Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Risk Factors for Midline Catheter Failure: A Secondary Analysis of an Existing Trial
Authors Bahl A ![]() , Johnson S
, Johnson S ![]() , Mielke N, Chen NW
, Mielke N, Chen NW
Received 23 July 2022
Accepted for publication 16 September 2022
Published 7 October 2022 Volume 2022:18 Pages 999—1007
DOI https://doi.org/10.2147/TCRM.S383502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Amit Bahl,1 Steven Johnson,1 Nicholas Mielke,2 Nai-Wei Chen3
1Department of Emergency Medicine, Beaumont Hospital, Royal Oak, MI, USA; 2Oakland University William Beaumont School of Medicine, Rochester, MI, USA; 3Research Institute, Beaumont Hospital, Royal Oak, MI, USA
Correspondence: Amit Bahl, Department of Emergency Medicine, Beaumont Hospital, Royal Oak, 3601 13 Mile Road, Royal Oak, MI, 48073, USA, Email [email protected]
Objective: While midline catheters (MCs) are considered to be a reliable form of vascular access, up to 25% of the placements culminate in failure. We aimed to explore risk factors for MC failure.
Methods: We performed an analysis of existing randomized controlled trial data involving a comparison of two midline catheters. The study aimed to assess risk factors related to MC failure, including patient, procedure, catheter, and vein characteristics. Cox regression was used for univariable and multivariable analyses to evaluate the association between characteristics and MC failure.
Results: Among 191 patients that were included in this secondary analysis, more patients were female (114/191 [59.7%]) and average age was 60.2 (SD = 16.7) years. Clinical indications for MC placement included antibiotics (60.7%), difficult venous access (32.5%), or both (6.8%). In a univariable Cox regression analysis, the increase in pulse rate (HR 1.02; 95% CI, 1.00– 1.04; P=0.02), temperature ≥ 38°C (HR 5.59; 95% CI, 1.96– 15.94; P=0.001), oxygen saturation < 93% (HR 2.91; 95% CI, 1.03– 8.24; P=0.04), norepinephrine in dextrose infusion (HR 2.41; 95% CI, 1.17– 4.97; P=0.02) and cephalic vein insertion (HR, 2.47; 95% CI, 1.09– 5.57; P=0.03) were all associated with higher risk of MC failure. In a multivariable Cox model, difficult venous access (aHR 2.05; 95% CI, 1.04– 4.05; P=0.04) and norepinephrine in dextrose (aHR 2.29; 95% CI, 1.09– 4.82; P=0.03) was associated with catheter failure.
Conclusion: Elevated pulse rate, decreased oxygen saturation level, temperature ≥ 38°C, and norepinephrine use were each associated with an increased risk of MC failure. These factors should be considered when selecting the most appropriate vascular access device for individual patients. Additionally, the cephalic vein insertion has the highest risk for MC failure and other access points could be preferentially considered.
Keywords: midline catheter, complications, risk factors, midline catheter failure, vesicants, vascular access
Introduction
With over 850,000 midline catheters (MCs) sold in the United States in 2019, establishing peripheral venous access with these devices is steadily gaining popularity.1 MCs are designed for intermediate duration intravenous therapies, generally ranging from 5 to 14 days and in some instances, greater than 15 days.2,3 They are typically inserted in the upper extremity, with the tip of the catheter located proximal to the axilla, but one study demonstrated successful placement in the femoral vein in the groin.4 MCs have been shown to be reliable across numerous investigations; however, a minority of these catheters do fail prior to completion of therapy, and risk factors for catheter failure are currently unknown.2,5–8 Nonetheless, there is some limited data on the premature removal rate of MCs. One systematic review, that included 31 individual manuscripts, reported a incidence range for MC failure of 2.6–57%, with an overall adjusted rate of 12.5%.5 Patients who experience MC failure have a multitude of downstream sequela as a result, including the need for repeat invasive procedures, venous depletion from repeated IV needlesticks, escalation to more invasive central venous access devices with associated higher risk profiles, extravasation with skin necrosis, catheter-associated bloodstream infections, interruption of medical therapies, and longer hospital stays.7,9,10
To date, there are limited data describing outcomes after MC failure and even less literature evaluating potential risk factors that may predict MC failure. In order to select the most effective and safest vascular access device for any given patient, it is imperative that we understand what potential risk factors may preclude MC use. Additionally, identifying a patient population that is low risk for premature MC failure would be just as beneficial. We believe that several variables including demographics, clinical, procedural, and line/vein characteristics may influence survival and help us better understand catheter failure. Thus, the goal of this analysis is to identify risk factors that are predictive of premature MC failure in order to help identify when and among which patients, a different vascular access device may be a more appropriate solution.
Materials and Methods
Study Sample
This was a secondary analysis of a previous randomized control trial at an 1100 bed tertiary care center with an annual emergency department census of approximately 120,000 visits that compared two midline catheters: a 4 French antithrombotic single-lumen 20 cm MC (MC-AT) from AngioDynamics (BioFlo 4F) and a 4.5 French antithrombotic and antimicrobial single-lumen 15 cm MC (MC-AT-AM) from Teleflex Inc (Arrowg+rd Blue Advance 4.5F). (ClinicalTrials.gov Identifier: NCT03725293)
In short, the primary study was approved for participants over 18 years who required MC placement for difficult vascular access, intermediate duration antibiotics (7–28 days), or both. Patients were excluded if they were previously enrolled in the study, required a catheter with multiple lumens, required alternative catheter diameter, or if they were receiving treatment dose anticoagulation (prophylactic dosages were permitted). Ultimately, 191 participants were included in the dataset. The primary outcome of the trial was catheter-related thrombosis. All participants in the trial provided informed consent and the trial was conducted in accordance with the Declaration of Helsinki. This secondary exploration of predictors of MC failure independent of catheter type was approved by the Institutional Review Board of Beaumont Health.
Outcome Measure
The study outcome was midline catheter failure. Catheter failure was defined as unresolvable malfunction or complication that resulted in catheter removal before completion of therapy. Potential causes of catheter removal included leaking, pain, dislodgement, complete occlusion, persistent withdrawal occlusion, and infiltration. Research staff abstracted the cause of failure from the medical record as this was not a prespecified aim of the original trial. Daily MC site and catheter evaluations performed by the research staff were used to identify functionality and premature catheter failure. A catheter was functional if clinical staff were able to withdraw 3–5 mL of blood and/or if the VAD flushed without resistance using 5 mL of normal saline.
Independent Variables
To identify the potential predictors of MC failure, we included the following variable categories: demographic, clinical, insertion/catheter, and line/vein factors. Demographic and clinical variables included age, gender, body mass index, vital signs immediately preceding catheter insertion, relevant medical history (venous thromboembolism, hypercoagulable state, major surgery, immobilization), indication of MC, and use of irritants or vesicants (Appendix with list of irritants/vesicants used in this study). MC-insertion-related data included location/side of vein of placement, vein depth/diameter, catheter-to-vein ratio, and distance from antecubital fossa (cm).
Primary Data Analysis
Continuous and categorical variables were expressed as means (standard deviations; SD) and frequencies (percentages), respectively. To explore the association between risk factors and premature MC failure, Cox regression was used for univariable and multivariable analyses. Following the univariable analysis, variables with a p-value <0.05 or variables determined by clinicians based on clinical rationale were subjected to a multivariable modeling strategy. There was no violation of proportional hazards assumption. The corresponding c-statistic and a bootstrap cross-validation were used to evaluate the performance of modeling in multivariable analysis. All tests with a p-value <0.05 were considered to indicate statistical significance. All statistical analyses were performed with SAS v9.4 (SAS Institute, Inc., Cary, NC).
Results
In total, 191 patients were included in this secondary analysis of existing data; 114 (59.7%) of 191 patients were female and the average age was 60.2 (SD = 16.7) years. Clinical indications for MC placement included antibiotics (60.7%), difficult venous access (32.5%), or both (6.8%). Premature MC failure occurred in 42 (22.0%) patients (Table 1).
 |
Table 1 Patient and Catheter-Related Characteristics |
Of the 42 failures, the most common reason for removal was leaking which occurred in 14 (33%) cases. This was followed closely by pain which occurred in 8 (19%) cases. While persistent withdrawal occlusion was the most frequent complication occurring in 18 (43%) cases, it was the primary cause of removal in only 7 cases (Table 2).
 |
Table 2 Primary Causes of Catheter Removal Among Failed Catheters |
In the univariable Cox regression analysis, the increase in pulse rate (unadjusted hazard ratio [HR], 1.02; 95% confidence interval [CI], 1.00–1.04; P = 0.02), oxygen saturation <93% (HR, 2.91; 95% CI, 1.03–8.24; P = 0.04), body temperature ≥38°C (HR, 5.59; 95% CI, 1.96–15.94; P = 0.001), catheter placement indication of both antibiotics and difficult venous access (HR, 4.17; 95% CI 1.67–14.41; P = 0.002), norepinephrine in dextrose use (HR, 2.41; 95% CI, 1.17–4.97; P = 0.02) and placement in the cephalic vein (HR, 2.47; 95% CI, 1.09–5.57; P = 0.03) were each associated with higher risk of catheter failure. The multivariable Cox model with an internal bootstrap validation (c-statistic 0.66, 95% CI 0.56–0.77) shows that indication of difficult venous access (aHR, 2.05; 95% CI, 1.04–4.05; P = 0.04) and norepinephrine in dextrose use (aHR, 2.29; 95% CI, 1.09–4.82; P = 0.03) were each associated with catheter failure (Table 3).
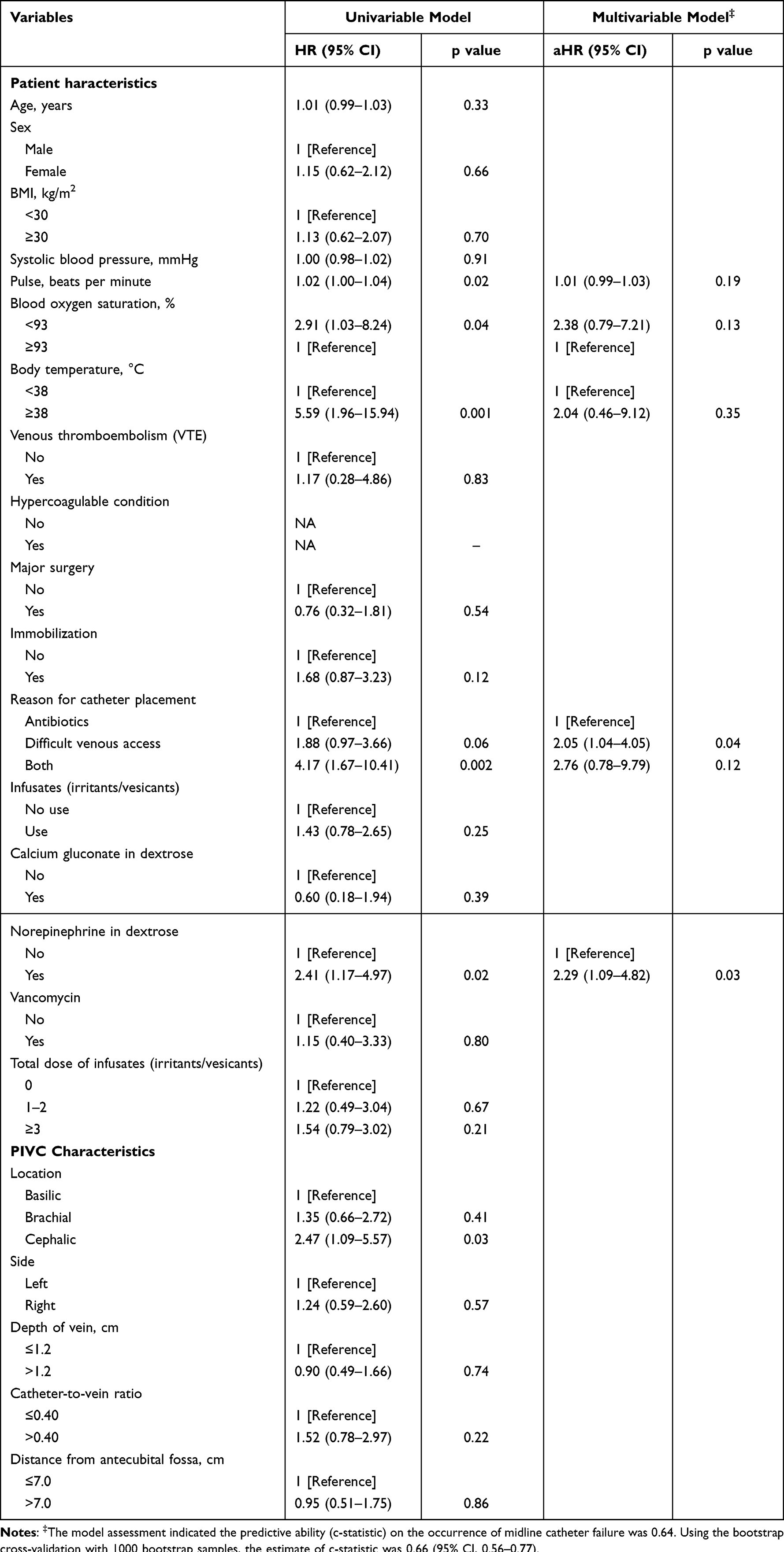 |
Table 3 Univariable and Multivariable Analyses for Midline Catheter Failure |
Discussion
In our cohort, we observed a relatively high rate of premature MC failure (22%). As we have previously described, existing literature suggests that the true MC failure rate is somewhere between 2.6% and 57%, which is consistent with our findings here.5 Our univariable analysis uncovered several variables associated with an increased risk of MC failure prior to completion of therapy, including body temperature ≥38°C, elevated pulse rate, decreased blood oxygen saturation, and norepinephrine in dextrose use. It is notable, however, that most of these variables were not statistically significant in a multivariable analysis. Given the overall small to moderate sample size of our population, it is plausible that these variables would reach statistical significance in a larger cohort. Regardless, our findings in the univariable analysis do suggest a population of patients where MCs may be a higher risk device and alternative vascular access devices could be considered.
Previous literature has described that critical illness and systemic inflammation (including sepsis) are associated with higher rates of catheter-related complications, specifically thrombosis.11–13 However, what is less well known is whether a patient with critical illness has an increased risk of catheter-associated complications or if catheter complications increase the duration and/or severity of critical illness. Our findings suggest the former. Patients in our analysis who presented with systemic inflammatory response syndrome (elevated pulse, fever, decreased oxygen saturation) had an increased risk of MC failure when compared to individuals without these vital sign abnormalities. These findings suggest that patients who meet systemic inflammatory response criteria upon arrival to the hospital, or prior to vascular access device insertion, may experience higher rates of MC failure than other populations. Therefore, among these patients, another vascular access device, such as a centrally inserted central catheter (CICC), may be more appropriate for their acute care needs. However, our findings must be replicated in a larger cohort and specifically evaluate if a diagnosis of sepsis vs another inflammatory disorder portrays a higher risk of catheter failure.
Another significant finding in our analysis was that cephalic vein placement was associated with a higher risk of MC failure prior to completion of therapy. More specifically, cephalic vein placements experienced a nearly two-fold increase in the risk of premature MC failure compared to devices placed in the basilic or brachial vein. This finding aligns with previous literature, which highlighted that MC placement in the cephalic vein is a high-risk venous access site that specifically increases the risk of catheter-related thrombosis.14 Given the high risk of complications with MC cephalic vein placement, clinicians should preferentially choose another location for MC placement when possible. Based on the findings of this analysis as well as prior literature, we suggest that in scenarios where the cephalic vein is the solely accessible option, clinicians should consider alternative venous access devices such as central venous catheters as a potentially more durable solution.15 It is also notable that shifting to a central line does not necessarily translate to an elevated safety risk. One recent publication found that when compared to MCs, PICCs did not increase the risk of thrombosis or infection across the study population as well as in a sub-analysis of sepsis and septic shock.16
After the implementation of widespread mandatory monitoring and reporting of central line associated blood stream infections since the early 2000s, many institutions have greatly reduced their utilization of CICCs in favor of other options. These regulations likely spurred some of the popularity of MCs which remain unregulated. Given the lack of surveillance, there has also been expanded use of MCs to include the delivery of caustic therapies that traditionally have been infused via CICCs. Minimal existing evidence has shown that infusion of vasoactive medications via MCs does not increase risk to the patient.17 In this investigation, while the use of vesicants/irritants as a general class did not confer risk of line failure, in univariable and multivariable analyses, use of norepinephrine in dextrose specifically was associated with an increased risk of line failure. As norepinephrine is a commonly used first-line vasopressor and was the second most frequently used caustic medication in this study, clinicians should consider the negative impact on MC survival when considering norepinephrine infusion via MCs. While other caustic substances did not clearly show an increased hazard of MC failure, it is plausible that there are likely several scenarios where a CICC may be preferred over MCs despite recent unchecked widespread adoption of MCs. However, additional larger trials are needed that account for type, dose, duration, and frequency of administration of these medications to determine the precise impact of vesicants on MC survival.
Limitations
This study had some limitations. First, this investigation was performed at a single, large academic suburban tertiary care center with a patient population that may not be generalizable to other sites. Second, as this was a secondary analysis of an existing trial dataset, the potential actionable strategies need to be further substantiated through a larger well-designed evidence-based experimental or observational study. Third, there was a small-to-moderate sample size which limits our conclusions. Fourth, the results are limited to the catheters analyzed in this trial and other factors such as multiple lumens or varying catheter diameters were not evaluated. Finally, details regarding etiology of failure were captured from the medical record based on observations and documentation of the clinical staff. As ultrasound was not used to evaluate all catheters with complications, the exact cause of failure, possibly multifactorial, was unknown.18,19
Conclusions
Patients with elevated pulse rates, decreased oxygen saturation levels, and temperatures ≥38°C, all had increased risk of MC failure prior to completion of therapy. Additionally, lines placed in the cephalic vein were at higher risk of failure compared to lines in the basilic or brachial veins. Our findings suggest that among patients who have clinical instability prior to vascular access device placement, MCs may have higher risk of failure and another device could be considered for their acute care needs. Additionally, if only the cephalic vein is available for MC placement, it may be prudent to consider another device as more appropriate.
Data Sharing Statement
The data that support the findings of this study are available via a data access agreement. Please contact the corresponding author for this request.
Ethics Committee Approval
This study was approved by the Beaumont Health Institutional Review Board. All trial participants provided informed consent and the trial was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Research was funded via and educational grant for research by Teleflex. The funder had no role in the study design, subject enrollment, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all study data in the study and had final responsibility for the decision to submit for publication.
Disclosure
Amit Bahl has research grant support from B. Braun Medical, Becton-Dickinson, Teleflex, Adhezion, Medline Industries, and Access Vascular. Amit Bahl is a paid consultant for B. Braun Medical, Teleflex, and Interad Medical. All other authors have no disclosures to report for this study.
References
1. IDATA. US market report suite for vascular access devices and accessories; 2020. Available from: https://idataresearch.com/product-category/vascular-access/.
2. Gorski LA, Hadaway L, Hagle ME, et al. Infusion therapy standards of practice, 8th edition. J Infusion Nurs. 2021;44(1SSuppl 1):S1–S224. doi:10.1097/NAN.0000000000000396
3. Chopra V, Flanders SA, Saint S, et al. The Michigan Appropriateness Guide for Intravenous Catheters (MAGIC): results from a multispecialty panel using the RAND/UCLA appropriateness method. Ann Intern Med. 2015;163(6 Suppl):S1–S39. doi:10.7326/M15-0744
4. Gidaro A, Samartin F, Salvi E, et al. Midline peripheral catheters inserted in the superficial femoral vein at mid-thigh: wise choice in COVID-19 acute hypoxemic respiratory failure patients with helmet continuous positive airway pressure. J Vasc Access. 2022;112972982210854. doi:10.1177/11297298221085450
5. Tripathi S, Kumar S, Kaushik S. The practice and complications of midline catheters: a systematic review. Crit Care Med. 2021;49(2):E140–E150. doi:10.1097/CCM.0000000000004764
6. Bahl A, Diloreto E, Jankowski D, Hijazi M, Chen NW. Comparison of 2 midline catheter devices with differing antithrombogenic mechanisms for catheter-related thrombosis: a randomized clinical trial. JAMA Network Open. 2021;4(10):e2127836. doi:10.1001/jamanetworkopen.2021.27836
7. Seo H, Altshuler D, Dubrovskaya Y, et al. The safety of midline catheters for intravenous therapy at a large academic medical center. Ann Pharmacother. 2020;54(3):232–238. doi:10.1177/1060028019878794
8. Alexandrou E, Ramjan LM, Spencer T, et al. The use of midline catheters in the adult acute care setting – clinical implications and recommendations for practice. J Assoc Vasc Access. 2011;16(1):35–41. doi:10.2309/JAVA.16-1-5
9. Sharp R, Esterman A, McCutcheon H, Hearse N, Cummings M. The safety and efficacy of midlines compared to peripherally inserted central catheters for adult cystic fibrosis patients: a retrospective, observational study. Int J Nurs Stud. 2014;51(5):694–702. doi:10.1016/j.ijnurstu.2013.09.002
10. Dickson HG, Flynn O, West D, Alexandrou E, Mifflin N, Malone M. A cluster of failures of midline catheters in a hospital in the home program: a retrospective analysis. J Infusion Nurs. 2019;42(4):203–208. doi:10.1097/NAN.0000000000000330
11. Wall C, Moore J, Thachil J. Catheter-related thrombosis: a practical approach. J Intensive Care Soc. 2016;17(2):160–167. doi:10.1177/1751143715618683
12. Del Principe MI, Buccisano F, Maurillo L, et al. Infections increase the risk of central venous catheter-related thrombosis in adult acute myeloid leukemia. Thromb Res. 2013;132(5):511–514. doi:10.1016/j.thromres.2013.08.007
13. Timsit JF, Farkas JC, Boyer JM, et al. Central vein catheter-related thrombosis in intensive care patients. Chest. 1998;114(1):207–213. doi:10.1378/chest.114.1.207
14. Lisova K, Hromadkova J, Pavelková K, Zauška V, Havlin J, Charvat J. The incidence of symptomatic upper limb venous thrombosis associated with midline catheter: prospective observation. J Vasc Access. 2018;19(5):492–495. doi:10.1177/1129729818761276
15. Xu T, Kingsley L, DiNucci S, et al. Safety and utilization of peripherally inserted central catheters versus midline catheters at a large academic medical center. Am J Infect Control. 2016;44(12):1458–1461. doi:10.1016/J.AJIC.2016.09.010
16. Bing S, Smotherman C, Rodriguez RG, Skarupa DJ, Ra JH, Crandall ML. PICC versus midlines: comparison of peripherally inserted central catheters and midline catheters with respect to incidence of thromboembolic and infectious complications. Am J Surg. 2022;223(5):983–987. doi:10.1016/J.AMJSURG.2021.09.029
17. Spiegel RJ, Eraso D, Leibner E, Thode H, Morley EJ, Weingart S. The utility of midline intravenous catheters in critically ill emergency department patients. Ann Emerg Med. 2020;75(4):538–545. doi:10.1016/j.annemergmed.2019.09.018
18. Passaro G, Pittiruti M, la Greca A. The fibroblastic sleeve, the neglected complication of venous access devices: a narrative review. J Vasc Access. 2021;22(5):801–813. doi:10.1177/1129729820951035
19. Bahl A, Johnson S, Mielke N, Karabon P. Early recognition of peripheral intravenous catheter failure using serial ultrasonographic assessments. PLoS One. 2021;16(6):e0253243. doi:10.1371/JOURNAL.PONE.0253243
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.