Back to Journals » International Journal of General Medicine » Volume 18
Risk Factors for Depression and Nomogram Prediction Among Chinese Coronary Heart Disease Patients: A Multi-Center Study from 2016 to 2018
Authors Tong H ![]() , Zhang J
, Zhang J ![]() , Jiang L, Dong L, Hu J
, Jiang L, Dong L, Hu J
Received 7 March 2025
Accepted for publication 10 April 2025
Published 16 June 2025 Volume 2025:18 Pages 3215—3226
DOI https://doi.org/10.2147/IJGM.S523513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Hongxuan Tong,1,* Jiale Zhang,1,* Lijie Jiang,1 Lei Dong,2 Jiatong Hu3
1Institute of Basic Theory for Chinese Medicine, China Academy of Chinese Medical Sciences, Beijing, 100700, People’s Republic of China; 2Breast Department, Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China; 3Acupuncture Department, Guang ‘anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongxuan Tong, Institute of Basic Theory for Chinese Medicine, China Academy of Chinese Medical Sciences, No. 16 Nanxiao Street of Dongzhimennei, Dongcheng District, Beijing, People’s Republic of China, Email [email protected] Jiatong Hu, Doctor, Acupuncture Department, Guang ‘anmen Hospital, China Academy of Chinese Medical Sciences, No. 5, Beixiangge Street, Xicheng District, Beijing, People’s Republic of China, Email [email protected]
Background: This study aimed to assess the prevalence and identify risk factors associated with depression among coronary heart disease (CHD) patients at different stages in China.
Methods: Conducted as a hospital-based, cross-sectional study across 48 hospitals in 23 provinces, the research spanned from October 2016 to April 2018. A total of 9044 patients were initially recruited, with 8353 deemed eligible for participation. Depression was assessed using the nine-item Patient Health Questionnaire-9 (PHQ-9) Scale. Univariate analysis identified predictors of postoperative depression, and binary logistic regression analysis was employed to ascertain risk factors associated with depressive symptoms. The predictive model was constructed using the “rms” package in R software, demonstrating robust predictive capabilities according to the ROC curve.
Results: In general, both the degree and overall score based on the PHQ-9 revealed a trend: as the severity of the disease increased, so did the severity of patient depression. Univariate analysis indicated statistical differences concerning general situations and lifestyles. The binary logistic regression model highlighted the proximity of depression to risk factors such as gender, nationality, marital status, education, drinking, BMI, sleep disturbance, and disease status. Utilizing these findings, a predictive nomogram for depression was developed. The model exhibited excellent predictive ability, with an AUC of 0.768 (95% CI = 0.757– 0.780).
Conclusion: This study systematically investigated the prevalence of depression among coronary heart disease patients at various stages. As coronary heart disease advanced, the level of depression intensified. The nomogram developed in this study proves valuable in predicting the incidence of depression in coronary heart disease patients.
Keywords: coronary heart disease, risk factors, depression, nomogram, ROC curve
Introduction
Despite a decline in mortality rates, coronary heart disease (CHD) remains a leading cause of death worldwide, primarily due to heart ischemia.1 In 2020, CHD led to 380,000 deaths.2 Furthermore, cardiac events and/or surgery not only significantly diminish patients’ quality of life but also contribute to mental health issues, as previously reported.3 Reports indicate that nearly 30% of patients with CHD face psychological challenges, particularly depression, highlighting a critical concern is particularly acute in China, where 2,670 of 5236 CHD patients were accompanied by depression from 23 hospitals.4,5
Given the prevalence of psychological symptoms such as depression or anxiety, numerous global studies have explored depression as a risk factor for incident CHD or cardiovascular morbidity and mortality in patients with established CHD.6,7 The mechanisms underlying this comorbidity have not been fully elucidated. Cross-sectional studies consistently reveal a significant increase in depression incidence in CHD patients, while CHD incidence also rises considerably in patients with depression.8,9 Depression is widely acknowledged to play a pivotal role in CHD pathogenesis or, at the very least, act as a predisposing factor for CHD.10 Patients with CHD are prone to mental disorders, particularly depression, due to prolonged illness and an unsatisfactory prognosis.4 The intricate causal relationship between the two conditions has led to the combination of psychological treatments with traditional approaches to enhance outcomes. Treatment for depression in CHD patients typically involves antidepressant medications such as selective serotonin reuptake inhibitors (SSRIs, eg, sertraline, fluoxetine), often combined with psychological interventions like cognitive-behavioral therapy, to alleviate symptoms and improve cardiovascular outcomes.11
Several studies have demonstrated that the comorbidity of CHD and depression increases the risk of cardiovascular events and mortality, resulting in higher readmission rates and medical costs.12–14 However, despite advancements in clinical departments, psychological intervention and detection are infrequently implemented in cardiovascular clinical practice. In this study, we aim to construct a nomogram model for predicting depression risk in CHD patients based on a previous study that includes demographic characteristics, clinical features, psychological factors, and lifestyle. This model forms a robust foundation for early screening and intervention in depression risk among CHD patients. Therefore, we hope that this study serves as a reminder for doctors and patients to assess the risk of depression based on readily available information, such as the current disease stage and general data, facilitating early clinical prevention and intervention.
Materials and Methods
Study Design and Participants
This was a hospital-based, cross-sectional study approved by the Ethics Committee of Institute of Basic Theory for Chinese Medicine, China Academy of Chinese Medical Sciences (approval Document No. 2016EC_KY_001) on September 7, 2016. This study was registered on the WHO International Clinical Trial Registry (ClinicalTrial.gov) and the registered ID was NCT02967718. This cross-sectional study was conducted at 48 clinical research centers across 23 provinces over the period from 01/10/2016 to 30/4/2018. Before commencing the study, researchers underwent standardized training in interview procedures, covering the recruitment of patients and utilization of self-reported questionnaires. Subsequently, they conducted on-site face-to-face interviews and posed questions to respondents. When necessary, Supplementary Information was obtained from the respondents’ family members. Reference to the Declaration of Helsinki, all methods would be performed in accordance with the relevant guidelines and regulations.
The survey spanned five consecutive days in each department. Inclusion criteria were as follows: (1) age 18 or older, (2) meeting criteria for healthy control population, metabolic syndromic individuals, chronic coronary disease patients, acute coronary syndrome patients, post-PCI individuals, and heart failure patients, (3) voluntary participation with signed informed consent, and (4) completion of questionnaires independently.
Exclusion criteria encompassed: (1) patients with a history of hand surgery, fever, trauma, or burn infection within the past week, active tuberculosis, or rheumatic immune disease, (2) patients with severe arrhythmias accompanied by hemodynamic changes, (3) patients with acute or subacute cerebrovascular diseases, (4) those with valvular heart disease or primary cardiomyopathy, (5) patients with acute exacerbation of chronic obstructive pulmonary disease or pulmonary heart disease or respiratory failure, (6) individuals with renal insufficiency, serum creatinine levels higher than 221 μmol/L in males and 177 μmol/L in females, (7) patients with liver dysfunction, alanine aminotransferase levels higher than 3 times the normal value or combined with cirrhosis, (8) individuals with severe primary diseases such as hematopoietic system disorders or malignant tumors, (9) organ transplant patients, (10) those with severe mental disorders, and (11) pregnant and lactating women.
For participants who meet the requirements, we first sign informed consent and then proceed to follow-up studies. Patients were required to complete information collection questionnaires covering socio-demographic characteristics, the nine-item Patient Health Questionnaire-9 (PHQ-9) Scale, and lifestyle information (drinking, smoking, sleeping, etc.).
Assessment Instrument: PHQ-9
The Patient Health Questionnaire-9 (PHQ-9) stands out as one of the most widely utilized self-report psychosocial assessments for evaluating participants’ depressive symptoms over the preceding two weeks.15 Positioned as an integral component of individual health management,16 this tool is designed to identify depression through nine questions, each scored from 0 (not at all) to 3 (nearly every day), yielding a total score ranging from 0 to 27.17 Key breakpoints at 5, 10, 15, and 20 signify at least mild, moderate, moderately severe, and severe levels of depression.15 The Chinese version of the PHQ-9, employed in our study, has exhibited robust reliability and validity across diverse conditions, including healthcare settings and the general population.18,19
In our investigation, a total score of 5 or higher on the PHQ-9 indicates the presence of depression in respondents. To assess current suicidal or self-injurious ideation, we utilized the ninth item in the PHQ-9, which gauges thoughts related to being better off dead or engaging in self-harm (not at all 0; several days 1; more than half the days 2; nearly every day 3). A score of 1 or higher on this item indicates the presence of suicidal thoughts or self-harm concerns over the past two weeks.
Statistical Analysis
Statistical analysis was conducted using SPSS 20.0 and R 4.3.2 software. Descriptive analysis was employed to summarize socio-demographic and lifestyle characteristics. Binary logistic regression analysis was utilized to identify risk factors, with socio-demographic and lifestyle characteristics serving as independent variables, for depression within the entire population and different groups. The positive group, indicating the presence of depression as the main variable, was identified when the total score of PHQ-9 exceeded 4. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated, and statistical significance was considered when the two-sided P value was <0.05.
Result
Socio-Demographic and Characteristics
A total of 9,044 patients were initially recruited, with 8,353 (response rate: 92.4%) completing the PHQ-9 and included in the analysis. The mean age of the total enrolled participants was 61.91±12.50 years (range: 39–89 years), with 56.0% under 65 years and 44.0% aged 65 or older. Regarding gender, 52.7% were male, and 47.3% were female. The Han population comprised 94.3%, while the minority population was 5.7%. Religious beliefs were absent in 92.7% of participants, and 7.3% reported having religious beliefs. Marital status distribution was 1.0% unmarried, 92.0% married, and 7.0% divorced or widowed.
Employment status revealed 19.5% unemployed, 52.6% retired, and 27.9% employed. Educational background varied, with 20.7% having primary education or below, 53.5% secondary school education, and 25.8% high education or above. In terms of technical titles, 70.2% had no title, 7.9% had a primary title, 13.5% were in the middle class, and 8.3% were in the high class. Regular exercise was reported by 47.1%, while 52.9% did not engage in regular exercise. Alcohol consumption patterns showed 76.9% never drank, 13.8% were current drinkers, and 9.3% were former drinkers. Smoking habits indicated 72.2% were never smokers, 13.9% were current smokers, and 13.9% were former smokers. The mean score on the PHQ-9 was 3.29±3.64.
Based on BMI standards, 2.5% were underweight, 64.8% were of normal weight, and 32.7% were overweight. Regarding sleep quality, 74.7% reported normal sleep, while 25.3% reported poor sleep. The study included six distinct groups: healthy individuals, those with metabolic syndrome (MS), chronic coronary disease population, acute coronary syndrome patients, post-PCI individuals, and heart failure patients. Their mean ages were 50.77±10.87, 59.26±11.79, 65.17±10.174, 64.14±10.68, 63.62±10.67, and 71.84±10.86, respectively. Comparisons between individuals with and without depression across different factors were conducted; detailed results are presented in Table 1.
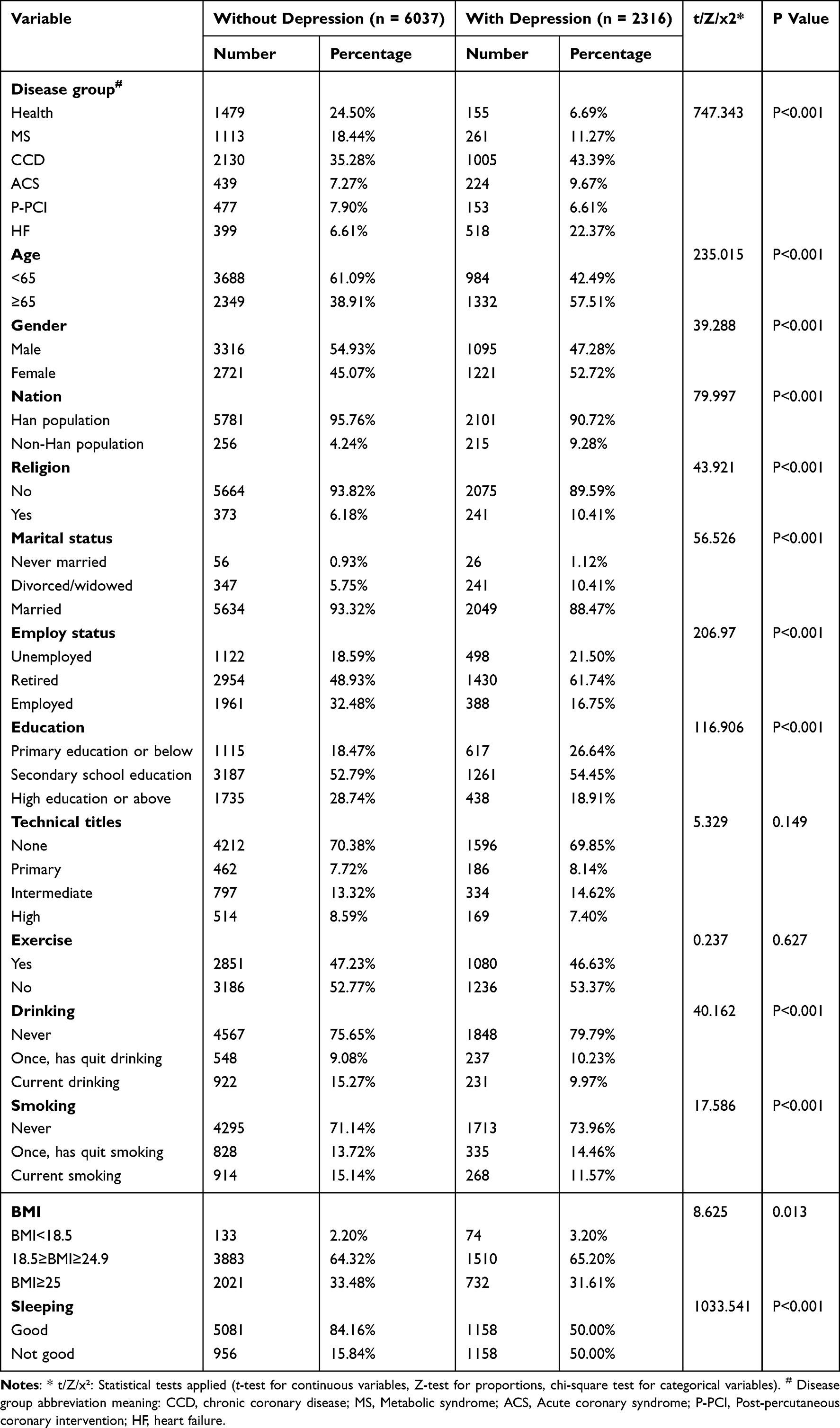 |
Table 1 Comparison of Different Factors Between Study Population with and without Depression |
Comparison of PHQ-9 Scores and Corresponding Depression Rates in Each Group
Within the entire population, the prevalence of depressive symptoms was 27.7% (2316/8353; 95% CI: 26.8–28.7%). Specifically, the prevalence of mild (PHQ-9 score: 5–9), moderate (PHQ-9 score: 10–14), and severe (PHQ-9 score: 15–27) depressive symptoms was 21.0% (1758/8353; 95% CI: 20.2–21.9%), 5.1% (424/8353; 95% CI: 4.6–5.6%), and 1.6% (134/8353; 95% CI: 1.4–1.9%), respectively. The prevalence of moderate to severe depressive symptoms (PHQ-9 score: 10–27) was 6.7% (558/8353, 95% CI: 6.2–7.2%). The scores and proportions of people with depressive symptoms among each group are depicted in Figure 1. Regarding detailed scores, pairwise comparisons among the six groups revealed statistical differences in each pair, except for the comparison between CCD and ACS, as well as the comparison between P-PCI and MS. Additionally, we presented the characteristics and comparison of subjects with and without depressive symptoms in different groups (see Supplement Table 1).
 |
Figure 1 The PHQ-9 score and proportion of depression degrees in different groups. (A) The PHQ-9 score for the six groups. (B) The proportion of depression degrees in different groups. |
Logistic Binary Regression Analysis of Risk Factors for Depression
We employed a binary logistic regression model to identify relevant factors associated with depressive and anxious symptoms in the entire population. The odds ratios (ORs) and 95% confidence intervals (CIs) are reported in Table 2. Significant risk factors for depressive symptoms include Gender (Male or Female) (OR=1.40; 95% CI: 1.22–1.61), Nation (Han or Minority) (OR=1.62; 95% CI: 1.24–2.11), Marital status: Never married (OR=1.70; 95% CI: 1.00–2.89), education: primary education or below (OR=1.40; 95% CI: 1.15–1.72), education: secondary school education (OR=1.26; 95% CI: 1.08–1.47), drinking: once, has quit drinking (OR=1.30; 95% CI: 1.02–1.66), BMI<18.5 (OR=1.78; 95% CI: 1.25–2.53), 18.5≥BMI≥24.9 (OR=1.23; 95% CI: 1.09–1.39), Sleep disturbance (OR=4.49; 95% CI: 4.00–5.04), Status: MS (OR=2.28; 95% CI: 1.79–2.92), Status: CAD (OR=3.54; 95% CI: 2.87–4.37), Status: ACS (OR=4.24; 95% CI: 3.28–5.48), Status: P-PCI (OR=3.14; 95% CI: 2.39–4.14), Status: HF (OR=8.79; 95% CI: 6.86–11.27).
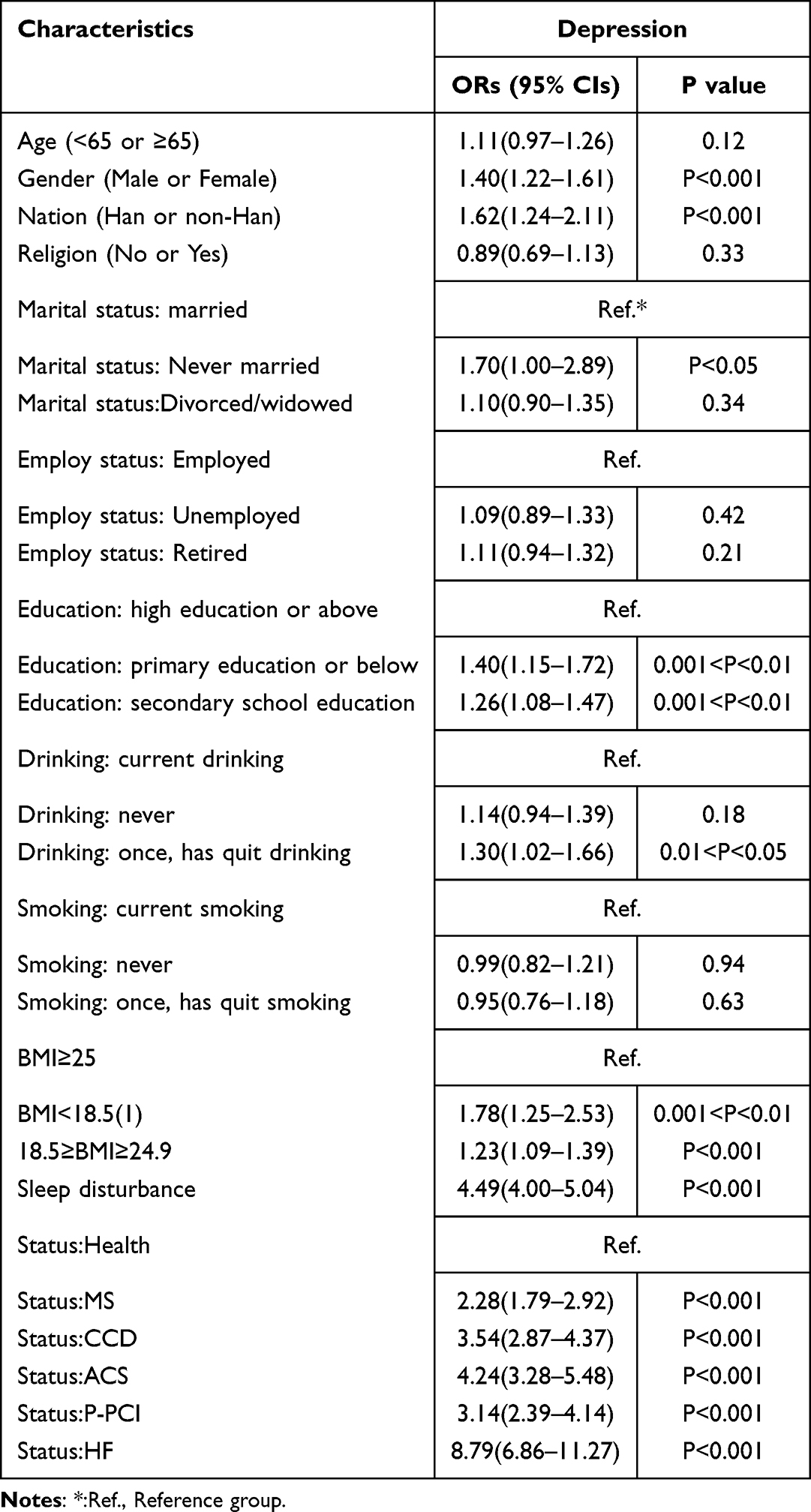 |
Table 2 The Binary Logistic Regression Analysis to Determine the Strongest Predictors of Depressive in All Population |
Risk factors identified for depression and anxiety in different groups respectively
Then we identify relevant factors for patients with depression in different groups by binary logistic regression model. Significant risk factors for depressive symptoms include (Table 3), Health group: age (<65 or ≥65) (OR=0.35; 95% CI: 0.17–0.73), Religion (No or Yes) (OR=2.03; 95% CI: 1.10–3.74), Sleep disturbance (OR=4.64; 95% CI: 3.13–6.90); MS group: Gender (Male or Female) (OR=1.62; 95% CI: 1.08–2.44), Marital status: Never married (OR=6.16; 95% CI: 1.79–21.29), 18.5≥BMI≥24.9 (OR=1.58; 95% CI: 1.15–2.18), Sleep disturbance (OR=5.23; 95% CI: 3.85–7.11); CCD group: age (<65 or ≥65) (OR=1.32; 95% CI: 1.09–1.59), Gender (Male or Female) (OR=1.68; 95% CI: 1.36–2.08), Marital status: Divorced/widowed (OR=1.40; 95% CI: 1.04–1.88), education: primary education or below (OR=1.45; 95% CI: 1.07–1.98), education: secondary school education (OR=1.30; 95% CI: 1.02–1.65), Sleep disturbance (OR=4.10; 95% CI: 3.46–4.85); ACS group: Nation (Han or Minority) (OR=3.09; 95% CI: 1.35–7.06) Religion (No or Yes) (OR=0.25; 95% CI: 0.10–0.59), Sleep disturbance (OR=3.81; 95% CI: 2.58–5.62); P-PCI group: education: secondary school education (OR=2.18; 95% CI: 1.03–4.62), technical titles: none (OR=0.28; 95% CI: 0.10–0.80), Sleep disturbance (OR=3.52; 95% CI: 2.23–5.56); HF group: Employ status: Retired (OR=2.48; 95% CI: 1.23–4.99), Sleep disturbance (OR=6.92; 95% CI: 4.96–9.67).
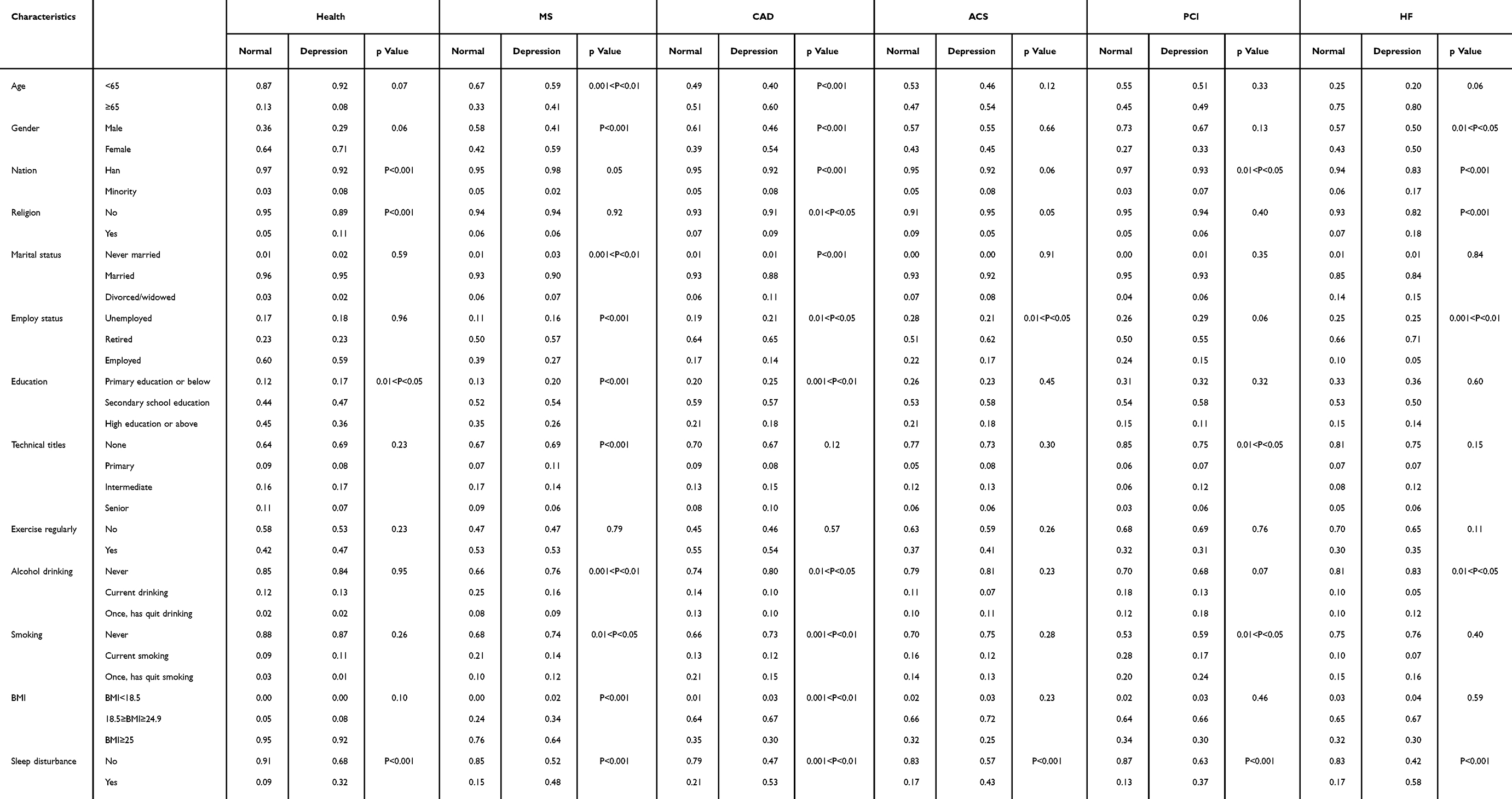 |
Table 3 Characteristics and Comparison of Subjects with and without Depressive Symptoms in Different Group |
Establishment of a Nomogram for Predicting Depression Risk
Utilizing logistic regression analysis, we developed a nomogram model to predict the risk of depression in coronary heart disease (Figure 2). Each factor was assigned a score ranging from 0 to 100, and the cumulative scores were computed to derive the total model score. The total score was then used to predict the risk probability of early depression in coronary heart disease. The risk of depression increases with the total score. The population categories were assigned numbers: 1 for health, 2 for metabolic syndrome, 3 for chronic coronary disease, 4 for acute coronary syndrome, 5 for post-PCI surgery, and 6 for heart failure patients. Gender was coded as 1 for male and 2 for female. Ethnicity was coded as 1 for Han ethnicity and 2 for non-Han ethnicity. Marital status was coded as 1 for unmarried, 2 for divorced and widowed, and 3 for married. Educational status was coded as 1 for primary education or below, 2 for secondary school education, and 3 for high education or above. Drinking status was coded as 1 for none, 2 for abstained, and 3 for still drinking. BMI was coded as 1 for BMI<18.5, 2 for BMI ≥ 18.5 and <24.9, and 3 for BMI ≥ 25. Sleep quality was coded as 0 for good and 1 for bad. Based on the ROC curve, the Area Under the Curve (AUC) value for our model in this study was 0.768 (95% CI: 0.757–0.786), indicating a certain level of accuracy and providing a valuable reference for assessing the risk of depression in patients with coronary heart disease (Figure 3).
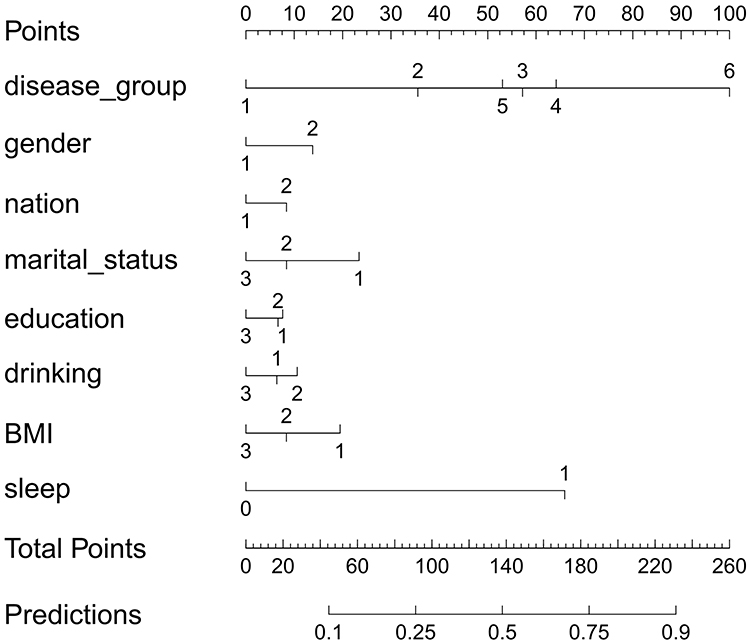 |
Figure 2 Nomogram for predicting the probability of depression for coronary heart disease. |
 |
Figure 3 The roc curve for the nomogram model in prediction of depression. |
Discussion
According to clinical epidemiological studies, psychological disorders are prevalent comorbidities in patients with coronary heart disease (CHD), significantly surpassing the rates observed in the general population, albeit with variations in screening tools and sampled populations.20 Previous investigations into psychological disorders among CHD patients have reported depression incidence ranging from 34.6% to 51%, with acute coronary syndrome showing rates of 31% to 45%, markedly higher than the World Health Organization’s estimated 4.3% in the general population.21 While numerous studies have explored the psychological aspects of coronary heart disease, a systematic evaluation of the psychological status across different stages of CHD remains lacking. Hence, our current study aimed to fill this gap by assessing the extent of depression at various stages of coronary heart disease.
In general, both the degree and overall scores on the PHQ-9 indicated a trend: the more severe the disease, the more pronounced the depression and anxiety in patients, with heart failure (HF) showing significantly higher rates than other groups. Interestingly, post-percutaneous coronary intervention (PCI), patients experienced a relief in depression, contrary to prior studies suggesting increased depression scores following cardiac coronary artery bypass graft surgery.22 This divergence may stem from increased patient confidence in follow-up prognosis. Furthermore, it contrasts with previous findings suggesting persistent depression despite treatment.20 Notably, in the healthy population, 9.7% exhibited depressive symptoms, a percentage higher than a study involving a rural Chinese population sample (5.9%), as determined by PHQ-9≥5.23
Subsequently, we conducted comparisons between individuals with and without depression across various factors. Statistical differences were observed for most general and lifestyle factors, excluding technical titles and exercise. Building on these findings, the binary logistic regression model explored risk factors contributing to depressive symptoms. Overall, depression correlated closely with gender, nation, marital status, education, drinking, BMI, sleep disturbance, and disease status. Paradoxically, while one study suggested no gender effect on depression,24 another attributed gender’s significance to the sex role hypothesis.25 In our study, gender was closely associated with depression, with women being more prone. Marital status also significantly related to depression,26 aligning with previous research demonstrating higher depression risk with lower education levels.23,27,28 Similar to prior studies, alcohol consumption and abnormal BMI were associated with depression.29–33 Sleep status showed a strong association with depression, and vice versa.34,35 Recognizing the reciprocal relationship, the integrated approach addressing both sleep problems and depression emerges as a vital strategy in preventing heart disease.36–38
In this study, the nomogram developed serves as a useful tool for predicting the risk of depression in CHD patients. This prediction model exhibits strong predictive capabilities, excellent calibration, and valuable clinical utility. It combines multiple predictors and presents them in a visual format, allowing medical professionals to easily assess the likelihood of depression based on the sum of relevant risk factors. At the same time, patients can obtain additional resources and information through the nomogram prediction model easily, improve their understanding of their own mental health status, and actively participate in the treatment and management process. Based on the above scoring results, we hope to quickly identify potential depression in patients, so as to prevent and intervene in advance, prevent the promoting effect of depression itself on the disease, and also make depression intervention in coronary heart disease patients more important.
Conclusion
Depression is one of the common symptom in coronary heart disease, and they can affect each other accentuating further disease. This study would like to help clinicians and researchers understand the degree of depression in patients with coronary heart disease quickly and accurately, especial in the different stages of coronary heart disease. At the same time, we find that depression is close to the risk factors of Gender, Nation, Marital status, education, drinking, BMI, Sleep disturbance, and Status of disease. Based on above, this study develops predictive nomogram models referred to these risk factors, in order to give an early judgment, prevention and intervention for coronary heart disease accurately.
Abbreviations
CHD, Coronary heart disease; CCD, Chronic coronary disease; MS, Metabolic syndrome; ACS, Acute coronary syndrome; P-PCI, Post-percutaneous coronary intervention; HF, Heart failure; PHQ-9, Patient Health Questionnaire-9; MDD, Major depressive disorder; ICT, The information collection form; ORs, Odds ratios; CIs, 95% Confidence intervals; AUC, Area Under the Curve.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
All participants signed an ethical consent form.
Acknowledgments
Hongxuan Tong and Jiale Zhang are co-first authors for this study. We thank all those who provided excellent technical support and assistance during the study. This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-3890258/v1
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The design of the study and the collection, analysis, and interpretation of data were supported by Scientific and Technological Innovation Project of China Academy of Chinese Medical Sciences, NO: CI2023C060YLL; The Fundamental Research Funds for the Central Public Welfare Research Institutes, No. YZX-202240 and YZX-202406.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Richards SH, Anderson L, Jenkinson CE, et al. Psychological interventions for coronary heart disease. Cochrane Database Syst Rev. 2017;4(4):Cd002902. doi:10.1002/14651858.CD002902.pub4
2. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart Disease and Stroke Statistics-2022 Update: a Report From the American Heart Association. Circulation. 2022;145(8):e153–e639. doi:10.1161/CIR.0000000000001052
3. Tully PJ, Cosh SM, Baumeister H. The anxious heart in whose mind? A systematic review and meta-regression of factors associated with anxiety disorder diagnosis, treatment and morbidity risk in coronary heart disease. J Psychosomatic Res. 2014;77(6):439–448. doi:10.1016/j.jpsychores.2014.10.001
4. Carney RM, Freedland KE. Depression and coronary heart disease. Nat Rev Cardiol. 2017;14(3):145–155. doi:10.1038/nrcardio.2016.181
5. Ren Y, Yang H, Browning C, et al. Prevalence of depression in coronary heart disease in China: a systematic review and meta-analysis. Chin Med J. 2014;127(16):2991–2998. doi:10.3760/cma.j.issn.0366-6999.20140036
6. Gale CR, Batty GD, Osborn DP, et al. Mental disorders across the adult life course and future coronary heart disease: evidence for general susceptibility. Circulation. 2014;129(2):186–193. doi:10.1161/CIRCULATIONAHA.113.002065
7. Roest AM, Martens EJ, De Jonge P, et al. Anxiety and risk of incident coronary heart disease: a meta-analysis. J Am College Cardiol. 2010;56(1):38–46. doi:10.1016/j.jacc.2010.03.034
8. Zahodne LB, Gilsanz P, Glymour MM, et al. Comparing Variability, Severity, and Persistence of Depressive Symptoms as Predictors of Future Stroke Risk. Am J Geriatric Psychiatry. 2017;25(2):120–128. doi:10.1016/j.jagp.2016.10.009
9. Ayerbe L, Ayis S, Wolfe CD, et al. Natural history, predictors and outcomes of depression after stroke: systematic review and meta-analysis. Br J Psychiatry. 2013;202(1):14–21. doi:10.1192/bjp.bp.111.107664
10. Jørgensen TS, Wium-Andersen IK, Wium-Andersen MK, et al. Incidence of Depression After Stroke, and Associated Risk Factors and Mortality Outcomes, in a Large Cohort of Danish Patients. JAMA psychiatry. 2016;73(10):1032–1040. doi:10.1001/jamapsychiatry.2016.1932
11. Skala JA, Freedland KE, Carney RM. Coronary heart disease and depression: a review of recent mechanistic research. Can J Psychiatry. 2006;51(12):738–745. doi:10.1177/070674370605101203
12. Palacios J, Khondoker M, Mann A, et al. Depression and anxiety symptom trajectories in coronary heart disease: associations with measures of disability and impact on 3-year health care costs. J Psychosomatic Res. 2018;104:1–8. doi:10.1016/j.jpsychores.2017.10.015
13. Foss-Nieradko B, Stepnowska M, Piotrowicz R. Effect of the dynamics of depression symptoms on outcomes after coronary artery bypass grafting. Kardiologia polska. 2012;70(6):591–597.
14. Hagström E, Norlund F, Stebbins A, et al. Psychosocial stress and major cardiovascular events in patients with stable coronary heart disease. J Internal Med. 2018;283(1):83–92. doi:10.1111/joim.12692
15. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
16. Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. JAMA. 1999;282(18):1737–1744.
17. Srivastava S, Sachin D, Dighe R. The American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). Springer US; 2013:84–85. doi:10.1007/978-0-387-79061-9_113
18. Chen S, Chiu H, Xu B, et al. Reliability and validity of the PHQ-9 for screening late-life depression in Chinese primary care. Int J Geriatr Psychiatry. 2010;25(11):1127–1133. doi:10.1002/gps.2442
19. Wang W, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
20. Wu Y, Zhu B, Chen Z, et al. New Insights Into the Comorbidity of Coronary Heart Disease and Depression. Curr Probl Cardiol. 2021;46(3):100413. doi:10.1016/j.cpcardiol.2019.03.002
21. Lichtman JH, Froelicher ES, Blumenthal JA, et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: systematic review and recommendations: a scientific statement from the American Heart Association. Circulation. 2014;129(12):1350–1369. doi:10.1161/CIR.0000000000000019
22. Korbmacher B, Ulbrich S, Dalyanoglu H, et al. Perioperative and long-term development of anxiety and depression in CABG patients. Thorac Cardiovasc Surg. 2013;61(8):676–681. doi:10.1055/s-0032-1333326
23. Zhou X, Bi B, Zheng L, et al. The prevalence and risk factors for depression symptoms in a rural Chinese sample population. PLoS One. 2014;9(6):e99692. doi:10.1371/journal.pone.0099692
24. Mumang AA, Syamsuddin S, Maria IL, et al. Gender Differences in Depression in the General Population of Indonesia: confounding Effects. Depress Res Treat. 2021;2021:3162445. doi:10.1155/2021/3162445
25. Robinson KM, Depression MJJ. Depressive Somatic or Nonsomatic Symptoms, and Function in a Primarily Hispanic Chronic Pain Population. ISRN Pain. 2013;2013:401732. doi:10.1155/2013/401732
26. Edmealem A, Olis CS. Factors Associated with Anxiety and Depression among Diabetes, Hypertension, and Heart Failure Patients at Dessie Referral Hospital, Northeast Ethiopia. Behav Neurol. 2020;2020:3609873. doi:10.1155/2020/3609873
27. Arslantas D, Ünsal A, Ozbabalik D. Prevalence of depression and associated risk factors among the elderly in Middle Anatolia, Turkey. Geriatr Gerontol Int. 2014;14(1):100–108. doi:10.1111/ggi.12065
28. Arachchi NSM, Ganegama R, Husna AWF, et al. Suicidal ideation and intentional self-harm in pregnancy as a neglected agenda in maternal health; an experience from rural Sri Lanka. Reprod Health. 2019;16(1):166. doi:10.1186/s12978-019-0823-5
29. Gea A, Beunza J, Estruch R, et al. Alcohol intake, wine consumption and the development of depression: the PREDIMED study. BMC Med. 2013;11(1):192. doi:10.1186/1741-7015-11-192
30. Hasin DS, Goodwin RD, Stinson FS, et al. Epidemiology of major depressive disorder: results from the National Epidemiologic Survey on Alcoholism and Related Conditions. Arch Gen Psychiatry. 2005;62(10):1097–1106. doi:10.1001/archpsyc.62.10.1097
31. Hasin DS, Stinson FS, Ogburn E, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2007;64(7):830–842. doi:10.1001/archpsyc.64.7.830
32. Raud B, Gay C, Guiguet-Auclair C, et al. Level of obesity is directly associated with the clinical and functional consequences of knee osteoarthritis. Sci Rep. 2020;10(1):3601. doi:10.1038/s41598-020-60587-1
33. Vafa M, Azizi-Soleiman F, Kazemi SM, et al. Comparing the effectiveness of vitamin D plus iron vs vitamin D on depression scores in anemic females: randomized triple-masked trial. Med J Islam Repub Iran. 2019;33:64. doi:10.34171/mjiri.33.64
34. Hoshikawa M, Uchida S, Hirano Y. A Subjective Assessment of the Prevalence and Factors Associated with Poor Sleep Quality Amongst Elite Japanese Athletes. Sports Med Open. 2018;4(1):10. doi:10.1186/s40798-018-0122-7
35. Ban MJ, Kim WS, Park KN, et al. Korean survey data reveals an association of chronic laryngitis with tinnitus in men. PLoS One. 2018;13(1):e0191148. doi:10.1371/journal.pone.0191148
36. Zhai K, Gao X, Wang G. The Role of Sleep Quality in the Psychological Well-Being of Final Year UndergraduateStudents in China. Int J Environ Res Public Health. 2018;15(12):2881. doi:10.3390/ijerph15122881
37. Redline S, Foody J. Sleep disturbances: time to join the top 10 potentially modifiable cardiovascular risk factors? Circulation. 2011;124(19):2049–2051. doi:10.1161/CIRCULATIONAHA.111.062190
38. Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA. 1989;262(11):1479–1484. doi:10.1001/jama.1989.03430110069030
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.