Back to Journals » Risk Management and Healthcare Policy » Volume 14
Risk Perception and Willingness to Work Among Doctors and Medical Students of Karachi, Pakistan During the COVID-19 Pandemic: A Web-Based Cross-Sectional Survey
Authors Khalid M, Khalid H ![]() , Bhimani S
, Bhimani S ![]() , Bhimani S, Khan S, Choudry E, Mahmood SU
, Bhimani S, Khan S, Choudry E, Mahmood SU
Received 8 May 2021
Accepted for publication 29 July 2021
Published 10 August 2021 Volume 2021:14 Pages 3265—3273
DOI https://doi.org/10.2147/RMHP.S310453
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chiara Verbano
Momina Khalid,1 Hiba Khalid,2 Sameer Bhimani,1 Simran Bhimani,2 Sheharyar Khan,3 Erum Choudry,4 Syed Uzair Mahmood5
1Department of Internal Medicine, Sindh Medical College, Jinnah Sindh Medical University, Karachi, Pakistan; 2Department of Internal Medicine, Dow Medical College, Dow University of Health Sciences, Karachi, Pakistan; 3Department of Medicine, Baqai Medical University, Karachi, Pakistan; 4Indus Hospital Research Center, The Indus Hospital and Health Network, Karachi, Pakistan; 5Department of Medicine, Health and Life Sciences, Queen’s University Belfast, Belfast, UK
Correspondence: Hiba Khalid
Dow Medical College, Dow University of Health Sciences, Baba-e-Urdu Road, Saddar, Karachi, 74200, Pakistan
Tel +923094379571
Email [email protected]
Purpose: During the timeline of twenty years, several epidemics and pandemics have occurred. Yet, a consistent feature of these public health crises is the surge in the demand for healthcare services exceeds the availability.
Materials and Methods: A cross-sectional web-based survey was conducted in the month of June and July 2020 in Karachi, Pakistan. The study participants included doctors and medical students residing in Karachi.
Results: Out of 187 doctors, 74.3% were working during the COVID-19 pandemic, of which 58.3% were willing to work. Out of 200 medical students, 93.5% were not volunteering during the COVID-19 pandemic, of which 46% were willing to volunteer. Doctors strongly agreed that they would be willing to work during the COVID-19 pandemic if they were healthy and able to do so (57.2%), if they were provided personal protective equipment (PPE) (51.3%), and if they were guaranteed coverage of treatment cost if they get infected while working (57.8%). Medical students strongly agreed that they would be willing to volunteer during the COVID-19 pandemic if they were provided PPE (49.0%), and if their parents were supportive of their decision to volunteer (44.5%). Most doctors (54.5%) felt that they were extremely likely to get infected while working during the COVID-19 pandemic and 59.4% felt that in turn, they were extremely likely to infect their families as well. Most medical students (40.5%) felt that they were somewhat likely to get infected while volunteering during the COVID-19 pandemic and 55.5% felt that in turn, they were extremely likely to infect their family as well. In the event of infection with COVID-19, 51.3% doctors and 42.0% medical students felt that they would recover without hospitalization.
Conclusion: Since future pandemics are likely, we encourage health-care policymakers to utilize the findings of this study to create a sustainable pandemic response.
Keywords: coronavirus disease 2019, SARS-CoV-2, physicians, risk, infection
Introduction
Viral diseases continue to emerge as a serious threat to public health. During the timeline of twenty years, there has been an emergence of several viral epidemics, including the Middle East respiratory syndrome coronavirus (MERS-CoV) in 2012, H1N1 influenza (H1N1pdm09) in 2009, and the Severe acute respiratory syndrome coronavirus (SARS-CoV) in 2002 to 2003.1 Yet, a consistent feature of these public health crises is that the surge in the demand for healthcare services exceeds the availability.2 This shortfall compounded by the absenteeism of Healthcare workers (HCWs) during a pandemic poses an even greater threat to the healthcare sector.3
It is often assumed that HCW’s have a professional obligation to report to duty despite any probable risks to their safety and data from previous pandemics has supported this assumption.4 However, there exist several reports of non-illness-related absenteeism during various disease outbreaks in the past. During the 2003 SARS epidemic HCWs evaded examining infected patients and in some cases completely declined from performing their duties.4 Another study reported that 12% of the study participants would consider early retirement or resignation in response to a pandemic.5 Studies also show that when the risk of infectivity and virulence is high, non-illness absenteeism rates are also high.5 A survey evaluating the willingness and ability of HCWs to work during a calamitous disaster observed that greater than 80% of the study participants were willing to report to work during a natural calamity, while only 48.4% to 61.1% were willing to report to work during a SARS or smallpox outbreak, respectively.6 Therefore, non-illness-related absenteeism accompanied by illness-related absenteeism leads to a drastic scarcity of human resources.
Consequently, determining the factors that influence the willingness of HCWs to work during a pandemic is imperative, in order to effectively plan, prepare, and ensure the continued delivery of essential health services during a pandemic. In turn, these determinants can also assist hospitals in remodelling and refining their pandemic preparedness. In Pakistan, there is a dearth of literature regarding the attitudes and willingness of healthcare providers to work during a pandemic. For this reason, we set out to assess the willingness of doctors and medical students in Karachi, Pakistan to provide health services during the COVID-19 pandemic and to highlight the motivators and barriers that encourage and/or limit doctors from providing essential health services and medical students from volunteering during a pandemic.
Materials and Methods
Study Setting and Population
A cross-sectional, web-based survey was distributed in the months of June and July 2020 in Karachi, Pakistan to assess the risk perception and willingness to work among doctors and medical students during the COVID-19 pandemic. The sample size was calculated using “OpenEpi: Open Source Epidemiologic Statistics for Public Health”, using an anticipated frequency of 50% (p value = 0.5), confidence limits ± 5% and a confidence level of 95%. The sample size following the above calculation was 384. To account for non-response rate, the sample size was inflated by 10%. The final sample size was 423. Given the social distancing, restricted movement and lockdown being observed all over the country as a result of the COVID-19 pandemic, a web-based survey was chosen on the grounds of time, cost, and accessibility. The study participants included doctors and medical students residing in Karachi. Healthcare professionals and students practicing or training in the fields of nursing, pharmacy, dentistry, physiotherapy, laboratory technology, allied health sciences or homeopathy and doctors that have retired were excluded from the study.
Study Tool
A structured, self-administered questionnaire was adapted from a study by Rosychuk et al.2 The questionnaire was pretested and verified (validated) on a group of 50 participants. In the pilot survey, reliability of the study questionnaire was computed by Cronbach’s alpha and a value of 0.67 was acquired. The questionnaire comprising of 25 questions for doctors and 23 questions for medical students was launched via Google forms on June 21, 2020 and distributed to the public via social media platforms, such as WhatsApp, Twitter, Instagram and Facebook. Additionally, we requested the participants to further circulate the survey link among their colleagues. Prior to the commencement of the survey, online informed consent was taken from all participants. Absolute anonymity was maintained ensuring that all the information provided by the respondents cannot be linked back to them in any manner or form, as names or any other identifying information was not collected. The survey took approximately 10 minutes to complete and utilized skip logic. The questionnaire for doctors consisted of 25 questions (24 + 10 sub-questions): 8 requested socio-demographic information, 1 dealt with source of COVID-19 information, 4 focused on risk perception of COVID-19, 12 related to willingness to work during the pandemic and the consequences of not working. The questionnaire for medical students consisted of 23 questions (22 + 10 sub-questions): 7 requested socio-demographic information, 1 dealt with source of COVID-19 information, 4 focused on risk perception of COVID-19, 11 related to willingness to volunteer during the pandemic and the consequences of not volunteering. Responses were mostly either Yes, No or I do not know or a 5-point Likert scale ie on a continuum from strongly disagree to strongly agree.
Statistical Analysis
Data was entered and analyzed using Statistical Package for the Social Sciences software (SPSS) version 24.0. Mean ± Standard Deviation (SD) and Median (Inter Quartile Range, IQR) were computed for all quantitative variables. All the categorical variables were presented as frequencies and percentages. Chi-square test was applied between various categorical variables, to find possible statistical correlations. P-value <0.05 was considered statistically significant.
Results
Out of the 491 respondents surveyed, 104 responses were discarded as they were incomplete, giving us a response rate of 78.8%. From the final sample size of 387 respondents, 187 were doctors and 200 were medical students.
Socio-Demographics
The mean age of the doctors was 27.5 years (SD 4.2) and gender was predominantly female (64.2%). Resident doctors formed the bulk of our respondents (31.0%). Good health status was reported by 57.8% doctors and 52.9% disclosed that they refer to official sources such as WHO, CDC, medical journals, and physicians for COVID-19 information.
The mean age of medical students was 21.5 years (SD 1.4) and gender was predominantly female (71.0%). Medical students in their third clinical years formed the majority of the respondents (37.0%). Good health status was reported by 60.0% of the medical students and 44.5% disclosed that they refer to unofficial sources such as WhatsApp, Facebook, Instagram, television, newspaper, and friends and family for COVID-19 information. Tables S1 and S2 display the socio-demographic characteristics of doctors and medical students, respectively. Moreover, the academic year of study of medical students was significantly associated with the information sources referred to for COVID-19 (p = 0.01), wherein fourth year medical students referred to unofficial sources and second year medical students referred to both official and unofficial sources (Table S3).
Willingness to Work or Volunteer
Out of 187 doctors, 74.3% were working during the COVID-19 pandemic, of which 58.3% were willing to work, 10.7% were not willing to work and 5.3% said “I don’t know”, while 25.7% were not working during the pandemic, of which 16.6% were willing to work, 4.8% were not willing to work and 4.3% said “I don’t know”. Doctors were mostly willing to report for their usual shift (71.1%) during the COVID-19 pandemic (Table S4). The level of training of doctors was significantly associated with working during the pandemic (p = <0.05), willingness to work during the pandemic (p = 0.038), and maximum shift willing to work during the pandemic (p = 0.027), such that willingness to work during the pandemic was greater in medical officers while house officers were more willing to work extended shifts during the pandemic (Table S5).
Out of 200 medical students, an overwhelming majority (93.5%) were not volunteering during the COVID-19 pandemic, of which 46% were willing to volunteer, 13.5% were not willing to volunteer and 34% said “I don’t know”, while 6.5% were volunteering during the pandemic. Concerning the hospital roles that medical students would be willing to volunteer for, almost half (48.5%) were in favor of volunteering in the Non-COVID hospital units and 26.5% were willing to volunteer in both (Non-COVID & COVID) hospital units (Table S6). The academic year of study of medical students was significantly associated with willingness to volunteer during the pandemic (p = 0.031)—specifically in second year medical students—and with the hospital roles medical students are willing to volunteer for (p = 0.003) (Table S3).
Moral Obligations
A considerable majority (66.8%) of doctors believed it a moral obligation to work during the pandemic but, at the same time, 44.9% believed they should have the right to refuse treatment to COVID-19 patients. In the event of a shortage of doctors, 44.4% felt that the government would be justified in requiring them to work but simultaneously, 80.2% disapproved of being penalized if they refused. On further questioning, however, 8.6% felt that doctors should have a pay cut, 4.3% felt that doctors should be terminated from work, and 3.7% felt that doctors should be fined for refusing the government. In contrast, further assessment revealed that an overwhelming majority (94.1%), were in agreement that all doctors should receive Hazard pay. Lastly, 46.5% agreed that retired doctors should also be encouraged to volunteer during an HCW shortage (Table S4). The training level of doctors was significantly associated with the belief of whether doctors have a moral obligation to work during the pandemic (p = 0.003)—residents, in particular, were of the belief that it is not a moral obligation—and with the belief of whether retired doctors should be strongly encouraged to volunteer in the event of a shortage of doctors during the pandemic (p = 0.044) (Table S5).
Medical students were divided in their belief as 38% believed it a moral obligation for them to volunteer during the pandemic, 39% replied negatively. Upon asking if the government would be justified in requiring them to volunteer, 40.5% replied negatively. On further assessment, 87.0% felt that medical students should not be penalized if they refuse the government. Moreover, upon inquiry of the type of penalty involved, 7.0% felt that medical students should be fined and 0.5% felt that medical students should be expelled from university. Oppositely, 63.5% felt that all volunteers should be given financial compensation by the hospital or government for volunteering during the pandemic. Furthermore, 45% agreed that retired doctors should be encouraged to volunteer in the event of a shortage of doctors (Table S6).
Pandemic Courses and Training
In our study, a vast majority of doctors (81.8%) had not taken any pandemic courses or training (Table S4). The level of training of doctors was significantly associated with having taken any pandemic course or training (p = 0.016), more so in consultants who had taken pandemic courses (Table S5). Moreover, the majority of medical students (82.5%) had also not taken any pandemic course or training (Table S6).
Factors Influencing Willingness to Work During the Pandemic
Doctors strongly agreed that they would be willing to work during the COVID-19 pandemic if they were healthy and able to do so (57.2%), if they felt that they had sufficient knowledge and skill (34.8%), and if they were provided personal protective equipment (PPE) (51.3%). Additionally, doctors strongly agreed that they would be willing to work if they were offered Hazard pay (52.4%), if they were guaranteed a vaccine for their family and themselves at the earliest availability (55.6%), and if they were guaranteed coverage of treatment cost if they get infected while working (57.8%). Table 1 displays the factors influencing willingness to work of doctors and willingness to volunteer of medical students during the COVID-19 pandemic. The training level of doctors was significantly associated with willingness to work during the pandemic if they have sufficient knowledge and skill (p = 0.023), if they are provided with PPE (p = 0.038), if they are offered a separate accommodation during their duration of work (p = 0.002), and if they are provided with transportation to and back from the hospital (p = <0.05)—wherein residents were more willing if provided with separate accommodation, and medical officers were more willing if provided with separate accommodation as well as transportation (Table S5).
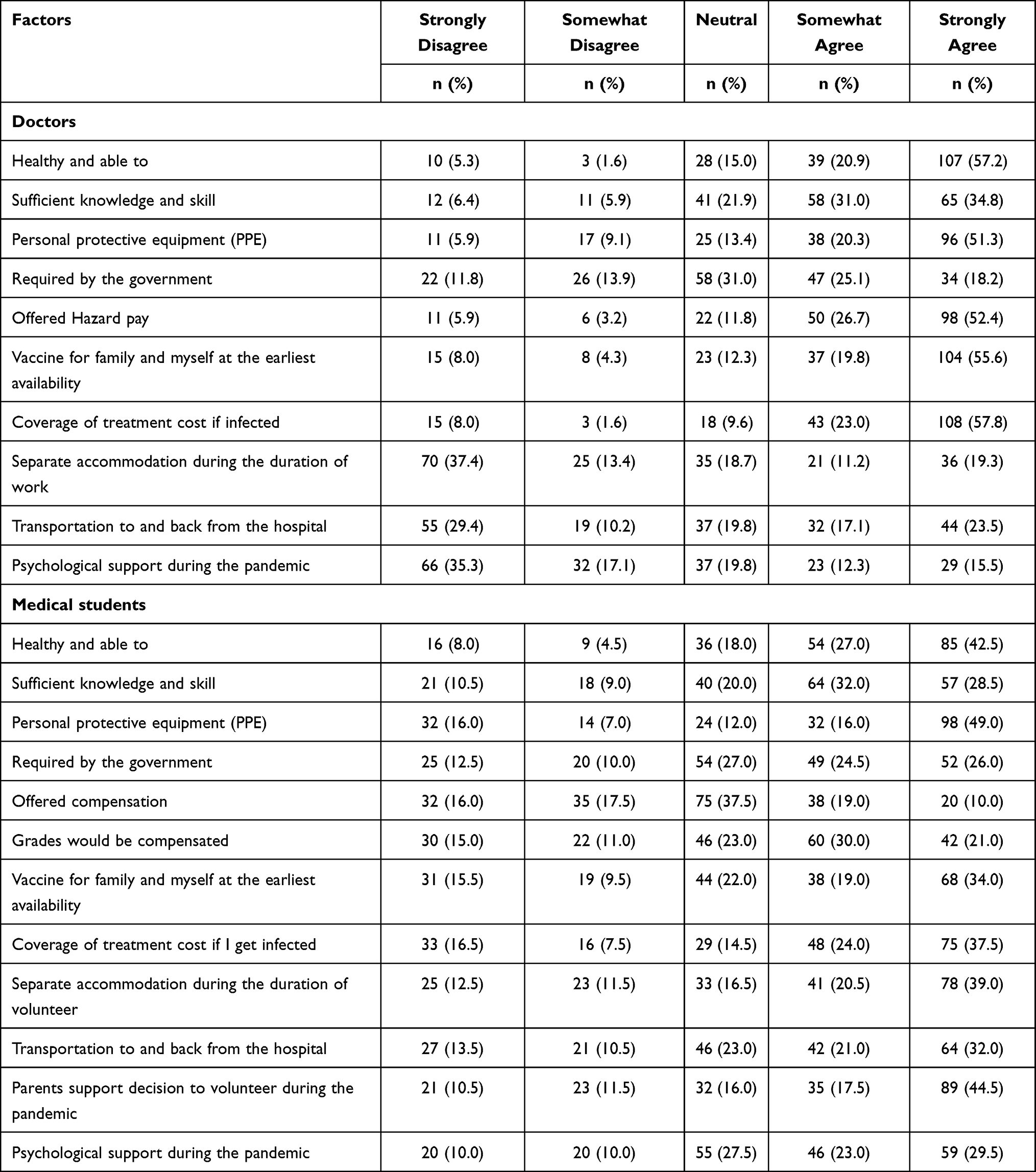 |
Table 1 Factors Influencing Willingness to Work of Doctors and Willingness to Volunteer of Medical Students During the COVID-19 Pandemic |
Medical students strongly agreed that they would be willing to volunteer during the COVID-19 pandemic if they were healthy and able to do so (42.5%), if they felt they had sufficient knowledge and skill (32.0%), and if they were provided PPE (49.0%). Additionally, medical students strongly agreed that they would be willing to volunteer if they were guaranteed a vaccine for their family and themselves at the earliest availability (34.0%), if they were guaranteed coverage of treatment cost if they get infected while volunteering (37.5%), if they were offered a separate accommodation during the duration of their volunteer work (39.0%), if they were provided with transportation to and back from the hospital (32.0%), and if their parents were supportive of their decision to volunteer (44.5%) (Table 1). The academic year of study of medical students was significantly associated with their willingness to volunteer during the pandemic if they felt they were healthy and able to (p = 0.023), and if they were offered compensation (p = 0.039), wherein third year medical students would be more willing if they were healthy and able to while final year medical students would be more willing if they were offered compensation. Additionally, academic year of study of medical students was significantly associated with their willingness to volunteer during the pandemic if they were assured their grades would not suffer and be compensated (p = 0.042), if they were guaranteed coverage of treatment cost if they get infected while volunteering (p = 0.043), if they were offered a separate accommodation during the duration of their volunteer work (p = 0.012), and if they were provided with psychological support (p = 0.024) (Table S3).
Risk Perception
Most doctors (54.5%) felt that they were extremely likely to get infected while working during the COVID-19 pandemic and 59.4% felt that in turn, they were extremely likely to infect their family as well. In the event of infection with COVID-19, 51.3% doctors felt that they would recover without hospitalization. Upon assessment of their level of confidence in the protection offered by PPE, the highest reported confidence was for face shields/goggles (44.4% “somewhat confident”). Table 2 discloses risk perception of doctors to work and medical students to volunteer during the COVID-19 pandemic as well as their confidence in PPE.
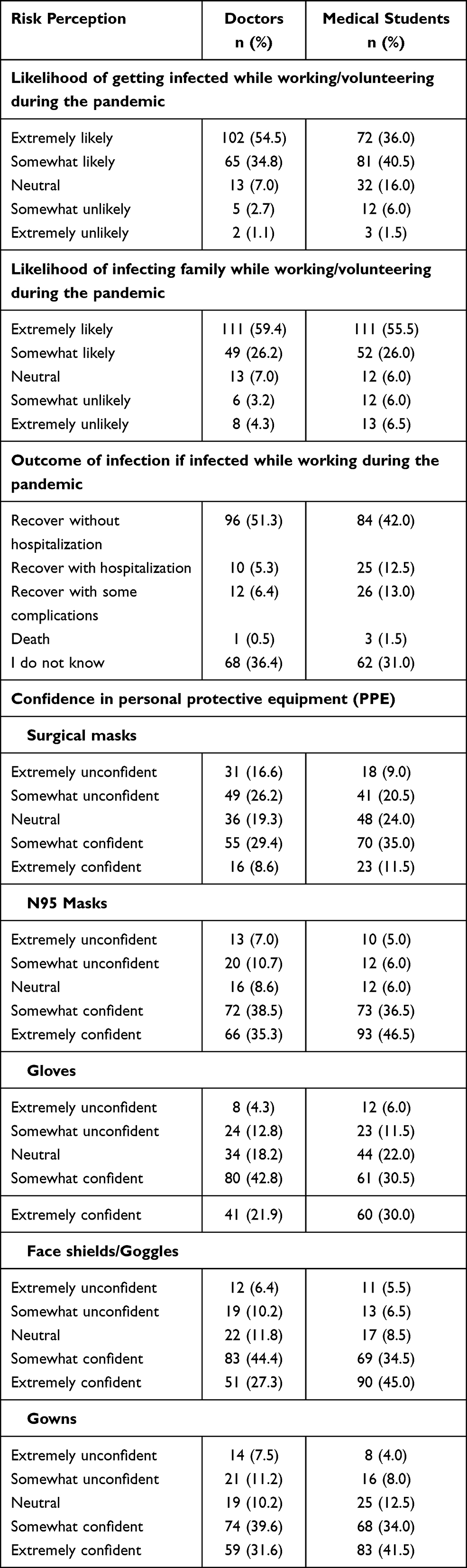 |
Table 2 Risk Perception of Doctors to Work and Medical Students to Volunteer During the COVID-19 Pandemic as Well as Their Respective Confidence in Personal Protective Equipment (PPE) |
Most medical students (40.5%) felt that they were somewhat likely to get infected while volunteering during the COVID-19 pandemic and 55.5% felt that in turn, they were extremely likely to infect their family as well. In the event of infection with COVID-19, 42.0% medical students felt that they would recover without hospitalization. Upon assessment of their level of confidence in the protection offered by PPE, the highest reported confidence was for N95 masks (46.5% “extremely confident”) (Table 2). The academic year of study was found to be significantly associated with the level of confidence in N95 masks (p = 0.070), Gloves (p = 0.016), and Gowns (p = 0.010) (Table S3).
Discussion
In our study, a high proportion of doctors (74.3%) were working during the COVID-19 pandemic, of which 58.3% were willing to work during the COVID-19 pandemic. A perusal of the literature published before the COVID-19 pandemic shows conflicting results, with hypothetical pandemic scenarios generally observing a higher willingness to work; 72% willingness observed in a study from Maryland, USA.7 On the other hand, willingness to work during past pandemics showed inconsistent results; 76.9% of community nurses were unwilling to work during the 2009 H1N1 influenza pandemic in Hong Kong8 whereas, in a study conducted in New York, a year after the H1N1 pandemic, 56.8% hospital workers said they would still be willing to work during a future pandemic.5
Gauging from the findings of previous similar studies, it is possible that the willingness to work observed in our study may also stem from a sense of professional obligation and general responsibility to continue working despite the potential risks, as 66.8% doctors believed it a moral obligation to work during the COVID-19 pandemic. Data from the influenza pandemic in the United Kingdom reported that 76.8% of the participants felt that doctors and nurses have a duty to work during a pandemic while at the same time one-third believed that HCWs should have the option to refuse to work with infected patients.9 Similarly in a study from Australia, 83.3% of the HCWs considered it a professional obligation to treat infected patients and work regardless of the possible risks.4
Nonetheless, even a small fraction of HCWs unwilling to work can be concerning especially during a pandemic, when patient influx more often than not exceeds hospital capacity. A frequently reported reason behind absenteeism during a pandemic is fear for personal and family safety.4,10 In our study, 59.4% of doctors felt that they were extremely likely to infect their family while working during the COVID-19 pandemic. This perceived risk of infection may be attributable to the higher average transmissibility (R0 = 2.5) of SARS-CoV-2 compared to SARS-CoV and influenza virus.11 A study analyzing the attitudes of Australian HCWs to pandemic influenza found that in the event of a family member getting infected, the rate of absenteeism doubled.4
Furthermore, a lack of confidence in the protection conferred by PPE may be an additional factor compounding the perceived risk of infection as the level of confidence observed in our study was lowest for surgical masks (38% confidence) and highest for N95 respirators (73.8% confidence). However, these fears are reasonably addressable as numerous studies have shown that with proper implementation of infection control measures, including appropriate use of PPE in the recommended settings and frequent hand hygiene, HCWs can significantly reduce the risk of self-contagion.12,13 With regards to confidence in PPE, a meta-analysis of 4 RCTs did not exhibit any superiority in the protection conferred by N95 respirators compared to medical masks against laboratory-confirmed viral infection or influenza.14 Likewise, providing HCWs with pandemic training and scheduling frequent intra-departmental discussions concerning new developments or protocols increases confidence in skill and knowledge while also optimizing patient care and boosting willingness to work. As supported by a recent meta-analysis involving 43 studies which showed that, confidence in personal safety, knowledge, and clinical skills as well as pandemic training are all positive influencers for willingness to work during a pandemic.15 In addition, employer and organizational preparedness towards the pandemic and provision of PPE are also motivators of willingness to work.15 It is also recommended that essential sector employers should plan out risk reduction measures and communicate them to HCWs.5
Moreover, certain personal obligations can arise that may interfere with HCWs ability to report to work, resulting in non-illness related absenteeism. This when compounded with illness-related absenteeism can create a shortage of HCW and reduce the efficiency of pandemic response. In such a case, recruiting medical students to supplement frontline HCWs may seem a feasible option but, simultaneously, it is worth mentioning that participation of medical students should be solely voluntary. In our study, more than half (52.5%) of the medical students said that they were willing to volunteer during the COVID-19 pandemic and there was a significant association (p= 0.031) of willingness to volunteer with the academic year of study. In a study on Belgian medical students, 70.8% of respondents were in agreement with the plan of their deployment in the event of an H5N1 influenza pandemic,16 while in another study, 87.8% of medical students from the United States (US) reported they would be willing to respond in the case of an influenza pandemic.17 However, it is important to bear in mind that the willingness to volunteer reported in these two studies is for hypothetical pandemic scenarios and therefore, is not an accurate representation of willingness to volunteer during an actual pandemic.
There are several factors influencing willingness to volunteer with the level of education and training, and provision of PPE being the most consistently reported motivators in literature3,17,18 as well as in our study findings. A study from the US revealed that 70% of medical students felt unready to take part in a crisis before taking a training course whereas, only 11% felt unskilled after training.19 Recently, a study from Spain highlighted that the majority of final year medical students working during the COVID-19 pandemic felt suboptimal in their skills and distressed.18 Therefore, to curb the emotional and physical adverse effects incurred by such crises it is equally important to provide psychological support as well. In our study, a significant association (p = 0.024) was observed between academic year of study and willingness to volunteer if provided with psychological support during the COVID-19 pandemic.
Despite the high willingness, it should not be expected of medical students to channel this spirit of volunteerism in dealing directly with COVID-19 patients. In our study, 48.5% of medical students were willing to volunteer in non-COVID hospital units, and 26.5% of medical students were willing to volunteer in both COVID and non-COVID-19 units. Indirect COVID-19 related patient roles that medical students can be assigned include monitoring and follow-up of COVID-19 patients via tele-clinics or handling hospital COVID-19 information helplines; while non-COVID hospital roles to consider include hospital clerical duties of maintaining patient records and files or scheduling appointments. Granted that hospitals and the government have limited funds, nevertheless, medical students in our study agreed that all volunteers should receive monetary compensation and 53% agreed to volunteer if offered priority access to the vaccine for themselves and their families. Conversely, a study on nursing students observed that 63.7% were in disagreement with receiving monetary compensation for volunteering whilst 60.8% agreed that volunteers should be given first access to scarce health resources or vaccines.3
We acknowledge that our study has certain limitations. First, considering the cross-sectional nature of our study, it provides a “snapshot” of responses at one moment in time. The study was undertaken in a single large city thus, limiting the generalizability of the findings to the rest of the country. However, considering the cultural context of Pakistan, we feel our findings, although not entirely reflective, are informative for other provinces. Since the study is a cross-sectional study, it is subjected to recall and participant biases. Majority of the doctors in our study were actively working during the COVID-19 pandemic; it is possible that we were unable to review those who had resigned immediately once the pandemic started because of serious physical or psychological effects. Our study did not catch rural areas as data was collected on electronic medium and hence, more studies need to be conducted to assess this point of view. Lastly, we recommend that a larger nationalized survey should be conducted to obtain a comprehensive outlook of perception and willingness to work among healthcare workers and healthcare students of Pakistan during the COVID-19 pandemic.
Conclusion
Our study revealed several factors associated with willingness to work or volunteer during the COVID-19 pandemic. Since future pandemics are likely, prior preparedness is key and therefore we encourage medical faculties, research centers, policymakers and health authorities to utilize the findings of this study. Integrating pandemic training into hospital and university courses with special emphasis on resilience training would serve as an appropriate initial step. Moreover, there is a need for policymakers and relevant health authorities to establish a formal healthcare student volunteer organization and maintain recruitment and registration of this volunteer network so that they may be deployed into a formal emergency/disaster response system when needed. Further recommendations for employers and institutions include the provision of adequate PPE, scheduling frequent correspondence regarding pandemic preparedness with hospital staff to boost confidence levels, as well as making arrangements for psychosocial support. Pandemics can be long and gruelling; therefore, it is crucial to address the factors influencing willingness to work or volunteer, so as to create a sustainable and robust pandemic response.
Ethics Approval
This study was approved by the Institutional Review Board of Dow University of Health Sciences. Participation in this study was voluntary and informed consent was obtained from all the participants. To ensure anonymity and confidentiality of the participants, no medical or personal information such as names, contact information or addresses was required. Hence, the responses received were anonymous and no personal data were obtained. Also, we confirm that this study was conducted in accordance with the declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cascella M, Rajnik M, Aleem A, Dulebohn SC, Di Napoli R. Features, evaluation, and treatment of coronavirus (COVID-19). In: StatPearls. Treasure Island (FL): StatPearls Publishing; April 20, 2021.
2. Rosychuk RJ, Bailey T, Haines C, et al. Willingness to volunteer during an influenza pandemic: perspectives from students and staff at a large Canadian university. Influenza Other Respir Viruses. 2008;2(2):71–79. doi:10.1111/j.1750-2659.2008.00042.x
3. Yonge O, Rosychuk RJ, Bailey TM, Lake R, Marrie TJ. Willingness of university nursing students to volunteer during a pandemic. Public Health Nurs. 2010;27(2):174–180. doi:10.1111/j.1525-1446.2010.00839.x
4. Seale H, Leask J, Po K, MacIntyre CR. “Will they just pack up and leave?” - attitudes and intended behaviour of hospital health care workers during an influenza pandemic. BMC Health Serv Res. 2009;9:30. doi:10.1186/1472-6963-9-30
5. Gershon RR, Magda LA, Qureshi KA, et al. Factors associated with the ability and willingness of essential workers to report to duty during a pandemic. J Occup Environ Med. 2010;52(10):995–1003. doi:10.1097/JOM.0b013e3181f43872
6. Qureshi K, Gershon RR, Sherman MF, et al. Health care workers’ ability and willingness to report to duty during catastrophic disasters. J Urban Health. 2005;82(3):378–388. doi:10.1093/jurban/jti086
7. Balicer RD, Barnett DJ, Thompson CB, et al. Characterizing hospital workers’ willingness to report to duty in an influenza pandemic through threat- and efficacy-based assessment. BMC Public Health. 2010;10:436. doi:10.1186/1471-2458-10-436
8. Wong EL, Wong SY, Kung K, Cheung AW, Gao TT, Griffiths S. Will the community nurse continue to function during H1N1 influenza pandemic: a cross-sectional study of Hong Kong community nurses? BMC Health Serv Res. 2010;10:107. doi:10.1186/1472-6963-10-107
9. Damery S, Draper H, Wilson S, et al. Healthcare workers’ perceptions of the duty to work during an influenza pandemic. J Med Ethics. 2010;36(1):12–18. doi:10.1136/jme.2009.032821
10. Seale H, Wang Q, Yang P, et al. Hospital health care workers’ understanding of and attitudes toward pandemic influenza in Beijing. Asia Pac J Public Health. 2012;24(1):39–47. doi:10.1177/1010539510365097
11. Petersen E, Koopmans M, Go U, et al. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect Dis. 2020;20(9):e238–e244. doi:10.1016/S1473-3099(20)30484-9
12. Sommerstein R, Fux CA, Vuichard-Gysin D, et al. Risk of SARS-CoV-2 transmission by aerosols, the rational use of masks, and protection of healthcare workers from COVID-19. Antimicrob Resist Infect Control. 2020;9(1):100. doi:10.1186/s13756-020-00763-0
13. Chu DK, Akl EA, Duda S, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395(10242):1973–1987. doi:10.1016/S0140-6736(20)31142-9
14. Bartoszko JJ, Farooqi MAM, Alhazzani W, Loeb M. Medical masks vs N95 respirators for preventing COVID-19 in healthcare workers: a systematic review and meta-analysis of randomized trials. Influenza Other Respir Viruses. 2020;14(4):365–373. doi:10.1111/irv.12745
15. Aoyagi Y, Beck CR, Dingwall R, Nguyen-Van-Tam JS. Healthcare workers’ willingness to work during an influenza pandemic: a systematic review and meta-analysis. Influenza Other Respir Viruses. 2015;9(3):120–130. doi:10.1111/irv.12310
16. Mortelmans LJ, De Cauwer HG, Van Dyck E, Monballyu P, Van Giel R, Van Turnhout E. Are Belgian senior medical students ready to deliver basic medical care in case of a H5N1 pandemic? Prehosp Disaster Med. 2009;24(5):438–442. doi:10.1017/s1049023x00007287
17. Kaiser HE, Barnett DJ, Hsu EB, Kirsch TD, James JJ, Subbarao I. Perspectives of future physicians on disaster medicine and public health preparedness: challenges of building a capable and sustainable auxiliary medical workforce. Disaster Med Public Health Prep. 2009;3(4):210–216. doi:10.1097/DMP.0b013e3181aa242a
18. Collado-Boira EJ, Ruiz-Palomino E, Salas-Media P, Folch-Ayora A, Muriach M, Baliño P. “The COVID-19 outbreak”-An empirical phenomenological study on perceptions and psychosocial considerations surrounding the immediate incorporation of final-year Spanish nursing and medical students into the health system. Nurse Educ Today. 2020;92:104504. doi:10.1016/j.nedt.2020.104504
19. Patel VM, Dahl-Grove D. Disaster preparedness medical school elective: bridging the gap between volunteer eagerness and readiness. Pediatr Emerg Care. 2018;34(7):492–496. doi:10.1097/PEC.0000000000000806
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.