Back to Journals » International Journal of General Medicine » Volume 16
Risk Factors for Diabetic Retinopathy in Chinese Patients with Different Diabetes Duration: Association of C-Peptide and BUN/Cr Ratio with Type 2 Diabetic Retinopathy
Authors Li J, Dong Z, Wang X, Wang X, Wang L, Pang S
Received 22 May 2023
Accepted for publication 22 August 2023
Published 6 September 2023 Volume 2023:16 Pages 4027—4037
DOI https://doi.org/10.2147/IJGM.S420983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jianting Li,1,2 Zhenhua Dong,2 Xiaoli Wang,2 Xin Wang,2 Lulu Wang,2 Shuguang Pang1– 3
1Department of Endocrinology, Jinan Central Hospital, Cheeloo College of Medicine, Shandong University, Jinan, 250013, People’s Republic of China; 2Department of Endocrinology, Central Hospital Affiliated to Shandong First Medical University, Jinan, 250013, People’s Republic of China; 3Department of Clinical Medicine, Weifang Medical College, Weifang Medical College, Weifang, People’s Republic of China
Correspondence: Shuguang Pang, Email [email protected]
Background and Aim: Controlling the risk factors was the most effective strategy to prevent diabetic retinopathy (DR). This study aimed to recognize the risk factors of DR, and explores whether the effect of those factors is modified by diabetes mellitus (DM) duration.
Methods: A total of 1058 DM patients with information about DR assessment were included. DR was measured by a complete ophthalmic examination and was classified as having one or more distinct microaneurysms in the eyes. Data from the lab and clinical factors were gathered. Multivariate logistic analysis was used to examine the risk factors, and the best-fitting model was selected by a backward stepwise based on A1C.
Results: In the current study, 274 (25.9%) patients developed DR. In the entire subjects, baseline age, the level of C-peptide, and urinary creatinine were all presented as protective effects of DR, whose odds ratios (ORs) and 95% confidence intervals (CIs) were 0.79 (0.62, 0.99), 0.75 (0.61, 0.91), and 0.70 (0.52, 0.93), respectively. Conversely, systolic pressure (SBP), urinary albumin, and BUN/Cr ratio were the important risk factors for DR with ORs (95% CIs) 1.21 (1.01, 1.46), 1.55 (1.30, 1.84), and 1.33 (1.11, 1.59), respectively. In stratification analysis, females with higher SBP would be more likely to develop DR in the short-duration group, while C-peptide and urinary creatinine showed protective effects in the long-duration group. BUN/Cr ratio all presented as a risk factor, with ORs 1.38 (p = 0.041) and 1.33 (p = 0.014) in short- and long-duration groups, respectively.
Conclusion: Although renal functions presented a significant association with DR in all DM patients, the risk factors of DR varied widely in different disease-duration subjects. Target strategies to prevent DR should be put forward individually, considering the patient’s DM duration. Improving the BUN/Cr ratio may be beneficial to delaying DR.
Keywords: diabetic retinopathy, clinical factors, C-peptide, BUN/Cr ratio, risk factors analyses
Introduction
In persons of working age, diabetic retinopathy (DR), a frequent microvascular consequence of diabetes, is the main factor contributing to irreversible vision loss. According to a global meta-analysis, diabetic retinopathy has been identified in close to one-third of diabetic individuals. It has been hypothesized that diabetic retinopathy is associated with a higher risk of systemic vascular problems, such as peripheral neuropathy, cardiovascular events, and nephropathy, all of which lower quality of life. Therefore, it is helpful to anticipate the state of diabetic retinopathy in a clinic by studying related risk factors.1,2
Numerous epidemiological researches, including a number of cross-sectional studies or cohort studies, have revealed the risk factors of diabetic retinopathy and attempted to prevent and treat the condition.3,4 Epidemiological information on diabetic retinopathy in the Chinese population is, however, still very scant, and the risk factors for the condition vary depending on the study’s design, grading criteria, and population sample. Numerous risk factors, such as a history of diabetes, high levels of glycosylated hemoglobin A1c (HbA1c), hyperglycemia, dyslipidemia, hypertension, and obesity, have been linked to the development of diabetic retinopathy.5,6
In China, the prevalence of diabetes mellitus (DM) has significantly increased over decades, creating a serious health issue.7,8 It has been projected that 12% of individuals have DM, and almost half of the adults have a state of pre-diabetes in China. As a major complication of DM, patients with DM usually develop diabetic retinopathy (DR). It was acknowledged as one of the major causes of vision loss and blindness.7,9,10 A high prevalence of DR among adults has been found in epidemiological studies (varying from 11.9% to 43.1%), individuals with DM, and this would further increase the risk of cardiovascular diseases and diabetic nephropathy.11–15 The lack of early diagnosis and effective therapies targeting DR is mainly responsible for the problem. These suggest that to prevent DR, it is vital to investigate the risk factors for DR and present focused prevention solutions.
Using data from China, Sweden, and America, the relationship between DR and various risk factors in individuals with DM was explored in previous observational studies.7,11,12,15–18 Some of these researches focused on clinical factors, such as body mass index (BMI) and systolic blood pressure (SBP).7,17–19 Diabetes duration is a significant risk factor for DM. Well, there are different risk factors between long and short diabetes duration. Several types of research studies have shown that risk factors were controversial. However, the results of these studies were still controversial, especially in terms of the duration of DM. Patients with different DM durations may be affected by various risk factors, widely.15–18 Other studies have reported that diabetic nephropathy was expressively linked with DR in patients with type 2 diabetes mellitus. However, the pathophysiology linking these two microvascular problems has not yet been thoroughly demonstrated. The literature that explored the associations between BUN/Cr and DR was still limited.20,21 In the present study, we hypothesized that kidney functions may significantly influence the DR, and the duration of DM would modify the effects of selected risk factors.
Using data from patients who were enrolled in the standardized metabolic management center (MMC) management. This study aimed to find various risk factors of DR, including demographic variables, body measurement indicators, and laboratory data, and explore whether the effects of these selected risk factors were discrepant between different duration of DM groups.
Materials and Methods
Study Population
By using the data obtained from patients who were enrolled in the standardized metabolic management center (MMC) management at Jinan Central Hospital Affiliated with Shandong First Medical University from 1 July 2020 to 30 December 2021. The following respondents were excluded from the study: (1) patients who were older than 75 or life expectancy shorter than 5 years; (2) patients with infection, liver disease, or progression or exacerbation of kidney disease; (3) patients having type 1 diabetes or any other types of diabetes. In this current study, 1127 patients with DM were enrolled. In these subjects, individuals without assessment of DR (n = 69) were excluded. Finally, 1058 DM patients (621 males with a mean age of 58.8 years at baseline) were included in the present study. The risk factors and the diagnosis of DR were examined at the first visit.
Data Collection
At the baseline and follow-up visits, data collection was carried out at local community clinics by trained study staff following a standard methodology. Trained interviewers distributed a questionnaire that asked questions on demographic details, lifestyle factors (such as drinking and smoking), family history, and medical history. Body mass index (BMI) was computed by dividing weight in kilograms by height in meters squared after height, and body weight were measured per a recognized technique.22 After an overnight fast of at least 10 hours, each participant conducted an oral glucose tolerance test. Blood samples were taken at 0 and 2 hours during the test. Under a strict quality control procedure, fasting and 2-hour plasma glucose concentrations were determined locally using a glucose oxidase or hexokinase technique within 2 hours of blood sample collection. High-performance liquid chromatography was used to determine the HbA1c in venous blood samples. Only fasting plasma glucose and HbA1c were tested in individuals with self-reported diabetes. An automatic biochemical analyzer was used to measure the levels of fasting plasma glucose, two-hour plasma glucose, serum total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and triglycerides. The ALT measured by IFCC, AST, UA, and BUN was measured by chemistry colorimetry, and GTT was measured by enzymatic colorimetry. Thyroid function was measured by the method of chemiluminescence. Cr was measured by enzymic method. Hcy was measured by enzymatic cycling methods.
Outcome
All patients got a thorough ophthalmic examination that included measuring intraocular pressure, visual acuity, examining the anterior segment with a slit lamp, and examining the fundus with direct and indirect ophthalmoscopy following dilation. Microaneurysm, dot-and-blot hemorrhages, hard exudates, cotton-wool spots, venous beading, intra-retinal microvascular abnormalities, retinal new vessels, vitreous hemorrhage, fibrous proliferation, tractional retinal detachments, or prior laser therapy were all used to identify and classify DR.23 Any DR had to have at least one distinct microaneurysm in either one or both of the eyes.
Statistical Methods
The distributions of diabetic retinopathy rate across the quantile of C-peptide and BUN/Cr ratio were described by bar charts. Multivariate logistic regression models were used to explore the risk factors of diabetic retinopathy. The important variables were selected using backward stepwise regression based on AIC. Once the best-fitting model was selected, we used it to predict the rate of diabetic retinopathy, and its performance of prediction was presented using Receiver Operating Characteristic (ROC) and Area Under the Curve (AUC). Furthermore, we defined long duration as their diabetes mellitus duration of more than 130 months (50th of the subjects) and divided the participants into subgroups. Stratification analyses were used to explore the different effects of selected variables in subgroups.
Individual characteristics were described and grouped by diabetic retinopathy. Variables were described using mean (SD), median [IQR] and n (%), as appropriate. Differences in these variables were assessed by a 2-sample t-test, Wilcoxon rank-sum test and chi-square test or Fisher exact test, as appropriate. All analyses were performed using R version 4.0.4. Hypothesis tests were 2-sided, and we considered p <0.05 as statistically significant.
Results
Table 1 shows baseline characteristics of the study variables by the diabetic retinopathy. Compared with the non-diabetic retinopathy group, those who developed diabetic retinopathy were more likely to be elders with higher baseline SBP, Cr, BUN, HbA1c, and urine protein, and their baseline C-peptide, Hb, RBC, HCT and urine Cr were lower than the non-diabetic retinopathy group.
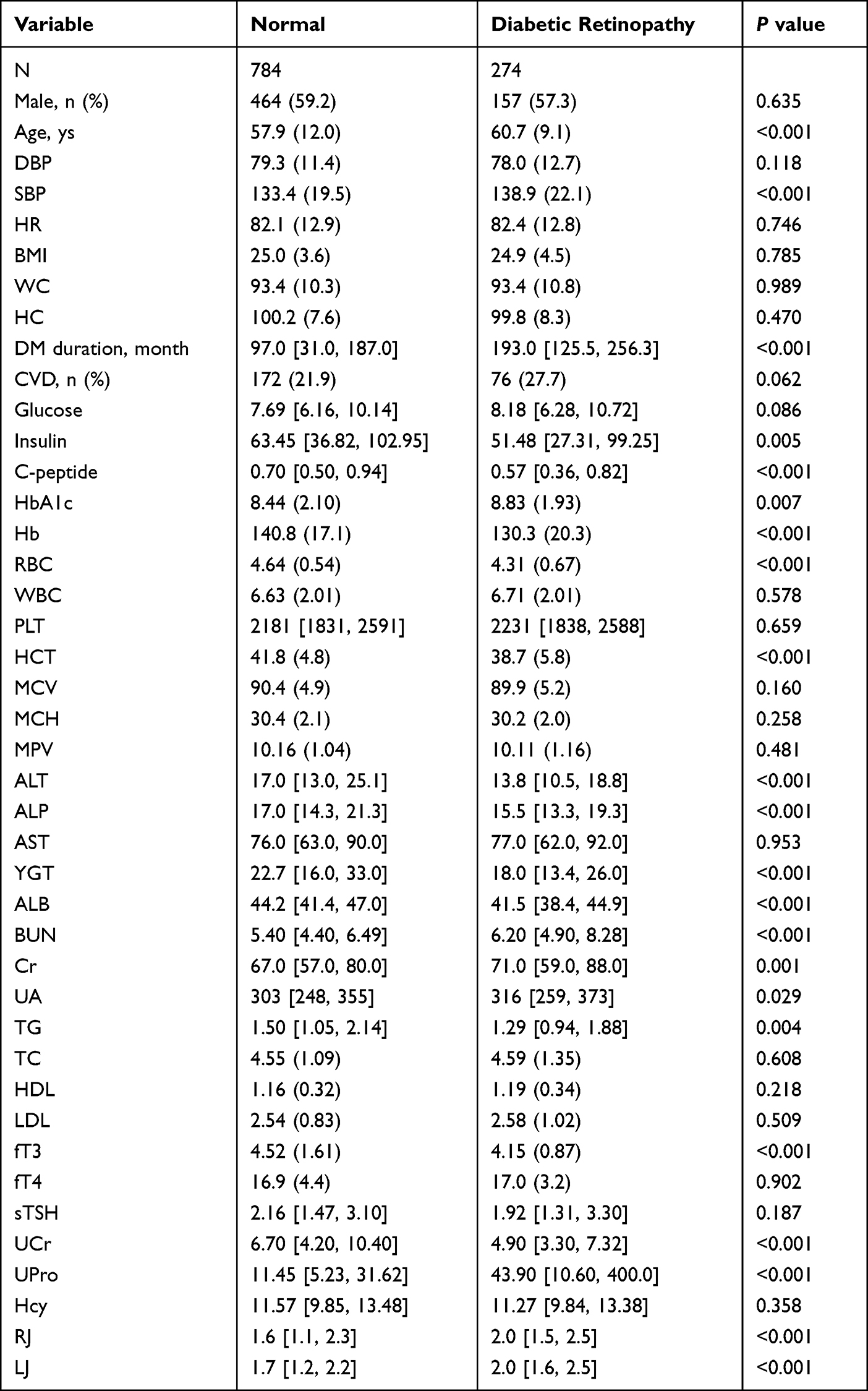 |
Table 1 The Baseline Characteristics of Participants by Diabetic Retinopathy |
DBP; Diastolic Blood pressure, SBP; Systolic blood pressure, HR; Heart Rate, BMI; Body mass index, WC; White blood cells, HC; Hematocrit; DM; Diabetes Mellitus, CVD; Cardiovascular diseases, HbA1c; Glycated hemoglobin, Hb; Hemoglobin, RBC; Red blood cells, WBC; White blood cells, PLT; Platelets, HCT; Hematocrit, MCV; Mean corpuscular volume, MCH; Mean Corpuscular Hemoglobin, MPV; Mean platelet volume ALT; Alanine transaminase, ALP; Alkaline phosphatase, AST; Aspartate aminotransferase, Gamma-glutamyl transferase, ALB; Albumin blood, BUN; Blood Urea Nitrogen, CR; Creatinine, UA; Urine analysis, TG; Triglycerides level, TC; Total count, HDL; High-density lipoproteins, HDL; High-density lipoproteins, FT3; free triiodothyronine, FT4; free thyroxine, STSH; Thyroid stimulating hormones, UCR; Urea and creatinine concentration, Upro; Urine protein quantitative, Hcy; Homocysteine, RJ: Right-carotid artery intima-media thickness, LJ: left-carotid artery intima-media thickness.
A continuous variable’s mean (SD) or median (IQR) values are displayed. Variables with a categorical nature are shown as n (%). Body mass index, or BMI;
Figure 1 showed the distribution of the diabetic retinopathy rate grouped by quantiles of DM duration. As compared with the quantile 4 group, the incidence of DR was significantly higher in the quantile 4 group.
 |
Figure 1 Rate of diabetic retinopathy in diabetes patients, across different categories of diabetes mellitus duration. |
Figure 2 showed the distribution of the diabetic retinopathy rate grouped by quantiles of C-peptide. Compared with the quantile 4 group, the diabetic retinopathy rate was significantly higher in the quantile 1 group. While the distribution of the diabetic retinopathy rate grouped by quantiles of the BUN/Cr ratio was shown in Figure 3. Compared with the quantile 1 group, individuals in the quantile 4 group were more likely to develop diabetic retinopathy, and these results remained consistent in males and females.
 |
Figure 2 Rate of diabetic retinopathy in the diabetes patients, across different categories of C-peptide group. |
 |
Figure 3 Rate of diabetic retinopathy in the diabetes patients, across different categories of BUN/Cr group. |
Table 2 presented standardized odds ratios (ORs) and 95% CIs between study variables and diabetic retinopathy. The results showed that age, level of C-peptide, HCT, and urine Cr were protective factors with the ORs 0.79 (0.62, 0.99), 0.75 (0.61, 0.91), 0.64 (0.52, 0.78), and 0.70 (0.52, 0.93), respectively. Inversely, SBP, diabetes mellitus duration, BUN/Cr ratio, urine protein and the thickness of the right-carotid artery were considered as risk factors with ORs 1.21 (1.01, 1.46), 1.74 (1.42, 2.13), 1.33 (1.11, 1.59), 1.55 (1.30, 1.84), and 1.30 (1.08, 1.57), respectively. The ROC and AUC of the rate of diabetic retinopathy prediction model were shown in Figure 4. It presented that AUC is equal to 0.786, which means that the effect of prediction is well.
 |
Table 2 Odds Ratios and 95% CI of the Diabetic Retinopathy |
 |
Figure 4 The diabetic retinopathy prediction model’s receiver operating characteristic curve and area under the curve. |
SBP; Systolic blood pressure, DM; Diabetes Mellitus, HCT; Hematocrit, BUN/Cr; Blood Urea Nitrogen/creatinine, UCr; Urea and creatinine concentration, UPr; Urine protein quantitative, RJ; Right-carotid artery intima-media thickness.
The diabetes mellitus duration was usually considered a major risk factor of diabetic retinopathy. We further defined long duration as diabetes mellitus duration of more than 130 months, and stratification analyses were used to explore the different effects of the selected variables on diabetic retinopathy in different subgroups. Table 3 presented the different effects in short-duration patients and long-duration patients. In the short-duration group, females usually presented a lower rate of diabetic retinopathy than males whose OR was 0.39 (0.18, 0.84), and the baseline SBP was a risk factor with OR 1.56 (1.14, 2.15). While in those long-duration patients, the effects of gender and SBP were no longer significant. Inversely, the levels of C-peptide and urine Cr showed protective effects, with ORs 0.61 (0.47, 0.78) and 0.60 (0.39, 0.89).
 |
Table 3 Influence Factor of the Diabetic Retinopathy by Diabetes Mellitus Duration |
Discussion
In the current study, we identified 10 risk factors for DR in patients with DM in China and discovered that the impact of diverse risk variables on DR varied greatly in groups with various levels of diabetes mellitus duration. Kidney functions should be given more consideration in all DM patients as they were strongly connected with DR in both long-duration and short-duration individuals with DM. Notably, in short-duration patients and long-duration patients, respectively, the effects of SBP and C-peptide on DR were found. This would support the idea of target prevention of DR in people with DM. Additionally, a prediction model with respectable prediction performance was created utilizing these chosen risk factors. Our findings suggest that, in order to prevent DR in DM patients, renal functioning should be given more thought. DR prevention techniques that are specific to the different stages of DM patients should be promoted.
In this research, the occurrence of DR in those with DM was 25.9%, and the study variables were expressively discrepant in the DR groups, as compared with those without DR. Previous studies, using data from China, have reported that the occurrence of DR was high in DM patients, with the prevalence ranging from 11.9% to 43.1%,11–13 which was in line with our result. Furthermore, the results of univariate analyses showed that those developed DR were more likely elders with higher baseline SBP, HBA1c and urine protein, longer duration of DM, and with lower C-peptide and urine creatinine, compared with those without DR. Previous studies have explored the relationship between DR and various risk factors.11–13,24–26 Trott et al reported that SBP and obesity would cause DR,24 while Rajalakshmi et al proved that HBA1c was an important risk factor for pre-diabetes,25 which was consistent with our current study. Besides these widely reported risk factors, we also discovered that kidney functions, such as urine protein and urine creatinine, were significantly associated with DR in DM patients. To our knowledge, this literature was still limited, especially in Chinese patients.
According to epidemiological data, there are currently 3.82 billion people worldwide who have been diagnosed with diabetes, of whom 1.26 billion have diabetic retinopathy and about 370 million have serious complications that pose a threat to their vision. This is a significant burden on the world’s health-care system and has a negative impact on patients’ daily activities and quality of life.27,28 The majority of diabetic chronic microvascular consequences include renal and retinal vascular impairment, which might hasten the development of cardiovascular disease.29,30 Therefore, identifying additional risk factors for diabetic retinopathy is crucial. Age, plasma glucose, blood lipids, blood pressure, HbA1c, and obesity are risk factors for diabetic retinopathy, according to earlier research.31,32
Notably, the results of univariate analyses may be affected by various confounders. We then established multivariate models to explore the risk factors of DR and used a backward stepwise regression strategy to select the best-fitting model. Our current study selected 10 important factors, including gender, baseline age, SBP, the duration of DM, C-peptide, HCT, BUN/Cr ratio, the thickness of the right carotid, and urine protein and creatinine. Qian et al have illustrated that males would more likely develop DR, compared with females.33 However, in the current study, gender was not expressively associated with DR. It may be caused by different study samples. Baseline SBP and the duration of DM were widely reported as major risk factors of DR in previous research.24–26,33,34 Liu et al demonstrated that higher SBP would cause DR, with OR and 95% CI 1.44 (1.19, 1.76).35 However, Hua et al discovered that those who developed DR were usually males, with a longer duration of DM, compared with those non-DR patients.34 These findings were consistent with the current research. However, a prior study found that DR risk factors included baseline age.36 In our study, baseline age was analyzed in univariate analyses as a risk factor and, conversely, in multivariate models as a protective factor. The interaction of the study’s factors may be to blame for this. Hua et al used univariate analysis to simply look at the relationship between age and DR, ignoring the influence of covariates.22
In the current study, C-peptide was found as a protective factor in our study, which was in line with previous reviews.36 The C-peptide was generally considered as an indicator of pancreas islet functions.36 Our result supported that individuals with DM should control the functions of the pancreas islet to prevent DR, and C-peptide may be a wonderful indicator to be monitored.36 Furthermore, HCT was considered as a protective factor, whose OR and 95 CI was 0.64 (0.52, 0.78) and was similar to a previous study.37 Besides these above, our current study also focused on the relationship between kidney functions and DR. We found urine protein was a risk factor for DR, while urine creatinine could prevent the DR, inversely. Previous research has demonstrated that DR patients would usually combine with kidney diseases.14,38,39 The DR would injure the blood vessel structure and further cause kidney diseases.14 However, the studies which explored the influence of kidney functions on DR were still limited, especially in terms of Chinese patients. Wang et al reported that diabetic kidney disease may present a risk effect on DR, and this effect was modified by anemia.38 Hwang et al using data from Korea has illustrated that the urine albumin-to-creatinine ratio was correlated with DR.40 However, this evidence would not be sufficient according to the results generated by univariate analyses, which could not control the effects of confounders, and they did not focus on urine protein and urine creatinine, separately.40 Our results provided evidence that the effects of urine protein and creatinine were opposite, and individuals with DM should control kidney functions to prevent DR.
In our study, we found another stable and readily available indicator of renal impairment, BUN/Cr. BUN/Cr ratio is used to assess prerenal azotemia, acute tubular necrosis and dehydration, with a threshold of 20. Our study showed that the prevalence of DR increased gradually with the increase of the BUN/Cr ratio. This has not been seen in previous reports. Before significant renal impairment, an elevated BUN/Cr ratio represents a state of water deficiency in the body. Water deficiency may lead to relative retinal vascular hypoperfusion. Enrico’s study showed that there is an association between choroidal capillary hypoperfusion and photoreceptors in non-proliferative diabetic retinopathy.41
Furthermore, we carried out a stratification analysis to explore the different effects of selected variables in different DM duration groups. We discovered that SBP may affect individuals with a short duration of DM, while the protective effect of C-peptide may only act on those with long disease duration. Previous studies recognized the duration of DM as an important risk factor of DR.42–44 However, these researchers only treated the duration of DM as a continuous variable, ignoring its modifiable effect on other variables. Even the same variable, like SBP, may cause different effects in disparate sub-groups. Our study investigated the controllable impact of DM duration on other variables and offered support for China’s targeted DR prevention. Due to their variable risk factors, DM patients may be split into different disease-duration sub-groups. Furthermore, both the short-duration and long-duration groups consistently showed a strong association between renal functions and DR, suggesting that DM patients should focus more on enhancing kidney functions to prevent DR.
There exist some strengths in the present study. Firstly, the current study is a large sample size research with comprehensive measurements. It allows us to explore the risk factors of DM, especially in terms of kidney functions. Secondly, using stratification analysis, we demonstrate that the effects of selected variables on DR are different in the short-duration group and long-duration group, which could provide evidence on the strategies of prevention DR. On the other hand, some limitations should be acknowledged. Firstly, our study was a single-center design within Chinese DM patients, which would reduce the generalization of the results. Moreover, the influences of unobserved confounders were unavoidable in observational studies. Although we have adjusted the confounders as possible as we can, there may still exist other variables that affected the results. Our results could provide evidence on target prevention strategies of DR. Further researches need to carry out a randomized clinical trial to verify the results. Finally, the missing data may disturb the results we discovered. The vitamins may also affect the occurrence of DR in patients with DM. However, our data on vitamin variables miss severely. Further studies need to consider the effects of vitamins, comprehensively.
Conclusions
In this study, we assessed the risk factors for DR in people with diabetes and discovered that different variables may have an impact on individuals with varying DM durations. It’s particularly crucial to consider each patient with DM’s DR prevention. Women with short-duration DM should manage their blood pressure, while women with long-duration DM may benefit from preventing DR by monitoring their C-peptide levels. Additionally, the BUN/Cr ratio would affect all DM patients, suggesting that glomerular filtration functions should receive more attention to prevent DR. The aim DR prevention techniques should be presented on an individual basis, taking into account the patients’ DM duration. Enhancing glomerular filtration capabilities may help postpone DR. Our findings might help with specialized DR prevention initiatives. The following study must undertake a randomized clinical trial to verify the results. Last but not least, the absence of data can invalidate our conclusions. The vitamins might affect DR in people with diabetes.
Institutional Review Board Statement
The Institutional Review Board at Jinan Central Hospital approved the study (approval no. 2020-124-01), which was carried out following the Declaration of Helsinki.
Data Sharing Statement
On reasonable request, the corresponding author will provide the information supporting the study’s conclusions.
Waiver of Informed Consent
This study utilized patient data and clinical baseline information from our institution’s standardized metabolic management center. Patient information was strictly confidential, and the study did not involve any data that could link subjects to their identities. It did not adversely affect patients’ rights or health, and there was no conflict of interest regarding patients’ benefits. Due to the objective inability to obtain informed consent from subjects, exemption from informed consent was granted.
Acknowledgments
This study was supported by Jinan Central Hospital and Qu Yanlin helped with data analysis.
Funding
The financial support for this study was provided by the Shandong Province Key R&D Plan (Grant No. 2016GSF201019), Jinan Science and Technology Innovation Program of Clinical Medicine (Grant No. 201705072), Latitudinal project of Shandong University (Grant No. 6020320001), Shandong Province Postdoctoral Innovation Program (Grant No. SDCX-ZG-202202004), and Academic promotion program of Shandong First Medical University (Grant No. 2019QL025).
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. Yau JW, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–564. doi:10.2337/dc11-1909
2. Liu Y, Yang J, Tao L, et al. Risk factors of diabetic retinopathy and sight-threatening diabetic retinopathy: a cross-sectional study of 13 473 patients with type 2 diabetes mellitus in mainland China. BMJ open. 2017;7(9):e016280. doi:10.1136/bmjopen-2017-016280
3. Zhang X, Saaddine JB, Chou C-F, et al. Prevalence of diabetic retinopathy in the United States, 2005–2008. JAMA. 2010;304(6):649–656. doi:10.1001/jama.2010.1111
4. Wang Y, Lin Z, Zhai G, et al. Prevalence of and risk factors for diabetic retinopathy and diabetic macular edema in patients with early-and late-onset diabetes mellitus. Ophthalmic Res. 2022;65(3):293–299. doi:10.1159/000508335
5. Ting DSW, Cheung GCM, Wong TY. Diabetic retinopathy: global prevalence, major risk factors, screening practices and public health challenges: a review. Clin Experiment Ophthalmol. 2016;44(4):260–277. doi:10.1111/ceo.12696
6. Kuo JZ, Wong TY, Rotter JI. Challenges in elucidating the genetics of diabetic retinopathy. JAMA Ophthalmol. 2014;132(1):96–107. doi:10.1001/jamaophthalmol.2013.5024
7. Zhang G, Chen H, Chen W, et al. Prevalence and risk factors for diabetic retinopathy in China: a multi-hospital-based cross-sectional study. Br J Ophthalmol. 2017;101(12):1591–1595. doi:10.1136/bjophthalmol-2017-310316
8. Chen C, Sun Z, Xu W, et al. Associations between alcohol intake and diabetic retinopathy risk: a systematic review and meta-analysis. BMC Endocr Disord. 2020;20(1):1–10. doi:10.1186/s12902-020-00588-3
9. Fotouhi F, Rezvan F, Hashemi H, et al. High prevalence of diabetes in elderly of Iran: an urgent public health issue. J Diabetes Metab Disord. 2022;21(1):777–784. doi:10.1007/s40200-022-01051-x
10. Hammes H-P, Feng Y, Pfister F, et al. Diabetic retinopathy: targeting vasoregression. Diabetes. 2011;60(1):9. doi:10.2337/db10-0454
11. Pang C, Jia L, Jiang S, et al. Determination of diabetic retinopathy prevalence and associated risk factors in Chinese diabetic and pre‐diabetic subjects: shanghai diabetic complications study. Diabetes Metab Res Rev. 2012;28(3):276–283. doi:10.1002/dmrr.1307
12. Wang FH, Liang YB, Peng XY, et al. Risk factors for diabetic retinopathy in a rural Chinese population with type 2 diabetes: the Handan eye study. Acta Ophthalmol. 2011;89(4):e336–e343. doi:10.1111/j.1755-3768.2010.02062.x
13. Xu J, Wei WB, Yuan MX, et al. Prevalence and risk factors for diabetic retinopathy: the Beijing Communities Diabetes Study 6. Retina. 2012;32(2):322–329. doi:10.1097/IAE.0b013e31821c4252
14. Foussard N, Saulnier P-J, Potier L, et al. Relationship between diabetic retinopathy stages and risk of major lower-extremity arterial disease in patients with type 2 diabetes. Diabetes Care. 2020;43(11):2751–2759. doi:10.2337/dc20-1085
15. Wykoff CC, Khurana RN, Nguyen QD, et al. Risk of blindness among patients with diabetes and newly diagnosed diabetic retinopathy. Diabetes Care. 2021;44(3):748–756. doi:10.2337/dc20-0413
16. Rathsman B, Haas J, Persson M, et al. LDL cholesterol level as a risk factor for retinopathy and nephropathy in children and adults with type 1 diabetes mellitus: a nationwide cohort study. J Intern Med. 2021;289(6):873–886. doi:10.1111/joim.13212
17. Bek T. Incidence and risk for developing proliferative diabetic retinopathy after photocoagulation for diabetic maculopathy. Curr Eye Res. 2020;45(8):986–991. doi:10.1080/02713683.2020.1712729
18. Cao K, Wang B, Friedman DS, et al. Diabetic retinopathy, visual impairment, and the risk of six-year death: a cohort study of a rural population in China. Ophthalmic Res. 2021;64(6):983–990. doi:10.1159/000512667
19. Park Y-H, Shin JA, Han J-H, et al. The association between chronic kidney disease and diabetic retinopathy: the Korea national health and nutrition examination survey 2008–2010. PLoS One. 2015;10(4):e0125338. doi:10.1371/journal.pone.0125338
20. Jiang W, Wang J, Shen X, et al. Establishment and validation of a risk prediction model for early diabetic kidney disease based on a systematic review and meta-analysis of 20 cohorts. Diabetes Care. 2020;43(4):925–933. doi:10.2337/dc19-1897
21. Vujosevic S, Aldington SJ, Silva P, et al. Screening for diabetic retinopathy: new perspectives and challenges. Lancet Diabetes Endocrinol. 2020;8(4):337–347. doi:10.1016/S2213-8587(19)30411-5
22. Craig CL, Marshall AL, Sj??str??m M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
23. Flaxel CJ, Adelman RA, Bailey ST, et al. Diabetic retinopathy preferred practice pattern®. Ophthalmology. 2020;127(1):P66–p145. doi:10.1016/j.ophtha.2019.09.025
24. Trott M, Driscoll R, Pardhan S. Associations between diabetic retinopathy and modifiable risk factors: an umbrella review of meta-analyses. Diabet Med. 2022;39(6):e14796. doi:10.1111/dme.14796
25. Rajalakshmi R, UmaSankari G, Sivaprasad S, et al. Prevalence and risk factors for diabetic retinopathy in prediabetes in Asian Indians. J Diabetes Complications. 2022;36(3):108131. doi:10.1016/j.jdiacomp.2022.108131
26. Zhang Y, Pan GP, Cai JW, Niu YM, Xie LC. Association between transcription factor 7-like 2 C/T polymorphism and diabetic retinopathy risk: a meta-analysis. Ophthalmic Res. 2022;66:66–74.
27. Ogurtsova K, da Rocha Fernandes JD, Huang Y, et al. IDF diabetes atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50. doi:10.1016/j.diabres.2017.03.024
28. Gangwani RA, Lian JX, McGhee SM, et al. Diabetic retinopathy screening: global and local perspective. Hong Kong Med J. 2016. doi:10.12809/hkmj164844
29. Grunwald JE, Ying G-S, Maguire M, et al. Association between retinopathy and cardiovascular disease in patients with chronic kidney disease (from the Chronic Renal Insufficiency Cohort [CRIC] Study). Am J Cardiol. 2012;110(2):246–253. doi:10.1016/j.amjcard.2012.03.014
30. Son J-W, Jang E-H, Kim M-K, et al. Diabetic retinopathy is associated with subclinical atherosclerosis in newly diagnosed type 2 diabetes mellitus. Diabetes Res Clin Pract. 2011;91(2):253–259. doi:10.1016/j.diabres.2010.11.005
31. Cunha-Vaz J, Ribeiro L, Lobo C. Phenotypes and biomarkers of diabetic retinopathy. Prog Retin Eye Res. 2014;41:90–111. doi:10.1016/j.preteyeres.2014.03.003
32. Chen D, Sun X, Zhao X, et al. Associations of serum uric acid and urinary albumin with the severity of diabetic retinopathy in individuals with type 2 diabetes. BMC Ophthalmol. 2020;20(1):1–5. doi:10.1186/s12886-020-01713-5
33. Qian J, Haq Z, Yang D, et al. Male sex increases the risk of diabetic retinopathy in an urban safety-net hospital population without impacting the relationship between axial length and retinopathy. Sci Rep. 2022;12(1):9780. doi:10.1038/s41598-022-13593-4
34. Hua R, Qu L, Ma B, et al. Diabetic optic neuropathy and its risk factors in Chinese patients with diabetic retinopathy. Invest Ophthalmol Vis Sci. 2019;60(10):3514–3519. doi:10.1167/iovs.19-26825
35. Liu L, Quang ND, Banu R, et al. Hypertension, blood pressure control and diabetic retinopathy in a large population-based study. PLoS One. 2020;15(3):e0229665. doi:10.1371/journal.pone.0229665
36. Bhatt MP, Lim YC, Ha KS. C-peptide replacement therapy as an emerging strategy for preventing diabetic vasculopathy. Cardiovasc Res. 2014;104(2):234–244. doi:10.1093/cvr/cvu211
37. Zhang P, Huang X-B, Xu Y, et al. Prevalence and risk factors of diabetic retinopathy in patients with type 2 diabetes in Shanghai. Int J Ophthalmol. 2021;14(7):1066–1072. doi:10.18240/ijo.2021.07.16
38. Wang J, Xin X, Luo W, et al. Anemia and diabetic kidney disease had joint effect on diabetic retinopathy among patients with type 2 diabetes. Invest Ophthalmol Vis Sci. 2020;61(14):25. doi:10.1167/iovs.61.14.25
39. Hung CC, Lin HY-H, Hwang D-Y, et al. Diabetic retinopathy and clinical parameters favoring the presence of diabetic nephropathy could predict renal outcome in patients with diabetic kidney disease. Sci Rep. 2017;7(1):1236. doi:10.1038/s41598-017-01204-6
40. Hwang H, Kim JY, Oh TK, et al. Relationship between clinical features of diabetic retinopathy and systemic factors in patients with newly diagnosed type II diabetes mellitus. J Korean Med Sci. 2020;35(23):e179. doi:10.3346/jkms.2020.35.e179
41. Borrelli E, Palmieri M, Viggiano P, et al. Photoreceptor damage in diabetic choroidopathy. Retina. 2020;40(6):1062–1069. doi:10.1097/IAE.0000000000002538
42. Huang JX, Liao YF, Li YM. Clinical features and microvascular complications risk factors of early-onset type 2 diabetes mellitus. Curr Med Sci. 2019;39(5):754–758. doi:10.1007/s11596-019-2102-7
43. Çolak S, Kazanci B, Ozçelik Soba D, et al. Effects of diabetes duration and HgA1C level on corneal endothelial morphology. Eur J Ophthalmol. 2021;31(3):967–975. doi:10.1177/1120672120914812
44. Crabtree GS, Chang JS. Management of complications and vision loss from proliferative diabetic retinopathy. Curr Diab Rep. 2021;21(9):33. doi:10.1007/s11892-021-01396-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Non-Linear Relationship Between Fasting C-Peptide and Retinopathy in Patients with Type 2 Diabetes Mellitus - A Retrospective Study
Ma J, Han C, Lv Y, Cai H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1035-1045
Published Date: 7 April 2025