")
Back to Journals » Psychology Research and Behavior Management » Volume 17
Risk Factors of Perinatal Negative Mood and Its Influence on Prognosis: A Retrospective Cohort Study
Authors Yang Z, Shao C, Tang C
Received 26 November 2023
Accepted for publication 21 February 2024
Published 1 March 2024 Volume 2024:17 Pages 853—865
DOI https://doi.org/10.2147/PRBM.S451843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Zheng Yang, Cuixiang Shao, Chen Tang
Department of Obstetrics, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China
Correspondence: Chen Tang, Department of Obstetrics, Affiliated Hospital of Jiangnan University, No. 1000, Hefeng Road, Wuxi, 214122, People’s Republic of China, Email [email protected]
Background: Maternal anxiety or depression in the perinatal period has a high prevalence. The negative emotion during the puerpera is unfavorable to the process of childbirth and also affects the recovery and the quality of life in postpartum patients significantly. The present study aimed to elucidate the risk factors of negative emotion in perinatal women and its influence on prognosis to provide a reference for improving maternal prognosis.
Methods: Initially, 350 expectant mothers were randomly enrolled in the present study between August 2021 and August 2022. Among these, after applying the established inclusion and exclusion criteria, 314 patients were eventually selected. The independent risk factors of negative emotion and poor prognosis were analyzed through binary logistics regression and multiple linear regression. Follow-up was conducted via telephone, email, and a follow-up visit one month after discharge.
Results: Among the included patients, 18 (5.7%) had prenatal anxiety, 16 (5.1%) had prenatal depression, 31 (9.9%) had postnatal anxiety, and 28 (8.9%) had postnatal depression. Perinatal negative emotional risk factors include age, marital relationship, regular prenatal examination, E2 level, 5-HT level before and after delivery, family monthly income, neonatal health, breastfeeding time, intrapartum hemorrhage, constipation and other complications. The development of postpartum negative emotions is a risk factor for maternal prognosis.
Conclusion: The results showed that the risk factors of perinatal depression and anxiety were complex. In order to improve the quality of life of pregnant women, maintain their long-term emotional stability, and promote their postpartum recovery, it may be considered to promote the use of screening tools to identify women at risk of anxiety and depression before and after delivery, and timely psychological counseling for patients with high risk factors to promote their mental health.
Keywords: anxiety, depression, puerpera, perinatal period, negative emotions
Introduction
Childbirth is a normal physiological phenomenon. However, due to the complex physiology associated with childbirth, most women experience great concerns and worry regarding the health of the fetus throughout pregnancy. In addition, changes in the hormonal levels in pregnant women often contribute further to negative emotions, such as tension and anxiety.1,2 The advancements in medical technologies have enabled a deeper understanding of people’s mental health while pursuing physical health. Decades of research in the fields of psychiatry and related disciplines have been invested in the symptoms of anxiety and depression experienced by women during pregnancy and in the postpartum period.3 With prevalence rates as high as 13%4,5 and 8–11%6 for postpartum depression and anxiety, respectively, these symptoms are considered normal in postpartum women. However, while anxiety and depression assist in improving the adaptability of the mother’s body to the childbirth and postpartum environment by increasing the activity of her sympathetic nervous system, these symptoms also exert negative effects on the body.7 Depression and its consequences may have a lasting impact on the mother, including limitations of physical and psychological functioning, while also adversely affecting the growth of the newborn. Anxiety may have similar consequences on the overall health and functioning of the mother, thereby increasing the stress levels associated with the concern of postpartum childcare.8
Negative emotions such as anxiety and depression in mothers during pregnancy may have several underlying causes. The influence of hormonal changes occurring in the body after delivery and changes in the physical, psychological, family, and social relationships during pregnancy and the postpartum period are reported as the main reasons for a series of mental health problems often experienced by new mothers.9–11 Pregnancy brings with it several changes in the physiological functioning of the mother’s body, along with certain psychological disturbances, which may have several adverse consequences.12 For instance, the quality of sleep is relatively poor in women with a combination of negative emotions. This is particularly common for first-time mothers.9 Saxbe et al13 used structural equation modeling to assess whether sleep quality played a mediatory role in the relationship between depressive symptoms measured at 1 month postpartum and those measured at 6 and 12 months postpartum. The authors observed that poor sleep quality was strongly associated with depressive symptoms at 6 and 12 months postpartum. In addition, negative emotions may lead to endocrine disorders, which involve disturbed secretion of several important hormones, such as contraction-related, lactogen, and adrenal hormones, which could, in turn, affect neonatal feeding, be detrimental to neonatal growth and even lead to complications such as increased postpartum hemorrhage.14,15 Recently, it was reported that most cases of maternal postpartum depression do not originate during pregnancy and rather much earlier.16 Therefore, it is crucial that the medical and nursing staff increase their efforts to educate family members of the mother-to-be regarding mental health knowledge, both during pregnancy and in the earlier preparatory period, to improve the level of understanding and obtain adequate cooperation of the family. Meanwhile, professional psychologists screen mothers with adverse emotions and provide them with psychological interventions to help them solve their psychological problems, give full play to the social support system, and encourage the patients to seek help at the right time for an effective resolution to their emotional problems, which would consequently reduce the adverse outcomes among affected mothers.17 Angarath et al18 found that high educational level, history of depression, preterm birth, negative experiences during delivery and the first week after delivery, and excessive infant crying were factors associated with high risk of postpartum anxiety. Biaggi et al19 showed that the factors most associated with prenatal depression or anxiety were: lack of partner or social support; A history of abuse or domestic violence; Personal history of mental illness; Accidental or unwanted pregnancy; Adverse life events and high perceived stress; Current/past pregnancy complications, etc. However, few studies have conducted continuous monitoring and comparative analysis of maternal anxiety and depression factors before and after delivery. Therefore, the present study aimed to determine the risk factors of negative perinatal maternal mood and its relationship with poor prognosis to provide a reference for reducing the occurrence of postpartum depression-related complications and improving the prognosis, thereby improving the quality of life of the mother after delivery.
Materials and Methods
Research Participants
A total of 314 maternal cases, who were admitted to the Affiliated Hospital of Jiangnan University between August 2021 and August 2022, were included in the present study.
The inclusion criteria were as follows: (I) gestational week ≥ 39 weeks; (II) age 22–39 years; (III) no history of depression or psychiatric disorders (determined by the patient’s past medical history); (IV) consciousness and normal communication skills; (V) complete clinical case information and informed consent from the mothers and their respective families.
The exclusion criteria were as follows: (I) combined malignant neoplastic disease; (II) history of psychiatric disease or cognitive impairment; (III) significant organ dysfunction; (IV) history of substance abuse; (V) incomplete clinical case information or failure to obtain informed consent from the mother or her family (Figure 1).
 |
Figure 1 Flow chart of patient selection. |
According to our previous study and studies published by other researchers, the prevalence of negative maternal perinatal emotions is about 15%. In this study, we set a tolerance error of 5% and a confidence level of 1-α = 0.95, and used PASS 15 software to calculate the sample size of 215 cases to be investigated. Assuming a patient nonresponse rate of 10%, the required sample size was 239 cases (N = 215 ÷ 0.9). Assuming a 90% questionnaire pass rate, the total sample size required was 266 cases (N = 239 ÷ 0.9). As a general rule of binary logistic regression, the ratio of items to sample size must be in the range of 1:5~1:10. Therefore, a sample size of 350 cases was selected initially for the present study. After applying the exclusion criteria and a few cases lost during the follow-ups, 314 cases were finally included in the present study.
The study was approved by the Ethics Committee of the Affiliated Hospital of Jiangnan University (approval no. LCKY2021352). All patients or their families participating in the study signed an informed consent form.
General Information Questionnaire
The general information questionnaire included demographic data [gender, age, BMI (body mass index), family residence, monthly family income, education level, and couple relationship] and clinical data [presence of hypertension, diabetes, mode of delivery, number of births, breastfeeding pattern, whether the newborn was healthy, whether regular births occurred, whether scoliosis occurred, the quality of sleep during pregnancy, and some serological indicators]. Basic information is collected upon admission.
Negative Emotion Assessment
All patients completed the Self-Rating Anxiety Scale (SAS)20 upon admission. The SAS was adopted to reflect the existence and the degree of anxiety. The scale comprised 20 items; each scored from 1 to 4. The scores for each item were summed to obtain a crude score, which was then multiplied by 1.25 to obtain the standard score. The evaluation criteria were as follows: the SAS score of <50 for no anxiety, 50–59 for mild anxiety, 60–69 for moderate anxiety, and 70 and above for severe anxiety. The scale has good reliability and validity, with a Cronbach’s α coefficient of above 0.75.
All patients completed the Self-Rating Depression Scale (SDS)20 at 7 days postpartum. The SDS was adopted to reflect the existence and the degree of depression. The scale comprised 20 items. An SDS score of >52 was used as the evaluation criterion. An SDS score of ≥53 was classified as depression, 53–62 as mild depression, 63–72 as moderate depression, and >72 as severe depression. The SDS has good reliability and validity, with a Cronbach’s α coefficient of above 0.75.
Based on SAS and SDS scores, patients were considered to be in the negative mood group if they presented with either or both anxiety or depressive symptoms. They were evaluated at admission and 1 week postpartum.
Serological Index Determination
All patients underwent intravenous blood collection at the last antenatal examination and 5 days after delivery. A good rest is ensured the day before the serological examination, and blood is usually taken intravenically when the patient is fasting in the morning. Serological indicators include: Estradiol (E2); Prolactin (PRL); Progesterone (P); 5-hydroxytryptamine (5-HT).
SF-36 Score
The 36-Item Short Form Health Survey (SF-36) is a popular questionnaire that measures the self-perceptions of the quality of life in a specific population. SF-36 comprises 36 questions on the following 8 dimensions: physical functioning (10 questions), role-physical (4 questions), body pain (3 questions), general health (5 questions), vitality (4 questions), social functioning (2 questions), role-emotional (3 questions), and mental health (5 questions). In addition, the questionnaire includes 2 summary scores – physical component summary (PCS) and mental component summary (MCS), representing the physical and mental components, respectively. Each dimension is scored on a scale range of 0 to 100, with higher scores indicating a higher quality of life.21
Evaluation was performed at 1 month postpartum. The last follow-up visit occurred in September 2022.
Statistical Analysis
The score results of each scale were input into a computer for score conversion, and statistical analysis was performed using SPSS 26 (IBM SPSS, USA). All measured data were expressed as mean and standard deviation, while the count data were expressed as frequencies and percentages. Statistical analysis between groups was performed using a t-test and chi-squared test. Based on SAS and SDS scores, patients were considered to be in the negative mood group if they experienced one or both of the anxiety or depressive symptoms, and the rest of the patients were categorized as being in the no-negative-mood group. Subsequently, indicators that differed in the univariate analysis were analyzed by including them in a multifactorial binary logistic regression in order to derive the factors influencing the occurrence of maternal negative emotions. Factors affecting prognosis were analyzed by multiple linear regression based on the SF-36 total score. A two-sided P < 0.05 was considered the threshold of statistical significance.
Results
Differential Analysis of SAS and SDS Scores and Prenatal and Postnatal Correlates
The results of the t-test revealed a significant difference (P < 0.05) in the prenatal SAS scores among the couple relationship, diabetes, hypertension, and sleep quality. The SAS score was 41.97±6.07 in 241 cases (76.8%) with a good couple relationship, 44.44 ±7.13 in 39 cases (12.4%) with diabetes, 45.00 ±8.18 in 24 cases (7.6%) with hypertension, and 43.32 ±6.57 in 146 cases (46.5%) with poor sleep quality. A significant difference in prenatal SDS was observed among age, number of births, and the presence of regular obstetric examinations (P < 0.05). A total of 141 patients (44.9%) were aged ≥30 years, with an SDS score of 46.38 ±6.16, while 162 patients (51.6%) were primiparous, with an SDS score of 46.07 ±6.39. A total of 28 patients (8.9%) who did not undergo regular maternity examinations had an SDS score of 49.64 ±6.88 (Table 1).
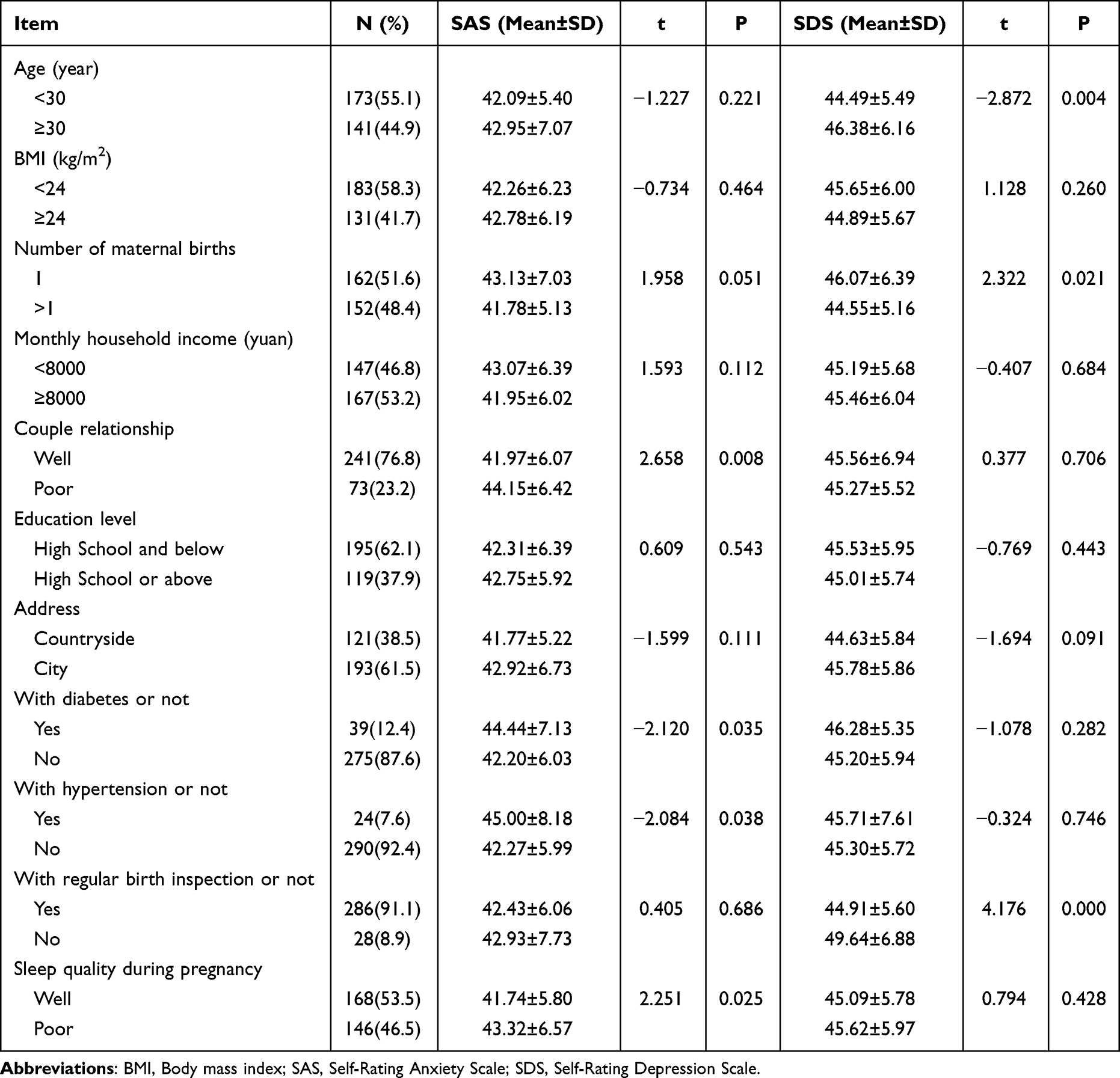 |
Table 1 SAS and SDS Scores in Patients Before Delivery |
The results of the t-test also revealed significant differences in both postpartum SAS and SDS scores among the monthly family income, mode of delivery, and whether the newborn was healthy (P < 0.05). A total of 147 patients (46.8%) had a monthly household income of <8000, with SAS and SDS scores of 44.07 ±8.20 and 46.36 ±6.94, respectively. Only 32 patients (10.2%) underwent a cesarean section, with SAS and SDS scores of 45.72 ±10.74 and 48.09 ±7.96, respectively, while just 65 patients (20.7%) had unhealthy newborns. In addition, the maternal SAS score was 42.07 ±6.83 for those aged <30 years, which was significantly different (P < 0.05) from the SAS score of those aged ≥30 years (Table 2).
 |
Table 2 SAS and SDS Scores in Patients After Delivery |
Serological Indicators of the Patients Prior to and After Delivery
The results of the t-test revealed that only E2 and 5-HT were significantly different (P < 0.05) between the patients with and without negative emotions prior to delivery. In the prenatal negative mood group, the mean Estradiol (E2) was 22.19 ±5.55 pmol/mL, while the mean 5-hydroxytryptamine (5-HT) level was 311.71 ±6.49 ng/L. In the prenatal without negative mood group, the mean E2 was 24.44 ±5.15 pmol/mL, and the mean 5-HT was 315.38 ±7.39 ng/L. In the postnatal period, the levels of E2, Prolactin (PRL), and 5- HT differed significantly between the two groups (P < 0.05). In the postpartum negative mood group, the levels of E2, PRL, and 5-HT were 19.61 ±4.37 pmol/mL, 172.78 ±21.33 ng/mL, and 380.96 ±13.05 ng/L, respectively. In the postpartum uncomplicated negative mood group, the levels of E2, PRL, and 5-HT were 21.21 ±4.84 pmol/mL, 182.85 ±18.40 ng/mL, and 385.21 ±10.54 ng/L, respectively (Table 3).
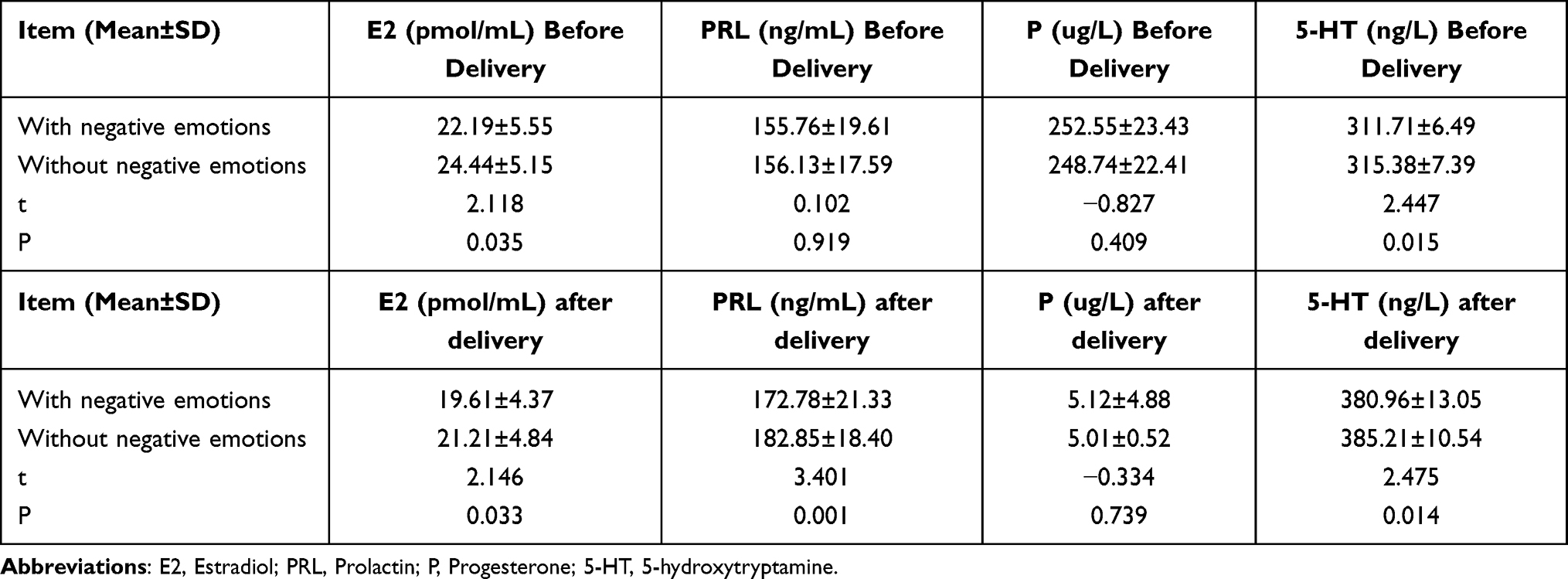 |
Table 3 Serological Indicators of the Patients Before and After Delivery |
Perinatal Index of the Patients with or Without Negative Emotions After Delivery
The results of the t-test revealed that among the perinatal indicators, the first stage of labor, the amount of bleeding during delivery, and the time to breastfeeding differed significantly between the patients with and without negative emotions in the postpartum period (P < 0.05). In the postpartum negative emotions group, the values for the first stage of labor, amount of bleeding during delivery, and time to breastfeeding were 385.08 ±74.31 min, 332.29 ±47.82 mL, and 2.21 ±0.77 d, respectively. In the postpartum without negative emotions group, the values of the first stage of labor, bleeding during delivery, and time to breastfeeding were 351.80 ±67.52 min, 306.74 ±43.76 mL, and 1.82 ±0.82 d, respectively, which were significantly lower than those in the postpartum negative emotion group (Table 4).
 |
Table 4 Perinatal Index of Patients with or Without Negative Emotions After Delivery |
Complications in Patients with or Without Negative Emotions After Delivery
The results of the chi-squared test revealed that among the postpartum complications, only urinary retention and constipation differed significantly (P < 0.05) between patients with and without negative postpartum mood. In the negative postpartum mood group, 6 patients (12.5%) had urinary retention, and 7 patients (14.6%) had constipation, while the corresponding numbers were 6 patients (2.3%) with urinary retention and 12 patients (4.5%) with constipation in the group without negative postpartum mood (Table 5).
 |
Table 5 Complications of Patients with or Without Negative Emotions After Delivery |
Binary Logistic Regression Analysis of the Prenatal and Postpartum Negative Emotions of Patients
The binary logistic regression analysis revealed patients’ age, couple relationship, whether regular maternity examinations were conducted, and prenatal E2 and 5-HT levels as risk factors of negative mood in patients prior to delivery (P < 0.05) (Table 6, Figure 2A). Patients’ age, monthly household income, whether the newborn was healthy, postpartum PRL and 5-HT levels, amount of bleeding during delivery, time to breastfeeding, and the presence of complications, such as constipation, were revealed as risk factors of negative emotions (P < 0.05) after delivery (Table 7, Figure 2B).
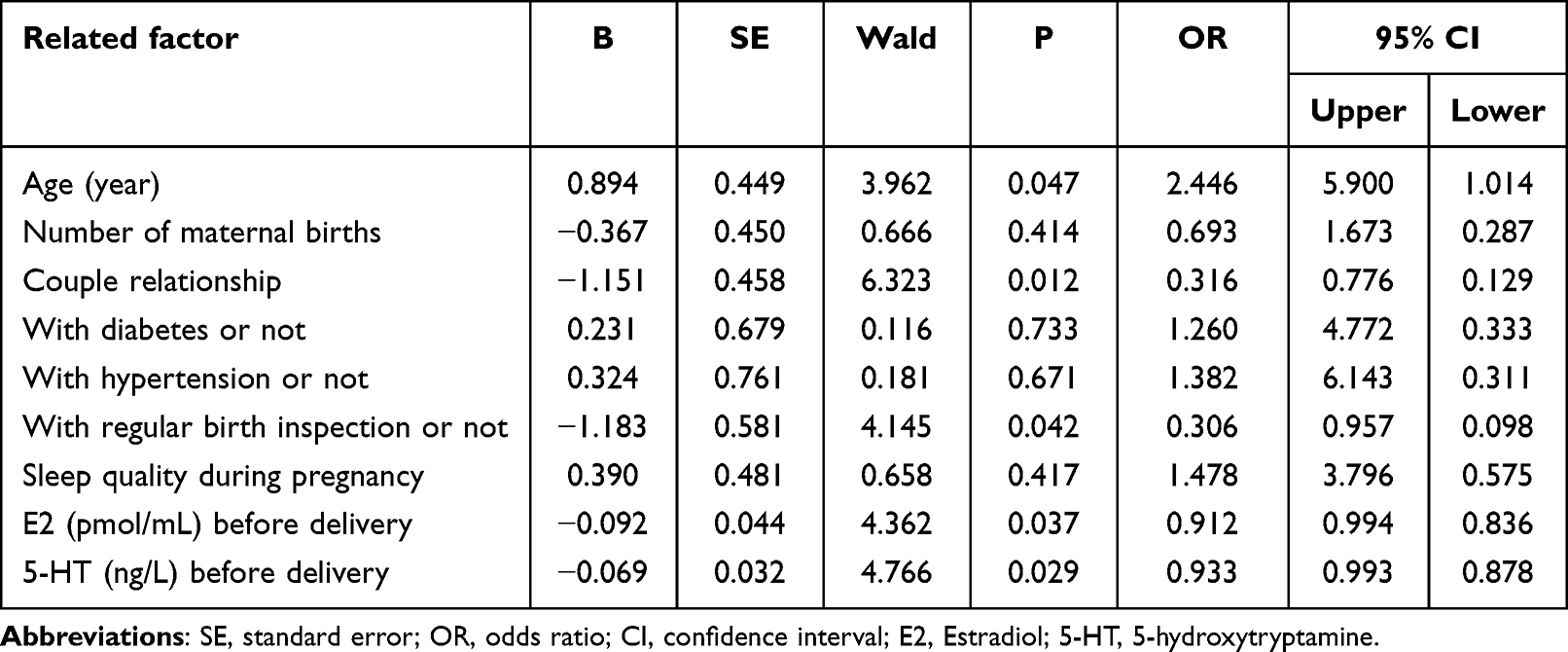 |
Table 6 Binary Logistic Regression Analysis of Patients’ Prenatal Negative Emotion |
 |
Table 7 Binary Logistic Regression Analysis of Patients’ Postpartum Negative Emotion |
 |
Figure 2 Binary logistic regression analysis of patients’ negative emotion (A) Binary logistic regression analysis of patients’ prenatal negative emotion; (B) Binary logistic regression analysis of patients’ postpartum negative emotion. |
SF-36 Score at 1 Month After Delivery in Patients Belonging to the Two Groups
In the SF-36 score analysis, all domains except for vitality scores were revealed to differ significantly (P < 0.05) between the patients with and without postpartum negative emotions. In the negative postpartum mood group, the scores for social functioning, role-emotional, mental health, general health, physical functioning, role-physical, and body pain were 70.98 ±4.25, 61.17 ±4.64, 60.90 ±5.28, 71.04 ±4.45, 73.63 ±5.38, 63.69 ±6.73, and 60.83 ±3.79, respectively, while the total score was 526.88 ±13.35. In the non-negative mood group, the scores for the above domains were 73.92 ±7.10, 64.27 ±5.69, 64.64 ±5.48, 73.53 ±6.31, 77.92 ±6.52, 66.04 ±7.29, and 64.35 ±5.81, respectively, while the total score was 550.25 ±21.24 (Table 8).
 |
Table 8 SF-36 Score at 1 Months After Delivery in Patients in Two Groups |
Multiple Linear Regression Analysis of the SF-36 Scores
The multiple linear regression analysis revealed negative postpartum emotions, age, place of residence, presence of gestational hypertension, mode of delivery, whether the newborn was healthy, whether with a perineal lateral incision, amount of bleeding during delivery, intestinal obstruction, and postoperative bleeding as independent risk factors (Table 9) affecting maternal postoperative prognosis (P < 0.05).
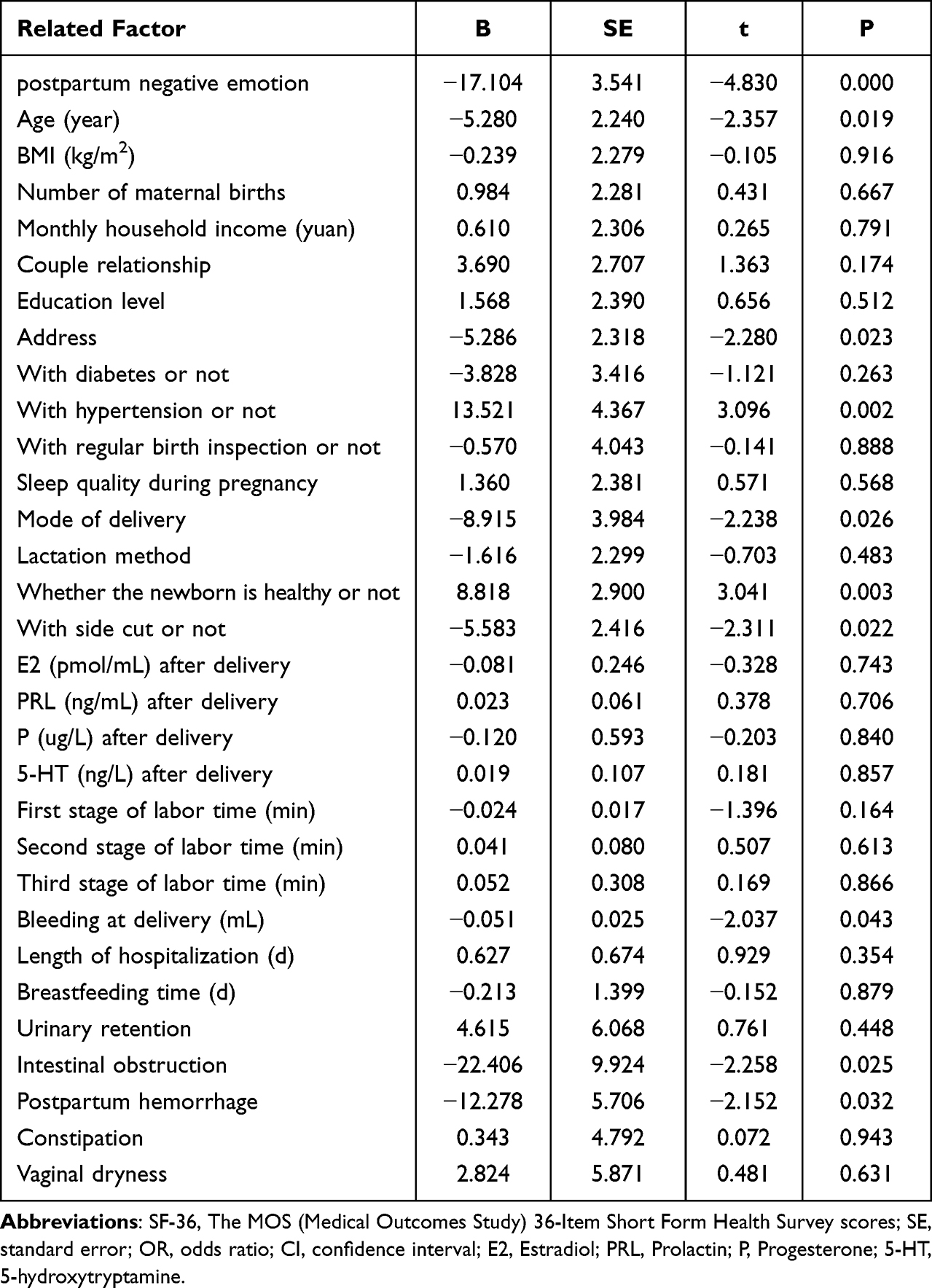 |
Table 9 Multiple Linear Regression Analysis ofSF-36 Score |
Discussion
The Current State of the Psychological Situation of Women in Labor and Its Causes
Maternal psychological conditions are of great concern in the current times.22 Epidemiological studies have demonstrated that the prevalence of antenatal anxiety and depression varies greatly from country to country. In developed nations, the prevalence of antenatal depression among pregnant women ranges from 7% to 20%, while in developing nations, it generally exceeds 20%.23 The incidence of postpartum depression has been exhibiting a certain upward trend. Currently, the incidence of postpartum depression in China is expected to reach approximately 272~483 cases per 10,000 mothers.24 The results of the present study revealed that the patient’s age, couple relationship, whether regular maternity visits were conducted, and prenatal E2 and 5-HT levels were the main risk factors of negative preoperative mood in mothers. In the case of advanced maternal age, a combined ossification of the sciatic, pubic, and skeletal bones occurs. In comparison to women of proper age, women with advanced age have worse organism status, greater comorbidities and complications during pregnancy, and a higher risk of miscarriage and postpartum hemorrhage. In addition, women of advanced age are under greater pressure from family, work, and society at large. Consequently, advanced maternal age was associated with a greater probability of experiencing negative emotions, such as anxiety and depression. According to a previous study,25 a good family environment may significantly suppress maternal dysphoria. The factors associated with the family environment, such as emotional expression and intimacy, play a protective role against maternal anxiety and depression, while a family environment with ambivalence may promote maternal anxiety and depression, which could then become chronic and persistent.26 The present study also revealed that patients’ age, monthly household income, the health of the newborn, postoperative PRL and 5-HT levels, intrapartum bleeding, time to breastfeeding, and complications such as constipation were the risk factors of negative emotions in the postpartum period. PRL, a protein hormone secreted by the anterior pituitary gland eosinophils and composed of 199 amino acid residues, regulates maternal lactation,27 maintains neuronal excitability and nerve nourishment, and also reduces the incidence of sleep disorders. According to a study,28 the peak secretion of lactogen occurs after 1 h of maternal sleep, and a high secretion level is maintained during sleep. However, maternal sleep quality and sleep duration reportedly decrease in women with anxiety and depression. Postpartum mothers are more psychologically dependent on their newborns, and lactation helps maintain the relationship between the mothers and the newborns while also enhancing the sense of responsibility and pride in the mother. Consequently, low prolactin levels and prolonged postoperative lactation time increases maternal anxiety and psychological burden. The metabolic levels of 5-HT are evidently associated with postpartum depression, as a decrease in these levels affects the degree of neuroelectrical excitation in the cerebral cortex, leading to the formation of inhibitory postsynaptic potentials and promoting the development of depression.29 Increasing evidence suggests that the onset of maternal anxiety and depression is associated with a combination of physiological, psychological, social, and cultural factors.3,30 Researchers should, therefore, be more attuned to the actual environment in which mothers dwell and consider the multiple influences they might be experiencing. Accordingly, certain less-measurable subtle variables, such as cultural factors, should not be ignored. Clinical workers should also identify maternal mental health problems by analyzing the status of the mother and accordingly implement targeted interventions to provide the necessary psychological care and moral.
The Relationship Between the Development of Negative Maternal Emotions and Prognosis
It is reported that negative emotions such as anxiety or depression during the perinatal period may lead to various adverse effects on maternal and fetal health, including immediate effects, such as preterm delivery, gradual growth, maternal postpartum depression, and postpartum complications,3,31 as well as long term effects, such as adverse impacts on offspring brain development and maternal prognosis.32 The present study revealed that negative postpartum emotions significantly affect maternal prognosis, which is consistent with the above-stated findings. Therefore, it is recommended that during pregnancy, mothers should be provided with complete care, an efficient and caring medical and nursing staff, a good doctor–patient relationship, and communication with a good attitude. After childbirth, complete care must be ensured for the mother as well as the newborn. In addition, changes in maternal psychology and emotions must be monitored during pregnancy as well as after childbirth, and accordingly, timely psychological guidance and intervention must be provided to ensure that the mother feels cared for with adequate warmth and kindness. It must be ensured that the mother remains in a good mood until and during delivery to reduce the incidence of negative emotions postpartum and also improve the prognosis of the mother afterward. The present study also revealed that the mode of delivery, whether gestational hypertension occurred, whether lateralization occurred, the amount of bleeding during delivery, intestinal obstruction, and postpartum hemorrhage were independent risk factors affecting the maternal postoperative prognosis. In recent decades, the rate of cesarean delivery has increased worldwide and is estimated to be 32% in the United States, 32% in Oceania, 40% in Latin America, and 25% in Europe.33 Cesarean section is the most common means used clinically to resolve obstructed labor and other obstetric syndromes to effectively reduce maternal and perinatal mortality. However, it may also cause different degrees of damage to the maternal body and is often accompanied by postoperative complications, such as postoperative bleeding, increased pain after anesthesia, and incisional infection, which affects the recovery of the mother’s body and may also endanger her life in critical cases.34 Hypertension during pregnancy increases the risk of obstetric adverse events, such as preterm delivery, intrauterine growth retardation, and even death, while also rendering the mother more prone to acute kidney injury.35 Currently, weak contractions are the main cause of postpartum hemorrhage.36 According to studies,37 postpartum hemorrhage may lead to hypopituitarism, which may seriously affect the quality of life of the mother after delivery. Another study38 reported that the emotional state of the mother prior to delivery could affect the amount of postpartum bleeding. With deeper levels of maternal anxiety and depression, the bleeding volume during delivery also increases. Therefore, in addition to caring for maternal mood during delivery, prenatal emotional interventions should also be conducted for the mother to reduce the impact of adverse emotions on maternal prognosis.
Summary
In conclusion, several risk factors lead to the development of negative maternal mood in the perinatal period, and timely and accurate assessment of the mental and emotional state of the mother in the perinatal period is, therefore, crucial. Active identification of the influencing factors leading to maternal anxiety and depression and the implementation of appropriate interventions to reduce the incidence of postpartum depression are key to promoting good postpartum recovery and constructing a harmonious family environment for primiparous women.
Limitations
As with all research, the present study also had certain limitations. For instance, due to limited manpower and time, fewer cases were included in the analysis. In addition, the follow-up period was short just one year. Therefore, studies with a greater study population and a longer follow-up period are warranted.
Conclusion
The results showed that the risk factors of perinatal depression and anxiety were complex. In order to improve the quality of life of pregnant women, maintain their long-term emotional stability, and promote their postpartum recovery, it may be considered to promote the use of screening tools to identify women at risk of anxiety and depression before and after delivery, and timely psychological counseling for patients with high risk factors to promote their mental health.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by Ethics Committee of Affiliated Hospital of Jiangnan University (No. LCKY2021352) and informed consent was taken from all the patients.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Pawluski JL, Lonstein JS, Fleming AS. The neurobiology of postpartum anxiety and depression. Trends Neurosci. 2017;40(2):106–120. doi:10.1016/j.tins.2016.11.009
2. Smith CA, Shewamene Z, Galbally M, et al. The effect of complementary medicines and therapies on maternal anxiety and depression in pregnancy: a systematic review and meta-analysis. J Affect Disord. 2019;245:428–439. doi:10.1016/j.jad.2018.11.054
3. Dunkel Schetter C, Tanner L. Anxiety, depression and stress in pregnancy: implications for mothers, children, research, and practice. Curr Opin Psychiatry. 2012;25(2):141–148. doi:10.1097/YCO.0b013e3283503680
4. Gavin NI, Gaynes BN, Lohr KN, et al. Perinatal depression: a systematic review of prevalence and incidence. Obstet Gynecol. 2005;106(5, Part 1):1071–1083. doi:10.1097/01.AOG.0000183597.31630.db
5. Wisner KL, Chambers C, Sit DK. Postpartum depression: a major public health problem. JAMA. 2006;296(21):2616–2618. doi:10.1001/jama.296.21.2616
6. Misri S, Swift E. Generalized Anxiety disorder and major depressive disorder in pregnant and postpartum women: maternal quality of life and treatment outcomes. J Obstet Gynaecol Can. 2015;37(9):798–803. doi:10.1016/S1701-2163(15)30150-X
7. Stützer PP, Berlit S, Lis S, et al. Elective caesarean section on maternal request in Germany: factors affecting decision making concerning mode of delivery. Arch Gynecol Obstet. 2017;295(5):1151–1156. doi:10.1007/s00404-017-4349-1
8. Misri S, Kendrick K, Oberlander TF, et al. Antenatal depression and anxiety affect postpartum parenting stress: a longitudinal, prospective study. Can J Psychiatry. 2010;55(4):222–228. doi:10.1177/070674371005500405
9. Uvnäs Moberg K, Ekström-Bergström A, Buckley S, et al. Maternal plasma levels of oxytocin during breastfeeding-A systematic review. PLoS One. 2020;15(8):e0235806. doi:10.1371/journal.pone.0235806
10. Dagher RK, Bruckheim HE, Colpe LJ, et al. Perinatal Depression: challenges and opportunities. J Womens Health. 2021;30(2):154–159. doi:10.1089/jwh.2020.8862
11. Suryawanshi O, Pajai S. A comprehensive review on postpartum depression. Cureus. 2022;14:e32745.
12. Okun ML, Mancuso RA, Hobel CJ, et al. Poor sleep quality increases symptoms of depression and anxiety in postpartum women. J Behav Med. 2018;41(5):703–710. doi:10.1007/s10865-018-9950-7
13. Saxbe DE, Schetter CD, Guardino CM, et al. Sleep quality predicts persistence of parental postpartum depressive symptoms and transmission of depressive symptoms from mothers to fathers. Ann Behav Med. 2016;50(6):862–875. doi:10.1007/s12160-016-9815-7
14. Walter MH, Abele H, Plappert CF. The role of oxytocin and the effect of stress during childbirth: neurobiological basics and implications for mother and child. Front Endocrinol. 2021;12:742236. doi:10.3389/fendo.2021.742236
15. Blair C, Granger D, Willoughby M, et al. Maternal sensitivity is related to hypothalamic-pituitary-adrenal axis stress reactivity and regulation in response to emotion challenge in 6-month-old infants. Ann N Y Acad Sci. 2006;1094(1):263–267. doi:10.1196/annals.1376.031
16. Patton GC, Romaniuk H, Spry E, et al. Prediction of perinatal depression from adolescence and before conception (VIHCS): 20-year prospective cohort study. Lancet. 2015;386(9996):875–883. doi:10.1016/S0140-6736(14)62248-0
17. Bleker LS, Milgrom J, Parker D, et al. Brain magnetic resonance imaging findings in children after antenatal maternal depression treatment, a longitudinal study built on a pilot randomized controlled trial. Int J Environ Res Public Health. 2019;16(10):1816. doi:10.3390/ijerph16101816
18. Van der Zee-van den Berg Angarath I, Boere-Boonekamp Magda M, Groothuis-Oudshoorn Catharina GM, et al. Postpartum depression and anxiety: a community-based study on risk factors before, during and after pregnancy. J Affective Disorders. 2021;286:158–165. doi:10.1016/j.jad.2021.02.062
19. Biaggi A, Conroy S, Pawlby S, et al. Identifying the women at risk of antenatal anxiety and depression: a systematic review. J Affective Disorders. 2015;191:62–77. doi:10.1016/j.jad.2015.11.014
20. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
21. Açma A, Carrat F, Hejblum G. Comparing SF-36 scores collected through web-based questionnaire self-completions and telephone interviews: an ancillary study of the SENTIPAT multicenter randomized controlled trial. J Med Internet Res. 2022;24:e29009.
22. Liu X, Wang S, Wang G. Prevalence and risk factors of postpartum depression in women: a systematic review and meta-analysis. J Clin Nurs. 2022;31(19–20):2665–2677. doi:10.1111/jocn.16121
23. Gelaye B, Rondon MB, Araya R, et al. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry. 2016;3(10):973–982. doi:10.1016/S2215-0366(16)30284-X
24. Thombs BD, Arthurs E, Coronado-Montoya S, et al. Depression screening and patient outcomes in pregnancy or postpartum: a systematic review. J Psychosom Res. 2014;76(6):433–446. doi:10.1016/j.jpsychores.2014.01.006
25. Garay SM, Savory KA, Sumption LA, et al. Seasonal variation in salivary cortisol but not symptoms of depression and trait anxiety in pregnant women undergoing an elective caesarean section. Psychoneuroendocrinology. 2019;108:14–19. doi:10.1016/j.psyneuen.2019.05.029
26. Dayi A, Kiray M, Sisman A, et al. Dose dependent effects of oxytocin on cognitive defects and anxiety disorders in adult rats following acute infantile maternal deprivation stress. Biotech Histochem. 2019;94(7):469–480. doi:10.1080/10520295.2018.1528384
27. Rana M, Jain S, Choubey P. Prolactin and its significance in the placenta. Hormones. 2022;21(2):209–219. doi:10.1007/s42000-022-00373-y
28. McLeod G, Sherriff J, Hartmann PE, et al. Comparing different methods of human breast milk fortification using measured v. assumed macronutrient composition to target reference growth: a randomised controlled trial. Br J Nutr. 2016;115(3):431–439. doi:10.1017/S0007114515004614
29. Popova NK, Tsybko AS, Naumenko VS. The Implication of 5-HT receptor family members in aggression, depression and suicide: similarity and difference. Int J Mol Sci. 2022;23(15):8814. doi:10.3390/ijms23158814
30. Yatziv T, Vancor EA, Bunderson M, Rutherford HJV. Maternal perinatal anxiety and neural responding to infant affective signals: insights, challenges, and a road map for neuroimaging research. Neurosci Biobehav Rev. 2021;131:387–399. doi:10.1016/j.neubiorev.2021.09.043
31. Norhayati MN, Hazlina NH, Asrenee AR, et al. Magnitude and risk factors for postpartum symptoms: a literature review. J Affect Disord. 2015;175:34–52. doi:10.1016/j.jad.2014.12.041
32. Van den Bergh BR, Mennes M, Oosterlaan J, et al. High antenatal maternal anxiety is related to impulsivity during performance on cognitive tasks in 14- and 15-year-olds. Neurosci Biobehav Rev. 2005;29(2):259–269. doi:10.1016/j.neubiorev.2004.10.010
33. Sorrentino F, Greco F, Palieri T, et al. Caesarean section on maternal request-ethical and juridic issues: a narrative review. Medicina. 2022;58(9):1255. doi:10.3390/medicina58091255
34. Nair AD, Manchanda S, Gamanagatti S, et al. Post caesarean section complications conundrum: role of imaging. Br J Radiol. 2022;95(1138):20211344. doi:10.1259/bjr.20211344
35. Bridwell M, Handzel E, Hynes M, et al. Hypertensive disorders in pregnancy and maternal and neonatal outcomes in Haiti: the importance of surveillance and data collection. BMC Pregnancy Childbirth. 2019;19(1):208. doi:10.1186/s12884-019-2361-0
36. Bateman BT, Tsen LC, Liu J, et al. Patterns of second-line uterotonic use in a large sample of hospitalizations for childbirth in the United States: 2007–2011. Anesth Analg. 2014;119(6):1344–1349. doi:10.1213/ANE.0000000000000398
37. Victora CG, Bahl R, Barros AJ, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475–490. doi:10.1016/S0140-6736(15)01024-7
38. De Bortoli J, Amir LH. Is onset of lactation delayed in women with diabetes in pregnancy? A systematic review. Diabet Med. 2016;33(1):17–24. doi:10.1111/dme.12846
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.