")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Risk Perception and Health Precautions Towards COVID-19 Among Older Culturally and Linguistically Diverse Adults in South Australia: A Cross-Sectional Survey
Authors Hamiduzzaman M , Siddiquee N, McLaren H, Tareque MI , Smith A
Received 12 October 2021
Accepted for publication 9 March 2022
Published 15 March 2022 Volume 2022:15 Pages 497—514
DOI https://doi.org/10.2147/JMDH.S343985
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Mohammad Hamiduzzaman,1 Noore Siddiquee,2 Helen McLaren,3 Md Ismail Tareque,4 Anthony Smith1
1The University of Newcastle Department of Rural Health, University of Newcastle, Taree, Australia; 2College of Business, Government & Law Flinders University, South Australia, Australia; 3College of Education, Psychology and Social Work, Flinders University, Adelaide, Australia; 4Department of Population Science and Human Resource Development University of Rajshahi, Rajshahi, 6205, Bangladesh
Correspondence: Mohammad Hamiduzzaman, Research Fellow, The University of Newcastle Department of Rural Health, University of Newcastle, NSW, Australia, Email [email protected]
Background: Risk perceptions and precaution-taking against COVID-19 are affected by individuals’ health status, psychosocial vulnerabilities and cultural dimensions. This cross-sectional study investigates risk perceptions associated with COVID-19 and specifically the problem- and emotion-focused health precautions of older, culturally and linguistically diverse (CALD) South Australians.
Methods: Cross-sectional research involving self-administration of an online survey. Participants were CALD adults living in South Australia, aged 60 years and above (n = 155). Multi-indicator surveys were analyzed using Stata/MP version 13.0 and multiple linear regression models fitted to examine associations between risk perceptions and problem- and emotion-focused health precautions.
Results: Dread risk returned the highest mean score; COVID-19 was perceived as a catastrophe. Mean scores for fear showed that participants were worried about COVID-19 and scared of becoming infected. Participants followed health advice as they were worried [β 0.15; 95% CI 0.07, 0.23] and realized the effect of COVID-19 on them [β 0.15; 95% CI 0.02, 0.28], or worried and had trust in experts’ knowledge and managing capacity [β 0.17; 95% CI 0.06, 0.28]. Age was negatively associated with sum-score of problem-focused coping: compared to participants aged 60– 69 years, 80+ years revealed a decrease in problem-focused health precautions. Variables like education (primary schooling [β 2.80; 95% CI 0.05, 5.55] and bachelor degree [β 3.16; 95% CI 0.07, 6.25] versus no formal education), self-confidence in reducing risk, and fear [β 0.84; 95% CI 0.31, 1.36] significantly affected emotional-focused health precautions.
Conclusion: This local study has global implications. It showed that COVID-19 has psychosocial and environmental implications for older CALD adults. When many CALD populations have existing vulnerabilities to intersecting disadvantage, cultural-tailoring of interventions and pandemic response plans may buffer the effects of compounding disaster. Larger studies are needed to compare risk perception and health response patterns across countries and cultural groupings.
Keywords: culturally and linguistically diverse community, older adults, risk perceptions, behavioral coping, emotional precautions, South Australia
Introduction
Australia recorded its first case Of COVID-19 on January 25, 2020. Early action helped to limit the spread and containment Of COVID-19, such as with social distancing, restricting international and inter-state travels, and quarantines for passengers arriving from overseas.1,2 Political decisions and health initiatives emphasized protecting certain members Of society as a priority, particularly those with ageing or disability related health conditions that increase vulnerability to COVID-19 infection.2 Residential aged care facilities in Australia, for example, restricted visits to limit the spread of disease,3 and telehealth services targeted at Australians ageing in-place.4 However, there is no retirement age in Australia (except for Judges legislated at 80yrs), and many older people undertake work or business well into their older years. Many have suffered lost livelihoods, diminished opportunity to save for retirement, and exacerbated financial insecurities due to the pandemic.5 There has also been loss of purpose and sense of agency associated with the psychological intangibility of COVID-19 in Australia, low infection rates and fear of the unknown.6
While pandemic efforts have kept most Australians safe from infection, many have experienced mental health and adversity associated with the highly restrictive lockdowns.7 In addition, experiences of fear and perceptions of risk may differ according to gender and cultural demography,8 which interact with formation of personality. These various factors have a role in negative progressive experience of risk, which is likely compounded by pre-COVID-19 experience of life adversities among older minority populations.9,10 As such, people who experience adversity may also perceive a greater risk leading to a variety of problem- and emotion-focused health precautions against COVID-19. Older culturally and linguistically diverse (CALD) adults in Australia is one such group that may have heightened risk perception and where increased problem- and emotional-health precautions may be an issue.
International studies have sought to understand the impact of COVID-19 on various populations. In a sample of 98 healthy adults, Mariani et al (2021) undertook a study in Italy on personality and emotional regulation three months prior to the pandemic, and repeated the study three months into the pandemic participants from the original sample.11 They showed that COVID-19 lockdown impacted emotional regulation and primary emotional systems, having negative progressive experience in perception of risk related to the pandemic situation.11 Kuo et al (2021) completed a 1-year longitudinal study of 139 older people in Taiwan.12 During an initial COVID-19 outbreak period, they showed a significant increase in fear of COVID-19 but no significant change to preventative behaviours. At follow up, preventative behaviours were significant indicating that negative progression in psychological status correlated with precaution behaviours. From the same study of 139 older people in Taiwan, Li et al (2021) showed that women who engaged with news reports and practice good infection prevention behaviours had lower levels of fear of COVID-19 compared to men.13 Pakpour et al (2021) replicated the study from Taiwan and compared results with their Iranian sample of 144 older people (>60 yrs) and also showed that fear was higher when precautionary behaviour was lower.14 Alternatively, Ahorsu et al (2020) surveyed 413 older adults (>50 yrs) in Iran and showed significant associations between insomnia, mental health, fear of covid, and health precautions.15 In this older population, the majority perceived they had poor health status, this was positively correlate with fear, fear of COVID-19 correlated with increased anxiety, and anxiety affected their sleep. While it is not known whether these studies were of native-born samples, it is not known whether similar results would be found in Australia among older CALD adults.
Approximately one quarter of people in Australia are born overseas, 46% have a parent born overseas, and 20% speak a language other than English in their home.16–18 The majority of Australia’s CALD population are from countries in Asia and Sub-Saharan Africa, and less from non-English speaking European countries such as Italy, Greece and Germany.17 CALD populations suffer from language barriers, lower socioeconomic status, poorer living conditions, and often they live in relative isolation having been separated through immigration from filial and social networks. They also have higher mortality rates compared to native Australians.19 CALD populations experience higher rates of disadvantage in the event of natural disasters, as they lack equitable access to information and services in Australia, have poorer health literacy, and are often unprepared for disasters, response and recovery measures.16,20,21 In order to advocate development of policy and practice frameworks in support of populations in greater need, this leads to our specific interest in the study of older CALD populations in Australia and their perceptions of risk and precautions related to COVID-19 during the first year of the pandemic.
This study’s overall aim was to investigate the associations between COVID-19 risk perceptions and precautions among CALD adults, aged 60 years and over, living in South Australia. While there is no clear definition of what constitutes being old, in Australia old is often conceptualized as the common retirement age of 65 years.17 What constitutes old differs across cultures, generations and countries. For the purpose of our study on CALD populations, we adopted the United Nations definition of old age to be 60 years or older.22 Specifically, explored the risk perception of being infected and/or affected by COVID-19 among older CALD people in South Australia and its association with the sample’s problem- and emotion-focused precautions.
Theoretical Perspectives and Assumptions
This study adhered to the principles of Richard Lazarus’s transactional theory of stress to explain the psychological and emotional health of older CALD adults.23,24 This theory signifies stress as a consequence of transaction of a person’s intellectual, physical, emotional, mental, neural aspects with his/her complex living circumstances.23 In the COVID-19 pandemic, the rapid spread of infections, associated symptoms and health conditions, together with physical (social) distancing and stay-at-home protocols, likely contribute to an experience of stress by older adults especially those among racial and ethnic minorities.
Older CALD adults are at increased risk of psychological and emotional health adversity associated with the pandemic.19,25,26 Many are ageing-in-place in the communities and have loneliness and prolonged exposure to cultural shocks and isolation since migration from their motherlands.19,27,28 The national or global health crisis, that is the COVID-19 pandemic, has interrupted normal activities of daily living and access to support services, such as homecare assistance, communications, and personal and emotional care.29 When the vast majority of older Australians both living alone and ageing-in-place experience high prevalence of psychological disorders,17 changes causal to COVD-19 are probable.
Psychiatric symptoms, isolation and loneliness are known to co-exist among older adults, especially those who are CALD and who may already be experiencing marginalization in Australia.28 Marginalization limits and interferes with the ability to prepare for and respond to large-scale disruptions in their lives.27 For example, the COVID-19 outbreak occurred in the wake of Australia’s 2019–2020 bushfire season in which almost 4.3 million hectares of land was destroyed, 3094 houses were lost and 33 people perished, with older Australians experiencing much higher rates of adverse health outcomes than young adults.30 The pandemic has likely compounded existing disaster and marginalization experiences of older CALD adults. It is possible that they are, therefore, at greater risk of psychological and emotional disorders and coping with the COVID-19 crisis. Despite the insightful appeal, these assumptions related to risk of COVID-19 infections, its effects on the older CALD adults, and their approaches to the pandemic remain untested and are unknown.
Theoretically, the cognitive, emotional, and social dimensions in combination characterize and direct individual’s risk perceptions.23,31 However, the COVID-19 literature on older adults’ coping behaviors underscores the importance of literacy and familiarity with the SARS-CoV-2 virus to address dread, unknown risks and fear about the effects of the pandemic.32 The relationship between risk perceptions and problem-focused coping has been the focus of several studies.25,31,33 Lohiniva et al (2020) collected qualitative data and grouped the findings into five risk perception domains: catastrophic potential; probability of dying; reasons for exposure; belief of being in control of the situation; and trust toward authorities.34 In a cross-cultural study in America, Europe, and Asia, Dryhurst et al (2020) revealed the influence of experience of virus, personal, and collective efficacy, knowledge, trust in governments’ initiatives, and professional advice on risk perceptions.35 Kwok et al (2020) found that risk perceptions of older adults toward COVID-19 was high, and most of them adopted problem-focused measures, perceiving them as effective.36 Additionally, De Bruin and Bennett (2020) assessed the older adults’ risks of COVID-19 infection and mortality and found that those who perceived greater risks were more likely to adopt protective measures.37 These studies investigated the older adults’ risk perceptions, including the CALD communities and their problem-focused coping with COVID-19. However, no studies could be found that have had exclusive focus on CALD communities’ problem-focused precautions in the pandemic. Investigating the relationships of the older CALD adults’ demographics and risk perceptions with their likelihood of practicing problem-focused precautions may inform the culturally-tailored response planning for these groups.
Emotional coping has been theorized in this study, using the microanalytic trait oriented coping theory that indicates a bipolar dimension - repression and sensitization - where an individual copes with stress either by denying the existence or reacting with rumination and obsession.38 COVID-19 has recently been characterized by WHO and the Australian Government as a “Controllable Pandemic”, in which all communities should work together within and across the nations. However, as a global and national catastrophe, the pandemic has been influencing the older Australians’ emotional states. Such emotional states are related with anxiety, frustration, confusion, uncertainty and inadequacy, which may provoke destructive consequences during or post-pandemic situations; for example, suicides and aggression.39,40 Flesia et al (2020) revealed that the unpredictability and uncontrollability of the COVID-19 lockdown had an impact on emotional wellbeing.41 Emotional precaution refers to the cognitive efforts that can help to decrease the burden of a traumatic situation.23,24 A recent study by Fuller and Huseth-Zosel (2021) reported that mean perceived emotional coping level of older adults was 7.9 (on a scale 1–10), where 87% of them rated their coping positively.19 The authors also related emotional coping with staying busy, seeking social support, and having a positive mindset. Minahan et al (2021) identified the avoidant coping as the strongest mediator of the relationship between pandemic-related stress and emotional precautions.42 These emotion-focused precautions appeared adaptive for most older adults in effort to show ameliorate perceived risks. Living in a culturally and linguistically different country during the pandemic is a challenge, especially for older adults who mostly rely on their family members and own community for emotional care. Emotional precaution in terms of repression and sensitization is an important aspect to be considered in order to understand how older CALD adults perceive and respond to risk during the pandemic.
Materials and Methods
This study employed a cross-sectional research design, involving demographic data collection and assessment of risk perceptions and precautions in older CALD adults. Approval for the study was received from the Flinders University Human Research Ethics Committee (ID 2215), following study protocols that were compliant with the Declaration of Helsinki 2000.
Sample and Data
At the time we commenced writing this article, in August 2021, South Australia was nearing 900 cases of COVID-19. This was the fifth lowest number of cases in comparison to Australia’s other states and territories. Despite the low numbers, COVID-19 has impacted the economy and socio-cultural circumstances of South Australia in general, and its healthcare and social services in particular. There had been three highly restrictive lockdowns. Strict limits were placed on international and domestic cross-border travel, and nonessential business operations. This had the potential to impact older CALD residents, many who had family networks dispersed across Australia and internationally.
South Australia is the home of people from 200 countries, who speak in 300 languages, and are affiliated with about 100 religions. The health system has a history of excellence in patient care, however older CALD adults’ health literacy, beliefs and behaviours in South Australia has always been an issue of concern in the field of public health.21 The COVID-19 crisis presents a challenging situation for these older adults living in South Australia. Given the above, the older CALD South Australians provide an important empirical context to study their COVID-19 risk perceptions and likelihood of practicing problem- and emotion-focused precautions in such a well-managed health environment.
On receipt of research ethics approval, an online survey was administered to older CALD adults (≥60 years) in South Australia from July 1 to December 31, 2020. During this time South Australia experienced intermittent lockdown, social distancing and other health measures designed to control the spread of COVID-19. The survey was designed in English to avoid the complexity of translating the questionnaire for all CALD communities. Several procedures as suggested in Podsakoff et al (2003) were adopted at the data collection stage to reduce the likelihood of respondents providing socially desirable answers such as ensured protection for participants’ anonymity, reduced the evaluation apprehension by saying in the participation information sheet that they should answer questions from an honest perspective, and improved the scale items through logical construction of the questions.43 While the scale was not validated, but the quality of the scale items for the older adults has been ensured by evidence and expert opinions. The items have been gathered from different research studies which investigated the same topic and included older adults as participants such as Gerhold (2020), Lanciano et al (2020), Minahan et al (2021), and Rojas-Lizana and Cordella (2020). Also, expert opinions were sought from social gerontologists in the process of scale development, eg, avoided confusing questions and kept the response choices simple and clear.
The survey [SurveyGizmo] was administered by sending an email request to 11 South Australian multicultural Non-Government Organisations. All multicultural Non-Government Organisations in South Australia were identified through South Australia Directory of Community Services and approached them to voluntarily distribute the Participation Information Sheet and Survey Link to their community members. Of them, 11 organisations agreed to support the project. Regular contact was made with the Non-Government Organisations in promoting the project via their organisations’ Web and Facebook pages to invite participation. Interested individuals responding to calls for participants were provided instructions on how to complete and submit the questionnaire online. None of the 155 respondents reported having tested positive for COVID-19. Participants’ confidentiality was maintained throughout the research process.
Measures of Variables
The 19-indicator ways (details in Supplementary File 1) of precaution practice scale was used, drawing on Folkman & Lazarus’s (1988) problem-focused and emotion-focused strategies.44 The scale includes nine items about problem-focused precautions and 10 items about emotional precautions for coping with the COVID-19 crisis. All items had 5-point Likert scales (1 = “strongly disagree” to 5 = “strongly agree”). The internal consistency among the nine items of problem-focused precautions (Cronbach’s α = 0.80) and among the 10 items of emotional precautions (Cronbach’s α = 0.70) indicate that the items are closely related and acceptable to form two separate group-scale for problem-focused and emotional precautions. In addition to 19 separate indicators, two sum-scores (nine items of problem-focused precautions, and 10 items of emotional precautions) were considered.
Several demographic characteristics and risk perception indicators were considered as explanatory variables in this study. Demographic characteristics include participants’ age (classified as 60–69, 70–79, and 80+ years), gender (male or female), education (no formal education, primary school, high school, Bachelor degree, or Masters and above), and ethnicity (country of birth; categorised as Asian, African, or non-English speaking European).
Two aspects of risk perception (15 indicators; detailed in the Appendix: Supplementary File 1. Survey Questionnaire) were considered. While the first one asks respondents to give a personal rating of the likelihood of being affected by COVID-19, the second focuses on fear and general concerns. The modified version [ie, a 15-indicator risk perception scale] of Gerhold’s (2020) COVID-19 risk perception measure was used,31 which was developed based on Slovic’s (1987) psychometric concepts:45 a. cognitive [ie, likelihood of being affected] and affective dimension [ie, fear and general concerns]; and b. psychometric paradigm [ie, severity, controllability, and personal impact]. In brief, the 15-indicator risk perception scale includes three items asking respondents to rate the perceived future likelihood of becoming infected by COVID-19, six items designed to elicit information about their personal feelings of dread risks, four items addressing the unknown risks, and two items about their fear of COVID-19. The three items in risk perception of being infected section had 5-point Likert scales (1 = “very unlikely” to 5 = “very likely”). All other items had 5-point Likert scales (1 = “strongly disagree” to 5 = “strongly agree”). The internal consistency among the three items of becoming infected (Cronbach’s α = 0.91) and among the two items of fear (Cronbach’s α = 0.89) indicate that the items are closely related and good to form two separate group-scale for becoming infected and fear. Therefore, instead of separate items for becoming infected and the fear, a sum-score of becoming infected and a sum-score of fear were used.
Models and Data Analysis Procedure
In the dataset (n=155), information on risk perception (15 indicators) and problem and emotion-focused precautions (19 indicators) were missing for 22.58% (n=35) participants. Mode imputation was used to impute missing cases, separately for each indicator. After imputation, internal consistencies among the risk perception and precautions related items were separately checked, and a few sum-scores were generated for the items whose internal consistencies were ≥ 0.70 (Cronbach’s α = 0.70).
Descriptive analysis was then conducted for demographics and the indicators of risk perceptions and the problem- and emotion-focused precautions. To examine the associations of the explanatory variables with the outcome measures, several multiple linear regression models (shown below) were fitted. Multicollinearity was checked in the regression analyses by examining the tolerance values. Tolerance values less than 0.40 indicate numerical problems such as multicollinearity among the explanatory variables (Chan 2004).46 No evidence of multicollinearity was observed. No sampling weights were provided with the data as such we do not apply sampling weights in the analyses. The analysis was performed with Stata/MP version 13.0 (StataCorp, LP, College Station, Texas, USA).
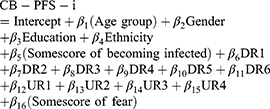
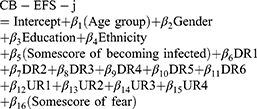
Equations (i) to (iv) are the fitted linear regression models, where different outcomes but the same explanatory variables were utilized. Beta represents the regression parameter. All outcomes and explanatory variables were elaborated in corresponding tables. Equation (i) was fitted for 9 outcomes of problem-focused precautions, where i ranges from 1 to 9.
Equation (ii) was fitted for 10 outcomes of emotion-focused precautions, where j ranges from 1 to 10.
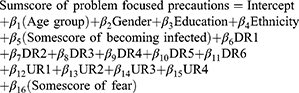
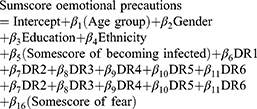
Equation (iii) and (iv) were fitted separately for two outcomes of problem-focused and emotional precautions.
Results
Descriptive Statistics
A total of 155 older adults (≥60 years) from 28 CALD communities completed the survey. Table 1 presents descriptive statistics. Among the participants, 22% were 60–69 years, 50.3% were 70–79, and the rest were 80+ years. 74.2% were female, and 53.6% were with high school or above education. In terms of ethnicity, 80.6% were non-English speaking European [self-nominated CALD], 16.8% Asian, and 2.6% African by background.
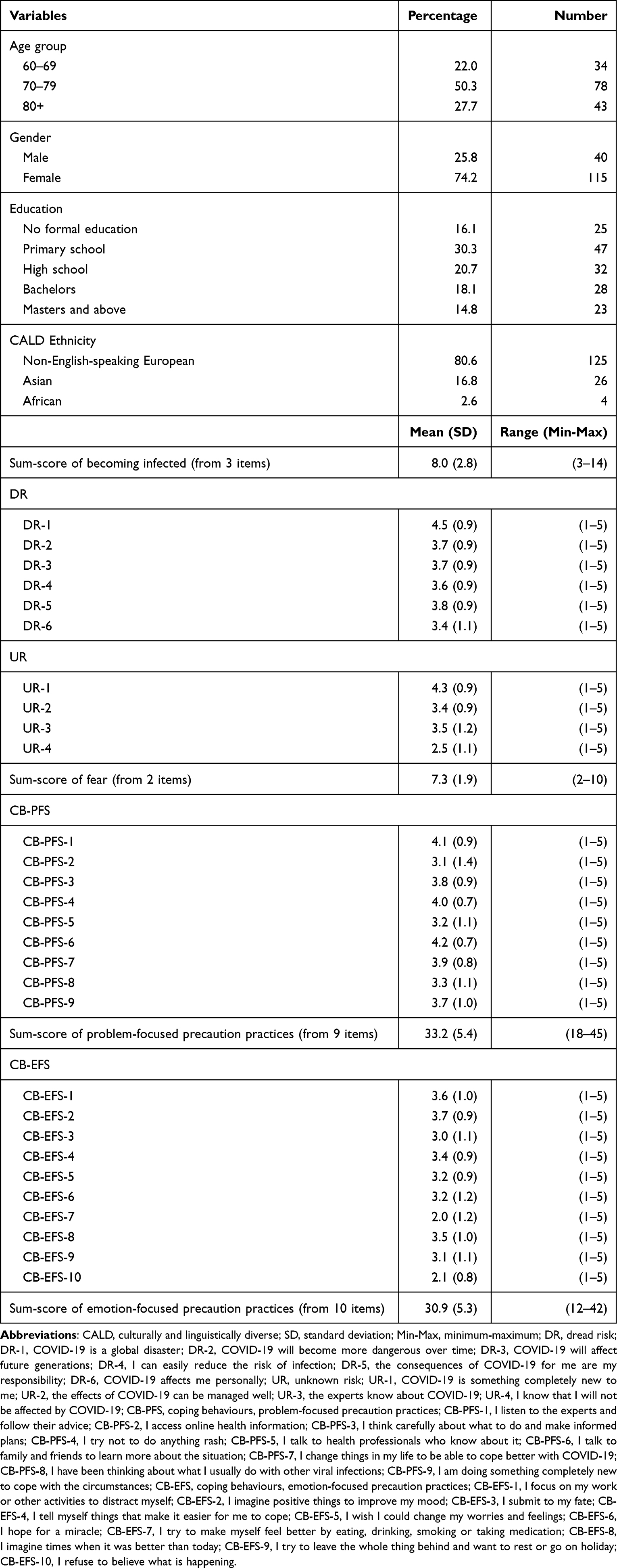 |
Table 1 Descriptive Statistics of Demographics and the Indicators of Risk Perceptions and Precautions (n=155) |
Table 2 shows the associations of explanatory variables with nine items of problem-focused precautions. Compared to respondents aged 60–69 years, those aged 80+ years old showed a 0.57 unit decrease in listening and following the expert advice. One unit increase in the perception of COVID-19 effect on participants was associated with a 0.15 unit increase in CB-PFS-1. The participants who perceived that COVID-19 could affect them personally and only experts know about COVID-19 positively influenced their commitment to seek expert advice. The fear factor was also positively associated with following expert advice.
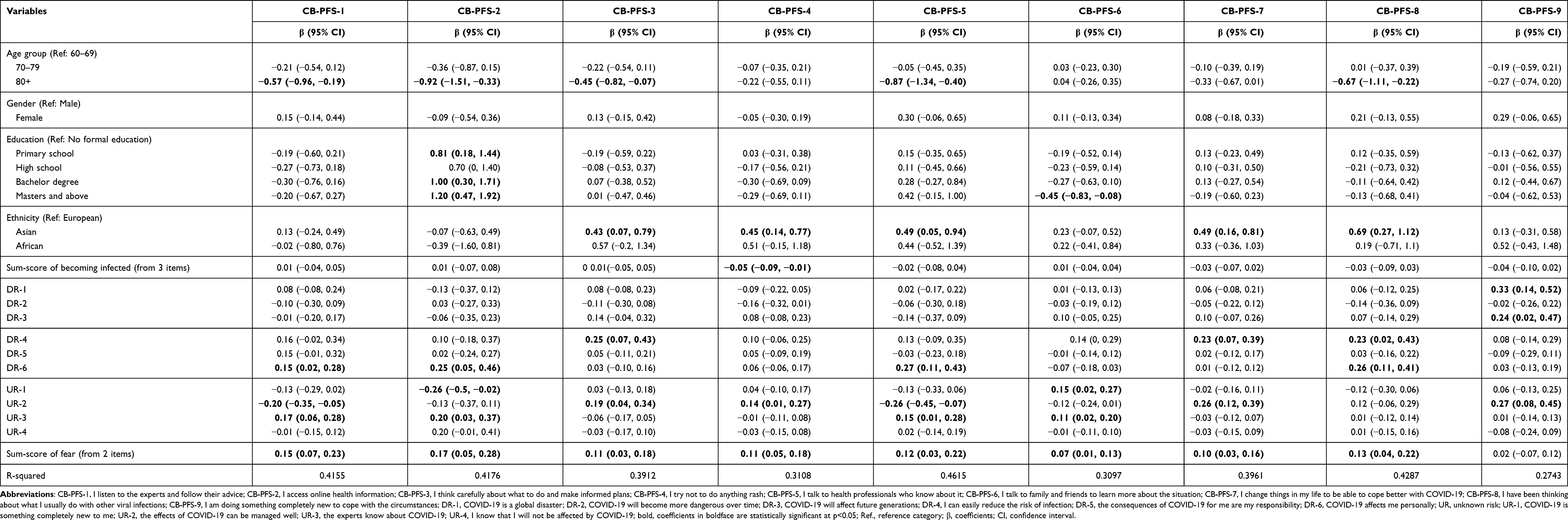 |
Table 2 Multiple Linear Regression Models Explaining the Problem-Focused Precautions (n=155) |
The frequency of online health information access was positively influenced by the participants’ education [for Master and above (versus no formal education), fear, perceptions of COVID-19 could affect them personally, and experts know how to manage COVID-19. Only age (80 years and over) had a negative influence on the participants making informed plans, whereas others were positively associated, including: ethnicity (Asian versus non-English Speaking CALD European); self-confidence in reducing the risk of infection and managing the effects of COVID-19, and fear. For the item of “not doing anything rush”, positively associated variables included: ethnicity (for Asian versus non-English Speaking CALD European); positive perceptions about managing the effects of COVID-19; and sum-score of fear.
The frequency of talking to health professionals was positively influenced by: ethnicity, perceptions that COVID-19 could affect them personally, only experts know about COVID-19, and fear. Learning about COVID-19 from family and friends was negatively associated with post-graduate degree. Changing things by the participants to cope better with COVID-19 was positively influenced by their ethnicity, fear, and self-confidence. Three items of risk perceptions ― COVID-19 is a global disaster, COVID-19 will affect future generations, and the effects of COVID-19 can be managed well - positively influenced the participants to do something completely new to cope with the pandemic.
Table 3 revealed that the participants’ tendency to often focus on work to distract themselves was positively associated with female (versus male), fear, and perception that the effects of COVID-19 can be managed well. For the item, “I tell myself thing that makes it easier for me to cope”, the participants’ gender [female (versus male), education, and perception that the effects of COVID-19 can be managed well, were positively associated variables, while only the sum-score of fear was positively associated with CB-EFS-5 (I wish I could change my worries and feelings). Many participants of African origin hoped for a miracle, and this hope was positively associated with fear, and negatively associated with their perception of COVID-19 as a global disaster.
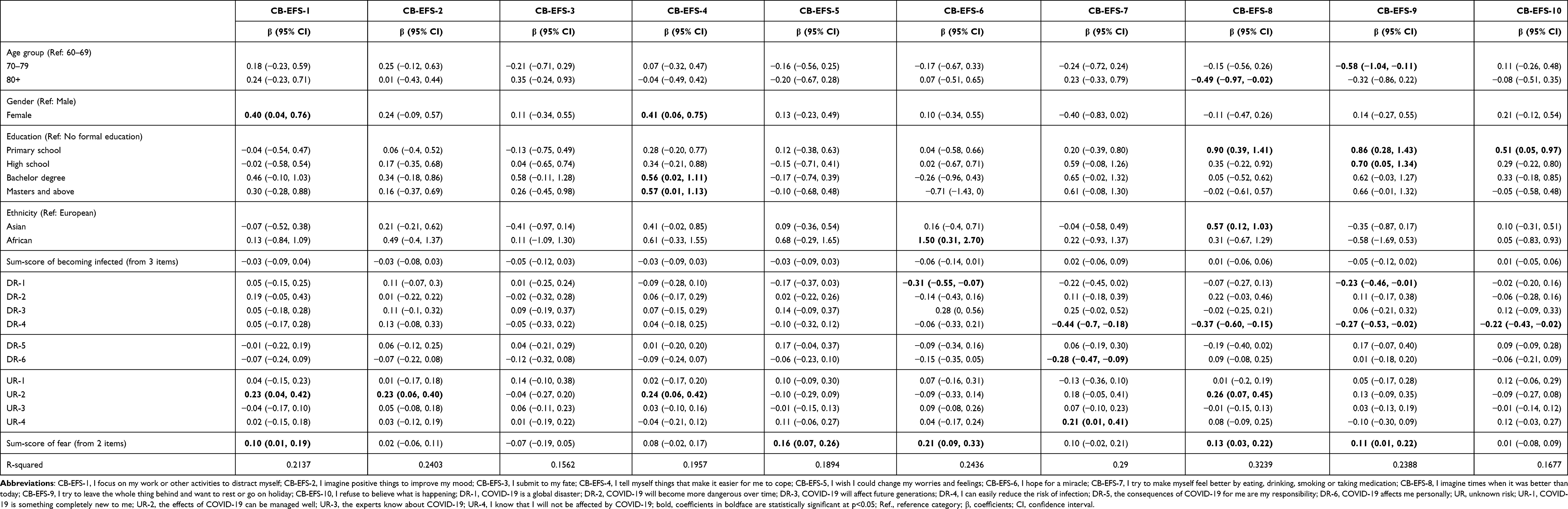 |
Table 3 Multiple Linear Regression Models Explaining the Emotion-Focused Precautions (n=155) |
The participants were trying to make themselves feel better by eating, drinking, smoking, or taking medications, which was positively associated with their perception that they will not be affected by COVID-19). For the item, “I imagine times when it was better than today”, positively associated variables were: education [for primary education (versus no formal education)], ethnicity [for Asian (versus European)], and fear. Their expectations to leave the whole thing behind and want to rest or go on holiday were positively influenced by education and sum-score of fear, while their being aged 70–79 years and perceived the COVID-19 as a global disaster and self-confidence had negative influence. Education had influence on their refusal to believe what is happening, while self-confidence in reducing the risk was negatively associated.
Table 4 presents the associations between explanatory variables and sum-scores of problems- and emotion-focused precautions. Only age group is negatively associated with sum-score of problem-focused precautions; compared to respondents aged 60–69 years, those aged 80+ years were significantly associated with decrease in sum-score of problem-focused precautions. Asian ethnicity (versus non-English speaking European), self-confidence in reducing the risks, perceiving COVID-19 could affect them personally, and fear were positively associated with sum-score of problem-focused precautions. Whereas, education (primary and bachelor versus no formal education; Primary schooling, Bachelor degree, and sum-score of fear were positively associated with their emotional precautions, and only “self-confidence in reducing the risks” was negatively associated with their emotional precautions.
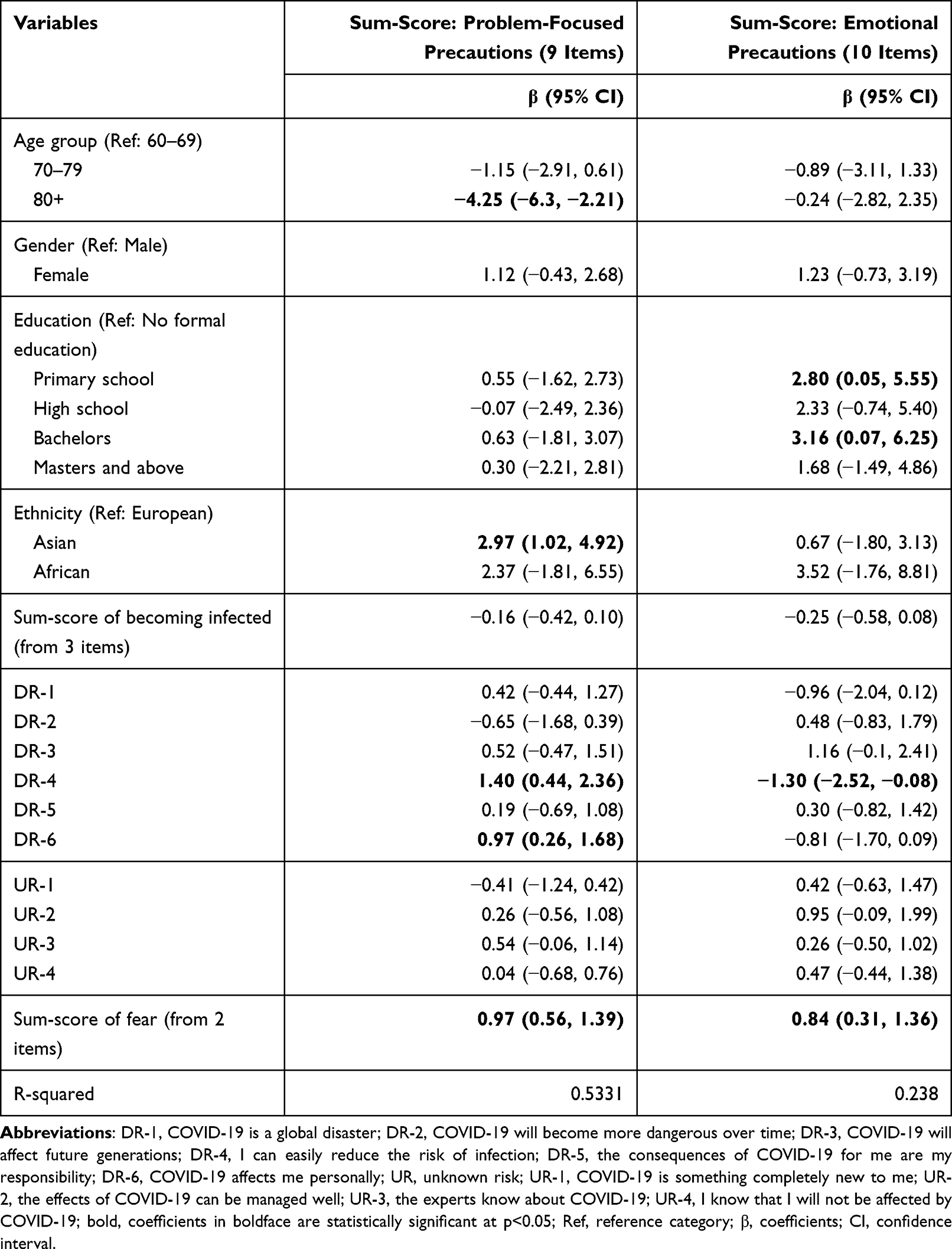 |
Table 4 Multiple Linear Regression Models Explaining the Sum-Scores of Problem-Focused and Emotion-Focused Precautions (n=155) |
Discussion and Implications
The effects of the pandemic and associated health and quarantine protocols are four-fold in South Australia: fear of infection due to global and national circumstances; access and utilization of health and social services; livelihood (economy-work) crisis; and stress and isolation.47–49 These effects of pandemic shape the perceptions and perspectives of people globally about ongoing and impending consequences, including the older CALD adults living in high-income countries like USA, UK, Europe and Australia.25,28,31,42 COVID-19 has caused considerable psychological and emotional burdens among the older CALD adults because of their lack of health education [16% with no formal education, and this proportion went up to 46.4% when primary schooling was added] and isolation due to old age. The risks for these older adults were identified in their cognitive, emotional, and social domains. These local effects, however, are set in a global context. The results have relevant consequences globally since the various critical situations associated with COVID-19 that impact people’s lives have been observed across jurisdictions and nations across the world. This includes spatial and temporal contexts in which vulnerability to the COVID-19 globally intersects with older CALD people’s personal and social spheres. These global issues include phenomena such as ageism, racism, and media influence, alongside levels of health literacy, health status and service access equity.
The study participants did not perceive a high probability of becoming infected, but they had fear for the imminent effects of COVID-19 across these personal and social spheres due to national and global circumstances. In South Australia, the fear can be related with the older CALD adults’ physical health conditions, psychological morbidity, and exposure to national and global news.49 The older adults in CALD communities are more likely to have chronic diseases and comorbidities in Australia;16,17 consistent with global health data where especially older, non-white adults in Anglophone countries have poorer health status.50,51 According to ABS (2021), 24% of people living alone are older Australians and, of those, about three-quarters are women.52 Having a high prevalence of chronic conditions, including depression and anxiety, together with living alone influence their psychological and emotional well-being, especially for those older CALD adults who are aged 80 years and over, and without education. In addition, studies show that older adults are obligated to listen to fearful messages from daily bulletin or newspapers about COVID-19 infections, respiratory problems, ventilation, bronchopulmonary allergic reactions, and deaths.48,53 The fear has been growing and may not disappear with the vaccination and virus control measures.49
High levels of fear demonstrated in this study suggest that older CALD adults are living in an environment of stress and anxiety during the pandemic. Theoretically, when people are worried and scared, they generally process and review information by either systematic or heuristic processes.54,55 According to Heuristic-Systematic Model, in order to form a judgment or make an informed plan, people engage themselves in systematic processing of any available news or information, or adopt heuristic processing that involves using learnings from their experiences.54 Many participants in this study found the COVID-19 as something new and this, followed by a recent devastating bushfire across Australia, placed older CALD adults at risk of psychological disorders. The reporting of global and national crises and of quarantine protocols by the government and the media has been contextualised from “emotional” rather than “rational” perspectives. Consequently, recipients of the reports perceive a risk of being affected by the pandemic, resulting in fear that triggers stress and anxiety. The findings of this study are consistent with earlier studies, which found that the fear that people experienced during the pandemic affects their perceptions of risk and the older CALD people may be prone to perceive a greater risk on the basis of a sense of uncertainty, vulnerability, and lack of control,9,10 or fear of unknown.6 It provides important understanding of the compounding nature of intersecting vulnerabilities, such as age, gender or culture, in the context of COVID-19, and contributes to global perspectives on the psychosocial impact of COVID-19 where there may also be social vulnerability,56 humanitarian crisis,57 or extreme weather events.58
Problem-focused precautions were apparent in the study participants, although many of them did not confirm in accessing online health information, consulting with health professionals, and relying on learnings from previous virus infection experience. Results reflect the conclusions of Bish and Michie (2020) in their review of the demographic variables.59 With no gender difference in risk perceptions, age and education seemed to influence the participants’ risk perceptions and problem-focused precautions. For example, understanding of COVID-19 effects at personal level, reliance on experts, listening and following expert advice, and search for online health information varied based on the age groups and levels of education. It is noted that oldest aged CALD people (80 years old and above) are not in the best position to access online health information, and that a lack of education could not protect them from irrational beliefs about the pandemic. A lack of access to health information from experts, websites, and health professionals was common, which could be attributed to their lack of education and associated inability to search health information online, reliance on family and friends for information rather than on experts, and a communication gap between the older CALD adults and the public health information dissemination system. The literature supports the difficulty in disseminating information about COVID-19 to the cultural and linguistically diverse communities.60 Therefore, it may be concluded that more education and accessible health information about the pandemic are associated with a decreased concern of being affected and a higher probability to taking problem-focused precautions.
Emotional precautions have received less attention in studies that have investigated the effects of COVID 19. In this study the mean sum-score of emotion-focused coping (on a scale of 10 items) during the pandemic was neither positive nor negative, which is dissimilar to the Fuller and Huseth-Zosel’s (2021) study that reported that mean perceived emotional coping level of older adults was 7.9 (on a scale 1–10),9 where 87% rated their coping positively. Older CALD adults were in a state of emotional vulnerability in South Australia at the time of the survey and were not adequately trying to make themselves feel better by eating, drinking, smoking or taking medications, but living the emotional effects of pandemic as in other countries.50 They are exposed to anxiety, frustration, confusion, uncertainty, and inadequacy that may provoke destructive consequences during or post-pandemic situations, for example, suicides and aggression.39,40 Flesia et al (2020) and Charter (2020) revealed that the unpredictability and uncontrollability of the COVID-19 lockdown had an impact on emotional wellbeing.39,41
Gender, education, self-confidence, and fear were significant factors that influenced the participants’ emotional precautions. Female older CALD adults reported taking a higher level of emotional precaution than males in terms of distractions and self-talk. Further, those with higher levels of education showed greater confidence and efforts to think positively about things or to cope more readily than the people with no formal education. As in other studies, fear was the most commonly cited factor in relation to emotional precaution.47,48,61,62 Living in a multicultural country during the pandemic is a challenge, especially for the oldest group and females, who mostly rely on their family members and own community people for emotional care. Most people from CALD communities have lower socio-economic profile than the native Australia-born populations, with a lack of education, income, independence, and access to services.60 There is a dilemma for someone who lives in such a poor socio-economic condition, especially in the older CALD adults about staying busy, seeking social support, and having a positive mindset that are important elements for lowering fear.23 Minahan et al (2021) identified avoidance as the strongest influence in response to perceived risk;42 therefore, emotional precaution is an important aspect to be considered in developing pandemic response plan for older CALD adults.
How government and public health initiatives support the older CALD communities in South Australia is potentially an exemplar in effective management of COVID-19 cross-infection, as well as in managing public health socio-economic development in pandemic. COVID-19 is now a controlled notifiable condition under the South Australian Public Health Act 2011. Due to uncertainty about the effectiveness of containment measures, COVID-19 remains a global and national catastrophe that continues to disturb South Australians’ everyday lives including older adults. From this study it is apparent that government measures and global circumstances extends to influence older CALD South Australians’ risk perceptions and problem- and emotion-focused precautions. Future research in this field should target the long-term effects of these life-changing disturbances and perturbations on the mental health and wellbeing of this vulnerable population. The findings of such investigations may inform the development of interventions to limit the impact of the COVID-19 pandemic, as well as other local or global disasters.
This study has several limitations. Firstly, as it is a cross-sectional study, causal inferences about the relationship between socio-demographic characteristics and risk perceptions and problem- and emotion-focused coping behaviours cannot be assumed. Secondly, the sample is small, and not representative of all CALD communities in South Australia and the findings cannot be generalised to other CALD populations, either in Australia or overseas. Thirdly, standardized measures were not used to assess levels of stress and fear. This study relied on an English-language questionnaire in data collection, which may have impacted on participation rates and on interpretation of questions in a sample for whom English was not their first language.
Conclusions
Despite the limitations, this study has generated knowledge about the association between risk perceptions and the likelihood of using problem- and emotion-focus health precautions in older CALD adults living in South Australia. Such knowledge has important implications for policy makers and public health officials in decision-making about the development of culturally and linguistically appropriate programs and materials to engage and communicate with the CALD older adults under stressful, lifestyle-threatening, if not life-threatening circumstances. This is critical for any vulnerable community, locally or globally, in context of COVID-19 where compounding vulnerabilities or disaster may also exist. Under the circumstances of the COVID-19 pandemic, it is arguable that CALD populations have been somewhat overlooked in the provision of information that can help individuals make reliable decisions about their protective health behaviour. Failure to engage effectively with the CALD community not only places individual members of that community at risk, but also places the entire CALD community at risk because of misunderstanding and non-compliance. It is imperative to put in place strategies that address the specific needs of all sections of the community and to provide advice in a context, format and language that is readily understood.
Data Sharing Statement
Data supporting the results can be obtained from the corresponding author upon reasonable request.
Ethics Approval
The study received ethics approval from Flinders University Human Research Ethics Committee, Australia [Project Number: HEL2215].
Consent to Participate
Participation consent was implied, by completing the survey.
Acknowledgments
We are thankful to the participants who provided time and shared their experiences about the COVID-19. We acknowledge the contribution of CALD community organisations which helped the researchers in distributing the survey questionnaire and encouraging people to participate. We thank Judy Baily, Research Assistant at Flinders University Rural Health SA for her valuable support in participants’ recruitment and data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The author(s) disclosed receipt of the following research grant for this project: Research was financed by the Flinders University Internal College COVID Grant [Grant Number: 01.455.10977 - 2020].
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Desborough J, Hall Dykgraaf S, de Toca L, et al. Australia’s national COVID −19 primary care response. Med J Aust. 2020;213(3):104–106. doi:10.5694/mja2.50693
2. Varghese C, Xu W. Quantifying what could have been–the impact of the Australian and New Zealand governments’ response to COVID-19. Infection, Disease & Health. 2020;25(4):242–244.
3. Chan DK, Mclaws ML, Forsyth DR. COVID-19 in aged care homes: a comparison of effects initial government policies had in the UK (primarily focussing on England) and Australia during the first wave. Int J Quality Health Care. 2021;33(1):mzab033.
4. Wang J, Fu Y, Lou V, Tan SY, Chui E. A systematic review of factors influencing attitudes towards and intention to use the long-distance caregiving technologies for older adults. Int J Med Inform. 2021;153:104536.
5. Siette J, Seaman K, Dodds L, et al. A national survey on COVID-19 second-wave lockdowns on older adults’ mental wellbeing, health-seeking behaviours and social outcomes across Australia. BMC Geriatr. 2021;21(1):1–6.
6. Lothian A. The COVID-19 pandemic in South Australia: a survey of RGSSA members. South Australian Geographical J. 2020;116(1):14–24.
7. Shakespeare-Finch J, Bowen-Salter H, Cashin M, et al. COVID-19: an Australian perspective. J Loss Trauma. 2020;25(8):662–672.
8. Bisht IP, Bisht RK, Sagar P. Effect of gender and age in fear and stress due to COVID-19. J Hum Behav Soc Environ. 2021;31(1–4):70–76.
9. Fuller HR, Huseth-Zosel A. Lessons in resilience: initial coping among older adults during the COVID-19 pandemic. Gerontologist. 2021;61(1):114–125.
10. Rutherford BR, Choi CJ, Chrisanthopolous M, et al. The COVID-19 pandemic as a traumatic stressor: mental health responses of older adults with chronic PTSD. Am J Geriatric Psychiatry. 2021;29(2):105–114.
11. Mariani R, Renzi A, Di Monte C, Petrovska E, Di Trani M. The impact of the COVID-19 pandemic on primary emotional systems and emotional regulation. Int J Environ Res Public Health. 2021;18(11):5742.
12. Kuo YJ, Chen YP, Wang HW, et al. Community outbreak moderates the association between COVID-19-related behaviors and COVID-19 fear among older people: a one-year longitudinal study in Taiwan. Front Med. 2021;8:756985.
13. Li YP, Lin CY, Kuo YJ, Chen YP, Griffiths MD. Gender differences in the factors associated with the fear of COVID-19 among Taiwanese older people. J Health Care Org Provision Financing. 2021;58:00469580211055587.
14. Pakpour AH, Liu CH, Hou WL, et al. Comparing fear of COVID-19 and preventive COVID-19 infection behaviors between Iranian and Taiwanese older people: early reaction may be a key. Front Public Health. 2021;9:740333.
15. Ahorsu DK, Lin CY, Pakpour AH. The association between health status and insomnia, mental health, and preventive behaviors: the mediating role of fear of COVID-19. Gerontol Geriatric Med. 2020;6:2333721420966081.
16. AIHW. culturally and linguistically diverse populations. Australian Institute of Health and Welfare. 2018: https://www.aihw.gov.au/getmedia/f3ba8e92-afb3-46d6-b64c-ebfc9c1f945d/aihw-aus-221-chapter-5-3.pdf.aspx.
17. AIWH. Australia’s Health – 2018: culturally and linguistically diverse populations. Australian Institute of Health and Welfare. 2018: https://www.aihw.gov.au/getmedia/f3ba8e92-afb3-46d6-b64c-ebfc9c1f945d/aihw-aus-221-chapter-5-3.pdf.aspx.
18. Pham TT, Berecki-Gisolf J, Clapperton A, O’Brien KS, Liu S, Gibson K. Definitions of culturally and linguistically diverse (CALD): a literature review of epidemiological research in Australia. Int J Environ Res Public Health. 2021;18(2):737.
19. Walker R, Belperio I, Gordon S, Hutchinson C, Rillotta F. Caring for a family member with intellectual disability into old age: applying the sociocultural stress and coping model to Italian and Greek migrants in Australia. J Appl Res Intellectual Disabilities. 2020;33(5):887–897.
20. Fountain L, Tofa M, Haynes K, Taylor MR, Ferguson SJ. Older adults in disaster and emergency management: what are the priority research areas in Australia? Int J Disaster Risk Reduction. 2019;39:101248.
21. Van Gaans D, Dent E. Issues of accessibility to health services by older Australians: a review. Public Health Rev. 2018;39(1):1–6.
22. Scherbov S, Sanderson WC. New approaches to the conceptualization and measurement of age and ageing. Dev Demographic Forecasting. 2020;243:1–261.
23. Lazarus RS, Folkman S. Stress, Appraisal, and Coping. Springer Publishing Company; 1984.
24. Lazarus RS. Theory-based stress measurement. Psychol Inq. 1990;1(1):3–13.
25. Lanciano T, Graziano G, Curci A, Costadura S, Monaco A. Risk perceptions and psychological effects during the Italian COVID-19 emergency. Front Psychol. 2020;11:2434.
26. Yıldırım M, Güler A. Positivity explains how COVID-19 perceived risk increases death distress and reduces happiness. Pers Individ Dif. 2021;168:110347.
27. Baker AE, Procter NG, Ferguson MS. Engaging with culturally and linguistically diverse communities to reduce the impact of depression and anxiety: a narrative review. Health Soc Care Community. 2016;24(4):386–398.
28. Rojas-Lizana S, Cordella M. Ageing in a foreign land: stressors and coping strategies in the discourse of older adult Spanish speakers in Australia. J Transient Migration. 2020;4(1):5–23.
29. Principe I. Issues in Health Care in South Australia for People from Culturally and Linguistically Diverse Backgrounds: A Scoping Study for the Health Performance Council. Government of South Australia, Health Performance Council; 2015.
30. Martin S. Bushfire Crisis: More Than Half of All Australians Found to Have Been Directly Affected. The Guardian Labs; 2020.
31. Gerhold L. COVID-19: Risk Perception and Coping Strategies - Results from a Survey in Germany 2020. Freie Universitat Berlin; 2020; doi:10.31234/osf.io/xmpk4
32. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920.
33. Cori L, Bianchi F, Cadum E, Anthonj C. Risk perception and COVID-19. Int J Environ Res Public Health. 2020;17(9):3114.
34. Lohiniva AL, Sane J, Sibenberg K, Puumalainen T, Salminen M. Understanding coronavirus disease (COVID-19) risk perceptions among the public to enhance risk communication efforts: a practical approach for outbreaks, Finland, February 2020. Eurosurveillance. 2020;25(13):2000317.
35. Dryhurst S, Schneider CR, Kerr J, et al. Risk perceptions of COVID-19 around the world. J Risk Res. 2020;23(7–8):994–1006.
36. Kwok KO, Li KK, Chan HH, et al. Community responses during early phase of COVID-19 epidemic, Hong Kong. Emerg Infect Dis. 2020;26(7):1575.
37. De Bruin WB, Bennett D. Relationships between initial COVID-19 risk perceptions and protective health behaviors: a national survey. Am J Prev Med. 2020;59(2):157–167.
38. Aldwin CM. Stress, Coping, and Development: An Integrative Perspective. Guilford Press; 2007.
39. Chater N. Facing up to the uncertainties of COVID-19. Nature Human Behav. 2020;4(5):439.
40. Lazzerini M, Putoto G. COVID-19 in Italy: momentous decisions and many uncertainties. Lancet Global Health. 2020;8(5):e641–2.
41. Flesia L, Monaro M, Mazza C, et al. Predicting perceived stress related to the Covid-19 outbreak through stable psychological traits and machine learning models. J Clin Med. 2020;9(10):3350.
42. Minahan J, Falzarano F, Yazdani N, Siedlecki KL. The COVID-19 pandemic and psychosocial outcomes across age through the stress and coping framework. Gerontologist. 2021;61(2):228–239.
43. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879.
44. Folkman S, Lazarus RS. Coping as a mediator of emotion. J Pers Soc Psychol. 1988;54(3):466.
45. Slovic P. Perception of risk. Science. 1987;236(4799):280–285.
46. Chan YH. Biostatistics 202: logistic regression analysis. Singapore Med J. 2004;45(4):149–153.
47. Dawes P, Siette J, Earl J, Johnco C, Wuthrich V. Challenges of the COVID‐19 pandemic for social gerontology in Australia. Australas J Ageing. 2020. doi:10.1111/ajag.12845
48. Siette J, Dodds L, Seaman K, et al. The impact of COVID‐19 on the quality of life of older adults receiving community‐based aged care. Australas J Ageing. 2021;40(1):84–89.
49. Strutt PA, Johnco CJ, Chen J, et al. Stress and coping in older Australians during COVID-19: health, service utilization, grandparenting, and technology use. Clin Gerontol. 2021;45(1):106–119.
50. Armitage R, Nellums LB. COVID-19 and the consequences of isolating the elderly. Lancet Public Health. 2020;5(5):e256.
51. Larrabee Sonderlund A, Charifson M, Schoenthaler A, Carson T, Williams NJ. Racialized economic segregation and health outcomes: a systematic review of studies that use the Index of Concentration at the Extremes for race, income, and their interaction. PLoS One. 2022;17(1):e0262962.
52. ABS. 2020. Household and Family Projections, Australia 1996 to 2021. Australian Bureau of Statistics. Cat. no. 3236.0.
53. Rahman MM, Bhattacharjee B, Farhana Z, et al. Age-related risk factors and severity of SARS-CoV-2 infection: a systematic review and meta-analysis. J Prev Med Hyg. 2021;62(2):E329.
54. Chaiken S. Heuristic versus systematic information processing and the use of source versus message cues in persuasion. J Pers Soc Psychol. 1980;39(5):752.
55. Averbeck JM, Jones A, Robertson K. Prior knowledge and health messages: an examination of affect as heuristics and information as systematic processing for fear appeals. Southern Commun J. 2011;76(1):35–54.
56. Henry FA, Wachtendorf T. Compounded social vulnerability: parole supervision and disasters. Corrections. 2020;25:1–35.
57. Harutyunyan H, Mukhaelyan A, Hertelendy AJ, et al. The psychosocial impact of compounding humanitarian crises caused by war and CoViD-19 informing future disaster response. Prehosp Disaster Med. 2021;36(5):501–502.
58. Wilhelmi OV, Howe PD, Hayden MH, O’Lenick CR. Compounding hazards and intersecting vulnerabilities: experiences and responses to extreme heat during COVID-19. Environ Res Lett. 2021;16(8):084060.
59. Bish A, Michie S. Demographic and attitudinal determinants of protective behaviours during a pandemic: a review. Br J Health Psychol. 2010;15(4):797–824.
60. Javanparast S, Naqvi SK, Mwanri L. Health service access and utilisation amongst culturally and linguistically diverse populations in regional South Australia: a qualitative study. Rural Remote Health. 2020;20(4):5694.
61. Hamiduzzaman M, Islam MR. Save life or livelihood: responses to COVID-19 among South-Asian poor communities. Local Development Soc. 2020;1(2):177–189.
62. Hamiduzzaman M, Siddiquee N and McLaren H. COVID-19 risk perceptions and precautions among the elderly: A study of CALD adults in South Australia. F1000Research. 2022;11:43. doi:10.12688/f1000research.74631.1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.