Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Risk Factors and Prediction of Chronic Obstructive Pulmonary Disease After Pulmonary Tuberculosis: A Prospective Cohort Study
Authors Ye X, Le S, Han S, Zhang Z, Li Q, Gao F
Received 7 January 2026
Accepted for publication 26 May 2026
Published 15 June 2026 Volume 2026:21 594436
DOI https://doi.org/10.2147/COPD.S594436
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Xingming Ye,1,* Shengbing Le,1,* Shiyun Han,2 Zhuo Zhang,3 Qian Li,1 Fen Gao1
1Department of Tuberculosis Internal Medicine II, Hunan Chest Hospital, Changsha, 410006, People’s Republic of China; 2Department of Electrophysiology, Hunan Chest Hospital, Changsha, 410006, People’s Republic of China; 3Department of Medical Iconography, Hunan Chest Hospital, Changsha, 410006, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fen Gao, Department of Tuberculosis Internal Medicine II, Hunan Chest Hospital, No. 519 Xian Jiahu Road Yuelu District, Changsha, 410006, People’s Republic of China, Tel +86-13575220627, Email [email protected] Qian Li, Department of Tuberculosis Internal Medicine II, Hunan Chest Hospital, No. 519 Xian Jiahu Road Yuelu District, Changsha, 410006, People’s Republic of China, Tel +86-15973180832, Email [email protected]
Background: Pulmonary tuberculosis (PTB) is increasingly recognized as a major precursor of chronic obstructive pulmonary disease (COPD). However, validated tools to predict the risk of COPD following PTB cure remain limited. Early identification of individuals at high risk is essential to facilitate targeted follow-up and preventive interventions.
Methods: This prospective cohort study was conducted at Hunan Chest Hospital. Adults with newly diagnosed PTB who completed standard anti-tuberculosis treatment were enrolled between January and June 2023 and followed until June 2025. Follow-up assessments were performed monthly during the first 3 months, quarterly from months 6 to 12, and every 6 months thereafter, with standardized evaluation of respiratory symptoms and lung function. Incident COPD was defined as a post-bronchodilator FEV1/FVC ratio < 0.70. Candidate predictors spanning demographic, clinical, inflammatory, and immunological domains were initially screened using random forest ranking and least absolute shrinkage and selection operator regression, followed by multivariable logistic regression. A prediction model was developed and internally validated using bootstrap resampling. Calibration was assessed using calibration plots with 1000 bootstrap iterations, and clinical utility was evaluated by decision curve analysis.
Results: During follow-up, 83 of 324 participants (25.6%) developed COPD. Older age (≥ 65 years), active smoking, cavitary PTB, invasive fungal disease, dyspnea, an elevated systemic immune–inflammation index (SII), and a reduced CD4⁺/CD8⁺ T-cell ratio were independently associated with COPD development. A prediction model incorporating these seven variables demonstrated good discrimination, with an area under the receiver operating characteristic curve of 0.806 (95% CI: 0.751– 0.861), and satisfactory calibration. Internal validation yielded a bootstrap-corrected concordance index of 0.787, indicating favorable clinical utility across a broad range of decision thresholds.
Conclusion: More than one-quarter of patients developed COPD after PTB cure, highlighting the substantial burden of post-tuberculosis respiratory sequelae. The proposed prediction model enables individualized risk stratification and may support early surveillance and targeted preventive strategies, extending post-TB care beyond microbiological cure to long-term respiratory outcomes.
Keywords: pulmonary tuberculosis, chronic obstructive pulmonary disease, risk prediction model, nomogram, receiver operating characteristic analysis
Introduction
Chronic obstructive pulmonary disease (COPD) is currently the third leading cause of death worldwide and affects hundreds of millions of individuals globally.1 Chronic respiratory diseases, particularly COPD, continue to impose a substantial and increasing global health burden. Recent estimates from the World Health Organization indicate that COPD will remain a major cause of morbidity and mortality, with important implications for health equity across regions (https://www.who.int/europe/publications/i/item/WHO-EURO-2025-12340-52112-79990). Modeling studies project that the global number of people aged ≥25 years living with COPD will increase by approximately 23% between 2020 and 2050, reaching nearly 600 million cases by mid-century.2 In 2019 alone, COPD accounted for an estimated 212.3 million prevalent cases, 3.3 million deaths, and 74.4 million disability-adjusted life years (DALYs) globally,3 showing its substantial and growing public health burden.
At the same time, post-tuberculosis lung disease (PTLD) represents a major yet underrecognized contributor to chronic respiratory morbidity. PTLD is estimated to account for nearly 50% of the total DALY burden attributable to tuberculosis (TB), imposing high social and economic costs.4 Epidemiological evidence increasingly supports a strong association between pulmonary TB (PTB) and subsequent COPD. A systematic review and meta-analysis showed that, compared with individuals without TB, those with a history of PTB have a significantly increased risk of developing COPD (odds ratio [OR] = 2.59, 95% confidence interval [CI]: 2.12–3.15; P< 0.001).5 Despite high microbiological cure rates with modern anti-tuberculosis chemotherapy, sputum conversion and radiographic improvement alone do not signify complete recovery. Recent commentaries have therefore emphasized the need to explicitly define and incorporate PTLD as a core long-term outcome in order to more comprehensively assess the enduring sequelae and functional consequences of PTB.6
Growing evidence indicates that structural lung damage and functional impairment often persist after PTB cure, with long-term implications for respiratory health.7,8 In a cohort of patients with confirmed TB, pulmonary function testing revealed abnormalities in approximately three-quarters of those assessed, including obstructive, restrictive, and impaired gas transfer patterns.9 These abnormalities reflect the core pathophysiological features of COPD, supporting a mechanistic link between post-PTB pulmonary sequelae and incident COPD. During active infection, intense inflammatory injury driven by Mycobacterium tuberculosis leads to parenchymal necrosis and tissue destruction.10 Notably, TB is characterized by simultaneous tissue injury and repair processes,11 such that even after bacteriological cure, patients frequently exhibit extensive fibrotic scarring, bronchiectasis, emphysema, and pleural thickening.12 These residual structural abnormalities disrupt normal lung architecture, impair pulmonary compliance and gas exchange, and create a pathological substrate for chronic respiratory symptoms and recurrent infections.9,13
Despite growing recognition of PTB as a precursor to chronic airflow limitation, robust evidence regarding risk factors for COPD development following PTB cure remains limited, and validated risk prediction models are lacking. This knowledge gap hampers targeted long-term follow-up and the implementation of early preventive interventions in clinical practice. Early identification and characterization of PTLD are therefore essential for tailored post-TB care, including targeted surveillance, smoking cessation, pulmonary rehabilitation and early therapeutic intervention for individuals at increased risk of long-term respiratory impairment.
To address this unmet need, the present prospective cohort study enrolled patients with newly diagnosed PTB who completed standard anti-tuberculosis treatment and were followed after cure. The study aimed to identify factors associated with COPD development after PTB cure and to develop an internally validated risk prediction model. This model is intended to support individualized risk stratification, guide tailored follow-up strategies and inform early preventive or therapeutic interventions, thereby improving clinical decision-making and long-term respiratory outcomes after PTB.
Materials and Methods
Ethics
This prospective study was approved by the Institutional Ethics Committee of Hunan Chest Hospital (Approval No. LS2025112602). Written informed consent was obtained from all participants prior to enrollment. The study was conducted in accordance with the Declaration of Helsinki and applicable national regulations.
Participants
Between January and June 2023, consecutive adult patients with newly diagnosed PTB who presented at our hospital were screened for eligibility. Patients were eligible if they were aged ≥18 years; met the diagnostic criteria for PTB according to the Chinese national standard Diagnosis for Pulmonary Tuberculosis (WS 288–2017);14 completed the full standard anti-tuberculosis treatment regimen at our institution; had sputum smear negativity during the final month of treatment; were able to understand the study procedures and comply with follow-up; and provided written informed consent.
The study cohort was established after completion of anti-tuberculosis treatment. In this study, “baseline” refers to the post-treatment assessment performed before hospital discharge and before the start of follow-up for incident COPD. This time point was used to collect candidate predictor variables and to confirm that participants had completed treatment and had no known COPD before follow-up. This investigation was designed as a prospective cohort study; therefore, no participant matching was performed, because the objective was to evaluate predictors of incident COPD within a single post-treatment PTB cohort.
Patients were excluded if they had a pre-existing diagnosis of COPD or other chronic respiratory diseases prior to their current PTB diagnosis; concomitant infectious diseases (including hepatitis or HIV); malignancy or autoimmune disease; pregnancy or lactation; incomplete clinical data or were lost to follow-up; or experienced a recurrence of PTB during the follow-up period. Participants with incomplete outcome data or loss to follow-up were excluded from the final analysis, and the number of excluded cases and reasons for exclusion are shown in the participant flow diagram.
Outcomes and Follow-Up
After completion of standard anti-tuberculosis treatment and discharge from hospital, participants were followed by trained study personnel through scheduled outpatient visits until June 2025. Follow-up assessments were conducted monthly during the first 3 months, every 3 months from months 6 to 12, and every 6 months thereafter.
At each follow-up visit, respiratory symptoms were assessed, and pulmonary function testing was performed. Incident COPD was defined as persistent airflow limitation, indicated by a post-bronchodilator forced expiratory volume in one second to forced vital capacity ratio (FEV1/FVC) of less than 70% or below the lower limit of normal, in accordance with international guidelines.15
Data Collection
Demographic and clinical information was collected using standardized case report forms based on structured patient interviews and electronic medical record review. All data were obtained by trained clinicians and research staff according to a predefined protocol. All candidate predictors used for model development were collected before the occurrence of incident COPD during follow-up, thereby ensuring the temporal sequence between predictor assessment and outcome development.
Demographic information was collected, including age, sex, height, weight, residential area, educational level, marital status, smoking status, alcohol consumption, hypertension, diabetes, prior tuberculosis, Bacillus Calmette–Guérin (BCG) vaccination status, and history of dust exposure. Smoking and alcohol consumption were assessed for the 6 months before the baseline survey. Active smoking was defined as a lifetime consumption of ≥100 cigarettes or equivalent tobacco exposure,16 whereas passive smoking was defined as exposure to secondhand smoke for more than 15 min per day.17 Alcohol consumption was defined as drinking at least once per week for a duration of six months18 or longer. Dust exposure was defined as occupational or environmental exposure for at least one year, with an average weekly duration exceeding 10 h.19
Clinical variables included active PTB, cavitary PTB, invasive fungal disease (IFD), systemic corticosteroid use, and pre-discharge symptoms (nutritional status, cough, dyspnea, chest tightness, and chest pain). Active and cavitary PTB were defined based on the WS 288–2017 criteria and chest computed tomography findings. IFD was assessed using serum galactomannan and (1→3)-β-D-glucan assays, combined with compatible clinical manifestations and radiologic features.20 Nutritional status was evaluated using the Nutritional Risk Screening 2002 (NRS-2002) tool, with a score of ≥3 indicating nutritional risk.21
Fasting peripheral venous blood samples were collected at admission for complete blood counts and lymphocyte subset analyses, including CD4⁺ and CD8⁺ T-cell counts. Blood cell–derived inflammatory indices, including the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), and systemic inflammation response index (SIRI), were calculated. Immune dysfunction was defined as a CD4⁺ T-cell count <500 cells/µL or a CD4⁺/CD8⁺ ratio <1.
Pulmonary function tests were conducted prior to discharge using standardized procedures. Measured parameters included FVC, peak expiratory flow (PEF), FEV1, and the FEV1/FVC ratio. Spirometry was performed by certified respiratory technicians and interpreted by experienced pulmonologists according to American Thoracic Society/European Respiratory Society guidelines.
Statistical Analysis
The final cohort comprised 324 participants, of whom 83 developed COPD during follow-up. This yielded an events-per-variable ratio of approximately 11.9 for the final seven-predictor model, exceeding the commonly used minimum threshold of 10 events per variable for multivariable logistic regression.22 This supported the adequacy of the sample size for the final model and helped reduce the risk of model overfitting.
Statistical analyses were performed using IBM SPSS Statistics version 25.0, R version 4.3.3, and MedCalc. The normality of continuous variables was assessed using the Shapiro–Wilk test. Normally distributed data are presented as mean ± standard deviation, whereas non-normally distributed data are presented as median (interquartile range). Categorical variables are reported as counts and percentages. Univariate comparisons between participants who developed COPD and those who did not were conducted using Student’s t-test, the Mann–Whitney U-test, or the χ²-test, as appropriate. Variables with P< 0.05 were considered for subsequent analyses.
To address collinearity among blood cell–derived inflammatory indices, a random forest model was used to rank their relative importance based on the percentage increase in mean squared error (%IncMSE). Least absolute shrinkage and selection operator (LASSO) regression was then applied to identify potential predictors among demographic, clinical, and laboratory variables. Variables retained in the most parsimonious model were entered into a multivariable binary logistic regression model to determine independent risk factors for post-PTB COPD.
A prediction model was constructed from the identified independent predictors and visualized using a nomogram. Model performance was evaluated using receiver operating characteristic (ROC) curves, area under the curve (AUC), sensitivity, specificity, and the Youden index. Internal validation was performed using bootstrap resampling with 1000 iterations. Discrimination was quantified using the concordance index, and calibration was assessed using bootstrap-corrected calibration plots comparing predicted and observed probabilities.23 The Hosmer–Lemeshow goodness-of-fit test was additionally performed. Clinical utility was evaluated using decision curve analysis, which quantified net benefit across a range of threshold probabilities. All statistical tests were two-sided, and P value <0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 697 patients with newly diagnosed PTB were initially screened. Of these, 373 were excluded for the following reasons: pre-existing COPD or other chronic respiratory diseases before the current PTB diagnosis (n = 60), concomitant infectious diseases such as hepatitis or HIV infection (n = 31), malignancy or autoimmune disease (n = 5), pregnancy or lactation (n = 10), incomplete clinical data (n = 75), loss to follow-up (n = 172), or recurrent PTB during follow-up (n = 22). Finally, 324 participants were included in the analysis. The participant selection process is shown in Figure 1. Baseline characteristics were compared between included and excluded patients and are presented inSupplementary Table 1. No statistically significant differences were observed between the two groups, indicating that the final analytic cohort was broadly comparable with the initially eligible population.
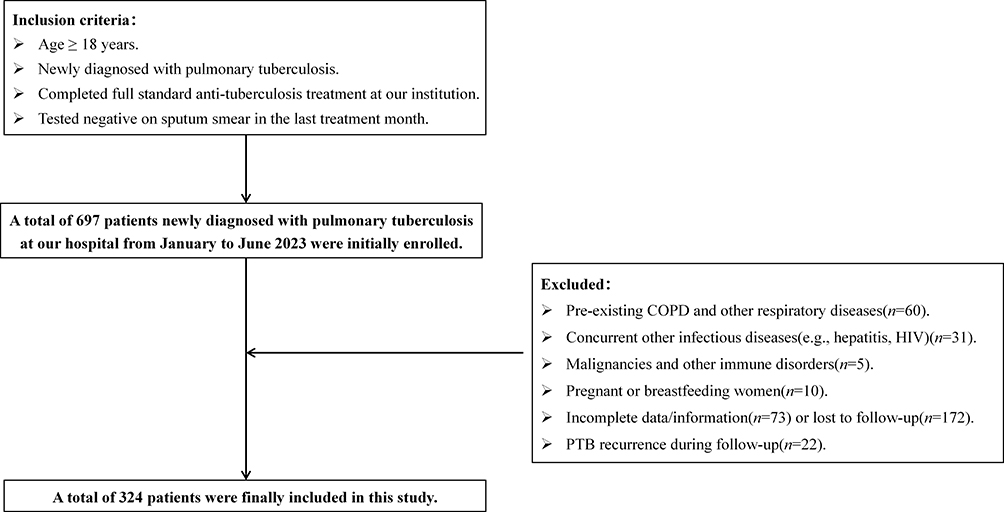 |
Figure 1 Flow diagram of participant screening, inclusion, and exclusion. |
The baseline characteristics of the 324 included participants are shown in Table 1. The mean age was 51.8 ± 15.9 years, with 23.8% aged ≥65 years, and 69.8% were male. The mean body mass index was 22.0 ± 3.5 kg m−². Active smoking was reported by 53.4% of participants and passive smoking by 58.0%. Hypertension and diabetes were present in 32.1% and 29.3%, respectively, and 87.3% had documented BCG vaccination.
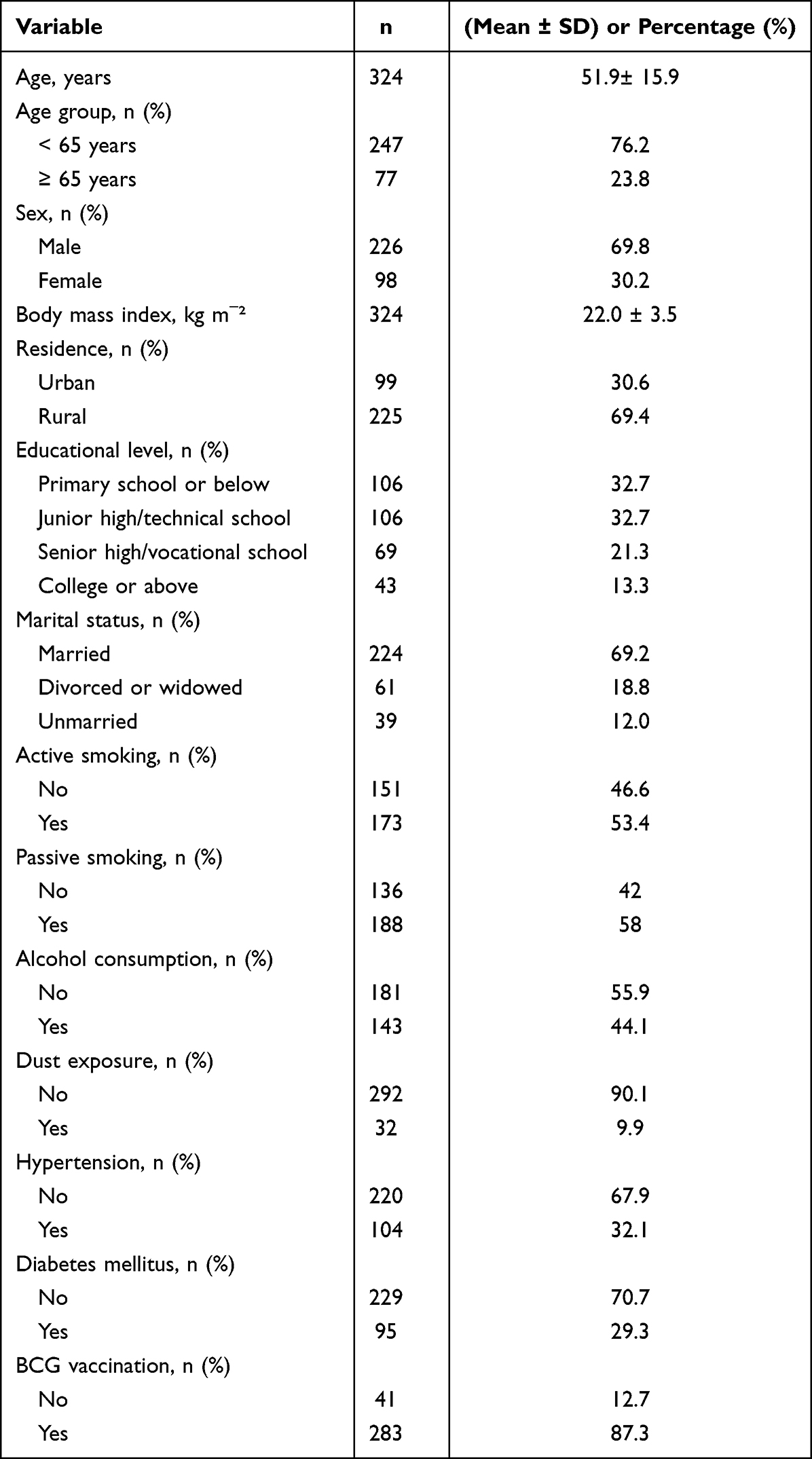 |
Table 1 Baseline Demographic Characteristics of Subjects in This Study (n = 324) |
Among them, pulmonary function tests showed a mean FVC of 2.6 ± 0.2 L, FEV1 of 1.8 ± 0.2 L, PEF of 72.7 ± 6.7 L/min, and FEV1/FVC ratio of 69.1 ± 7.8%. During follow-up, 83 of 324 participants developed COPD, corresponding to a cumulative incidence of 25.6%.
Risk Factors for COPD After PTB
Univariate Analysis
Baseline demographic characteristics, clinical features, and laboratory indices in the non-COPD and COPD groups are shown in Table 2. Participants who developed COPD were older and more likely to report active smoking, passive smoking, dust exposure, and absence of BCG vaccination (all P< 0.05). They also had higher prevalences of cavitary pulmonary tuberculosis, IFD, systemic corticosteroid use, cough, and dyspnea. Laboratory analyses revealed lower lymphocyte counts, higher neutrophil counts, elevated inflammatory indices (NLR, PLR, SII, and SIRI), and a reduced CD4⁺/CD8⁺ T-cell ratio (all P< 0.05). Correlation analyses showed positive associations between COPD occurrence and inflammatory indices (Supplementary Figure 1). Random forest analysis identified SII as the most influential inflammatory marker and selected it for subsequent modeling (Supplementary Figure 2).
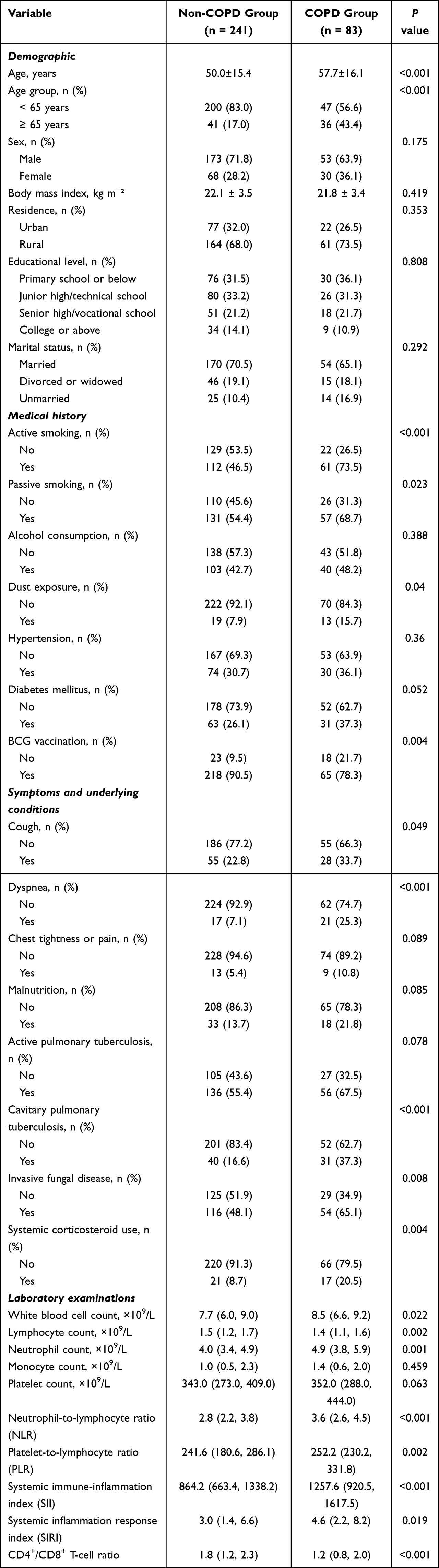 |
Table 2 Comparison of Baseline Demographic Characteristics, Clinical Features, and Laboratory Indices Between Non-COPD Group and COPD Group (n=324) |
Identification of Candidate Predictors Using LASSO Regression
Thirteen variables associated with COPD occurrence in univariate analyses (P< 0.05) were entered into a LASSO regression model (Table 3). As shown in Figure 2, regression coefficients were progressively shrunk toward zero to minimize overfitting. Using ten-fold cross-validation, the most parsimonious model retained 11 variables with non-zero coefficients: age, active smoking, dust exposure, BCG vaccination status, cavitary pulmonary tuberculosis, IFD, systemic corticosteroid use, cough, dyspnea, SII, and the CD4⁺/CD8⁺ T-cell ratio.
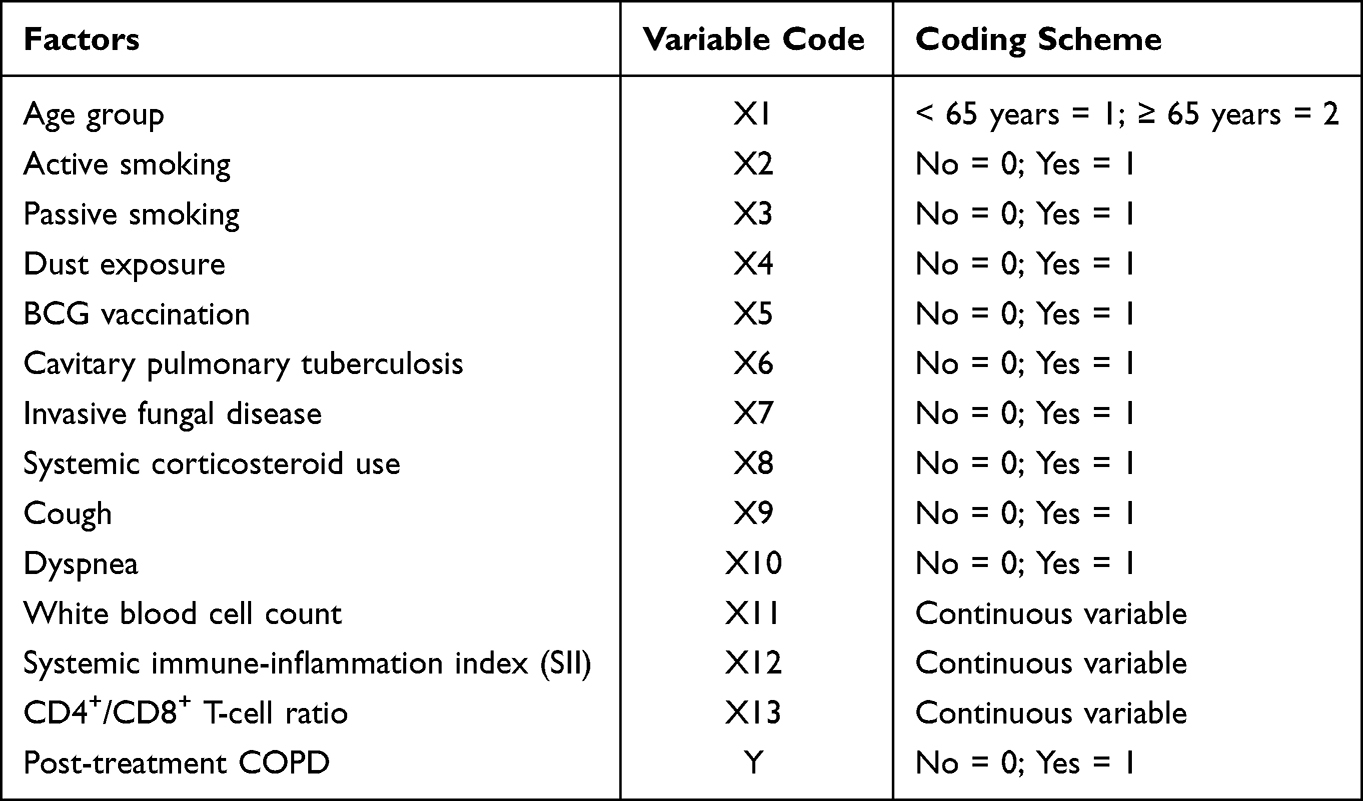 |
Table 3 Coding Scheme for Variables Included in the Regression Analyses |
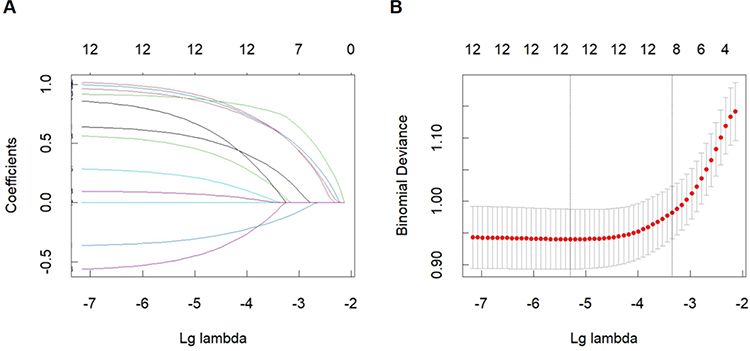 |
Figure 2 Variable selection for predictors of post-tuberculosis COPD using LASSO regression. (A) Coefficient profiles of candidate predictors as a function of the penalization parameter (λ). (B) Ten-fold cross-validation for selection of the optimal λ, resulting in retention of 11 variables with non-zero coefficients. |
Multivariable Logistic Regression Analysis
The 11 variables selected by LASSO regression were subsequently entered into a multivariable logistic regression model. Collinearity diagnostics showed variance inflation factors <2 for all predictors, indicating no significant multicollinearity (Supplementary Table 2). The omnibus test of model coefficients was significant (χ²=90.270, P<0.05). Model calibration was satisfactory, as indicated by the Hosmer–Lemeshow goodness-of-fit test (χ²=3.553, P=0.895).
As shown in Table 4, seven variables were independently associated with the development of COPD after PTB cure. Participants aged ≥65 years had a higher risk of COPD compared to those aged <65 years (OR 2.512, 95% CI 1.258–5.016; P=0.009). Active smoking was associated with an almost threefold increased risk (OR 2.815, 95% CI 1.505–5.263; P=0.001). Cavitary pulmonary tuberculosis was also an independent risk factor (OR 2.689, 95% CI 1.305–5.541; P=0.007), as was IFD (OR 1.923, 95% CI 1.039–3.560; P=0.037).
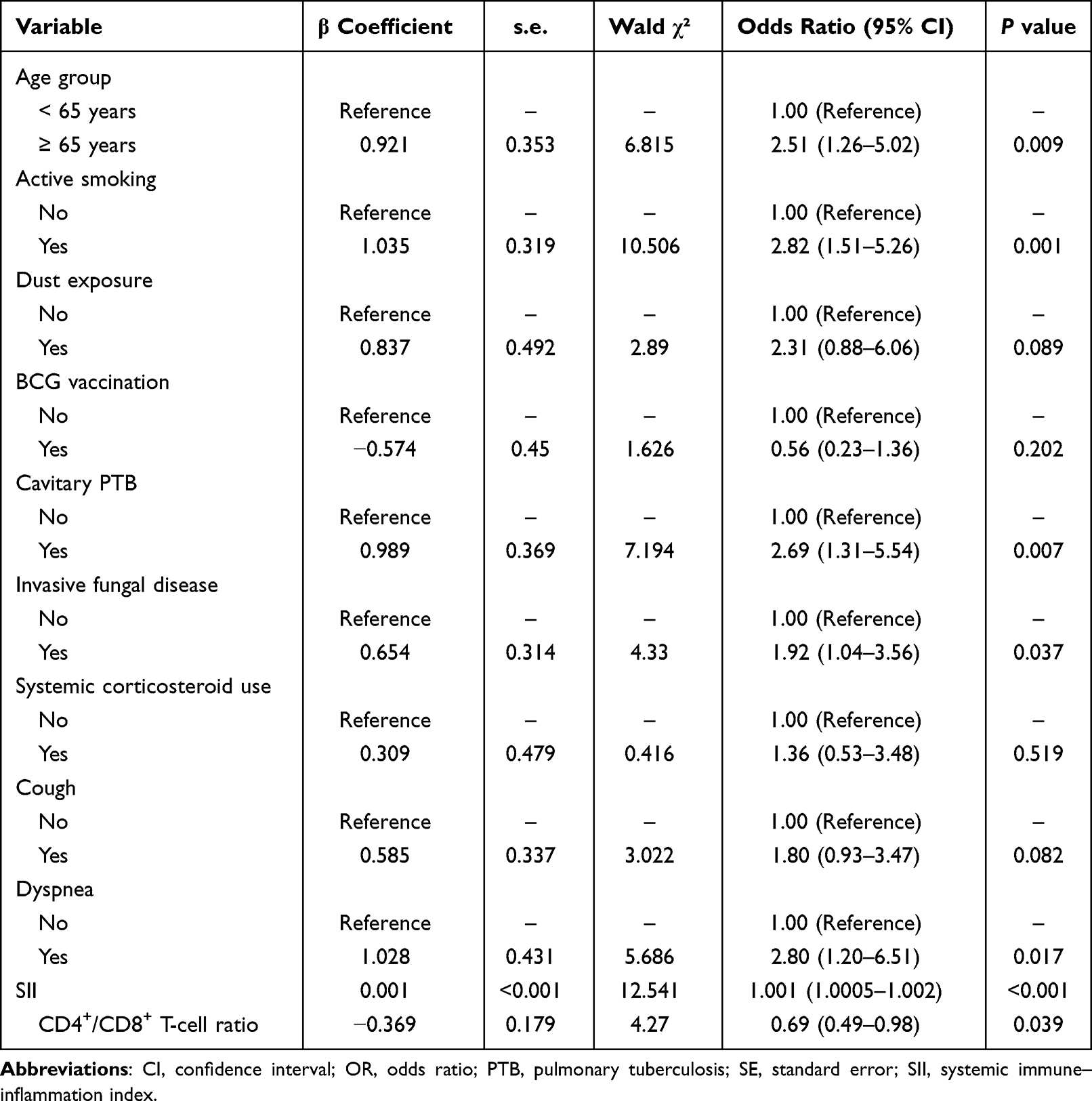 |
Table 4 Multivariable Logistic Regression Analysis of Factors Associated with COPD After PTB Cure |
Dyspnea was significantly associated with increased COPD risk (OR, 2.796, 95% CI 1.201–6.510; P=0.017). Higher SII values were independently associated with a greater risk of COPD (OR, 1.001; 95% CI, 1.0005–1.002; P<0.001), whereas a lower CD4⁺/CD8⁺ T-cell ratio was also a significant predictor of increased risk (OR, 0.692, 95% CI 0.487–0.981; P=0.039).
Development and Validation of the Prediction Model
A prediction model incorporating age, active smoking, cavitary pulmonary tuberculosis, IFD, dyspnea, SII, and the CD4⁺/CD8⁺ T-cell ratio was developed and visualized as a nomogram (Supplementary Table 3 and Figure 3). Model discrimination was assessed using ROC analysis (Figure 4). The AUC was 0.806 (95% CI, 0.751–0.861), with a sensitivity of 74.7%, specificity of 78.8%, and a Youden index of 0.535.
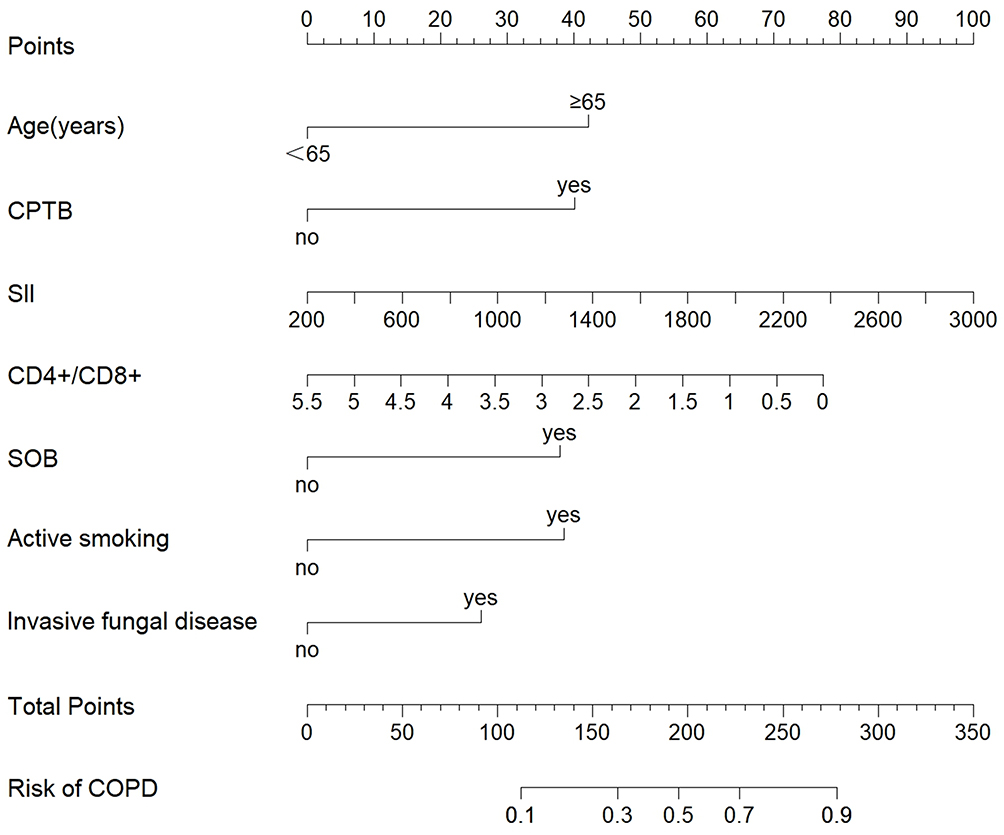 |
Figure 3 Nomogram for predicting the risk of chronic obstructive pulmonary disease after pulmonary tuberculosis cure. The nomogram integrates age, active smoking status, cavitary pulmonary tuberculosis (CPTB), invasive fungal disease, dyspnea, systemic immune-inflammation index (SII), and the CD4⁺/CD8⁺ T-cell ratio to estimate individualized COPD risk. |
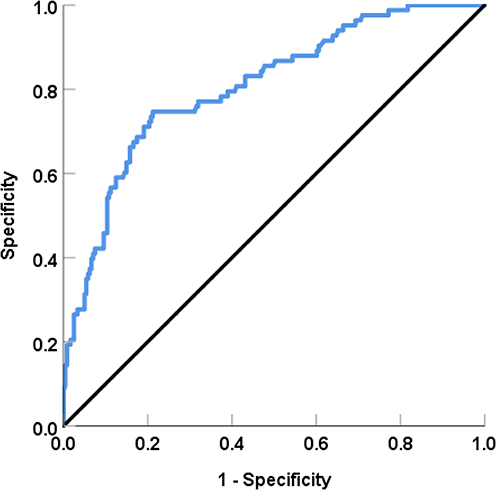 |
Figure 4 Discriminative performance of the prediction model for chronic obstructive pulmonary disease after pulmonary tuberculosis cure. Receiver operating characteristic curve illustrating the ability of the prediction model to discriminate between participants who did and did not develop COPD after pulmonary tuberculosis cure. The area under the curve was 0.806 (95% CI 0.751–0.861). At the optimal cut-off value, the model achieved a sensitivity of 74.7% and a specificity of 78.8%, corresponding to a Youden index of 0.535. The diagonal line represents the reference line of no discrimination. |
Internal validation using bootstrap resampling (1000 iterations) yielded a concordance index of 0.806 before optimism correction and 0.787 after correction, indicating stable discriminative performance. Calibration analysis showed close agreement between predicted and observed risks, with a mean absolute error of 0.025 (Supplementary Figure 3). Decision curve analysis demonstrated that the prediction model provided a net clinical benefit across a wide range of threshold probabilities (0.08–0.94). Within this range, the model consistently outperformed both the treat-all and treat-none strategies, supporting its favorable clinical utility for risk stratification after PTB cure (Supplementary Figure 4).
Discussion
Approximately 60% of individuals experience persistent pulmonary function impairment following the completion of PTB treatment, highlighting the substantial burden of PTLD.7 Although the diagnostic criteria for chronic respiratory diseases such as COPD continue to evolve, persistent airflow limitation remains a central feature of their definition. Despite growing international evidence linking PTB to the subsequent development of COPD, validated tools for predicting the risk of COPD after PTB cure remain limited. Early identification is clinically important, as it enables timely intervention. However, post-TB COPD is clinically heterogeneous, often presenting with overlapping respiratory symptoms and, in some cases, residual tuberculosis-related systemic manifestations, which complicate early recognition and management.4 These challenges highlight the need for reliable risk-prediction tools.
This prospective cohort study was therefore designed to identify risk factors for COPD following PTB cure and to develop a clinically applicable prediction model. During follow-up, 83 of 324 participants (25.6%) developed COPD, confirming the substantial burden of post-tuberculosis respiratory sequelae. Multivariable analysis identified older age (≥65 years), active smoking, cavitary PTB, IFD, dyspnea, an elevated SII, and a reduced CD4⁺/CD8⁺ T-cell ratio as independent predictors. By integrating these seven variables, we constructed and internally validated a prediction model that demonstrated good discrimination (AUC = 0.806; 95% CI, 0.751–0.861), satisfactory calibration, and favorable clinical utility as evidenced by decision curve analysis. Compared with previous studies that relied primarily on cross-sectional or retrospective designs to identify risk factors for post-tuberculosis airflow limitation, the present study provides prospective evidence and integrates these predictors into a unified, clinically applicable risk prediction model. The model therefore extends existing knowledge by offering a pragmatic framework for individualized risk assessment and informed clinical decision-making in post-TB care.
At present, evidence on the development of COPD following successful treatment of PTB remains limited, primarily derived from cross-sectional studies and retrospective analyses. For example, Park et al24 reported that a history of PTB adversely affected COPD severity and that this effect persisted for several years, ultimately leading to poorer long-term outcomes. Similarly, Wang et al25 demonstrated that COPD patients with prior PTB exhibited more severe airflow limitation and a greater symptom burden. Long-term functional impairment after PTB has also been documented by Nishi et al,26 who showed that residual parenchymal destruction following cure leads to impaired lung compliance, peripheral airway collapse, air trapping, and progressive decline in pulmonary function. Imaging-based studies further support these observations. Salvagno et al27 identified residual fibrotic lesions and bronchiectasis after PTB as key anatomical substrates driving COPD-like pathological changes, particularly among patients with multilobe involvement or cavitary disease. Collectively, these findings indicate a clear association between PTB and subsequent COPD. Consistent with this evidence, our prospective cohort demonstrated that a substantial proportion of newly diagnosed PTB patients developed COPD after completing standard anti-tuberculosis therapy, with an incidence of 25.6% (83/324). These results align with recent prospective data from a Chinese cohort,28 which reported a considerable burden of post-tuberculosis obstructive disease even among never-smokers, and with a multicentre study from Romania29 showing that prior PTB accelerates both the onset and severity of COPD, with cavitary disease identified as a significant risk factor. Together, these prospective findings strengthen the evidence for a temporal and potentially causal relationship between PTB and COPD.
In the present study, older age and active smoking emerged as independent risk factors for COPD following PTB cure. Patients aged ≥65 years had a significantly higher risk of developing COPD than younger individuals, consistent with the established epidemiological characteristics of COPD and prior reports by Wang et al30 and Guo et al31 Age-related physiological changes, including reduced lung elastic recoil and progressive small airway dysfunction, may synergize with PTB-induced structural lung injury, collectively accelerating the progression of airflow limitation.32,33 Unlike most previous studies that focused solely on active smoking, we evaluated both active and passive tobacco exposure. Although both were associated with COPD occurrence in univariate analyses, only active smoking remained significant in multivariable models. Toxic components of cigarette smoke directly damage the airway epithelium and lung parenchyma while amplifying the chronic inflammatory milieu that persists after PTB cure, resulting in a synergistic detrimental effect on lung structure and function.34,35 While smoking is a well-recognized risk factor for COPD,36,37 the potential contribution of passive smoking should not be overlooked, particularly in susceptible populations.38 Emerging evidence further indicates that COPD in low- and middle-income countries is increasingly driven by factors beyond smoking, including prior pulmonary infections such as tuberculosis, environmental exposures, and socioeconomic determinants.39,40 These observations underscore the relevance of tuberculosis as a key contributor to chronic airflow limitation and reinforce the clinical importance of identifying at-risk individuals following PTB cure.
We further identified cavitary pulmonary tuberculosis, IFD, and dyspnea as independent predictors of COPD following PTB cure. Cavitary PTB represents one of the most destructive forms of tuberculosis and plays a pivotal role in post-PTB COPD development. Extensive parenchymal destruction and fibrosis associated with cavitary disease result in ineffective ventilation and irreversible airway distortion, leading to dynamic airflow limitation.41,42 Even after mycobacterial clearance, the fibrotic and granulomatous cavity wall may persist as a chronic, non-infectious inflammatory focus,43 continuously releasing inflammatory mediators that promote ongoing tissue remodeling and systemic immune activation, thereby providing a clear anatomical and biological basis for persistent airflow obstruction.
Emerging evidence suggests that IFD is a novel risk factor for COPD development after PTB cure.44,45 Residual cavities and bronchiectatic airways provide an optimal environment for fungal colonization or infection. Persistent fungal burden may trigger recurrent local immune activation, resulting in airway wall thickening, mucus retention, and progressive functional impairment.46 Such a “secondary insult” may play a critical role in the pathophysiological evolution of PTB-associated COPD.
Dyspnea persisting after PTB cure likely reflects early airflow limitation or impaired pulmonary reserve and may serve as a readily identifiable clinical signal of impending COPD. Its inclusion as a predictor highlights the importance of symptom-based surveillance for early risk identification.
In addition to clinical and radiological factors, elevated SII and a reduced CD4⁺/CD8⁺ T-cell ratio were independently associated with COPD development following PTB cure. Previous studies have highlighted the roles of neutrophils, cytokines, and other inflammatory mediators in lung injury and PTLD.47–49 Inflammatory biomarkers have also been implicated in tuberculosis-associated obstructive pulmonary disease; for example, the systemic inflammation response index (SIRI) has been shown to predict an increased risk of obstructive disease in patients with tuberculosis, supporting the biological plausibility of inflammation-driven airway remodeling.39 SII, a composite index integrating neutrophil, platelet, and lymphocyte counts, provides a more comprehensive reflection of systemic inflammatory status and immune balance. Consistent with findings from Yu et al50 and Mammadova et al51 higher SII levels were associated with an increased risk of COPD, likely reflecting sustained systemic inflammation that exacerbates chronic lung injury and aberrant repair processes.52 This inflammatory milieu may synergize with structural lung damage, directly promoting airway remodeling and emphysematous changes.53 Notably, SII has also been linked to PTB disease severity and may serve as a predictive biomarker.54 The CD4⁺/CD8⁺ T-cell ratio is a central indicator of immune homeostasis.55 A reduced CD4⁺/CD8⁺ T-cell ratio suggests immune imbalance, potentially related to immunosenescence or chronic immune activation leading to T-cell exhaustion.56,57 The persistence of this imbalance after PTB cure implies incomplete immune recovery and a shift toward chronic immune dysregulation, which may impair the immune-mediated regulation of lung repair and regeneration.58,59 Together, the dominance of inflammatory injury (as indicated by high SII) and the relative deficiency in immune repair capacity (reflected by a low CD4⁺/CD8⁺ ratio) constitute a key pathophysiological framework driving COPD development and progression following PTB.
In this study, we developed a prediction model incorporating seven variables—age, active smoking, cavitary pulmonary tuberculosis, IFD, dyspnea, SII, and the CD4⁺/CD8⁺ T-cell ratio—and demonstrated good discriminative performance, with an AUC of 0.806 (95% CI, 0.751–0.861). The model exhibited stable and reliable predictive performance, suggesting a reasonable degree of generalizability. This robustness can be attributed to the rigorous methodological framework employed. Specifically, machine-learning–assisted variable selection was combined with multivariable logistic regression, and model performance was comprehensively evaluated using complementary indices of discrimination, calibration, and clinical utility.
This approach facilitated the identification of an optimal and parsimonious model while mitigating overfitting and selection bias. In addition, the contribution of individual predictors was quantified using SHAP values, enhancing model transparency and interpretability. From a clinical perspective, the integration of demographic, behavioral, disease severity–related, inflammatory, and immune parameters enables a multidimensional and pragmatic approach to risk assessment. This model enables the rapid estimation of individual risk following PTB cure and supports early risk stratification. Its application may facilitate targeted follow-up, early warning, and timely preventive interventions in routine clinical practice, thereby improving long-term respiratory outcomes and advancing comprehensive post-tuberculosis care. Importantly, the proposed model is intended for risk stratification and clinical prediction rather than for establishing causal relationships. Given the observational design and the application of multiple variable selection techniques, including random forest ranking and LASSO regression, the identified predictors should be interpreted as indicators of risk rather than direct causal determinants of post-PTB COPD.
Despite its strengths as a prospective, disease-specific cohort study with comprehensive risk assessment, several limitations merit consideration. First, this was a single-center study without external validation; however, internal validation using bootstrap resampling was performed to maximize data utilization and ensure model robustness, and the adequate number of outcome events relative to predictors further mitigated the risk of overfitting. Second, given the chronic and progressive nature of COPD, the relatively short follow-up period may have led to an underestimation of COPD incidence. Third, exclusion of participants with missing data or loss to follow-up may have introduced selection bias; nevertheless, the prospective design with structured follow-up and the relatively low proportion of excluded participants likely attenuated this impact. Fourth, other incident respiratory diseases during follow-up, such as asthma, bronchiectasis, or interstitial lung disease, were not systematically evaluated and may have contributed to airflow limitation, potentially leading to outcome misclassification and affecting the accuracy of incidence estimates and the predictive performance of the model. Fifth, patients with recurrent PTB after cure were excluded to ensure cohort homogeneity; however, these individuals represent a particularly high-risk group for chronic pulmonary sequelae, potentially limiting the generalizability of the findings. Moreover, differences in tuberculosis prevalence, smoking behaviors, comorbidity profiles, and healthcare resources across clinical settings and countries may influence model performance. External validation in independent cohorts from diverse geographic regions and clinical environments is therefore essential before widespread clinical implementation. Finally, the formal definition of PTLD was published in 2025, after the study was designed; consequently, COPD cases were not classified according to PTLD criteria.60 Future studies should incorporate standardized PTLD definitions to enhance comparability and interpretability across investigations.
Conclusion
In conclusion, this prospective cohort study showed that COPD was common among patients after completion of treatment for newly diagnosed PTB. Older age, active smoking, cavitary PTB, invasive fungal disease, dyspnoea, elevated SII and a reduced CD4⁺/CD8⁺ T-cell ratio were independently associated with COPD development. By integrating these clinical, radiological, inflammatory and immunological predictors, we developed and internally validated a risk prediction model with good discrimination and satisfactory calibration. This model may provide a practical framework for individualized risk stratification and risk-guided post-TB follow-up. However, given the single-centre design, lack of external validation and relatively limited follow-up duration, the findings should be interpreted with caution. External validation in independent and geographically diverse cohorts is warranted before broader clinical implementation.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding authors, Fen Gao ([email protected]) or Qian Li ([email protected]), upon reasonable request.
Ethics Approval and Informed Consent
This prospective study was approved by the Institutional Ethics Committee of Hunan Chest Hospital (Approval No. LS2025112602). Written informed consent was obtained from all participants prior to enrollment. The study was conducted in accordance with the Declaration of Helsinki and applicable national regulations.
Funding
This study was supported by the Hunan Provincial Natural Science Foundation (Grant No. 2026JJ82347).
Disclosure
The authors report no conflicts of interest in this work. Xingming Ye and Shengbing Le should be regarded as co-first authors.
References
1. de Oca MM, Perez-Padilla R, Celli B, et al. The global burden of COPD: epidemiology and effect of prevention strategies. Lancet Respir Med. 2025;13(8):709–16. doi:10.1016/S2213-2600(24)00339-4
2. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
3. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the global burden of disease study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
4. Sehgal IS, Dhooria S, Muthu V, Salzer HJF, Agarwal R. Burden, clinical features, and outcomes of post-tuberculosis chronic obstructive lung diseases. Curr Opin Pulm Med. 2024;30(2):156–166. doi:10.1097/MCP.0000000000001026
5. Fan H, Wu F, Liu J, et al. Pulmonary tuberculosis as a risk factor for chronic obstructive pulmonary disease: a systematic review and meta-analysis. Ann Transl Med. 2021;9(5):390. doi:10.21037/atm-20-4576
6. Pontali E, Centis R. TB survivors: why curing TB is sometimes not enough. IJTLD Open. 2024;1(12):531–532. doi:10.5588/ijtldopen.24.0530
7. Ivanova O, Hoffmann VS, Lange C, Hoelscher M, Rachow A. Post-tuberculosis lung impairment: systematic review and meta-analysis of spirometry data from 14 621 people. Eur Respir Rev. 2023;32(168):220221. doi:10.1183/16000617.0221-2022
8. Ratnakumar S, Hayward SE, Denneny EK, et al. Post-pulmonary tuberculosis lung function: a systematic review and meta-analysis. Lancet Glob Health. 2025;13(6):e1020–e1029. doi:10.1016/S2214-109X(25)00105-6
9. Byrne A, Al-Hindawi Y, Plit M, et al. The prevalence and pattern of post tuberculosis lung disease including pulmonary hypertension from an Australian TB service; a single-centre, retrospective cohort study. BMC Pulm Med. 2025;25(1):84. doi:10.1186/s12890-025-03549-5
10. Silva DR, Mello FCQ, Migliori GB. Diagnosis and management of post-tuberculosis lung disease. J Bras Pneumol. 2023;49(2):e20230055. doi:10.36416/1806-3756/e20230055
11. Hussain A, Khurana AK, Goyal A, et al. Effect of pulmonary rehabilitation in patients with post-tuberculosis sequelae with functional limitation. Indian J Tuberc. 2024;71(2):123–129. doi:10.1016/j.ijtb.2023.04.012
12. Fumagalli G, Mencarini J, Sini I, et al. Post-tuberculosis lung disease: a guide for clinicians. Infection. 2025;54(1):15–24. doi:10.1007/s15010-025-02645-2
13. Meghji J, Auld SC, Bisson GP, et al. Post-tuberculosis lung disease: towards prevention, diagnosis, and care. Lancet Respir Med. 2025;13(5):460–472. doi:10.1016/S2213-2600(24)00429-6
14. Health N, China FPCotPsRo. Diagnosis for pulmonary tuberculosis (WS 288-2017). Electr J Emerg Infect Dis. 2018;3:59–61.
15. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. doi:10.1164/rccm.200703-456SO
16. Jamal A, Phillips E, Gentzke AS, et al. Current cigarette smoking among adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(2):53–59. doi:10.15585/mmwr.mm6702a1
17. Zhou T, Huang X, Ma J, et al. Association of plasma soluble CD14 level with asthma severity in adults: a case control study in China. Respir Res. 2019;20(1):19. doi:10.1186/s12931-019-0987-0
18. Song S, Lei L, Zhang R, et al. Circadian disruption and breast cancer risk: evidence from a case-control study in China. Cancers. 2023;15(2):419. doi:10.3390/cancers15020419
19. Blanc PD, Annesi-Maesano I, Balmes JR, et al. The occupational burden of nonmalignant respiratory diseases. an official American thoracic society and European respiratory society statement. Am J Respir Crit Care Med. 2019;199(11):1312–1334. doi:10.1164/rccm.201904-0717ST
20. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the European organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
21. Zhu M, Zha Y, Cui L, et al. Assessment of nutritional risk scores (the nutritional risk screening 2002 and modified nutrition risk in critically ill scores) as predictors of mortality in critically ill patients on extracorporeal membrane oxygenation. ASAIO J. 2024;70(6):510–516. doi:10.1097/MAT.0000000000002142
22. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
23. Van Calster B, McLernon DJ, van Smeden M, Wynants L, Steyerberg EW. Calibration: the Achilles heel of predictive analytics. BMC Med. 2019;17(1):230. doi:10.1186/s12916-019-1466-7
24. Park HJ, Byun MK, Kim HJ, et al. History of pulmonary tuberculosis affects the severity and clinical outcomes of COPD. Respirology. 2018;23(1):100–106. doi:10.1111/resp.13147
25. Wang Y, Li Z, Li F. Impact of previous pulmonary tuberculosis on chronic obstructive pulmonary disease: baseline results from a prospective cohort study. Comb Chem High Throughput Screen. 2023;26(1):93–102. doi:10.2174/1386207325666220406111435
26. Nishi MP, Mancuzo EV, Sulmonett N, Almeida IN, Cesar ALA, Miranda SS. Pulmonary functional assessment: longitudinal study after treatment of pulmonary tuberculosis. Rev Inst Med Trop Sao Paulo. 2021;63:e65. doi:10.1590/s1678-9946202163065
27. Salvagno GL, Henry BM, Pighi L, De Nitto S, Gianfilippi G, Lippi G. Three-month ad interim analysis of total anti-SARS-CoV-2 antibodies in healthy recipient of a single BNT162b2 vaccine booster. Clin Chem Lab Med. 2022;60(8):e181–e183. doi:10.1515/cclm-2022-0385
28. Chang W, Li Z, Liang Q, Zhao W, Li F. The incidence, risk factors, and predictive model of obstructive disease in post-tuberculosis patients. Int J Chron Obstruct Pulmon Dis. 2024;19:2457–2466. doi:10.2147/COPD.S489663
29. Cioboata R, Vlasceanu SG, Mitroi DM, et al. History of pulmonary tuberculosis accelerates early onset and severity of COPD: evidence from a multicenter study in Romania. J Clin Med. 2025;14(17):5980. doi:10.3390/jcm14175980
30. Wang J, Yu L, Yang Z, et al. Development of chronic obstructive pulmonary disease after a tuberculosis episode in a large, population-based cohort from Eastern China. Int J Epidemiol. 2025;54(2):dyae174. doi:10.1093/ije/dyae174
31. Guo C, Li Q, Wei L, Liu Y, Sun D, Ding C. Surgical treatment outcomes and risk factors for post-TB lung disease. IJTLD Open. 2024;1(11):516–521. doi:10.5588/ijtldopen.24.0322
32. Hulya S, Naz I, Karadeniz G, Erkan S. Clinical effects of TB sequelae in patients with COPD. Int J Tuberc Lung Dis. 2022;26(4):363–368. doi:10.5588/ijtld.21.0419
33. Joo DH, Kim MC, Sin S, et al. Incidence and risk factors of tuberculosis-associated chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2025;20:2091–2102. doi:10.2147/COPD.S523732
34. Allwood BW, Byrne A, Meghji J, Rachow A, van der Zalm MM, Schoch OD. Post-tuberculosis lung disease: clinical review of an under-recognised global challenge. Respiration. 2021;100(8):751–763. doi:10.1159/000512531
35. Akalu TY, Clements ACA, Liyew AM, Gilmour B, Murray MB, Alene KA. Risk factors associated with post-tuberculosis sequelae: a systematic review and meta-analysis. EClinicalMedicine. 2024;77:102898. doi:10.1016/j.eclinm.2024.102898
36. Le Y, Cao W, Zhou L, et al. Infection of mycobacterium tuberculosis promotes both M1/M2 polarization and MMP production in cigarette smoke-exposed macrophages. Front Immunol. 2020;11:1902. doi:10.3389/fimmu.2020.01902
37. Wang Y, Zhu J, Wang S, Zhou J. Disease burden and attributable risk factors for chronic obstructive pulmonary disease in China, Japan, and South Korea: trends for 1990 to 2021 period and predictions for 2031. Front Med Lausanne. 2025;12:1609322. doi:10.3389/fmed.2025.1609322
38. Liu Z, Jiao M, Lv J, Han Q. Increased incidence of chronic obstructive pulmonary disease in women due to long-term passive smoking. Int J Chron Obstruct Pulmon Dis. 2025;20:2745–2752. doi:10.2147/COPD.S534060
39. Hu S, Yu Q, Liu F, Gong F. A novel inflammatory indicator for tuberculosis-associated obstructive pulmonary disease (TOPD): the systemic inflammatory response index (SIRI). J Inflamm Res. 2024;17:4219–4228. doi:10.2147/JIR.S468232
40. Cioboata R, Balteanu MA, Mitroi DM, et al. Beyond smoking: emerging drivers of COPD and their clinical implications in low- and middle-income countries: a narrative review. J Clin Med. 2025;14(13):4633. doi:10.3390/jcm14134633
41. Song M, Zhang M, Han J, Fu W. Construction and validation of a nomogram to identify the risk of cavitation in pulmonary tuberculosis. Infect Drug Resist. 2024;17:2803–2813. doi:10.2147/IDR.S459330
42. Li X, Ye J, Wang S, et al. Factors associated with post-treatment resorption of lung cavities in individuals with first episodes of drug-sensitive cavitary pulmonary tuberculosis in China. BMC Infect Dis. 2025;25(1):899. doi:10.1186/s12879-025-11287-6
43. Kempker RR, Salindri AD, Avaliani T, et al. High rates of post-tuberculosis lung disease among persons successfully treated for drug-susceptible and resistant tuberculosis. Thorax. 2025;81(2):170–178.
44. Bongomin F. Post-tuberculosis chronic pulmonary aspergillosis: an emerging public health concern. PLoS Pathog. 2020;16(8):e1008742. doi:10.1371/journal.ppat.1008742
45. Neubock MJ, Gunther G, Barac A, et al. Chronic pulmonary aspergillosis as a considerable complication in post-tuberculosis lung disease. Semin Respir Crit Care Med. 2024;45(1):102–113. doi:10.1055/s-0043-1776913
46. Yan H, Guo L, Pang Y, Liu F, Liu T, Gao M. Clinical characteristics and predictive model of pulmonary tuberculosis patients with pulmonary fungal coinfection. BMC Pulm Med. 2023;23(1):56. doi:10.1186/s12890-023-02344-4
47. Santos AP, Rodrigues LS, Rother N, Mello FCQ, Magis-Escurra C. The role of neutrophil response in lung damage and post-tuberculosis lung disease: a translational narrative review. Front Immunol. 2025;16:1528074. doi:10.3389/fimmu.2025.1528074
48. Jumaar C, Malefane L, Jacobs S, et al. Delineating the significance of several inflammatory markers in a lung tuberculosis cohort during the active and post-tuberculosis stages of the disease: an observational study in Cape Town, South Africa (2019 to 2024). Infect Dis Rep. 2025;17(3):52. doi:10.3390/idr17030052
49. Malefane L, Maarman G. Post-tuberculosis lung disease and inflammatory role players: can we characterise the myriad inflammatory pathways involved to gain a better understanding? Chem Biol Interact. 2024;387:110817. doi:10.1016/j.cbi.2023.110817
50. Han Y, Wu Y, Li Y, et al. Prevalence and prognostic significance of systemic inflammation index and diet quality in patients with chronic obstructive pulmonary disease: evidence from the cohort study of NHANES 2007-2018. Int J Chron Obstruct Pulmon Dis. 2025;20:3093–3109. doi:10.2147/COPD.S536178
51. Mammadova A, Naurzvai N. Association of systemic immune-inflammation index and aggregate index of systemic inflammation with clinical status in stable and exacerbated COPD: a single-center retrospective study. Medicine. 2025;104(39):e44589. doi:10.1097/MD.0000000000044589
52. He X, Hou H, Jiang Y, Huang X. Association between indices of peripheral blood inflammation and cavitary pulmonary tuberculosis. Int J Gen Med. 2024;17:5133–5142. doi:10.2147/IJGM.S483185
53. Di Y, Yang F, Che C, Xu S, Qi Y. Correlation between serum inflammatory factor level changes and disease severity in patients with chronic obstructive pulmonary disease complicated by tuberculosis. Int J Gen Med. 2025;18:3547–3556. doi:10.2147/IJGM.S522251
54. Arghir IA, Arghir OC, Otelea MR, Andronache IT, Ion I. Adenosine deaminase and systemic immune inflammatory index-a biomarker duet signature of pulmonary tuberculosis severity. Medicina. 2025;61(6):1096. doi:10.3390/medicina61061096
55. Webber T, Macdonald C, Tameris M, et al. Immune, metabolic, anatomical, and functional features of people after successful tuberculosis treatment: an exploratory analysis. Sci Rep. 2025;15(1):18392. doi:10.1038/s41598-025-01656-1
56. Scriba TJ, Maseeme M, Young C, Taylor L, Leslie AJ. Immunopathology in human tuberculosis. Sci Immunol. 2024;9(102):eado5951. doi:10.1126/sciimmunol.ado5951
57. Zhang Y, Zhang Y, Ma N, Huang Z. Correlation between elderly patients with COPD and the impact on immunity in tuberculosis patients: a retrospective study. Medicine. 2024;103(42):e40140. doi:10.1097/MD.0000000000040140
58. An HR, Bai XJ, Liang JQ, et al. The relationship between absolute counts of lymphocyte subsets and clinical features in patients with pulmonary tuberculosis. Clin Respir J. 2022;16(5):369–379. doi:10.1111/crj.13490
59. Singh S, Allwood BW, Chiyaka TL, et al. Immunologic and imaging signatures in post tuberculosis lung disease. Tuberculosis. 2022;136:102244. doi:10.1016/j.tube.2022.102244
60. Bisson GP, Allwood B, Byrne A, et al. Post-tuberculosis lung disease: a case definition for use in research studies. Lancet Infect Dis;2025. S1473–3099(1425)00548–00541. doi:10.1016/S1473-3099(25)00548-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.