Back to Journals » Infection and Drug Resistance » Volume 17
Risk Factors Analysis and Prediction Model Establishment for Carbapenem-Resistant Enterobacteriaceae Colonization: A Retrospective Cohort Study
Authors Guo X, Wu D, Chen X, Lin J, Chen J ![]() , Wang L, Shi S, Yang H, Liu Z
, Wang L, Shi S, Yang H, Liu Z ![]() , Hong D
, Hong D
Received 21 August 2024
Accepted for publication 18 October 2024
Published 28 October 2024 Volume 2024:17 Pages 4717—4726
DOI https://doi.org/10.2147/IDR.S485915
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiaolan Guo,1 Dansen Wu,1 Xiaoping Chen,2 Jing Lin,1 Jialong Chen,1 Liming Wang,1 Songjing Shi,1 Huobao Yang,1 Ziyi Liu,3 Donghuang Hong1,4
1Department of Critical Care Medicine, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou University Affiliated Provincial Hospital, Fuzhou, Fujian, People’s Republic of China; 2Computer Science and Mathematics, Fujian University of Technology, Fuzhou, Fujian, People’s Republic of China; 3Department of Urology, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 4Fujian Provincial Key Laboratory of Critical Care Medicine, Fuzhou, Fujian, People’s Republic of China
Correspondence: Ziyi Liu, Department of Urology, Renji Hospital, Shanghai Jiao Tong University School of Medicine, No. 160, Pujian Road, Pudong District, Shanghai, 200127, People’s Republic of China, Email [email protected] Donghuang Hong, Department of Critical Care Medicine, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou University Affiliated Provincial Hospital, No. 134, Dongjie Street, Gulou District, Fuzhou, Fujian, 350001, People’s Republic of China, Email [email protected]
Purpose: The objective of this study was to identify the risk factors associated with Carbapenem-resistant Enterobacteriaceae (CRE) colonization in intensive care unit (ICU) patients and to develop a predictive risk model for CRE colonization.
Patients and Methods: In this study, 121 ICU patients from Fujian Provincial Hospital were enrolled between January 2021 and July 2022. Based on bacterial culture results from rectal and throat swabs, patients were categorized into two groups: CRE-colonized (n = 18) and non-CRE-colonized (n = 103). To address class imbalance, Synthetic Minority Over-sampling Technique (SMOTE) was applied. Statistical analyses including T-tests, Chi-square tests, and Mann–Whitney U-tests were employed to compare differences between the groups. Feature selection was performed using Lasso regression and Random Forest algorithms. A Logistic regression model was then developed to predict CRE colonization risk, and the results were presented in a nomogram.
Results: After applying SMOTE, the dataset included 198 CRE-colonized patients and 180 non-CRE-colonized patients, ensuring balanced groups. The two groups were comparable in most clinical characteristics except for diabetes, previous emergency department admission, and abdominal infection. Eight independent risk factors for CRE colonization were identified through Random Forest, Lasso regression, and Logistic regression, including Acute Physiology and Chronic Health Evaluation (APACHE) II score > 16, length of hospital stay > 31 days, female gender, previous carbapenem antibiotic exposure, skin infection, multi-site infection, immunosuppressant exposure, and tracheal intubation. The risk prediction model for CRE colonization demonstrated high accuracy (87.83%), recall rate (89.9%), precision (85.6%), and an AUC value of 0.877. Patients were categorized into low-risk (0– 90 points), medium-risk (91– 160 points), and high-risk (161– 381 points) groups, with corresponding CRE colonization rates of 1.82%, 7.14%, and 58.33%, respectively.
Conclusion: This study identified independent risk factors for CRE colonization and developed a predictive model for assessing the risk of CRE colonization.
Keywords: carbapenem-resistant Enterobacteriaceae, intensive care unit, colonization, risk factors, risk prediction model
Introduction
The escalation of bacterial drug resistance has emerged as a significant worldwide public health concern, characterized by the proliferation of multidrug-resistant and pandrug-resistant bacteria.1 Following the initial identification of carbapenem-resistant Enterobacteriaceae (CRE) in 1995, the rapid dissemination of CRE on a global scale has positioned it as a prominent drug-resistant pathogen.2,3 In China, the situation with CRE is equally alarming, evidenced by escalating rates of infection and drug resistance annually.4 According to the China Antimicrobial Surveillance Network (CARSS), the detection rate of carbapenem-resistant Klebsiella pneumoniae (CR-KPN) has significantly risen from 6.4% to 10% between 2014 and 2019.5 CRE infections pose a significant economic burden on health care systems and threaten hospitalized patients.6,7
Patients in the intensive care unit (ICU) are particularly susceptible to CRE infections, and factors contributing to the greater susceptibility to infections include combination antibiotic treatment, duration of mechanical ventilation ≥7 days, and invasive catheterization.8,9 Furthermore, studies found that CRE infection is associated with a higher mortality rate in ICU patients.10
CRE colonization is a known risk factor for subsequent CRE infections.11,12 The rate of CRE infections following colonization varies between 19% and 89%, with a post-infection mortality rate ranging from 30% to 75%.12,13 However, few medical institutions actively monitor the colonization of CRE in high-risk patients due to high testing costs, delayed culture results, and lack of personnel.14–16 In this context, developing a tool for assessing the risk of CRE colonization becomes urgent. By identifying patients at a high risk of CRE colonization and initiating early infection prevention and control measures, the incidence of CRE infections can be effectively reduced.17,18
This study aimed to identify risk factors for CRE colonization in ICU and to establish a CRE colonization risk prediction model to reduce the burden of CRE infections.
Materials and Methods
Study Design and Patients
This is a retrospective database-based cohort study conducted in Fujian Provincial Hospital. The establishment of the database was approved by the institutional ethics committee of Fujian Provincial Hospital (K2022-09-013). Broad informed consent was obtained from each participant on using the clinical and laboratory data for academic research. The clinical and laboratory data were collected and stored in a web-based electronic database. Additionally, guidelines outlined in the Declaration of Helsinki were followed.
All patients who underwent CRE colonization screening and were hospitalized in the ICU from January 2021 to July 2022 were included in the study. For all patients, rectal swabs and throat swabs were taken for bacterial culture every seven days from their first day of admission. Sampling stopped when the patient was discharged or after six tests. Patients who tested positive for CRE at any point were classified as the CRE-colonized group, while those who consistently tested negative for CRE were classified as the non-CRE-colonized group.
Patients with any of the following conditions were excluded: (1) age under 18 years; (2) length of ICU admission less than 24 hours; (3) Patients who were pregnant or confirmed CRE infection or colonization before ICU admission.
CRE Identification
Samples were obtained via throat or rectal swabs. CRE culture and identification were carried out by the hospital’s microbiology laboratory. Susceptibility testing conformed to the Clinical and Laboratory Standards Institute (CLSI) 2020 guidelines.
CRE is defined as follows: (1) resistance to any carbapenem antibiotic, with resistance to imipenem, meropenem, or doripenem (minimum inhibitory concentration [MIC] ≥4 mg/L), or ertapenem resistance (MIC ≥2 mg/L). For organisms intrinsically less sensitive to imipenem (such as Morganella morganii spp., Proteus spp., Providencia spp)., MICs for meropenem and ertapenem were considered;19 (2) Production of carbapenemase.20 Polymerase chain reaction (PCR) was performed to detect carbapenemase. The primers used are consistent with previous studies.21
CRE colonization is defined as a positive CRE culture from any throat or rectal swab collected after ICU admission that does not meet the criteria for CRE infections. CRE infection diagnosis criteria include: (1) CRE positive from a clinically relevant sterile site; (2) satisfies the criteria in the National Healthcare Safety Network (NHSN)22 and ‘Standards For Hospital Infection Diagnosis’ published by the National Health Commission of the People’s Republic of China in 2001.
Data Collection
Clinical data were collected from electronic medical records, including demographics (gender, age); underlying diseases (diabetes, hypertension, malignant tumor); admission source (emergency, internal medicine, surgery department, other ICU); site of infection (lung, bloodstream, abdominal cavity, skin, multi-site); drug exposure (carbapenem antibiotic, β-lactam antibiotic, quinolone antibiotic, combined antibiotic, immunosuppressant); invasive procedures (central venous catheterization, tracheal intubation, tracheotomy, surgery); severity of illness (number of organ failures, length of hospital stay, Acute Physiology and Chronic Health Evaluation [APACHE] II score, Sequential Organ Failure Assessment [SOFA] score). Organ failure was defined as an organ specific SOFA score of equal or greater than two. Antibiotic exposure and immunosuppressant exposure were defined as the use of only one class of antibiotics or immunosuppressant for more than 48 hours within the 90 days prior to CRE colonization. Combined antibiotic exposure was defined as the simultaneous use of two or more antibiotics for more than 48 hours within the 90 days prior to CRE colonization.
Statistical Analysis
The Kolmogorov–Smirnov test was used to determine the normality of data distribution. Non-normally distributed continuous variables were expressed as median with percentiles [M (P25, P75)] and compared by the Mann–Whitney U-test. Categorical data were compared using the Pearson Chi-square test.
The dataset was balanced using SMOTE. The optimal cutoff values for length of hospital stay, number of organ failures, SOFA score, and APACHE II score, were chosen based on the area under the receiver operating characteristic (ROC) curve (AUC). Random forest and Lasso regression were used to select significant independent variables. The dataset was split into 70% for training and 30% for testing. The Random Forest model stabilized when it included approximately 500 decision trees. Shapley Additive Explanations (SHAP) were used to describe the contributions of features to outcome predictions in Random Forest. The intersection of the Random Forest and Lasso regression results was used to construct the CRE colonization risk prediction model using Logistic regression. The total score of the CRE colonization risk prediction model was categorized into low-risk, medium-risk, and high-risk groups using X-tile (version 3.6.1). The Hosmer-Lemeshow test was used to assess the model’s fitting quality. The model was also assessed by four indicators: accuracy, sensitivity, specificity, and AUC. Data processing for this study was performed using R version 4.3.0, and Python version 3.11.4. A two-sided test with P < 0.05 was considered statistically significant.
Results
Clinical Characteristics
This retrospective study included a total of 121 ICU patients who were screened for CRE colonization, from whom 534 samples were collected. Based on the screening results, the study participants were classified into two groups: the CRE-colonized group (n = 18, 14.9%) and the non-CRE-colonized group (n = 103, 85.1%). An overview of the demographic and clinical characteristics of the participants is presented in Table 1, and details of the CRE screening results are shown in Tables S1 and S2. There were 82 males (67.8%) and 39 females (32.2%), originating from the emergency department (n = 53, 43.8%), internal medicine department (n = 25, 20.7%), surgical department (n = 28, 23.1%), and other ICU departments (n = 15, 12.4%). There was no significant difference between the two groups in age, gender, underlying diseases, bloodstream infection, drug exposure (β-lactam antibiotic, quinolone antibiotic), and invasive procedures.
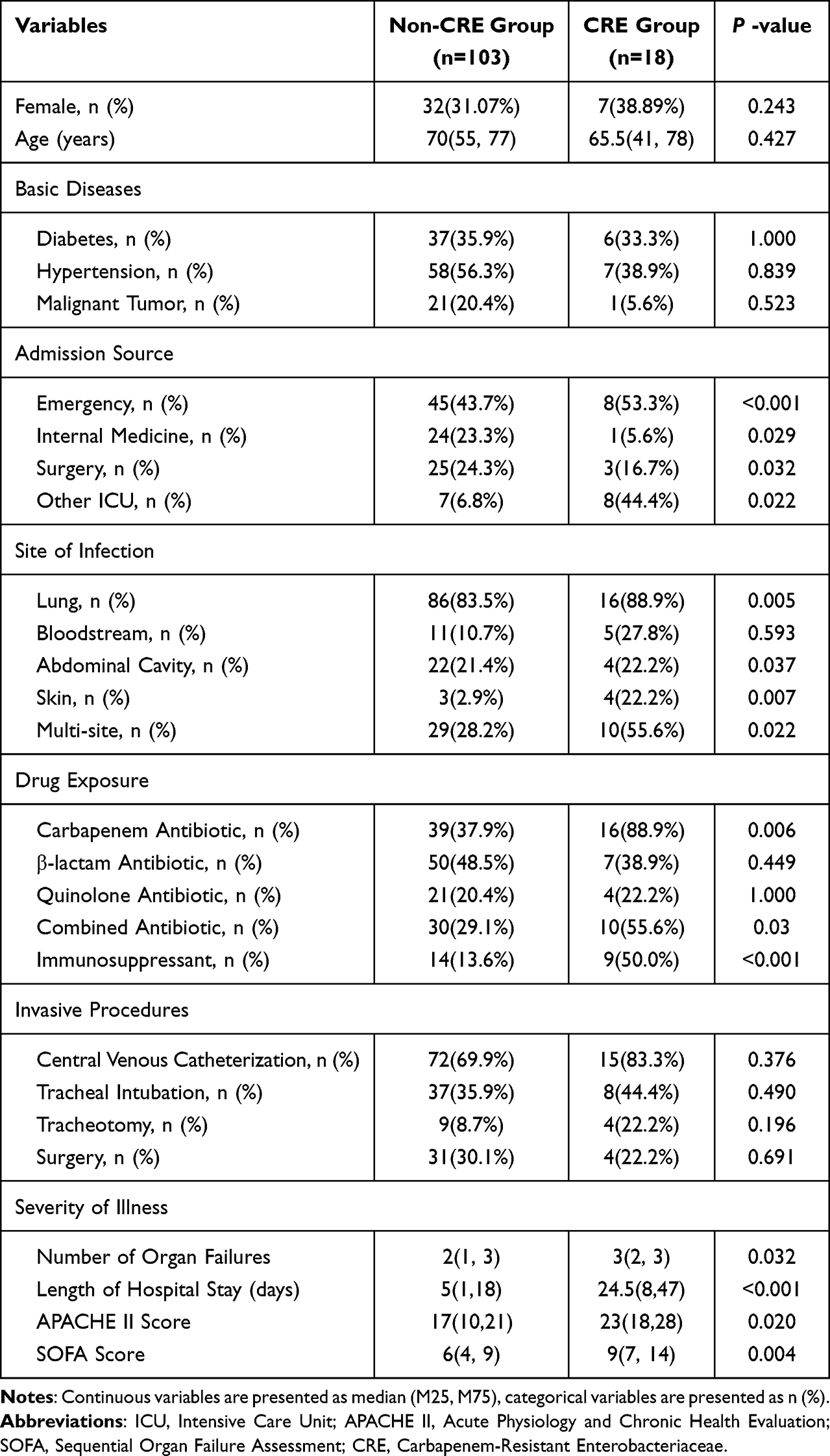 |
Table 1 Clinical Characteristics of the Original Cohort |
A balanced cohort was constructed by SMOTE, resulting in 180 cases in the non-CRE-colonized group and 198 cases in the CRE-colonized group. The clinical characteristics of the balanced cohort are shown in Table 2. Overall, the CRE-colonized group exhibited a higher proportion of females, a lower average age, fewer underlying diseases (hypertension, malignant tumor), fewer transfers from three departments (internal medicine department, surgery department, other ICU departments), more infections (lung, bloodstream, skin, multi-site), more drug exposure (carbapenem antibiotic, β-lactam antibiotic, quinolone antibiotic, combined antibiotic, immunosuppressant), more invasive procedures (central venous catheterization, tracheal intubation, tracheotomy, surgery), higher severity of illness (number of organ failures, length of hospital stay, APACHE II score, SOFA score).
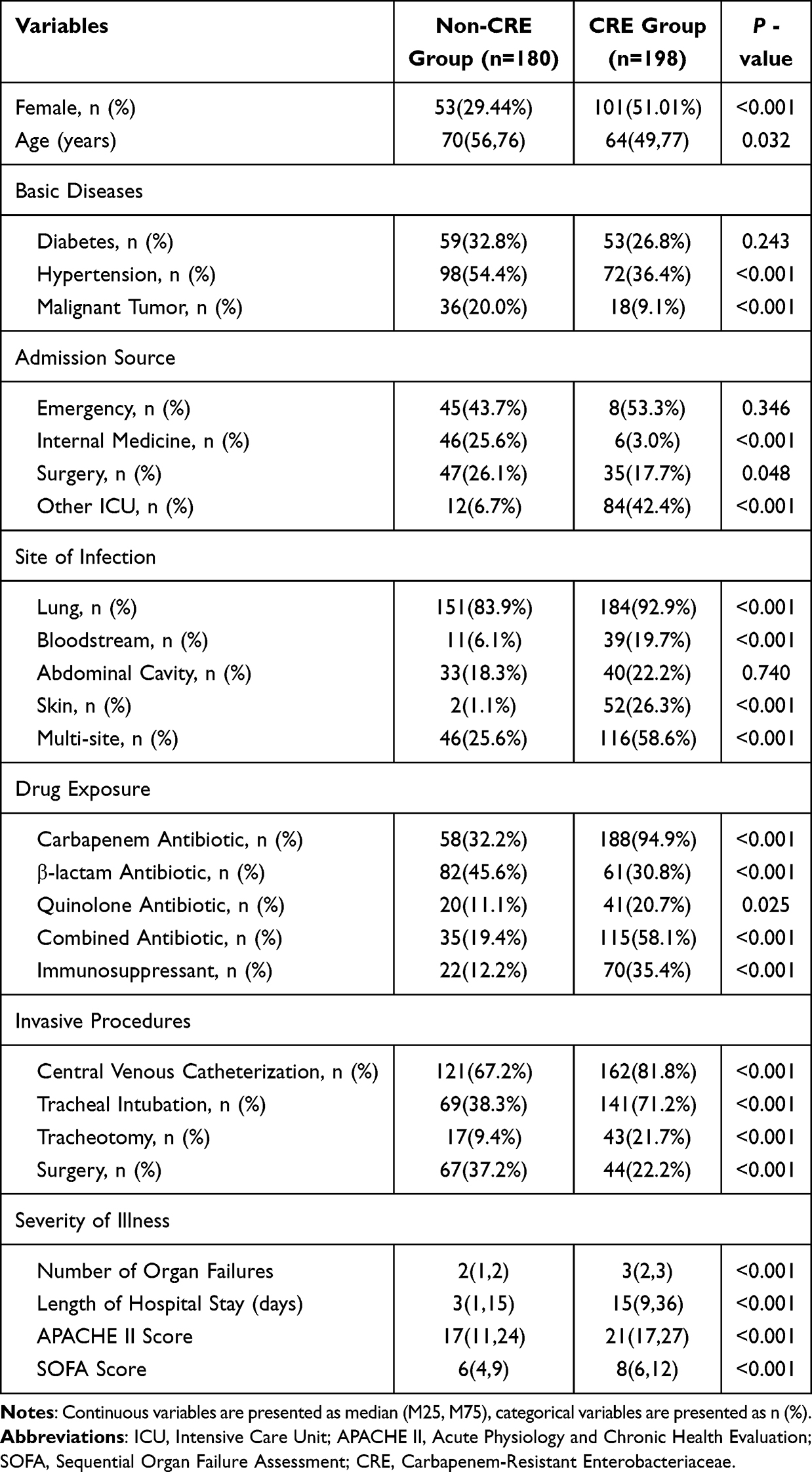 |
Table 2 Clinical Characteristics of the Balanced Cohort |
The optimal cutoff values for SOFA score, APACHE II score, number of organ failures, and length of hospital stay were identified by AUC, which were 16 points, 6 points, 2 organs, and 31 days, respectively. ROC curve and AUC are shown in Figure S1 and Table S3.
Selection of Predictors by Lasso Regression Analysis
Univariate analysis and Lasso regression analysis identified 13 significant variables, including female gender, infection site (lung infection, bloodstream infection, skin infection, multi-site infection), drug exposure (carbapenem antibiotic, immunosuppressant), invasive procedures (central venous catheterization, tracheal intubation, tracheotomy), severity of illness (number of organ failures > 2, APACHE II score > 16, length of hospital stay > 31 days). The selection process operated by LASSO is represented in Figure 1.
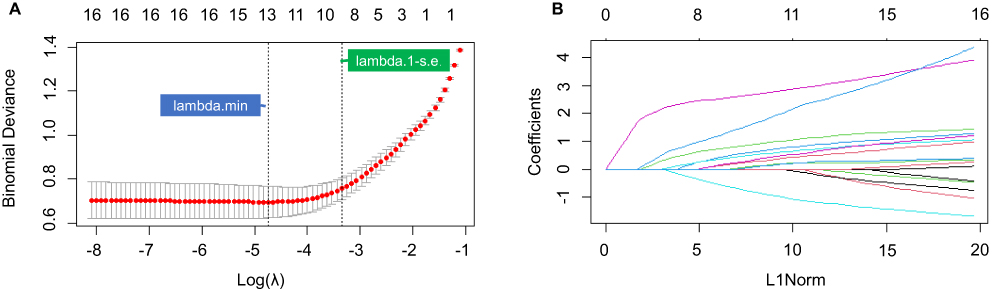 |
Figure 1 LASSO regression Analysis; (A) Cross-validation curve; (B) Distribution of coefficients for the 16 risk factors. |
Selection of Predictors by Random Forest
The contribution of features to Random Forest is depicted in Figure 2. Variables contributing to Random Forest model included carbapenem antibiotic exposure, previous other ICU department admission, number of organ failures > 2, length of hospital stay > 31 days, APACHE II score > 16, previous internal medicine admission, SOFA score > 6, previous emergency department admission, age > 60, tracheal intubation, female gender, multi-site infection, combined antibiotic exposure, immunosuppressant exposure, previous surgery department admission, skin infection, β-lactam antibiotic exposure, malignant tumor, hypertension, diabetes.
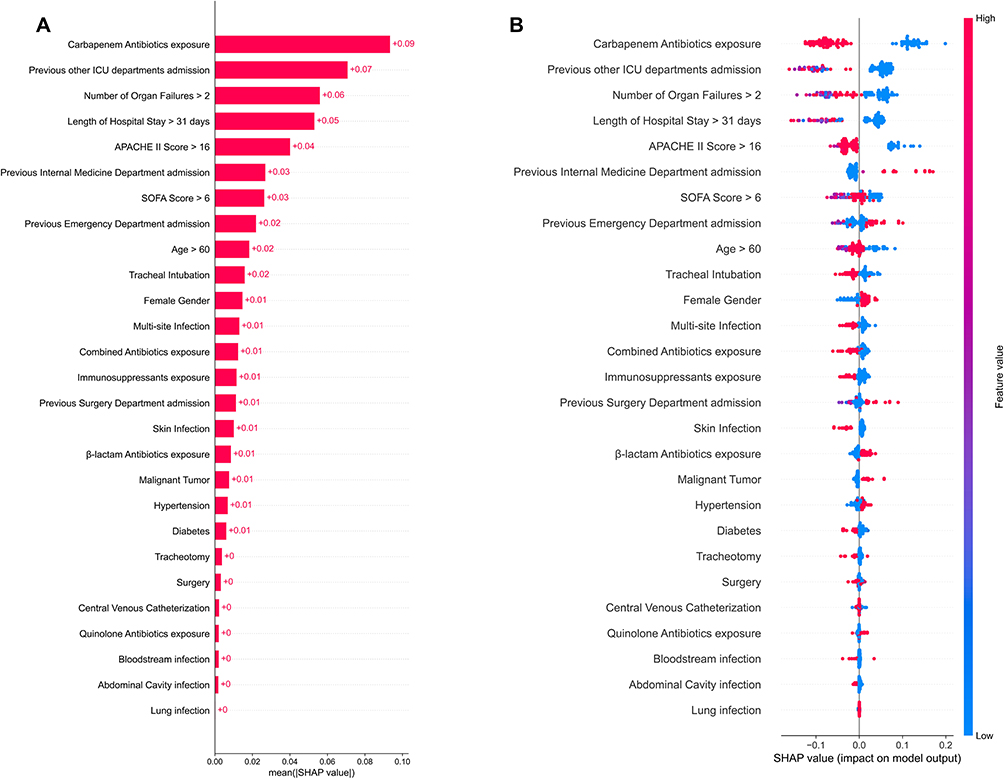 |
Figure 2 Feature contributions in Random Forest; (A) Summary Plot; (B) Beeswarm plot. |
Construction and Evaluation of the Risk Prediction Model
Taking the intersection of the results from Lasso regression and Random Forest analysis as significant variables into the Logistic regression model. Eight variables were identified as independent risk factors for CRE colonization, including female gender, carbapenem antibiotic exposure, length of hospital stay > 31 days, tracheal intubation, APACHE II score > 16, skin infection, multi-site infection, immunosuppressant exposure. Using these variables, a risk prediction model was constructed and shown by a nomogram in Figure 3. The model’s accuracy, sensitivity, specificity, and AUC were 87.83%, 85.6%, 89.9%, and 0.877, respectively. Collinearity testing showed that all VIF values were less than 5, indicating no multicollinearity among variables. The Hosmer-Lemeshow test showed that this model fitted well (P = 0.192 > 0.05).
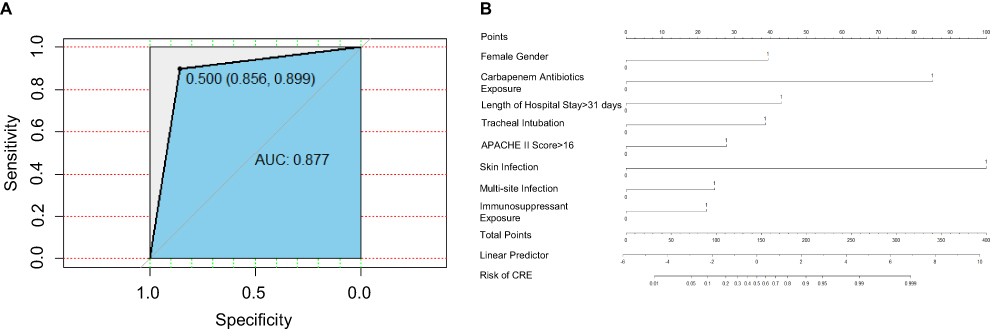 |
Figure 3 The ROC curve and nomogram of the risk prediction model for CRE colonization; (A)ROC curve of the risk prediction model for CRE colonization; (B) Nomogram of CRE colonization risk prediction model. Eight risk factors: Female: 0 (male), 1 (female), corresponding score of 39. Carbapenem antibiotic exposure: 0 (none), 1 (yes), corresponding score of 85. Length of hospitalization >31 days: 0 (none), 1 (yes), corresponding score 43. Tracheal intubation: 0 (none), 1 (yes), the corresponding score is 39. APACHE II > 16 scores: 0 (none), 1 (yes), the corresponding score is 28. Skin infection: 0 (none), 1 (yes), corresponding score of 100. Multi-site infection: 0 (none), 1 (yes), corresponding score of 25. Immunosuppressant exposure: 0 (none), 1 (yes), corresponding score of 22. Each patient’s total score corresponds to the predicted probability of CRE colonization. |
The total score was categorized into three risk groups by X-tile software: low-risk (0–90 points), moderate-risk (91–160 points), and high-risk (161–381 points). In this study, the rates of CRE colonization in the low-risk, moderate-risk, and high-risk groups were 1.82%, 7.14%, and 58.33%, respectively.
Discussion
In this study, we found that female gender, carbapenem antibiotic exposure, length of hospital stay > 31 days, tracheal intubation, APACHE II score > 16, skin infection, multi-site infection, immunosuppressant exposure were independent risk factors for CRE colonization. Few studies have quantitatively assessed these factors, making it difficult for clinicians to determine the risk of CRE colonization. We have constructed a new predictive model comprising these risk factors to provide healthcare professionals with a tool to assess the risk of CRE colonization.
The APACHE II score is widely used in ICUs to assess the severity of patients, with high values associated with increased infection rates and mortality.23 A retrospective study showed that the APACHE II scores differed significantly between the CRE group and the non-CRE group.24 Seo H et al identified a high APACHE II score as an independent risk factor for 14-day mortality in patients with CRE.25 Consistent with these previous research, our study identified APACHE II score > 16 as an independent risk factor for CRE colonization in ICU patients.
The possibility of CRE colonization can significantly increase with the length of hospital stay.26 Similar to our results, Aleidan FAS et al found that prolonged ICU length of stay (LOS) is an independent risk factor associated with CRE infection.27 Two possible reasons are that patients requiring longer hospital stays often have poorer conditions and that prolonged stays increase patients’ exposure risks.
We also identified skin infection as a risk factor for CRE colonization among ICU patients, consistent with the conclusions of previous studies.28 Skin infections may facilitate CRE colonization by disrupting the skin barrier, creating an environment conducive to the invasion and growth of CRE.
In our study, female gender was identified as a risk factor for CRE colonization. This finding is different from previous studies reporting on gender-based susceptibility. Certain studies have suggested that males exhibit a higher propensity for CRE colonization, whereas others have reported no significant correlation between gender and CRE colonization.29–32 A study of antibiotic resistance revealed hormonal fluctuations in females during childbearing and premenopausal age may influence the development of resistance mechanisms.33 Consequently, these hormonal changes in female patients may contribute to the gender differences in CRE colonization observed in our study. Another possible explanation is that women are more prone to urinary tract infections.34 More urinary tract infections lead to greater antibiotic exposure, which in turn provides more opportunities for CRE to colonize more easily.
Exposure to carbapenem antibiotic and immunosuppressant were found to be independent risk factors for CRE colonization, consistent with previous research findings.35,36 Patients who require immunosuppressant often have severe conditions or are experiencing autoimmune diseases. Exposure to immunosuppressants can further weaken their immune capabilities. However, our study did not explore the relationship between the duration and dosage of corticosteroids and the risk of CRE colonization. Additionally, the use of other antibiotics has been reported to be associated with CRE colonization.32,37,38 For instance, Gomides et al found that quinolone antibiotic exposure increases the risk of CRE colonization.32 However, quinolone exposure was not selected as a significant risk factor in our study, possibly due to the low usage of quinolones in our ICU. Given the overuse of antibiotics has been identified as a major cause of emerging bacterial resistance, controlling the use of carbapenem antibiotics is crucial for reducing the formation and spread of CRE resistance.39–41
Invasive procedures, including central venous catheterization, urinary catheterization, and endoscopic diagnostics, have been linked to CRE colonization in ICU patients.26,41,42 Our findings indicated that tracheal intubation is a risk factor for CRE colonization. Other invasive procedures, like central venous catheterization, are also associated with CRE colonization. These invasive procedures disrupt the body’s natural defense barriers and thereby increase the risk of infections in ICU patients. Compared to other invasive procedures, the tube directly contacts the respiratory tract after tracheal intubation, and patients may receive relatively few infection prevention measures. These factors make it a risk factor instead of others.
Based on the eight previously identified risk factors, we constructed a risk prediction model for CRE colonization, which was subsequently represented through a nomogram. This model showed satisfactory accuracy, recall rate, precision, AUC value and fitness. There is a limited body of research that identifies risk factors for CRE colonization and develops a risk prediction model. In comparison to the study conducted by Song JY et al, our model stratifies patients’ risk of CRE colonization into low, moderate, or high categories, providing healthcare professionals with a valuable tool to assess the risk of CRE colonization.43
However, we acknowledge that there were some limitations in this study. First, this is a single-center retrospective cohort study, and the results may differ from those in other regions due to sample size, demographic characteristics, and selection bias. Second, the measures against the transmission of hospital-acquired infections such as healthcare workers’ hand hygiene practices were not taken into consideration. Third, the use of SMOTE to balance data may lead to overfitting and the generation of less realistic synthetic samples, potentially impacting the model’s performance.
Conclusion
Our study contributes to the identification of multiple significant risk factors associated with CRE colonization in ICU patients. Based on these risk factors, we developed a nomogram for CRE colonization with good predictive performance, which may be useful for implementing prevention strategies against CRE transmission.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from two Natural Science Foundations of Fujian Province of China (No. 2022J01404 and No. 2020J011071).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Collaborators AR, Ikuta KS, Sharara F. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
2. Cui X, Zhang H, Du H. Carbapenemases in Enterobacteriaceae: detection and antimicrobial therapy. Front Microbiol. 2019;10:1823. doi:10.3389/fmicb.2019.01823
3. Suay-García B, Pérez-Gracia MT. Present and Future of Carbapenem-resistant Enterobacteriaceae (CRE) infections. Antibiotics. 2019;8(3):122. doi:10.3390/antibiotics8030122
4. Zhang R, Chan EW-C, Zhou H, Chen S. Prevalence and genetic characteristics of carbapenem-resistant Enterobacteriaceae strains in China. Lancet Infect Dis. 2017;17(3):256–257. doi:10.1016/S1473-3099(17)30072-5
5. China Antimicrobial Resistance Surveillance System. Antimicrobial resistance of bacteria: surveillance report from China antimicrobial resistance surveillance system in 2014-2019[J]. Chin J Infect Control. 2021;20(1):15–31.
6. Kengkla K, Wongsalap Y, Chaomuang N, Suthipinijtham P, Oberdorfer P, Saokaew S. Clinical and economic outcomes attributable to carbapenem-resistant Enterobacterales and delayed appropriate antibiotic therapy in hospitalized patients. Infect Control Hosp Epidemiol. 2022;43(10):1349–1359. doi:10.1017/ice.2021.446
7. Tangsawad W, Kositamongkol C, Chongtrakool P, Phisalprapa P, Jitmuang A. The burden of carbapenem-resistant Enterobacterales infection in a large Thai tertiary care hospital. Front Pharmacol. 2022;13:972900.
8. Liao Q, Feng Z, Lin H, et al. Carbapenem-resistant gram-negative bacterial infection in intensive care unit patients: antibiotic resistance analysis and predictive model development. Front Cell Infect Microbiol. 2023;13:1109418. doi:10.3389/fcimb.2023.1109418
9. Li Q, Zhou X, Yang R, et al. Carbapenem-resistant Gram-negative bacteria (CR-GNB) in ICUs: resistance genes, therapeutics, and prevention – a comprehensive review. Front Public Health. 2024;12:1376513. doi:10.3389/fpubh.2024.1376513
10. Papadimitriou-Olivgeris M, Marangos M, Fligou F, et al. KPC-producing Klebsiella pneumoniae enteric colonization acquired during intensive care unit stay: the significance of risk factors for its development and its impact on mortality. Diagn Microbiol Infect Dis. 2013;77(2):169–173. doi:10.1016/j.diagmicrobio.2013.06.007
11. McConville TH, Sullivan SB, Gomez-Simmonds A, Whittier S, Uhlemann A-C. Carbapenem-resistant Enterobacteriaceae colonization (CRE) and subsequent risk of infection and 90-day mortality in critically ill patients, an observational study. PLoS One. 2017;12(10):e0186195. doi:10.1371/journal.pone.0186195
12. Lin Q, Wang Y, Yu J, et al. Bacterial characteristics of carbapenem-resistant Enterobacteriaceae (CRE) colonized strains and their correlation with subsequent infection. BMC Infect Dis. 2021;21(1):638. doi:10.1186/s12879-021-06315-0
13. Tischendorf J, Avila RA, Safdar N. Risk of infection following colonization with carbapenem-resistant Enterobacteriaceae: a systematic review. Am J Infect Control. 2016;44(5):539–543. doi:10.1016/j.ajic.2015.12.005
14. Ho KW, Ng W-T, Ip M, You JHS. Active surveillance of carbapenem-resistant Enterobacteriaceae in intensive care units: is it cost-effective in a nonendemic region? Am J Infect Control. 2016;44(4):394–399. doi:10.1016/j.ajic.2015.10.026
15. Cheng B, Li Z, Wang J. Comparison of the performance between sepsis-1 and sepsis-3 in ICUs in China: a retrospective multicenter study. Shock. 2017;48(3):301–306. doi:10.1097/SHK.0000000000000868
16. Zaidah AR, Mohammad NI, Suraiya S, Harun A. High burden of Carbapenem-resistant Enterobacteriaceae (CRE) fecal carriage at a teaching hospital: cost-effectiveness of screening in low-resource setting. Antimicrob Resist Infect Control. 2017;6(1):42. doi:10.1186/s13756-017-0200-5
17. Ilan MB, Kjerulf A. Who should be screened for carbapenemase-producing Enterobacterales and when? A systematic review. J Hosp Infect. 2023;142:74–87. doi:10.1016/j.jhin.2023.09.018
18. Chen H-Y, Jean -S-S, Lee Y-L, et al. Carbapenem-resistant enterobacterales in long-term care facilities: a global and narrative review. Front Cell Infect Microbiol. 2021;11:601968. doi:10.3389/fcimb.2021.601968
19. China antimicrobial surveillance network [homepage on the Internet]. CHINET China Bacterial Resistance Monitoring Network Technical solution (2020 update). Available from: http://www.chinets.com.
20. Centers or Disease Control and Prevention [website on the Internet]. Guidance for Control of Carbapenem-resistant Enterobacteriaceae (CRE); 2012 CRE toolkit; 2012. Available form: https://stacks.cdc.gov/view/cdc/13205.
21. Wu Y, Chen J, Zhang G, et al. In vitro activities of the essential antimicrobial agents including aztreonam/avibactam, eravacycline, colistin, and other comparators against carbapenem-resistant bacteria with different carbapenemase genes: a multicenter study in China, 2021[J]. Int J Antimicrob Agents. 2024;64(5):107341. doi:10.1016/j.ijantimicag.2024.107341
22. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–332. doi:10.1016/j.ajic.2008.03.002
23. Frost SA, Alexandrou E, Bogdanovski T, et al. Severity of illness and risk of readmission to intensive care: a meta-analysis. Resuscitation. 2009;80(5):505–510. doi:10.1016/j.resuscitation.2009.02.015
24. Dickstein Y, Edelman R, Dror T, Hussein K, Bar-Lavie Y, Paul M. Carbapenem-resistant Enterobacteriaceae colonization and infection in critically ill patients: a retrospective matched cohort comparison with non-carriers. J Hosp Infect. 2016;94(1):54–59. doi:10.1016/j.jhin.2016.05.018
25. Seo H, Lee SC, Chung H, et al. Clinical and microbiological analysis of risk factors for mortality in patients with carbapenem-resistant Enterobacteriaceae bacteremia. Int J Antimicrob Agents. 2020;56(4):106126. doi:10.1016/j.ijantimicag.2020.106126
26. Tran DM, Larsson M, Olson L, et al. High prevalence of colonisation with carbapenem-resistant Enterobacteriaceae among patients admitted to Vietnamese hospitals: risk factors and burden of disease. J Infect. 2019;79(2):115–122. doi:10.1016/j.jinf.2019.05.013
27. Aleidan FAS, Alkhelaifi H, Alsenaid A, et al. Incidence and risk factors of carbapenem-resistant Enterobacteriaceae infection in intensive care units: a matched case-control study. Exp Rev Anti-Infective Ther. 2021;19(3):393–398. doi:10.1080/14787210.2020.1822736
28. Eser F, Yilmaz GR, Güner R, Hasanoğlu İ, Ürkmez Korkmaz FY, Açikgöz ZC. Risk factors for rectal colonization of carbapenem-resistant Enterobacteriaceae in a tertiary care hospital: a case-control study from Turkey. Turk J Med Sci. 2019;49(1):341–346. doi:10.3906/sag-1810-65
29. Sun JD, Huang SF, Yang SS, Pu SL, Zhang CM, Zhang LP. Impact of carbapenem heteroresistance among clinical isolates of invasive Escherichia coli in Chongqing, southwestern China. Clin Microbiol Infect. 2015;21(5):469–e1. doi:10.1016/j.cmi.2014.12.013
30. W-Q W, Zhang Y-Q, Xu J, et al. Risk factors for carbapenem-resistant Enterobacteriaceae colonization and the effect on clinical outcomes and prognosis in allogeneic hematopoietic stem cell transplanted patients. Infect Drug Resist. 2023;16:6821–6831. doi:10.2147/IDR.S424048
31. Chiotos K, Tamma PD, Flett KB, et al. Multicenter study of the risk factors for colonization or infection with carbapenem-resistant Enterobacteriaceae in children. Antimicrob. Agents Chemother. 2017;61(12):10.1128/aac.01440–01417. doi:10.1128/AAC.01440-17
32. Gomides MDA, Fontes A, Silveira AOSM, Matoso DC, Ferreira AL, Sadoyama G. The importance of active surveillance of carbapenem-resistant Enterobacterales (CRE) in colonization rates in critically ill patients. PLoS One. 2022;17(1):e0262554. doi:10.1371/journal.pone.0262554
33. Sahuquillo-Arce JM, Selva M, Perpinan H. Antimicrobial resistance in more than 100,000 Escherichia coli isolates according to culture site and patient age, gender, and location. Antimicrob Agents Chemother. 2011;55(3):1222–1228. doi:10.1128/AAC.00765-10
34. Alhazmi AH, Alameer KM, Abuageelah BM, et al. Epidemiology and antimicrobial resistance patterns of urinary tract infections: a cross-sectional study from southwestern Saudi Arabia[J]. Medicina. 2023;59(8):1411. doi:10.3390/medicina59081411
35. Bhargava A, Hayakawa K, Silverman E. Risk factors for colonization due to carbapenem-resistant Enterobacteriaceae among patients exposed to long-term acute care and acute care facilities. Infect Control Hosp Epidemiol. 2014;35(4):398–405. doi:10.1086/675614
36. Mills JP, Talati NJ, Alby K, Han JH. The epidemiology of carbapenem-resistant Klebsiella pneumoniae colonization and infection among long-term acute care hospital residents. Infect Control Hosp Epidemiol. 2016;37(1):55–60. doi:10.1017/ice.2015.254
37. Eshetie S, Unakal C, Gelaw A, Ayelign B, Endris M, Moges F. Multidrug resistant and carbapenemase producing Enterobacteriaceae among patients with urinary tract infection at referral hospital, Northwest Ethiopia. Antimicrob Resist Infect Control. 2015;4(1):12. doi:10.1186/s13756-015-0054-7
38. Hassoun-Kheir N, Hussien K, Karram M, et al. Clinical significance and burden of carbapenem-resistant Enterobacterales (CRE) colonization acquisition in hospitalized patients. Antimicrob Resist Infect Control. 2023;12(1):129. doi:10.1186/s13756-023-01323-y
39. Li Y, Xia X, Li X, Xiao K, Zhuang X. Correlation between the use of antibiotics and development of a resistant bacterial infection in patients in the ICU. Biosci Trends. 2018;12(5):517–519. doi:10.5582/bst.2018.01130
40. Yan L, Sun J, Xu X, Huang S. Epidemiology and risk factors of rectal colonization of carbapenemase-producing Enterobacteriaceae among high-risk patients from ICU and HSCT wards in a university hospital. Antimicrob Resist Infect Control. 2020;9(1):155. doi:10.1186/s13756-020-00816-4
41. Moghnieh R, Abdallah D, Jadayel M. Epidemiology, risk factors, and prediction score of carbapenem resistance among inpatients colonized or infected with 3rd generation cephalosporin resistant Enterobacterales. Sci Rep. 2021;11(1):14757. doi:10.1038/s41598-021-94295-1
42. Sharma K, Tak V, Nag VL, Bhatia PK, Kothari N. An observational study on carbapenem-resistant Enterobacterales (CRE) colonisation and subsequent risk of infection in an adult intensive care unit (ICU) at a tertiary care hospital in India. Infect Prevent Pract. 2023;5(4):100312. doi:10.1016/j.infpip.2023.100312
43. Song JY, Jeong IS. Development of a risk prediction model of carbapenem-resistant Enterobacteriaceae colonization among patients in intensive care units[J]. Am J Infect Control. 2018;46(11):1240–1244. doi:10.1016/j.ajic.2018.05.001
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.