Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Risk of COPD Exacerbations Associated with Statins versus Fibrates: A New User, Active Comparison, and High-Dimensional Propensity Score Matched Cohort Study
Authors Sun SH, Chang CH, Zhan ZW, Chang WH, Chen YA, Dong YH ![]()
Received 10 June 2021
Accepted for publication 3 September 2021
Published 1 October 2021 Volume 2021:16 Pages 2721—2733
DOI https://doi.org/10.2147/COPD.S323391
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Shu-Hui Sun,1 Chia-Hsuin Chang,2– 4 Zhe-Wei Zhan,5 Wen-Hsuan Chang,5 Yu-An Chen,6 Yaa-Hui Dong5– 7
1Department of Pharmacy, Far Eastern Memorial Hospital, Banciao, New Taipei City, Taiwan; 2Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan; 3Department of Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan; 4Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taipei, Taiwan; 5Department of Pharmacy, College of Pharmaceutical Sciences, National Yang Ming Chiao Tung University, Taipei, Taiwan; 6Institute of Public Health, School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan; 7Institute of Hospital and Health Care Administration, School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
Correspondence: Yaa-Hui Dong
Department of Pharmacy, College of Pharmaceutical Sciences, National Yang Ming Chiao Tung University, 155, Sec 2, Linong Street, Taipei, 112, Taiwan
Tel +886-2-28267986
Fax +886-2-28237929
Email [email protected]
Background: Several observational studies have found that statins may materially decrease the risk of chronic obstructive pulmonary disease (COPD) exacerbations. However, most of these studies used a prevalent user, non-user comparison approach, which may lead to overestimation of the clinical benefits of statins. We aimed to explore the risk of COPD exacerbations associated with statins with a new user, active comparison approach to address potential methodological concerns. We selected fibrates, another class of lipid-lowering agents, as the reference group because no evidence suggests that fibrates have an effect on COPD exacerbations.
Methods: We identified patients with COPD who initiated statins or fibrates from a nationwide Taiwanese database. Patients were followed from cohort entry to the earliest of the following: hospitalization for COPD exacerbations, death, end of the data, or 180 days after cohort entry. Stratified Cox regression models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) of COPD exacerbations comparing statins with fibrates after variable-ratio propensity score (PS) matching and high-dimensional PS (hd-PS) matching, respectively.
Results: We identified a total of 134,909 eligible patients (110,726 initiated statins; 24,183 initiated fibrates); 1979 experienced COPD exacerbations during follow-up. The HRs were 1.10 (95% CI, 0.96 to 1.26) after PS matching and 1.08 (95% CI, 0.94 to 1.24) after hd-PS matching. The results did not differ materially by type of statins and patient characteristic and did not change with longer follow-up durations.
Conclusion: This large-scale, population-based cohort study did not show that use of statins was associated with a reduced risk of acute exacerbations in patients with COPD using state-of-the-art pharmacoepidemiologic approaches. The findings emphasize the importance of applying appropriate methodology in exploring statin effectiveness in real-world settings.
Keywords: chronic obstructive pulmonary disease, statins, acute exacerbations, cohort study, new users, active comparison, high-dimensional propensity score
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by chronic airflow limitation, systematic and pulmonary inflammation, and respiratory symptoms.1 Patients with COPD may experience 0.5 to 3.5 acute deteriorations in respiratory symptoms requiring additional treatment (ie, exacerbations) per year.2 It has been reported that patients with COPD exacerbations requiring hospitalization within one year may have a 2 to 4-fold increased risk of death compared to those without corresponding episodes.3 In addition, COPD exacerbations increase resource utilization, undermine the quality of life, and are associated with faster disease progress.4 Therefore, it is important to manage COPD exacerbations in this population.
Statins are commonly used medications in lowering blood cholesterol levels and have important roles in the primary and secondary prevention of cardiovascular diseases.5,6 However, in vitro and in vivo studies have shown that statins may have anti-inflammatory, immunomodulatory, and pleiotropic actions and may therefore confer beneficial effects in reducing COPD exacerbations.7 One meta-analysis of observational studies suggested that use of statins may materially decrease the risk of COPD exacerbations (hazard ratio [HR], 0.64; 95% confidence [CI], 0.55 to 0.75).8 However, the prospective randomized placebo-controlled trial of Simvastatin in the Prevention of COPD Exacerbations (STATCOPE) trial indicated that new use of simvastatin, one type of commonly used statins, neither lowered exacerbation rates (simvastatins versus placebo: 1.36 versus 1.61 episodes per person-year, p-value=0.54) nor delayed the time to a first exacerbation (simvastatins versus placebo: 223 versus 231 days, p-value=0.34) in patients with COPD who did not have concomitant cardiovascular disease and diabetes.9 The discordant findings have raised an argument whether the profound protective effect of statins is due to methodological challenges of existing observational studies. Specifically, most of these observational studies identified patients who have been on statin treatment for a period and selected non-users of statins as the reference group. This prevalent user, non-user comparison approach tends to yield spurious benefits given the depletion of susceptible population, immortal time bias, and incomparability between treatment groups.10−14 On the other hand, there may be heterogeneous effects across individual statins and across patients with various comorbidities because type of statins and patient characteristics were different between available observational studies and the STATCOPE trial.8,9
The present study aimed to examine the risk of COPD exacerbations associated with statins through a new user, active comparison approach, which facilitates to address the aforementioned methodological concerns.13,14 We selected fibrates, another class of lipid-lowering agents, as the reference group because no evidence suggests that fibrates have an effect on COPD exacerbations. We also examined if the effect of statins varied by individual drug and patient characteristic.
Materials and Methods
Data Source
A single-payer National Health Insurance program was implemented in Taiwan since 1995 and reached an enrollment rate of 99% by June of 2020.15 The Taiwan National Health Insurance Research Database consists of comprehensive information on demographic and enrollment records, diagnosis and procedure data from outpatient visits and hospital admissions, and pharmacy dispensing claims from outpatient visits and hospital admissions for 99% of the total Taiwanese population (approximately 23 million). All the data of patients and health-care providers are deidentified.16 The study protocol was approved by the National Yang-Ming University Research Ethics Committee. Informed consent was waived given the retrospective nature of the study and the analysis of anonymous data.
Study Population and Study Drugs
We identified patients who initiated statins or fibrates at outpatient visits between January 1, 2009 and December 31, 2014 using the World Health Organization’s Anatomical Therapeutic Chemical classification system codes (see Appendix Table 1 for list of codes). Initiation of statins or fibrates was defined as a first statin or fibrate dispensing during the study period without any prior dispensing for both study drugs in the preceding 365 days. The index date was the date of the first dispensing of either study drug. To obtain sufficient data to measure patient characteristics at baseline, we required patients having continuous enrollment within 365 days before the index date, defined as having at least one outpatient visit or hospital admission during this window. We further restricted the cohort patients to those having at least one outpatient or inpatient COPD diagnosis (International Classification of Diseases, 9th Revision, Clinical modification [ICD-9-CM] codes 491, 492, 496) within the same window. The algorithm had a sensitivity of 85.0% and a specificity of 78.4%.17
Most patients with COPD were diagnosed at 40 years old or above.1 Therefore, we excluded patients with age less than 40 years on the index date. To prevent influence from an extreme old age or potential coding errors in birth dates, we also excluded patients with age more than 100 years on the index date. Moreover, we excluded patients with missing or ambiguous information on age or sex, patients initiating both a statin and a fibrate on the index date, or patients initiating more than one statin on the index date.
Outcome and Follow-Up
Our outcome of interest was COPD exacerbations, which was defined as the first hospitalization for COPD exacerbations during follow-up based on the International Classification of Diseases, 9th Revision, Clinical modification [ICD-9-CM] codes of 491, 492, and 496 in the primary diagnosis position. The algorithm had a specificity of 99.8% and a positive predictive value of 85.6%.18
Using the “first exposure carried forward” analysis, we followed patients from the index date to the earliest of outcome occurrence, death, end of the study (December 31, 2015), or 180 days after the index date. This approach classifies patients based on their index exposure groups and preserves the baseline comparability between groups. We truncated the follow-up time at 180 days after the index date to address potential exposure misclassification during long-term follow-up.
Ascertainment of Predefined Covariates at Baseline
Baseline predefined covariates included age on the index date, sex, COPD duration (defined as duration from the first COPD diagnosis date to the index date), calendar year of the index date, mean dose of the index prescription, as well as resource utilization, comorbidities, and other medication use recorded within 365 days before the index date. Specifically, we included several substantial covariates highly associated with COPD exacerbations including cardiovascular-related comorbidities, medications, outpatient visits, and hospitalizations; proxies for COPD severity (COPD duration, COPD-related outpatient visits, and COPD-related hospitalizations); infection-related variables (diagnosis of pneumonia, influenza, or acute bronchitis and use of antibiotics); and use of inhaled treatment.
We measured resource utilization based on records of outpatient visits and hospital admission. We ascertained comorbidities based on outpatient and inpatient diagnosis and procedure files and assessed medication use based on pharmacy dispensing claims of the outpatient clinics, community pharmacies, and hospital admission. Appendix Tables 2–4 provide more detailed covariate information.
Statistical Analysis
To control for multiple measured confounders, we estimated baseline propensity scores (PS) for each individual, defined as the probability of initiating statins versus fibrates derived from a logistic regression model conditional on the covariates mentioned above.19 To further mitigate potential unmeasured confounding, we conducted high-dimensional PS (hd-PS) estimation, which is a semi-automated algorithm that identifies and prioritizes a large number of empirical covariates that are simultaneously associated with exposure and outcome. The hd-PS approach therefore facilitates to control for confounders that are not predefined or that are imbalanced between exposure and outcomes by chance.20,21 We chose a total of 100 empirically identified variables and combined these with the above mentioned predefined covariates to estimate baseline hd-PS for each patient by logistic regression.
Since we had many more patients who initiated statins, we matched up to 10 patients who initiated statins to each patient who initiated fibrates using a nearest-neighbor algorithm without replacement and with a maximum matching caliper of 0.025 on the PS and hd-PS scales, respectively.22 We used Cox proportional hazard models to estimate HRs and 95% CIs of COPD exacerbations comparing statins versus fibrates in the 10:1 variable-ratio PS and hd-PS matched cohorts, respectively. To account for the variable-ratio matching, the Cox model was stratified on the matching ratio.22 We also plotted Kaplan–Meier curves to demonstrate the probability of free of COPD exacerbations over time.
Variable-ratio matching yields covariate balance within each matched set, but not marginally in the overall matched population.22 We therefore randomly selected one initiator of statins from each set of patients matched to each fibrate initiator and examined whether adequate balance in covariates was achieved between treatment groups using the index of standardized difference23,24 among this sample. To compute this index, the difference in mean was divided by the pooled standardized deviation between groups with an absolute value of less than 0.1 suggesting no substantial difference. As compared to a traditional p-value, the index of standardized difference is less likely sensitive to sample size, tends to identify a clinically meaningful difference (rather than a statistically significant difference), if any, and are specifically useful for studies with large sample size.
Sensitivity and Subgroup Analyses
In the sensitivity analyses, we examined if the risk of COPD exacerbations associated with statins changed materially by follow-up duration (365, 730 days, or no truncation at maximum follow-up duration). In addition, to prevent exposure misclassification, we also applied an on-treatment analysis that followed patients from the index date to outcome occurrence, death, end of the study (December 31, 2015), 180 days after the index date, or treatment discontinuation or change, whenever came first. Treatment discontinuation was defined using a grace period of up to 30 days between the end of one prescription and the date of the next prescription, if any. Treatment change was defined as the dispensing of a fibrate for statin initiators or the dispensing of a statin for fibrate initiators.
In the subgroup analyses, we separately compared individual statins with fibrates to explore potential differential risk by type of statins. We also conducted the analyses by age (≥65 and <65 years), sex (male and female), history of cardiovascular disease, diabetes, or asthma, and prior hospitalizations due to COPD. We re-estimated the hd-PS and re-matched patients in each of these analyses.25
Results
Eligible Cohorts and Baseline Characteristics
We included a total of 134,909 eligible patients; 110,726 initiated statins (82%) and 24,183 initiated fibrates (18%). Among patients who initiated statins, atorvastatin (40%), rosuvastatin (21%), and simvastatin (17%) were used most frequently. Among patients who initiated fibrates, fenofibrate (64%) and gemfibrozil (31%) were prescribed predominantly (Figure 1). The mean (SD) age of the cohort was 67 (11) years and 51% were male. In terms of chronic comorbidities, most patients had hypertension (68%) and hyperlipidemia (67%); 42% had gastritis or peptic ulcer disease; 37% had diabetes; and 32% had ischemic heart disease. In terms of acute respiratory infections, 53% had pneumonia, influenza, or acute bronchitis within one year before the index date (Table 1 and Appendix Table 5).
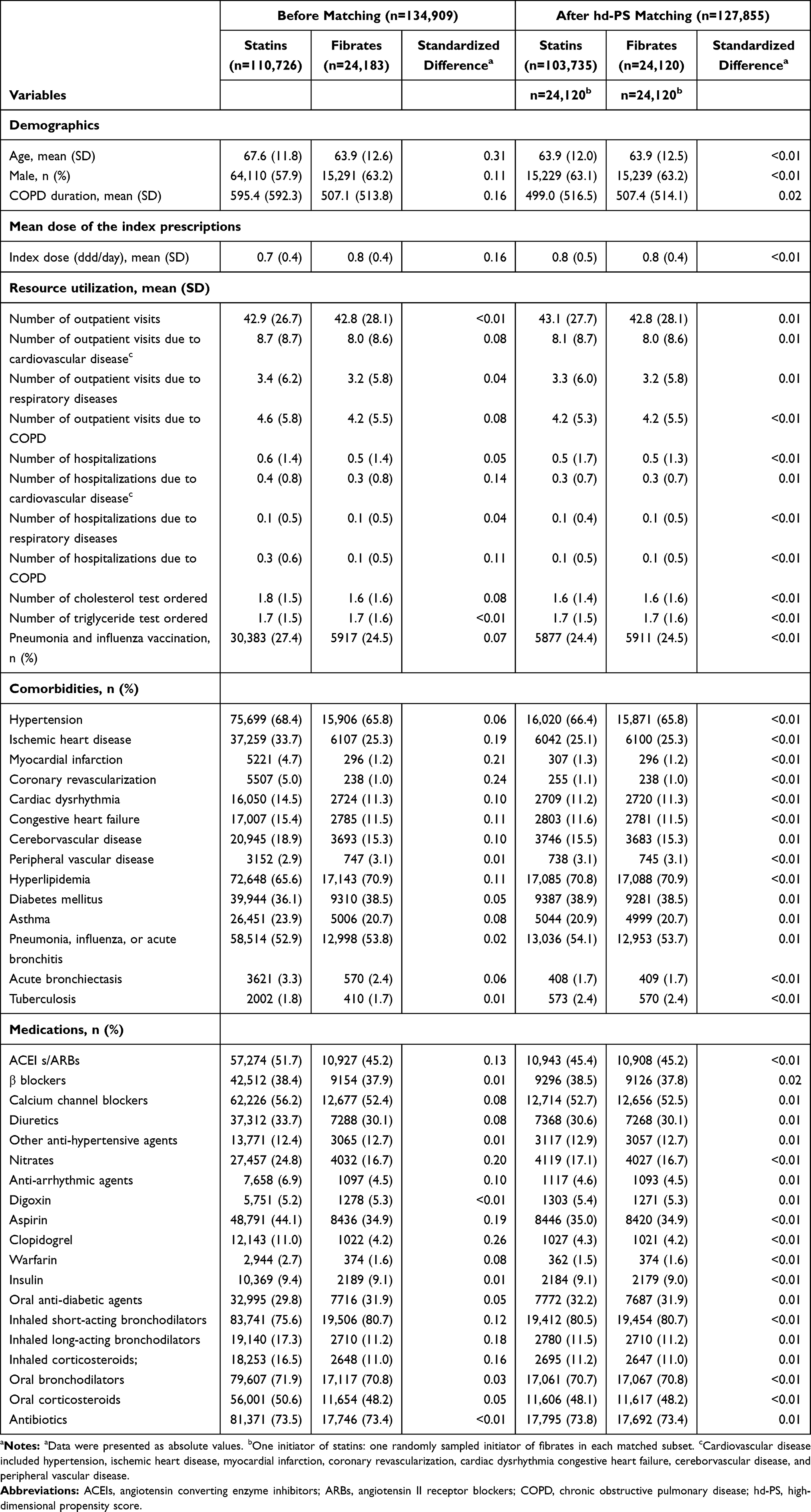 |
Table 1 Selected Baseline Characteristics of the Eligible Cohort |
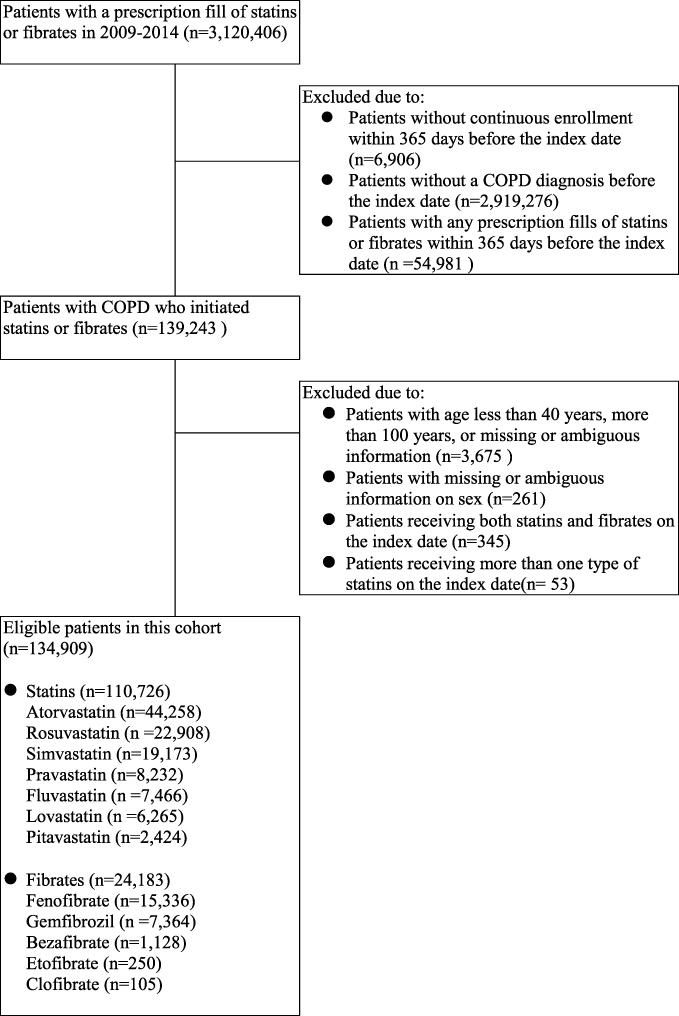 |
Figure 1 Flowchart of the study cohort assembly. Abbreviation: COPD, chronic obstructive pulmonary disease. |
Before matching, patients who initiated statins were older; had more frequent hospitalizations due to cardiovascular disease and COPD; were more likely to have had a diagnosis of cardiovascular disease; and were more likely to have used cardiovascular medications, inhaled long-acting bronchodilators, and inhaled corticosteroids compared to patients who initiated fibrates. Instead, patients who initiated fibrates tended to be male; had a higher mean dose of the index prescription; were more likely to have had a diagnosis of hyperlipidemia, chronic liver disease, and gout; and were more likely to have used inhaled short-acting bronchodilators and anti-gout medications. After hd-PS matching, a total of 127,855 patients (103,735 statin initiators and 24,120 fibrate initiators; 95% of the total study cohort) were included in the analysis. All patient characteristics were well balanced between statin initiators and fibrate initiators, with most standardized differences less than 0.01 (Table 1 and Appendix Table 5).
Risk of COPD Exacerbations Associated with Statins versus Fibrates
The crude incidence rate of COPD exacerbations was 32.41 per 1000 person-years (95% CI, 30.92 to 33.97) in the statin initiators and 20.71 per 1000 person-years (95% CI,18.27 to 23.48) in the fibrate initiators with the “first exposure carried forward” analysis during 180 days of follow-up, which corresponded to a crude HR of 1.56 (95% CI, 1.37 to 1.79) comparing statins with fibrates. However, after adjustment for baseline covariates, there was no significantly different risk associated with statin use. The HRs after PS matching and after hd-PS matching were 1.10 (95% CI, 0.96 to 1.26) and 1.08 (95% CI, 0.94 to 1.24), respectively (Table 2). The Kaplan–Meier curves comparing the probability of free of COPD exacerbations between statin initiators and fibrate initiators were consistent with the findings (Figure 2).
 |
Table 2 Follow-Up, Event Rates, and Risk of COPD Exacerbations Comparing Statins with Fibrates |
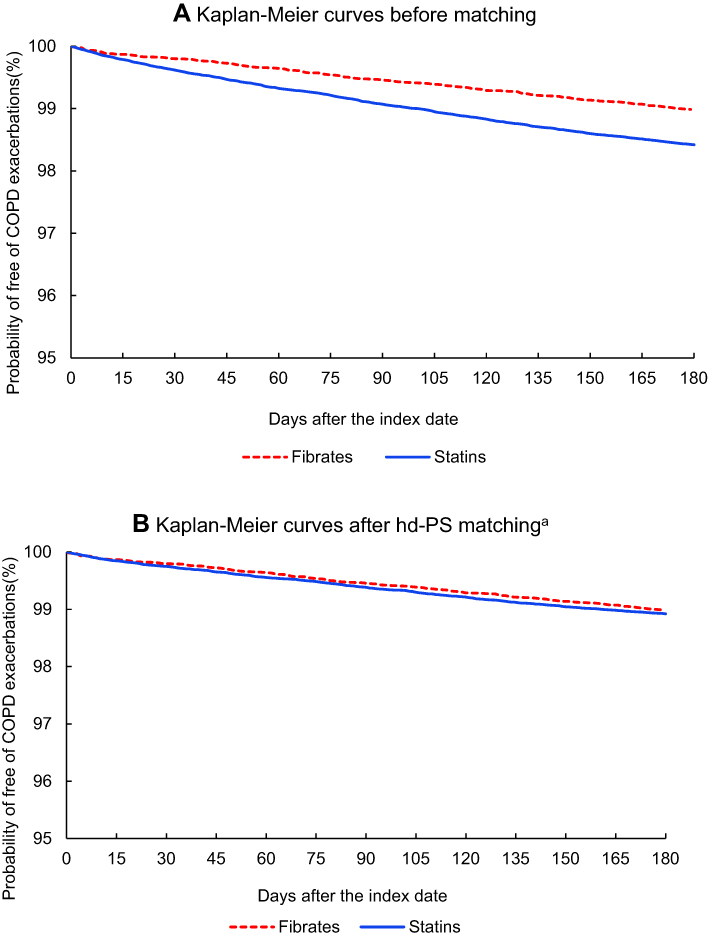 |
Figure 2 Kaplan–Meier curves for the probability of free of COPD exacerbations within 180 days after the index date (A) Kaplan–Meier curves before matching. (B) Kaplan–Meier curves after hd-PS matchinga. aData were weighted by matching ratio in the hd-PS matching analysis. Abbreviations: COPD, chronic obstructive pulmonary disease; hd-PS, high-dimensional propensity score. |
Findings of the Sensitivity and Subgroup Analyses
The findings were similar when we followed patients for longer periods or when we conducted the on-treatment analysis (Table 3). We also did not observe material change when stratifying by type of statins (atorvastatin, rosuvastatin, simvastatin, and other statins) or patient characteristic (age, sex, history of cardiovascular disease, diabetes, or asthma, and prior hospitalizations due to COPD) (Table 4).
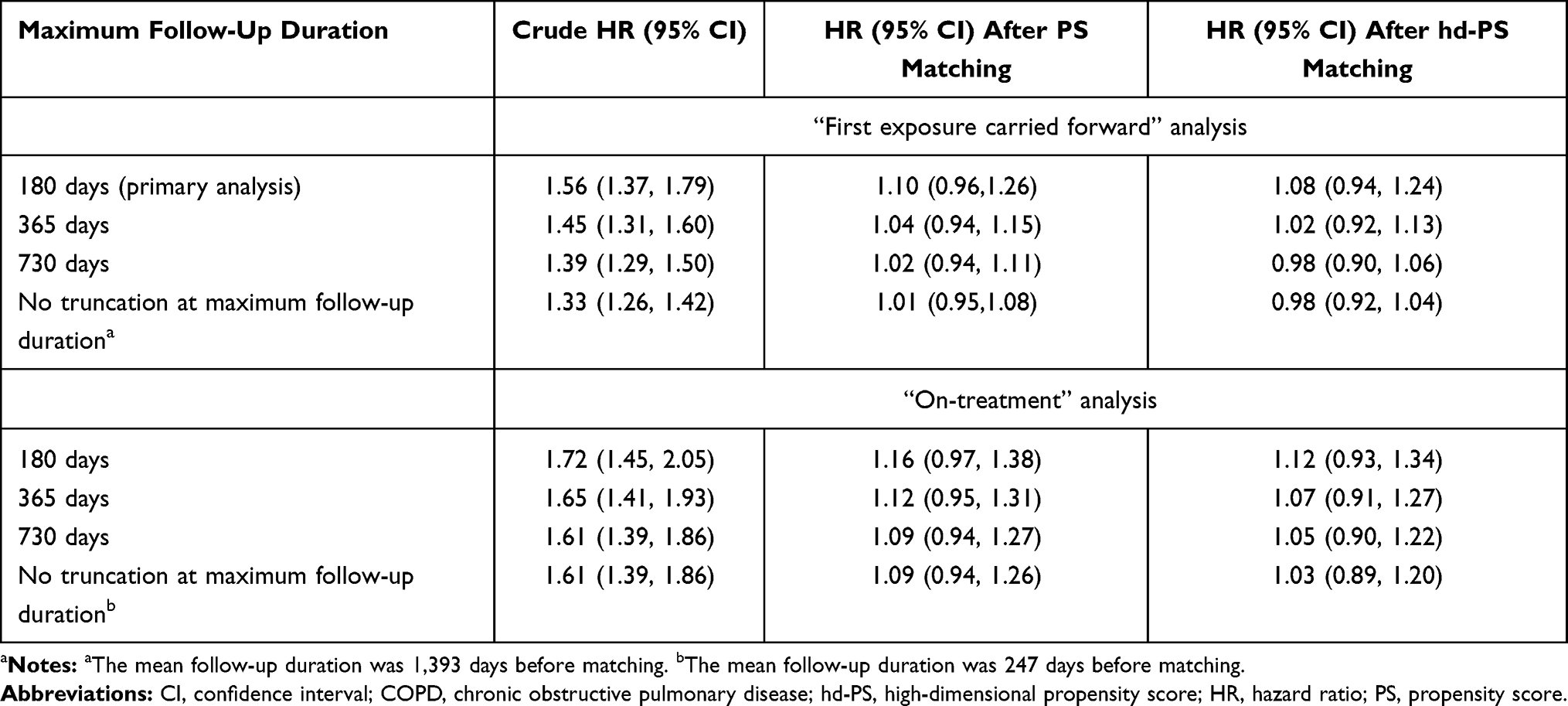 |
Table 3 Risk of COPD Exacerbations Comparing Statins with Fibrates, by Maximum Follow-Up Duration and Follow-Up Scheme |
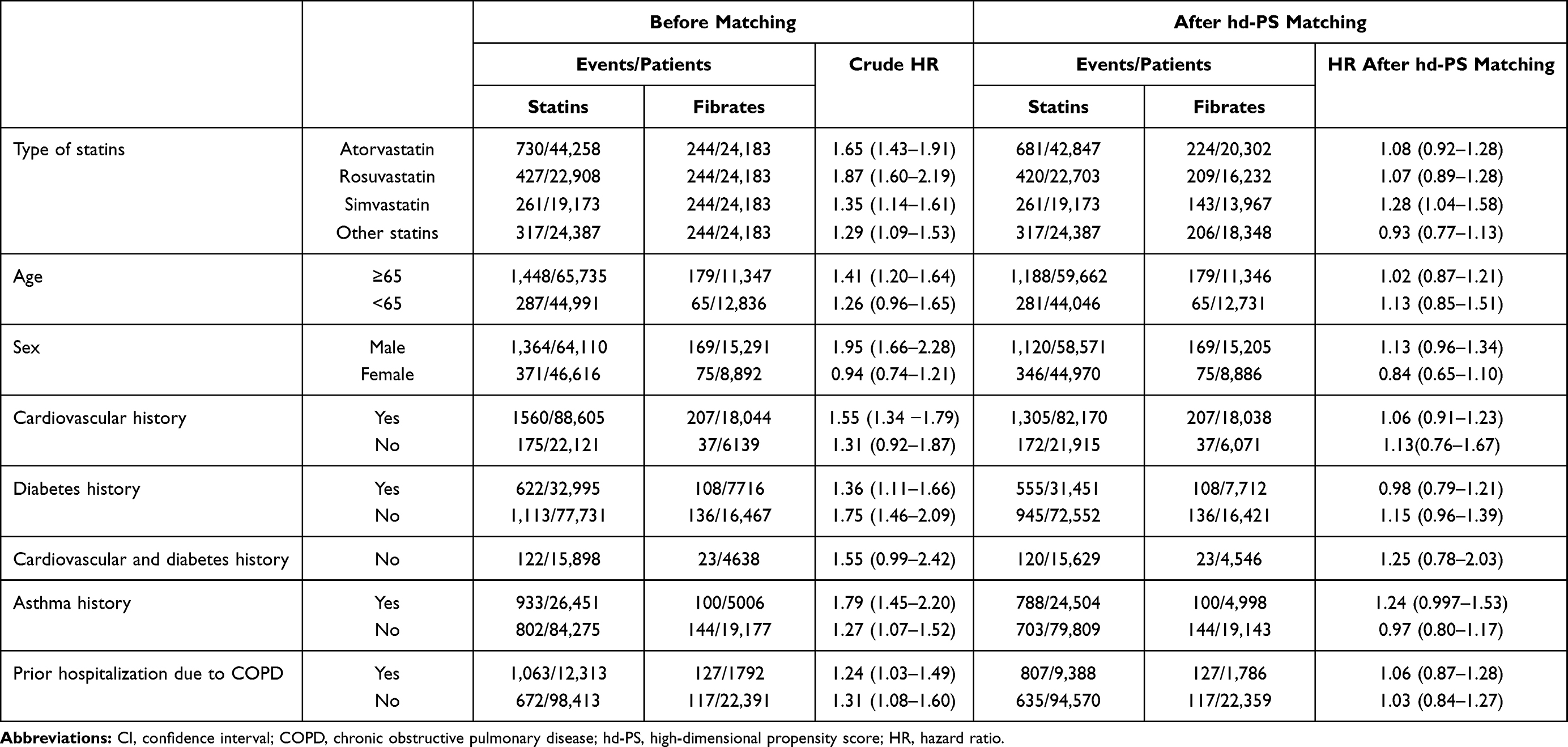 |
Table 4 Risk of COPD Exacerbations Comparing Statins with Fibrates, by Type of Statins and Patient Characteristic |
Discussion
In this large-scale, population-based cohort study, we examined the risk of COPD exacerbations associated with statins in patients with COPD with a new user, active comparison, hd-PS matched design. There was no strong evidence to suggest a decreased risk of COPD exacerbations associated with statins compared to fibrates. The findings were robust when we applied different follow-up durations or follow-up schemes. There were also no differential risks by type of statins and patient characteristic.
Challenges of Exploring Statin Effectiveness in Real-World Settings
A number of observational studies have examined the role of statins in reducing COPD exacerbations with a prevalent user, non-user comparison approach (Appendix Table 6).26–37 Most of them suggested that use of statins may have a remarkable benefit, with relative risks of 0.19 to 0.89 compared to the non-use of statins.26–32,34–36
The benefit associated with statins is even larger than the mainstay COPD treatment – long-acting β2 agonists, long-acting muscarinic antagonists, and long-acting β2 agonists and inhaled corticosteroids combinations – which decrease acute exacerbations leading to hospitalizations by 14% to 18%.38,39 On the other hand, although in vitro and in vivo studies have suggested that statins may have anti-inflammatory effects,7 one meta-analysis of six randomized placebo-controlled trials did not identify a significant reduction in the C-reactive protein level associated with the use of statins.40 Moreover, the STATCOPE trial did not observe that use of simvastatin lowered exacerbation rates or delayed the time to a first exacerbation during a mean follow-up of 640 days.8 Collectively, the profound protective effect of statins should be interpreted with caution because of the potential design limitations of available observational studies.
The prevalent user, non-user comparison approach is convenient to implement and has an advantage of reserving the sample size. However, corresponding methodological issues have also been discussed in the examples exploring statin effectiveness not only for COPD exacerbations,10 but also for influenza-like outcomes11 and overall mortality.12 Specifically, the prevalent user design, which identifies patients who have received statins for a period, may deplete susceptible population because patients who are not responding well to statins tend to stop treatment and therefore have less chances to be included in the analysis.11,12 In addition, the non-user comparison design usually decides use or non-use of statins based on the exposure status after cohort entry. Patients who receive statins may accordingly have a non-exposure follow-up time prior to treatment in which the outcome could not occur, ie, “immortal time,” which guarantees the calculation of less events in the statin group than in the non-statin group.10 The depletion of susceptible population and the immortal time bias have been demonstrated to overestimate statin effectiveness.10−12 Moreover, in the non-user comparison design, patient characteristics are usually not comparable between users and non-users of stains, leading to potential confounding by indication.13,14 Unlike the available observational studies shown in Appendix Table 6, the present study applied a new user, active comparison design and did not find a decreased risk of COPD exacerbations associated with statin initiators compared with fibrate initiators. The results replicated the findings of the STATCOPE trial, which supports our assumption and study validity.
Potential Differential Influence on COPD Exacerbations Across Individual Statins and Subgroup Patients
Another issue is that type of statins and patient characteristics were different between the available observational studies and the STATCOPE trial. Specifically, observational studies included study patients who used a variety of statins and had concomitant cardiovascular disease,8 but the STATCOPE trial only focused on simvastatin and enrolled patients simultaneously without cardiovascular diseases and diabetes.9 Some observational studies have also suggested that the benefit of statins in ameliorating COPD exacerbations is only restricted to patients with cardiovascular comorbidities.30,31,34 However, the present study did not observe a benefit associated with statin use regardless of type of statin or history of cardiovascular diseases, diabetes, or asthma. Further randomized controlled trials that examine different statin use and include patients with significant cardiovascular disease may facilitate to elucidate the potential differential influence on COPD exacerbations across individual statins and specific subgroup of patients.
Strength and Limitation of the Present Study
Our study identified more than 100,000 patients from a population-based healthcare claims database. The large sample size enables us to apply the rigorous new user, active comparison design to address potential methodological considerations. The large sample size also facilitates to examine potential effect modification by type of statins and patient characteristic. In addition, we applied a validated algorithm to identify hospitalized exacerbation events, which mitigated potential outcome misclassification. Moreover, we matched statin and fibrate initiators not only using traditional PS which included more than 50 potential predefined confounders but also using advanced hd-PS which additionally accounted for 100 empirically driven covariates. The good balance in patient characteristics between the treatment groups, to a certain extent, indicated that the confounding effects might be minimal in our study.
Our study has several limitations. First, to minimize potential exposure misclassification during long-term follow-up, our main analysis of the “first exposure carried forward” approach followed patients up to 180 days after cohort entry. This may not identify the long-term effectiveness of statins, if any, accordingly. However, the sensitivity analyses followed patients up to 365 days or 730 days, respectively, or even did not restrict the maximum follow-up duration. The null findings supported the result robustness. In addition, to improve confounding control, we applied the active comparison design, included proxies for COPD severity (such as COPD duration and prior hospitalizations due to COPD) and risk factors of COPD exacerbations (such as history of exacerbation attacks or respiratory infections), and matched study patients with the sophisticated hd-PS algorithm. However, we need to recognize that we could not capture certain important information on health behavior and clinical measurements such as smoking, lung function tests, or eosinophil counts, which is an inherent limitation of health-care claims databases.
Conclusion
This large-scale, population-based cohort study did not show that use of statins was associated with a reduced risk of acute exacerbations in patients with COPD using state-of-the-art pharmacoepidemiologic approaches. The findings emphasize the importance of applying appropriate methodology in exploring statin effectiveness in real-world settings. Statins should not be used as a routine treatment in patients with COPD, especially for patients without cardiovascular indications.
Data Sharing Statement
No additional data available.
Author Contributions
Shu-Hui Sun, Chia-Hsuin Chang, and Yaa-Hui Dong designed the study. Yaa-Hui Dong acquired data. Zhe-Wei Zhan, Wen-Hsuan Chang, and Yu-An Chen analyzed data. Shu-Hui Sun, Chia-Hsuin Chang, Zhe-Wei Zhan, Wen-Hsuan Chang, Yu-An Chen, and Yaa-Hui Dong interpreted data. Yaa-Hui Dong drafted the manuscript. Shu-Hui Sun and Chia-Hsuin Chang provided critical suggestion on the manuscript. Shu-Hui Sun and Yaa-Hui Dong obtained funding. Dr Dong is the grantor. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Role of the Funder/Sponsor
The funding source has no role in study design, collection, analysis and interpretation of data, writing of the report, and in the decision to submit the article for publication.
Funding
This study was partly supported by National Yang-Ming University Far Eastern Memorial Hospital Joint Research Program (#NYMU-FEMH 108DN09) and the research grant from National Yang-Ming University (107F016-3). The results were presented, in part and in a poster abstract, at the ISPE’s 35th International Conference on Pharmacoepidemiology and Therapeutic Risk Management (ICPE 2019) on August 24-28, 2019 at the Pennsylvania Convention Center, Philadelphia, Pennsylvania. The poster abstract was published in “Poster Abstracts” in Pharmacoepidemiol Drug Saf. 2019;28(Supplement 2):7. https://onlinelibrary.wiley.com/toc/10991557/2019/28/S2.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Diseases. Report; 2021. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
2. Seemungal TA, Hurst JR, Wedzicha JA. Exacerbation rate, health status and mortality in COPD – a review of potential interventions. Int J Chron Obstruct Pulmon Dis. 2009;4:203–223.
3. Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931.
4. Wedzicha JA, Seemungal TA. COPD exacerbations: defining their cause and prevention. Lancet. 2007;370(9589):786–796.
5. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;74(10):1376–1414.
6. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the Management of Blood Cholesterol: executive Summary: a Report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2019;73(24):3168–3209.
7. Young RP, Hopkins R, Eaton TE. Pharmacological actions of statins: potential utility in COPD. Eur Respir Rev. 2009;18(114):222–232.
8. Cao C, Wu Y, Xu Z, et al. The effect of statins on chronic obstructive pulmonary disease exacerbation and mortality: a systematic review and meta-analysis of observational research. Sci Rep. 2015;5:16461.
9. Criner GJ, Connett JE, Aaron SD, et al. COPD Clinical Research Network; Canadian Institutes of Health Research. Simvastatin for the prevention of exacerbations in moderate-to-severe COPD. N Engl J Med. 2014;370(23):2201–2210.
10. Suissa S. Simvastatin in moderate-to-severe COPD. N Engl J Med. 2014;371(10):969–970.
11. Brassard P, Wu JW, Ernst P, Dell’Aniello S, Smiechowski B, Suissa S. The effect of statins on influenza-like illness morbidity and mortality. Pharmacoepidemiol Drug Saf. 2017;26(1):63–70.
12. Danaei G, Tavakkoli M, Hernán MA. Bias in observational studies of prevalent users: lessons for comparative effectiveness research from a meta-analysis of statins. Am J Epidemiol. 2012;175(4):250–262.
13. Lund JL, Richardson DB, Stürmer T. The active comparator, new user study design in pharmacoepidemiology: historical foundations and contemporary application. Curr Epidemiol Rep. 2015;2(4):221–228.
14. D’Arcy M, Stürmer T, Lund JL. The importance and implications of comparator selection in pharmacoepidemiologic research. Curr Epidemiol Rep. 2018;5(3):272–283.
15. National Health Insurance Administration. 2020-2021 National Health Insurance Annual Report. Available from: https://www.nhi.gov.tw/resource/Webdata/2020-2021%E5%85%A8%E6%B0%91%E5%81%A5%E5%BA%B7%E4%BF%9D%E9%9A%AA%E5%B9%B4%E5%A0%B1.pdf. Accessed August 13, 2021.
16. Lin LY, Warren-Gash C, Smeeth L, Chen PC. Data resource profile: the National Health Insurance Research Database (NHIRD). Epidemiol Health. 2018;40:e2018062.
17. Gershon AS, Wang C, Guan J, Vasilevska-Ristovska J, Cicutto L, To T. Identifying individuals with physician diagnosed COPD in health administrative databases. COPD. 2009;6(5):388–394.
18. Stein BD, Bautista A, Schumock GT, et al. The validity of International Classification of Diseases, Ninth Revision, Clinical Modification diagnosis codes for identifying patients hospitalized for COPD exacerbations. Chest. 2012;141:87–93.
19. Rubin DB. Estimating causal effects from large data sets using propensity scores. Ann Intern Med. 1997;127(8 Pt 2):757–763.
20. Schneeweiss S, Rassen JA, Glynn RJ, Avorn J, Mogun H, Brookhart MA. High-dimensional propensity score adjustment in studies of treatment effects using health care claims data. Epidemiology. 2009;20(4):512–522.
21. Schneeweiss S. Automated data-adaptive analytics for electronic healthcare data to study causal treatment effects. Clin Epidemiol. 2018;10:771–788.
22. Rassen JA, Glynn RJ, Brookhart MA, Schneeweiss S. Pharmacoepidemiology Toolbox. Boston, MA: Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School. Available from: https://www.drugepi.org/dope/software#Pharmacoepidemiology.
23. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–3107.
24. Mamdani M, Sykora K, Li P, et al. Reader’s guide to critical appraisal of cohort studies: 2. Assessing potential for confounding. BMJ. 2005;330(7497):960–962.
25. Rassen JA, Glynn RJ, Rothman KJ, Setoguchi S, Schneeweiss S. Applying propensity scores estimated in a full cohort to adjust for confounding in subgroup analyses. Pharmacoepidemiol Drug Saf. 2012;21(7):697–709.
26. Mancini GB, Etminan M, Zhang B, Levesque LE, FitzGerald JM, Brophy JM. Reduction of morbidity and mortality by statins, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers in patients with chronic obstructive pulmonary disease. J Am Coll Cardiol. 2006;47(12):2554–2560.
27. Blamoun AI, Batty GN, DeBari VA, Rashid AO, Sheikh M, Khan MA. Statins may reduce episodes of exacerbation and the requirement for intubation in patients with COPD: evidence from a retrospective cohort study. Int J Clin Pract. 2008;62(9):1373–1378.
28. Bartziokas K, Papaioannou AI, Minas M, et al. Statins and outcome after hospitalization for COPD exacerbation: a prospective study. Pulm Pharmacol Ther. 2011;24(5):625–631.
29. Huang CC, Chan WL, Chen YC, et al. Statin use and hospitalization in patients with chronic obstructive pulmonary disease: a nationwide population-based cohort study in Taiwan. Clin Ther. 2011;33(10):1365–1370.
30. Ozyilmaz E, Kokturk N, Teksut G, Tatlicioglu T. Unsuspected risk factors of frequent exacerbations requiring hospital admission in chronic obstructive pulmonary disease. Int J Clin Pract. 2013;67(7):691–697.
31. Wang MT, Lo YW, Tsai CL, et al. Statin use and risk of COPD exacerbation requiring hospitalization. Am J Med. 2013;126(7):598–606.
32. Ingebrigtsen TS, Marott JL, Nordestgaard BG, Lange P, Hallas J, Vestbo J. Statin use and exacerbations in individuals with chronic obstructive pulmonary disease. Thorax. 2015;70(1):33–40.
33. Citgez E, van der Palen J, Koehorst-Ter Huurne K, Movig K, van der Valk P, Brusse-Keizer M. Statins and morbidity and mortality in COPD in the COMIC study: a prospective COPD cohort study. BMJ Open Respir Res. 2016;3(1):e000142.
34. Ajmera M, Shen C, Sambamoorthi U. Association between statin medications and COPD-specific outcomes: a real-world observational study. Drugs Real World Outcomes. 2017;4(1):9–19.
35. Lin CM, Yang TM, Yang YH, et al. Statin use and the risk of subsequent hospitalized exacerbations in COPD Patients with frequent exacerbations. Int J Chron Obstruct Pulmon Dis. 2020;15:289–299.
36. Huang YJ, Kao S, Kao LT, et al. Association between statin use and exacerbation of chronic obstructive pulmonary disease among patients receiving corticosteroids. Int J Chron Obstruct Pulmon Dis. 2021;16:591–602.
37. Damkjær M, Håkansson K, Kallemose T, Ulrik CS, Godtfredsen N. Statins in high-risk chronic obstructive pulmonary disease outpatients: no impact on time to first exacerbation and all-cause mortality - the STATUETTE cohort study. Int J Chron Obstruct Pulmon Dis. 2021;16:579–589.
38. Calverley PM, Anderson JA, Celli B, et al. TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789.
39. Tashkin DP, Celli B, Senn S, et al. UPLIFT Study Investigators. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554.
40. Zhang W, Zhang Y, Li CW, Jones P, Wang C, Fan Y. Effect of statins on COPD: a meta-analysis of randomized controlled trials. Chest. 2017;152(6):1159–1168.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.