")
Back to Journals » International Journal of General Medicine » Volume 16
Risk Factors for 30-Day Mortality in Patients with Bacteremic Pneumonia Caused by Escherichia coli and Klebsiella pneumoniae: A Retrospective Study
Authors Zhao C, Zheng Y , Hang Y, Chen Y, Liu Y, Zhu J, Fang Y, Xiong J, Hu L
Received 30 October 2023
Accepted for publication 20 December 2023
Published 28 December 2023 Volume 2023:16 Pages 6163—6176
DOI https://doi.org/10.2147/IJGM.S447354
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Chuwen Zhao,1,2,* Yunwei Zheng,1,* Yaping Hang,1 Yanhui Chen,1 Yanhua Liu,1 Junqi Zhu,1,2 Youling Fang,1,2 Jianqiu Xiong,3 Longhua Hu1
1Department of Jiangxi Provincial Key Laboratory of Medicine, Clinical Laboratory of the Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 2School of Public Health, Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 3Department of Nursing, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Longhua Hu, Department of Jiangxi Provincial Key Laboratory of Medicine, Clinical Laboratory of the Second Affiliated Hospital of Nanchang University, Mingde Road No. 1, Nanchang, Jiangxi, 330006, People’s Republic of China, Email [email protected] Jianqiu Xiong, Department of Nursing, the Second Affiliated Hospital of Nanchang University, Mingde Road No. 1, Nanchang, Jiangxi, 330006, People’s Republic of China, Email [email protected]
Objective: Escherichia coli and Klebsiella pneumoniae are prevalent Gram-negative microorganisms responsible for pneumonia, as well as the primary Enterobacteriaceae pathogens causing bacteremic pneumonia. The objective of this research is to analyze the risk factors associated with bacteremic pneumonia caused by these pathogens and develop a predictive model.
Patients and Methods: This retrospective investigation encompassed a cohort of 252 patients diagnosed with Escherichia coli or Klebsiella pneumoniae-induced bacteremic pneumonia between 2018 and 2022. The primary endpoint was 30-day mortality, which was analyzed using multifactorial logistic regression, nomogram construction, and Bootstrap validation.
Results: Among the 252 patients diagnosed with Escherichia coli and Klebsiella pneumoniae, 65 succumbed to the disease while 187 survived. The overall 30-day mortality was found to be 25.8%. A multifactorial logistic regression analysis revealed that diastolic blood pressure, cerebrovascular diseases/transient ischemic attacks (TIA), immunosuppression, blood urea nitrogen, Pitt score, and CURB-65 score were statistically significant factors. The Nomogram model demonstrated an AUC of 0.954, which closely aligns with the Bootstrap-derived mean AUC of 0.953 (95% CI: 0.952– 0.954).
Conclusion: In patients with bacteremic pneumonia caused by Escherichia coli and Klebsiella pneumoniae, Low diastolic blood pressure (≤ 61 mmHg), pre-existing cerebrovascular disease/ transient ischemic attacks (TIA), immunosuppression status, elevated blood urea nitrogen levels (≥ 8.39 mmol/L), high Pitt score (≥ 3), and a high CURB-65 score (≥ 2) are all independent risk factors for Escherichia coli and Klebsiella pneumoniae bacteremic pneumonia, among which the first three warrant particular attention.
Keywords: Klebsiella pneumoniae, Escherichia coli, bacteremic pneumonia, 30-day mortality, nomogram
Introduction
Pneumonia remains a prevalent infectious disease globally, particularly in low- and middle-income countries (LMICs), with high morbidity and mortality rates.1 Even before the emergence of COVID-19, pneumonia-related deaths continued to rise annually across all age groups worldwide.2 Bacteremic pneumonia, characterized by a higher mortality rate and more severe course, is commonly observed in critically ill patients. Despite advancements in medical technology, it remains an intractable problem that places a significant burden on healthcare systems.3
Gram-positive bacteria are the primary cause of most community-acquired pneumonia (CAP), while Gram-negative bacteria are often linked to hospital-acquired and ventilator-associated pneumonia. In recent decades, their impact on pneumonia has gained increased attention due to the rise in Gram-negative bacterial resistance.4,5 A large retrospective cohort study in the United States found that Escherichia coli (7.7%) and Klebsiella pneumoniae (5.6%) were the two most pathogenic bacteria after Pseudomonas aeruginosa (10%) in patients with Gram-negative pneumonia.6 In Africa and Southeast Asia, the primary pathogens of severe bacteremia have shifted from Streptococcus pneumoniae to Gram-negative bacteria such as Klebsiella pneumoniae in certain situations.1
Escherichia coli and Klebsiella pneumoniae are among the most common pathogens of community-acquired and hospital-acquired pneumonia, as well as the most prevalent carbapenem-resistant Enterobacteriaceae (CRE). CRE has been rapidly increasing in recent years and is associated with significantly higher mortality in bacteremic pneumonia compared to non-bacteremic pneumonia, posing a significant threat to human health.7,8 Consequently, there has been a growing interest among scholars to investigate the epidemiology, risk factors, and prognostic outcomes of these Gram-negative pneumonias.
Studies have shown that the mortality rate of Gram-negative bacterial pneumonia is still significant even when the optimal antibiotic therapy is provided.9 Therefore, comprehensive management targeting both patients and pathogens is crucial. This implies that it is necessary to pay attention to the clinical characteristics and risk factors of bacteremic pneumonia caused by these bacteria. Although previous studies have reported risk factors for Klebsiella pneumoniae bacteremic pneumonia, they have been limited to hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP), and there have been limited studies on Escherichia coli bacteremic pneumonia. However, given that the clinical outcomes of bacteremic pneumonia caused by these two pathogens have been confirmed to be statistically insignificant, they belong to the same genus of Enterobacteriaceae and are the most common bacteria among CREs, therefore we combined them for research.10 Our aim is to study the clinical characteristics and 30-day mortality risk factors of Gram-negative pneumonia caused by Enterobacteriaceae bacteria represented by Escherichia coli and Klebsiella pneumoniae, while establishing a risk prediction model for clinical use. This model will be applicable to various types of bacteremic pneumonia caused by Escherichia coli and Klebsiella pneumoniae (including CAP, HAP/VAP), and provide certain assistance for clinical decision-making and improving the quality of comprehensive management in our region.
Materials and Methods
Research Design and Patients
In this single-center retrospective study, we analyzed the clinical data of patients with bacteremic pneumonia caused by Escherichia coli or Klebsiella pneumoniae admitted to a large provincial third-level hospital in China from January 1, 2018 to December 31, 2022. All data were obtained from the Laboratory Information System (LIS), Hospital Information System (HIS), and integrated research databases.
The inclusion criteria for patients in this study were as follows: 1) age ≥18 years; 2) diagnosis of pneumonia based on guidelines issued by the American Thoracic Society, the Infectious Diseases Society of America, and the Respiratory Diseases Society of the Chinese Medical Association, which indicated lung infiltration or consolidation on chest imaging, elevated laboratory indicators such as white blood cells and C-reactive protein, and clinical symptoms including high fever, chills, and purulent sputum; 3) receipt of blood culture within 48 hours before or after the diagnosis of pneumonia, with results indicating infection by Escherichia coli or Klebsiella pneumoniae, and if concomitant sputum cultures or sputum smear results are available, they must be consistent with these results (consistent results include Gram-negative bacteria on sputum smear, negative results on sputum culture or smear, invalid results on sputum culture or smear, and the absence of both sputum smear and culture results).
The exclusion criteria for patients were as follows: 1) missing key data; 2) multiple microbial infections, defined as blood culture; the sputum culture unequivocally demonstrated the presence of one or more other pathogenic bacteria (sputum quality was deemed acceptable with a white blood cell count >25 cells/LP and epithelial cell count <10 cells/LP; at the same time, the sputum culture was determined to be non-contaminated); bronchoalveolar lavage fluid culture results containing pathogens other than Escherichia coli or Klebsiella pneumoniae within 48 hours after the diagnosis of pneumonia; 3) Patients with infections other than pneumonia (including viral infections, fungal pneumonia, severe biliary disease, upper urinary tract infection, intra-abdominal infection, severe external trauma, deep skin infection, osteomyelitis, pulmonary tuberculosis, disseminated infections). Only the first episode of bacteremic pneumonia for each patient was considered in the analysis.
Definitions and Outcomes
The definition of hospital-acquired pneumonia is pneumonia that occurs more than 48 hours after admission to the hospital, while community-acquired pneumonia refers to pneumonia that has occurred before admission or is diagnosed within 48 hours of admission. Ventilator-associated pneumonia (VAP) is defined as pneumonia that develops after 48 hours of mechanical ventilation in patients who have undergone intubation or tracheostomy. Immunosuppression is defined as a state in which patients are chronically taking glucocorticoid medications (the equivalent dose of prednisone is ≥ 20 mg / d, with a course of treatment ≥ 14 days, or the total dose of equivalent prednisone is > 700 mg), undergoing organ transplantation, have congenital or acquired immunodeficiency diseases, or are undergoing radiation or chemotherapy. Immunomodulators include Bacillus Calmette-Guérin (BCG), thymosin, heat shock proteins, levamisole, mizoribine, pidotimod, and polysaccharides (astragalus polysaccharide, lentinan). Appropriate empiric treatment refers to the use of at least one antibiotic drug effective against the causative pathogen prior to clinical susceptibility results. In contrast, inappropriate empiric treatment refers to the use of antibiotic drugs that are ineffective against the causative pathogen prior to clinical susceptibility results. Given that the course of treatment for pneumonia and gram-negative bacteremia is typically one to two weeks (and may extend beyond three weeks in severe cases), the 30-day mortality rate serves as the outcome of interest in this study (defined as the time from the diagnosis of pneumonia with a positive blood culture result to the patient’s death).
Data Collection
In this study, patient demographics (age, gender), vital signs, department of admission, type of pneumonia (hospital-acquired or community-acquired), pathogens (Escherichia coli or Klebsiella pneumoniae), underlying diseases, invasive procedures, laboratory parameters, disease severity (Pitt score, SOFA score, aCCI index, CURB-65 score), treatment (appropriate empiric treatment, inappropriate empiric treatment, antibiotic use ≥3 during hospitalization), length of hospital stay, and outcomes (survival or death) were recorded. Vital signs and laboratory parameters were obtained within 24 hours before and after blood culture collection from the patient. The Pitt score, SOFA score, aCCI index, and CURB-65 score were also assessed based on the above time frame. Invasive procedures were limited to those occurring during hospitalization.
Microbiological Tests
The Escherichia coli and Klebsiella pneumoniae isolates from patients were identified using the VITEK®2 Compact system (bioMérieux, Marcy l’Étoile, France) and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) system (Smart MS 5020, bioMérieux). The identification of bacterial species was performed using MALDI-TOF MS. Antimicrobial susceptibility testing was conducted using the Kirby-Bauer method or VITEK®2 Compact system, with MICs determined according to CLSI standards. Additionally, ESBL production was detected using a combination disk method with ceftazidime and cefpodoxime alone or in combination with clavulanic acid, as recommended by the CLSI. CRE was determined based on the results of routine susceptibility testing (disk diffusion and MIC) according to the definition provided by the Centers for Disease Control and Prevention (CDC). Carbapenemase production was screened using the CLSI recommended method (eCIM / mCIM, carbapenemase inhibitor enhancement test). The Escherichia coli strain ATCC 8739 is used as a quality control strain for MALDI-TOF MS. The strains Escherichia coli ATCC 25922 and Staphylococcus aureus ATCC 29213 are employed as quality control strains for antimicrobial susceptibility testing. Klebsiella pneumoniae ATCC 700603 is utilized as a quality control strain for ESBL production.
Statistical Analysis
The data was analyzed and images were plotted using SPSS 20 and R language. For continuous variables that met the normal distribution, the mean ± standard deviation was used for representation, while for count variables that did not meet the normal distribution, the interquartile range was used. Two-independent sample t-test was performed on continuous variables that met the normal distribution, while Mann–Whitney U-test was used for count variables that did not meet the normal distribution. Chi-square test or Fisher’s exact test was used for count data. The ROC curve was used to convert skewed continuous variables into binary variables. Univariate and multivariate logistic regression analyses were performed to identify risk factors for 30-day mortality. Nomograms were constructed to predict 30-day mortality. The performance of the model was evaluated using ROC curves, PR curves, and calibration curves. Decision curve analysis was used to assess the clinical value of the model. Bootstrap was used for internal validation of the model. The missing values were imputed using multiple imputation by chained equations (MICE). P < 0.05 was considered statistically significant.
Results
Clinical Characteristics
According to the inclusion and exclusion criteria, a total of 252 patients were included in this study, with 65 patients who died within 30 days being included in the non-survival group and 187 patients who were discharged due to improvement or cure being included in the survival group (Figure 1). The clinical characteristics of the two groups are summarized in Table 1. The mean age of all patients was 59.5 (SD: 15.5). In the survival group, most patients had higher blood pressure, surgical history during hospitalization, received appropriate empirical treatment, and the causative pathogen was Escherichia coli. In contrast, in the non-survival group, males and ICU patients accounted for the majority, and their respiratory rate, pulse rate, blood urea nitrogen values, Pitt score, SOFA score, and CURB-65 score were higher than those in the survival group. The causative pathogen was mostly carbapenem-resistant Klebsiella pneumoniae. Patients with underlying diseases such as cerebrovascular disease/TIA, chronic kidney disease, chronic liver disease, hypoproteinemia, anemia, invasive procedures such as deep vein catheterization, organ resection, mechanical ventilation, or immunosuppression status had a higher 30-day mortality rate (p < 0.05). Among all patients, there were 71 cases (28.2%) of inappropriate empirical treatment, of which 34 cases (47.9%) died within 30 days.
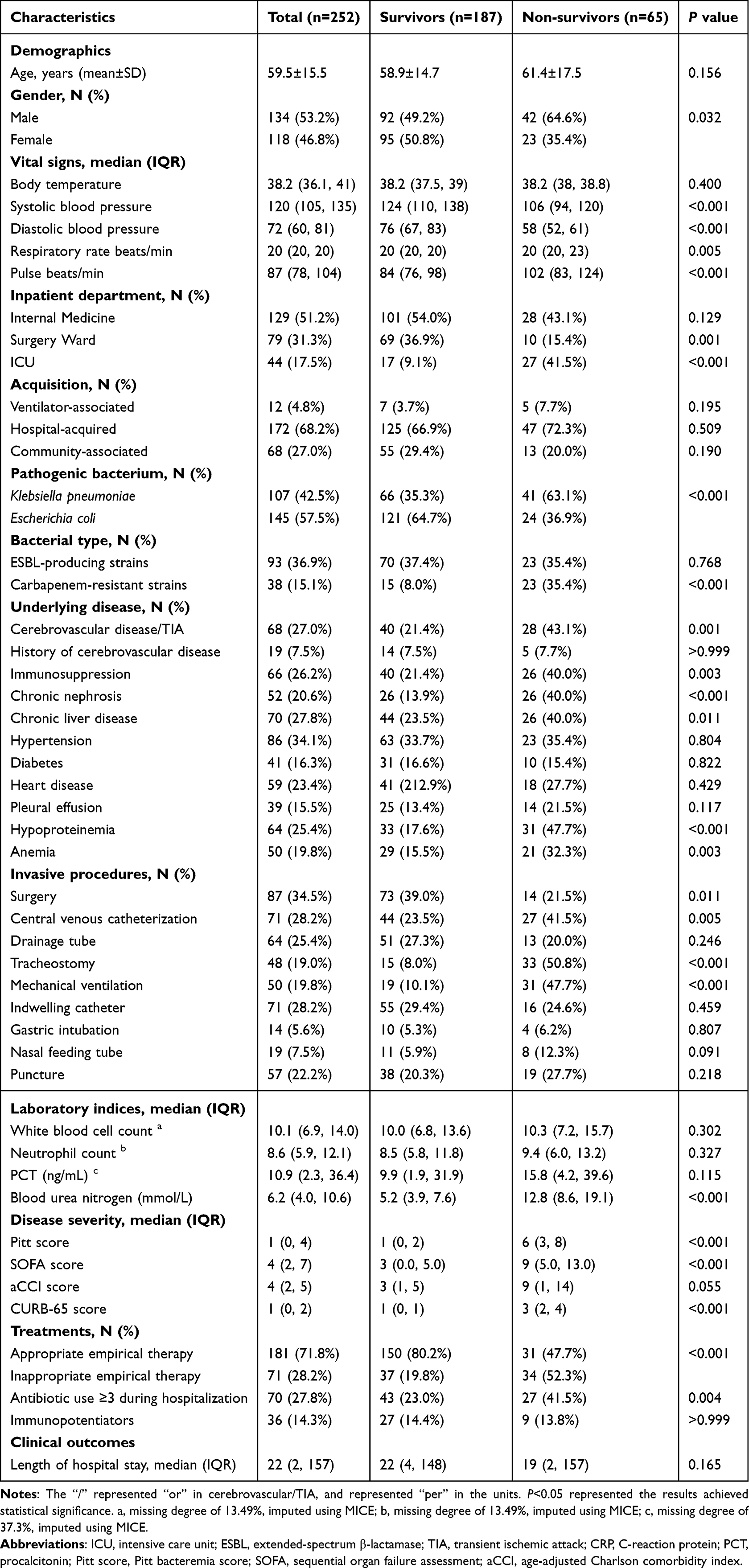 |
Table 1 Clinical Characteristics of Survival and Non-Survival Groups in Patients with Escherichia Coli or Klebsiella Pneumoniae Bacteremic Pneumonia |
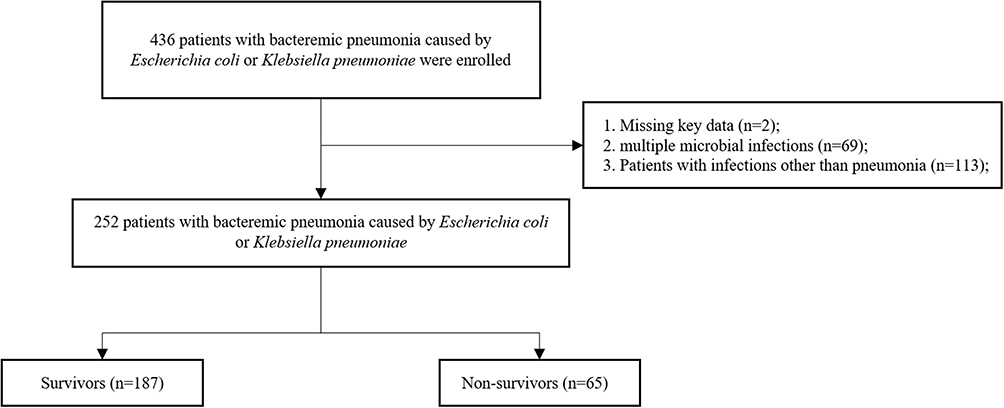 |
Figure 1 Patient inclusion process flow diagram. |
Microbiological Characteristics
The antibiotic resistance of the isolated strains of Escherichia coli and Klebsiella pneumoniae from 252 patients is shown in Table 2. Among all the isolates, both Escherichia coli and Klebsiella pneumoniae showed high levels of resistance to cephazolin (61.4% vs 51.6%), followed by ciprofloxacin (52.7% vs 53.2%) and ceftriaxone (57.2% vs 48.6%). The drugs with higher sensitivity for both Escherichia coli and Klebsiella pneumoniae among all the isolates were ertapenem (100% vs 100%), amikacin (98.6% vs 83.2%), and tigecycline (100.0% vs 79.6%), with no resistant strains found for ertapenem among all the isolates with drug susceptibility results. For imipenem, nitrofurantoin, and piperacillin, the resistance rates of Klebsiella pneumoniae were significantly higher than those of Escherichia coli (p < 0.001).
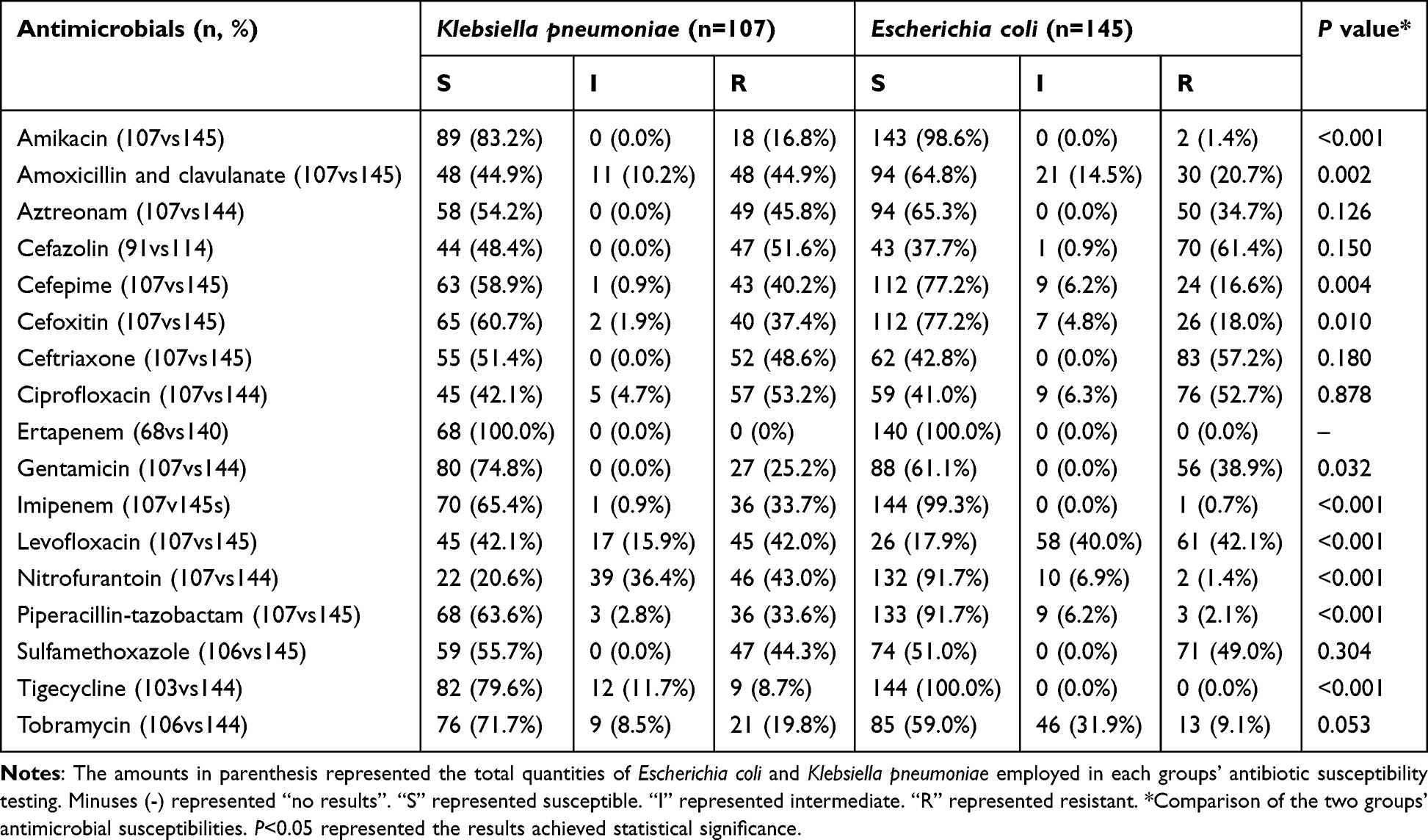 |
Table 2 Antimicrobial Resistance of Escherichia Coli and Klebsiella Pneumoniae Isolated from Patients with Bacteremic Pneumonia |
Risk Factors
The overall 30-day mortality rate of patients with Gram-negative bacteremic pneumonia caused by Escherichia coli and Klebsiella pneumoniae was 25.8% (65/252), with a mortality rate of 60.5% (23/38) for CRE infections. We plotted violin plots for some non-normally distributed quantitative data, including vital signs (systolic blood pressure, diastolic blood pressure, respiratory rate, pulse), laboratory indicators (blood urea nitrogen), as well as Pitt score, SOFA score, and CURB-65 score to understand the differences and distribution between the two groups (Figure 2). Systolic blood pressure (SBP), Diastolic blood pressure (DBP), Blood urea nitrogen (BUN), Pitt score, and CURB-65 score showed significant differences in distribution between the survival and non- survival groups. ROC curve analysis was also performed to determine the cutoff values of each indicator by calculating the Youden index, which were then converted into binary variables, as shown in Table 3. The AUC of CURB-65 score was the largest at 0.94, while that of respiratory rate was the smallest at 0.61. After converting some variables into binary variables and removing some variables based on their correlation (endotracheal intubation was removed, while mechanical ventilation was retained), single factor and multifactor logistic regression analyses were performed (Table 4) to identify independent risk factors for this type of bacteremic pneumonia. Single factor regression analysis showed that male gender, low blood pressure, fast respiratory rate, rapid heart rate, ICU patient, carbapenem-resistant strain, cerebrovascular disease/TIA, immunosuppression, chronic liver disease, chronic nephrosis, anemia, hypoproteinemia, mechanical ventilation, central venous catheterization, high BUN, high Pitt score, high SOFA score, high CURB-65 score, and antibiotic use ≥3 during hospitalization were significantly associated with a 30-day mortality rate (p < 0.05). Multifactor regression analysis showed that DBP ≤61, cerebrovascular disease/TIA, immunosuppression status, high BUN (≥8.39), high Pitt score (≥3), and high CURB-65 score (≥2) were independent risk factors for this type of bacteremic pneumonia.
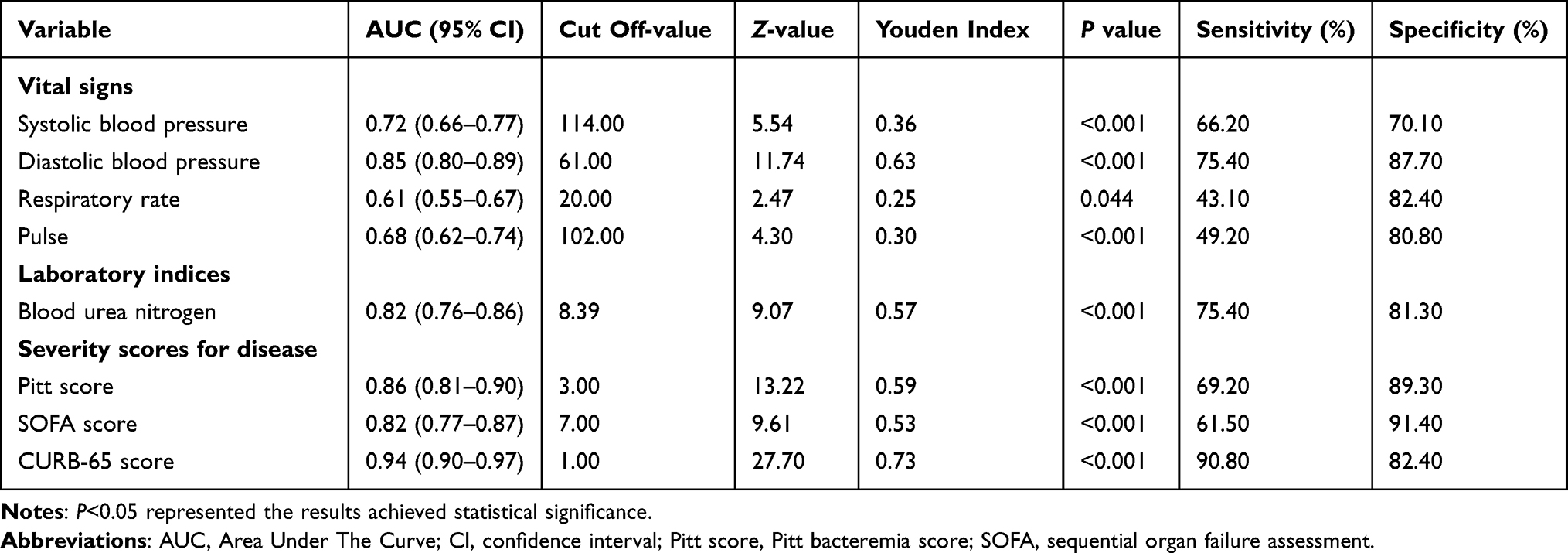 |
Table 3 ROC Curve Parameters for Vital Signs, Laboratory Indices, and Severity Scores for Disease |
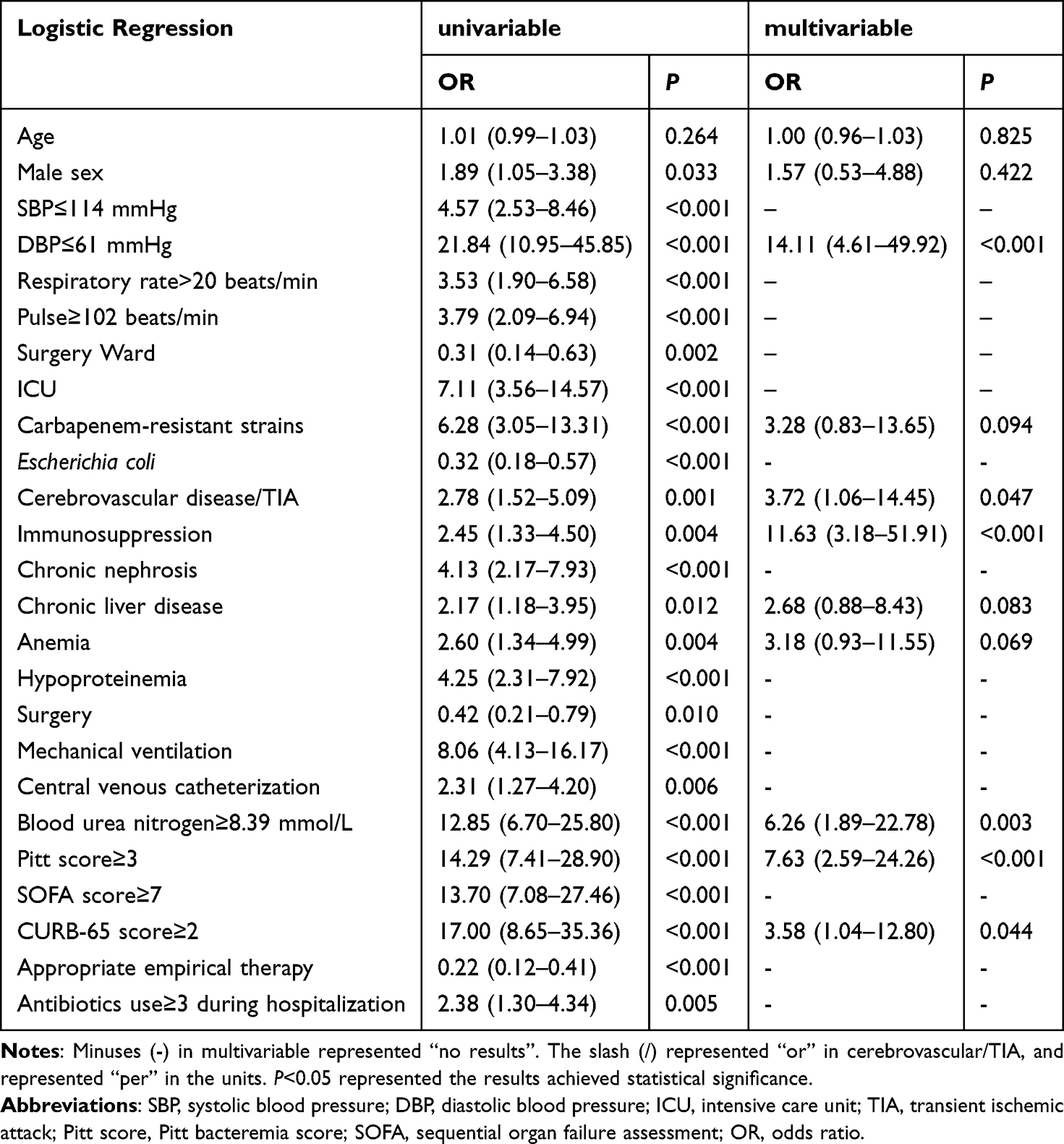 |
Table 4 Risk Factors for 30 Day Mortality in Patients with Escherichia coli and Klebsiella pneumoniae Bacteremic Pneumonia |
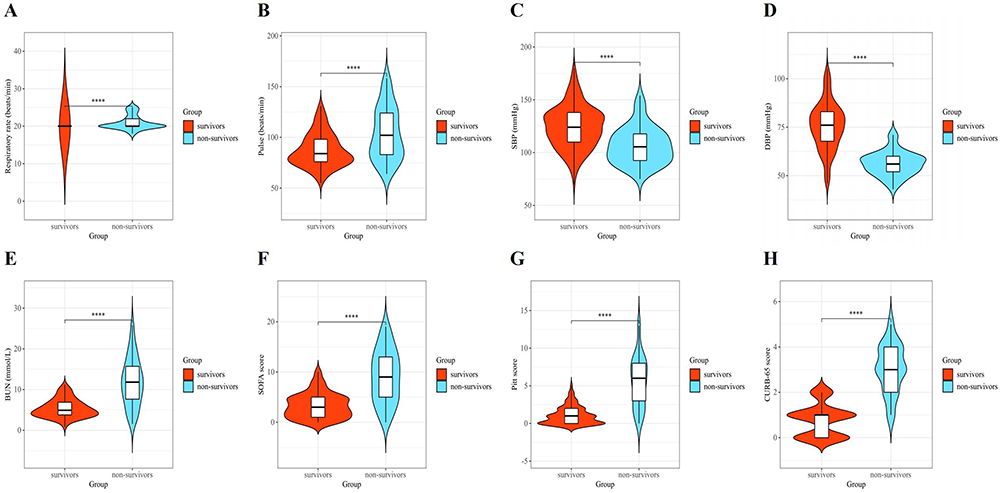 |
Figure 2 Violin plot of respiratory rate (A), pulse (B), SBP (C), DBP (D), BUN (E), SOFA score (F), Pitt score (G) and CURB-65 (H) for patients with bacteremia complicated by pneumonia. Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; BUN, blood urea nitrogen; Pitt score, Pitt bacteremia score; SOFA, sequential organ failure assessment. Notes: “****” represented that P-value for the comparison of groups survivor and non-survivor is less than 0.001. |
Modeling and Assessment
In order to conduct a comprehensive analysis and evaluation of the above-mentioned independent risk factors, we have established a 30-day mortality prediction model. We assigned corresponding weights to each independent risk factor, as shown in the regression line chart (Figure 3). When low DBP (≤61), immunosuppression status, high Pitt score (≥3), high BUN (≥8.39), pre-existing cerebrovascular disease/TIA, or high CURB-65 score (≥2), their scores were assigned values of 100, 92.5, 82.5, 70, 52.5, and 50 respectively. If the total score exceeds 300, the patient’s risk of death within 30 days will exceed 90%. Figure 4 presents the performance evaluation of the established risk prediction model. Both the ROC curve (A) and PR curve (B) indicate that the risk prediction model performs well, with an area under the ROC curve of 0.954. The PR curve also suggests that the model performs well even when the proportions of positive (non-survival group) and negative (survival group) cases are imbalanced. The calibration curve (C) demonstrates the fitting of the fractional prediction model, with a discriminatory index of 0.703 and a low Brier score of 0.057, indicating good accuracy and precision of the risk prediction model. The decision curve (D) shows that there is a good net benefit when the threshold probability is between 0.06 and 0.85. The internal validation of the model was conducted using Bootstrap with a sample size of 252 and 1000 iterations, resulting in an average AUC of 0.9528 (95% CI: 0.9517–0.9539), which is not significantly different from the AUC of the model, indicating good reproducibility.
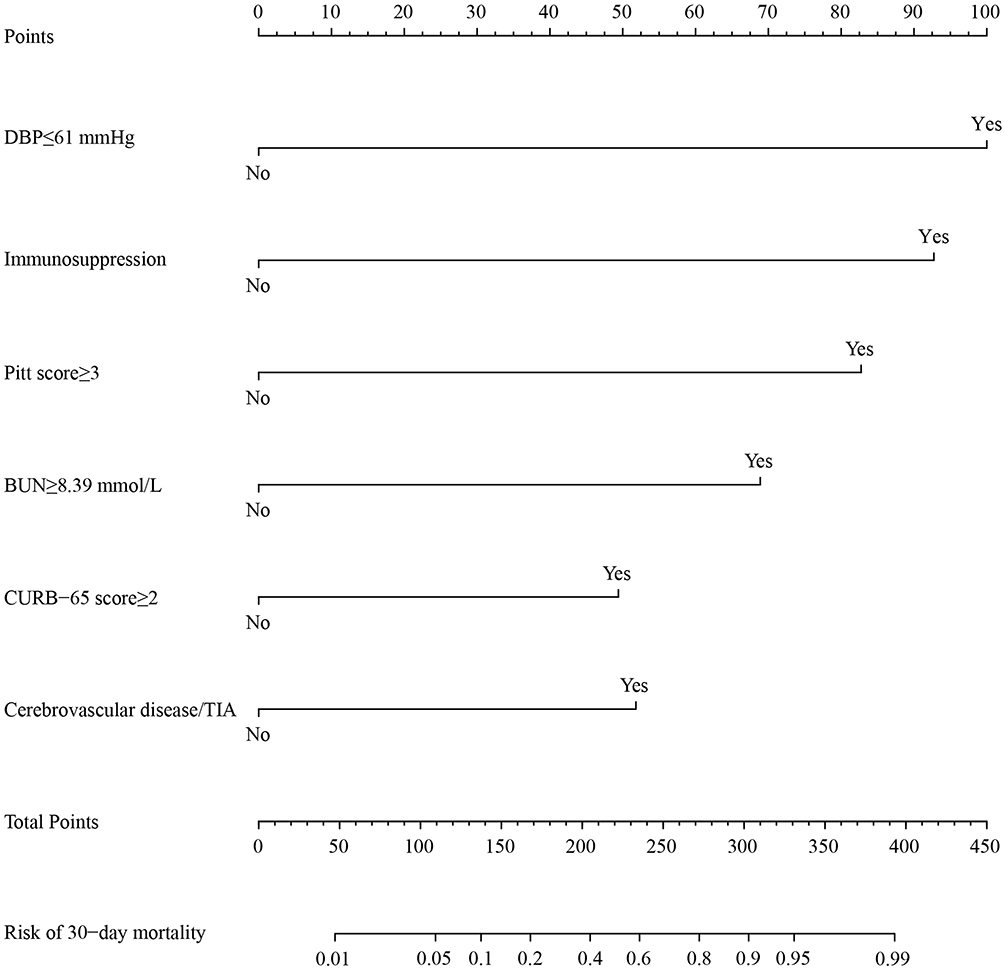 |
Figure 3 Nomogram for the results of multiple logistic regression analysis in Table 4. Abbreviations: DBP, diastolic blood pressure; Pitt score, Pitt bacteremia score; BUN, blood urea nitrogen; TIA, transient ischemic attack. Notes: “Yes” represented “occurrence of the event”. “No” represented “the event did not occur”. The nomogram is able to visualize the results of multiple logistic regression analysis, score each value level of each indexes, and ultimately predict the likelihood of clinical outcome. |
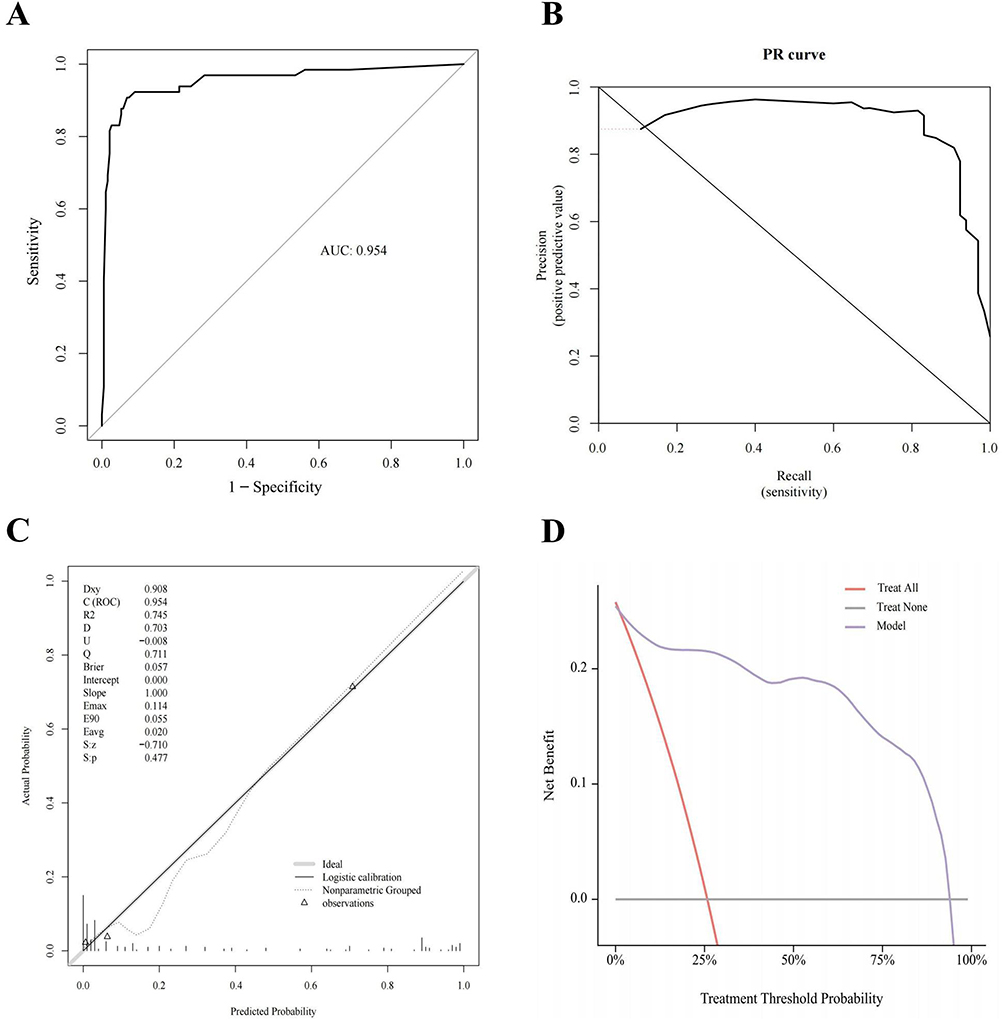 |
Figure 4 (A) ROC curve of the risk assessment model for patients with bacteremia complicated by pneumonia. (B) PR curve of the risk assessment model for patients with bacteremia complicated by pneumonia. (C) Calibration curve of the risk assessment model for patients with bacteremia complicated by pneumonia. (D) Clinical decision curve of the risk assessment model for patients with bacteremia complicated by pneumonia. Abbreviations: AUC, area under ROC curve; PR curve, precision-recall curve; D, discrimination index; U, unreliability index; Q, quality index; Brier, Brier Score. Notes: “Dxy” in (C) represented “correlation between predicted and actual values”. “C(ROC)” in C represented “area under ROC curve”. “R2” in (C) represented “coefficient of multiple determination”. “S: z” in (C) represented “Z value of Spiegelhalter Z-test”. “S: p” in (C) represented “P value of Spiegelhalter Z-test”. |
Discussion
This study retrospectively analyzed the clinical characteristics, antibiotic susceptibility of pathogens to 17 antibiotics, and risk factors for 30-day mortality in 252 patients with Gram-negative bacteremic pneumonia caused by Escherichia coli and Klebsiella pneumoniae from January 2018 to December 2022. There were multiple differences in clinical characteristics between the survival and non- survival groups. Consistent with epidemiology, the population of this disease is mainly middle-aged and elderly, and we found that males have a higher risk of death than females, which may be due to male smoking and other unhealthy lifestyle habits being more common than in females, as well as a higher prevalence of COPD underlying diseases.11,12 At the same time, this may also be affected by immunological differences between the sexes. Chlamydas S found that testosterone induction of immune suppression in males after puberty leads to immunological differences between the sexes, thus affecting the immune response to infection.13 Patients in the ICU ward had a high mortality rate, but interestingly, in our study, the mortality rate in the surgical ward was lower, and univariate regression analysis showed that surgery may be a potential protective factor. A large prospective study by Raymond DP seems to explain this, they found no difference in outcomes between surgical and non-surgical patients with bacteremic pneumonia in the surgical ward, suggesting that bloodstream infection does not worsen patient outcomes.14 However, the surgeries we recorded included any form of surgery that patients underwent during their pneumonia, which were likely for their initial hospitalization diagnosis. This may be one of the reasons for the deviation in our results. Nonetheless, it is also evidence in a sense that surgery is not a risk factor for bacteremic pneumonia. In addition, carbapenem drugs are widely used in clinical practice as the first choice for serious infections caused by ESBL-producing microorganisms, which has led to an increase in CRE. Klebsiella pneumoniae is the most common CRE. By 2019, the resistance rates of Escherichia coli and Klebsiella pneumoniae to imipenem were 25.3% and 2.0%, respectively. We also found that among Klebsiella pneumoniae strains, 36 (33.7%) were resistant to imipenem, while only 1 (0.7%) strain of Escherichia coli was resistant, which is likely one of the reasons why there was a statistically significant difference in the 30-day mortality of patients with Klebsiella pneumoniae bacteremic pneumonia in univariate analysis.15,16 Because the mortality rate of CRE infections in our study was 60.5%. However, after adjusting for confounding factors, Klebsiella pneumoniae was not an independent risk factor for 30-day mortality, which is consistent with previous studies.6,10 In terms of treatment, whether appropriate empirical treatment and receiving antibiotics ≥3 during hospitalization differed between groups, and univariate analysis showed them as risk factors. The benefit of combined antibiotic therapy for bacteremic pneumonia is currently unclear and can only reduce the mortality rate in critically ill patients. The majority of people in our study who received antibiotics ≥3 during hospitalization may have been due to receiving inappropriate empirical treatment or because of liver and kidney dysfunction that cannot tolerate medication, leading to treatment failure and ultimately affecting the final outcome. Therefore, we suggest that clinicians should pay attention to the results of drug susceptibility tests in a timely manner and guide medication as soon as possible according to the results of drug susceptibility tests, minimizing the number of antibiotic exposures for patients.
Immunosuppression was demonstrated to be an independent risk factor for 30-day mortality in our study of Gram-negative bacteremic pneumonia caused by Escherichia coli or Klebsiella pneumoniae. This appears to contradict the conclusions of some similar studies. In a study of risk factors for Streptococcus pneumoniae bacteremic pneumonia, all eight patients with bacteremic pneumonia who were also receiving immunosuppressive therapy survived (p=1). Another study found that among 60 patients with Klebsiella pneumoniae bacteremic pneumonia and immunosuppression, 34 died within 28 days, but this was not statistically significant on univariate analysis (p=0.054).17,18 However, there are also some similar studies that support our conclusion, finding that septic patients in an immunosuppressed state have a higher mortality rate than those with normal immune function, both at four and twenty-eight days.19 It is undeniable that we have a larger sample size of patients with immunosuppression, which gives our conclusions certain advantages. The lung is the most common target organ for infection in immunosuppressed hosts. A multicenter international study found that the mortality rate of community-acquired pneumonia in immunocompromised hosts (ICH-CAP) was higher than in non-immunocompromised hosts, which also confirms the rationality of our conclusion to some extent.20 However, the small sample size and different definitions of immunosuppressed patients among scholars may be one of the reasons for the different results.
It is worth noting that Pitt score was consistent with previous similar research results in our study and was considered an independent risk factor for 30-day mortality in bacteremic pneumonia, while SOFA score was only significant on univariate analysis.21,22 Although this is different from the conclusion of Chen IR that SOFA score is an independent risk factor for mortality in patients with Klebsiella pneumoniae bacteremic pneumonia, Shu C’s study found that Pitt score was better than SOFA score in terms of mortality from Klebsiella pneumoniae bacteremia.17,23 The Pitt score is widely used to predict mortality in patients with bloodstream infections and has been proven to have good value for both 14-day mortality in patients with bloodstream infections and non-bloodstream infections. As one of the widely used scoring systems, SOFA score is also a powerful tool for predicting patient prognosis. It is possible that due to patient heterogeneity, some iatrogenic confounding factors, and the clinical characteristics of Escherichia coli bacteremic pneumonia, the Pitt score is better than the SOFA score in predicting 30-day mortality in Gram-negative bacteremic pneumonia caused by Escherichia coli or Klebsiella pneumoniae.21
Bacteremic pneumonia is associated with a higher risk of cardiovascular disease and cerebrovascular diseases compared to non-bacteremic pneumonia and other respiratory infections.24 Previous studies have reported a strong association between cardiovascular and cerebrovascular diseases and Streptococcus pneumoniae bacteremic pneumonia, with a 26-fold and 3-fold increase in the risk of myocardial infarction and stroke, respectively, after infection with Streptococcus pneumoniae.25 Additionally, cerebrovascular disease has been confirmed as an independent risk factor for Streptococcus pneumoniae bacteremic pneumonia.18 Our study also found similar results in patients with bacteremic pneumonia caused by Escherichia coli or Klebsiella pneumoniae, with higher 30-day mortality risk in patients with underlying cardiovascular or cerebrovascular diseases, which may be due to similar mechanisms whereby Gram-negative bacteria such as Escherichia coli and Klebsiella pneumoniae exacerbate or induce cerebrovascular diseases in these patients, affecting their prognosis. It is worth noting that we also compared the differences between patients with and without a history of cerebrovascular disease, but the results showed no significant difference (P>0.999). However, due to the small sample size, this finding needs to be confirmed in future studies. Nevertheless, it still suggests that we should be highly vigilant for patients with bacteremic pneumonia caused by either Streptococcus pneumoniae or Gram-negative bacteria such as Escherichia coli or Klebsiella pneumoniae, especially those with underlying cerebrovascular diseases. In addition, during the diagnosis and treatment of cardiovascular and cerebrovascular diseases, we should actively prevent respiratory infections, especially bacteremic pneumonia. For instance, in patients with cerebrovascular disease, it may be beneficial to separate them from those with infectious diseases, strictly adhere to aseptic principles during invasive procedures, and promptly identify the cause of mild infection symptoms and administer antibiotics accordingly.
The severity score CURB-65 is considered to have good predictive value for mortality in bacterial pneumonia and viral pneumonia including COVID-19. Our study also confirms that it has some value in predicting 30-day mortality in patients with Gram-negative bacteremic pneumonia caused by Escherichia coli or Klebsiella pneumoniae.26,27 Generally, when CURB-65 ≥3, it is considered severe or requires admission to the ICU. Our cutoff value was CURB-65 ≥2, which gave us higher sensitivity in our prediction. Spindler C. found that when the cutoff value of CURB-65 was reduced from 3 to 2, the sensitivity increased by 30%, while the specificity decreased from 86% to 67%.28 However, our ROC analysis showed that when the cutoff value was set at 2, the sensitivity reached 90.8%, while the specificity remained at 82.4%. DBP and BUN are both criteria for evaluating CURB-65. We analyzed their weights in relation to mortality. DBP ≤61 scored highest in the nomogram, suggesting that we should pay more attention to blood pressure in clinical practice, especially DBP. As mentioned earlier, elderly patients are more prone to hypotension due to decreased elasticity of blood vessels. Therefore, if the critical value is set as SBP <90 and DBP≤60, DBP may have better efficacy. Blood pressure is an important vital sign and one of the signs of septic shock, so it makes sense that it scores high in our prediction model.29 On the other hand, BUN scored relatively low, which may be because although BUN reflects a patient’s nutritional and metabolic status and is also affected by kidney function and other complex factors, it is not directly related to mortality in patients with bacteremic pneumonia.
In addition, we established a nomogram risk prediction model based on the above six independent risk factors. The ROC curve and PR curve both showed that the model had good performance. Although the calibration curve showed that our model had low goodness of fit, it had some discriminative power, and the low reliability index (−0.008) and brier value (0.057) also indicated that the model had high reliability and accuracy. The decision curve (DCA) showed that the model had certain clinical value and effectiveness. In summary, all data in our study came from a large third-level hospital in our region, which has certain regional representativeness, making our model more suitable for this region. Furthermore, among the risk factors in our model, only one is a laboratory indicator and has been widely used in clinical practice; the remaining five are non-laboratory indicators, making our model convenient to use in clinical settings. In addition, to ensure the accuracy and reliability of our model, we collected comprehensive clinical data and used strict statistical methods for variable selection and model performance evaluation and internal validation to obtain the best model. The establishment of our model aims to provide some reference significance for clinical decision-making in our region. The results of our analysis showed that DBP, immunosuppression, and Pitt score were all above 80 points, suggesting that clinicians should pay attention to changes in these factors during diagnosis and treatment and take appropriate interventions to improve patient outcomes. However, the results of our model prediction are only for reference purposes; clinicians should also make decisions based on their clinical experience.
Limitations
Our study has some limitations. Firstly, this is a single-center study and can only represent the situation in the research hospital; it may not have direct applicability for database modeling but can still provide some reference value for local clinical decision-making. Secondly, retrospective studies inevitably suffer from selection bias and the inability to establish causation; patients with negative blood cultures and undiagnosed pneumonia were not included in this study. Thirdly, the state or reason for admission of patients and the use of antibiotics may affect their final mortality rate. Fourthly, we did not perform sample size estimation, which may lead to statistical inference bias and affect the accuracy of understanding the overall picture. Fifthly, we did not perform multiple comparison corrections. Sixthly, some variables in the baseline table were imputed using MICE, which may lead to inaccurate results. Seventhly, our inclusion and exclusion criteria may not completely exclude the possibility of polymicrobial infection, which may cause some bias in the results. Finally, we only performed internal validation and practice of the model established in this study; we did not supplement updated clinical data for external validation of the model in future studies. This will be our focus in subsequent studies, and we also look forward to similar larger sample studies verifying our findings.
Conclusion
In conclusion, our study provides a relatively comprehensive analysis of the risk factors associated with bacteremic pneumonia caused by Enterobacterales bacteria, specifically Escherichia coli and Klebsiella pneumoniae, in patients with Gram-negative pneumonia. Our findings indicate that DBP (≤61Hgmm), cerebrovascular disease/TIA, immunosuppression, BUN (≥8.39 mmol/L), Pitt score (≥3), and CURB-65 score (≥2) are independent risk factors for 30-day mortality in these patients. And to aid in predicting the risk of 30-day mortality, we have developed a nomogram based on these risk factors. Our nomogram highlights the significant impact of low DBP, pre-existing cerebrovascular disease/TIA, and immunosuppression status on patient outcomes. This has the potential to enhance the quality of comprehensive management and contribute to clinical decision-making, timely prevention of related risks, and ultimately improved patient outcomes.
Ethics Approval and Consent to Participate
Informed consent was acquired from each participant included in the study. Ethics approval was obtained by the Research Ethics Committee of the Second Affiliated Hospital of Nanchang University. Our study complies with the Declaration of Helsinki.
Acknowledgments
This study was supported by a grant from Natural Science Foundation Committee of Jiangxi Province, Youth Fund Project (No.20202BAB216021), Jiangxi Provincial Health Commission, Science and Technology Program Project (No.20201034), the Medical Health Science and Technology Project of Jiangxi Provincial Health Commission (No.202130412), and the Chinese Medical Science and Technology Research Projects of Jiangxi Provincial Administration of Traditional Chinese Medicine (No.2023Z030).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jackson P, Muyanja SZ, Siddharthan T. Health equity and respiratory diseases in low- and middle-income countries. Clin Chest Med. 2023;44(3):623–634. doi:10.1016/j.ccm.2023.03.015
2. Kyu HH, Vongpradith A, Sirota SB, et al. Age-sex differences in the global burden of lower respiratory infections and risk factors, 1990–2019: results from the global burden of disease study 2019. Lancet Infect Dis. 2022;22(11):1626–1647. doi:10.1016/s1473-3099(22)00510-2
3. Guillamet CV, Vazquez R, Noe J, Micek ST, Kollef MH. A cohort study of bacteremic pneumonia: the importance of antibiotic resistance and appropriate initial therapy? Medicine. 2016;95(35):e4708. doi:10.1097/md.0000000000004708
4. Assefa M. Multi-drug resistant gram-negative bacterial pneumonia: etiology, risk factors, and drug resistance patterns. Pneumonia. 2022;14(1):4. doi:10.1186/s41479-022-00096-z
5. Bassetti M, Magnè F, Giacobbe DR, Bini L, Vena A. New antibiotics for Gram-negative pneumonia. Europ Respirat Rev. 2022;31(166):220119. doi:10.1183/16000617.0119-2022
6. John TM, Deshpande A, Brizendine K, Yu PC, Rothberg MB. Epidemiology and outcomes of community-acquired Escherichia coli pneumonia. Open Forum Infect Diseases. 2022;9(1):ofab597. doi:10.1093/ofid/ofab597
7. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. an official clinical practice guideline of the American thoracic society and infectious diseases society of America. Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi:10.1164/rccm.201908-1581ST
8. Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious diseases society of America 2022 guidance on the treatment of extended-spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with difficult-to-treat resistance (DTR-P. aeruginosa). Clinl Infect Dis. 2022;75(2):187–212. doi:10.1093/cid/ciac268
9. Gao CA, Morales-Nebreda L, Pickens CI. Gearing up for battle: harnessing adaptive T cell immunity against gram-negative pneumonia. Front Cell Infect Microbiol. 2022;12:934671. doi:10.3389/fcimb.2022.934671
10. Cheng WL, Hsueh PR, Lee CC, et al. Bacteremic pneumonia caused by extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae: appropriateness of empirical treatment matters. J Microbiol Immunol Infect. 2016;49(2):208–215. doi:10.1016/j.jmii.2014.05.003
11. Chang D, Sharma L, Dela Cruz CS, Zhang D. Clinical epidemiology, risk factors, and control strategies of Klebsiella pneumoniae infection. Front Microbiol. 2021;12:750662. doi:10.3389/fmicb.2021.750662
12. Fei F, J Siegert R, Zhang X, Gao W, Koffman J. Symptom clusters, associated factors and health-related quality of life in patients with chronic obstructive pulmonary disease: a structural equation modelling analysis. J Clin Nurs. 2023;32(1–2):298–310. doi:10.1111/jocn.16234
13. Chlamydas S, Markouli M, Strepkos D, Piperi C. Epigenetic mechanisms regulate sex-specific bias in disease manifestations. J Molecul Med. 2022;100(8):1111–1123. doi:10.1007/s00109-022-02227-x
14. Raymond DP, Pelletier SJ, Crabtree TD, Gleason TG, Pruett TL, Sawyer RG. Impact of bloodstream infection on outcomes among infected surgical inpatients. Annals of Surgery. 2001;233(4):549–555. doi:10.1097/00000658-200104000-00011
15. Gutiérrez-Gutiérrez B, Rodríguez-Baño J. Current options for the treatment of infections due to extended-spectrum beta-lactamase-producing Enterobacteriaceae in different groups of patients. Clin Microbiol Infect. 2019;25(8):932–942. doi:10.1016/j.cmi.2019.03.030
16. Parker JK, Gu R, Estrera GA, et al. Carbapenem-Resistant and ESBL-producing enterobacterales emerging in central Texas. Infect Drug Resist. 2023;16:1249–1261. doi:10.2147/idr.S403448
17. Chen IR, Lin SN, Wu XN, Chou SH, Wang FD, Lin YT. Clinical and microbiological characteristics of bacteremic pneumonia caused by Klebsiella pneumoniae. Front Cell Infect Microbiol. 2022;12:903682. doi:10.3389/fcimb.2022.903682
18. Kang CI, Song JH, Kim SH, et al. Risk factors and pathogenic significance of bacteremic pneumonia in adult patients with community-acquired pneumococcal pneumonia. J Infect. 2013;66(1):34–40. doi:10.1016/j.jinf.2012.08.011
19. Poutsiaka DD, Davidson LE, Kahn KL, Bates DW, Snydman DR, Hibberd PL. Risk factors for death after sepsis in patients immunosuppressed before the onset of sepsis. Scand J Infect Dis. 2009;41(6–7):469–479. doi:10.1080/00365540902962756
20. Di Pasquale MF, Sotgiu G, Gramegna A, et al. Prevalence and etiology of community-acquired pneumonia in immunocompromised patients. Clinl Infect Dis. 2019;68(9):1482–1493. doi:10.1093/cid/ciy723
21. Henderson H, Luterbach CL, Cober E, et al. The Pitt bacteremia score predicts mortality in nonbacteremic infections. Clinl Infect Dis. 2020;70(9):1826–1833. doi:10.1093/cid/ciz528
22. Kim YC, Choi H, Kim YA, et al. Risk factors and microbiological features of recurrent Escherichia coli bloodstream infections. PLoS One. 2023;18(1):e0280196. doi:10.1371/journal.pone.0280196
23. Su C, Tsai IT, Lai CH, Lin KH, Chen CC, Hsu YC. Prediction of 30-day mortality using the quick Pitt bacteremia score in hospitalized patients with Klebsiella pneumoniae infection. Infect Drug Resist. 2023;16:4807–4815. doi:10.2147/idr.S420569
24. Musher DM, Abers MS, Corrales-Medina VF. Acute Infection and Myocardial Infarction. New Engl J Med. 2019;380(2):171–176. doi:10.1056/NEJMra1808137
25. Rögnvaldsson KG, Bjarnason A, Kristinsson K, et al. Acetylsalicylic acid use is associated with improved survival in bacteremic pneumococcal pneumonia: a long-term nationwide study. J Internal Med. 2022;292(2):321–332. doi:10.1111/joim.13485
26. Barlow G, Nathwani D, Davey P. The CURB65 pneumonia severity score outperforms generic sepsis and early warning scores in predicting mortality in community-acquired pneumonia. Thorax. 2007;62(3):253–259. doi:10.1136/thx.2006.067371
27. Wellbelove Z, Walsh C, Perinpanathan T, Lillie P, Barlow G. Comparing the 4C mortality score for COVID-19 to established scores (CURB65, CRB65, qSOFA, NEWS) for respiratory infection patients. J Infect. 2021;82(3):414–451. doi:10.1016/j.jinf.2020.10.015
28. Spindler C, Ortqvist A. Prognostic score systems and community-acquired bacteraemic pneumococcal pneumonia. Europ Resp J. 2006;28(4):816–823. doi:10.1183/09031936.06.00144605
29. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.