")
Back to Journals » Infection and Drug Resistance » Volume 16
Risk Factors and Mortality of Elderly Patients with Hospital-Acquired Pneumonia of Carbapenem-Resistant Klebsiella pneumoniae Infection
Authors Zhou C, Sun L , Li H, Huang L, Liu X
Received 18 July 2023
Accepted for publication 14 October 2023
Published 20 October 2023 Volume 2023:16 Pages 6767—6779
DOI https://doi.org/10.2147/IDR.S431085
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Chaoe Zhou,1 Liying Sun,2 Haixia Li,2 Lei Huang,2,* Xinmin Liu1,*
1Department of Geriatrics, Peking University First Hospital, Beijing, People’s Republic of China; 2Department of Clinical Laboratory, Peking University First Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinmin Liu, Department of Geriatrics, Peking University First Hospital, Beijing, 100034, People’s Republic of China, Tel +86-10-8357-2128, Email [email protected] Lei Huang, Department of Clinical Laboratory, Peking University First Hospital, Beijing, 100034, People’s Republic of China, Tel +86-10-8357-5546, Email [email protected]
Purpose: Hospital-acquired pneumonia (HAP) caused by carbapenem-resistant K. pneumoniae (CRKP), especially in elderly patients, results in high morbidity and mortality. Studies on risk factors, mortality, and antimicrobial susceptibility of CRKP pulmonary infection among elderly patients are lacking.
Patients and Methods: A retrospective case–control study was conducted from January 2019 to December 2021. The elderly inpatients (≥ 65 years) who were diagnosed with HAP caused by K. pneumoniae were enrolled. Clinical data were collected. Univariate and multivariate logistic regression analyses were used to identify risk factors. Propensity score matching was used to minimize the effect of potential confounding variables. Kaplan–Meier analysis was used to compare survival.
Results: A total of 115 patients with CRKP infection and 78 patients with carbapenem-susceptible K. pneumoniae (CSKP) infection were recruited. There were four independent risk factors for CRKP infection: history of intensive care unit (ICU) stays from hospital admission to positive respiratory specimen culture for K. pneumoniae (odds ratio (OR)=2.530), Charlson comorbidity index score ≥ 3 (OR = 2.420), prior exposure to carbapenems (OR = 5.280), and prior K. pneumoniae infection or colonization in the preceding 3 years (OR = 18.529). The all-cause 30-day mortality was 22.3%, the mortality of CRKP and CSKP infection was 28.7% and 12.8%, respectively. Independent risk factors for mortality included: older age (OR = 1.107), immunocompromised patients (OR = 8.632), severe pneumonia (OR = 51.244), quick Sepsis-related Organ Failure Assessment (qSOFA) score ≥ 2 (OR = 6.187), exposure to tigecycline before infection (OR = 24.702), and prolonged ICU stay (OR = 0.987). Thirty-day mortality was significantly lower in patients receiving ceftazidime-avibactam (CAZ-AVI) containing regimens than patients receiving polymyxin B sulfate (PB) containing regimens (P = 0.048). qSOFA score had a good prognostic effect [area under receiver operating characteristic curve (AUROC) of 0.838].
Conclusion: Active screening of CRKP for the high-risk populations, especially elderly patients, is significant for early detection and successful management of CRKP infection.
Keywords: elderly, hospital-acquired pneumonia, CRKP, CSKP, ceftazidime-avibactam, qSOFA
Introduction
Hospital-acquired pneumonia (HAP) is an infection of lung parenchyma caused by pathogens within the hospital environment. It is the second-most common nosocomial infection and the leading cause of death.1 The incidence of HAP varies from 5 to more than 20 cases per 1000 hospitalized patients.2 The incidence of HAP in Chinese is 1.74% to 6.4%.3,4 Elderly patients are more likely to develop severe pneumonia due to decreased immunity, vomiting reflex disorders, weakened fever response, and cardiopulmonary dysfunction.
The most common cause of HAP in the elderly is bacterial infection, particularly K. pneumoniae, a gram-negative capsulated bacterium that can cause severe pneumonia, especially in immunocompromised patients.5 Since carbapenems were first used to treat infections caused by K. pneumoniae, the emergence of CRKP has become a major concern worldwide.6 In 2017, the World Health Organization listed CRKP as one of the resistant pathogens in urgent need of new antimicrobial agents.7 The number of CRKP had increased significantly year by year. According to the China Antimicrobial Surveillance Network (CHINET, http://www.chinets.com/), the isolation rate of CRKP based on meropenem resistance increased significantly from 2.9% in 2005 to 27.5% in 2022.
The mortality rate of patients with CRKP pulmonary infection was high. A previous study showed that the 14-day mortality rate of patients with CRKP pulmonary infection was 23.2%, and the in-hospital mortality rate was 34.8% (73.9% of carbapenem-resistant Enterobacterales were CRKP).8 Risk factors associated with mortality of CRKP infection included older age, malignancy, high SOFA score, and inappropriate therapy.8–10 Additionally, several studies had demonstrated that CRKP infected patients had higher mortality and longer hospital stays than CSKP infected patients.11,12
However, it is worth noting that there are few studies researching the risk factors and mortality of elderly patients with CRKP infection. The objective of this study is to identify the risk factors and mortality associated with CRKP pulmonary infection in the elderly.
Materials and Methods
Study Design
This retrospective case–control study was conducted from 1 January 2019 to 31 December 2021 at Peking University First Hospital, a tertiary hospital with 1805 beds in Beijing, China. Elderly inpatients (≥65 years) with confirmed with K. pneumoniae HAP were recruited. K. pneumoniae HAP was defined as a new pulmonary infiltrate confirmed by X-ray or computed tomography (occurred ≥48 h after admission) associated with at least one of the following: new or worsening cough with or without sputum production, fever (temperature >37.8◦C) or hypothermia (<35.6◦C), leukocytosis, left shift, or leukopenia based on local normal values, as well as isolation of K. pneumoniae from lower respiratory tract secretions (sputum, bronchoalveolar lavage fluid, bronchoscopic needle aspiration, or blood).13 The exclusion criteria were: a) age <65 years; b) incomplete medical records; c) K. pneumoniae colonization (did not meet the criteria for infection);14 d) outpatients or emergency patients; e) infection acquired from outside of hospital setting. Only the first episode of K. pneumoniae HAP was included. A total of 193 episodes were enrolled in this study.
Data Collection
The patient data were collected from the hospital’s computerized microbiology laboratory database and information system. The main variables included demographic characteristics; underlying diseases; Charlson comorbidity index;15 past medical history (surgery, smoke, alcohol, exposure to antibiotics, and K. pneumoniae infection or colonization); sepsis/septic shock,16 Pitt bacteremia score,17 and quick Sepsis-related Organ Failure Assessment (qSOFA) score16 at infection onset; laboratory findings; co-infection with other pathogens; therapeutic processes (admission to ICU after infection, mechanical ventilation); antibiotics therapy; clinical outcomes (30-day mortality, failure rate of microbiological clearance, length of hospital stay, length of ICU stay). The events that occurred before CRKP infection were considered for analyzing risk factors. Thirty-day mortality was defined as death within 30 days from diagnosis of infection (including patients who died within 30 days, and patients who discharged within 30 days were confirmed dead by telephone follow-up). To further compare the clinical outcomes between CRKP and CSKP groups, propensity score matching was used to minimize the effect of potential confounding variables, including age, admission to ICU before infection, and Charlson comorbidity index.
Definition of Terms
Patient conditions to be considered immunocompromised were: a) primary immune deficiency diseases; b) active malignancy or malignancy within 1 year of community-acquired pneumonia, excluding patients with localized skin cancers or early-stage cancers; c) receiving cancer chemotherapy; d) human immunodeficiency virus infection with a CD4 T-lymphocyte count <200 cells/mL or percentage <14%; e) solid organ transplantation; f) hematopoietic stem cell transplantation; g) receiving corticosteroid therapy with a dose ≥20 mg prednisone or equivalent daily for ≥14 d or a cumulative dose >600 mg of prednisone; h) receiving biological immune modulators; i) receiving disease-modifying antirheumatic drugs or other immunosuppressive drugs (eg, cyclosporin, cyclophosphamide, hydroxychloroquine, methotrexate).18 Severe pneumonia was diagnosed if one or more major criteria (invasive mechanical ventilation or septic shock with the need for vasopressors) and/or three minor criteria [respiratory rate ≥30 breaths/min, PaO2/FiO2 ratio ≤250, multilobar infiltrates, confusion/disorientation, uremia (blood urea nitrogen level ≥20 mg/dL), leukopenia (white blood count <4000 cells/mm3), thrombocytopenia (platelet count <100,000 cells/mm3), hypothermia (core temperature <36°C), hypotension requiring aggressive fluid resuscitation] met.19 Failure rate of microbiological clearance was defined as the persistence of positive cultures (presence of pathogens initially isolated from the site of infection).20,21 The definition of co-infection was defined as detection 2 or more bacteria in the same sample. Longer hospitalization time was defined as the patient’s hospital stay more than 30 days after the first positive culture.
Empirical and targeted therapies were defined as antibiotics administered before and after obtaining the result of an antimicrobial susceptibility test. Appropriate therapy was defined as using at least one in vitro active agent, with or without inactive companion agents. Monotherapy was defined as only one active agent using, combination therapy was defined as more than one active agent using. Inappropriate therapy was defined as selection of agents without activity against responsible pathogens.22
Antimicrobial Susceptibility Test
K. pneumoniae was identified by Matrix-assisted laser desorption ionization time-of-flight mass spectrometry (Bruker Microflex LT, Bremen, Germany).23 Antibiotics susceptibility testing was completed using a Vitek 2 automated system (bio-Mérieux, France), which was performed by adopting the broth microdilution method. Gram-negative susceptibility (GNS) cards were used to determine the minimal inhibitory concentration (MIC) of strains for various antibiotics (8–64 ug/mL for amikacin, 2–32 ug/mL for aztreonam, 0.25–32 ug/mL for cefepime, 8–32 ug/mL for cefoperazone/sulbactam, 0.25–32 ug/mL for ceftazidime, 0.5–4 ug/mL for ciprofloxacin, 1–16 ug/mL for doxycycline, 1–12 ug/mL for imipenem, 0.25–8 ug/mL for levofloxacin, 0.5–12 ug/mL for meropenem, 2/4-48/8 ug/mL for piperacillin/tazobactam, 2–8 ug/mL for minocycline, 0.75–4 ug/mL for tigecycline, 8–64 ug/mL for tobramycin, 8/2-64/2 ug/mL for ticarcillin/clavulanate and 1/19-16-304 ug/mL for trimethoprim/sulfamethoxazole). Antibiotic susceptibility testing for colistin was performed using the test kit (BIO-KONT®), with the method of broth microdilution. Susceptibility testing results were interpreted according to the criteria recommended by the Clinical and Laboratory Standards Institute (CLSI M100 31th),24 except tigecycline, which was interpreted according to the American Food and Drug Administration (FDA) standard (https://www.fda.gov/drugs/development-resources/tigecycline-injection-products).
Statistical Analysis
SPSS version 26.0 and MatchIt package in R 3.5 were used for statistical analyses. For continuous variables, patient characteristics were presented as median and IQR (interquartile range), Student’s t-test was used to compare normally distributed variables, and Mann–Whitney U-test was used to compare non-normally distributed variables. For categorical variables, patient characteristics were presented with rate. Chi-square test or Fisher’s exact test was used to compare categorical variables. In the multivariate logistic regression model, variables with P <0.01 in the univariate analysis were analyzed. Variables whose P <0.05 and OR >1 was considered as independent risk factors. Additionally, OR and the 95% confidence interval (CI) were calculated for each variable.
Results
A total of 193 patients were included in this study, including 115 patients with CRKP infection, and 78 patients with CSKP infection (Figure 1). The mean age was 76.0 years old, and the age ranged from 65 to 99 years. 66.8% (129/193) of patients were male, 33.2% (64/193) of patients were female.
 |
Figure 1 Flowchart outlining of the patients included in this study. |
Results of K. pneumoniae Susceptibility Test
Detailed findings for susceptibilities of CRKP and CSKP are shown in Figure 2. In vitro antimicrobial susceptibility test showed that CRKP strains were significantly resistant to ciprofloxacin, piperacillin-tazobactam, aztreonam, ceftazidime, levofloxacin, cefoperazone, cefepime, minocycline, doxycycline, tobramycin, and amikacin, the resistance rate was 50%–100%. The proportion of CRKP resistant to tigecycline and colistin was 5.9% and 14.8%, respectively. CSKP strains were sensitive to most antibiotics.
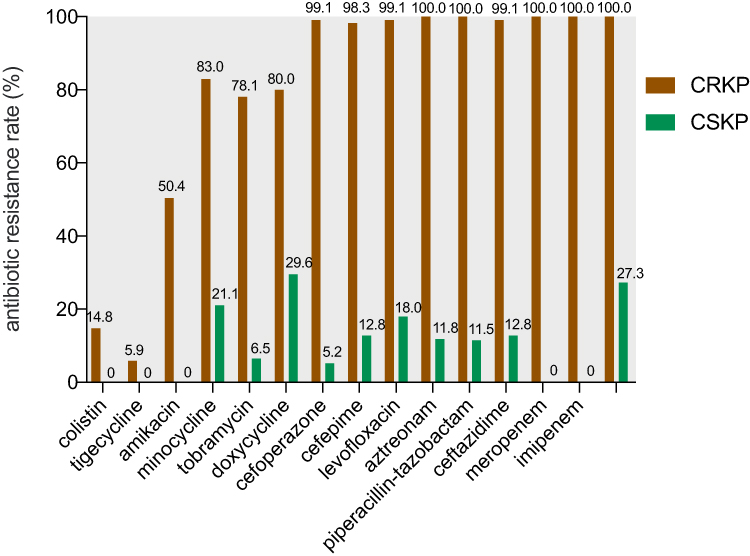 |
Figure 2 The results of antimicrobial susceptibility test of K. pneumoniae strains. |
The Risk Factors for CRKP Infection
The demographic and clinical characteristics of patients are summarized in Table 1. The majority of patients infected with CRKP (77/115, 67.0%) and CSKP (52/78, 66.7%) were male. Patients with CRKP infection (median age = 79.0 years) were older than patients with CSKP infection (median age = 73.0 years). Patients with history of ICU stays from hospital admission to positive respiratory specimen culture for K. pneumoniae, Charlson comorbidity index score ≥3, long hospital stay before infection, prior K. pneumoniae infection or colonization in the preceding 3 years, exposure to carbapenems or tigecycline within 3 months before a positive culture were more likely to be infected with CRKP.
 |
Table 1 Univariate Analysis of Risk Factors for CRKP Infection |
Multivariate logistic regression analysis showed that independent risk factors for CRKP infection were history of ICU stays from hospital admission to positive respiratory specimen culture for K. pneumoniae (OR = 2.530, 95% CI: 1.195–5.356; P=0.015), Charlson comorbidity index score ≥3 (OR = 2.420, 95% CI: 1.097–5.338; P=0.029), prior exposure to carbapenems (OR = 5.280, 95% CI: 2.330–11.966; P<0.001), and prior K. pneumoniae infection or colonization in the preceding 3 years (OR = 18.529, 95% CI: 3.801–90.336; P<0.001) (Table 2).
 |
Table 2 Multivariate Analysis of Risk Factors for CRKP Infection |
The Clinical Outcomes Between CRKP and CSKP Infected Patients
The all-cause 30-day mortality was 22.3% (43/193) in all patients, the 30-day mortality of CRKP infection was 28.7% (33/115), and the 30-day mortality of CSKP infection was 12.8% (10/78). The all cause in-hospital mortality was 41.5% (80/193) in all patients, the in-hospital mortality of CRKP infection was 53.9% (62/115), and the in-hospital mortality of CSKP infection was 23.1% (18/78). Patients with CRKP infection had higher mortality than patients with CSKP infection (P=0.009). Compared with patients with CSKP infection, patients with CRKP infection were more likely to have sepsis/septic shock (29/78 vs 8/73, P<0.001), severe pneumonia (31/78 vs 12/78 P=0.001), and long hospital stay (40/78 vs 20/78, P<0.001). In addition, CRKP strains were more difficult to clear up than CSKP strains (49/78 vs 16/78 P<0.001) (Figure 3).
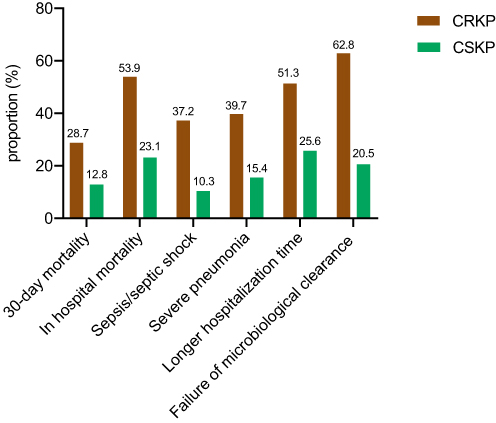 |
Figure 3 The clinical outcomes of patients with CRKP and CSKP infection. |
The Risk Factors for All-Cause 30-Day Mortality
In univariate analysis, the following factors were associated with 30-day mortality, including history of ICU stays from hospital admission to positive respiratory specimen culture for K. pneumoniae, immunocompromised patients, exposure to carbapenems or tigecycline within 3 months prior to a positive culture, Pitt bacteremia score ≥3, qSOFA ≥2, received mechanical ventilation treatment, sepsis/septic shock occurred, ICU admission after infection, severe pneumonia, CRKP infection, and prolonged ICU stay. Some laboratory variables, such as high procalcitonin, sensitivity C-reactive protein, D-dimer, neutrophils, and low lymphocytes, were also associated with mortality (Table 3).
 |
Table 3 Univariate Analysis of Risk Factors for 30-Day Mortality |
Multivariate logistic regression showed that older age (OR = 1.107; 95% CI: 1.016–1.206; P=0.020), immunocompromised status (OR = 8.632; 95% CI: 1.926–38.680; P=0.005), severe pneumonia (OR = 51.244; 95% CI, 10.181–257.918; P<0.001), qSOFA score ≥2 (OR = 6.187; 95% CI, 1.445–26.481; P=0.014), exposure to tigecycline before infection (OR = 24.702; 95% CI, 2.418–252.408; P=0.007), and prolonged ICU stay (OR = 0.987; 95% CI, 0.977–0.997; P=0.013) were independent risk factors for 30-day mortality (Table 4). Kaplan–Meier analyses also confirmed that 30-day mortality was higher in patients with CRKP infection than patients with CSKP infection (Figure 4A). The patients with severe pneumonia had higher 30-day mortality than patients without severe pneumonia (P<0.001) (Figure 4B). The 30-day mortality of elderly patients with severe pneumonia was 62.9%. In addition, immunocompromised patients had higher 30-day mortality than immunocompetent patients (P<0.001) (Figure 4C). The 30-day mortality of patients with immunocompromised pneumonia was 42.3%.
 |
Table 4 Multivariate Analysis of Risk Factors for 30-Day Mortality |
 |
Figure 4 Kaplan–Meier analysis was used to compare the 30-day survival rate for (A) CRKP vs CSKP infection; (B) severe pneumonia vs non-severe pneumonia; (C) immunocompromised vs immunocompetent patients, and (D) patients receiving CAZ-AVI containing regimes vs polymyxin B sulfate (PB) containing regimes. The data were analyzed using SPSS 26 to obtain p-values (SPSS 26_analyze_survival_Kaplan-Meier_log-rank_p value), and the drawing was made using Prism 8 app. |
Antimicrobial Therapy
Among 193 patients included, 122 patients received appropriate targeted therapy. Among those received appropriate targeted therapy, 102 patients received monotherapy, 20 patients received combination therapy. Tigecycline and carbapenems were the most commonly used monotherapy options for patients with CRKP and CSKP infection, respectively. In combination therapy, amikacin combined with tigecycline, and PB combined with tigecycline were common treatment options (Supplemental Table 1). In particular, 30-day mortality was significantly lower in patients received CAZ-AVI containing regimens than in patients received PB containing regimens (25.0% vs 64.3%, P=0.048) (Figure 4D).
Relationship Between qSOFA Score and the Prognosis of Patients
The distribution of qSOFA score and its relationship with 30-day mortality are shown in Figure 5. When qSOFA score was 0 point, the 30-day mortality rate of patients was 3.0% (2/65), qSOFA score was 1 point, the 30-day mortality of patients was 8.0% (4/50), qSOFA score ≥2, the 30-day mortality of patients was 47.4% (37/78). Among the died, 86.0% of patients had a qSOFA ≥2, the AUROC was 0.838.
 |
Figure 5 Distribution and mortality of patients by qSOFA score. (A) Distribution of qSOFA score (0–3) and its association with 30-day mortality (the x axis indicated the specific value of the qSOFA score when the patient developed K. pneumoniae infection) (B) the area under receiver operating characteristic curve (AUROC) predicted the prognosis of patients using qSOFA score. The (A) was made using Prism 8 app., the (B) was made using SPSS 26 analysis (SPSS 26_analyze_category_ROC curve). |
Discussion
HAP caused by CRKP infection was commonly reported to be associated with higher mortality,25 but data regarding risk factors and clinical outcomes for CRKP pulmonary infection in the older patients was still limited. Therefore, this purpose of this study was to systematically review HAP caused by CRKP infection, especially the risk factors of morbidity and mortality and clinical outcomes, so as to provide clinical value for the treatment and control of CRKP infection.
Early identification of people at high-risk of CRKP infection is important. Previous studies demonstrated that prior central venous catheter use, sputum suction, continuous renal replacement therapy, exposure to fluoroquinolones,26 hypertension, exposure to carbapenems, ICU stay,27 hematologic malignancies, ICU acquired infection,28 β-lactam/β-lactamase inhibitor combinations exposure, solid organ transplantation,29 liver cirrhosis, and length of hospital stay over the previous 14 days30 were independent risk factors for the morbidity of CRKP infection. In this study, we found that history of ICU stays from hospital admission to positive respiratory specimen culture for K. pneumoniae, Charlson comorbidity index score ≥3, prior exposure to carbapenems, and prior K. pneumoniae infection or colonization in the preceding 3 years were independent risk factors for CRKP infection.
ICU patients were more likely to undergo invasive procedures, which may hinder airway clearance, increase the risk of CRKP colonization. In addition, such invasive measures exposed ICU patients to pathogens carried by roommates or presented in the hospital environment. Therefore, the use of invasive devices should be minimized for the elderly. In humans, K. pneumoniae often colonizes at various mucosal surfaces, including the upper respiratory tract and the gut. In hospitalized patients, colonization rates in the nasopharynx rise to 19%, while it can be as high as 77% in the gastrointestinal tract.31,32 Gastrointestinal colonization serves as a major reservoir for transmission and infection to other sites. Previous study found that 16% of the patients colonized with K. pneumoniae were found to be infected, compared to only 3% in the non-carriers, whole-genome sequencing revealed that the patients were infected with the same strain they carried in the form of colonization.33 This indicated that K. pneumoniae colonization in high-risk units (such as intensive care, transplant surgery, hematology oncology wards) at admission should be actively monitored and continuously monitored during subsequent hospitalization.
Comparing with CSKP infected patients, CRKP infected patients had higher mortality. Regarding risk factors for mortality, different populations, regions and types of infection could contribute to different results. Previous studies showed that treatment failure for infection,26 CRKP infection and isolation in ICU,27 severe sepsis or septic shock incidents, inadequate empirical antimicrobial therapy, corticosteroids use,28 CRKP bloodstream infections, mechanical ventilation >96 hours, and platelet counts <100×109/L29 were independent risk factors for mortality of CRKP infection. In this study, we found that the independent risk factors for mortality included older age, immunocompromised status, severe pneumonia, qSOFA score ≥2, empirical use of tigecycline, and prolonged ICU stay.
It has been demonstrated that age ≥65 years was an independent risk factor for hospital mortality of patients with pneumonia.34 The incidence of pneumonia increased rapidly with age and peaked between 60 and 79 years of age.35 Immunocompromised patients were prone to acquire pneumonia with high mortality. Different from the general immunocompetent population, the etiologies of lung infection in immunocompromised patients were more diverse, and the possibility of co-infection should be considered. Due to the failure to implement early and rapid diagnosis, many patients were initially treated with inappropriate antibiotics, which may cause several serious comorbidities such as respiratory failure and infectious shock, further increasing mortality.36 In this study, empirical use of tigecycline before infection was associated with death. This is probably because the standard dose of tigecycline (50 mg of tigecycline every 12 h after a 100-mg loading dose) was absolutely insufficient to eradicate strains with tigecycline MIC >0.5 mg/L.37 In this study, the tigecycline MIC >0.5 mg/L in 71.3% of the strains. With suboptimal pharmacokinetics properties in certain sites of infection increased potential for toxicity. High doses of tigecycline (received 100 mg of tigecycline every 12 h after a 200-mg loading dose) and combination therapy can be considered for HAP caused by multidrug-resistant bacterial infections, but caution is needed for its side effects, such as gastrointestinal.38
In addition, treatment options against CRKP infections are very limited. Clinicians are compelled to use last-resort antimicrobials, like CAZ-AVI and PB. In this study, we found that the 30-day mortality was significantly lower in patients received CAV-AZI containing regimens than patients received PB containing regimens, providing encouraging results. More recently, several new agents with activity against carbapenem-resistant pathogens have been approved for clinical use or are reaching late-stage clinical development, they include β-lactam-β-lactamase inhibitor combinations (ceftolozane-tazobactam, meropenem-vaborbactam, imipenem-cilastatin-relebactam), plazomicin, eravacycline, and cefiderocol. Clinicians appear to generally favor newer agent over previous best available therapy.39
The knowledge of the exact mechanism of CRKP was crucial for the selection of the most appropriate antimicrobial.39,40 For example, ceftazidime/avibactam was not active against strains producing class B metallo-β-lactamases (MBLs), the combination of aztreonam-ceftazidime/avibactam had a treating effect against 86% of MBLs producing members of Enterobacteriaceae family.41 In addition, the antibiotic resistance and virulence factors could co-exist in CRKP isolates.42 Antibiotic resistance and virulence genes can be transmitted horizontally through plasmids, which lead to the accelerated spread of multidrug resistance among different populations of pathogens.43 Understanding the direct relationship between the frequency of the genes involved in the development of virulence and resistance, which could provide a highly effective model for physicians to prescribe suitable antibiotics.44 Determining genetic diversity for the identification of dominant species and complete knowledge of biofilm formation were necessary to stop the spread of infections in hospitals and to control and manage associated infections.45 The information on genetic resistance profile is not reported in this article, we have collected all strains, and will further study the genetic resistance profile of strains in the future.
qSOFA has been proposed as a screening and prognostic tool in patients with suspected infection, sepsis, or septic shock, it can be used to predict the prognosis of patients.16 In this study, we found that qSOFA score ≥2 could predict the mortality of patients with HAP infected with K. pneumoniae. Previous study had shown that the accuracy of qSOFA score in predicting in-hospital mortality of elderly hospitalized patients with suspected infection was low (AUROC = 0.680).46 One plausible reason for this difference may be that this study only focused on older patients with HAP who were infected with K. pneumoniae. The accuracy of qSOFA score in predicting the prognosis of patients with HAP needs to be further verified by more studies in the future.
The present work has several limitations: first, the number of cases were relatively small; second, this study mainly focused on HAP caused by K. pneumoniae, and lacked analysis of K. pneumoniae infections in other sites; third, due to the limited data available in retrospective studies, some predictors may be missing from the data analysis.
Conclusion
In summary, history of ICU stays from hospital admission to positive respiratory specimen culture for K. pneumoniae, Charlson comorbidity index score ≥3, prior exposure to carbapenems, and prior K. pneumoniae infection or colonization in the preceding 3 years were associated with the development of CRKP pulmonary infection. We also found a high mortality caused by K. pneumoniae pulmonary infection in elderly patients with older age, immunocompromised status, severe pneumonia, qSOFA ≥2, exposure to tigecycline, and prolonged ICU stays. Ceftazidime-avibactam-based regimes were associated with better outcomes. Active screening of CRKP for high-risk groups, especially for elderly patients, is conducive to the early identification, treatment and control of CRKP infections, so as to achieve the successful management.
Data Sharing Statement
The data for this study may be available by contacting the corresponding author (Lei Huang) upon reasonable request.
Ethics Approval and Consent to Participate
The Ethics Committee of Peking University First Hospital, Beijing, China, provided ethical approval for this research (2022-yan-498). As it was an observational study, informed consent was waived.
Acknowledgments
We thank Home for Researchers editorial team for language editing service.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key R&D Program of China Research on the Precision Diagnosis, Treatment, and Integrated Prevention, Control for the elderly with common infectious disease (2020YFC2005401), Youth Clinical Research Project of Peking University First Hospital (2018CR27), National High Level Hospital Clinical Research Funding (Interdepartmental Research Project of Peking University First Hospital) (2023IR46).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J. 2017:50. doi:10.1183/13993003.00582-2017
2. American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416. doi:10.1164/rccm.200405-644ST
3. Tao XB, Qian LH, Li Y, et al. Hospital-acquired infection rate in a tertiary care teaching hospital in China: a cross-sectional survey involving 2434 inpatients. Int J Infect Dis. 2014;27:7–9. doi:10.1016/j.ijid.2014.05.011
4. Zhu J, Zhang X, Shi G, Yi K, Tan X, Chamberlain AM. Atrial fibrillation is an independent risk factor for hospital-acquired pneumonia. PLoS One. 2015;10(7):e0131782. doi:10.1371/journal.pone.0131782
5. Russo TA, Marr CM. Hypervirulent Klebsiella pneumoniae. Clin Microbiol Rev. 2019;32. doi:10.1128/cmr.00001-19
6. Pitout JD, Laupland KB. Extended-spectrum beta-lactamase-producing Enterobacteriaceae: an emerging public-health concern. Lancet Infect Dis. 2008;8(3):159–166. doi:10.1016/s1473-3099(08)70041-0
7. Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318–327. doi:10.1016/s1473-3099(17)30753-3
8. Chen IR, Huang PH, Wu PF, Wang FD, Lin YT. Clinical characteristics and outcomes of 56 patients with pneumonia caused by carbapenem-resistant Klebsiella pneumoniae. J Glob Antimicrob Resist. 2021;25:326–330. doi:10.1016/j.jgar.2021.03.028
9. Chen IR, Lin SN, Wu XN, Chou SH, Wang FD, Lin YT. Clinical and microbiological characteristics of bacteremic pneumonia caused by Klebsiella pneumoniae. Front Cell Infect Microbiol. 2022;12:903682. doi:10.3389/fcimb.2022.903682
10. Wang Z, Qin RR, Huang L, Sun LY. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection and mortality of Klebsiella pneumoniae infection. Chin Med J. 2018;131(1):56–62. doi:10.4103/0366-6999.221267
11. Schwaber MJ, Klarfeld-Lidji S, Navon-Venezia S, Schwartz D, Leavitt A, Carmeli Y. Predictors of carbapenem-resistant Klebsiella pneumoniae acquisition among hospitalized adults and effect of acquisition on mortality. Antimicrob Agents Chemother. 2008;52(3):1028–1033. doi:10.1128/aac.01020-07
12. Debby BD, Ganor O, Yasmin M, et al. Epidemiology of carbapenem resistant Klebsiella pneumoniae colonization in an intensive care unit. Eur J Clin Microbiol Infect Dis. 2012;31(8):1811–1817. doi:10.1007/s10096-011-1506-5
13. Qin X, Wu S, Hao M, et al. The colonization of carbapenem-resistant Klebsiella pneumoniae: epidemiology, resistance mechanisms, and risk factors in patients admitted to intensive care units in China. J Infect Dis. 2020;221(Supplement_2):S206–S214. doi:10.1093/infdis/jiz622
14. van Duin D, Perez F, Rudin SD, et al. Surveillance of carbapenem-resistant Klebsiella pneumoniae: tracking molecular epidemiology and outcomes through a regional network. Antimicrob Agents Chemother. 2014;58(7):4035–4041. doi:10.1128/aac.02636-14
15. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
16. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
17. Henderson H, Luterbach CL, Cober E, et al. The Pitt bacteremia score predicts mortality in nonbacteremic infections. Clin Infect Dis. 2020;70(9):1826–1833. doi:10.1093/cid/ciz528
18. Ramirez JA, Musher DM, Evans SE, et al. Treatment of community-acquired pneumonia in immunocompromised adults: a consensus statement regarding initial strategies. Chest. 2020;158(5):1896–1911. doi:10.1016/j.chest.2020.05.598
19. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–S72. doi:10.1086/511159
20. Tumbarello M, Trecarichi EM, Corona A, et al. Efficacy of ceftazidime-avibactam salvage therapy in patients with infections caused by Klebsiella pneumoniae Carbapenemase–producing K. pneumoniae. Clin Infect Dis. 2019;68(3):355–364. doi:10.1093/cid/ciy492
21. Fang J, Li H, Zhang M, et al. Efficacy of ceftazidime-avibactam versus polymyxin B and risk factors affecting clinical outcomes in patients with carbapenem-resistant Klebsiella pneumoniae infections a retrospective study. Front Pharmacol. 2021;12:780940. doi:10.3389/fphar.2021.780940
22. Lu J, Zhang A, Han L, et al. Clinical outcomes and risk factors for death following carbapenem-resistant Klebsiella pneumoniae infection in solid organ transplant recipients. Microbiol Spectr. 2023;11(1):e0475522. doi:10.1128/spectrum.04755-22
23. Croxatto A, Prod’hom G, Greub G. Applications of MALDI-TOF mass spectrometry in clinical diagnostic microbiology. FEMS Microbiol Rev. 2012;36(2):380–407. doi:10.1111/j.1574-6976.2011.00298.x
24. Clinical and Laboratory Standards Institute W, PA. Performance Standards for Antimicrobial Susceptibility Testing, M100.
25. Pang F, Jia XQ, Zhao QG, Zhang Y. Factors associated to prevalence and treatment of carbapenem-resistant Enterobacteriaceae infections: a seven years retrospective study in three tertiary care hospitals. Ann Clin Microbiol Antimicrob. 2018;17(1):13. doi:10.1186/s12941-018-0267-8
26. Zuo Y, Zhao D, Song G, Li J, Xu Y, Wang Z. Risk factors, molecular epidemiology, and outcomes of carbapenem-resistant Klebsiella pneumoniae infection for hospital-acquired pneumonia: a matched case-control study in eastern china during 2015–2017. Microb Drug Resist. 2021;27(2):204–211. doi:10.1089/mdr.2020.0162
27. Chen Y, Chen Y, Liu P, et al. Risk factors and mortality for elderly patients with bloodstream infection of carbapenem resistance Klebsiella pneumoniae: a 10-year longitudinal study. BMC Geriatr. 2022;22(1):573. doi:10.1186/s12877-022-03275-1
28. Chen J, Ma H, Huang X, et al. Risk factors and mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection in a tertiary-care hospital in China: an eight-year retrospective study. Antimicrob Resist Infect Control. 2022;11(1):161. doi:10.1186/s13756-022-01204-w
29. Cao Z, Yue C, Kong Q, Liu Y, Li J. Risk factors for a hospital-acquired carbapenem-resistant Klebsiella pneumoniae bloodstream infection: a five-year retrospective study. Infect Drug Resist. 2022;15:641–654. doi:10.2147/idr.S342103
30. Hsu JY, Chuang YC, Wang JT, Chen YC, Hsieh SM. Healthcare-associated carbapenem-resistant Klebsiella pneumoniae bloodstream infections: risk factors, mortality, and antimicrobial susceptibility, 2017–2019. J Formos Med Assoc. 2021;120(11):1994–2002. doi:10.1016/j.jfma.2021.04.014
31. Pollack M, Charache P, Nieman RE, Jett MP, Reimhardt JA, Hardy PH. Factors influencing colonisation and antibiotic-resistance patterns of gram-negative bacteria in hospital patients. Lancet. 1972;2(7779):668–671. doi:10.1016/s0140-6736(72)92084-3
32. Podschun R, Ullmann U. Klebsiella spp. as nosocomial pathogens: epidemiology, taxonomy, typing methods, and pathogenicity factors. Clin Microbiol Rev. 1998;11(4):589–603. doi:10.1128/cmr.11.4.589
33. Gorrie CL, Mirceta M, Wick RR, et al. Gastrointestinal carriage is a major reservoir of Klebsiella pneumoniae infection in intensive care patients. Clin Infect Dis. 2017;65(2):208–215. doi:10.1093/cid/cix270
34. Yin Y, Zhao C, Li H, et al. Clinical and microbiological characteristics of adults with hospital-acquired pneumonia: a 10-year prospective observational study in China. Eur J Clin Microbiol Infect Dis. 2021;40(4):683–690. doi:10.1007/s10096-020-04046-9
35. Santella B, Serretiello E, De Filippis A, et al. Lower respiratory tract pathogens and their antimicrobial susceptibility pattern: a 5-year study. Antibiotics. 2021;10(7):851. doi:10.3390/antibiotics10070851
36. Cheng WL, Hsueh PR, Lee CC, et al. Bacteremic pneumonia caused by extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae: appropriateness of empirical treatment matters. J Microbiol Immunol Infect. 2016;49(2):208–215. doi:10.1016/j.jmii.2014.05.003
37. Nicasio AM, Crandon JL, Nicolau DP. In vivo pharmacodynamic profile of tigecycline against phenotypically diverse Escherichia coli and Klebsiella pneumoniae isolates. Antimicrob Agents Chemother. 2009;53(7):2756–2761. doi:10.1128/aac.01678-08
38. Xu L, Wang YL, Du S, Chen L, Long LH, Wu Y. Efficacy and safety of tigecycline for patients with hospital-acquired pneumonia. Chemotherapy. 2016;61(6):323–330. doi:10.1159/000445425
39. Karampatakis T, Tsergouli K, Behzadi P. Carbapenem-resistant Klebsiella pneumoniae: virulence factors, molecular epidemiology and latest updates in treatment options. Antibiotics. 2023;12(2):234. doi:10.3390/antibiotics12020234
40. Ahmadi Z, Noormohammadi Z, Behzadi P, Ranjbar R. Molecular detection of gyrA mutation in clinical strains of Klebsiella pneumoniae. Iran J Public Health. 2022;51(10):2334–2339. doi:10.18502/ijph.v51i10.10992
41. Behzadi P, García-Perdomo HA, Karpiński TM, Issakhanian L. Metallo-ß-lactamases: a review. Mol Biol Rep. 2020;47(8):6281–6294. doi:10.1007/s11033-020-05651-9
42. Fasciana T, Gentile B, Aquilina M, et al. Co-existence of virulence factors and antibiotic resistance in new Klebsiella pneumoniae clones emerging in south of Italy. BMC Infect Dis. 2019;19(1):928. doi:10.1186/s12879-019-4565-3
43. Algammal A, Hetta HF, Mabrok M, Behzadi P. Editorial: emerging multidrug-resistant bacterial pathogens “superbugs”: a rising public health threat. Front Microbiol. 2023;14:1135614. doi:10.3389/fmicb.2023.1135614
44. Ahmadi M, Ranjbar R, Behzadi P, Mohammadian T. Virulence factors, antibiotic resistance patterns, and molecular types of clinical isolates of Klebsiella Pneumoniae. Expert Rev Anti Infect Ther. 2022;20(3):463–472. doi:10.1080/14787210.2022.1990040
45. Fasciana T, Ciammaruconi A, Gentile B, et al. Draft genome sequence and biofilm production of a carbapenemase-producing Klebsiella pneumoniae (KpR405) sequence type 405 strain isolated in Italy. Antibiotics. 2021;10(5):560. doi:10.3390/antibiotics10050560
46. Falsetti L, Martino M, Zaccone V, et al. SOFA and qSOFA usefulness for in-hospital death prediction of elderly patients admitted for suspected infection in internal medicine. Infection. 2020;48(6):879–887. doi:10.1007/s15010-020-01494-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.