Back to Journals » Infection and Drug Resistance » Volume 16
Risk Factors and Disease Profile Associated with the Nucleic Acid Conversion Time of COVID-19 Patients Infected with the SARS-CoV-2 Omicron Variant in Fangcang Shelter Hospitals
Authors Ma S ![]() , Wang H
, Wang H ![]() , Zhu K
, Zhu K ![]() , Chen H, Xie J, Huang Y
, Chen H, Xie J, Huang Y
Received 10 March 2023
Accepted for publication 15 June 2023
Published 20 June 2023 Volume 2023:16 Pages 3945—3954
DOI https://doi.org/10.2147/IDR.S410086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Shaolei Ma,* Haofei Wang,* Kongbo Zhu, Hui Chen, Jianfeng Xie, Yingzi Huang
Jiangsu Provincial Key Laboratory of Critical Care Medicine, Department of Critical Care Medicine, Zhongda Hospital, Nanjing, 210009, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yingzi Huang, Jiangsu Provincial Key Laboratory of Critical Care Medicine, Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, 210009, People’s Republic of China, Tel +86-025-83262553, Email [email protected]
Purpose: This study aimed to determine the clinical profile connected to the nucleic acid conversion time of COVID-19 patients harboring the SARS-CoV-2 Omicron variant at the hospitals at the Fangcang shelter.
Methods: We reported 39,584 COVID-19 patients who were hospitalized in Shanghai, China, between April 5 and May 5, 2022, and who had contracted the Omicron strain of SARS-CoV-2. Demographic data, medical and vaccination history, clinical symptoms, and NCT were reported for the patient.
Results: The median age of the patients with COVID-19 included in this study was 45 (interquartile range [IQR]: 33– 54), and 64.2% of them were male. The two most prevalent comorbidities among the patients were hypertension and diabetes. Additionally, we discovered that the percentage of unimmunized patients was negligible (13.2%). We found that male sex, age under 60, and other comorbidities including hypertension and diabetes are significant risk factors for extending NCT when we analyzed the risk variables for NCT. We discovered that vaccination with two or more doses can significantly reduce NCT. The analysis of the young (18– 59 years) and older (60 years) populations produced the same outcomes.
Conclusion: Our findings confirm that a full COVID-19 vaccine series or booster doses are highly recommended to significantly reduce NCT. In order to reduce NCT, it is also advised that elderly people who have no clear contraindications take vaccination shots.
Keywords: COVID-19, nucleic acid conversion time, Fangcang shelter hospitals, vaccination
Introduction
The global coronavirus disease 2019 (COVID-19) pandemic has been ongoing for three years.1 Since then, the B.1.1.529 (Omicron) variation has emerged as COVID-19’s main infectious agent and has been linked to epidemics across the globe.2 Due to these factors, there are growing worries regarding whether the Omicron variety will have more severe immune evasion and pathogenic effects than the prior strains. People are starting to worry about whether immunization can prevent illness aggravation and reduce nucleic acid conversation time (NCT) due to the high mutation rate and infectiousness of the Omicron strain.3,4 The airborne transmission should be recognized as an important mode of transmission of the SARS-CoV-2,5 precautions such as hand washing and social distancing are appropriate but insufficient, and we still need to explore the risk factors and other possible protective measures that affect patients with COVID-19.
Fangcang shelter hospitals are the main platform for centralized management of COVID-19 patients, especially asymptomatic and mild patients, first decided to establish by the Chinese government.6 Most of these individuals recover on their own and do not require any additional medical assistance. It is essential to control them centrally to stop them from spreading and to safeguard individuals who are vulnerable to severe acute respiratory system coronavirus 2 (SARS-COV-2) infection, such as those with underlying diseases. Severe COVID-19 patients are swiftly moved to the designated hospital for active treatment when they are discovered in the neighborhood or within Fangcang shelter hospitals. However, the operation of Fangcang shelter hospitals requires a lot of medical staff, and the operation speed for COVID-19 patients is several hundred times that of ordinary hospitals.7 Determining whether a patient who can have a shorter NCT in the early evaluation stage could be discharged from the Fangcang shelter hospital is of great significance for effectively diverting patients and improving the operation efficiency of the Fangcang shelter hospital.8
Several studies have analyzed and compared the clinical characteristics of patients infected with the wild-type or delta/Omicron variant of SARS-CoV-2.9–11 After the COVID-19 pandemic, global cooperation highlighted scientific and technological progress, leading to the rapid development of a series of effective vaccines.12 However, the difference in vaccine efficacy in the real world is very significant, and many countries have different results on vaccine efficacy. In addition, different host factors also affect the efficacy of vaccines. It has been reported that vaccines are less effective in the elderly and patients with underlying health conditions (such as chronic respiratory diseases, cardiovascular diseases, immunodeficiency, obesity, etc.).13 In this study, we investigated the demographic information and baseline characteristics of confirmed COVID-19 patients infected with the Omicron variant during the recent coronavirus flare-up in the city of Shanghai, China, in April and May 2022. We sought to identify the risk factors of NCT in COVID-19 patients infected with the SARS-CoV-2 Omicron variant.
Materials and Methods
Study Design and Participants
This retrospective study included 39,854 COVID-19 patients who were admitted to the LinGang Fangcang shelter hospital in Shanghai, China, from April 5 to May 5, 2022. COVID-19 infections were confirmed as reported.
The exclusion criteria were as follows: patients younger than 18 years of age, patients with incomplete clinical data, and patients transferred to the hospital for other reasons, such as confirmed critically ill patients with COVID-19. All patient information remained anonymous, this study was authorized by the Ethics Commission for Clinical Research of Zhongda Hospital, affiliated with Southeast University (2022ZDSYLL190-P01). Informed consent was waived due to the nature of the study as a retrospective study. The study was conducted by the principles described in the Declaration of Helsinki and the confidentiality of patients was guaranteed.
Procedure
COVID-19 patients infected with SARS-CoV-2 omicron variants were hospitalized, as previously reported. Baseline data were obtained from electronic medical records, including sex, age, medical history, underlying diseases, vaccines, and other baseline conditions. The date of the first positive nucleic acid test in the community and the date when the nucleic acid test was negative were also collected. NCT was defined as the time between a patient’s first positive viral nucleic acid test in the community and the first negative test in a Fangcang shelter hospital, with two consecutive negative viral nucleic acid tests.
Statistical Analysis
Data were summarized as median and interquartile range (IQR) values for continuous variables and frequencies for categorical variables. For comparisons between the two groups, the Mann–Whitney U-test was used for continuous variables. Categorical variables were examined using the chi-squared test. Univariate regression analysis was used to identify the risk factors for NCT, and multivariate regression analysis was performed for meaningful variables. All calculated p-values were two-sided, and p-values < 0.05 were considered statistically significant. All statistical analyses were performed using SPSS 25.0 and GraphPad Prism 7.0.
Results
In our study, from April 5, 2022, to May 5, 2022, a total of 44,964 COVID-19 patients were admitted to Shanghai Lingang Fangcang, of which 1670 patients were younger than 18 years of age; 3599 patients had incomplete epidemiological information, vaccination status, or medical record information; 111 patients were transferred for other reasons; a total of 39,584 patients were finally included in this study (Figure 1).
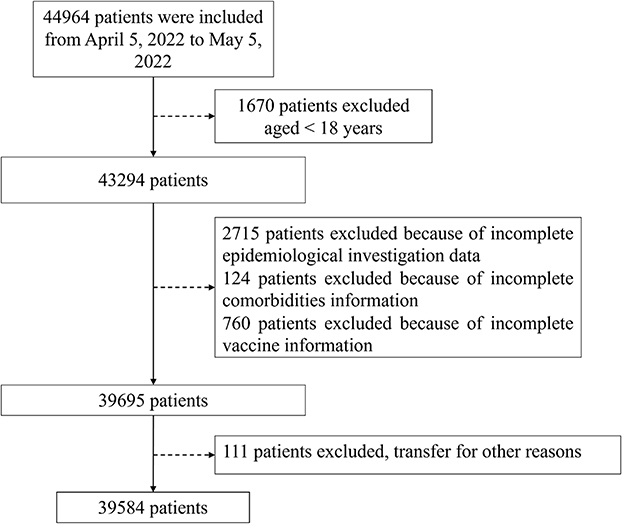 |
Figure 1 Flow diagram for total COVID-19 patients included in the study. |
Baseline Characteristics of COVID-19 Patients Infected by the Omicron Variant of SARS-CoV-2
In this study, from April to May 2022, 39,584 patients infected with the SARS-CoV-2 Omicron were hospitalized at the Lingang Fangcang shelter hospital in Shanghai, China. Here, we defined NCT≤10 days as the nucleic acid detection turning negative in the short term, and NCT>10 days as nucleic acid detection not turning negative in the long term. Their mean age was 45.0 years (IQR:33.0–54), 64.2% were male, and the most common comorbidity was hypertension, followed by diabetes. Among them, 13.2% were unvaccinated, 3.9% were vaccinated with one injection, 32.7% were vaccinated with two injections, and 50.2% were vaccinated with three injections (Table 1).
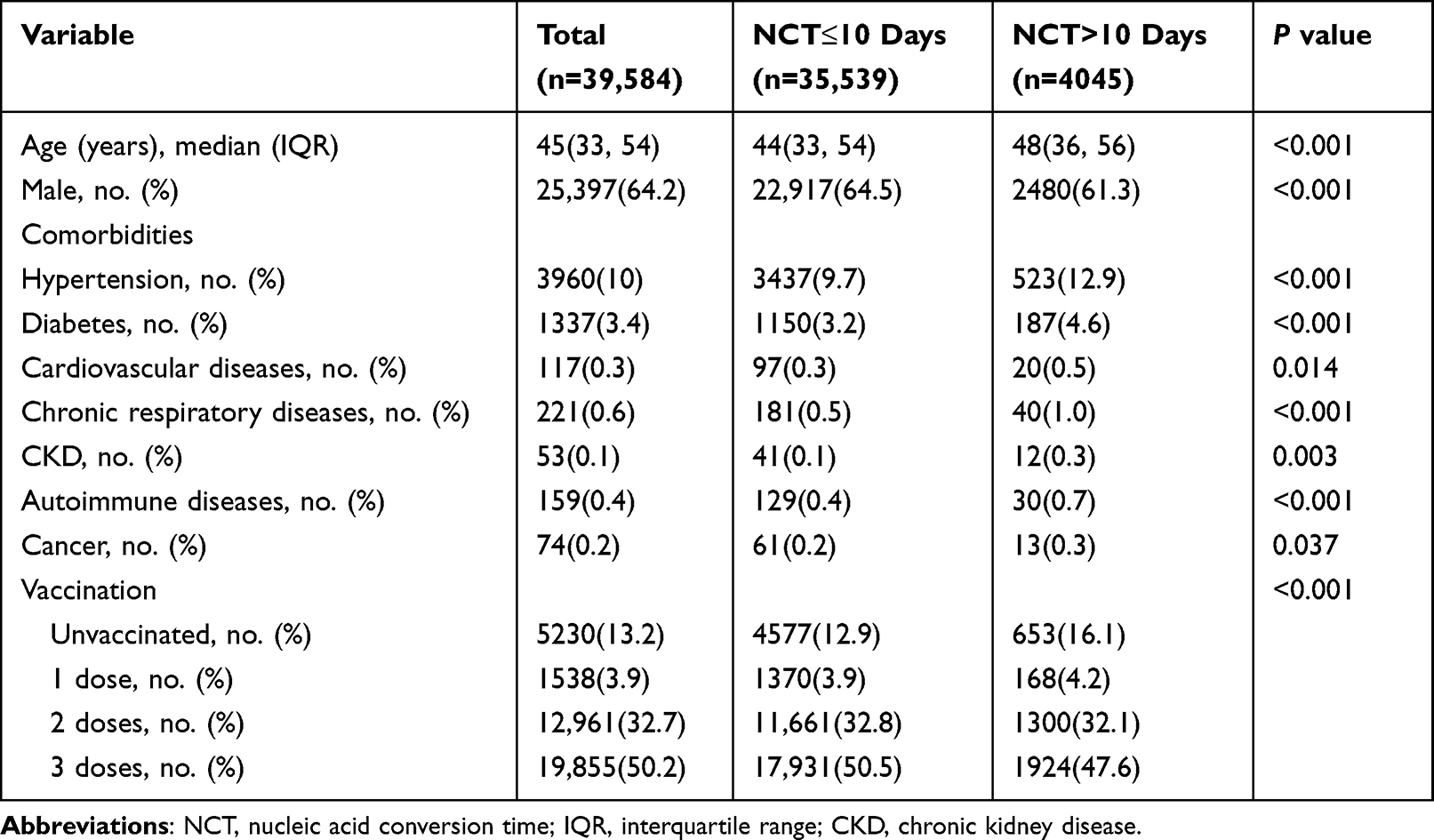 |
Table 1 Clinical Characteristics of the Patients with COVID-19 |
We divided patients into an ordinary group (age <60 years) and an advanced age group (age ≥60 years) according to the age of patients and reported the clinical characteristics of patients with NCT >10 and NCT≤10 days. We found that both age and male sex were risk factors for prolonged NCT, and among the underlying comorbidities, NCT was longer in patients with hypertension, diabetes, cardiovascular disease, or chronic kidney disease (CKD). More importantly, we found that the NCT of vaccinated patients was significantly shorter than that of the unvaccinated patients (Table 2).
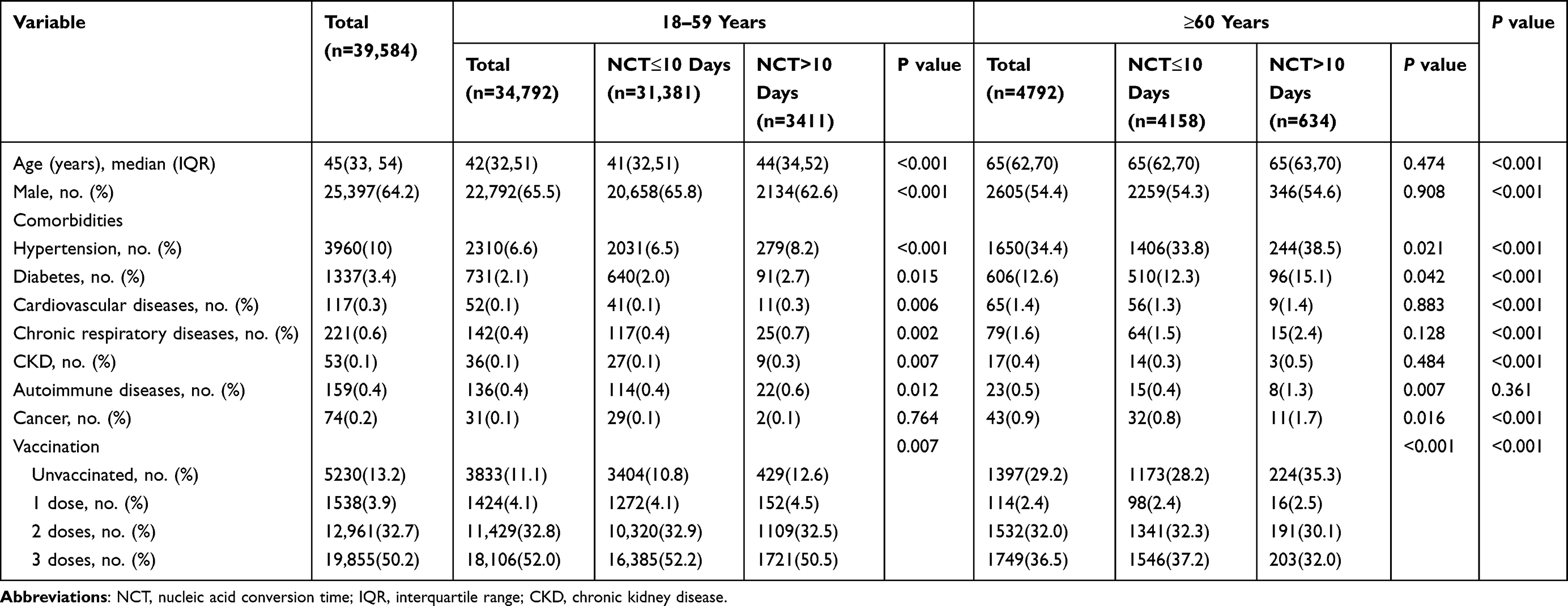 |
Table 2 Clinical Characteristics of the Patients with COVID-19 with Different Ages |
To further clarify whether the vaccine is effective in shortening the NCT, we analyzed different vaccination situations as subgroups. The clinical characteristics of unvaccinated and vaccinated patients with different dosage forms are shown in (Table 3).
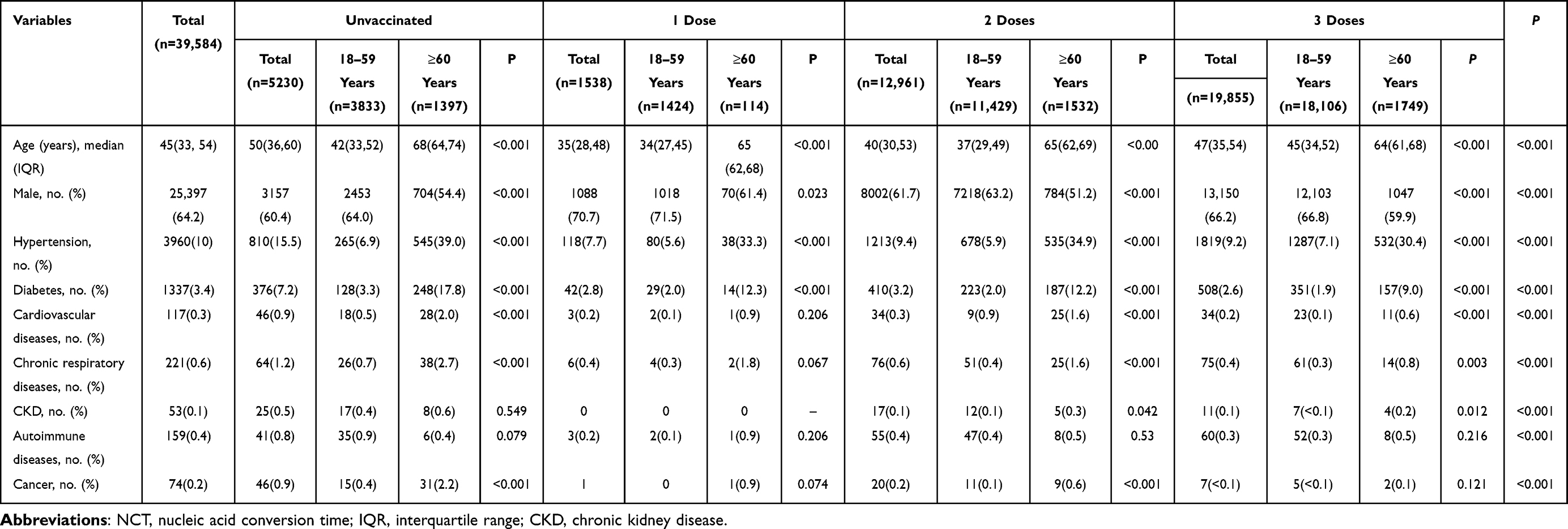 |
Table 3 Clinical Characteristics of the Patients with COVID-19 with Different Vaccination |
We attempted to analyze all risk factors and disease profiles that affect COVID-19 patients with NCT ≤ 10 days (Figure 2). First, we performed univariate regression analysis on the factors affecting the NCT ≤ 10 days and found that male sex, age ≥ 60 years, hypertension, diabetes, respiratory disease, cardiovascular disease, CKD, autoimmune diseases, cancer, and vaccination all significantly affected the NCT of COVID-19 patients (Figure 2A). Next, these above variables were added to the multiple regression analysis and notably, we found that male sex and 2 and 3-dose vaccinations were all favorable factors for NCT≤10 days. Conversely, age ≥60 years, hypertension, diabetes, respiratory disease, CKD, and autoimmune disease were risk factors for NCT≤10 days (Figure 2B).
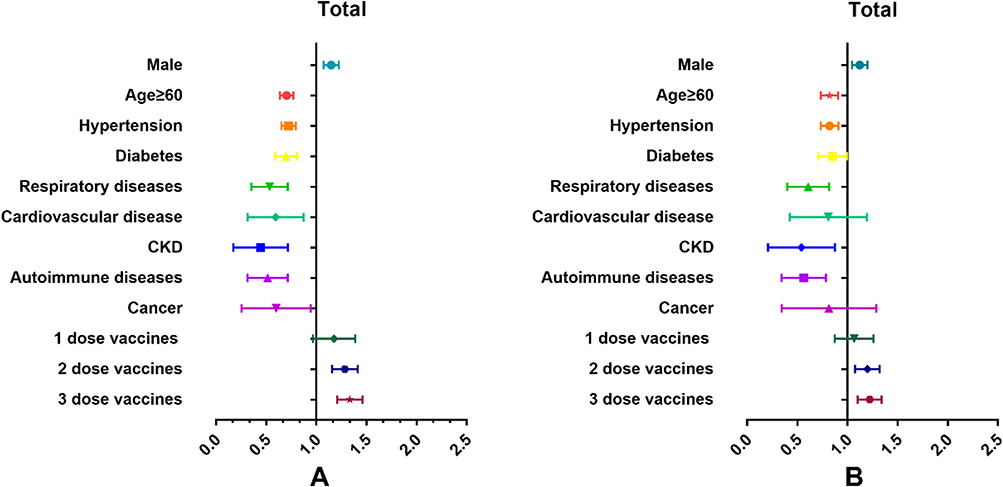 |
Figure 2 The risk factors and disease profiles that affect COVID-19 patients with NCT ≤ 10 days. (A) univariate regression analysis on the factors affecting the NCT ≤ 10 days in all patients. (B) multiple regression analysis on the factors affecting the NCT ≤ 10 days in all patients. Abbreviations: CKD, chronic kidney disease; NCT, nucleic acid conversion time. |
Many reports have focused on the factors affecting the age of COVID-19 patients, and there has been controversy over whether older patients should be vaccinated. In this study, according to whether the patients were older than 60 years, they were divided into two subgroups: elderly and non-elderly. We performed the same univariate and multivariate regression analysis on the risk factors and disease profiles of these two groups of patients (Figure 3). We found that autoimmune diseases, cancer, 2-dose and 3-dose vaccination were important factors for NCT in the elderly group (Figure 3A), and multivariate regression analysis also showed that 2-dose or 3-dose vaccination was an important favorable factor (Figure 3B). In the non-elderly group (ages 18–59), univariate regression analysis showed that hypertension, diabetes, respiratory, cardiovascular, and cerebrovascular disease, CKD, autoimmune diseases, 2-dose and 3-dose vaccination were all important factors for NCT (Figure 3C), and multivariate regression analysis showed that male sex, 2-dose or 3-dose vaccination was an important favorable factor (Figure 3D).
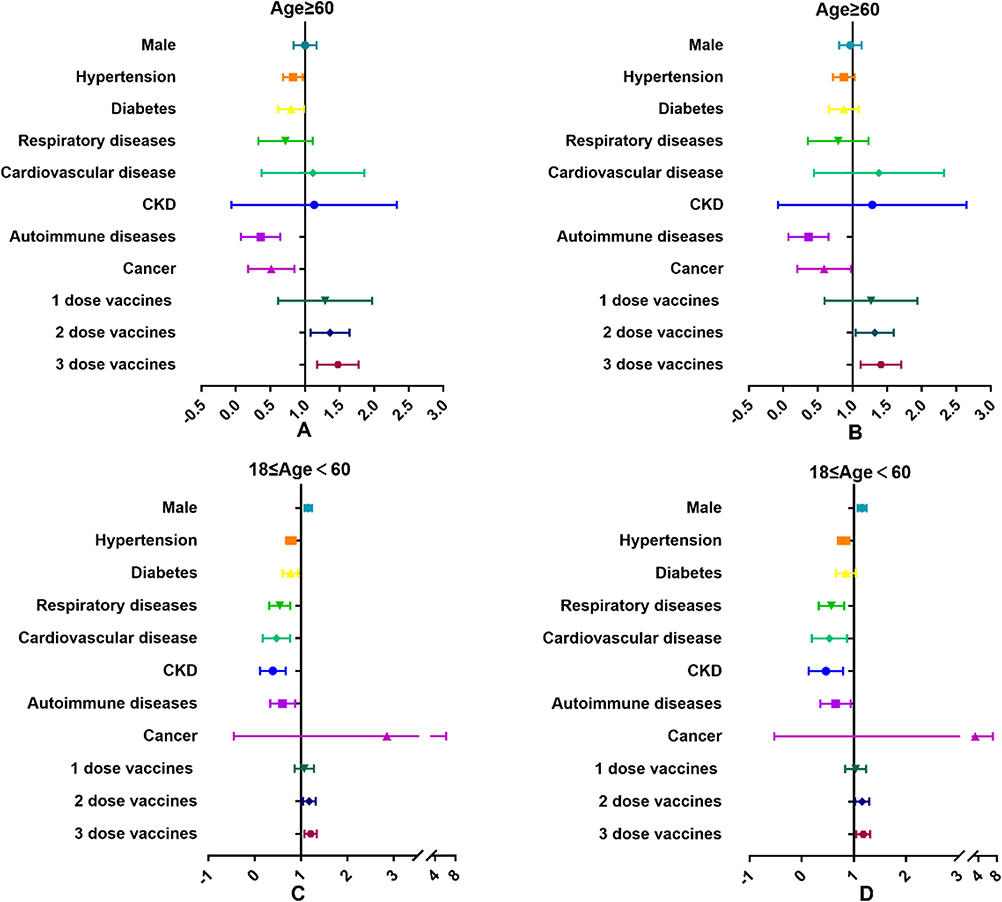 |
Figure 3 The risk factors and disease profiles that affect elderly and non-elderly COVID-19 patients with NCT ≤ 10 days. (A) univariate regression analysis on the factors affecting the NCT ≤ 10 days in elderly patients. (B) multiple regression analysis on the factors affecting the NCT ≤ 10 days in elderly patients. (C) univariate regression analysis on the factors affecting the NCT ≤ 10 days in non-elderly patients. (D) multiple regression analysis on the factors affecting the NCT ≤ 10 days in non-elderly patients. Abbreviations: CKD, chronic kidney disease; NCT, nucleic acid conversion time. |
We found that two or more doses of the vaccine may be effective in shortening NCT in all COVID-19 patients. We divided all COVID-19 patients into those who were unvaccinated and who received one dose (groups 0 and 1) and those who received more than two doses (groups 2 and 3) and found that the incidence of NCT was significantly higher in groups 2 and 3 than in groups 0 and 1 in the incidence of NCT ≤10 days (Figure 4).
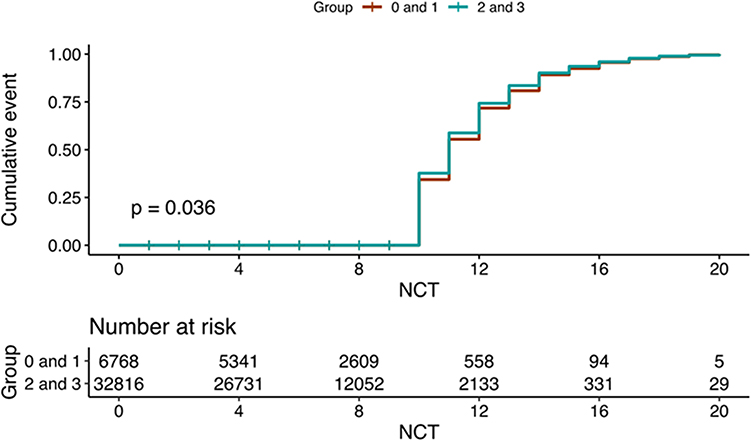 |
Figure 4 NCT≤10 days in COVID-19 patients with different vaccination doses. Abbreviation: NCT, nucleic acid conversion time. |
Discussion
This study retrospectively analyzed the demographic, epidemiological, and other medical information of a cohort of inpatients with COVID-19 in the Shanghai Lingang Fangcang shelter hospital. The objective was to study the risk factors of NCT in asymptomatic or mild COVID-19 patients admitted to Fangcang. We have made a simple definition of NCT, and according to our clinical research and experience, NCT ≤ 10 days is regarded as detection as nucleic acid-negative in a short time.
To the best of our knowledge, this is the first study of NCT-related factors in COVID-19 patients in Fangcang shelter hospitals. We found that age, sex, and underlying diseases were important risk factors for NCT. This finding is consistent with reports from multiple studies.14–18 In different age groups, there were obvious favorable factors for 2-dose and 3-dose vaccination, which was reflected in the effective shortening of NCT.
Fangcang shelter hospitals have now become the main locations for the centralized management of COVID-19 patients.19 It has characteristics that are different from those of general hospitals, including fast patient turnover, incomplete patient data, and insufficient inspection and testing equipment. NCT is an important criterion for transfer into and out of Fangcang shelter hospitals, and early identification of the risk factors affecting NCT is of great value to clarify which patients may require long-term hospitalization. It is worth mentioning that some studies have shown that patients with prolonged NCT have a high risk of developing severe disease.20,21
When the vaccine for the SARS-COV-2 virus was just developed and put into use, it was reported that elderly patients should be vaccinated against SARS-COV-2 with caution.22–24 However, as the technology continues to mature, the safety of the vaccine has improved significantly since the early days of COVID-19. In our study, age was an important factor affecting NCT, particularly in the elderly population. However, vaccination in elderly patients is also effective in shortening the NCT, while clear vaccine safety issues have not been reported. This gives us confidence in recommending a similar COVID-19 vaccine to older adults. Vaccination alone was an effective intervention for shortening NCT in our multivariate analysis. On the one hand, vaccination conferred the same protective effect on the elderly as on adults, which provides evidence for our continued advocacy for vaccination. On the other hand, for unvaccinated patients, prolonged hospitalization and isolation may be sensible. These findings have important implications for decision-making regarding quarantine protocols and for promoting optimal antiviral interventions.
This study had several limitations. First, compared with other studies,25 our sample size was sufficiently large, but the variables were relatively small. This is because of the particularity of Fangcang shelter hospitals, and we could not obtain all test results and symptoms in a timely and accurate manner. We could only use the most intuitive and simple factors that were analyzed. Second, our definition of NCT is based on other studies, although there is currently insufficient evidence to suggest that other definitions may be more accurate, which may still cause data bias. Finally, we demonstrated the effectiveness of vaccination in elderly patients but did not show the results in patients younger than 18 years of age in this study. We expect more comprehensive studies to clarify NCT-related studies in children and young adults.
Conclusions
This study establishes that older age and underlying medical conditions are associated with delayed NCT in hospitalized patients with COVID-19, and we demonstrate that vaccines, both in adults and the elderly, are an important way to effectively shorten NCT. We hope that these risk factors can provide clues for the early identification of patients with prolonged NCT and provide a direction for the development of optimal isolation protocols and treatment strategies.
Abbreviations
COVID-19, coronavirus disease 2019; NCT, nucleic acid conversation time; SARS-COV-2, severe acute respiratory system coronavirus 2; IQR, Interquartile range; CKD, chronic kidney disease.
Data Sharing Statement
Data are available on request.
Ethics Approval and Consent to Participate
This study was authorized by the Ethics Commission for Clinical Research of Zhongda Hospital, affiliated with Southeast University (2022ZDSYLL190-P01). Informed consent was waived due to the nature of the study as a retrospective study. The study was conducted by the principles described in the Declaration of Helsinki and confidentiality of patients was guaranteed.
Acknowledgments
We thank Southeast University and Zhongda Hospital for their financial support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The present study is supported by the National Natural Science Foundation of China (81971812), Jiangsu Province Key Research and Development Program (Social Development) Special Project (BE2021734), and Science Foundation of the Commission of Health of Jiangsu Province (ZDB2020009).
Disclosure
The authors declare that they have no competing interests.
References
1. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020;91(1):157–160. doi:10.23750/abm.v91i1.9397
2. Del Rio C, Omer SB, Malani PN. Winter of omicron-the evolving COVID-19 pandemic. JAMA. 2022;327(4):319–320. doi:10.1001/jama.2021.24315
3. Dandan T, Yanhong S, Huihong X, et al. The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 Omicron variant. J Med Virol. 2022;94:2376–2383. doi:10.1002/jmv.27643
4. Annika R, Lydia R, David B, et al. SARS-CoV-2 omicron variant neutralization in serum from vaccinated and convalescent persons. N Engl J Med. 2022;386:698–700. doi:10.1056/NEJMc2119236
5. Choudhary Om Prakash P, Indraj S, Singh I, et al. Aerosol transmission of SARS-CoV-2: the unresolved paradox. Travel Med Infect Dis. 2020;37:101869. doi:10.1016/j.tmaid.2020.101869
6. Simiao C, Zongjiu Z, Juntao Y, et al. Fangcang shelter hospitals: a novel concept for responding to public health emergencies. Lancet. 2020;395:1305–1314. doi:10.1016/S0140-6736(20)30744-3
7. Shang L, Xu J, Cao B. Fangcang shelter hospitals in COVID-19 pandemic: the practice and its significance. Clin Microbiol Infect. 2020;26:976–978. doi:10.1016/j.cmi.2020.04.038
8. Saeed K, Ali G, Gholamreza M, et al. Post-hospital discharge strategy for COVID-19 treatment and control: focus on Fangcang hospitals. Disaster Med Public Health Prep. 2022;16:1795–1797. doi:10.1017/dmp.2021.83
9. Jianguo Z, Nan C, Daguo Z, et al. Clinical characteristics of COVID-19 patients infected by the omicron variant of SARS-CoV-2. Front Med. 2022;9:912367. doi:10.3389/fmed.2022.912367
10. Michela A, Penfold Rose S, Jordi M, et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID symptom study app: a prospective, community-based, nested, case-control study. Lancet Infect Dis. 2022;22:43–55. doi:10.1016/S1473-3099(21)00460-6
11. Jingwen A, Haocheng Z, Yi Z, et al. Omicron variant showed lower neutralizing sensitivity than other SARS-CoV-2 variants to immune sera elicited by vaccines after boost. Emerg Microbes Infect. 2022;11:337–343. doi:10.1080/22221751.2021.2022440
12. Choudhary OP. Vaccine efficacy against COVID-19: a foresight on the host-associated factors. J Formos Med Assoc. 2021;120:1405–1407. doi:10.1016/j.jfma.2020.11.021
13. Om Prakash C, Singh I. Making sound public health policy decisions for COVID-19 vaccination: vaccine effectiveness, safety, affordability, programmatic logistics and roll-out globally. J Travel Med. 2021;taab031. doi:10.1093/jtm/taab031
14. Xuefeng M, Shousheng L, Lizhen C, et al. The clinical characteristics of pediatric inpatients with SARS-CoV-2 infection: a meta-analysis and systematic review. J Med Virol. 2021;93:234–240. doi:10.1002/jmv.26208
15. Hongye W, Dongshan Y, Ya L, et al. Clinical and antibody characteristics reveal diverse signatures of severe and non-severe SARS-CoV-2 patients. Infect Dis Poverty. 2022;11:15. doi:10.1186/s40249-022-00940-w
16. Youjiang L, Danping J, Wangyu C, et al. Clinical characteristics, cause analysis and infectivity of COVID-19 nucleic acid repositive patients: a literature review. J Med Virol. 2021;93:1288–1295. doi:10.1002/jmv.26491
17. Abdulrahman A, Waleed A, Fahad F, et al. Clinical characteristics and predictors of 28-day mortality in 352 critically ill patients with COVID-19: a retrospective study. J Epidemiol Glob Health. 2021;11:98–104. doi:10.2991/jegh.k.200928.001
18. Bo Y, Gaoke F, Dedong C, et al. Epidemiological and clinical characteristics of 214 families with COVID-19 in Wuhan China. Int J Infect Dis. 2021;105:113–119. doi:10.1016/j.ijid.2021.02.021
19. Bin H, Wei C, Tingyu Y, et al. Study on the localization of fangcang shelter hospitals during pandemic outbreaks. Front Public Health. 2022;10:876558. doi:10.1016/j.ijid.2021.02.021
20. Xin Z, Liangkun X, Junyao Z, et al. The value of early positive nucleic acid test and negative conversion time of SARS-CoV-2 RNA in the clinical outcome of COVID-19 patients. Front Med. 2022;9:826900. doi:10.3389/fmed.2022.826900
21. Pingzheng M, Liping D, Xiaoping L, et al. Risk factors for delayed negative conversion of SARS-CoV-2 in patients with COVID-19 pneumonia: a retrospective cohort study. Epidemiol Infect. 2020;148:e293. doi:10.1017/S0950268820002940
22. Kuldeep D, Shailesh Kumar P, Senthilkumar N, et al. COVID-19 in the elderly people and advances in vaccination approaches. Hum Vaccin Immunother. 2020;16:2938–2943. doi:10.1080/21645515.2020.1842683
23. Julia H-C, Martina P, Mei Xue W, et al. Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and SARS-CoV-2 positive testing: self-controlled case series study. BMJ. 2021;374:n1931. doi:10.1136/bmj.n1931
24. Soiza Roy L, Chiara S, Thomson Emma C. Efficacy and safety of COVID-19 vaccines in older people. Age Ageing. 2021;50:279–283. doi:10.1093/ageing/afaa274
25. Xiaowen H, Yuhan X, Jing J, et al. Factors associated with negative conversion of viral RNA in patients hospitalized with COVID-19. Sci Total Environ. 2020;728:138812. doi:10.1016/j.scitotenv.2020.138812
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Why Does COVID-19 Vaccine Acceptance Rate Remain Low Among Patients with Chronic Diseases? Evidences from Public Hospitals of Ethiopia
Daba C, Asefa L, Lemma H, Atamo A, Kebede E, Gebrehiwot M
Patient Preference and Adherence 2022, 16:1371-1380
Published Date: 27 May 2022
Effects of Obstructive Sleep Apnea on SARS-CoV-2 Antibody Response After Vaccination Against COVID-19 in Older Adults
Tufik S, Andersen ML, Rosa DS, Tufik SB, Pires GN
Nature and Science of Sleep 2022, 14:1203-1211
Published Date: 28 June 2022
Determinant Factors of COVID-19 Vaccine Hesitancy Among Adult and Elderly Population in Central Java, Indonesia
Utami A, Margawati A, Pramono D, Nugraheni A, Pramudo SG
Patient Preference and Adherence 2022, 16:1559-1570
Published Date: 28 June 2022
New Onset of Severe Plaque Psoriasis Following COVID-19 Vaccination: A Case Report
Hu YQ, Zhang JZ, Zhao Y
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1485-1487
Published Date: 2 August 2022
Risk of Severe COVID-19 in Non-Adherent OSA Patients
Genzor S, Prasko J, Mizera J, Jakubec P, Sova M, Vanek J, Šurinová N, Langova K
Patient Preference and Adherence 2022, 16:3069-3079
Published Date: 9 November 2022