Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Risk Prediction Models for Perioperative Hypothermia: A Systematic Review
Authors Liu J, Liu F, Xu W, Du L, Li Y, Liang A, Li B, Zhang M
Received 13 May 2025
Accepted for publication 24 July 2025
Published 30 July 2025 Volume 2025:18 Pages 4443—4452
DOI https://doi.org/10.2147/JMDH.S538891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Jinghui Liu,1,2,* Fangli Liu,2,3,* Wenqi Xu,1,2 Libaihe Du,1 Yun Li,1 Aiqun Liang,1 Binfei Li,1 Mingyang Zhang1
1Surgery and Anesthesiology Department 3, Zhongshan People’s Hospital, Zhongshan, Guangdong, People’s Republic of China; 2School of Nursing and Health, Henan University, Kaifeng, Henan, People’s Republic of China; 3Institution of Nursing and Health, Henan University, Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mingyang Zhang, Surgery and Anesthesiology Department 3, Zhongshan People’s Hospital, 2 Sun Wen East Road, Zhongshan, Guangdong Province, People’s Republic of China, 528400, Email [email protected]
Background: Perioperative hypothermia is a frequent complication causing patient discomfort and increasing risks like surgical site infection, coagulation dysfunction, slow drug metabolism, cardiovascular events, and prolonged hospitalization, which severely affect prognosis. Due to its significant impact, this study systematically reviews and evaluates existing risk prediction models for perioperative hypothermia. The aim is to provide clinical staff with a reference for selecting or developing an appropriate prediction model.
Methods: A systematic search was carried out in PubMed, Embase, Web of Science, the Cochrane Library, and CINAHL to find relevant studies on perioperative hypothermia risk prediction models from the inception of databases to May 23, 2024. Two reviewers independently screened abstracts and full texts for eligibility. Data collection followed the checklist for critical appraisal and data extraction for systematic reviews of prediction modelling studies (CHARMS). The prediction model risk of bias assessment tool (PROBAST) checklist assessed the risk of bias and applicability of the data.
Results: This study included 11 papers (14 risk prediction models). Models showed good predictive performance (the area under the curve (AUC) range: 0.700– 0.870). Nine studies reported calibration; validation involved internal (n=3), external (n=3), or both (n=3). PROBAST indicated high risk of bias in all 11 papers, primarily due to insufficient model validation. The most common predictors were age, baseline temperature, BMI, fluid/infusion/rehydration volume, operating room temperature, anesthetic time, and operative time.
Conclusion: The overall discrimination and applicability of perioperative hypothermia risk prediction models are good, but the risk of bias is high and the quality of studies needs to be further improved. In the future, a more standardized approach should be used to optimize existing models, develop more targeted prediction models with a low risk of bias, and conduct internal and external validation to improve their predictive accuracy in clinical application.
Keywords: perioperative hypothermia, prediction, model, systematic review
Introduction
Perioperative hypothermia, also known as unplanned perioperative hypothermia, is defined as a core body temperature below 36°C occurring during the perioperative period unrelated to intentional medical cooling1 and it is one of the most common surgical complications. Even mild hypothermia increases the incidence of wound infection (relative risk [RR] 3.25, 95% confidence interval [CI] 1.35–7.84), post-operative ischemic myocardial events (RR 4.49, 95% CI 1.00–20.16), and intraoperative blood loss (RR 1.33, 95% CI 1.06–1.66), and it prolongs post-operative recovery.2,3 Thus, maintaining normothermia throughout the perioperative period is critical for optimal surgical outcomes, patient safety, and satisfaction.1 Studies have shown that the incidence of perioperative hypothermia is as high as 44.3% in China,4 while internationally reported rates vary widely, ranging from 4% to more than 70%,5–9 as exemplified by documented cases: 4% in Arizona, USA;6 56.7% in Brasília, Brazil;7 and 72.1% in New York, USA.8
Accurate assessment of patients’ risk factors is crucial to the prevention of perioperative hypothermia. Clinical risk prediction models are statistical models based on disease predictive factors that estimate the probability of an individual developing a particular disease.10,11 Risk prediction models are widely applied across medical practice for multiple purposes, including predicting disease development, treatment response, or patient prognosis. In surgery, these models are commonly used to forecast the risk of adverse outcomes after intervention. Surgical risk prediction models can be used to facilitate clinical decision-making, define thresholds for intervention, or for risk-adjusting outcome data for benchmarking purposes.11 Commonly used model-building methods include logistic regression, Cox regression, and machine learning.11 The machine learning algorithms most frequently identified as having the best performance were support vector machines (SVM), extreme gradient boosting (XGBoost), and random forests (RF).12
Despite growing research on perioperative hypothermia risk prediction models in recent years, a critical knowledge gap persists: systematic evaluation of the methodological quality and clinical applicability of existing models remains understudied. This gap not only challenges the validation of model robustness but also obstructs evidence-based clinical adoption, potentially undermining hypothermia prevention strategies and negatively impacting patient outcomes. This systematic review aims to characterize and synthesize the current landscape of perioperative hypothermia risk prediction models. By retrieving and analyzing relevant studies, we will systematically compare existing models based on their basic characteristics, construction methods, methodological quality, predictive efficacy, and influencing factors. This review will help clinicians identify models with optimal reliability and utility for clinical decision-making while informing future research directions for model development, ultimately guiding healthcare providers toward more effective, evidence-based practices that improve patient safety and outcomes.
Materials and Search Methods
Methods
The systematic review followed the checklist outlined by transparent reporting of multivariable prediction models for individual prognosis or diagnosis: checklist for systematic reviews and meta-analyses (TRIPOD-SRMA) guidance13 and was registered in the PROSPERO database (ID: CRD42024555249) (Supplementary table 1).
Search Strategy
Key questions for the systematic appraisal of prediction models were constructed using the PICOTS concepts of the Cochrane prognostic methods group.14 P(Population): Perioperative patients ≥18 years of age. I (Intervention model): Develop, validate, or update hypothermia risk prediction models. C(Comparator): None. O(Outcome): The predicted outcome was hypothermia. T(Timing): Real-time prediction in the perioperative period. S(Setting): It is employed to anticipate the development of perioperative hypothermia in hospitalized patients.
Five databases including PubMed, Embase, Web of Science, the Cochrane Library, and CINAHL were systematically searched from the inception of databases to May 23, 2024. Searches were conducted using subject words combined with free words, and supplemented by PubMed search with Ingui filter, Haynes filter, and Geersing filter. The reference lists of the retrieved articles were also reviewed for the identification of additional studies. English search terms included: “perioperative period”/ operative/ intraoperative/ postoperative/ preoperative; hypothermia*/ “hypothermia*accidental”/ “accidental hypothermia*”/ “unintended hypothermia”/ “unplanned hypothermia”/ “inadvertent hypothermia”/ “body temperature declin*”/ piloerection/ shiver*; model/ predict*/ prognostic/ risk/ early warning/ risk score/ risk assessment/ nomogram/ assessment scale. The detailed search strategy is available in Supplementary table 2.
Inclusion and Exclusion Criteria
The inclusion criteria of studies included the following: (1) the subjects were surgical patients aged ≥18 years and did not experience preoperative hypothermia; (2) the content of the study was to construct and/ or verify the risk prediction model of perioperative hypothermia; (3) the process and statistical methods of modeling, evaluation, and comparison are clear; (4) the type of study was cohort or case-control study; (5) English literature. Exclusion criteria of studies included the following: (1) only risk factors were analyzed, and no risk prediction model was established; (2) full text not available or incomplete data; (3) duplicate literature; (4) conference abstracts, grey literature, and other informal publications.
Study Selection
Two researchers independently conducted a systematic literature search and imported the results into the EndNote X9 reference manager software to remove duplicates and streamline the screening process. After screening abstracts and titles, they examined full texts to identify papers that met the predetermined inclusion and exclusion criteria. Until a consensus was formed, all conflicts were discussed and settled by a third researcher.
Data Extraction
Using standardized forms, two review authors separately extracted key information. The list of extracted items was based on the critical appraisal and data extraction for systematic reviews of prediction modelling studies (CHARMS) checklist.15 The information extracted from each study included the name of the first author, year published, country, study design, study object, temperature measuring instrument, site, and frequency, candidate variables, continuous variable handling methods, sample size, the proportion of outcome events, missing data and handling methods, model method, model performance, calibration method, model validation, model presentation, number of factors and final predictors. The third author conducted discussions to settle disagreements until an agreement was reached.
Quality Assessment
The methodological quality and applicability of the included studies were assessed separately by two authors using the prediction model risk of bias assessment tool (PROBAST).10 The third author conducted talks to resolve disagreements until an agreement was achieved.
Bias evaluation consists of four main areas: participants, predictors, outcome, and analysis, with twenty questions in total. The risk of bias is considered low if all questions in each area are answered “yes” or “probably yes”. Conversely, if any question is answered “no” or “probably no”, the risk of bias is deemed high. If there is insufficient information, the risk of bias is labeled unclear. Since all four areas have a low risk of bias, the overall risk of bias in this study is low. However, if one or more areas have a high risk of bias or if there is no external validation for the predictive model despite low risk in all four areas, the overall risk of bias is high. Similarly, if one or more areas have an unclear risk of bias while the rest have a low risk, the overall risk of bias in the study is considered unclear.
Applicability evaluation encompasses three main areas: participants, predictors, and outcome. Each domain is assessed for “good applicability”, “poor applicability”, or “unclear”. In this study, all three domains were found to have low applicability risk, indicating an overall good applicability. However, if one or more domains show high applicability risk, the overall applicability of the study is considered poor. Additionally, if one or more domains are unclear while others show low applicability risk, the overall applicability of the study is deemed unclear.
Synthesis of Results
The main traits of the prediction models have been highlighted by summarizing the descriptive statistics of the data in tables. A meta-analysis was not feasible due to the heterogeneous nature of the studies. The 11 final articles were synthesized qualitatively for integration.
Results
Study Selection
A total of 3019 articles were found through database searches. After removing duplicates, 2413 articles remained. Two researchers excluded 2388 articles by reading the titles and abstracts of the articles and based on the exclusion criteria. Three articles were excluded because they were not retrieved. We read the full text of 22 articles, of which 11 were excluded for the following reasons: review articles (2 studies), did not fit the type of study (4 studies), and did not fit the study population (5 studies). Finally, a total of 14 models from 11 studies were included in the systematic review. The flow diagram of the search results is shown in Figure 1.
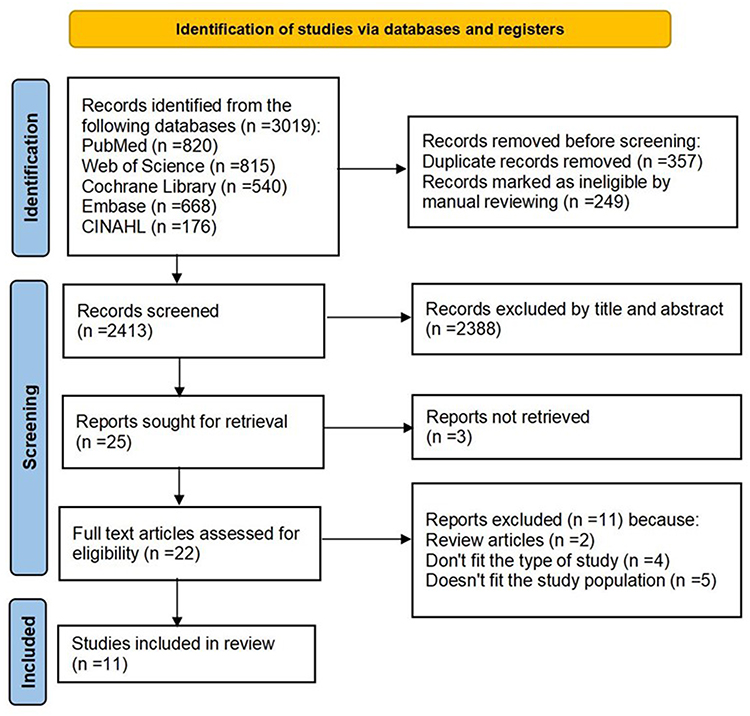 |
Figure 1 PRISMA flow chart for the process of literature selection. Adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons. |
Study Characteristics
Among the 11 studies16–26 included, 7 were conducted in China,17,20–25 1 in Colombia,16 1 in Japan,18 1 in France,19 and 1 in South Korea.26 The oldest model was reported in 2002,18 and the latest one in 2024.24 Six studies16,19,21,22,25,26 were prospective cohort studies, of which one16 was a multi-center study, 4 studies17,20,23,24 were retrospective cohort studies, and 1 study18 was a retrospective case-control study. Thermometry sites varied, with 2 studies using nasopharyngeal measurements,23,24 7 using tympanic measurements,16–19,21,22,26 1 using axillary measurement,25 and 1 using either nasopharyngeal or distal esophagus measurement.20 A total of fourteen models were developed in the literature reviewed, of which Rincón et al16 developed two models, the full model and the simplified model, both with consistent predictors. Desgranges et al19 built two models with inconsistent predictors, Model A had five predictors while Model B had six predictors. Kim et al26 have developed three models that describe the incidence of hypothermia at three different times during surgery. Dai et al25 validated a model without specifying how the model was modelled. The remaining studies constructed one model. The basic characteristics of the studies that were included are summarized in Supplementary table 3.
A total of 14 models were constructed and the incidence of hypothermia ranged from 22.56% to 54.42%. Logistic regression was applied to all studies except Dai et al.25 Seven studies16,18,20,21,23,25,26 reported specific missing data and direct deletion of missing values, while the remaining four studies17,19,22,24 reported no missing values (Supplementary table 4).
Nine studies16,17,19–25 reported the AUC values of the models, which ranged from 0.700 to 0.870, and the models showed good predictive performance (AUC>0.700). Nine studies16,17,19,21–26 reported calibration by calibration curve, Hosmer-Lemeshow test, decision curve analysis, and Brier score. In terms of model validation, 3 studies16,20,21 performed internal validation, 3 studies17,18,25 performed external validation, 3 studies22–24 combined internal and external validation, and 2 studies19,26 did not specify whether internal or external validation was conducted. The models reported a minimum of 4 predictors and a maximum of 13 predictors, and the predictors that appeared more frequently in the multivariate models were age, baseline temperature, BMI, fluid/infusion/rehydration volume, operating room temperature, anesthetic time, and operative time. Model presentation was reported in all but 2 studies25,26 (Supplementary table 4).
Quality Assessment
Eleven included studies16–26 showed a high risk of bias, primarily attributed to the statistical methods, such as small data sets, improper handling of missing data, use of univariate analysis for variable screening, and lack of validation. Regarding applicability, nine studies16–20,22,23,25,26 showed good applicability. (Figure 2, Supplementary table 5).
 |
Figure 2 Evaluation of the risk of bias of the studies included in the review (n=11). |
Five articles17,18,20,23,24 in the area of research subjects were at high risk of bias. This is because retrospective studies rely on existing data, which can lead to a large difference between predicted and actual outcomes. The risk of bias was unclear in 5 articles17,18,20,23,24 in the area of predictors, and high in 1 article16 because studies that used multicentre clinical data modelling did not state whether the predictor measures were consistent between centers. Two studies19,26 in the outcome domain had a low risk of bias and 9 studies16–18,20–25 had an unclear risk of bias because the method of hypothermia classification was not reported. All data analysis studies had a high risk of bias. Five development studies16,19,21,23,26 had events per variable <10 and no subsequent parameter adjustment, which could lead to overfitting. Three studies16,18,22 had a model validation sample size <100, which could lead to reduced confidence in the results. Three articles17,23,24 categorized continuous variables, which may lead to the loss of some information. Seven articles16,18,20,21,23,25,26 include missing data removal, which may lead to biased results and overestimation of the model’s ability to discriminate. Seven articles16–22 screen variables based on single-factor analysis without considering the mutual influence and intrinsic link between multiple variables, which may lead to bias due to the omission of independent variables. Five model construction studies17–19,25,26 did not use internal validation and three16,21,22 used only simple randomized split validation, all of which may introduce an optimism bias in the assessment of model performance. None of the studies reported content related to data complexity (Supplementary table 5).
Two studies21,24 were rated as having low applicability because they selected only older patients over 60 years of age to build the model, which limits the generalizability of the findings to younger or more diverse patient populations. The remaining nine studies were rated as having good applicability (Supplementary table 5).
Discussion
This systematic review included 11 studies comprising a total of 14 predictive models. The AUC values of 10 models were all greater than 0.700, suggesting that these models generally demonstrate good predictive power for perioperative hypothermia occurrence. Internal validation assesses a model’s reproducibility and helps reduce overfitting, while external validation evaluates the model’s generalizability and prevents performance overestimation.27,28 Therefore, after developing a predictive model, researchers should complete both internal and external validation of the model and report the results. Prediction models in medicine have proliferated in recent years, but their reporting has been consistently suboptimal. It is therefore essential that key details of how a prediction model was developed and validated be clearly reported to enable synthesis and critical appraisal of all relevant information.29 The transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD) statement29 explicitly covers the development and validation of prediction models for diagnosis and prognosis, for all medical domains and all types of predictors. It is recommended that future studies strictly adhere to the TRIPOD statement, as this standardization enhances methodological rigor and reporting quality, enabling clinicians to select more accurate and clinically beneficial models.
The PROBAST assessment results showed that all 11 studies presented a high risk of bias, especially in the area of analysis, mainly due to the reliance on retrospective studies to construct predictive models, insufficient sample size, improper handling of missing data, and the use of univariate analysis to screen variables. By analyzing the main bias problems of the included models, this paper draws the following insights: (1) It is recommended to use prospective cohort studies to construct models. Because retrospective data may lead to information bias and the predictors available for modelling are not comprehensive enough, while the “cause and effect” design principle of cohort studies can better reveal the natural course of disease development, it is more recommended to use prospective cohort studies to construct predictive models. (2) Ensure adequate sample size. The larger the sample size of the developed model, the more stable the model performance will be. However, most predictive models fail to meet the sample size requirement due to too many candidate variables and limited sources of clinical data. Therefore, researchers should avoid including variables that are difficult to obtain, inaccurate to measure, or costly to measure into the model, and may consider conducting multicentre studies or developing models through electronic medical record data or calculations using the machine learning sample size calculation method proposed by Riley et al may be considered.30 (3) Complete report on the treatment of missing data to avoid screening candidate variables using only one-way analyses. Proper handling of missing data can reduce the loss of sample size and improve the accuracy of the model. There are numerous methods to deal with missing data,31 among which multiple interpolation is considered to be the most appropriate treatment method,10 which can be used by researchers to fill in the missing data and described in detail in the report. (4) Add variable screening methods. Expert knowledge and practical analysis should be combined to reduce reliance on univariate analysis. There are a variety of variable screening methods, which can be broadly classified into two categories based on regression analysis (eg, forward, backward, stepwise screening, full subset screening methods, LASSO regression, elasticity network) and based on machine learning (eg, Random Forest, Regularised Random Forest, Boruta, Gradient Enhancement Feature Screening),32 which can reduce the risk of overfitting, and it is suggested that the future screening of variables can be combined with the clinical reality of adopting new methods to improve the accuracy of screening.
Early research on hypothermia risk prediction models began earlier in other countries, and most of the early prediction models lacked calibration and internal/external validation, leading to overfitting and hindering the models’ applicability. Research on hypothermia risk prediction models in China started late but has a substantial number of publications. Of the literature included in this study, 7 were from China, with 6 published within the last three years. This significant recent surge reflects a growing prioritization of this research area in China. The focus on developing and validating these models aims to enable timely interventions through individualized risk prediction, ultimately improving perioperative outcomes and optimizing resource utilization. Currently, some progress has been made in hypothermia risk prediction model research, but further research is still needed in model construction, validation, and reporting.
The results of this review showed that the predictors of hypothermia in perioperative patients were focused on four main areas: patient factors, surgical factors, anesthetic factors, and environmental factors. Among the 11 papers included, the predictors with more repetitions were age, baseline temperature, BMI, fluid/infusion/rehydration volume, operating room temperature, anesthetic time, and operative time.
Decreased body function, reduced central nervous system regulation, reduced muscle layers and subcutaneous adipose tissue, slow blood circulation, low basal metabolic rate, and reduced metabolic rate32 in older patients are all important reasons for the higher risk of hypothermia. The temperature difference between core and peripheral tissues is increased in patients with low preoperative basal body temperatures, and core heat redistribution is exacerbated after induction of anesthesia, increasing the risk of intraoperative hypothermia. Therefore, preoperative pre-warming should be actively performed using active warming methods to reduce core body temperature decrease and heat redistribution, such as the use of inflatable warming devices, intravenous fluid warming devices, and conduction heating systems, and other measures should be continued until the postoperative period.33,34 The exposure of the body cavity in open surgery, the establishment of carbon dioxide pneumoperitoneum in laparoscopic surgery, and the large volume of intraoperative irrigation fluids are all prone to perioperative hypothermia, and it is recommended that all irrigation fluids and carbon dioxide pneumoperitoneum be heated before use. BMI is an important individual factor that influences the incidence of hypothermia during surgery, and the decrease in core temperature during the body heat redistribution phase is inversely related to the percentage of fat in the body or BMI,35 so patients with a low BMI are at greater risk of developing hypothermia. Conversely, a higher BMI with a relatively high percentage of body fat reduces the risk of hypothermia due to the protective effect of fat and reduced body surface heat loss.32 Intraoperative administration of 1 liter of fluid or 1 unit of 4°C stored blood intravenously will reduce core body temperature by 0.25 °C; the risk of perioperative hypothermia is increased if more than 1 liter of unheated fluid is administered intravenously.36,37 Intraoperative warming should be applied to fluids and blood products that are infused at a rate of more than 500 mL/h, and intraoperative irrigations should be preheated to 38–40°C.38 Hypothermia is easily caused by hypovolemia and hypothermia reduces the activity of many enzymes in the body, reduces platelet function, reduces platelet count, activates fibrinolysis, and releases tissue factor to increase blood viscosity, further exacerbating the incidence of bleeding and DVT.21
The incidence of perioperative hypothermia is significantly higher in patients undergoing surgery for more than 2 h, especially in those under general anesthesia,36 reminding us that preoperative preparation should be as adequate as possible to reduce the duration of surgery. Intraoperatively, under the influence of anesthesia and sedative drugs, there is an inhibitory effect on the regulation of central body temperature, and some studies have pointed out that there are three time-phase changes in the temperature of the patient’s nucleus pulposus after the induction of anesthesia, and the first time-phase, that is, 1 h after the induction of anesthesia, the temperature of the patient’s nucleus pulposus will fall by 1.0–1.5°C.39 Radiation and convection cause 85% of heat loss in the perioperative period, and the loss of radiant heat is mainly dependent on the temperature difference between the patient’s skin and the environment. Studies40 have shown that a room temperature of <23°C is a risk factor for hypothermia in patients undergoing general surgery, and therefore the room temperature can be increased proactively without interfering with the operation. Other studies have shown that hypothyroid patients are more prone to hypothermia during surgery, which may be related to the fact that thyroid function affects the body’s energy metabolism, leading to an imbalance between heat production and heat loss,41 and that patients with comorbid metabolic disorders should implement active warming as early as possible to avoid hypothermia. It is suggested that future predictive modeling studies could focus on the above seven predictors, most of which are readily obtainable clinical variables, making the model more convenient to use. This approach would facilitate timely risk stratification and targeted interventions for specific risk factors, thereby enabling normalization of the patient’s core body temperature.
Limitations
This study has several limitations. First, the inability to perform meta-analysis stems from substantial heterogeneity across included studies, particularly in data sources, methodological approaches (eg, divergent model construction techniques, such as differing variable selection methods or statistical algorithms), and evaluation indexes (eg, some studies reported AUC values while others used calibration curve or decision curve analysis). Consequently, only qualitative synthesis was feasible. Second, the paucity of multicenter data and externally validated models remains a critical gap. Most studies relied on single-center datasets, which may introduce selection bias and limit generalizability to diverse clinical settings. Validation efforts were frequently constrained to small sample sizes or conducted within the same center where models were developed, failing to account for variations in patient demographics and anesthesia practices across healthcare systems. This limitation stems from challenges in establishing multicenter collaborations, such as data-sharing barriers, lack of standardized data collection tools, and the resource-intensive nature of external validation. Future research should prioritize partnerships between institutions to build large, diverse datasets, implement pre-registered validation protocols, and consistently apply TRIPOD reporting guidelines.
Conclusion
In our systematic review, all included models showed high risk of bias due to issues like reliance on retrospective data, small sample sizes, and non-transparent variable selection (eg, using univariate instead of multivariate analysis), with most lacking external validation that limits their generalizability to diverse clinical settings. Although no model is currently suitable for direct clinical use, consistently reported predictors such as age, baseline temperature, and fluid volume provide actionable references for hypothermia prevention. Future research should prioritize developing models with prospective multicenter data involving diverse populations, applying PROBAST-guided rigor and transparent variable selection (eg, multivariate or machine learning methods), and validating them internally and externally; additionally, translating findings into clinical practice through EHR-integrated real-time risk assessment tools paired with provider training to implement targeted interventions (eg, warming protocols for high-risk patients) will enhance model utility and support evidence-based hypothermia management.
Data Sharing Statement
Data is available on request from the corresponding author.
Ethics Approval and Consent to Participate
An ethics statement is not applicable because this study is based exclusively on published literature.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by a grant from the Zhongshan City Healthcare General Project 2023 (2023B1003) and Guangdong Provincial Medical Research Fund 2023 (B2023066), Zhongshan City, Guangdong Province, China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rauch S, Miller C, Bräuer A, Wallner B, Bock M, Paal P. Perioperative hypothermia-A narrative review. Int J Environ Res Public Health. 2021;18(16):8749. doi:10.3390/ijerph18168749
2. Ruetzler K, Kurz A. Consequences of perioperative hypothermia. Handb Clin Neurol. 2018;157:687–697. doi:10.1016/B978-0-444-64074-1.00041-0
3. Torossian A, Bräuer A, Höcker J, Bein B, Wulf H, Horn EP. Preventing inadvertent perioperative hypothermia. Dtsch Arztebl Int. 2015;112(10):166–172. doi:10.3238/arztebl.2015.0166
4. Yi J, Lei Y, Xu S, et al. Intraoperative hypothermia and its clinical outcomes in patients undergoing general anesthesia: national study in China. PLoS One. 2017;12(6):e0177221. doi:10.1371/journal.pone.0177221
5. Ribeiro E, Ferreira RC, Montanari FL, Botelho MTSL, Correia MDL, Duran ECM. Conceptual and operational definition of the components of the nursing diagnosis hypothermia (00006) in the perioperative period. Rev Bras Enferm. 2021;74(2):e20190684. doi:10.1590/0034-7167-2019-0684
6. Burns SM, Piotrowski K, Caraffa G, Wojnakowski M. Incidence of postoperative hypothermia and the relationship to clinical variables. J Perianesth Nurs. 2010;25(5):286–289. doi:10.1016/j.jopan.2010.07.001
7. Mendonça FT, Ferreira JDS, Guilardi VHF, Guimarães GMN. Prevalence of inadvertent perioperative hypothermia and associated factors: a cross -sectional study. Ther Hypothermia Temp Manag. 2021;11(4):208–215. doi:10.1089/ther.2020.0038
8. Long KC, Tanner EJ, Frey M, et al. Intraoperative hypothermia during primary surgical cytoreduction for advanced ovarian cancer: risk factors and associations with postoperative morbidity. Gynecol Oncol. 2013;131(3):525–530. doi:10.1016/j.ygyno.2013.08.034
9. Alfonsi P, Bekka S, Aegerter P. SFAR research network investigators. prevalence of hypothermia on admission to recovery room remains high despite a large use of forced-air warming devices: findings of a non-randomized observational multicenter and pragmatic study on perioperative hypothermia prevalence in France. PLoS One. 2019;14(12):e0226038. doi:10.1371/journal.pone.0226038
10. Moons KGM, Wolff RF, Riley RD, et al. PROBAST: a tool to assess risk of bias and applicability of prediction model studies: explanation and elaboration. Ann Intern Med. 2019;170(1):W1–W33. doi:10.7326/M18-1377
11. Grant SW, Collins GS, Nashef SAM. Statistical primer: developing and validating a risk prediction model. Eur J Cardiothorac Surg. 2018;54(2):203–208. doi:10.1093/ejcts/ezy180
12. Silva GFS, Fagundes TP, Teixeira BC, Chiavegatto Filho ADP. Machine learning for hypertension prediction: a systematic review. Curr Hypertens Rep. 2022;24(11):523–533. doi:10.1007/s11906-022-01212-6
13. Snell KIE, Levis B, Damen JAA, et al. Transparent reporting of multivariable prediction models for individual prognosis or diagnosis: checklist for systematic reviews and meta-analyses (TRIPOD-SRMA). BMJ. 2023;381:e073538. doi:10.1136/bmj-2022-073538
14. Moons KG, Hooft L, Williams K, Hayden JA, Damen JA, Riley RD. Implementing systematic reviews of prognosis studies in Cochrane. Cochrane Database Syst Rev. 2018;10(10):ED000129. doi:10.1002/14651858.ED000129
15. Moons KG, de Groot JA, Bouwmeester W, et al. Critical appraisal and data extraction for systematic reviews of prediction modelling studies: the CHARMS checklist. PLoS Med. 2014;11(10):e1001744. doi:10.1371/journal.pmed.1001744
16. Rincón DA, Valero JF, Eslava-Schmalbach J. Construcción y validación de un modelo predictivo de hipotermia intraoperatoria [Construction and validation of a model to predict intraoperative hypothermia]. Rev Esp Anestesiol Reanim. 2008;55(7):401–406. doi:10.1016/s0034-9356(08)70610-8
17. Yi J, Zhan L, Lei Y, et al. Establishment and validation of a prediction equation to estimate risk of intraoperative hypothermia in patients receiving general anesthesia. Sci Rep. 2017;7(1):13927. doi:10.1038/s41598-017-12997-x
18. Kasai T, Hirose M, Yaegashi K, Matsukawa T, Takamata A, Tanaka Y. Preoperative risk factors of intraoperative hypothermia in major surgery under general anesthesia. Anesth Analg. 2002;95(5):1381–1383. doi:10.1097/00000539-200211000-00051
19. Desgranges FP, Bapteste L, Riffard C, et al. Predictive factors of maternal hypothermia during Cesarean delivery: a prospective cohort study. Can J Anaesth. 2017;64(9):919–927. doi:10.1007/s12630-017-0912-2
20. Hu Z, Li W, Liang C, Li K. Risk factors and prediction model for inadvertent intraoperative hypothermia in patients undergoing robotic surgery: a retrospective analysis. Sci Rep. 2023;13(1):3687. doi:10.1038/s41598-023-30819-1
21. Zhao B, Zhu Z, Qi W, et al. Construction and validation of a risk prediction model for intraoperative hypothermia in elderly patients undergoing total Hip arthroplasty. Aging Clin Exp Res. 2023;35(10):2127–2136. doi:10.1007/s40520-023-02500-0
22. Li L, Lu Y, Yang LL, Xu W, Yu JK. Construction and validation of postoperative hypothermia prediction model for patients undergoing joint replacement surgery. J Clin Nurs. 2023;32(13–14):3831–3839. doi:10.1111/jocn.16503
23. Zhang B, Pan AF. Development and evaluation of a novel predictive nomogram for assessing the risk of intraoperative hypothermia in patients undergoing thoracoscopic pulmonary tumor surgery. Heliyon. 2023;9(12):e22574. doi:10.1016/j.heliyon.2023.e22574
24. Yuan X, Liu Q, Zhou H, et al. Development and validation of a predictive model for intraoperative hypothermia in elderly patients undergoing craniocerebral tumor resection: a retrospective cohort study. World Neurosurg. 2024;184:e593–e602. doi:10.1016/j.wneu.2024.01.174
25. Dai Z, Zhang Y, Yi J, Huang Y. Validation of a prediction model for intraoperative hypothermia in patients receiving general anesthesia. Int J Clin Pract. 2022;2022:6806225. doi:10.1155/2022/6806225
26. Kim EJ, Yoon H. Preoperative factors affecting the intraoperative core body temperature in abdominal surgery under general anesthesia: an observational cohort. Clin Nurse Spec. 2014;28(5):268–276. doi:10.1097/NUR.0000000000000069
27. Moons KG, Kengne AP, Woodward M, et al. Risk prediction models: i. Development, internal validation, and assessing the incremental value of a new (bio)marker. Heart. 2012;98(9):683–690. doi:10.1136/heartjnl-2011-301246
28. Steyerberg EW, Harrell FE. Prediction models need appropriate internal, internal-external, and external validation. J Clin Epidemiol. 2016;69:245–247. doi:10.1016/j.jclinepi.2015.04.005
29. Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD Statement. BMJ. 2015;350:g7594. doi:10.1136/bmj.g7594
30. Riley RD, Ensor J, Snell KIE, et al. Calculating the Sample Size Required for Developing a Clinical Prediction Model. BMJ. 2020;368:m441. doi:10.1136/bmj.m441
31. Wang YY, Bu ZJ, Li YX, et al. Variable selection methods and comparison in clinical prediction models. Mod Chin Clin Med. 2024;31(2):6–12. doi:10.3969/j.issn.2095-6606.2024.02.002
32. Collins S, Budds M, Raines C, Hooper V. Risk factors for perioperative hypothermia: a literature review. J Perianesth Nurs. 2019;34(2):338–346. doi:10.1016/j.jopan.2018.06.003
33. Madrid E, Urrútia G, Roqué I Figuls M, et al. Active body surface warming systems for preventing complications caused by inadvertent perioperative hypothermia in adults. Cochrane Database Syst Rev. 2016;4(4):CD009016. doi:10.1002/14651858.CD009016.pub2
34. Yoo JH, Ok SY, Kim SH, et al. Efficacy of active forced air warming during induction of anesthesia to prevent inadvertent perioperative hypothermia in intraoperative warming patients: comparison with passive warming, a randomized controlled trial. Medicine. 2021;100(12):e25235. doi:10.1007/s12630-017-0912-2
35. Boddu C, Cushner J, Scuderi GR. Inadvertent perioperative hypothermia during orthopedic surgery. Am J Orthop Belle Mead NJ. 2018;47(7). doi:10.12788/ajo.2018.0056
36. National Center for Quality Assurance of Anesthesia. Chinese expert consensus statement for prevention and management of perioperative hypothermia. Med J of Peking Union Med Coll Hosp. 2023;14(04):734–743.
37. Ma H, Lai B, Dong S, et al. Warming infusion improves perioperative outcomes of elderly patients who underwent bilateral Hip replacement. Medicine. 2017;96(13):e6490. doi:10.1097/MD.0000000000006490
38. Sabbag IP, Hohmann FB, Assunção MSC, et al. Postoperative hypothermia following non-cardiac high-risk surgery: a prospective study of temporal patterns and risk factors. PLoS One. 2021;16(11):e0259789. doi:10.1371/journal.pone.0259789
39. Iden T, Höcker J. Vermeidung unbeabsichtigter perioperativer hypothermie: ein Leitfaden [prevention of perioperative hypothermia - guidelines for daily clinical practice]. Anasthesiol Intensivmed Notfallmed Schmerzther. 2017;52(7–08):554–562. doi:10.1055/s-0041-103653
40. Zeba S, Surbatović M, Marjanović M, et al. Efficacy of external warming in attenuation of hypothermia in surgical patients. Vojnosanit Pregl. 2016;73(6):566–571. doi:10.2298/vsp150330032z
41. Giuliano KK, Hendricks J. Inadvertent perioperative hypothermia: current nursing knowledge. AORN J. 2017;105(5):453–463. doi:10.1016/j.aorn.2017.03.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.