failure, those with episodes of falls or syncope, those with symptoms upon standing, those who are elderly or frail, or those taking multiple medications. Initial evaluations should include questions about postural symptoms and measurement of orthostatic BP and heart rate. A review of medications for potential agents that can have hypotensive effects should be performed before initiating treatment. Treatment for nOH may include non-pharmacologic measures and pharmacologic therapy. Droxidopa and midodrine are approved by the US Food and Drug Administration for the treatment of symptomatic nOH and symptomatic OH, respectively. nOH is associated with the coexistence of supine hypertension, and the two disorders must be carefully managed. In conclusion, timely screening and diagnosis of patients with nOH can streamline the path to disease management and treatment, potentially improving patient outcomes.
Keywords: blood pressure, autonomic nervous system, screening, diagnosis
Plain language summary
People with Parkinson’s disease or other medical conditions related to nervous system problems may feel faint or dizzy when standing up. These symptoms can be caused by a medical condition called neurogenic orthostatic hypotension (nOH). nOH is caused when a person’s blood pressure drops too much when standing up after sitting or lying down. Many people who have nOH feel faint or dizzy, but others may feel tired, weak, nauseous (“feeling sick to your stomach”), have pain in their neck or shoulders, or have blurry vision when standing. Because of nOH symptoms, a person is at an increased risk of falling, which can potentially cause serious injury. nOH can also limit a person’s ability to do activities of daily living and/or impair their quality-of-life because they have difficulty maintaining an upright posture. Therefore, it is extremely important to recognize and treat the symptoms of nOH. If a person feels symptoms such as weakness or dizziness when standing up, he or she should talk with their health care provider (nurse or doctor). Their health care provider can easily test for nOH by asking questions about symptoms and taking blood pressure and heart rate measurements when lying or sitting down and standing up. If nOH is diagnosed, the health care provider can then discuss ways to reduce the symptoms. The first steps in treatment are lifestyle changes, such as drinking more water, increasing salt intake, and doing recumbent exercises. If these measures do not help, a medication may be prescribed.
Introduction
Orthostatic hypotension (OH) is defined as a sustained decrease in blood pressure (BP) upon standing. Specifically, after 3 minutes of standing (or 3 minutes of head-up tilt at 60° during tilt-table testing), a decrease of ≥20 mmHg in systolic BP or a decrease of ≥10 mmHg in diastolic BP indicates that a patient has OH.1 OH can result from reduced cardiac output or the failure of vasoconstrictor mechanisms from neurogenic or non-neurogenic pathologic factors.1–4 Importantly, OH symptoms can be caused or exacerbated by a variety of drugs, including vasodilators, dopamine agonists, diuretics, tricyclic antidepressants, and monoamine oxidase inhibitors.1,2 Use of these medications is one of the most common causes of OH. Other common non-neurogenic causes of OH include venous pooling, hypovolemia, and cardiac pump failure (Figure 1).2 Further, it is important to recognize that the prevalence of OH increases with age, with the observed OH prevalence in a prospective cohort study increasing from 5% in individuals aged 71–74 to 11% in individuals ≥85 years old.5
 | Figure 1 Causes of OH. Note: Data from these studies.2,3,10,21,80,81 Abbreviations: nOH, neurogenic orthostatic hypotension; OH, orthostatic hypotension; PDE5, phosphodiesterase type 5. |
Neurogenic orthostatic hypotension (nOH) is a type of OH caused by the failure of the autonomic nervous system to adequately respond to orthostatic stress.1,4 nOH frequently occurs in patients with a variety of neurologic conditions, including Parkinson’s disease (PD), multiple system atrophy (MSA), and pure autonomic failure.6 Comorbidity of nOH with these conditions can worsen negative effects on activities of daily living (ADL), quality-of-life, and health care costs.7–9 Diagnosis and management of nOH can mitigate some of these negative effects.8,9
In addition to patients with conditions causing autonomic failure as described above, there are other patients routinely encountered in clinical practice that may also be at risk for nOH and should be considered for screening.10 These include patients who are reaching developmental milestones (eg, adolescent and elderly patients, menopausal women) that affect the hypothalamic pituitary adrenal axis; patients with endocrine disorders such as diabetes, thyroid conditions, and Addison’s disease;10 patients who have experienced acute or chronic inflammatory conditions or traumatic brain injury;11,12 patients with Ehlers-Danlos syndrome;13 and those with long-standing poorly controlled hypertension or sleep apnea.14,15
Because of their interaction with patients, nurses and nurse practitioners are ideally positioned to screen for signs and symptoms of nOH. Recognition of the types of patients at risk for nOH and routine screening of these patients for nOH symptoms can facilitate more efficient diagnosis and management of the condition. This article provides a narrative review of the pathophysiology, prevalence, and signs and symptoms of nOH, as well as guidance for the diagnosis and management of this condition.
Methods
Source data
PubMed searches were conducted from April to August 2017 using the terms “orthostatic hypotension” or “neurogenic orthostatic hypotension” combined with “epidemiology,” “pathophysiology,” “supine hypertension,” “diagnosis,” “management,” “pharmacologic,” “non-pharmacologic,” “drug,” “fall,” or “treatment,” and were limited to the past 5 years and published in English. Additional references, some of which exceeded the 5-year time period of the PubMed searches, were identified while reviewing the articles identified in the original search. For this narrative review, specific importance was given to guidelines, consensus documents, opinions of relevant organizations, randomized controlled trials, and large retrospective database studies.
Pathophysiology of nOH
When a person rises from a supine position to a standing position, the blood distribution shifts to the lower extremities, with ≥500 mL pooling in the lower half of the body.16,17 This results in a decrease in BP and venous return.17,18 To compensate for this shift and maintain normal circulation and organ perfusion, baroreceptors in the carotid sinus and aortic arch initiate a signaling cascade that evokes a sympathetic response from the central nervous system.16,17,19 In the brain, the medulla sends a signal down the spinal cord to sympathetic postganglionic neurons, triggering the release of norepinephrine (NE).16,18 The release of NE stimulates vasoconstriction and increased cardiac contractility and heart rate (HR) (Figure 2). In healthy individuals, these responses restore normotension within a few seconds of standing.17 In patients with nOH, inadequate release of NE blunts this orthostatic response, resulting in a drop in BP and hypoperfusion of the brain.18,20 This hypoperfusion causes signature nOH symptoms such as dizziness or light-headedness, presyncope, and syncope; these symptoms put patients with nOH at greater risk for falls, and, consequently, fear of falling.18,21–23
 | Figure 2 Hemodynamics of postural change in healthy subjects and patients with nOH. Note: Data from these studies.18,82 Abbreviations: BP, blood pressure; HR, heart rate; NE, norepinephrine; nOH, neurogenic orthostatic hypotension. |
Prevalence of nOH
The mean age of patients with nOH is ~70 years.24 Prevalence estimates suggest that nOH is common in patients with a variety of neurodegenerative disorders.25 All patients with pure autonomic failure also have nOH.26,27 nOH prevalence is higher in patients with MSA (75%–81%) compared with PD (18%–58%) and dementia with Lewy bodies (42%–52%).25,28–32
Symptoms and clinical features of nOH
Common presenting symptoms of nOH include light-headedness, dizziness, and the sensation of blacking out upon standing. Patients with nOH may also present with falls that may or may not be preceded by syncope.21 Other non-specific symptoms associated with nOH include generalized weakness, lethargy, fatigue, nausea, leg buckling, orthostatic dyspnea (difficulty breathing due to ventilation perfusion mismatch), and visual blurring, as well as pain in the suboccipital, shoulder, and posterior cervical regions of the head and neck (called the “coat hanger” configuration or “coat hanger” headache; Figure 3).1,18,21
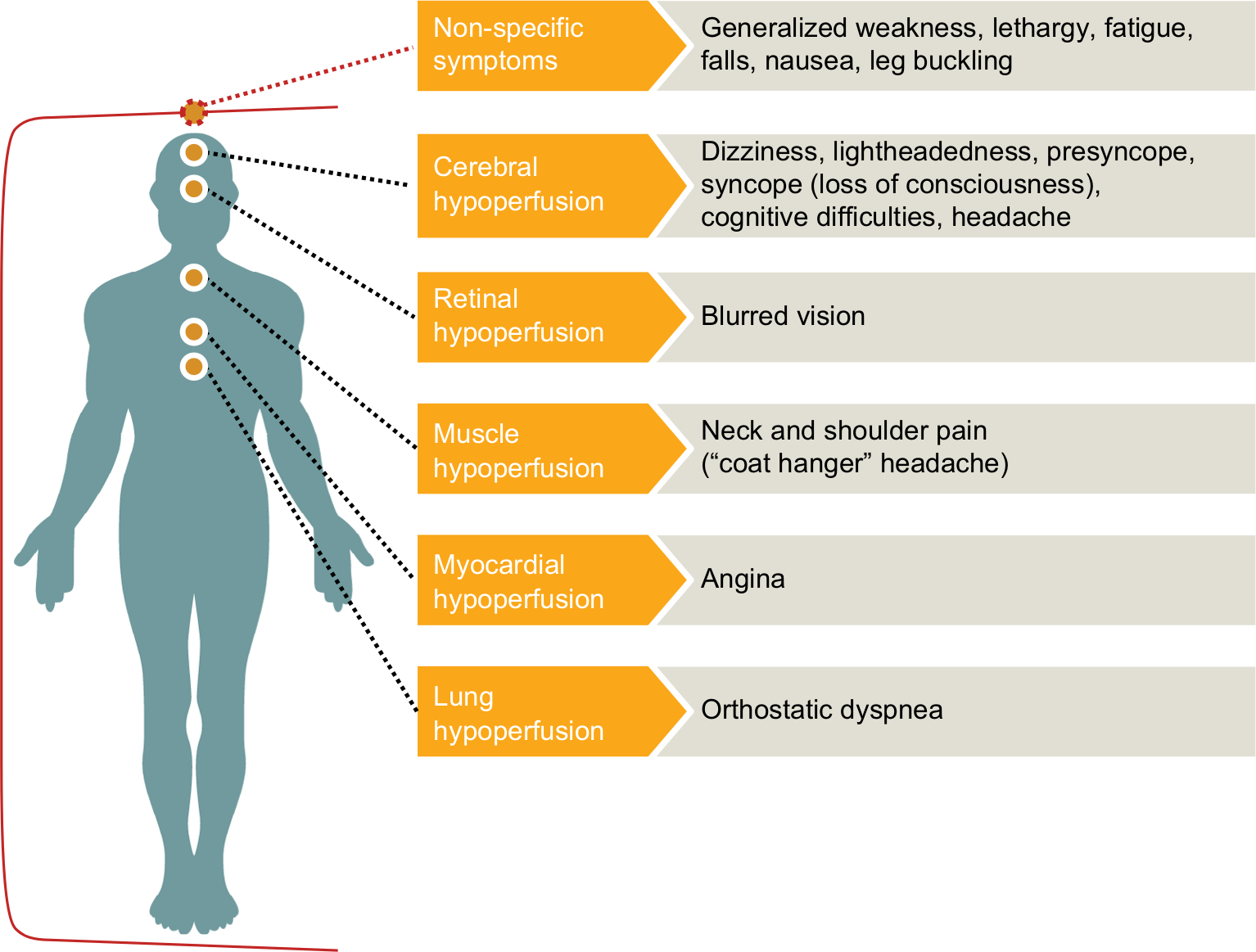 | Figure 3 Signs and symptoms of neurogenic orthostatic hypotension. |
Patients with nOH can also experience significant orthostatic reductions in cognitive function upon postural change.33 Poda et al33 performed cognitive function testing on adults with nOH in the 1) supine and 2) head-up position on a tilt table. All patients scored in the “normal” range in the supine position; however, patients performed significantly worse (P<0.005) in the head-up position, especially on tasks requiring executive function.33 This nOH “brain fog” is distinct from cognitive impairment caused by neurodegenerative disease, because all patients in the study scored normally on the Mini-Mental State Examination (part of the study’s inclusion criteria) and normally on cognitive testing when not under orthostatic stress.33
Some patients with nOH may demonstrate an orthostatic drop in BP without experiencing any obvious symptoms.34 These asymptomatic patients may meet the diagnostic criteria for OH (≥20 mmHg drop in systolic BP and ≥10 mmHg drop in diastolic BP) but not experience any symptoms of hypoperfusion, likely because orthostatic BP remains within the normal range despite the orthostatic drop. Conversely, some patients do not meet the criteria for OH, but have low mean BP (~75 mmHg) and thus experience some orthostatic symptoms.34
Impact of nOH on quality-of-life
nOH can have a significant negative impact on patients’ ability to function and on their quality-of-life.9 A recent survey of patients with PD, MSA, or pure autonomic failure and OH/nOH (or symptoms of OH/nOH) and their caregivers conducted by Harris Poll found that both patients (59%) and caregivers (75%) believed that patients’ nOH symptoms had a negative impact on their quality-of-life; 65% of caregivers and 40% of patients considered this impact “drastic.”9 In a questionnaire given to patients with PD, 53% reported that orthostatic dizziness had “a lot” or “very much” of an impact on their ADLs.7
A major consequence of symptomatic nOH is increased fall frequency. Fall rates in patients with PD range from 15% in mild PD to 58% in more severe PD;35 comorbid nOH also increases the risk of falling.23 In the Harris Poll survey, 57% of patients and 80% of caregivers reported a fall due to nOH symptoms in the past year.9 After adjusting for physical impairment, increased fall frequency correlated with a decreased ability to perform ADLs and frequency of physical activity, and increased percentage of limited ADLs, fatigue, and fear of falling.36 Fear of falling can severely impact a patient’s day-to-day functioning and quality-of-life, leading to immobilization. In turn, immobilization can lead to social isolation, more rapid disease progression, cognitive decline, depression, nursing home admission, and increased mortality.37,38
Health care costs for patients with nOH can be substantial. In patients with PD, comorbid nOH results in a 285% increase in days of hospitalization, a 156% increase in emergency room (ER) visits, and a 256% increase in overall health care costs in comparison with PD patients without nOH.8 Hospitalizations and ER visits to treat falls are also more common in PD patients with nOH.8 The estimated cost savings for avoiding a single fall (resulting in a moderate/major injury) is $24,866 (US dollars).39 The effect of nOH on patients’ quality-of-life and ADL and health care costs highlights the critical need for effective screening, identification, and management of nOH to mitigate the negative impact of this condition.
Screening and diagnosis of nOH
Screening for nOH in various care settings, although not an evidence-based practice, is strongly recommended based on expert clinical opinion. Stepwise screening for nOH includes asking key questions about patient symptoms, reviewing patient history including medications, and measuring BP and HR before and after postural change to evaluate potential causes of OH/nOH. If warranted, autonomic testing may be performed to confirm the autonomic origins of the condition. Nurses can play a key role in this screening process by recognizing which patients are at risk for OH/nOH and implementing most of the screening (eg, taking detailed patient history, noting relevant medications [eg, antihypertensives], performing BP testing). Most of this can be done in ~10 minutes, and could be incorporated into a clinic visit before consulting the physician. Efficient screening for and diagnosis of nOH can potentially improve the path to treatment and reduce the risk of serious complications (eg, syncope, falls).
Recommendations of a consensus panel concerning the screening, diagnosis, and treatment of nOH were published in 2017.21 The recommendations detail the types of patients who may be at higher risk of OH/nOH and could benefit from enhanced screening (Figure 4). Briefly, patients should be screened for orthostatic symptoms if they 1) have a neurodegenerative disorder or peripheral neuropathy related to autonomic dysfunction (eg, PD, MSA, pure autonomic failure, dementia with Lewy bodies), 2) have unexplained falls or syncope, 3) are ≥70 years old and frail or taking multiple medications, or 4) report any postural symptoms (eg, dizziness, other symptom) upon standing.21
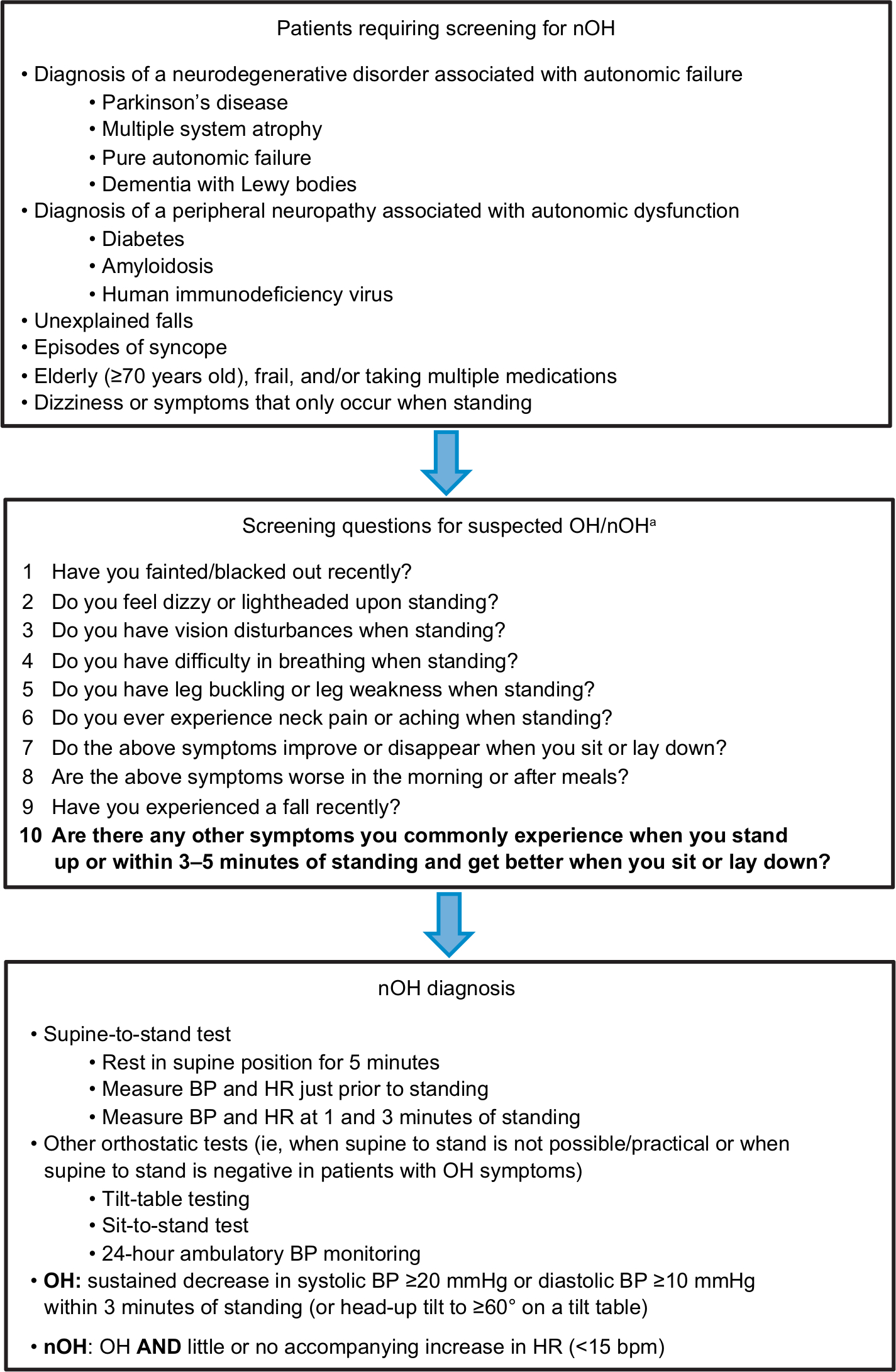 | Figure 4 Screening and diagnosis of nOH. Notes: Key question and diagnosis are presented in bold. aAny positive response should prompt further investigations with BP measurements. Partial data from Freeman et al.1 10 OH/nOH Screening Questions (middle box) adapted from Gibbons CH, Schmidt P, Biaggioni I, et al. The recommendations of a consensus panel for the screening, diagnosis, and treatment of neurogenic orthostatic hypotension and associated supine hypertension. J Neurol. 2017;264(8):1567–1582. Creative Commons license and disclaimer available from: http://creativecommons.org/licenses/by/4.0/.21 Abbreviations: BP, blood pressure; bpm, beats per minute; HR, heart rate; nOH, neurogenic orthostatic hypotension; OH, orthostatic hypotension. |
The consensus panel identified 10 targeted questions that may be used to efficiently recognize nOH symptoms (including type of symptom, frequency, and severity) and their impact on functionality (eg, ability to stand and perform ADLs).21 These 10 questions are provided in Figure 4. At minimum, the panel suggests that patients should be asked “Do you have symptoms when you stand up or within 3–5 minutes of standing that get better when you sit or lay down?”21 This question may be used when a detailed assessment of nOH symptoms is not practical.21 The next step is measurement of orthostatic BP. The patient should initially rest in the supine position for ≥5 minutes. The first BP measurement should be taken just before the patient stands. Additional BP measurements should be taken after the patient stands for 1 and then 3 minutes.21 A drop of ≥20 mmHg systolic BP and ≥10 mmHg diastolic BP upon standing meets the criteria for an OH diagnosis.21 Although the supine-to-stand test is the gold standard for orthostatic BP testing, some patients with limited mobility may require a modified protocol. The sit-to-stand test substitutes the seated position for the supine one, but otherwise follows the same protocol as the supine-to-stand test.21 However, it is important to note that the magnitude of BP drop may be smaller during a sit-to-stand test; for optimal sensitivity and specificity for sit-to-stand, a modified OH diagnostic cutoff (≥15 mmHg systolic, ≥7 mmHg diastolic) may be useful.40
Because OH may present differently depending on time of day, meals, hydration, and activity level, the consensus panel suggests that patients should also monitor BP and HR at home to create a 1-week BP/HR diary.21 Patients, their caregivers, or a nurse should measure supine-to-standing BP (or seated-to-standing BP) upon waking (before taking medications), when symptoms occur, and at bedtime.21 A recent study suggests that home BP monitoring (three consecutive measurements in the seated position followed by one in the standing position two times per day [upon waking and in the evening after dinner] for 3 consecutive days) may identify more cases of OH than a single, clinic-based, orthostatic BP test; these cases do not necessarily align with clinic-identified cases.41 When OH is suspected but not confirmed in the clinic, home BP monitoring or 24-hour ambulatory BP monitoring (with patient/caregiver annotation of postural changes) may be considered.21 In elderly patients, home 24-hour ambulatory BP monitoring may be preferable to continuous BP monitoring in the hospital setting because BP tends to be higher in the hospital than at home, resulting in misclassification of patients as hypertensive.42 Twenty-four-hour BP monitoring can detect OH, even when patients are asymptomatic, ensuring that clinicians implement an informed treatment plan and counsel patients and their caregivers on appropriate management.42
Evaluation of any change in HR from supine to standing (or seated to standing) can be useful to determine if OH could be neurogenic in origin. Among many patients with nOH, there is little to no compensatory increase in HR, despite the drop in BP.18 Although HR may increase slightly, especially in milder cases of nOH, these increases in HR do not correlate with the magnitude of the decrease in BP.43 When the patient’s HR increases proportionally (>15 beats per minute) upon standing but BP falls by ≥20/≥10 mmHg, the diagnosis may be non-neurogenic OH.44 Non-neurogenic causes of OH should be considered and excluded (Figure 1). Tachycardia upon standing in a patient with OH suggests dehydration, vasodilator use, or hemorrhage as a potential cause of symptoms.45,46
In some cases, patients may have nOH that is exacerbated by coexistent non-neurogenic causes (eg, use of concomitant medications with hypotensive effects).21 Consequently, expert opinion suggests that a full medication review should be completed by a nurse or other health care practitioner (HCP) for all patients with suspected or confirmed OH/nOH.21
The consensus panel suggests that a definitive diagnosis of nOH may be necessary when a patient reports serious, unexplained orthostatic symptoms (eg, syncope, falls) and standard testing does not reveal nOH. Specialized tests for this purpose usually require referral of patients to centers that specialize in autonomic disorders.21 These types of testing, including autonomic reflex testing (HR variation during paced breathing), HR and BP responses to a Valsalva maneuver, continuous BP response to prolonged head-up tilt testing, plasma-fractionated catecholamine levels, and sudomotor function testing, may aid in diagnosis.21,43
Despite the significant impact of nOH symptoms on patient quality-of-life, a Harris Poll survey found that only 36% of patients with OH or nOH symptoms reported a formal diagnosis of either condition. Once nOH was formally diagnosed, 70% of patients reported improved symptom management.9
Treatments for nOH
Although BP abnormalities are diagnostic, expert opinion suggests that normalization of postural BP is not the goal of therapy.47 Rather, the aims of nOH management are to reduce orthostatic symptoms generally, decrease the risk and incidence of syncope and falls, improve mobility and standing time, restore the ability to independently perform ADLs, and improve patient quality-of-life.21 It is usually not possible to achieve these management goals through pharmacologic treatment alone; HCPs should collaborate with patients to produce a management plan that includes several key lifestyle modifications as well as pharmacotherapy when necessary.21,48,49
Non-pharmacologic measures
As an initial management step, expert opinion suggests that a medication review should be conducted to identify agents that may cause OH or exacerbate nOH symptoms; if appropriate, such medications can be considered for discontinuation or dose reduction (Figure 1).21 Additionally, the patient should be evaluated for vitamin B12 deficiency or anemia; correction of either or both of these can help ameliorate orthostatic symptoms.21
As the next step, clinical consensus suggests that patient education and implementation of non-pharmacologic measures are generally appropriate (Table 1). Patients should be counseled to avoid factors that may induce OH symptoms, including hot environments, carbohydrate-rich meals, and strenuous exercise.21,50 Clinical observations suggest that patients can potentially improve orthostatic symptoms by increasing salt intake,21 maintaining hydration (specifically by drinking water and not other types of beverages),21 and elevating the head of the bed 6–9 inches by placing risers under the legs or headboard (stacked pillows are not sufficient).21 A recent study suggests bolus water ingestion before standing may be particularly effective in managing OH symptoms.51 Compression garments that include the abdominal region and physical counter-maneuvers may also prove helpful in managing orthostatic symptoms.51 Knee-high compression stockings are not effective alone, but inflatable or elastic abdominal binders may help ameliorate symptoms in the absence of leg compression, especially in hot environments where full compression stockings are not practical.21,51 Patients should also be counseled how to safely improve physical conditioning through low-impact exercise (eg, recumbent stationary bicycle, aquatic workouts, rowing machine).21
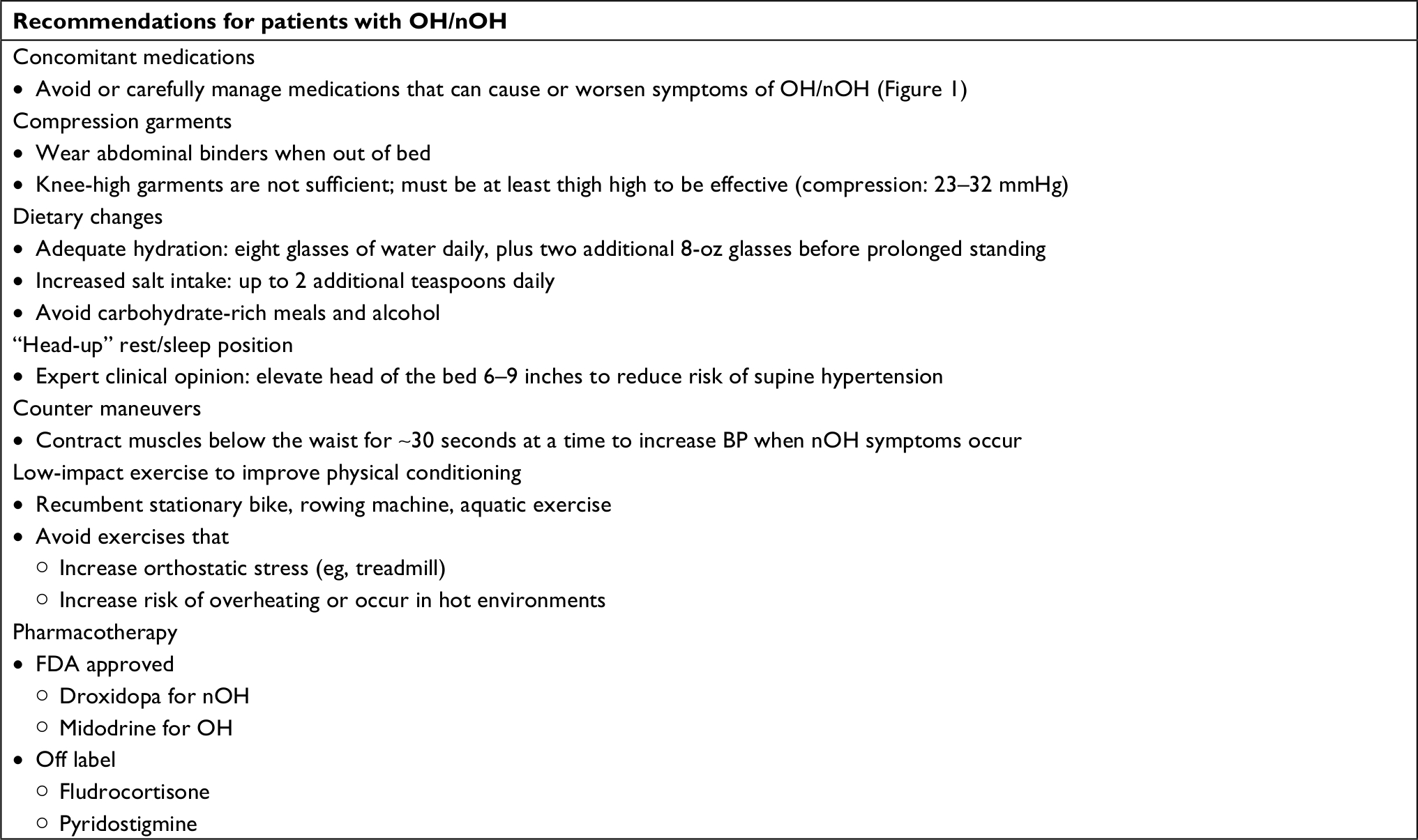 | Table 1 Options for the management of OH/nOH Note: Data from these studies.21,49,51 Abbreviations: BP, blood pressure; FDA, US Food and Drug Administration; nOH, neurogenic orthostatic hypotension; OH, orthostatic hypotension. |
Pharmacologic treatment
If nOH symptoms are not adequately managed by non-pharmacologic interventions, clinical consensus suggests that the use of pharmacotherapy may be necessary.21 Patients who are experiencing syncope, near-syncope, or falls may require first-line treatment with pharmacologic agents alongside non-pharmacologic measures.21 There are currently two drugs to treat OH/nOH symptoms approved by the US Food and Drug Administration (FDA): midodrine and droxidopa. Midodrine is approved for the treatment of OH symptoms and droxidopa is approved for the treatment of nOH symptoms.52,53
Midodrine
Midodrine acts through the α-adrenergic system to increase vascular tone and BP, effectively raising systolic and diastolic BP in supine, sitting, and standing positions.21,53 The prescribing information for midodrine suggests that administration of 10 mg can increase standing systolic BP by 15–30 mmHg in patients with OH symptoms.53 However, the evidence that midodrine significantly improves orthostatic symptoms is fairly weak.54–56 Standard dosing of midodrine begins with 2.5 mg up to three times daily (TID) at 3- to 4-hour intervals (doses upon waking, before lunch, and at mid-afternoon) and can be further titrated to 10 mg three times daily for maximum symptom relief.53 Because midodrine also increases supine BP, patients taking this drug are at increased risk of supine hypertension.53 Patients should not lie down within a few hours of each midodrine dose, and midodrine should not be taken within 4–5 hours of bedtime.53 Expert opinion suggests that, while taking midodrine, the supine position should be avoided during all rest; instead, the patient should always recline in a head-up position.21,53 Other common adverse events include piloerection, paresthesia, pruritus, and urinary retention.53
Droxidopa
Droxidopa was approved by the FDA in 2014 for the treatment of adults with symptomatic nOH resulting from PD, MSA, or pure autonomic failure.52 In randomized clinical trials, treatment with droxidopa resulted in significant improvement compared with placebo in a composite of nOH symptoms.57,58 These studies also demonstrated improvements in standing BP, dizziness/light-headedness, symptom impact on standing and walking, weakness, fatigue, and vision disturbance.57–59 In a randomized clinical trial of patients with PD and symptomatic nOH, fewer falls and fall-related injuries (eg, contusions, lacerations) were reported in patients receiving droxidopa compared with placebo.60 A 2016 meta-analysis of the safety and efficacy of droxidopa in nOH suggested droxidopa may have reduced efficacy after 8 weeks of treatment.61 However, in a subsequent 6-month, non-interventional, prospective study of patients with nOH, significant improvements in nOH symptoms, number of falls, functionality, and quality-of-life were reported with 1 month of droxidopa treatment, with data suggesting that the benefits persisted at 3 and 6 months following treatment initiation.62
Droxidopa dosing is initiated at 100 mg TID and can be titrated in increments of 100 mg TID until the patient experiences symptomatic relief, up to a maximum dose of 600 mg TID.52 Because food intake can affect droxidopa absorption, it should be taken consistently either with food or without food.63 Headache, dizziness, and fatigue are the most common adverse events.57–59 A recent meta-analysis indicated that midodrine significantly increases the risk of supine hypertension (risk ratio, 5.1), whereas droxidopa does not (risk ratio, 1.4).64 However, the prescribing information for droxidopa indicates a risk of supine hypertension, so caution is warranted. To minimize this risk, clinical opinion suggests that patients taking droxidopa should elevate the head of the bed, avoid resting in the supine position during the day, and avoid taking droxidopa within 5 hours of bedtime.21,52
Off-label treatments
The drugs fludrocortisone and pyridostigmine are not approved by the FDA to treat OH, but are commonly used off-label to treat this condition. Fludrocortisone increases intravascular blood volume and vascular resistance.65 Although clinical evidence of its efficacy is limited and, according to a recent meta-analysis, the quality of this evidence is low, some studies have found improvements in standing BP and other symptoms.66–68 Fludrocortisone can also increase the risk of supine hypertension as well as the risk of all-cause hospitalization in comparison with midodrine.21,50,69 Pyridostigmine is an acetylcholinesterase inhibitor that works by promoting cholinergic signaling at the sympathetic ganglia during orthostatic stress21 and shows some evidence of improving orthostatic symptoms.70 One distinct advantage of pyridostigmine is that it does not increase the risk of supine hypertension.21,70 Because its mechanism of action requires some function of the autonomic nervous system, expert clinical opinion suggests that it is more likely to be helpful for patients with mild cases of nOH.21
Supine hypertension in nOH
Patients with autonomic failure can experience overall large variations in BP throughout the day, resulting in OH when standing (ie, during the daytime) and supine hypertension when lying down (ie, at night; Figure 5).3,71 In a study of patients with PD, ~78% of patients with PD and nOH had a nocturnal BP pattern consistent with supine hypertension.72 Because many of the treatments for nOH increase the risk of supine hypertension, expert opinion suggests that it is critical to balance the opposing treatments for both conditions.21 Hypertension carries significant long-term risks, but the risks posed by nOH symptoms, particularly falls, can be immediate and potentially catastrophic.21 Falls are one of the most common causes of hospital admission among PD patients, and can lead to injury, fear of falling, and increased health care utilization and costs.8,73–75 However, studies have found associations between supine hypertension and both renal failure76 and left ventricular hypertrophy77 in patients with pure autonomic failure, all of whom also have nOH. The clinical decision regarding whether to treat nOH or supine hypertension more aggressively must necessarily vary by the individual patient.21
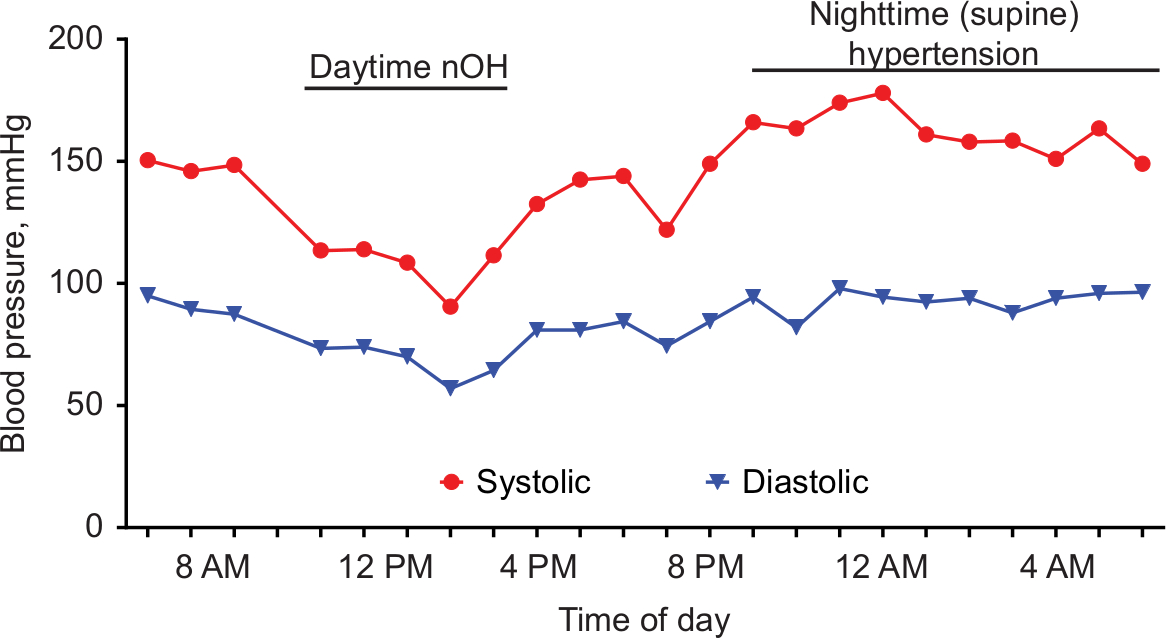 | Figure 5 24-Hour blood pressure variability in a patient with autonomic failure leading to daytime nOH and nighttime supine hypertension. Abbreviation: nOH, neurogenic orthostatic hypotension. |
Based on expert consensus, patients taking midodrine, droxidopa, or fludrocortisone should avoid a completely horizontal supine position whenever possible and should take the last dose of these drugs at least 5 hours before going to bed.21 Among patients with marked supine hypertension, a short-acting antihypertensive drug (eg, nitroglycerine patch, clonidine) can be taken in the evening to alleviate this symptom.78,79 However, patients taking antihypertensive medication in this manner should be cautioned that OH symptoms may be particularly pronounced during nighttime trips to the bathroom.21 These patients should also avoid diuretics and long-acting antihypertensive agents because both can exacerbate symptoms of nOH.21,78
Conclusion
Because nOH substantially affects patient quality-of-life, identifying individuals at risk for this condition should be a priority for medical professionals across specialties. Patients with nOH present commonly in many clinical settings, including primary care and general practices. Unfortunately, nOH may not be readily recognized because it is sometimes viewed as a condition that only autonomic specialists see. The recognition of nOH symptoms by nurses and nurse practitioners can facilitate screening and subsequent diagnosis and management, ultimately resulting in improvements in both clinical outcomes and quality-of-life.
Implementation of non-pharmacologic options to manage the symptoms of nOH is appropriate as an initial treatment approach. However, when non-pharmacologic management strategies do not adequately alleviate symptoms of nOH, pharmacologic treatment is warranted. It is important to screen patients with nOH for supine hypertension, a common comorbidity that may necessitate tailoring treatment approaches for each patient.
Abbreviations
ADL, activities of daily living; BP, blood pressure; ER, emergency room; FDA, US Food and Drug Administration; HCP, health care practitioner; HR, heart rate; MSA, multiple system atrophy; NE, norepinephrine; nOH, neurogenic orthostatic hypotension; OH, orthostatic hypotension; PD, Parkinson’s disease; TID, 3 times daily.
Acknowledgments
The authors received editorial assistance from CHC Group (North Wales, PA), which was supported by Lundbeck. Lundbeck, the manufacturer of droxidopa, provided funding for medical writing and editorial support in the development of this manuscript and reviewed a draft of the manuscript before submission. Draft versions of some figures in this manuscript have been presented in an electronic poster available as a members-only resource on the American Academy of Ambulatory Care Nursing website (https://www.aaacn.org/professional-development/poster-presentations/2018-poster-presentations).
Author contributions
All authors made substantial contributions to conception, drafting and critically revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
BK is a consultant and speaker for Lundbeck. DT is a speaker for Lundbeck. All authors report no other conflicts of interest in this work.
References
Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21(2):69–72. | ||
Goldstein DS, Sharabi Y. Neurogenic orthostatic hypotension: a pathophysiological approach. Circulation. 2009;119(1):139–146. | ||
Isaacson S, Skettini J. Neurogenic orthostatic hypotension in Parkinson’s disease: evaluation, management, and emerging role of droxidopa. Vasc Health Risk Manag. 2014;10:169–176. | ||
Ibrahim MM. Localization of lesion in patients with idiopathic orthostatic hypotension. Br Heart J. 1975;37(8):868–872. | ||
Masaki KH, Schatz IJ, Burchfiel CM, et al. Orthostatic hypotension predicts mortality in elderly men: the Honolulu Heart program. Circulation. 1998;98(21):2290–2295. | ||
Ejaz AA, Haley WE, Wasiluk A, Meschia JF, Fitzpatrick PM. Characteristics of 100 consecutive patients presenting with orthostatic hypotension. Mayo Clin Proc. 2004;79(7):890–894. | ||
Magerkurth C, Schnitzer R, Braune S. Symptoms of autonomic failure in Parkinson’s disease: prevalence and impact on daily life. Clin Auton Res. 2005;15(2):76–82. | ||
Merola A, Sawyer RP, Artusi CA, et al. Orthostatic hypotension in Parkinson disease: impact on health care utilization. Parkinsonism Relat Disord. 2018;47:45–49. | ||
Claassen DO, Adler CH, Hewitt LA, Gibbons C. Characterization of the symptoms of neurogenic orthostatic hypotension and their impact from a survey of patients and caregivers. BMC Neurol. 2018;18(1):125. | ||
Blum I, Barkan A, Yeshurun D. Thyrotoxicosis presenting as orthostatic hypotension. Postgrad Med J. 1980;56(656):425–426. | ||
Johansson M, Ricci F, Aung N, Sutton R, Melander O, Fedorowski A. Inflammatory biomarker profiling in classical orthostatic hypotension: insights from the SYSTEMA cohort. Int J Cardiol. 2018;259:192–197. | ||
Luther MS, Krewer C, Müller F, Koenig E. Orthostatic circulatory disorders in early neurorehabilitation: a case report and management overview. Brain Inj. 2007;21(7):763–767. | ||
Gazit Y, Nahir AM, Grahame R, Jacob G. Dysautonomia in the joint hypermobility syndrome. Am J Med. 2003;115(1):33–40. | ||
Shen S, He T, Chu J, He J, Chen X. Uncontrolled hypertension and orthostatic hypotension in relation to standing balance in elderly hypertensive patients. Clin Interv Aging. 2015;10:897–906. | ||
Guilleminault C, Faul JL, Stoohs R. Sleep-disordered breathing and hypotension. Am J Respir Crit Care Med. 2001;164(7):1242–1247. | ||
Smit AA, Halliwill JR, Low PA, Wieling W. Pathophysiological basis of orthostatic hypotension in autonomic failure. J Physiol. 1999;519 Pt 1:1–10. | ||
Wieling W, Groothuis JT. Physiology of upright posture. In: Robertson D, Biaggioni I, Burnstock G, Low PA, Paton JFR, editors. Primer on the Autonomic Nervous System. 3rd ed. London, UK: Academic Press; 2012:193–195. | ||
Freeman R. Clinical practice. Neurogenic orthostatic hypotension. N Engl J Med. 2008;358(6):615–624. | ||
Victor RG, Mark AL. Interaction of cardiopulmonary and carotid baroreflex control of vascular resistance in humans. J Clin Invest. 1985;76(4):1592–1598. | ||
Loavenbruck A, Sandroni P. Neurogenic orthostatic hypotension: roles of norepinephrine deficiency in its causes, its treatment, and future research directions. Curr Med Res Opin. 2015;31(11):2095–2104. | ||
Gibbons CH, Schmidt P, Biaggioni I, et al. The recommendations of a consensus panel for the screening, diagnosis, and treatment of neurogenic orthostatic hypotension and associated supine hypertension. J Neurol. 2017;264(8):1567–1582. | ||
Shaw BH, Claydon VE. The relationship between orthostatic hypotension and Falling in older adults. Clin Auton Res. 2014;24(1):3–13. | ||
van der Marck MA, Klok MPC, Okun MS, et al. Consensus-based clinical practice recommendations for the examination and management of falls in patients with Parkinson’s disease. Parkinsonism Relat Disord. 2014;20(4):360–369. | ||
Maule S, Milazzo V, Maule MM, Di Stefano C, Milan A, Veglio F. Mortality and prognosis in patients with neurogenic orthostatic hypotension. Funct Neurol. 2012;27(2):101–106. | ||
Ha AD, Brown CH, York MK, Jankovic J. The prevalence of symptomatic orthostatic hypotension in patients with Parkinson’s disease and atypical parkinsonism. Parkinsonism Relat Disord. 2011;17(8):625–628. | ||
Metzler M, Duerr S, Granata R, Krismer F, Robertson D, Wenning GK. Neurogenic orthostatic hypotension: pathophysiology, evaluation, and management. J Neurol. 2013;260(9):2212–2219. | ||
Kaufmann H. Consensus statement on the definition of orthostatic hypotension, pure autonomic failure and multiple system atrophy. Clin Auton Res. 1996;6(2):125–126. | ||
Senard JM, Rai S, Lapeyre-Mestre M, et al. Prevalence of orthostatic hypotension in Parkinson’s disease. J Neurol Neurosur Psychiatry. 1997;63(5):584–589. | ||
Köllensperger M, Geser F, Ndayisaba JP, et al. Presentation, diagnosis, and management of multiple system atrophy in Europe: final analysis of the European multiple system atrophy registry. Mov Disord. 2010;25(15):2604–2612. | ||
Thaisetthawatkul P, Boeve BF, Benarroch EE, et al. Autonomic dysfunction in dementia with Lewy bodies. Neurology. 2004;62(10):1804–1809. | ||
Allan LM, Ballard CG, Allen J, et al. Autonomic dysfunction in dementia. J Neurol Neurosurg Psychiatry. 2007;78(7):671–677. | ||
Sonnesyn H, Nilsen DW, Rongve A, et al. High prevalence of orthostatic hypotension in mild dementia. Dement Geriatr Cogn Disord. 2009;28(4):307–313. | ||
Poda R, Guaraldi P, Solieri L, et al. Standing worsens cognitive functions in patients with neurogenic orthostatic hypotension. Neurol Sci. 2012;33(2):469–473. | ||
Palma JA, Gomez-Esteban JC, Norcliffe-Kaufmann L, et al. Orthostatic hypotension in Parkinson disease: how much you fall or how low you go? Mov Disord. 2015;30(5):639–645. | ||
Rascol O, Perez-Lloret S, Damier P, et al. Falls in ambulatory non-demented patients with Parkinson’s disease. J Neural Transm (Vienna). 2015;122(10):1447–1455. | ||
Bryant MS, Rintala DH, Hou JG, Protas EJ. Relationship of falls and fear of falling to activity limitations and physical inactivity in Parkinson’s disease. J Aging Phys Act. 2015;23(2):187–193. | ||
Voermans NC, Snijders AH, Schoon Y, Bloem BR. Why old people fall (and how to stop them). Pract Neurol. 2007;7(3):158–171. | ||
Bloem BR, van Vugt JP, Beckley DJ. Postural instability and falls in Parkinson’s disease. Adv Neurol. 2001;87:209–223. | ||
François C, Hauser RA, Aballéa S, Dorey J, Kharitonova E, Hewitt LA. Cost-effectiveness of droxidopa in patients with neurogenic orthostatic hypotension: post-hoc economic analysis of phase 3 clinical trial data. J Med Econ. 2016;19(5):515–525. | ||
Shaw BH, Garland EM, Black BK, et al. Optimal diagnostic thresholds for diagnosis of orthostatic hypotension with a “sit-to-stand test”. J Hypertens. 2017;35(5):1019–1025. | ||
Cremer A, Rousseau A-Laure, Boulestreau R, Kuntz S, Tzourio C, Gosse P. Screening for orthostatic hypotension using home blood pressure measurements. J Hypertens. Epub 2018 Nov 9. doi: 10.1097/HJH.0000000000001986 | ||
Cappelleri C, Janoschka A, Berli R, et al. Twenty-four-hour ambulatory blood pressure monitoring in very elderly patients: comparison of in-hospital versus home follow-up results. Medicine (Baltimore). 2017;96(34):e7692. | ||
Palma JA, Kaufmann H. Epidemiology, diagnosis, and management of neurogenic orthostatic hypotension. Mov Disord Clin Pract. 2017;4(3):298–308. | ||
Shibao C, Lipsitz LA, Biaggioni I. Ash position paper: evaluation and treatment of orthostatic hypotension. J Clin Hypertens (Greenwich). 2013;15(3):147–153. | ||
Biaggioni I. Treatment: special conditions: orthostatic hypotension. J Am Soc Hypertens. 2015;9(1):67–69. | ||
Little RA, Kirkman E, Driscoll P, Hanson J, Mackway-Jones K. Preventable deaths after injury: why are the traditional ‘vital’ signs poor indicators of blood loss? J Accid Emerg Med J. 1995;12(1):1–14. | ||
Sharabi Y, Goldstein DS. Mechanisms of orthostatic hypotension and supine hypertension in Parkinson disease. J Neurol Sci. 2011;310(1–2):123–128. | ||
Arbique D, Cheek D, Welliver M, Vongpatanasin W. Management of neurogenic orthostatic hypotension. J Am Med Dir Assoc. 2014;15(4):234–239. | ||
Figueroa JJ, Basford JR, Low PA. Preventing and treating orthostatic hypotension: as easy as a, B, C. Cleve Clin J Med. 2010;77(5):298–306. | ||
Lahrmann H, Cortelli P, Hilz M, Mathias CJ, Struhal W, Tassinari M. EFNS guidelines on the diagnosis and management of orthostatic hypotension. Eur J Neurol. 2006;13(9):930–936. | ||
Newton JL, Frith J. The efficacy of nonpharmacologic intervention for orthostatic hypotension associated with aging. Neurology. 2018;91(7):e652–e656. | ||
Northera® (droxidopa). Full Prescribing Information. Deerfield, IL: Lundbeck; 2017. | ||
ProAmatine® (midodrine hydrochloride). Full Prescribing Information. Lexington, MA: Shire us Inc.; 2017. | ||
Logan IC, Witham MD. Efficacy of treatments for orthostatic hypotension: a systematic review. Age Ageing. 2012;41(5):587–594. | ||
Izcovich A, González Malla C, Manzotti M, Catalano HN, Guyatt G. Midodrine for orthostatic hypotension and recurrent reflex syncope: a systematic review. Neurology. 2014;83(13):1170–1177. | ||
Parsaik AK, Singh B, Altayar O, et al. Midodrine for orthostatic hypotension: a systematic review and meta-analysis of clinical trials. J Gen Intern Med. 2013;28(11):1496–1503. | ||
Biaggioni I, Freeman R, Mathias CJ, et al; Droxidopa 302 Investigators. Randomized withdrawal study of patients with symptomatic neurogenic orthostatic hypotension responsive to droxidopa. Hypertension. 2015;65(1):101–107. | ||
Kaufmann H, Freeman R, Biaggioni I, et al. Droxidopa for neurogenic orthostatic hypotension: a randomized, placebo-controlled, phase 3 trial. Neurology. 2014;83(4):328–335. | ||
Hauser RA, Isaacson S, Lisk JP, Hewitt LA, Rowse G. Droxidopa for the short-term treatment of symptomatic neurogenic orthostatic hypotension in Parkinson’s disease (NOH306B). Mov Disord. 2015;30(5):646–654. | ||
Hauser RA, Heritier S, Rowse GJ, Hewitt LA, Isaacson SH. Droxidopa and reduced falls in a trial of Parkinson disease patients with neurogenic orthostatic hypotension. Clin Neuropharmacol. 2016;39(5):220–226. | ||
Elgebaly A, Abdelazeim B, Mattar O, Gadelkarim M, Salah R, Negida A. Meta-analysis of the safety and efficacy of droxidopa for neurogenic orthostatic hypotension. Clin Auton Res. 2016;26(3):171–180. | ||
Kymes S, François C, McLeod K, et al. Prospective study of real-world outcomes in the treatment of neurogenic orthostatic hypotension with droxidopa. Neurology. 2017;66(16 suppl 1):P5.319. | ||
Chen JJ, Hewitt LA. Comparison of the pharmacokinetics of droxidopa after dosing in the fed versus fasted state and with 3-times-daily dosing in healthy elderly subjects. Drugs R D. 2018;18(1):77–86. | ||
Chen JJ, Han Y, Tang J, Portillo I, Hauser RA, Dashtipour K. Standing and supine blood pressure outcomes associated with droxidopa and midodrine in patients with neurogenic orthostatic hypotension: a Bayesian meta-analysis and mixed treatment comparison of randomized trials. Ann Pharmacother. 2018;52(12):1182–1194. | ||
National Institutes of Health, US National Library of Medicine. Label: fludrocortisone acetate – fludrocortisone acetate tablet. Available from: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=4ed382df-f2d5-46a4-a68b-aba807777093. Accessed February 16, 2018. | ||
Eschlböck S, Wenning G, Fanciulli A. Evidence-based treatment of neurogenic orthostatic hypotension and related symptoms. J Neural Transm (Vienna). 2017;124(12):1567–1605. | ||
Matsubara S, Sawa Y, Yokoji H, Takamori M. Shy-Drager syndrome. Effect of fludrocortisone and L-threo-3,4-dihydroxyphenylserine on the blood pressure and regional cerebral blood flow. J Neurol Neurosurg Psychiatry. 1990;53(11):994–997. | ||
Schoffer KL, Henderson RD, O’Maley K, O’Sullivan JD. Nonpharmacological treatment, fludrocortisone, and domperidone for orthostatic hypotension in Parkinson’s disease. Mov Disord. 2007;22(11):1543–1549. | ||
Grijalva CG, Biaggioni I, Griffin MR, Shibao CA. Fludrocortisone is associated with a higher risk of all-cause hospitalizations compared with midodrine in patients with orthostatic hypotension. J Am Heart Assoc. 2017;6(10):e006848. doi: 10.1161/JAHA.117.006848 | ||
Singer W, Sandroni P, Opfer-Gehrking TL, et al. Pyridostigmine treatment trial in neurogenic orthostatic hypotension. Arch Neurol. 2006;63(4):513–518. | ||
Senard JM, Chamontin B, Rascol A, Montastruc JL. Ambulatory blood pressure in patients with Parkinson’s disease without and with orthostatic hypotension. Clin Auton Res. 1992;2(2):99–104. | ||
Berganzo K, Díez-Arrola B, Tijero B, et al. Nocturnal hypertension and dysautonomia in patients with Parkinson’s disease: are they related? J Neurol. 2013;260(7):1752–1756. | ||
Tan LC, Tan AK, Tjia HT. The profile of hospitalised patients with Parkinson’s disease. Ann Acad Med Singapore. 1998;27(6):808–812. | ||
Woodford H, Walker R. Emergency hospital admissions in idiopathic Parkinson’s disease. Mov Disord. 2005;20(9):1104–1108. | ||
Rudzińska M, Bukowczan S, Stożek J, et al. Causes and consequences of falls in Parkinson disease patients in a prospective study. Neurol Neurochir Pol. 2013;47(5):423–430. | ||
Garland EM, Gamboa A, Okamoto L, et al. Renal impairment of pure autonomic failure. Hypertension. 2009;54(5):1057–1061. | ||
Vagaonescu TD, Saadia D, Tuhrim S, Phillips RA, Kaufmann H. Hypertensive cardiovascular damage in patients with primary autonomic failure. Lancet. 2000;355(9205):725–726. | ||
Espay AJ, LeWitt PA, Hauser RA, Merola A, Masellis M, Lang AE. Neurogenic orthostatic hypotension and supine hypertension in Parkinson’s disease and related synucleinopathies: prioritisation of treatment targets. Lancet Neurol. 2016;15(9):954–966. | ||
Baker J, Kimpinski K. Management of supine hypertension complicating neurogenic orthostatic hypotension. CNS Drugs. 2017;31(8):653–663. | ||
Low PA. Prevalence of orthostatic hypotension. Clin Auton Res. 2008;18(Suppl 1):8–13. | ||
Levy B, Fritz C, Tahon E, Jacquot A, Auchet T, Kimmoun A. Vasoplegia treatments: the past, the present, and the future. Crit Care. 2018;22(1):52. | ||
Robertson D. The pathophysiology and diagnosis of orthostatic hypotension. Clin Auton Res. 2008;18(Suppl 1):2–7. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.