")
Back to Journals » International Journal of General Medicine » Volume 16
Rise of Pregabalin Poisoning and Abuse Cases in Serbia: A Ten-Year Retrospective Study
Authors Antunovic M , Vucinic S, Kotur-Stevuljevic J , Krstic K, Jovic-Stosic J, Kilibarda V, Perkovic-Vukcevic N , Djordjevic S
Received 21 January 2023
Accepted for publication 3 April 2023
Published 8 April 2023 Volume 2023:16 Pages 1239—1250
DOI https://doi.org/10.2147/IJGM.S405616
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Satish Chandrasekhar Nair
Marko Antunovic,1,2 Slavica Vucinic,1,2 Jelena Kotur-Stevuljevic,3 Kristijan Krstic,4 Jasmina Jovic-Stosic,1,2 Vesna Kilibarda,1,2 Natasa Perkovic-Vukcevic,1,2 Snezana Djordjevic1,2
1Medical Faculty Military Medical Academy, University of Defense, Belgrade, Serbia; 2National Poison Control Center, Military Medical Academy, Belgrade, Serbia; 3Department of Medical Biochemistry, Faculty of Pharmacy, University of Belgrade, Belgrade, Serbia; 4Department of Physical Medicine and Rehabilitation, Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
Correspondence: Marko Antunovic, National Poison Control Center, Military Medical Academy, Crnotravska 17, Belgrade, 11040, Serbia, Tel +381 11 3608 264, Fax +381 11 367 21 87 264, Email [email protected]
Purpose: The aim of this study was to analyze data on gabapentinoid-related attendances to the National Poison Control Center of Serbia (NPCC), particularly abuse cases; to estimate its changes and to compare it with trends in national consumption rates of these drugs. We also aimed to analyze the main characteristics of the study population and to investigate the major clinical effects in poisoned patients.
Patients and Methods: This is a retrospective study of patients admitted to the NPCC for acute poisoning involving gabapentinoids from 1 May 2012 to 1 October 2022.
Results: There were 357 (95.5%) pregabalin-related and 17 (4.5%) gabapentin-related poisoning cases in 302 patients. Abuse of pregabalin was detected in 27.8% (84/302), while gabapentin abuse occurred in 0.7% (2/302) of all patients. A steady increase in rates of pregabalin poisoning and abuse cases strongly correlated with the increase in overall consumption of this drug, while there were no significant changes in rates of gabapentin consumption, poisoning and abuse rate during the study period. Most patients who abused pregabalin pregabalin were males (84.5%) and the median age was 26 years (range: 15– 45 years). Almost 60% of patients who abused pregabalin (48/84) belonged to the migrant population. Co-ingestions occurred in 89.4% of pregabalin-related cases (319/357), resulting in more severe poisoning. The most often co-ingested drugs were benzodiazepines and among them clonazepam was detected in the largest number of cases.
Conclusion: The poisoning and abuse cases involving pregabalin are on the rise in Serbia, which coincided with an increase in its overall consumption during the study period. Isolated pregabalin ingestions resulted in mild poisoning, although severe symptoms such as coma and bradycardia were recorded. When prescribing pregabalin to patients at risk of abuse caution is needed. Strengthening the measures for dispensing of pregabalin may reduce the risks associated with its abuse.
Keywords: gabapentinoids, overdose, misuse, drug consumption, psychoactive substances
Plain Language Summary
Drug abuse is a serious health problem worldwide, and acute poisoning remains a significant cause of death. Gabapentinoids (pregabalin and gabapentin) are a group of drugs that have not traditionally been abused. However, as their therapeutic use has increased, so have the number of reports describing an increase in abuse and overdose with these drugs. In this paper, we present data on the number of patients admitted to the National Poison Control Center of Serbia (NPCC) for acute poisoning with gabapentinoids. We looked at the toxicity levels of these drugs and assessed whether, and to what extent the phenomenon of gabapentinoid abuse is present in Serbia. We found that pregabalin is used much more frequently in therapy in our country compared to gabapentin. The number of patients who abused pregabalin and were treated in NPCC has increased significantly over the past decade. During the same period, therapeutic use and the number of poisoning and abuse cases related to gabapentin were significantly lower and even decreased. When patients took pregabalin alone, it did not cause severe poisoning. However, this drug is mainly used or abused together with other psychoactive substances, which carries a higher risk of developing more serious clinical effects. In some countries pregabalin and/or gabapentin are classified as controlled psychoactive substances, and the results of our study may serve the authorities in Serbia to consider such a possibility, in response to the growing trend of pregabalin poisoning and abuse in our country.
Introduction
Pregabalin and gabapentin are psychoactive agents that belong to the drug group gabapentinoids. Although synthesized as structural analogs of γ-aminobutyric acid (GABA), gabapentinoids do not bind to GABA receptors, but exert their effects primarily by inhibiting voltage-gated calcium channels, resulting in attenuation of neuronal calcium influx, reduction of neurotransmitter release and slowing of neuronal excitability.1 In many countries, the prescribing and overall consumption of gabapentinoids has increased sharply.2,3 A significant part of this trend is attributed to the common off-label use of gabapentinoids and the ongoing efforts of clinicians not to rely on opioids in the treatment of various pain conditions.4 In Serbia, gabapentinoids are approved for the treatment of neuropathic pain and as adjunctive therapy for focal seizures in patients with epilepsy, while pregabalin has an additional indication for the treatment of generalized anxiety disorder. In some countries pregabalin is approved for the treatment of fibromyalgia syndrome.5 According to the Medicines and Medical Devices Agency of Serbia annual reports on prescription and dispensing of drugs, the consumption of pregabalin has increased more than 200 times in the last decade. At the same time, there has been a remarkably smaller change in the use of gabapentin.6 In parallel with widespread use, there are a growing number of reports of misuse, abuse and acute poisonings associated with gabapentinoids.7–10 It seems that pregabalin is more prone to abuse due to its pharmacokinetic and pharmacodynamic properties.11 It has non-saturable absorption and higher bioavailability, faster onset of action, and six times higher potency compared to gabapentin.11,12 Among the poisoning cases, there is great interindividual variability regarding the clinical effects and ingested dose of drug.13 Severe signs and symptoms mainly occur in cases when other drugs are co-ingested, but have also been reported in isolated poisoning as well.14
Currently, there are no official data on gabapentinoid poisonings in Serbia and little is known about the patterns of abuse in our country. The aim of this study is to present data on gabapentinoid related attendances to the National Poison Control Center in Serbia (NPCC; a reference institution in our country for the treatment of patients with acute poisoning), particularly abuse cases, estimate their changes and compare them with changes in consumption rates of these drugs in Serbia. We also aimed to describe the main characteristics and clinical manifestations of the study population, in order to improve the current knowledge about gabapentinoid toxicity.
Materials and Methods
Study Design
This is a retrospective study of patients admitted to the NPCC for acute poisoning involving pregabalin or gabapentin during the 10-year period (May 1, 2012-October 1, 2022). The NPCC was established in Military Medical Academy, Belgrade, Serbia in 1997, and consists of two major organizational units - the Clinic of Emergency Medicine and Clinical Toxicology and the Institute of Toxicology and Pharmacology (both units work 24/7). There are approximately 4500 patients with acute poisoning treated at the NPCC every year.
Terminology and Data
Data collected on admission and during the hospitalization (demographic data, anamnestic and hetero-anamnestic data, laboratory findings, clinical effects, complications, treatment and outcome) are archived in the medical record for each patient. Following patient discharge all data are entered into the toxicology database of NPCC, after prior review and assessment of the poisoning severity by a clinical toxicologist.
In the available literature an overlap in definitions and various explanations for drug misuse- and abuse-related events could be found. For this study, we decided to use the classification adopted in the Analgesic, Anesthetic, and Addiction Clinical Trials, Translations, Innovations, Opportunities, and Networks (ACTTION) group review, which suggested following definitions: Abuse - any intentional, nontherapeutic use of a drug, even on a one-time basis, to achieve a desired psychological or physiological effect; Misuse - any intentional therapeutic use of a drug product in an inappropriate manner; Suicide-related event - self-injurious or potentially self-injurious behavior associated with at least some intent to die or that resulted in death. Evidence that the individual intended to kill him/herself, at least to some degree, can be explicit or inferred from the behavior or circumstance. A suicide attempt may or may not result in actual injury.15
The Poisoning Severity Score (PSS), a system that grades the severity of poisoning based on the overall clinical course, regardless of the ingested dose, concentration, type and number of agents involved, was used.16 Poisonings are classified into five grades: PSS 0 - no symptoms of poisoning (None); PSS 1- mild symptoms or signs (Minor); PSS 2 - pronounced or prolonged symptoms or signs (Moderate), PSS 3 - severe or life-threatening symptoms or signs (Severe) and PSS 4 - death (Fatal).
A history of problematic substance use was defined on previous documented evidence in patient history (eg drug related self-harm or suicide-related event, past hospitalization due to substance misuse/abuse/overdose, history of substance abuse treatment). The information on ingested dose was self-reported and collected from anamnestic or hetero-anamnestic data. For detection and quantification of pregabalin in plasma samples of patients, we validated an in-house liquid chromatography coupled with the tandem mass spectrometer (LC-MS/MS) method using a ACQUITY UPLC H-Class System coupled with a XEVO TQD triple quadruple mass spectrometer (Waters Corp., Milford, MA, USA).17
Data related to drug consumption are presented in terms of defined daily doses per 1000 inhabitants per day (DDD/1000 inhabitants/day) using the ATC/DDD methodology recommended by WHO. Data related to acute poisonings and abuse cases are presented as absolute numbers or a number of cases per 100,000 inhabitants.18 Trends in gabapentinoid acute poisoning and abuse cases were estimated from annual data from the NPCC database, whereas changes in drug consumption were estimated from annual reports on prescribing and dispensing of drugs from the Medicines and Medical Devices Agency of Serbia.6
Ethics Approval
This study was conducted with the approval of the Ethics Committee of the Military Medical Academy (resolution number 25/2022) in accordance with the ethical principles of the Declaration of Helsinki and the International Council for Harmonization (ICH) guidelines for good clinical practice (GCP). For this type of study, a formal informed consent was not required by the Ethics Committee. Data were analyzed without identifying patients and confidentiality was maintained throughout the study.
Statistical Analysis
The distribution of continuous data was tested with the Kolmogorov–Smirnov and the Shapiro–Wilk test. Since most of the dataset were with non-normal distribution, continuous variables were expressed as medians and interquartile values (Q1 (25. percentile) - Q3 (75. percentile)). The difference between groups was compared with the Mann–Whitney U-test, and the relationship between data was tested with the Spearman correlation coefficient. Categorical variables were expressed as absolute numbers or frequencies of specific categories and the Chi-Square test was used for the analysis. A p-value of <0.05 was considered statistically significant.
Results
During the study period, there were 374 cases of gabapentinoid-related acute poisoning in 302 patients admitted to NPCC, with 51 repeat readmissions (median: 1 readmission; range: 1–5 readmissions). Most cases involved pregabalin (95.5% - 357/374) and a much smaller proportion involved gabapentin (4.5% - 17/374). The proportion of patients who abused pregabalin and gabapentin was 27.8% (84/302) and 0.7% (2/302) of the study population, respectively. The gender difference was most pronounced in the group of patients who abused pregabalin (males: 71/84–84.5%), whereas the majority of patients in the suicide-related events group were female (79/112–70.5%). The age distribution was significantly different in the group of patients who abused pregabalin (median: 26 years, range: 15–45 years) compared to the misuse (median: 42 years, range: 13–87 years) and suicide-related events group (median: 41 years, range: 16–84 years). In all groups, concurrent use of other psychoactive substances was more common than isolated pregabalin poisoning, and benzodiazepines were the most common coingestants. The main route of administration was ingestion and only one patient took pregabalin intranasally. Where the reasons were reported, most of the patients abused pregabalin and gabapentin to achieve a psychoactive effect or to potentiate effects of other co-ingested substances, while in two cases drugs were taken to increase arousal and sexual desire.
Trends in Acute Poisonings, Abuse Cases and Consumption of Gabapentinoids in Serbia
Examining the average maintenance daily dose (Defined Daily Dose: DDD) for gabapentinoids in the period between 2012 and 2021, there was a steady increase in pregabalin consumption in Serbia (from 0.02 DDD/1000 inhabitants/day in 2012 to 4.58 DDD/1000 inhabitants/day in 2021). In the same period, the rate of acute poisonings involving pregabalin increased from 0.01 cases of poisoning per 100,000 inhabitants (one case) in 2012 to 1.13 cases of poisoning per 100,000 inhabitants (78 cases) in 2021. The first case of pregabalin abuse was detected in 2016 (it was the only one in that year) and the highest number of abuse-related poisonings (30 cases) was detected in 2020. The rising trend in pregabalin consumption between 2012 and 2021 was in a strong positive correlation with both increase in the annual rate of both acute poisonings (r=0.900, p<0.001; Spearman correlation coefficient) and abuse cases among them (r=0.957, p<0.001; Spearman correlation coefficient) (Figure 1). Gabapentin consumption in Serbia decreased slightly over the 10-year period (from 0.15 DDD/1000 inhabitants per day in 2012 to 0.11 DDD/1000 inhabitants per day in 2021). During the study period, the maximum number of poisoning cases related to gabapentin was recorded in 2012 and 2019 (four cases in each year). Abuse was detected in three cases in 2012, and in only one case in 2019. There were no significant changes nor correlation between the consumption of gabapentin and the rates of acute poisonings or abuse cases.
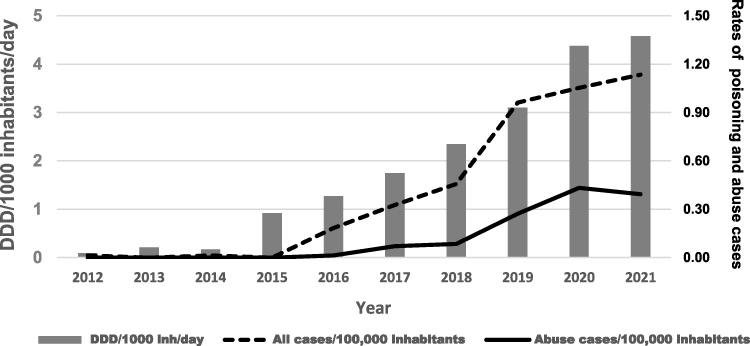 |
Figure 1 Pregabalin consumption and poisoning cases in National Poison Control Center of Serbia for ten-year period (2012–2021). |
Due to disproportion and evident higher frequency of pregabalin in acute poisonings and abuse-related cases, data concerning only this drug will be presented in further analysis.
The Main Characteristics of the Patients with Pregabalin-Related Acute Poisoning
To distinguish the main sociodemographic differences and patterns of pregabalin use among the patients in this study, we classified the cases into the following groups: suicide-related events, misuse- and abuse-related cases as presented in Table 1. Suicide-related events accounted for 40.9% of all cases (146/357), with the majority of patients being female (70.5%) (p<0.001; Chi-Square test). Pregabalin abuse was detected in 28.9% (103/357) of all poisoning cases. Most patients who abused pregabalin were male (84.5%) (p<0.001; Chi-Square test) and younger than 40 years (70.3% of them were younger than 30 years and 21.4% were between 30 and 40 years old). The age distribution in all groups is presented in Figure 2.
 |
Table 1 The Main Characteristics of the Study Population (Pregabalin-Related) and Differences Among Suicide-Related Events, Misuse and Abuse Cases |
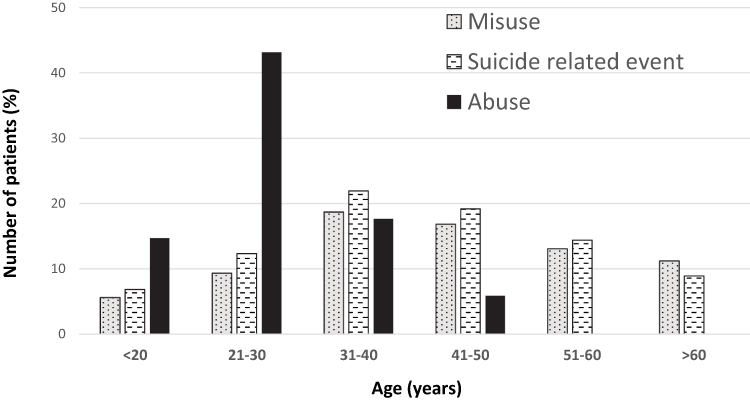 |
Figure 2 Age distribution (%) of the study population in misuse, abuse and suicide related events. |
The dose of pregabalin was recorded in 59.7% (213/357) of all study cases. Suicide-related events (median: 600 mg, Q1-Q3: 350–1300 mg) and abuse cases (median: 600 mg, Q1-Q3: 450–1000 mg) involved significantly higher doses of pregabalin than misuse-related cases (median: 237 mg, Q1-Q3: 150–475 mg) (p<0.001; Chi-Square test). A history of problematic substance use was present in almost half of the patients in all poisoning cases (Table 1).
In all groups, concurrent use of other psychoactive substances was more frequent than isolated pregabalin poisoning. Benzodiazepines were the commonest coingestants, although there were differences among the groups in frequencies of specific benzodiazepine drugs. The most notable difference was observed for clonazepam. Following benzodiazepines, alcohol and opioids were the most frequently co-ingested substances in the group of patients who abused pregabalin. Illicit drugs (eg heroin, cannabis, amphetamines and cocaine) were detected in a small number of cases. For a detailed description of the psychoactive substances most commonly co-ingested with pregabalin, see Supplementary Table 1 Parts 1 and 2.
Sociodemographic data showed that a large number of patients belonged to the migrant population (55 patients) and among them, 87.3% (48/55) were related to abuse of pregabalin while 12.7% (7/55) were in a misuse-related group (Table 1). In this subgroup of the study population, concomitant use of pregabalin and clonazepam was extremely common and detected in 85.4% of them (data not shown here).
Clinical Features of Pregabalin Acute Poisonings
The main clinical features of patients admitted to the NPCC due to acute poisoning involving pregabalin are listed in Table 2. The majority of all patients were discharged after the treatment in emergency department (64.4%), however patients were admitted more often to the clinic for further treatment when other drugs and substances were co-ingested. Seizures were recorded in only two patients. One of them had a history of epilepsy, while in the other patient the seizure occurred on the eighteenth day of hospitalization, followed by a fatal outcome. Only one patient (age 31 years) with no history of cardiovascular disease presented with sinus bradycardia, after ingesting only 750 mg of pregabalin. The patient was taking prescribed pregabalin for some time, but on the day of admission he took a higher dose than recommended. On admission he was somnolent, with a heart rate of 38/min, which later improved to 42/min. After treatment and observation in the emergency department, the patient recovered and was referred to a cardiologist.
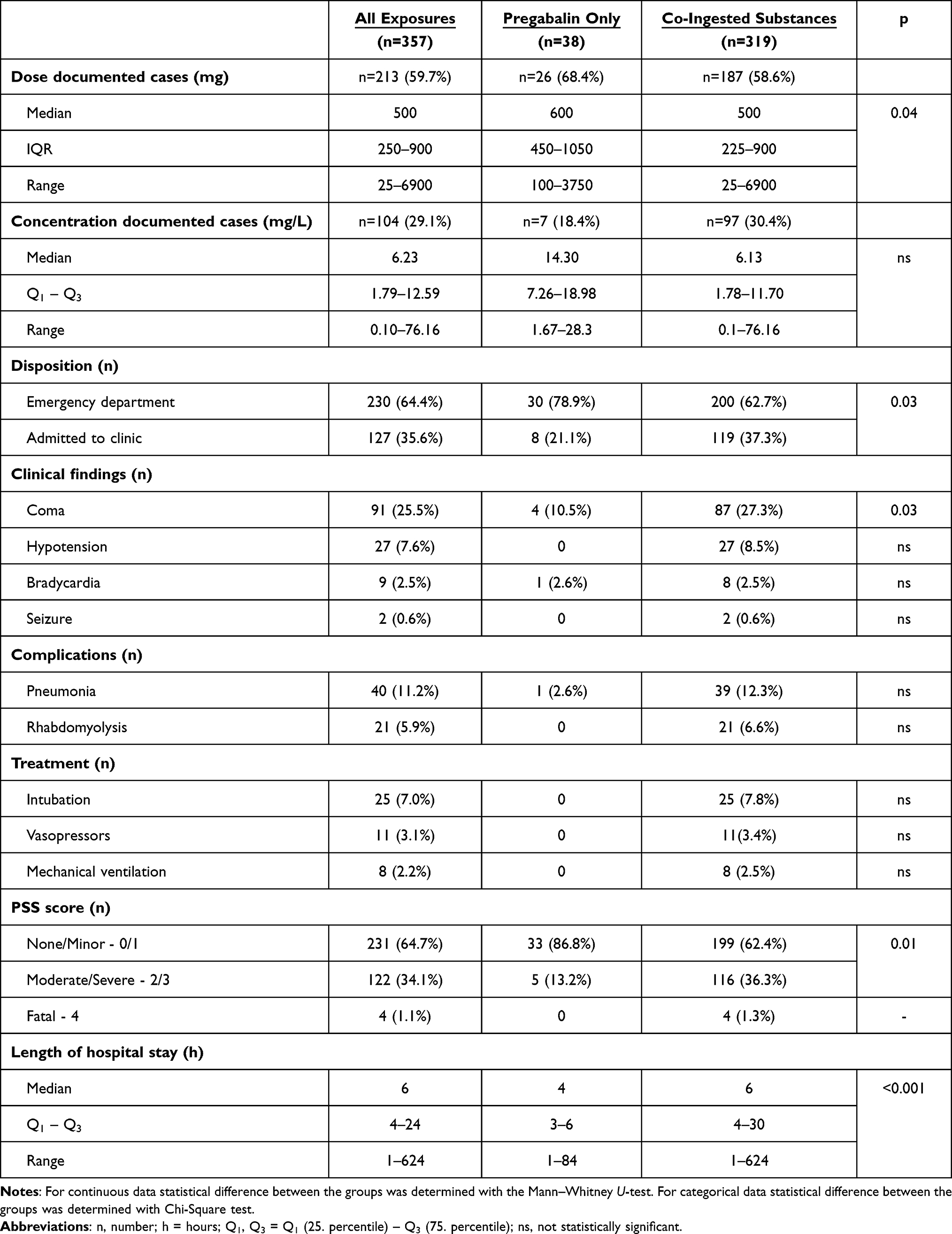 |
Table 2 Clinical Features of Study Population and Differences Among Pregabalin Isolated and Polysubstance Poisonings |
Co-ingestion of other psychoactive substances was more common and these cases involved significantly higher doses of pregabalin in severe (PSS 3 - median dose: 1750 mg, Q1-Q3:675–2800 mg) and moderate poisonings (PSS 2 - median dose: 1200 mg, Q1-Q3:900–2100 mg) comparing to the mild poisonings (PSS 1 - median dose: 375 mg, Q1-Q3:150–600 mg), (p<0.001; Chi-Square test) and asymptomatic patients (PSS 0 - median dose: 150 mg, Q1-Q3:100–300 mg) (p<0.001; Chi-Square test).
Significantly higher pregabalin plasma concentrations were found in patients hospitalized in the clinic for further treatment and in cases required intubation and mechanical ventilation (Supplementary Table 2). The highest pregabalin plasma concentration in this study was found in a female patient (age 45 years) admitted 3 hours after ingestion of an unknown dose of pregabalin. In this case, pregabalin plasma concentrations were 76.16 mg/L (at admission), 28.26 mg/L (12 hours later) and declined to <1 mg/L (36 hours after admission). The patient was admitted to NPCC in a coma with hypotension (80/50 mmHg), normal heart rate (70/min), and low oxygen saturation (80%), while a toxicology screening revealed a low blood ethanol concentration (0.1‰) and co-ingestion of several drugs (diazepam, zolpidem, citalopram, mirtazapine and paracetamol) that were within the therapeutic range. Intubation was performed for airway protection and short-term mechanical ventilation was required because of respiratory failure.
The patient’s mental status improved, and she was extubated on the third day of hospitalization. Six days after admission, the patient made a full recovery and was discharged from the NPCC clinic. A significant positive correlation was found between the concentration, reported dose, severity of poisoning and length of hospitalization (Supplementary Table 2).
In cases of isolated pregabalin poisonings, the median dose of pregabalin was significantly higher in patients within PSS 1 group (median: 750 mg, Q1-Q3: 500–1275 mg) comparing to patients in PSS 0 group (300 mg, Q1-Q3: 300–450 mg) (p<0.01; Chi-Square test). The dose was recorded in only one patient within the PSS 2 group, that was admitted to the clinic in a coma, after ingesting 2100 mg of pregabalin. After the treatment with only supportive therapy, the patient recovered and was discharged after 20 hours of hospitalization. In isolated pregabalin poisonings we also found a positive correlation of the ingested dose with the PSS score (r=0.390, n=26, p<0.05; Spearman correlation coefficient) and the length of hospitalization (r=0.553, n=26, p<0.01; Spearman correlation coefficient). Concentration was measured in only seven cases with isolated pregabalin poisoning so there was no sufficient data for correlation analysis.
Discussion
The most significant finding of this study was the detection of an immense increase in pregabalin poisoning and abuse cases in Serbia. A growing body of literature indicates an increasing global trend in the use/misuse/abuse and overdose cases with gabapentinoid drugs.7–10,12,14 The first signals of problematic use of pregabalin came from Sweden, Norway and Finland in 2009, when it was reported as a new psychoactive substance to the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) via Early warning system.19 Available literature data suggests that abuse and misuse are more common among pregabalin users compared with gabapentin, which is in accordance with our results.10–12,20 In most of the cases of our study, patients were admitted to the NPCC for acute poisoning involving pregabalin (95.5%), whereas the number of cases related to gabapentin was much lower (4.5%). In addition, abuse was detected to a much greater extent in the poisoning cases related to pregabalin compared with gabapentin.
The strong correlation between the increase in pregabalin poisonings and overall consumption rates in Serbia since 2012 (the first year in our observation period), are similar to findings from an Australian study, which showed a 10-fold increase in pregabalin misuse-related events in the period between 2012 and 2017, which was strongly associated with an increase in the national prescription rate of this drug.21 It is important to note that a study related to Middle East and North African (MENA) countries found that most of the gabapentinoids abuse-related events, reported for this region, were associated with pregabalin.22 Almost 20% of the patients in our study belonged to the migrant population, mostly coming from MENA countries, and all of them were using pregabalin. Interestingly, in a report from France, most of the patients who abused pregabalin were adolescents living in migrant shelters. In the same report, half of the patients who co-ingested other drugs were found to be using clonazepam.23 In general, this combination was very common in our study population, especially in abuse-related cases, nevertheless the highest frequency was observed in the subpopulation of migrants who abused pregabalin.
The association between antiepileptic drug use and increased suicide risk remains conflicting.24 Nevertheless, some studies suggest that gabapentinoid use may be associated with an increased risk of suicide.25,26 It is interesting to note that in our study, the majority of cases in the suicide-related events group were women. However, we did not have enough data to analyze this phenomenon in more detail. Our results confirmed previous findings that younger men are a vulnerable group for pregabalin abuse.27 In most of the study cases, we could not identify the source of the drug. However, some patients that abused pregabalin reported acquiring the drug on the black market, which is consistent with data from the current literature and confirms that this phenomenon also occurs in our country.28,29
Oral ingestion is the main route of administration, although other routes are possible if pregabalin is abused (intravenous injection, intranasal snorting, rectal administration etc).30 In one case in this study, a young male patient (age 28 years) took 20 capsules of pregabalin (50 mg) and snorted the entire contents because he had previously experienced that high doses of pregabalin improved his sexual function, which is consistent with some previously published case reports.31–33 Abuse of pregabalin is associated with administration of supra-therapeutic doses and more likely in combination with other psychoactive substances such as benzodiazepines, opioids, and ethanol to enhance their effects.10,14,21 We obtained the same results, although concomitant use of opioids and illicit substances (eg heroin, amphetamines, cannabis, etc) was confirmed in a relatively small number of patients (Supplementary Table 1). This can be explained by the fact that pregabalin concentration in NPCC is determined only at the request of the clinician, when it is considered clinically relevant. Performing the analysis with this protocol risks underestimating the frequency of pregabalin in acute poisonings. A study from England suggested that the number of deaths associated with gabapentinoids would be underestimated by more than 50% of cases, when the analysis was not included in laboratory toxicology screening protocol.34
In general, pregabalin did not cause severe toxicity in isolated poisoning cases in our study. Coma was recorded in 25.5% of all cases but only in four patients ingesting pregabalin only. The product summary indicates sinus bradycardia as a possible rare side effect and there are some published reports of adverse cardiac effects associated with pregabalin use and overdose cases.35–37 In our study, bradycardia was recorded in 9 cases, although most patients co-ingested drugs that may have contributed to the slow heart rate (eg β-blockers, opioids, high doses of antidepressants). In one case, a young patient with no history of cardiovascular diseases, presented with sinus bradycardia, after ingesting 750 mg of pregabalin only. Although the possibility of seizures occurring in poisoning with pregabalin has been reported in the literature, we could not associate them with pregabalin use in two patients from our study.
Concomitant ingestion of other psychoactive substances occurred more frequently and resulted in more severe poisoning. In these cases, we found a positive correlation between ingested dose and pregabalin plasma concentration with PSS score and length of hospital stay. Significantly higher doses of pregabalin were found in patients with coma, bradycardia, and hypotension and in patients who developed pneumonia during hospitalization. Higher doses were also involved in cases requiring more aggressive treatment such as administration of vasopressors, intubation, and mechanical ventilation (Supplementary Table 2). At first glance this could imply pregabalin has a dose-dependent additive effect, however more rigorous methodological approach is needed to make this claim.
Determination of pregabalin concentration is useful in making a diagnosis when the cause of poisoning is not known or the amount of the ingested drug cannot be reported. Higher pregabalin plasma concentrations were found in patients with more severe poisoning (Supplementary Table 2). Clinicians treating acutely poisoned patients should consider pregabalin concentration in the context of the time elapsed between ingestion and hospitalization, and the relatively short half-life of this drug. Together with the relatively small number of patients with analytical confirmation of pregabalin, this may be the reason why we found a better correlation of dose than concentration with the severity of poisoning.
The therapeutic plasma range is 2–8 mg/L, but steady state plasma concentration were up to 14.2 mg/L in patients maintained in daily dose of 600 mg.38 Several case reports of intentional poisoning with high pregabalin concentrations have been published.39,40 In one patient in this study, we recorded the highest pregabalin concentration reported in the literature to date – the pregabalin plasma concentration on admission was 76.16 mg/L. In cases of large ingestion and extremely high plasma concentrations of pregabalin, extracorporeal methods of drug elimination might be considered because of its pharmacokinetic properties.41 Nevertheless, this patient recovered fully after treatment with supportive measures only and was discharged from the NPCC clinic six days after admission.
Most of the study patients were treated only with symptomatic measures and the administration of intravenous fluids. In cases where mechanical ventilation was required, all patients co-ingested opioids and/or benzodiazepines. In 2019, the Food and Drug Administration (FDA) released a warning on gabapentinoids use and the risk of respiratory depression, especially when combined with other CNS depressants or in patients with impaired lung function.42
Despite the fact that the abuse potential of gabapentinoids is well recognized to date, there are still differences between countries when it comes to the legal status of these drugs. Pregabalin is classified as a Schedule V controlled substance (ie substances with the lowest potential for abuse) at the federal level in the United States, whereas there is debate about whether gabapentin should have the same status.43 In the United Kingdom, both pregabalin and gabapentin have been classified as Schedule C substances (ie the least harmful group of controlled drugs) since 2019.44 The results of a study from Saudi Arabia suggest that introduction of restriction measures on dispensing of pregabalin has led to a decline in the increasing trend in the overall consumption. The authors stated that this change may help to reduce the risk of abuse.45 To date, pregabalin and gabapentin are prescription drugs in Serbia. Based on the results of our study and the previous findings from literature, the authorities in Serbia should consider strengthening the regulatory measures for the prescription and dispensing of pregabalin, especially for the population at high risk for drug abuse.
Strengths and Limitations of the Study
The strength of this study is the use and comparison of two data sources, yet there are some limitations. The most important is the retrospective design, which has the potential for inaccuracies in data reporting and bias in risk assessment. However, only trained NPCC staff enter data into the NPCC database after a prior review by a clinical toxicologist. For the purpose of this study, all study cases were additionally reviewed by two experienced toxicologists.
For most of the cases we could not identify the source of drugs or indication when the drug was prescribed, since this data were not collected systematically in medical records. The information on ingested dose was self-reported. Finally, there is a possibility that the rates of pregabalin poisoning and abuse in Serbia are underestimated for several reasons. As mentioned earlier, analytical confirmation of poisoning cases was done in a third of all study cases, and analysis was performed when deemed necessary by the clinician. In addition, not all poisonings in Serbia are treated in NPCC, however it is a reference facility for acute poisonings and our data may reflect the frequency of poisonings and drug abuse in our country.
Conclusion
The results of our study show that the cases of poisoning and abuse of pregabalin are on the rise in Serbia. This coincided with a steady increase in overall pregabalin consumption during the study period. Although there is no evidence of widespread use, abuse and overdose of gabapentin in our country, caution and constant monitoring will be critical in the future.
Isolated ingestions of pregabalin lead to minor poisonings, but in most cases other psychoactive substances were co-ingested, resulting in more severe clinical manifestations in the poisoned patients. Clinicians and policy makers should be aware of the risk, and caution should be exercised when prescribing pregabalin to patients at risk of abuse such as socially disadvantaged populations and patients with a history of problematic substance use. Due to the growing toxicological significance of gabapentinoids, analytical laboratories should consider including them in toxicological screening protocols when feasible.
In addition to treating acute poisonings as the main task, the National Poison Control Centre in Belgrade will continue to conduct toxicovigilance, in order to prevent and reduce the possible risk for the community and to undertake appropriate and timely measures. Since data on the proportion of gabapentinoids in drug-related deaths are still not available for Serbia, future studies should be conducted to obtain a comprehensive picture of the gabapentinoid abuse in our country. Finally, this study did not aim to diminish the importance and role of gabapentinoids in clinical practice, but to raise awareness of potential risks associated with the growing trend of use of these drugs.
Acknowledgments
This work is part of the project of the Military Medical Academy Medical Faculty, University of Defense, Belgrade, Serbia (Project Number: MF VMA 06/22-24).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agree on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chincholkar M. Gabapentinoids: pharmacokinetics, pharmacodynamics and considerations for clinical practice. Br J Pain. 2020;14(2):104–114. doi:10.1177/2049463720912496
2. Kurdi A. Opioids and gabapentinoids utilisation and their related-mortality trends in the United Kingdom primary care setting, 2010–2019: a cross-national, population-based comparison study. Front Pharmacol. 2021;12:732345. doi:10.3389/fphar.2021.732345
3. Johansen ME. Gabapentinoid use in the United States 2002 through 2015. JAMA Intern Med. 2018;178(2):292–294. doi:10.1001/jamainternmed.2017.7856
4. Goodman CW, Brett AS. Gabapentin and pregabalin for pain - is increased prescribing a cause for concern? N Engl J Med. 2017;377(5):411–414. doi:10.1056/NEJMp1704633
5. Boomershine CS. Pregabalin for the management of fibromyalgia syndrome. J Pain Res. 2010;3:81–88. doi:10.2147/jpr.s7884
6. ALIMS. Home page; 2022. Available from: https://www.alims.gov.rs/english/.
7. Evoy KE, Sadrameli S, Contreras J, Covvey JR, Peckham AM, Morrison MD. Abuse and misuse of pregabalin and gabapentin: a systematic review update. Drugs. 2021;81(1):125–156. doi:10.1007/s40265-020-01432-7
8. Chiappini S, Schifano F. A decade of gabapentinoid misuse: an analysis of the European Medicines agency’s “suspected adverse drug reactions” database. CNS Drugs. 2016;30(7):647–654. doi:10.1007/s40263-016-0359-y
9. Daly C, Griffin E, Ashcroft DM, Webb RT, Perry IJ, Arensman E. Intentional drug overdose involving pregabalin and gabapentin: findings from the national self-harm registry Ireland, 2007–2015. Clin Drug Investig. 2018;38(4):373–380. doi:10.1007/s40261-017-0616-y
10. Hägg S, Jönsson AK, Ahlner J. Current evidence on abuse and misuse of gabapentinoids. Drug Saf. 2020;43(12):1235–1254. doi:10.1007/s40264-020-00985-6
11. Evoy KE, Peckham AM, Covvey JR, Tidgewell KJ. Gabapentinoid pharmacology in the context of emerging misuse liability. J Clin Pharmacol. 2021;61(Suppl 2):S89–S99. doi:10.1002/jcph.1833
12. Schifano F. Misuse and abuse of pregabalin and gabapentin: cause for concern? CNS Drugs. 2014;28(6):491–496. doi:10.1007/s40263-014-0164-4
13. Rietjens SJ, Sikma MA, Hunault CC, de Lange DW, Hondebrink L. Pregabalin poisoning: evaluation of dose-toxicity relationship. Br J Clin Pharmacol. 2022;88(3):1288–1297. doi:10.1111/bcp.15073
14. Isoardi KZ, Polkinghorne G, Harris K, Isbister GK. Pregabalin poisoning and rising recreational use: a retrospective observational series. Br J Clin Pharmacol. 2020;86(12):2435–2440. doi:10.1111/bcp.14348
15. Smith SM, Dart RC, Katz NP, et al. Classification and definition of misuse, abuse, and related events in clinical trials: ACTTION systematic review and recommendations. Pain. 2013;154(11):2287–2296. doi:10.1016/j.pain.2013.05.053
16. Persson HE, Sjöberg GK, Haines JA, Pronczuk de Garbino J. Poisoning severity score. Grading of acute poisoning. J Toxicol Clin Toxicol. 1998;36(3):205–213. doi:10.3109/15563659809028940
17. Antunovic M, Dzudovic J, Kilibarda V, Vucinic S, Djordjevic S. Validation of the rapid and simple LC-MS/MS method for the quantification of pregabalin in plasma of acutely poisoned patients. Acta Chromatographica. 2023. doi:10.1556/1326.2023.01104
18. Statistical Office of the Republic of Serbia. Home. Available from: https://www.stat.gov.rs/en-US/.
19. EMCDDA Annual Report. Annual report 2010-The State of the drugs problem in Europe 2010. State Drugs Probl Eur. Available from: http://www.emcdda.europa.eu/system/files/publications/926/EMCDDA_AR2010_EN_242720.pdf.
20. Tambon M, Ponté C, Jouanjus E, et al. Gabapentinoid abuse in France: evidence on health consequences and new points of vigilance. Front Psychiatry. 2021;12:639780. doi:10.3389/fpsyt.2021.639780
21. Crossin R, Scott D, Arunogiri S, Smith K, Dietze PM, Lubman DI. Pregabalin misuse-related ambulance attendances in Victoria, 2012–2017: characteristics of patients and attendances. Med J Aust. 2019;210(2):75–79. doi:10.5694/mja2.12036
22. Alsheikh MY, Alshahrani AM, Almutairi RD, et al. Analysis of gabapentinoids abuse-reports in the Middle East and North Africa region utilizing the Food and Drug Administration Adverse Event Reporting System. Pharmacol Toxicol Biomed Rep. 2021;7(1):5–8. doi:10.5530/ptb.2021.7.2
23. Dufayet L, Care W, Deheul S, et al. Increase in pregabalin recreational use in adolescents in France. Clin Toxicol. 2021;59(11):1027–1030. doi:10.1080/15563650.2021.18927191
24. Mula M. Suicidality and antiepileptic drugs in people with epilepsy: an update. Expert Rev Neurother. 2022;22:405–410. doi:10.1080/14737175.2022.2064744
25. Molero Y, Larsson H, D’Onofrio BM, Sharp DJ, Fazel S. Associations between gabapentinoids and suicidal behaviour, unintentional overdoses, injuries, road traffic incidents, and violent crime: population based cohort study in Sweden. BMJ. 2019;l2147. doi:10.1136/bmj.l2147
26. Patorno E. Anticonvulsant medications and the risk of suicide, attempted suicide, or violent death. JAMA. 2010;303(14):1401. doi:10.1001/jama.2010.410
27. Evoy KE, Covvey JR, Peckham AM, Ochs L, Hultgren KE. Reports of gabapentin and pregabalin abuse, misuse, dependence, or overdose: an analysis of the Food And Drug Administration Adverse Events Reporting System (FAERS). Res Social Adm Pharm. 2019;15(8):953–958. doi:10.1016/j.sapharm.2018.06.018
28. Lancia M, Gambelunghe A, Gili A, Bacci M, Aroni K, Gambelunghe C. Pregabalin abuse in combination with other drugs: monitoring among methadone patients. Front Psychiatry. 2020;10:1022. doi:10.3389/fpsyt.2019.01022
29. Schifano F, D’Offizi S, Piccione M, et al. Is there a recreational misuse potential for pregabalin? Analysis of anecdotal online reports in comparison with related gabapentin and clonazepam data. Psychother Psychosom. 2011;80(2):118–122. doi:10.1159/000321079
30. Elsayed M, Zeiss R, Gahr M, Connemann BJ, Schönfeldt-Lecuona C. Intranasal pregabalin administration: a review of the literature and the worldwide spontaneous reporting system of adverse drug reactions. Brain Sci. 2019;9(11):322. doi:10.3390/brainsci9110322
31. Osman M, Casey P. Pregabalin abuse for enhancing sexual performance: case discussion and literature review. Ir J Psychol Med. 2014;31(4):281–286. doi:10.1017/ipm.2014.41
32. Murphy R, McGuinness D, Hallahan B. Pregabalin-induced sexual disinhibition. Ir J Psychol Med. 2017;37(1):55–58. doi:10.1017/ipm.2017.5
33. Bucur M. Pregabalin and libido- case reports. Open Neuropsychopharmacol J. 2011;5(1):8–9. doi:10.2174/1876523801104010008
34. Nahar LK, Murphy KG, Paterson S. Misuse and mortality related to gabapentin and pregabalin are being under-estimated: a two-year post-mortem population study. J Anal Toxicol. 2019;43(7):564–570. doi:10.1093/jat/bkz036
35. Aksakal E, Bakirci EM, Emet M, Uzkeser M. Complete atrioventricular block due to overdose of pregabalin. Am J Emerg Med. 2012;30(9):2101.e1–2101.e21014. doi:10.1016/j.ajem.2012.02.008
36. Schiavo A, Stagnaro FM, Salzano A, et al. Pregabalin-induced first degree atrioventricular block in a young patient treated for pain from extrapulmonary tuberculosis. Monaldi Arch Chest Dis. 2017;87(3):838. doi:10.4081/monaldi.2017.838
37. Rajesh K, Jathinder K, Ihtisham M, Gordon P. Pregabalin overdose causing sinus bradycardia – a rare complication. J Cardiovasc Med Cardiol. 2021;007–009. doi:10.17352/2455-2976.000160
38. Patsalos PN, Spencer EP, Berry DJ. Therapeutic drug monitoring of antiepileptic drugs in epilepsy: a 2018 update. Ther Drug Monit. 2018;40(5):526–548. doi:10.1097/FTD.0000000000000546
39. Wood DM, Berry DJ, Glover G, Eastwood J, Dargan PI. Significant pregabalin toxicity managed with supportive care alone. J Med Toxicol. 2010;6(4):435–437. doi:10.1007/s13181-010-0052-3
40. Braga AJ, Chidley K. Self-poisoning with lamotrigine and pregabalin. Anaesthesia. 2007;62(5):524–527. doi:10.1111/j.1365-2044.2006.04913.x
41. Bouchard J, Yates C, Calello DP, et al. Extracorporeal treatment for gabapentin and pregabalin poisoning: systematic review and recommendations from the EXTRIP workgroup. Am J Kidney Dis. 2022;79(1):88–104. doi:10.1053/j.ajkd.2021.06.027
42. FDA, DSC. FDA Warns About Serious Breathing Problems with Seizure and Nerve Pain Medicines Gabapentin (Neurontin, Gralise, Horizant) and Pregabalin (Lyrica, Lyrica CR). United States: FDA; 2019.
43. Peckham AM, Ananickal MJ, Sclar DA. Gabapentin use, abuse, and the US opioid epidemic: the case for reclassification as a controlled substance and the need for pharmacovigilance. Risk Manag Healthc Policy. 2018;11:109–116. doi:10.2147/RMHP.S168504
44. Torjesen I. Pregabalin and gabapentin: what impact will reclassification have on doctors and patients? BMJ. 2019;364:l1107. doi:10.1136/bmj.l1107
45. Althunian TA, Alomran MI, Alsagri GM, Alrasheed MM, Alshammari TM. The impact of regulatory restrictions on pregabalin use in Saudi Arabia: an interrupted time series analysis. Pharmacoepidemiol Drug Saf. 2022;31(5):577–582. doi:10.1002/pds.5408
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.