")
Back to Journals » Degenerative Neurological and Neuromuscular Disease » Volume 13
Risk of Obstructive Sleep Apnea in Saudi Male Boys with Duchenne Muscular Dystrophy (DMD)
Received 15 May 2023
Accepted for publication 8 August 2023
Published 15 August 2023 Volume 2023:13 Pages 45—53
DOI https://doi.org/10.2147/DNND.S421399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Thomas Müller
Ahmed Bamaga,1 Lama Alqarni2
1Neuromuscular Medicine Unit, Department of Pediatrics, Faculty of Medicine, King Abdulaziz Univeristy and Hospital, Jeddah, Saudi Arabia; 2Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Ahmed Bamaga, FRCPC, Associate Professor of Pediatric Neurology, Department of Pediatrics, Faculty of Medicine, King Abdulaziz University, P.O. Box 80216, Jeddah, 2158, Saudi Arabia, Email [email protected]
Background: Duchenne muscular dystrophy (DMD) patients are at a high risk of developing sleep-related breathing disorders (SRBD) such as obstructive sleep apnea (OSA). This study aimed to determine the risk of developing OSA among DMD patients.
Methods: This cross-sectional study was conducted from February 2022 to July 2022 in a tertiary healthcare facility. As a screening tool for OSA, we used the Pediatric Sleep Questionnaire (PSQ).
Results: Subjects included 60 boys with DMD, mean age 10.15 ± 3.54 years. The mean BMI for all subjects was 18.9 ± 4.08 kg/m2. Of these, 22 (36.7%) children were at high risk of OSA. Children who were overweight, and on steroids tended to be at higher risk of developing OSA (P < 0.043) and (P < 0.029) respectively.
Conclusion: Our study shows a significant risk of OSA in DMD patients. Therefore, Sleep studies should be part of the standard of care for DMD patients.
Keywords: Duchenne muscular dystrophy, obstructive sleep apnea, pediatric sleep questionnaire, Saudi Arabia
Introduction
Duchenne muscular dystrophy (DMD) is the most prevalent hereditary neuromuscular disease affecting approximately 1 in 3600–6000 male newborns.1–3 DMD is an X-linked disorder that affects boys while girls are carriers.1 The disease-causing mutation in the dystrophin gene leads to decreased or absent dystrophin, a 427-kDa cytoskeletal protein essential for developing and maintaining muscle tissue, which results in impaired muscle function, decreased physical ability, inability to walk, respiratory system impairment, a wide range of comorbidities, and shortened life expectancy.4–7 Patients with DMD have higher rates of learning difficulties (26%), intellectual disabilities (17–27%), attention deficit hyperactivity disorder (32%), and autistic spectrum disorder (15%). They are more prone to experience anxiety and depression.8 Also, they are at high risk of developing sleep-related breathing disorders, including obstructive sleep apnea (OSA) and sleep-related hypoventilation. Snoring, morning headaches, and lethargy are some of the clinical signs of OSA found in DMD patients.6
OSA is a condition in which the soft tissues at the back of the throat become relaxed and collapse partially or completely during sleep, causing a blockage in the airway and hindering breathing. The person affected by OSA struggles to breathe, leading to episodes of apnea. When the patient attempts to maintain breathing and overcome the obstruction caused by a decrease in blood oxygenation, arousal with snorts or gasps can occur.9–11 Children with OSA experience symptoms during both the day and night, including snoring, restless sleep, mouth breathing, apneas, gasping, laborious or paradoxical breathing, and hyperextension of the neck while sleeping. Common daytime symptoms include difficulty concentrating, behavioral and emotional issues, morning headaches, excessive daytime sleepiness (EDS), and failure to thrive.12 OSA is more prevalent among males than females, with higher occurrence noted in African Americans and obese children.13 Children with adenoid and/or tonsil hypertrophy, allergic rhinitis, and craniofacial abnormalities are at higher risk of developing OSA.14 It is estimated that between 1% to 4% of children suffer from OSAS, but in high-risk populations, such as obese children, the incidence can be as high as 36.6%.15 In Saudi Arabia, approximately 21% of children are diagnosed with sleep-breathing disorders.16
A study conducted in Brazil with a sample size of 44 DMD patients found that the DMD group had a higher overall number of apneas compared to the control group, particularly obstructive apneas.6 Similarly, a cross-sectional study published in Switzerland in 2012 reported that 15.6% of the 64 surveyed patients with DMD had sleep-related breathing disorders.17 In 2020, a case-control study involving 12 DMD patients and 8 control patients revealed that 58% of DMD patients showed at least one symptom, such as snoring, observed apnea, or difficulty sleeping.18 Additionally, a study in 2012 showed that 16.6% of 12 patients with DMD had OSA.19 Despite numerous studies on the prevalence of OSA in DMD patients, limited research has been conducted in Saudi Arabia. Consequently, this study aims to evaluate the risk of OSA among DMD patients at King Abdulaziz University Hospital (KAUH) in city of Jeddah in western region of Saudi Arabia.
Methodology
Study Design and Study Population
This cross-sectional study was conducted between February 2022 and July 2022 at KAUH in Jeddah, Saudi Arabia. The study involved a review of the medical records of 64 participants who met the inclusion criteria, which required them to be diagnosed with DMD at KAUH and aged between 2–18 years. Asthmatic patients and children with other chronic respiratory diseases were excluded from the study.
Ethical Approval
The study was approved by the National Biomedical Ethics Committee at King Abdulaziz University (Ref.91–22). To ensure ethical standards were maintained, all parents were contacted via phone and provided with an information note outlining the study’s objectives. The information notes also acted as a consent form for participation in the study, and all parents provided their agreement to participate. As the study was based on an interview-based questionnaire, the consent form was crucial to ensure that the participants were aware of their rights and what their involvement would entail. The study involving human participants was in accordance with the ethical standards of the institutional research committee and with the Helsinki Declaration and its later amendments or comparable ethical standards.
The Questionnaire and the Translation
The questionnaire used in this study was divided into two sections. The first section was designed to collect demographic information from each patient such as age, gender, nationality, and detailed history of DMD, including ambulant or non-ambulant status, steroid use, and consanguineous marriage of the parents. The second section assessed OSA using an Arabic version of the Pediatric Sleep Questionnaire (PSQ), a reliable and valid screening tool for detecting OSAS (Figure 1). The PSQ was directed to parents and contained 22 questions grouped into three domains: snoring, sleepiness, and behavioral, consisting of 9, 7, and 6 items, respectively. The response options were “yes”, “no”, and “I do not know”, with “yes” given a score of 1, “no” a score of 0, and “do not know” scored as missing. Scores of 33% or higher indicated an increased risk of sleep-disordered breathing (SDB), while scores lower than 33% indicated low risk.20
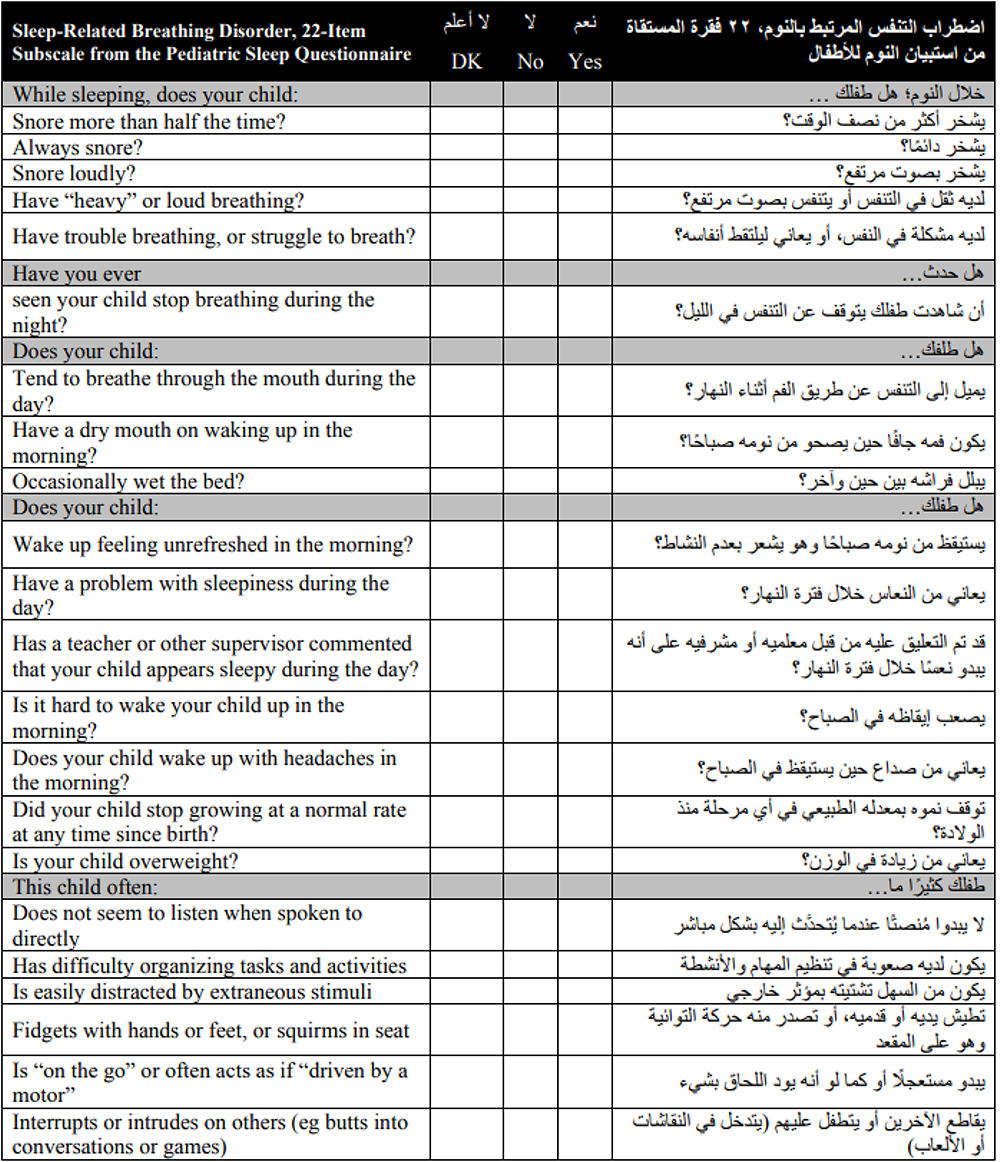 |
Figure 1 Pediatric Sleep Questionnaire (PSQ) in English and Arabic versions. Notes: Translated with permission from the U-M Pediatric Sleep Questionnaire (PSQ). Copyright 2007 The Regents of the University of Michigan.21 |
To ensure the questionnaire was appropriate for use in this study, permission to use and translate the PSQ into Arabic was obtained from the first author, RD Chervin, and the University of Michigan, USA. The questionnaire was translated from English to Arabic using a forward/backward translation method, as recommended by the World Health Organization (WHO).
Statistical Analysis
SPSS (Statistical packaging social science) version 26 was used for data analysis. Categorical variables, such as primary variables, were described using frequencies, whereas continuous variables with regularly distributed values were described using means and standard deviations. Odds ratios, confidence intervals (95%) of odds ratios, and p-values were generated for the side effects using a binary logistic regression test for categorical data to find every potential risk factor. Statistical significance was set at p < 0.05.
Results
The study enrolled 64 patients, of whom four did not meet the inclusion criteria, leaving a final sample of 60 participants. The mean age of the sample was 10.15 ± 3.54 years (range 4–18), with 56 (93.3%) being of Saudi nationality. The sample was divided into three age categories for subsequent analysis: Preschool (4–6 years), nine children (15%), school (7–12 years), 39 children (65%), and adolescence (13–18 years), 12 children (20%).
The mean body mass index (BMI) and BMI percentile for all subjects were 18.9 ± 4.08 kg/m2 and 63.7 ± 34.08 kg/m2, respectively, while the mean BMI z-score was 0.38 ± 1.55. To evaluate the physical disability, ambulatory status was used, and 19 (31%) participants were wheelchair dependent. Steroid use was reported in 28 (46.7%) patients, and 23 (38.3%) were born to consanguineous parents. Additional sample characteristics are presented in (Table 1).
 |
Table 1 Participant’s Characteristics Overall and According to the Risk of OSA |
In the PSQ, 22 out of the 60 participants (36.7%) scored 8 or higher and were considered positive for OSAS. Among the symptoms evaluated by the questionnaire, 17 participants (28.3%) snored more than half of the time while sleeping, 7 (11.7%) snored most days, 15 (25%) breathed through their mouths, and 3 (5%) had sleep apnea. However, the most prominent symptoms reported were difficulty organizing tasks and activities, being “on the go”, or often acting as if driven by a motor (55%), feeling unrefreshed upon waking, and being easily distracted by extraneous activities (51.7%) (Figure 2).
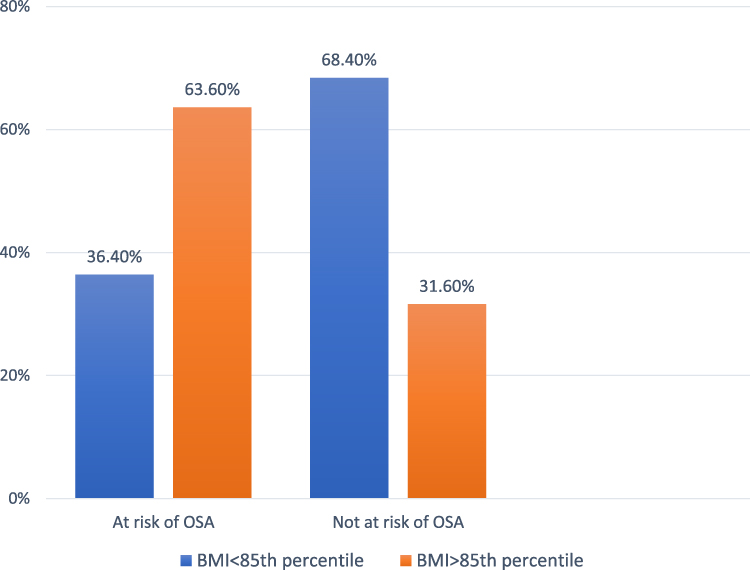 |
Figure 2 Weight status category of patients with or without OSA. Abbreviation: BMI, body mass index. |
According to binary logistic regression analysis, patients who were on steroids had a higher risk of developing OSA (OR: 3.92; 95% CI 1.15–13.34; p<0.05), while participants with a BMI above the 85th percentile were also at a higher risk of developing OSA (OR: 3.54; 95% CI 1.03–12.05; p<0.05) (Table 2). In contrast, the average PSQ score was not related to age categories (p=0.840) (Figure 3).
 |
Figure 3 Age category of patients with or without OSA. |
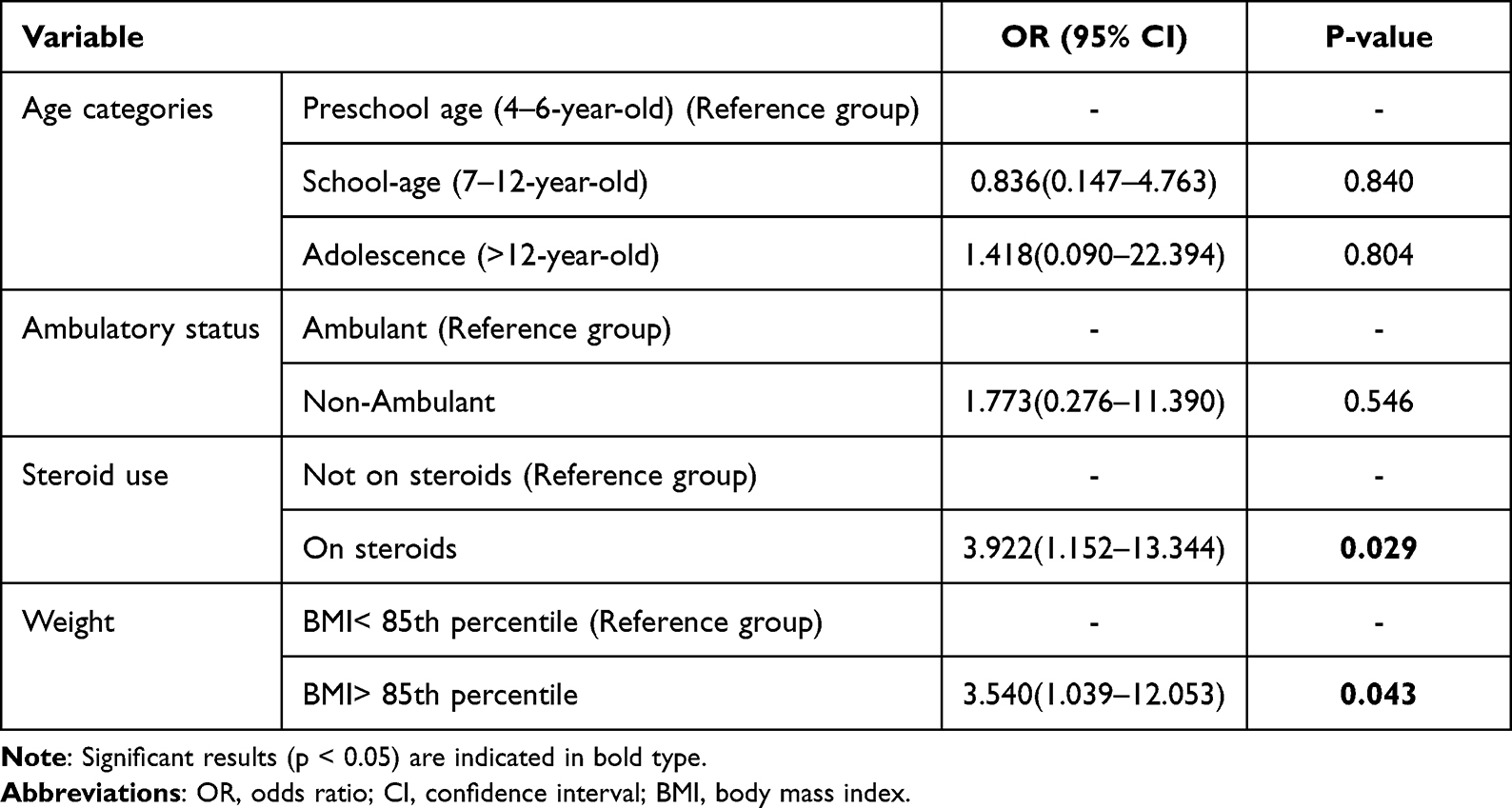 |
Table 2 Logistic Regression with Odds Ratios, Confidence Intervals, and p-values for the Associations Between OSA and Different Predictors |
Discussion
Sleep-related breathing disorders can have a significant impact on the health and well-being of individuals with neuromuscular diseases, including DMD. These disorders can lead to poor quality sleep, decreased cognitive function, and cardiovascular problems. Furthermore, individuals with neuromuscular diseases like DMD are at a higher risk of developing sleep apnea due to the weakening of respiratory muscles. Therefore, early detection and management of sleep-related breathing disorders are crucial for improving outcomes in DMD patients. Studies has shown that up to 80% of people with neuromuscular diseases have issues with pulmonary gas exchange and sleep architecture,22,23 with OSA and other breathing abnormalities commonly reported in DMD patients.6 Our current study aimed to investigate the risk of OSA and associated risk factors in boys with DMD, highlighting the potential for poor sleep quality in this population.
In our study, we found that 36.7% of the children with DMD were at a high risk of developing OSA, which is consistent with the findings of previous studies. For instance, a study conducted in Brazil reported an OSA prevalence of 18% among 44 children diagnosed with DMD. Another study found that sleep disturbances were experienced by 62.5% of DMD patients. These results highlight the need for early screening and management of sleep-related breathing disorders in DMD patients.6,24,25 Differences in study populations, selection criteria, assessment tools, and age ranges may account for the varying prevalence rates reported in different studies.
Our study also found that overweight children, especially those above the 85th percentile, had a higher risk of OSA, with 63.3% of such children identified as high risk for the condition. Of these children, 11 were taking steroids. These results are similar to those of a US-based study, which found that the group of DMD patients with OSA was significantly more overweight than their peers.26,27 Additionally, our study discovered that 68.2% of the high-risk children were taking steroids, a therapy that can promote weight gain and, in turn, OSA. However, while steroids can impact sleep and behavior, they could also improve sleep, health, and well-being throughout the day.28 Due to incomplete or missing data on steroid use and other risk factors such as adenoid and tonsillar hypertrophy, we did not evaluate the patients’ level of steroid exposure using hospital medical records.
In individuals with DMD, lung capacity reduction and ventilation heterogeneity are associated with age-related decline.29 Our study found that the risk of developing OSAS was highest in children aged 7–12 years (59.1%), consistent with a similar study with a mean age of 9.9 ± 2.7 years.26 Conversely, preschool children had the lowest incidence of OSA in our study (13.6%), possibly due to their younger age, less severe disease, and healthier BMI, as well as their functional ambulation status.
Habitual snoring was reported by 28.3% of children in our sample, and 5% reported sleep apnea. In another study, DMD patients reported an 18% prevalence of habitual snoring.26 Meanwhile, 25% of our sample exhibited daytime mouth breathing. A study in Australia demonstrated that daytime respiratory performance could predict sleep-related hypoventilation in individuals with DMD, potentially playing a role in respiratory failure’s pathophysiology.29 Our study revealed that 40.9% of the patients were non-ambulant, which is a warning sign for respiratory failure.30 However, being ambulatory does not guarantee better pulmonary function, as demonstrated by Ekici et al.30 Moreover, ambulatory patients tend to have longer apnea-hypopnea duration than non-ambulatory patients.19 Hence, children with DMD should undergo pulmonary function testing by a pediatric respiratory physician as early as 4–6 years of age, before being confined to a wheelchair.31
Attention deficit hyperactivity disorder (ADHD) is four times more prevalent in DMD children than in typically developing children.32–34 However, children with SDB, including OSA, may exhibit hyperactive behavior during the day due to lack of sleep, leading to a misdiagnosis of ADHD.35 Conversely, children with ADHD may have underlying SDB.36
Parents of children with high OSA risk reported that their child is easily distracted, has trouble planning activities and tasks, and does not listen when spoken to directly. These symptoms are consistent with SDB, and were reported by 72.7%, 81.8%, and 59.1% of parents, respectively.37,38 The prevalence of bedwetting was also higher (36.4%) in the high-risk group, consistent with previous studies.38,39 In contrast, a lower percentage of parents in the low-risk group reported these symptoms (41.7% and 55%).
Although the symptoms of ADHD and pediatric OSA are similar, the PSQ score is determined more by non-specific symptoms than particular symptoms. However, Patients should be investigated for ADHD before obtaining the PSQ to minimize unnecessary screening for false-positive findings.40
The study has both strengths and limitations. One of the strengths is the use of an internationally validated questionnaire, which has good sensitivity and specificity in assessing children’s sleep patterns over the past month, reducing reporting bias. Additionally, the sample size of DMD patients on steroids is considered significant given the low prevalence of the disease. The study findings suggest a link between steroid use and respiratory disorders associated with weight gain.
However, the study also has limitations. Due to the cross-sectional design, the study lacks long-term follow-up information on the progression of OSA in DMD patients. Other factors such as strength and function, and scoliosis, were not evaluated. Lastly, the dose and duration of steroid exposure were not considered. Therefore, further longitudinal investigations and follow-up for OSA problems in young DMD patients are recommended.
Conclusion
Our study showed a high risk of OSA among DMD patients, with 36.7% of the sample at increased risk of SDB. This study highlights the importance of early diagnosis and treatment of sleep-related breathing disorders in DMD patients to improve their quality of life and prevent complications. Further studies are recommended to determine the effectiveness of interventions aimed at managing OSA in DMD patients.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, [AB].
Author Contributions
A Bamaga, and LA made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, or publication of this article.
Disclosure
The authors have no conflict of interest to report.
References
1. Bello L, Pegoraro E. The “usual suspects”: genes for inflammation, fibrosis, regeneration, and muscle strength modify Duchenne muscular dystrophy. J Clin Med. 2019;8(5):649. doi:10.3390/jcm8050649
2. Emery AE. Population frequencies of inherited neuromuscular diseases—a world survey. Neuromuscular Disorders. 1991;1(1):19–29. doi:10.1016/0960-8966(91)90039-U
3. Bradley D, Parsons E. Newborn screening for Duchenne muscular dystrophy. Semin Neonatol. 1998;3(1):27–34. doi:10.1016/S1084-2756(98)80146-2
4. Blake DJ, Weir A, Newey SE, Davies KE. Function and genetics of dystrophin and dystrophin-related proteins in muscle. Physiol Rev. 2002;82(2):291–329. doi:10.1152/physrev.00028.2001
5. Barbe F, Quera-Salva MA, McCann C, et al. Sleep-related respiratory disturbances in patients with Duchenne muscular dystrophy. Eur Respir J. 1994;7(8):1403–1408. doi:10.1183/09031936.94.07081403
6. Nozoe KT, Moreira GA, Tolino JR, Pradella-Hallinan M, Tufik S, Andersen ML. The sleep characteristics in symptomatic patients with Duchenne muscular dystrophy. Sleep Breath. 2015;19(3):1051–1056. doi:10.1007/s11325-014-1103-9
7. Bushby K, Finkel R, Birnkrant DJ, et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol. 2010;9(1):77–93. doi:10.1016/S1474-4422(09)70271-6
8. Birnkrant DJ, Bushby K, Bann CM, et al. Diagnosis and management of Duchenne muscular dystrophy, part 3: primary care, emergency management, psychosocial care, and transitions of care across the lifespan. Lancet Neurol. 2018;17(5):445–455. doi:10.1016/S1474-4422(18)30026-7
9. Mansukhani MP, Wang S, Somers VK. Chemoreflex physiology and implications for sleep apnoea: insights from studies in humans. Exp Physiol. 2015;100(2):130–135. doi:10.1113/expphysiol.2014.082826
10. Gleeson KE, Zwillich CW, White DP. Chemosensitivity and the ventilatory response to airflow obstruction during sleep. J Appl Physiol. 1989;67(4):1630–1637. doi:10.1152/jappl.1989.67.4.1630
11. Stepanski E, Lamphere J, Badia P, Zorick F, Roth T. Sleep fragmentation and daytime sleepiness. Sleep. 1984;7(1):18–26. doi:10.1093/sleep/7.1.18
12. Kheirandish-Gozal L, Gozal D, editors. Sleep Disordered Breathing in Children: A Comprehensive Clinical Guide to Evaluation and Treatment. Springer; 2012.
13. Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):242–252. doi:10.1513/pats.200708-135MG
14. Gulotta G, Iannella G, Vicini C, et al. Risk factors for obstructive sleep apnea syndrome in children: state of the art. Int J Environ Res Public Health. 2019;16(18):3235. doi:10.3390/ijerph16183235
15. Bin-Hasan S, Katz S, Nugent Z, et al. Prevalence of obstructive sleep apnea among obese toddlers and preschool children. Sleep Breath. 2018;22(2):511–515. doi:10.1007/s11325-017-1576-4
16. Baidas L, Al-Jobair A, Al-Kawari H, AlShehri A, Al-Madani S, Al-Balbeesi H. Prevalence of sleep-disordered breathing and associations with orofacial symptoms among Saudi primary school children. BMC Oral Health. 2019;19(1):1–8. doi:10.1186/s12903-019-0735-3
17. Bloetzer C, Jeannet PY, Lynch B, Newman CJ. Sleep disorders in boys with Duchenne muscular dystrophy. Acta Paediatr. 2012;101(12):1265–1269. doi:10.1111/apa.12025
18. Senel GB, Arkali NB, Kilic H, et al. Obstructive sleep apnea syndrome and autonomic dysfunction in Duchenne muscular dystrophy. Sleep Breath. 2021;25(2):941–946. doi:10.1007/s11325-020-02139-5
19. Polat M, Sakinci O, Ersoy B, Sezer RG, Yilmaz H. Assessment of sleep-related breathing disorders in patients with Duchenne muscular dystrophy. J Clin Med Res. 2012;4(5):332. doi:10.4021/jocmr1075w
20. Chervin RD, Hedger K, Dillon JE, Pituch KJ. Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000;1(1):21–32. doi:10.1016/S1389-9457(99)00009-X
21. The U-M Pediatric Sleep Questionnaire (PSQ). Available from: https://mydoctor.kaiserpermanente.org/ncal/Images/Pediatric%20Sleep%20Questionnaire_tcm75-1299493.pdf.
22. Brunetti L, Rana S, Lospalluti ML, et al. Prevalence of obstructive sleep apnea syndrome in a cohort of 1207 children of southern Italy. Chest. 2001;120(6):1930–1935. doi:10.1378/chest.120.6.1930
23. Gozal D. Pulmonary manifestations of neuromuscular disease with special reference to Duchenne muscular dystrophy and spinal muscular atrophy. Pediatr Pulmonol. 2000;29(2):141–150. doi:10.1002/(SICI)1099-0496(200002)29:2<141::AID-PPUL9>3.0.CO;2-Y
24. Koken OY, Gultutan P, Gurkas E, Degerliyurt A. Sleep: how is it affected in patients with DMD and their mothers? Minerva Pediatr. 2021:06281. doi:10.23736/S2724-5276.21.06281-9
25. Suresh S, Wales P, Dakin C, Harris MA, Cooper DG. Sleep‐related breathing disorder in Duchenne muscular dystrophy: disease spectrum in the paediatric population. J Paediatr Child Health. 2005;41(9‐10):500–503. doi:10.1111/j.1440-1754.2005.00691.x
26. Sawnani H, Thampratankul L, Szczesniak RD, Fenchel MC, Simakajornboon N. Sleep disordered breathing in young boys with Duchenne muscular dystrophy. J Pediatr. 2015;166(3):640–645. doi:10.1016/j.jpeds.2014.12.006
27. Krasner AS. Glucocorticoid-induced adrenal insufficiency. JAMA. 1999;282(7):671–676. doi:10.1001/jama.282.7.671
28. Hartman AG, Terhorst L, Little N, Bendixen RM. Uncovering sleep in young males with Duchenne muscular dystrophy. Eur J Paediatr Neurol. 2020;26:20–28. doi:10.1016/j.ejpn.2020.02.012
29. Hukins CA, Hillman DR. Daytime predictors of sleep hypoventilation in Duchenne muscular dystrophy. Am J Respir Crit Care Med. 2000;161(1):166–170. doi:10.1164/ajrccm.161.1.9901057
30. Ekici B, Ergül Y, Tatlı B, et al. Being ambulatory does not secure respiratory functions of Duchenne patients. Ann Indian Acad Neurol. 2011;14(3):182. doi:10.4103/0972-2327.85889
31. Sterni LM, Collaco JM, Baker CD, et al. An official American thoracic society clinical practice guideline: pediatric chronic home invasive ventilation. Am J Respir Crit Care Med. 2016;193(8):e16–35. doi:10.1164/rccm.201602-0276ST
32. Hendriksen JG, Vles JS. Neuropsychiatric disorders in males with Duchenne muscular dystrophy: frequency rate of attention-deficit hyperactivity disorder (ADHD), autism spectrum disorder, and obsessive—compulsive disorder. J Child Neurol. 2008;23(5):477–481. doi:10.1177/0883073807309775
33. Pane M, Lombardo ME, Alfieri P, et al. Attention deficit hyperactivity disorder and cognitive function in Duchenne muscular dystrophy: phenotype-genotype correlation. J Pediatr. 2012;161(4):705–709. doi:10.1016/j.jpeds.2012.03.020
34. Conway KC, Mathews KD, Paramsothy P, et al. Neurobehavioral concerns among males with dystrophinopathy using population-based surveillance data from the muscular dystrophy surveillance, tracking, and research network. J Dev Behav Pediatr. 2015;36(6):455. doi:10.1097/DBP.0000000000000177
35. Blunden S, Lushington K, Lorenzen B, Wong J, Balendran R, Kennedy D. Symptoms of sleep breathing disorders in children are underreported by parents at general practice visits. Sleep Breath. 2003;7(4):167–176. doi:10.1007/s11325-003-0167-8
36. Owens JA. A clinical overview of sleep and attention-deficit/hyperactivity disorder in children and adolescents. J Can Acad Child Adolesc Psychiatry. 2009;18(2):92.
37. Tsukada E, Kitamura S, Enomoto M, et al. Prevalence of childhood obstructive sleep apnea syndrome and its role in daytime sleepiness. PLoS One. 2018;13(10):e0204409. doi:10.1371/journal.pone.0204409
38. Capua M, Ahmadi N, Shapiro C. Overview of obstructive sleep apnea in children: exploring the role of dentists in diagnosis and treatment. J Can Dent Assoc (Tor). 2009;75(4):285–289.
39. Kapoor P, Chowdhry A, Sengar P, Mehta A. Development, testing, and feasibility of a customized mobile application for obstructive sleep apnea (OSA) risk assessment: a hospital-based pilot study. J Oral Biol Craniofacial Res. 2022;12(1):109–115. doi:10.1016/j.jobcr.2021.11.004
40. Ferry AM, Wright AE, Ohlstein JF, Khoo K, Pine HS, Khoo K. Efficacy of a pediatric sleep questionnaire for the diagnosis of obstructive sleep apnea in children. Cureus. 2020;12(12). doi:10.7759/cureus.12244
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.