Back to Journals » Risk Management and Healthcare Policy » Volume 19
Risk Factors of Thyroid Dysfunction in Patients with Acute Pancreatitis and Predictive Value of TSH for Disease Severity
Authors Li L, Li X, Liu B, Yu H, Yuan M
Received 21 October 2025
Accepted for publication 11 March 2026
Published 27 March 2026 Volume 2026:19 575782
DOI https://doi.org/10.2147/RMHP.S575782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Keon-Hyung Lee
Lujiao Li, Xiaohui Li, Bing Liu, Hengchi Yu, Mingxia Yuan
Department of Endocrinology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China
Correspondence: Mingxia Yuan, Department of Endocrinology, Beijing Friendship Hospital, Capital Medical University, No. 95 Yongan Road, Xicheng District, Beijing, 100050, People’s Republic of China, Email [email protected]
Background: Patients with acute pancreatitis (AP) commonly present with thyroid dysfunction in clinic. The present study aimed to characterize thyroid dysfunction in AP patients, identify the risk factors, assess its dynamics during AP resolution and evaluate its value for predicting AP severity.
Methods: A total of 182 AP patients and 61 age- and gender-matched patients with chronic pancreatitis (CP) were enrolled. Demographic characteristics, biochemical parameters and thyroid function were collected.
Results: AP patients had an average age of 53.3± 16.7 years and 61.5% were males; CP patients had an average age of 52.7± 11.9 years and 59.0% were males. Compared with CP group, the level of T3, T4, FT3 and TSH was significantly lower in AP group. A high prevalence of thyroid dysfunction (87.4%), manifested as decreased thyroid hormones and TSH, was observed in AP patients. The extent of hormone reduction was progressively exacerbated with increasing the disease severity. Albumin (Alb) was independently positive correlation, and hs-CRP and lactate (Lac) were independently negatively correlated with thyroid function. The levels of thyroid hormones and TSH increased during AP resolution. TSH demonstrated superior predictive value for moderate-to-severe AP compared to traditional markers (hs-CRP, Alb, Ca) and established severity scores (APACHE II, BISAP). The cut-off value of TSH was 0.42 μIU/mL with the highest AUC (0.772 (0.693– 0.851)) and the highest Youden’s index (0.478).
Conclusion: Thyroid dysfunction was common in AP patients, characterized by a reduction in thyroid hormones and TSH. Lower Alb and higher hs-CRP and Lac were independent risk factors of thyroid dysfunction. During AP resolution, thyroid dysfunction could spontaneously recover. Furthermore, a low level of TSH at admission showed promising predictive value for moderate to severe AP in the early stage.
Keywords: thyroid dysfunction, thyroid stimulating hormone, thyroid hormone, predictive value, acute pancreatitis
Introduction
As an essential part of endocrine system, the thyroid gland producing and secreting thyroid hormones plays crucial roles in regulating the energy metabolism, cardiovascular function (heart rate and contractility), and the development of the nervous and musculoskeletal systems.1 Thyroid hormones consist mainly of thyroxine (T4, ~90%) and triiodothyronine (T3, ~10%). As the active form, T3 binds directly to nuclear thyroid hormone receptors, whereas T4 converts to T3 to exert its biological effects.2 Under physiological conditions, circulating levels of T4 and T3 are maintained within a stable range through negative feedback inhibition of thyroid stimulating hormone (TSH) and thyrotropin-releasing hormone.3 However, in critical illness, alterations in thyroid hormone levels are not always due to intrinsic thyroid disease but often represent an adaptive physiological response known as non-thyroidal illness syndrome (NTIS). This dysregulation of the hypothalamic-pituitary-thyroid axis underlies multiple disorders characterized by thyroid dysfunction phenotypes. 4,5
Acute pancreatitis (AP) is a prevalent inflammatory condition of pancreas that can process to multi-organ dysfunction syndrome, characterized by cardiovascular failure, acute respiratory distress syndrome, acute kidney injury and gastrointestinal injury.6–8 The systemic inflammatory response in AP, characterized by a cytokine storm (eg, IL-6, TNF-α), is known to inhibit peripheral conversion of T4 to T3 and suppress TSH secretion, providing a pathophysiological link between AP and thyroid hormone alterations.9–11 However, the impact of AP on endocrine system remains inadequately characterized. Clinical observations frequently identify thyroid dysfunction in AP patients, yet limited research has focused on the association. Key unresolved questions contain: (1) the characteristics of thyroid dysfunction; (2) the potential risk factors of thyroid dysfunction; (3) the necessity for clinical intervention; and (4) its prognostic value in predicting AP severity. Early and accurate prediction of AP severity is clinically urgent to guide timely intensive interventions, improve patient triage, and potentially reduce mortality. 12
To bridge the gaps, the study was designed to: (1) characterize thyroid dysfunction profiles and identify their risk factors in AP patients; (2) longitudinally evaluate the natural trajectory of thyroid dysfunction following clinical resolution of AP; (3) determine the prognostic value of thyroid dysfunction for AP severity and compare it with traditional biomarkers and established severity scores.
Methods
Participants
This was a retrospective study. A total of 182 adult patients diagnosed with AP in Beijing Friendship Hospital, Capital Medical University from January 2017 to December 2023 were enrolled. To serve as a control, 61 age- and gender-matched patients with chronic pancreatitis (CP) were recruited at a ratio of approximately 3:1. We specifically selected patients with CP who were in a clinically stable phase, without elevated inflammatory markers and with normal thyroid function, as controls. This design allowed us to contrast thyroid alterations in the acute inflammatory state of AP against a baseline of stable pancreatic disease, minimizing confounding from demographic factors while focusing on changes related to acute illness.13 There were 29 AP patients who had follow-up thyroid function data collected during outpatient visits at varying time points (ranging from 1 to 9 months) after the baseline assessment. These data were included to longitudinally analyze changes in thyroid function from baseline to after clinical improvement.
Inclusion criteria were as follows: 1. age was equal or older than 18 years; 2. the Han nationality; 3. for the case group, meeting the AP diagnostic criteria,12 which required at least two of the following three criteria: 1) persistent pain in upper abdomen with or without radiating to the back, 2) amylase and/or lipase increasing more than three-times the upper limit of normal, 3) evidence of AP from abdominal imaging examinations including contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI) or abdominal ultrasound; 4. for the control group, meeting the CP diagnostic criteria,13 which required at least one of the following criteria: 1) evidence of CP revealed by CT/magnetic resonance cholangiopancreatography (MRCP)/endoscopic retrograde cholangiopancreatography (ERCP)/endoscopic ultrasonography (EUS), 2) evidence of CP revealed by histopathology; 5. for the control group, who were in a stable phase with no elevation of inflammatory indicators (eg, normal white blood cell count and hs-CRP) and had thyroid function (T3, T4, FT3, FT4, TSH) within the normal reference ranges.
Exclusion criteria were as follows: 1. with a previous history of thyroid disease; 2. with other diseases that affected thyroid function; 3. recently receiving drugs that affected thyroid hormone secretion and metabolism, such as glucocorticoids, amiodarone; 4. with a previous history cancer, chronic liver and kidney disease, autoimmune diseases; 5. without sufficient or detailed medical records.
This study was approved by the Scientific Ethics Committee of Beijing Friendship Hospital, Capital Medical University (Approval number: 2021-P2-432-01). The committee granted a waiver of informed consent for this retrospective analysis of anonymized clinical data, as the research involved no more than minimal risk to participants, and obtaining consent was impracticable given the study’s retrospective nature. This waiver is in accordance with national regulations and ethical guidelines (eg, the Ethical Review Measures for Biomedical Research Involving Humans, 2016). All patient data were kept confidential and used solely for research purposes.
Clinical Evaluation for AP
According to the guidelines for diagnosis and treatment of acute pancreatitis in China (2021):12 AP was classified as biliary origin acute pancreatitis (BAP), hypertriglyceridemia-related acute pancreatitis (HAP), alcohol-related acute pancreatitis (AAP) and others by the etiologies. And by the severity, AP was classified as mild acute pancreatitis (MAP), moderately severe acute pancreatitis (MSAP) and severe acute pancreatitis (SAP) based on the revised Atlanta classification (RAC). MAP was defined as AP without organ failure and local or systemic complications. MSAP was defined as AP with transient organ failure and/or local complications (spontaneously resolved within 48h). SAP was defined as AP with persistent organ failure (persisting for at least 48h). Organ failure was assessed based on the modified Marshall scoring system, which was defined as a score more than 2. Additionally, to benchmark the predictive performance of TSH against established tools, the Acute Physiology and Chronic Health Evaluation II (APACHE II) and the Bedside Index for Severity in Acute Pancreatitis (BISAP) scores were calculated for all AP patients upon admission based on clinical data from the first 24 hours.
Biochemical Measurements
All serum biochemical parameters were measured in the central clinical laboratory of Beijing Friendship Hospital, Capital Medical University. Serum samples were obtained from all patients between 8:00 and 10:00 am after an overnight fast. Blood samples for thyroid function and other biochemical markers were collected within 48 hours after admission. The median (interquartile range) time from symptom onset to blood sampling was 4 (3, 5) days (mean ± SD: 4.27 ± 1.70 days), which captures the early inflammatory phase of AP. Triiodothyronine (T3), thyroxine (T4), free triiodothyronine (FT3), free thyroxine (FT4) and thyroid stimulating hormone (TSH) were quantified using an access immunoassay system (Unicel DxI 800; Beckman Coulter, America). The reference ranges of these indicators were 66–161 ng/dL for T3, 54.4–118.5 ng/mL for T4, 2.14–4.21 pg/mL for FT3, 0.59–1.25 ng/mL for FT4, 0.49–4.91 µIU/mL for TSH, respectively. The definition of thyroid dysfunction was that one or more of these indicators were outside the reference range. Meanwhile, blood routine examination, hypersensitive C reactive protein (hs-CRP), alanine aminotransferase (ALT), aspartate transaminase (AST), gamma-glutamyl transpeptidase (GGT), alkaline phosphatase (ALP), albumin (Alb), total bilirubin (TBil), direct bilirubin (DBil), total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), creatinine (Cr), calcium (Ca), lactate (Lac), amylase (AMY) and lipase (LPS) levels were measured using automated analyzers.
Statistical Analysis
Continuous data of normal distribution were expressed as mean ± standard deviation (SD). Continuous data of abnormal distribution were expressed as median (P25th, P75th). Categorical data were expressed as number and percentage (%). Independent sample t-test, rank-sum test and chi-square test were utilized to analyze continuous variables and categorical variables in cross-sectional comparison. ANOVA was used to analyze continuous variables among three groups, and Bonferroni post-hoc test was used for pairwise comparisons. The distribution of TSH was highly skewed (Shapiro–Wilk P < 0.001); therefore, a logarithmic transformation [ln(TSH)] was applied to achieve normality for use in multiple linear regression analysis. Multiple linear regressions were applied to examine the influence factors of thyroid hormones and ln(TSH). Multicollinearity among independent variables (including hs-CRP and Lac) was assessed using Variance Inflation Factors (VIF); all VIF values were <5, indicating no significant multicollinearity (Supplementary Table S1) Paired samples t-test and paired rank-sum test were used to longitudinally compare the change of thyroid function between baseline and after AP improvement. Receiver operating characteristic (ROC) curve analysis was performed to investigate the predictive values of thyroid function, biochemical markers, and severity scores (APACHE II, BISAP) for moderate to severe AP by calculating the cut-off value, area under curve (AUC), Youden’s index, sensitivity (SE), specificity (SP), positive predictive value (PPV) and negative predictive value (NPV). All statistical analyses were performed using SPSS version 27.0 software for Windows (SPSS Inc., Chicago, IL, USA). The statistical significance was indicated as two-tailed P < 0.05.
Results
Characteristics of Thyroid Dysfunction in AP Patients
The study enrolled 182 AP patients (average age 53.3 ± 16.7 years; 61.5% male) and 61 CP controls (average age 52.7 ± 11.9 years; 59.0% male). AP subtypes included 102 (56%) BAP, 38 (21%) HAP, 8 (4%) AAP and 34 (19%) other etiologies (Supplemental Figure 1). Compared with CP patients, AP patients exhibited significantly elevated levels of white blood cell, hematocrit, hs-CRP, ALT, AST, GGT, TBil, DBil, TC, AMY and LPS, alongside reduced Ca and Alb concentrations (Table 1). Notably, Alb levels were significantly higher in the stable CP group compared to the AP group (Table 1), reflecting the different metabolic and nutritional baselines between the acute illness and stable chronic disease states.
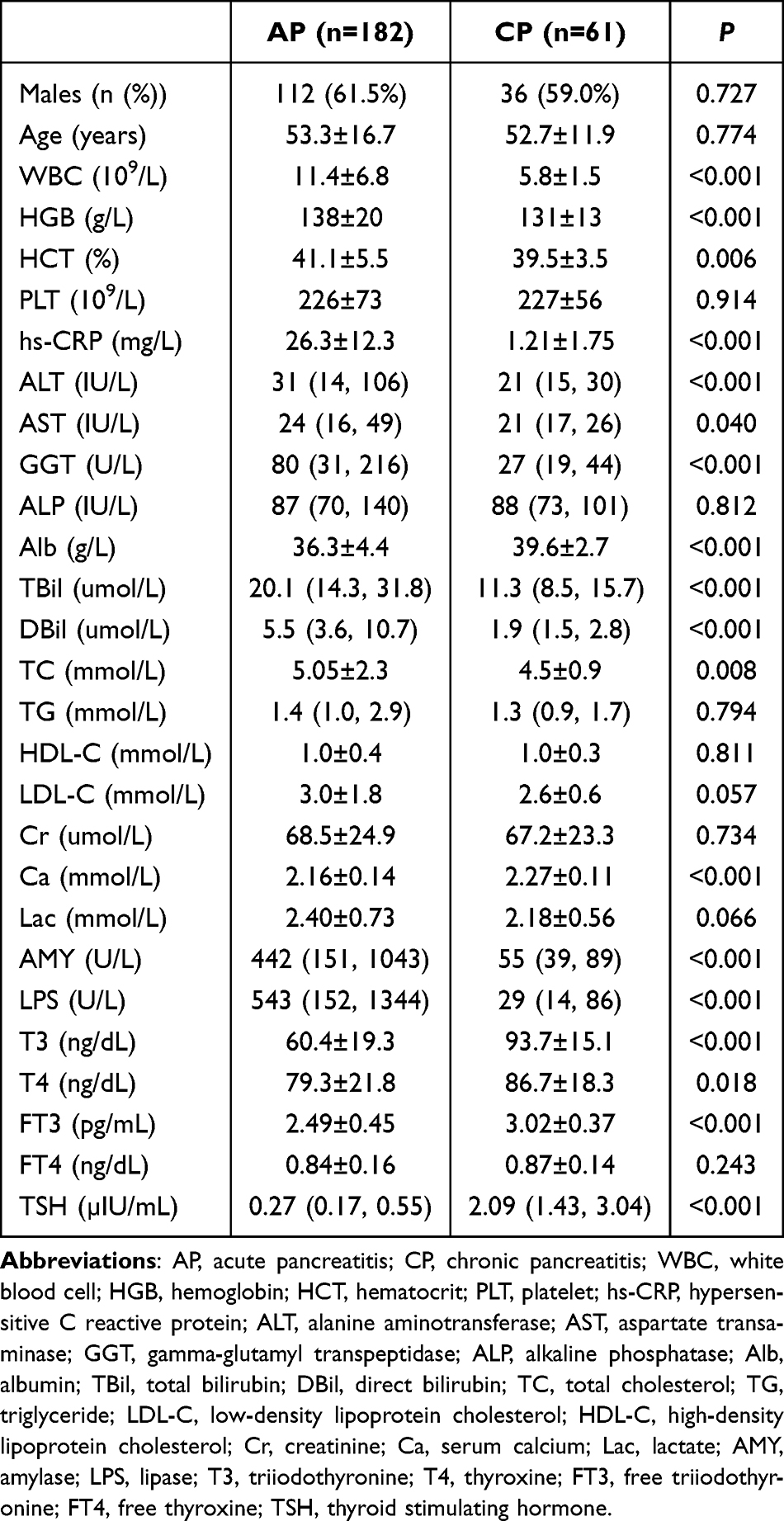 |
Table 1 Comparative Characteristics of AP vs. CP Patients |
Thyroid dysfunction was present in 87.4% of AP patients. Among these patients with thyroid dysfunction, 70.4% were classified as MSAP or SAP. The specific hormonal abnormalities detected included decreased levels of T3 (61.5%), T4 (9.9%), FT3 (20.3%), and FT4 (4.9%), as well as decreased TSH (71.4%) (Supplemental Figure 2). Thyroid dysfunction in AP patients was characterized by decreased levels of thyroid hormones (decreased levels of at least one thyroid hormone: T3, T4, FT3, or FT4, and TSH). In AP group, serum levels were: T3, 60.4 ± 19.3 ng/dL; T4,79.3 ± 21.8 ng/dL; FT3,2.49 ± 0.45 pg/mL; and TSH,0.27 [0.17, 0.55] µIU/mL. All these values were significantly lower than those in CP group (T3: P < 0.001; T4: P = 0.018; FT3: P < 0.001; TSH: P < 0.001) (Table 1).
Severity-Stratified Reductions in Thyroid Hormones Across AP Patients
Among the 182 AP patients, severity stratification identified 64 (35.2%), 69 (37.9%), and 49 (26.9%) as MAP, MSAP and SAP cases, respectively. No significant intergroup differences existed in age or gender distribution. Compared to MAP patients, those with MASP/SAP exhibited significantly elevated white blood cell counts, hs-CRP and Lac, alongside reduced Ca and Alb level. Critically, thyroid hormone levels demonstrated severity-dependent reductions: SAP patients showed the lowest values: T3 (47.5 ± 15.9 ng/dL), T4 (70.9 ± 18.5 ng/dL), FT3 (2.30 ± 0.42 pg/mL), TSH (0.19 (0.09–0.27) µIU/mL). MSAP patients displayed intermediate levels: T3 (60.3 ± 15.9 ng/dL), T4 (78.5 ± 17.4 ng/dL), FT3 (2.48 ± 0.43 pg/mL), TSH (0.26 (0.17–0.44) µIU/mL). MAP patients had the highest levels: T3 (70.1 ± 19.6 ng/dL), T4 (86.4 ± 25.8 ng/dL), FT3 (2.67 ± 0.44 pg/mL), TSH (0.51 (0.28–0.89) µIU/mL) (Table 2).
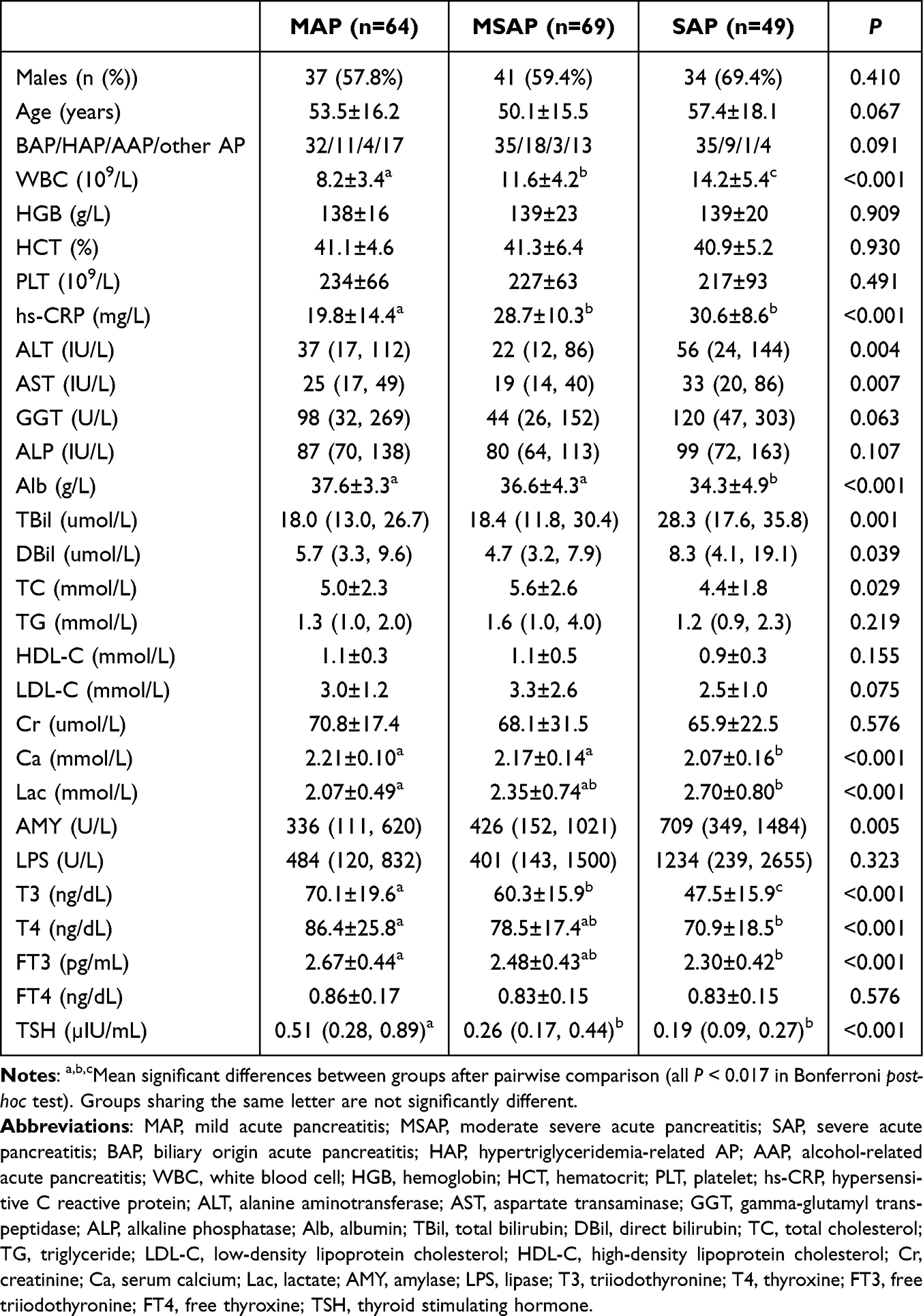 |
Table 2 Differential Patterns of Demographic, Clinical and Laboratory Profiles in AP Severity Cohorts |
Risk Factors of Thyroid Dysfunction in AP Patients
To identify the independent determinants of thyroid function in AP patients, hematocrit, hs-CRP, Ca, Alb and Lac from the univariate correlation analysis and age and gender were entered into the model for multivariate testing. As shown in Table 3, after controlling for confounding factors, Alb was positively correlated to T3 (β = 0.41, P < 0.001) and FT3 (β = 0.33, P < 0.001), hs-CRP was negatively correlated to T3 (β = −0.21, P = 0.003), T4 (β = −0.15, P = 0.043), FT3 (β = −0.14, P = 0.048), FT4 (β = −0.17, P = 0.032), ln(TSH) (β = −0.20, P = 0.011), and Lac was negatively correlated to T4 (β = −0.18, P = 0.021), FT3 (β = −0.24, P = 0.001), FT4 (β = −0.17, P = 0.026).
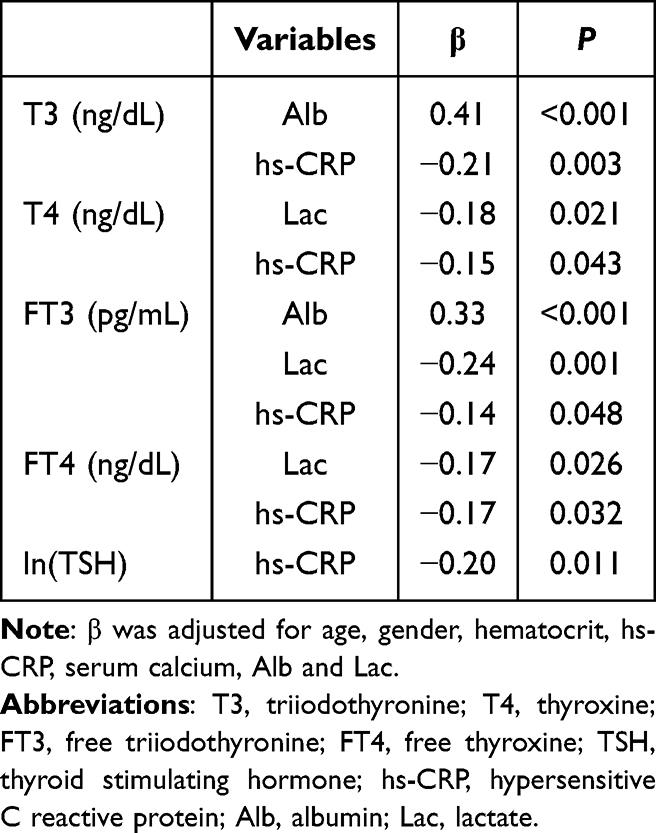 |
Table 3 Independent Influence Factors of Thyroid Function in AP Patients |
Dynamic Changes of Thyroid Function After AP Recovering
Follow-up thyroid function data were available for 29 AP patients. (15.9% of the total AP cohort). The follow-up time points varied (1–9 months) as this was a retrospective review of medical records, not a prospectively planned follow-up study, which is a limitation. At baseline, these patients exhibited high rates of thyroid hormone deficiencies: decreased T3 (58.6%), T4 (17.2%), FT3 (31.0%), FT4 (13.8%), and TSH (86.2%). Following clinical improvement of AP, significant increases were observed in T3 (90.0 ± 30.2 ng/dL), FT3 (3.07 ± 0.61 pg/mL), and TSH (1.22 (0.82–1.80) µIU/mL) (all P < 0.001) compared to baseline. Although T4 (87.4 ± 21.6 ng/dL) and FT4 (0.88 ± 0.16 ng/dL) showed non-significant upward trends, these dynamic changes collectively indicate spontaneous normalization of thyroid dysfunction with disease recovering (Table 4).
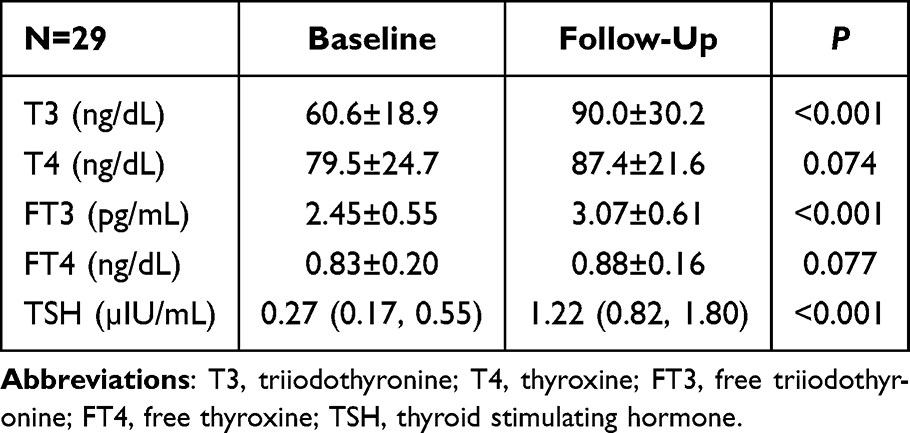 |
Table 4 Changes of Thyroid Function in AP Patients After Recovering |
Values of Thyroid Function in Predicting Severity of AP
ROC curve analysis compared the diagnostic utility of thyroid parameters (TSH, T3, T4), conventional severity biomarkers (hs-CRP, Alb, Ca) and established severity scores (APACHE II, BISAP) for predicting moderate-severe AP. The cut-off values, AUC, SE, SP, PPV and NPV were derived and contrasted in Table 5 and Figure 1. The AUC and Youden’s index of TSH in predicting moderate-severe AP was 0.772 (0.693–0.851) and 0.478, which was the highest among these indicators, with the SE 0.661, SP 0.817, PPV 0.793 and NPV 0.639. The best cut-off values of TSH for predicting moderate to severe of AP were 0.42µIU/mL. Importantly, the AUC of TSH was also higher than those of traditional biomarkers (hs-CRP, Alb, Ca) and the established severity scores APACHE II and BISAP in this cohort (Table 5 and Figure 1).
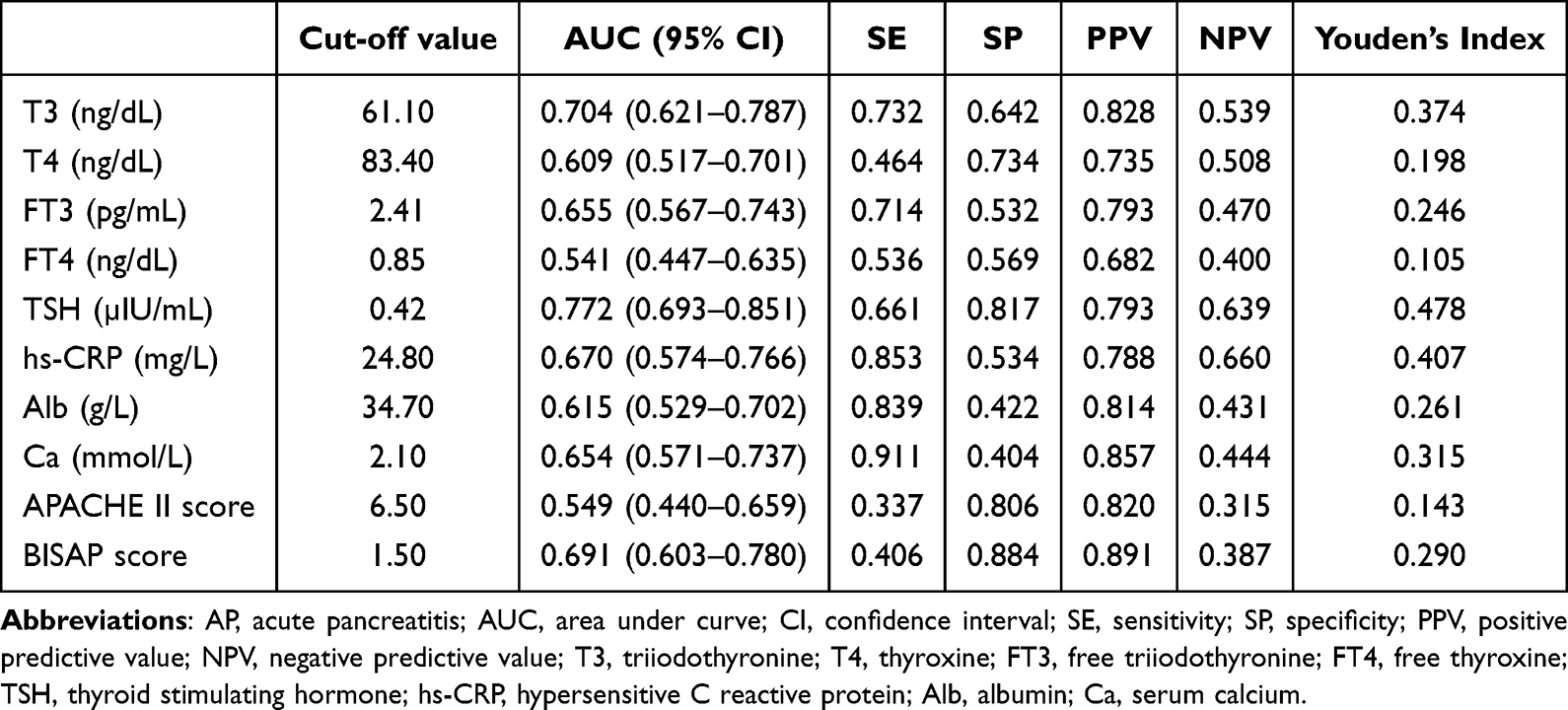 |
Table 5 Values of Thyroid Disfunction in Predicting Moderate to Severe AP |
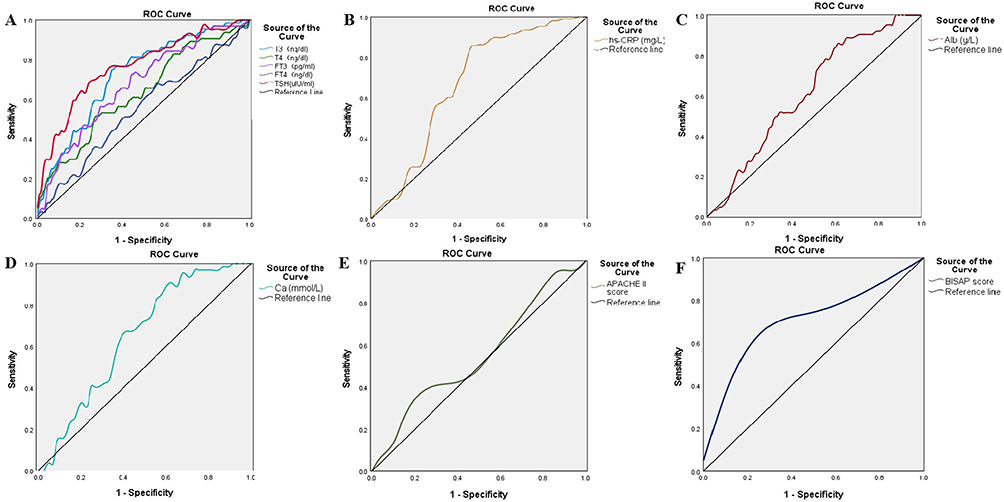 |
Figure 1 ROC curves evaluating thyroid hormones, biochemical markers, and severity scores for predicting moderate-to-severe AP. (A) Thyroid function panel: T3 (triiodothyronine), T4 (thyroxine), FT3 (free triiodothyronine), FT4 (free thyroxine), TSH (thyroid-stimulating hormone). (B) hs-CRP (Hypersensitive C-reactive protein). (C) Alb (Albumin). (D) Ca (calcium). (E) APACHE II score. (F) BISAP score. |
Discussions
Our data revealed significant associations between thyroid dysfunction and AP. Nearly 90% AP patients exhibited thyroid dysfunction characterized by the decreased level in both thyroid hormones and TSH. Besides, lower Alb and higher Lac and hs-CRP were found as independent risk factors for thyroid dysfunction in AP patients. Furthermore, our longitudinal data suggest that thyroid dysfunction could spontaneously return to normal with AP recovering. Most importantly, TSH could be a potential biomarker to predict AP severity, showing superior predictive value compared to traditional markers and established severity scores in our analysis.
Thyroid dysfunction was highly prevalent in AP patients, characterized by the reduction in serum T3, T4, FT3 and TSH, and accompanied by the worsening of AP, the level of T3, T4, FT3 and TSH gradually decreased. These characteristics align with the biochemical profile of non-thyroidal illness syndrome (NTIS), which was reported in a variety of acute illnesses including COVID‑19, sepsis, anorexia nervosa, myocardial infarction, cerebral infarction and many other disorders.14–18 In mild condition, only a decrease in serum T3 levels was observed, while throughout deterioration of condition, a drop in serum T4 would occur as well.19 This impairment results from reduced activity of thyroxine 5’-deiodinase, which catalyzes the conversion from T4 to T3.20 Furthermore, feedback regulation of thyroid axis was also out of the order. Furthermore, inflammatory cytokines (eg, IL-6, TNF-α) released during the systemic inflammatory response syndrome (SIRS) in AP can directly suppress hypothalamic-pituitary-thyroid axis function, leading to reduced TSH secretion and exacerbating the NTIS phenotype.9–11 Recent studies have further elucidated that oxidative stress and mitochondrial dysfunction in critical illness also contribute to the dysregulation of thyroid hormone metabolism.21
The pathogenesis of NTIS is complicated and multifactorial. Several possible mediators have been identified including a lack of nutrients, hypoxia, oxidative stress and release of cytokines.22,23 The present study evidenced that with the increasing of Alb, thyroid dysfunction was revising; inversely, with the increasing Lac and hs-CRP, it was worsening. Diet prohibition was a necessary therapeutic measure for AP patients, and the level of albumin reflected the patient’s nutritional status,24 thus a high level of Alb could prevent thyroid dysfunction in AP patients. This aligns with recent findings highlighting the role of nutritional status in modulating the endocrine response to stress. 25 The level of Lac represented the degree of tissue hypoxia.26 Thus, a high level of Lac could aggravate thyroid dysfunction in AP patients. The level of hs-CRP is an indicator of reflecting the severity of inflammation. Higher hs-CRP concentrations are associated with increased release of inflammatory cytokines, which could impair the hypothalamic–pituitary–thyroid axis, reduce the release of TSH and inhibit the synthesis or conversion of thyroid hormones.9–11
The necessity of treating reduced thyroid hormone levels in NTIS remains debated, as conclusive evidence for long-term efficacy of alternative therapies is lacking.27–30 Some studies have indicated that the alteration of thyroid function in the illness condition represent an adaptive response to protect the organism against the hyper- catabolism and deleterious energy expenditure.31,32 But another study indicated that NTIS could create a state of persistent hypothyroidism.33 It was also reported that thyroid hormone alternative therapy could increase the rate of remission of NTIS in patients with nephrotic syndrome.34 As concerns AP patients in the present study, 29 patients have follow-up thyroid function data. Thyroid dysfunction could spontaneously return to normal with the disease recovering in one to nine months. Therefore, the treatment of thyroid dysfunction in AP patients should be focused on management of underlying medical illness and dynamic monitoring of thyroid function. However, the small follow-up sample size (n=29) and the retrospective nature of follow-up data collection, with non-standardized time points, introduce potential selection bias and limit statistical power. Thus, these findings regarding spontaneous recovery should be interpreted with caution and require confirmation in larger prospective studies. Additionally, it should be noted that many AP patients undergo CT imaging with iodine-based contrast media, which may acutely influence thyroid function due to iodine load; however, our study design did not specifically adjust for this potential confounder. Future studies with larger cohorts are needed to confirm the observation.
It is crucial to rapidly identify and assess the severity of AP in the early stage to prevent disease aggravation.12 Although some biomarkers had been found to be related with AP severity, there was limited attention to dynamic changes of endocrine system during the disease progression.35 Although some score models could assess the disease severity to some extent, these methods were complex or time consuming to assess the prognosis of the disease, which could not better meet the clinical needs.36 In contrast, a single, rapidly available laboratory parameter like TSH could offer practical advantages in the emergency setting. Hence, it was critical to identify rapidly more severe cases in the early stage and to take intensive interventions to prevent the poor outcome. The predictive value for severity of AP among thyroid dysfunction and other traditional pancreatic severity markers including hs-CRP, Alb and Ca and established severity scores (APACHE II, BISAP) were compared in this study, we found that TSH was another applicable indicator, which might be superior to other related biomarkers and established severity scores in this cohort. However, the predictive performance of TSH needs to be validated in broader and specific patient populations, such as the elderly, those with underlying comorbidities (eg, chronic kidney disease, heart failure), or different ethnicities, as these factors might influence thyroid hormone metabolism and the NTIS response.37,38 There were two previous studies identifying that FT3 being valuable to predict the disease severity of AP and better compared to traditional serum indicators and scoring systems.39,40 But in the early stage of disease, TSH was better than FT3 to predict severity of AP. This may be because TSH, as the primary regulator of the thyroid axis, shows an earlier and more sensitive suppression in response to severe inflammation and stress compared to peripheral thyroid hormones. Therefore, detection of thyroid function in the initial stage of AP could help to identify more severe cases in the clinical work.
This study has several limitations. First, its retrospective design precluded the collection of dynamically monitored thyroid function data. Consequently, we were unable to analyze variations in thyroid function across different stages of AP. Second, we analyzed the follow-up data of thyroid function in AP patients and found that thyroid dysfunction could spontaneously return to normal; however, the follow-up sample size was limited (n=29) and the follow-up time points were not standardized, which may affect the results and introduce selection bias. Third, while restricting the study population to individuals of Han nationality enhanced genetic homogeneity, it limits the generalizability of the findings to other ethnic groups. Fourth, we used stable CP patients as controls rather than healthy individuals; while this controls for some pancreatic-related factors, differences in nutritional status (eg, Alb) between groups were noted, which itself is a driver of NTIS. Further prospective multicenter study with large sample could be necessary to provide the clinical rules for intervention on thyroid dysfunction in patients with AP.
Conclusions
In conclusion, thyroid dysfunction was commonly presented in the patients with AP, characterized by the decreased level of thyroid hormones and TSH. Lower serum Alb and higher Lac and hs-CRP were identified as independent risk factors of thyroid dysfunction. Preliminary follow-up data suggest that with AP recovering, thyroid dysfunction could spontaneously return to normal, though this observation needs confirmation in larger prospective studies. TSH could be a potential biomarker to predict the severity of AP in the early stage, demonstrating promising predictive value compared to traditional markers and severity scores. Future research should focus on validating TSH in diverse populations and investigating its utility in guiding early therapeutic decisions.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study is approved by the Scientific Ethics Committee of Beijing Friendship Hospital, Capital Medical University (Approval number: 2021-P2-432-01), which received the waiver for the informed consent. All methods were carried out in accordance with Declaration of Helsinki.
Acknowledgments
We would like to thank Dr. Jie Yin for her assistance during the initial phase of our research. This paper is available as a preprint on SSRN at: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4807010.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by grants from the Beijing Municipal Science and Technology Program (No.Z221100003522026).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Johnstone C, Hendry C, Farley A, McLafferty E. Endocrine system: part 1. Nurs Stand. 2014;28(38):42–11. doi:10.7748/ns.28.38.42.e7471
2. Mebis L, Van den Berghe G. Thyroid axis function and dysfunction in critical illness. Best Pract Res Clin Endocrinol Metab. 2011;25(5):745–757. doi:10.1016/j.beem.2011.03.002
3. Fliers E, Alkemade A, Wiersinga WM, Swaab DF. Hypothalamic thyroid hormone feedback in health and disease. Prog Brain Res. 2006;153:189–207. doi:10.1016/S0079-6123(06)53011-0
4. Fliers E, Bianco AC, Langouche L, Boelen A. Thyroid function in critically ill patients. Lancet Diabetes Endocrinol. 2015;3(10):816–825. doi:10.1016/S2213-8587(15)00225-9
5. Bello G, Ceaichisciuc I, Silva S, Antonelli M. The role of thyroid dysfunction in the critically ill: a review of the literature. Minerva Anestesiol. 2010;76(11):919–928.
6. Boxhoorn L, Voermans RP, Bouwense SA, et al. Acute pancreatitis. Lancet. 2020;396(10252):726–734. doi:10.1016/S0140-6736(20)31310-6
7. Lee PJ, Papachristou GI. New insights into acute pancreatitis. Nat Rev Gastroenterol Hepatol. 2019;16(8):479–496. doi:10.1038/s41575-019-0158-2
8. Greenberg JA, Hsu J, Bawazeer M, et al. Clinical practice guideline: management of acute pancreatitis. Can J Surg. 2016;59(2):128–140. doi:10.1503/cjs.015015
9. Wajner SM, Goemann IM, Bueno AL, Larsen PR, Maia AL. IL-6 promotes nonthyroidal illness syndrome by blocking thyroxine activation while promoting thyroid hormone inactivation in human cells. J Clin Invest. 2011;121(5):1834–1845. doi:10.1172/JCI44678
10. Croce L, Gangemi D, Ancona G, et al. The cytokine storm and thyroid hormone changes in COVID-19. J Endocrinol Invest. 2021;44(5):891–904. doi:10.1007/s40618-021-01506-7
11. Poth M, Tseng YC, Wartofsky L. Inhibition of TSH activation of human cultured thyroid cells by tumor necrosis factor: an explanation for decreased thyroid function in systemic illness? Thyroid. 1991;1(3):235–240. doi:10.1089/thy.1991.1.235
12. Pancreatic Surgery Group. Surgical Society of Chinese Medical Association, Guidelines for diagnosis and treatment of acute pancreatitis in China (2021). Chin J Sur. 2021;59(7):578–587. doi:10.3760/cma.j.cn112139-20210416-00172
13. Chronic Pancreatitis Group of Chinese Medical Doctor Association. Guidelines for the diagnosis and treatment of chronic pancreatitis in China (2018 edition). Hepatobiliary Pancreat Dis Int. 2019;18(2):103–109. doi:10.1016/j.hbpd.2019.02.004
14. Beltrão FEL, Beltrão DCA, Carvalhal G, et al. Thyroid Hormone Levels During Hospital Admission Inform Disease Severity and Mortality in COVID-19 Patients. Thyroid. 2021;31(11):1639–1649. doi:10.1089/thy.2021.0225
15. Padhi R, Kabi S, Panda BN, Jagati S. Prognostic significance of nonthyroidal illness syndrome in critically ill adult patients with sepsis. Int J Crit Illn Inj Sci. 2018;8(3):165–172. doi:10.4103/IJCIIS.IJCIIS_29_17
16. Schorr M, Miller KK. The endocrine manifestations of anorexia nervosa: mechanisms and management. Nat Rev Endocrinol. 2017;13(3):174–186. doi:10.1038/nrendo.2016.175
17. Wang B, Liu S, Li L, et al. Non-thyroidal illness syndrome in patients with cardiovascular diseases: a systematic review and meta-analysis. Int J Cardiol. 2017;226:1–10. doi:10.1016/j.ijcard.2016.10.039
18. Dong XF, Kong FZ, Shen MQ, et al. Triiodothyronine levels were positively correlated with opening of collateral circulation in cerebral infarction patients with large artery atherosclerosis. Arch Med Sci. 2019;16(1):51–57. doi:10.5114/aoms.2020.91286
19. Fliers E, Boelen A. An update on non-thyroidal illness syndrome. J Endocrinol Invest. 2021;44(8):1597–1607. doi:10.1007/s40618-020-01482-4
20. Bianco AC, Kim BW. Intracellular pathways of iodothyronine metabolism/implications of deiodination for thyorid hormone action. In: Werner and Ingbar’s the Thyroid: A Fundamental and Clinical Text. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:103–126.
21. Xu X, Pang Y, Fan X. Mitochondria in oxidative stress, inflammation and aging: from mechanisms to therapeutic advances. Signal Transduct Target Ther. 2025;10(1):190. doi:10.1038/s41392-025-02253-4
22. Boonen E, Van den Berghe G. Endocrine responses to critical illness: novel insights and therapeutic implications. J Clin Endocrinol Metab. 2014;99(5):1569–1582. doi:10.1210/jc.2013-4115
23. Boelen A, Kwakkel J, Fliers E. Beyond low plasma T3: local thyroid hormone metabolism during inflammation and infection. Endocr Rev. 2011;32(5):670–693. doi:10.1210/er.2011-0007
24. Eckart A, Struja T, Kutz A, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: a prospective study. Am J Med. 2020;133(6):713–722. doi:10.1016/j.amjmed.2019.10.031
25. Wiese ML, Perra T, Porcu A. Editorial: nutrition in pancreatic diseases: the role of nutritional status and nutrition therapy in the management of pancreatitis and pancreatic cancer. Front Nutr. 2026;12:1753147. doi:10.3389/fnut.2025.1753147
26. Bakker J, Postelnicu R, Mukherjee V. Lactate: where are we now? Crit Care Clin. 2020;36(1):115–124. doi:10.1016/j.ccc.2019.08.009
27. Peeters RP. Non thyroidal illness: to treat or not to treat? Ann Endocrinol. 2007;68(4):224. doi:10.1016/j.ando.2007.06.011
28. Lee S, Farwell AP. Euthyroid Sick Syndrome. Compr Physiol. 2016;6(2):1071–1080. doi:10.1002/cphy.c150017
29. Krysiak R, Kędzia A, Kowalcze K, Okopień B. Euthyroid sick syndrome: an important clinical problem. Wiad Lek. 2017;70:376–385.
30. Nistal-Nuño B. Euthyroid sick syndrome in pediatric and adult patients requiring extracorporeal circulatory support and the role of thyroid hormone supplementation: a review. Perfusion. 2021;36(1):21–33. doi:10.1177/0267659120914136
31. Everts ME, de Jong M, Lim CF, et al. Different regulation of thyroid hormone transport in liver and pituitary: its possible role in the maintenance of low T3 production during nonthyroidal illness and fasting in man. Thyroid. 1996;6(4):359–368. doi:10.1089/thy.1996.6.359
32. Langouche L, Vander Perre S, Marques M, et al. Impact of early nutrient restriction during critical illness on the nonthyroidal illness syndrome and its relation with outcome: a randomized, controlled clinical study. J Clin Endocrinol Metab. 2013;98(3):1006–1013. doi:10.1210/jc.2012-2809
33. Lado-Abeal J, Diaz C, Berdine G, et al. High prevalence of non-thyroidal illness syndrome in patients at long-term care facilities. Endocrine. 2020;70(2):348–355. doi:10.1007/s12020-020-02321-5
34. Liu H, Yan W, Xu G. Thyroid hormone replacement for nephrotic syndrome patients with euthyroid sick syndrome: a meta-analysis. Ren Fail. 2014;36(9):1360–1365. doi:10.3109/0886022X.2014.949559
35. Meher S, Mishra TS, Sasmal PK, et al. Role of biomarkers in diagnosis and prognostic evaluation of acute pancreatitis. J Biomark. 2015;519534. doi:10.1155/2015/519534
36. Venkatesh NR, Vijayakumar C, Balasubramaniyan G, et al. Comparison of different scoring systems in predicting the severity of acute pancreatitis: a prospective observational study. Cureus. 2020;12(2):e6943. doi:10.7759/cureus.6943
37. Haja A, Rizwan BM, Michael J, Babu AJ, Varghese AM, Berlin SV. Assessment of Thyroid hormone status among patients with chronic kidney disease in a tertiary care center: a cross-sectional study. Cureus. 2025;17(12):e99501. doi:10.7759/cureus.99501
38. Mahashabde ML, Kumar L, Bhimani YR, Reddy SK, Nitendra Saketh BV, Gharge SS. A critical investigation of sick euthyroid syndrome in chronic heart failure patients: addressing the need for accurate thyroid assessment. Cureus. 2024;16(8):e65985. doi:10.7759/cureus.65985
39. Yang N, Zhang DL, Hao JY, Wang G. Serum levels of thyroid hormones and thyroid stimulating hormone in patients with biliogenic and hyperlipidaemic acute pancreatitis: difference and value in predicting disease severity. J Int Med Res. 2016;44(2):267–277. doi:10.1177/0300060515618052
40. Yang WQ, Yang Q, Chen WJ, et al. Low FT3 is a valuable predictor of severe acute pancreatitis in the emergency department. J Dig Dis. 2018;19(7):431–438. doi:10.1111/1751-2980.12609
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.