Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Risk Factors of Developing Dysmobility Syndrome in Elderly Patients with Type 2 Diabetes Mellitus
Authors Zhang Y, Wu G, Wang C, Zhang W, Zhang W, Lou D
Received 18 January 2025
Accepted for publication 5 August 2025
Published 12 August 2025 Volume 2025:18 Pages 2815—2823
DOI https://doi.org/10.2147/DMSO.S518190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Yue Zhang, Guangfei Wu, Cuijuan Wang, Weinan Zhang, Wenqiang Zhang, Donghui Lou
Department of Endocrinology, The First Hospital of Qinhuangdao, Qinhuangdao, Heibei, People’s Republic of China
Correspondence: Donghui Lou, The first Hospital of Qinhuangdao, 258 Wenhua Road, Haigang District, Qinhuangdao, Hebei Province, People’s Republic of China, Email [email protected]
Background: Population aging is a worldwide phenomenon, and aging-related diseases need to be given great attention. Dysmobility syndrome (DMS) was considered as a comprehensive approach to evaluate the condition of musculoskeletal system and adverse health problems in older population.
Aim: There is little research data on the correlation between type 2 diabetes and DMS in the elderly. The purpose of our study is to identify the risk factors for dysmobility syndrome (DMS) in elderly patients with type 2 diabetes mellitus (T2DM).
Methods: A total of 262 patients aged > 60 years who were diagnosed with T2DM at our department were included in a cross-sectional study and were divided into groups according to the development of DMS and the number of presentations, including osteoporosis, low muscle strength and mass, obesity, falls, and slow walking speed. Consequently, 128 patients with non-DMS were assigned to group A, 84 patients with to 2– 3 presentations (without falls) were assigned to group B, and 50 patients with to 4– 5 presentations (without falls) were assigned to group C. Demographic data, diabetes-related complications, and history of falls in the past year were compared to identify risk factors for developing DMS in elderly T2DM patients.
Results: It showed that 50.4% of the elderly T2DM patients developed DMS, and 25.2% of them had at least one episode of falling. The average age of the patients and the occurrence of diabetic nephropathy were higher, while diastolic blood pressure and 25-(OH) vitamin D serum calcium and albumin levels were lower in group C than in group A and B(p < 0.05). The occurrence of falls was lower in group A than in the other groups (p = 0.001).
Conclusion: Aging, 25 (OH) vitamin D deficiency, and accidental fall history are associated with an increased risk of DMS in elderly patients with T2DM.
Keywords: geriatric, dysmobility syndrome, type 2 diabetes mellitus, falls
Introduction
Population aging is a worldwide demographic phenomenon that poses great challenges to modern society, especially in terms of medical burden. Aging is a major risk factor for the development of type 2 diabetes (T2DM). In 2019, the prevalence of type 2 diabetes in China increased by 12.75% and 50% in the population aged >60 years.
In addition, body composition and physical function are age-dependent, which might help explain the increasing prevalence of sarcopenia and osteoporosis in the elderly population. In 2013, Binkley et al1 first proposed the concept of dysmobility syndrome (DMS) to describe elderly patients with at least 3 of the following phenotypes: increased body fat, decreased muscle mass, decreased muscle strength, osteoporosis, slow gait, and history of falls. Although no consensus has been reached regarding this definition, most physicians have adopted the diagnostic criteria proposed by Binkley et al. Dysmobility syndrome is a comprehensive entity that assesses the condition of the musculoskeletal system and the possibility of developing high-risk accidents such as falls, fractures, and disabilities in the elderly population.
It has been well studied that The incidence and prevalence of accidental falls and the severity of their complications gradually increase after the age of 60.2 Accidental falls are not only associated with the occurrence of disability but can also link with loss of independence, fear of falls, social isolation, and even death, all of which significantly affect the quality of life of the elderly population.3,4
Although DMS involves a multidimensional and comprehensive assessment of the locomotor system, muscles and bones, which are the target organs for energy metabolism and endocrine hormones, are also one of the target organ damage caused by patients with type 2 diabetes and their chronic complications. Previous studies have indicated that patients with hyperglycemia are more likely to develop DMS.5 Capodaglio and Falchetti reported that the probability of DMS in patients with type 2 diabetes is significantly higher than that in patients without T2DM.6 However, there are currently limited literature reports on people with type 2 diabetes versus DMS.
Therefore, a cross-sectional clinical study was conducted to determine the risk factors of developing DMS in elderly patients with type 2 diabetes, and are expected to provide a theoretical basis for early identification, early diagnosis and early prevention of DMS in clinical work.
Methods
Patients
A total of 262 patients with type 2 diabetes mellitus (T2DM) diagnosed at the Department of Endocrinology of the First Hospital of Qinhuangdao from October 1, 2019, to January 30, 2022, were included in this study. Patients who fulfilled the following criteria were included in the screening: (1) diagnosis of type 2 diabetes mellitus; (2) age over 60 years; and (3) basic communication, comprehension, and behavioral capability. Patients with the following conditions were excluded from the study: (1) diagnosis of type 1 diabetes or other special types of diabetes; (2) uncorrected hyperglycemic conditions, such as diabetic ketoacidosis and hyperosmolar hyperglycemic state; (3) complications with acute cerebrovascular disease, gastrointestinal bleeding, acute renal failure, severe abnormal liver function and a history of severe physical damage; (4) complications with severe osteoarthrosis or neuromuscular disease affecting daily activities; (5) complications with acute infectious diseases; (6) complications with malignant tumors; and (7) complications with severe visual and hearing impairment.
Basic demographic parameters, including sex, age, duration of type 2 diabetes history, fall events in the last year, diabetic microvascular complications, diabetic peripheral macrovascular complications, and occurrence of diabetic peripheral neuropathy, were collected and compared among groups. This study was approved by the Ethics Committee of the First Hospital of Qinhuangdao, and followed the provisions of the Declaration of Helsinki. Informed consent was obtained from all participants, and patient anonymity was preserved.
Measurements
Demographic Parameters Measurements
Height and weight: Height and weight of the patients were measured twice and averaged. Height and weight were measured to the nearest 1 cm and the weight was measured to the nearest 0.1 kg. The body mass index (BMI) = weight/height ² (kg/m ²) was calculated for each patient. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured in the patient’s right upper arm according to standard procedures after calm rest.
Muscle Strength
Grip strength was measured as an index of overall muscle strength by using a JAMAR electric grip dynamometer. The patients were asked to sit and bend their elbows at an angle of 90 °. A professionally trained doctor measured the subject’s grip strength on both hands according to the same standard, taking three measurements and averaging them, with precision to 0.1 kg.
Gait Speed
Patients were asked to perform a 6-meter walking test at natural speed. Required time (s) and walking speed were calculated to the nearest 0.01 m/s.
Bone Mineral Density and Total Body Composition
Dual-energy X-ray absorptiometry (DXA) was applied to evaluate the basic condition of the subjects based on their specific age, sex, height, and weight. Patients were then asked to lie down on the operating table in a relaxed environment, and the bone mineral density (BMD) of the hip joint, L1-L4 vertebral body, total body muscle mass, limb skeletal muscle mass, and total body fat were measured by A medical professional who holds a work permit for radiologists. Body weight was used as the calibration index. The total body limb-skeletal muscle mass index (ASM) was calculated using the following formula: ASM = limb skeletal muscle mass/height² (kg/m²).
Sample Collection and Measurement
On the second day after admission, 3 mL of fasting venous blood was drawn from each patient and fasting glycosylated hemoglobin, 25-hydroxyvitamin D, calcium, phosphorus, and albumin levels were measured using an automatic biochemical analyzer.
Definition
Osteoporosis
Based on the bone mineral density of the axial skeleton (lumbar vertebra 1–4, femoral neck, or total hip) measured using DXA, patients were diagnosed with osteoporosis if they had at least one site with a mineral density value lower than 2. Five standard deviations of the normal peak values were obtained for the same sex.7
Obesity
Total body fat mass was measured using DXA, and patients with total body fat > 30% in male and > 40% in female and/or BMI ≥ 28 kg/m² were diagnosed with obesity.8
Low Muscle Mass
Male patients with ASMI≤ 7.26 kg/m² and female patients with ASMI≤ 5.45 kg/m² were considered as low muscle mass.9
Low Muscle Strength
Patients with a mean grip strength of less than 30 kg in both hands in male and 20 kg in female were considered to have low muscle strength.10
Fall History
Patients who reported at least one accidental fall event in the past year were considered to have a history of fall.1
Slow Gait
Patients with a walking speed < 0.8 m/s were considered to have a slow walking speed.10
Dysmobility Syndrome
Patients with at least 3 of the following conditions were diagnosed with movement disorder syndrome: osteoporosis, increased body fat, decreased muscle mass, decreased muscle strength, and slow gait and balance problems.
Type 2 Diabetes Mellitus
Patients with typical diabetes symptoms (polyuria, polydipsia, polyphagia, weight loss) plus fasting blood glucose ≥ 7.0 mmol/L, or random blood glucose/2h after glucose load blood glucose monitoring ≥ 11.1 mmol/L were diagnosed as T2DM. For patients without typical diabetes symptoms, at least two fasting or random blood glucose levels above the upper normal limit are required for diagnosis.11
Statistical Analysis
All experimental data were analyzed using SPSS software (version 26.0). Before the data analysis, normality and homogeneity of variance tests were performed. Data conforming to a normal distribution are presented as mean ± standard deviation, and non-normally distributed data are described as binary classification. The homogeneity of variance among the three groups was analyzed, and the χ ² test was applied to examine the differences between variables, as appropriate. Multiple logistic regression analysis was conducted to identify potential risk factors. Statistical significance was set at p < 0.05.
Study Design
Patients were divided into different groups according to the presence of dysmobility syndrome (DMS) and number of presentations. A total of 128 patients with non- DMS were assigned to group A, 84 patients with 2–3 presentations (without falls) to group B, and 50 patients with 4–5 presentations (without falls) to group C.
Result
A total of 262 patients with T2DM were enrolled in this study, and 50.4% had complications associated with DMS. In addition, our data showed that 25.2% of all patients had at least one episode of accidental falls.
Demographic Parameters
Demographic parameters of the enrolled patients are shown in Table 1. The average ages of patients in the three groups were 68.58 ± 5.31 years, 71.7 ± 6.25 years, and 74.58 ± 7.05 years, respectively, and 50%, 45.2%, and 30% of the patients were male, respectively. The mean age of patients in the group C was significantly higher compared to other two groups (p < 0.05) while the 25-hydroxyvitamin D level (39.66 ± 11.9) nmol/L was lower than that of group B (43.30 ± 15.0) nmol/L and group A (47.15 ± 12.03) nmol/L (p < 0.05). Furthermore, the serum calcium level in the group C (2.31 ± 0.21) mmol/L was lower than that of group B (2.33 0.10) mmol/L and group A (2.36 ± 0.10) mmol/L (p < 0.05) and the albumin level of group C (40.73 ± 4.87) g/L was lower than that of group B (41.92 ± 5.14) g/L and group A (42.82 ± 4.11) g/L. In addition, the mean diastolic blood pressure of patients in group C (77.42 ± 11.72) mmHg was lower than that of group B (82.24 ± 10.73) mmHg and group A (83.00 ± 11 mmHg) (p < 0.05). In contrast, 7.8% of patients in group A had experienced accidental falls within the past 1 year which was lower than that of 26.5% in group B and 22% in group C (p < 0.05). There were no significant differences in sex, serum phosphorus level, systolic blood pressure, glycosylated hemoglobin level, or history of diabetes among the three groups (p > 0.05).
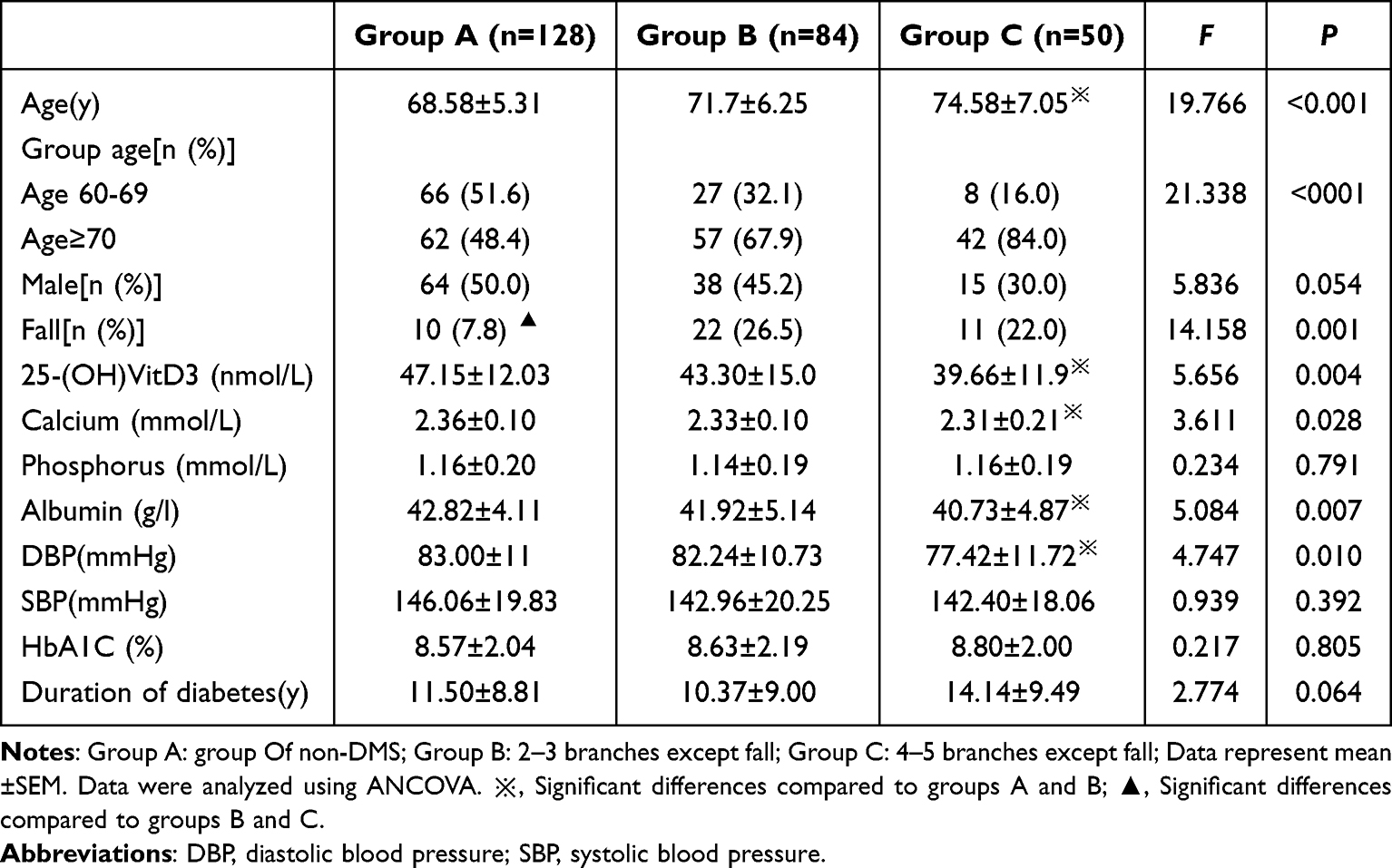 |
Table 1 Comparison of Demographic Parameters Among Different Groups |
Comparison of Diabetic Complications
The number of diabetic complications was compared (Table 2) and no significant differences in diabetic retinopathy (19% vs 9.6% vs 20.0%), diabetic peripheral neuropathy (40.9% vs.31.3% vs 42.0%), carotid atherosclerosis (88.1% vs 86.7% vs 90%), and lower-extremity arteriosclerosis (86.7% vs 88.0% vs 86.0%) were identified among the three groups (p > 0.05). However, the occurrence of diabetic nephropathy in group C was significantly higher than that in group B and group A (22%, 7.1%, and 12.6%; respectively p < 0.05).
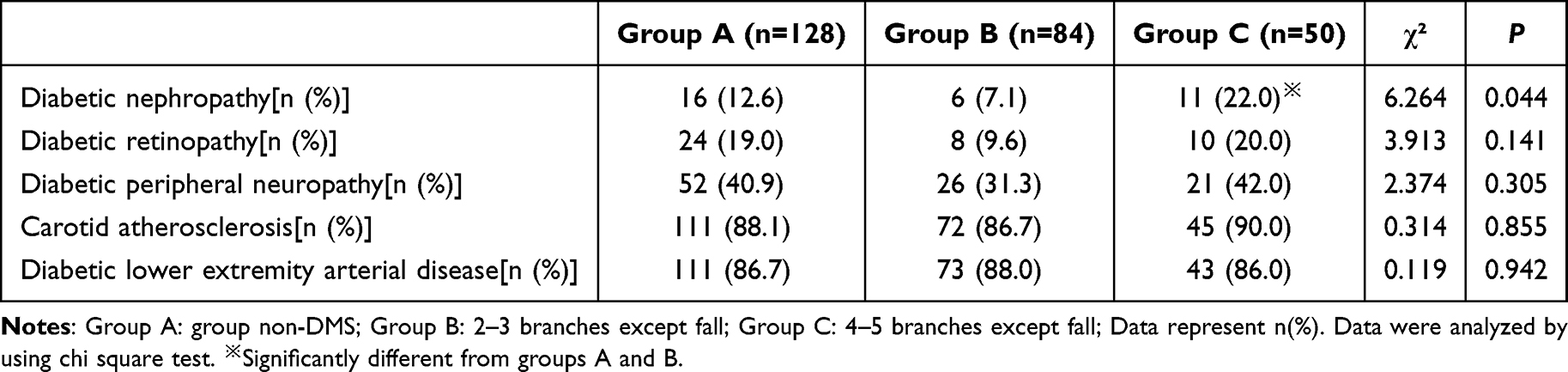 |
Table 2 Comparison of Diabetic Complications |
Multivariate Analysis to Identify Risk Factors for Dysmobility Syndrome in Elderly Patients with Type 2 Diabetes Mellitus
To determine the risk factors for developing DMS, we performed multiple regression analyses with independent variables including age, 25 (OH) vitamin D level, and history of falls within 1 year. Our data showed that patients with 25 (OH) vitamin D ≤ 43.7 mmol/L and aged ≥ 70 years were independent risk factors for DMS in elderly patients with T2DM and specific fold increase of risk were listed in the Table 3.
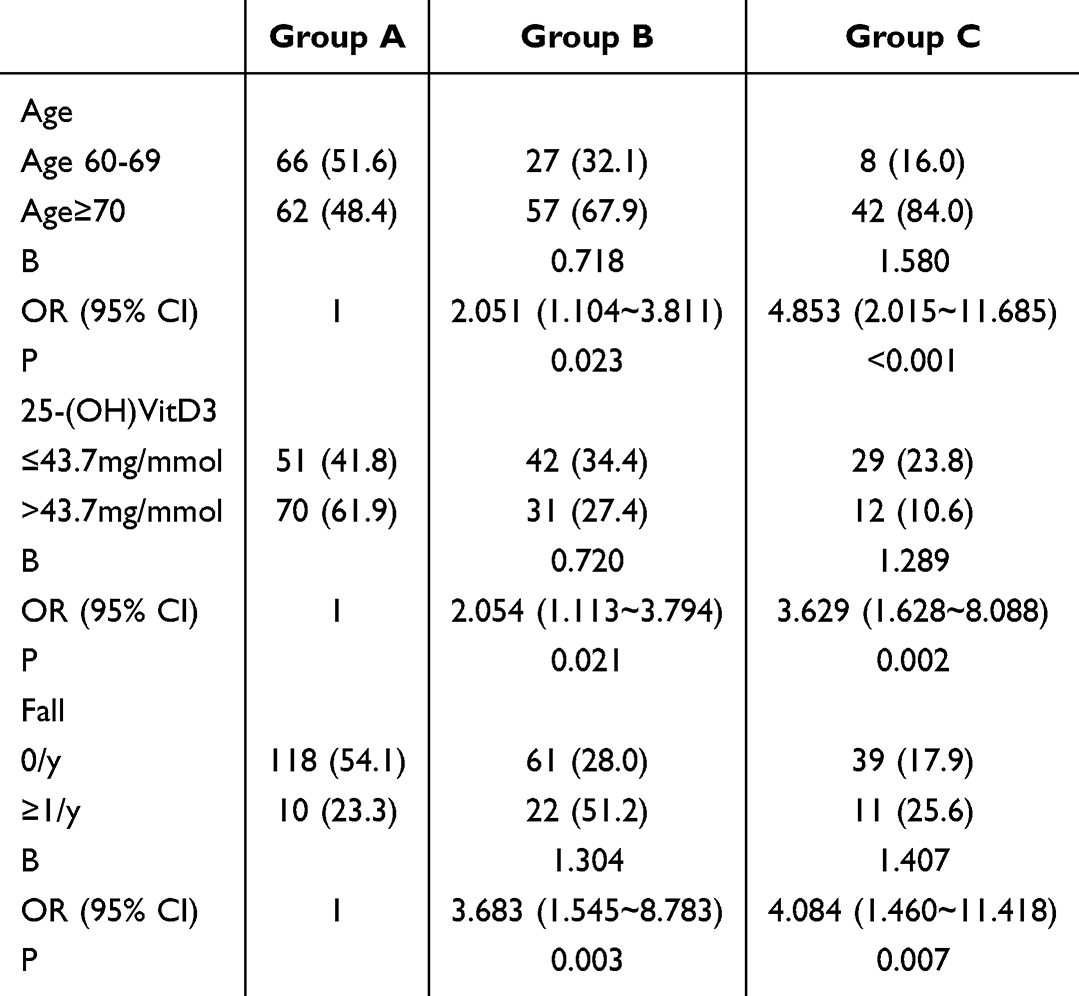 |
Table 3 Multiple Logistic Regression Analysis of Developing DMS |
Discussion
As a metabolic disease, T2DM alters internal homeostasis and severely affects the normal function of the musculoskeletal system owing to insulin resistance and insufficient insulin secretion. It has been well established that Aging is the main risk factor for the development of T2DM, and a large proportion of T2DM patients are overweight or obese, which may contribute to the development of DMS.
In this study, we identified risk factors for dysmobility syndrome in elderly patients with type 2 diabetes. Our data showed that the incidence of DMS is relatively high in elderly patients with T2DM. Compared to patients who did not have complicated DMS, patients with DMS were older, had a higher incidence of diabetic nephropathy and falls, and had lower diastolic blood pressure, 25-hydroxyvitamin D, serum calcium, and albumin levels. In addition, our data showed that aging, 25-hydroxyvitamin D level, and a history of falls were independent risk factors for the development of dysmobility syndrome in elderly patients with type 2 diabetes. A better understanding of the association between DMS and T2DM is critical for the development of comprehensive prevention and treatment strategies.
The prevalence of DMS varies among populations and largely depends on the definition of dysmobility syndrome used in different studies. Binkley et al1 reported a 34% prevalence of dysmobility syndrome among 97 Caucasian adults aged> 70 years. Dos Santos et al12 reported a prevalence of 27% in a study of 375 community-dwelling older adults over 60 years of age. Other studies have reported that the prevalence of dysmobility syndrome in different populations ranges from 20% to 25%.13–15In Japan, Asakura et al reported that the prevalence of DMS in type 2 diabetes was 54.8%, which was significantly higher than that in without T2DM.16 Our data showed that 50.4% of the patients developed DMS, which was much higher than that reported in most previous studies, indicating that patients with T2DM are more vulnerable to physical function deterioration and show physical restraints. We believe that this may be related to the lack of vitamin D and calcium intake in traditional Chinese diet and the insufficient attention paid by people to fall prevention (such as home environment modification, gait training).
Aging is associated with decreased efficiency of different cognitive functions as well as physical changes. Previous studies have shown that both DMS1 and type 2 diabetes are age-related diseases. Our study showed that aging is an independent risk factor for developing dysmobility syndrome in elderly patients with type 2 diabetes. Therefore, patients with type 2 at an advanced age should receive additional attention to prevent the occurrence of dysmobility syndrome.
Persistent hyperglycemia and metabolic disorders can induce renal tissue injury, and up to 50% of patients with type 2 diabetes have diabetic nephropathy in developed countries.17 Previous studies have shown a close relationship between sarcopenia and renal function, in which decreased skeletal muscle mass increases the risk of developing proteinuria.18 Sato et al reported that the causative pathological mechanism of uremic sarcopenia is metabolic alterations by uremic toxin indoxyl sulfate in a mouse model of CKD.19 Moreover, a significant inverse association between plasma indoxyl sulfate and skeletal muscle mass in CKD patients was observed in clinical research.19 Previous reports indicate that indoxyl sulfate may be a pathogenic factor for sarcopenia in CKD. It has been known that about 50% of diabetic nephropathy patients undergoing maintenance hemodialysis have skeletal muscle atrophy and decreased muscle strength.20
The skeletal muscle is one of the main target organs of glucose metabolism. Decreased skeletal muscle mass in patients with diabetic nephropathy may be associated with decreased glucose uptake and availability, increased blood glucose, aggravated insulin resistance, and a vicious cycle.21 In this study, we found that the occurrence of diabetic nephropathy was increased in patients with DMS. Patients with diabetic nephropathy often have insulin resistance and increased accumulation of glycation end products under persistent hyperglycemia and abnormal protein metabolism caused by inflammatory reactions and oxidative stress. Collectively, these changes result in damage to vascular structure and function, mitochondrial dysfunction, and reduced skeletal muscle mass, muscle strength, and function, and eventually contribute to the pathogenesis of dysmobility syndrome. Therefore, elderly patients with type 2 diabetes should strictly control their blood glucose levels and blood pressure to avoid or delay the occurrence of diabetic nephropathy.
This study showed that 25.2% of patients with DMS experienced at least one accidental fall, which has also been recognized as an independent risk factor for developing dysmobility syndrome in elderly patients with type 2 diabetes. In patients with T2DM, fat redeposition may be related to decreased muscle strength, and conditions such as hyperglycemia, insulin resistance, diabetic peripheral nerves, and vascular damage in T2DM may be linked to muscle atrophy. Consequently, decreased muscle strength can suggest imbalance and accidental falls.22,23 Reports have demonstrated that elderly patients with diabetes are at a high risk of falls,24,25 and these patients often suffer from fall-associated complications such as fractures, head injuries, and disabilities.26,27 Movement disorder syndrome has been shown to be associated with an increased risk of falls, fractures and death in Caucasian and Asian population.14,28–31 Therefore, measures should be implemented to prevent accidental falls in older patients with diabetes.
Calcium and vitamin D are important regulators of muscle and bone metabolisms. Vitamin D can promote intestinal calcium and phosphorus absorption, maintain blood calcium concentration, provide raw materials for bone mineralization, and directly regulate the activity of osteoblasts and osteoclasts. Vitamin D receptor is widely distributed in skeletal muscle, affecting myocyte differentiation, contractile protein synthesis and mitochondrial function. Owing to its long half-life and high concentration, 25- (OH) VitD has been considered a reliable surrogate for estimating vitamin D nutritional status.32 Previous studies have shown that vitamin D can improve insulin resistance and secretion.33,34 However, 25- (OH) VitD deficiency is common in elderly T2DM patients, and often suggest reduced bone turnover and resorption which ultimately result in osteoporosis. Moreover, studies have shown that osteoporosis severity is associated with the degree of serum 25 (OH) VitD deficiency.35 A large prospective cohort study conducted in the Netherlands showed that poor muscle function in patients with low vitamin D levels is an important risk factor for accidental falls.36 Other studies have also confirmed that reduced calcium absorption and changes in calcium homeostasis are associated with sarcopenia in the elderly.37,38 Appropriate supplementation of vitamin D and calcium can effectively prevent occurrence of accidental falls.39,40 Ma et al has reported an association between low vitamin D levels and an increased risk of DMS in patients with poorly controlled type 2 diabetes.41 Our study also found that in elderly patients with type 2 diabetes, decreased blood calcium levels are associated with the occurrence of DMS and, 25-(OH)VitD deficiency is an independent risk factor for developing DMS. Therefore, vitamin D and calcium supplementation should be recommended for elderly patients with type 2 diabetes and dysmobility syndrome, under appropriate conditions.
An association between protein level and muscle mass has been previously reported. In the 1990s, Castaneda et al42 found that elderly women on a low protein diet had decreased body weight and muscle function. In contrast, Campbell et al43 found that individuals with a high protein intake had significantly higher skeletal muscle growth than those with a low protein intake. Additionally, loss of appetite and malnutrition may be correlated with decreased muscle mass and increased fat mass.44 Our study found that albumin levels were low in the elderly patients with type 2 diabetes and DMS. Many factors can contribute to decreased albumin levels, including unbalanced nutritional intake and insufficient muscle synthesis. In addition, most elderly people have a decreased appetite and inadequate exercise. Furthermore, the prevalence of many wasting diseases and malignancies significantly increases in the elderly, often resulting in protein synthesis imbalance and sarcopenia. Increase dietary protein intake is one of the most important treatments for inhibiting muscle loss. It has been known that protein-rich nutritional supplements can prevent and reverse muscle loss and improve overall physical function in elderlies.45,46
Interestingly, our study showed that elderly patients with type 2 diabetes and DMS had a lower diastolic blood pressure. Diastolic blood pressure (DBP) is crucial for maintaining coronary and cerebral perfusion, especially during the heart’s diastolic phase. When DBP falls below 60 mmHg, it can lead to cerebral hypoperfusion, particularly when changing positions (such as from sitting to standing). This can be associated with transient ischemic attacks, dizziness, or fainting, thereby increasing the risk of falls. The association of type 2 diabetes with orthostatic hypotension significantly increased both the risk of falls and the risk of in-hospital mortality.47 This suggests that for the elderly, frail or type 2 diabetes patients, excessive blood pressure reduction should be avoided.
This study had several limitations. First, Although the study adjusted for known confounders through multivariate models, residual confounding is still possible. For example, physical activity levels and nutrient intake other than albumin may affect the results. SecondThe history of falls depends on the patient’s self-report, which may be affected by recall bias, and even with standardized procedures, the bias can still lead to an underestimation of risk associations. Finally, the sample size was relatively small owing to strict inclusion criteria. Currently, we are conducting a multicenter study with a larger sample size to examine nutritional and physical interventions for elderly T2DM with dysmobility syndrome.
In conclusion, our data suggests that elderly patients with T2DM have a higher prevalence of DMS. Aging, 25 (OH) vitamin D deficiency, and accidental fall history are associated with an increased risk of DMS in elderly patients with T2DM. The study suggests that routine screening for vitamin D and enhanced fall prevention care in elderly patients with type 2 diabetes may have potential clinical value.
Ethic Statement
This study was performed in line with the principles of the Declaration of Helsinki 2013 version. This study was approved by the Human Research Ethics Committee at Qinhuangdao First Hospital(2020B004).
Informed Consent
Informed consent was obtained from all participants.
Acknowledgments
This study was supported by the China Hebei Provincial Science and Technology Special Fund (grant number: 20377708D).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no financial relationships or conflicts of interest regarding this work.
References
1. Binkley N, Krueger D, Buehring B. What’s in a name revisited: should osteoporosis and sarcopenia be considered components of “dysmobility syndrome?”. Osteoporosis Int. 2013;24(12):2955–2959. doi:10.1007/s00198-013-2427-1
2. Kalula SZ, Ferreira M, Swingler GH, et al. Risk factors for falls in older adults in a South African Urban Community. BMC Geriatr. 2016;16(1):ARTN51. doi:10.1186/s12877-016-0212-7
3. Hosseini SR, Zohani Z, Kheyrkhah F, et al. Relationship between falling and chronic diseases in the elderly: a study derived from amirkola health and ageing project. Iran Red Crescent Me. 2020;22:ARTNe53.
4. Kelsey JL, Procter-Gray E, Hannan MT, et al. Heterogeneity of falls among older adults: implications for public health prevention. Am J Public Health. 2012;102(11):2149–2156. doi:10.2105/AJPH.2012.300677
5. Chen Y, Kao T-W, Wang -C-C, et al. Exploring the link between metabolic syndrome and risk of dysmobility syndrome in elderly population. PLoS One. 2018;13(12):e0207608. doi:10.1371/journal.pone.0207608
6. Capodaglio P, Falchetti A. Metabolic syndromes and dysmobility: why should physical medicine and rehabilitation care? Ame J Phys Med Rehab. 2021;100(3):e32–e33. doi:10.1097/PHM.0000000000001466
7. Michael P, Shelby B, Wang michael Y. Consensus guidelines for the treatment of osteoporosis. Neurosurgery. 2018;82(1):N6–N7. doi:10.1093/neuros/nyx530
8. Dufour AB, Hannan MT, Murabito JM, Kiel DP, McLean RP. Sarcopenia definitions considering body size and fat mass are associated with mobility limitations: the Framingham study. J Gerontol A Biol Sci Med Sci. 2013;68:168–174. doi:10.1093/gerona/gls109
9. Baumgartner RN, Koehler KM, Gallagher D, et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol. 1998;147:755–763. doi:10.1093/oxfordjournals.aje.a009520
10. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39:412–423. doi:10.1093/ageing/afq034
11. Michael D. Management of hyperglycaemia in type 2 diabetes. Consensus Report 2018 by the ADA and EASD. MMW-Fortschritte der Med. 2019;161(16):55–56.
12. V.r.d S, Diniz TA, Batista VC, et al. Practice of physical activity and dysmobility syndrome in community-dwelling older adults. J Exercise Rehab. 2019;15(2):294–301. doi:10.12965/jer.1938034.017
13. A.c L. Dysmobility syndrome and mortality risk in US men and women age 50 years and older. Osteoporosis Int. 2015;26(1):93–102. doi:10.1007/s00198-014-2904-1
14. M.a C, Edwards MH, Buehring B, et al. Definitions of sarcopenia: associations with previous falls and fracture in a population sample. Calcified Tissue Int. 2015;97(5):445–452. doi:10.1007/s00223-015-0044-z
15. Hong N, Kim CO, Youm Y, et al. Low peak jump power is associated with elevated odds of dysmobility syndrome in community-dwelling elderly individuals: The Korean urban rural elderly (KURE) study. Osteoporosis Int. 2018;29(6):1427–1436. doi:10.1007/s00198-018-4466-0
16. Asakura R, Miyatake N, Mochimasu KD, et al. Comparison of health-related quality of life between type 2 diabetic patients with and without locomotive syndrome. Environ Health Prev Med. 2016;21(5):356–360. doi:10.1007/s12199-016-0537-z
17. Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease: a report from an ADA consensus conference. Diabetes Care. 2014;37(10):2864–2883. doi:10.2337/dc14-1296
18. Ida S, Kaneko R, Imataka K, Murata K. Association between sarcopenia and renal function in patients with diabetes: a systematic review and meta-analysis. J Diab Res. 2019;2019:1365189. doi:10.1155/2019/1365189
19. Sato E, Mori T, Mishima E, et al. Metabolic alterations by indoxyl sulfate in skeletal muscle induce uremic sarcopenia in chronic kidney disease. Sci Rep. 2016;6(1):36618. doi:10.1038/srep36618
20. Mesinovic J, Zengin A, De Courten B, Ebeling PR, Scott D. Sarcopenia and type 2 diabetes mellitus: a bidirectional relationship. Diabetes Metab Syndr Obes. 2019;12:1057–1072. doi:10.2147/DMSO.S186600
21. Anagnostis P, Gkekas NK, Achilla C, et al. Type 2 diabetes mellitus is associated with increased risk of sarcopenia: a systematic review and meta-analysis. Calcified Tissue Int. 2020;107:453–463. doi:10.1007/s00223-020-00742-y
22. Andersen H, Nielsen S, Mogensen CE, et al. Muscle strength in type 2 diabetes. Diabetes. 2004;53(6):1543–1548. doi:10.2337/diabetes.53.6.1543
23. Wang CP, Hazuda HP. Better glycemic control is associated with maintenance of lower-extremity function over time in Mexican American and European American older adults with diabetes. Diabetes Care. 2011;34(2):268–273. doi:10.2337/dc10-1405
24. Lee PG, Pokhrel KP, William H. Herman, Fall risk in individuals with type 2 diabetes: the look ahead study. Diabetes. 2019;68(Supplement_1):1446–P. doi:10.2337/db19-1446-P
25. M.m J, Gerami H, Heidarzadeh A, et al. Balance performance in older adults and its relationship with falling. Aging Clin Exp Res. 2015;27(3):287–296. doi:10.1007/s40520-014-0273-4
26. Ong WF, Kamaruzzaman, Shahrul SB, Tan MP. Falls in older persons with type 2 diabetes in the Malaysian elders longitudinal research (MELoR) study. Int J Clin Pract. 2021;75(12):e14999. doi:10.1111/ijcp.14999
27. Burgueno-Aguilar K, Cons-Molina FF, Garcia-Jimenez D, Bejarano-Lopez LE, Gudino-Barroso MA. Dysmobility syndrome: a case-series study describing a musculoskeletal syndrome in postmenopausal Mexican women. Arch Osteoporosis. 2021;16(1):54. doi:10.1007/s11657-021-00897-7
28. Buehring B, Hansen KE, Lewis BL. Dysmobility syndrome independently increases fracture risk in the osteoporotic fractures in men (MrOS) prospective cohort study. J Bone Miner Res. 2018;33(9):1622–1629. doi:10.1002/jbmr.3455
29. Iolascon G, Moretti A, Giamattei MT, Migliaccio S, Gimigliano F. Prevalent fragility fractures as risk factor for skeletal muscle function deficit and dysmobility syndrome in post-menopausal women. Aging Clin Exp Res. 2015;27(Suppl 1):S11–S16. doi:10.1007/s40520-015-0417-1
30. Lee W-J, Liu L-K, Hwang A-C, Peng L-N, Lin M-H, Chen L-K. Dysmobility syndrome and risk of mortality for community-dwelling middle-aged and older adults: the nexus of aging and body composition. Sci Rep. 2017;7(1):8785. doi:10.1038/s41598-017-09366-z
31. Looker AC. Dysmobility syndrome and mortality risk in US men and women age 50 years and older. Osteoporos Int. 2014;26:93–102.
32. Kuchuk NO, Pluijm SMF, van Schoor NM, et al. Relationships of serum 25-hydroxyvitamin D to bone mineral density and serum parathyroid hormone and markers of bone turnover in older persons. J Clin Endocrinol Metab. 2009;94(4):1244–1250. doi:10.1210/jc.2008-1832
33. Ardabili HR, Gargari BP, Farzadi L. Vitamin D supplementation has no effect on insulin resistance assessment in women with polycystic ovary syndrome and vitamin D deficiency. Nutr Res. 2012;32:195–201. doi:10.1016/j.nutres.2012.02.001
34. Roth CL, Elfers C, Kratz M, et al. Vitamin D deficiency in obese children and its relationship to insulin resistance and adipokines. J Obes. 2011;2011:495101. doi:10.1155/2011/495101
35. Lu L, Sheng H, Li H, et al. Associations between common variants in GC and DHCR7/NADSYN1 and vitamin D concentration in Chinese Hans. Hum Genet. 2012;131(3):505–512. doi:10.1007/s00439-011-1099-1
36. Snijder M, Van Schoor N, Pluijm S, et al. Vitamin D status in relation to one-year risk of recurrent falling in older men and women. J Clin Endocrinol Metab. 2006;91(8):2980–2985. doi:10.1210/jc.2006-0510
37. Brotto M. Aging, sarcopenia and store-operated calcium entry: a common link? Cell Cycle. 2011;10:4201–4202. doi:10.4161/cc.10.24.18645
38. Fleet JC, Schoch RD. Molecular mechanisms for regulation of intestinal calcium absorption by vitamin D and other factors. Crit Rev Clin Lab Sci. 2010;47:181–195. doi:10.3109/10408363.2010.536429
39. Bischoff-Ferrari HA, Orav EJ, Dawson-Hughes B. Effect of cholecalciferol plus calcium on falling in ambulatory older men and women: a 3-year randomized controlled trial. Arch Intern Med. 2006;166:424–430. doi:10.1001/archinte.166.4.424
40. Al-Said Y, Al-Rached H, Al-Qahtani H, et al. Severe proximal myopathy with remarkable recovery after vitamin D treatment. Can J Neurol Sci. 2009;36(3):336–339. doi:10.1017/S0317167100007083
41. Yongfang M, Liu B, Yin F, et al. Vitamin D level as a predictor of dysmobility syndrome with type 2 diabetes. Sci Rep. 2024;14(1):19792. doi:10.1038/s41598-024-70400-y
42. Castaneda C, Charnley JM, Evans WJ, Crim MC. Elderly women accommodate to a low-protein diet with losses of body cell mass, muscle function, and immune response. Am J Clin Nutr. 1995;62(1):30–39. doi:10.1093/ajcn/62.1.30
43. Campbell WW, Ml B Jr, Cyr-Campbell D, et al. Effects of an omnivorous diet compared with a lactoovovegetarian diet on resistance-training-induced changes in body composition and skeletal muscle in older men. Am J Clin Nutr. 1999;70:1032–1039. doi:10.1093/ajcn/70.6.1032
44. Wilson MM, Morley JE. Invited review: aging and energy balance. J Appl Physiol. 2003;95:1728–1736. doi:10.1152/japplphysiol.00313.2003
45. Tieland M, van de Rest O, Dirks ML, et al. Protein supplementation improves physical performance in frail elderly people: a randomized, double-blind, placebo-controlled trial. J Am Med Dir Assoc. 2012;13:720–726. doi:10.1016/j.jamda.2012.07.005
46. Oh C, Jho S, No JK, et al. Body composition changes were related to nutrient intakes in elderly men but elderly women had a higher prevalence of sarcopenic obesity in a population of Korean adults. Nutr Res. 2015;35:1–6. doi:10.1016/j.nutres.2014.07.018
47. Beretta MV, Milan VB, Hoffmeister MC, Rodrigues TC. Orthostatic hypotension, falls and in-hospital mortality among elderly patients with and without type 2 diabetes. J Hypertension. 2022;40:1.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk of Falls in HIV-Infected Patients on Antiretroviral Therapy and Its Associated Factors
Wahyudi ER, Putri RF, Yunihastuti E, Shatri H
HIV/AIDS - Research and Palliative Care 2022, 14:355-363
Published Date: 2 August 2022