Back to Journals » ImmunoTargets and Therapy » Volume 13
Revolutionizing Immunotherapy: Unveiling New Horizons, Confronting Challenges, and Navigating Therapeutic Frontiers in CAR-T Cell-Based Gene Therapies
Authors Srivastava S, Tyagi A ![]() , Pawar VA, Khan NH
, Pawar VA, Khan NH ![]() , Arora K, Verma C
, Arora K, Verma C ![]() , Kumar V
, Kumar V ![]()
Received 11 May 2024
Accepted for publication 20 August 2024
Published 27 August 2024 Volume 2024:13 Pages 413—433
DOI https://doi.org/10.2147/ITT.S474659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Shivani Srivastava,1,* Anuradha Tyagi,2,* Vishakha Anand Pawar,3,* Nawaid Hussain Khan,4,* Kavita Arora,5,6 Chaitenya Verma,7,8 Vinay Kumar9
1Department of Pathology, School of Medicine, Yale University, New Haven, CT, USA; 2Department of cBRN, Institute of Nuclear Medicine and Allied Science, Delhi, India; 3The University of Texas MD Anderson Cancer Center, Houston, TX, USA; 4Faculty of Medicine, Ala-Too International University, Bishkek, Kyrgyz Republic; 5Advanced Instrumentation Research Facility, Jawaharlal Nehru University, New Delhi, India; 6School of Computational & Integrative Sciences, Jawaharlal Nehru University, New Delhi, India; 7Department of Pathology, Wexner Medical Center, Ohio State University, Columbus, OH, USA; 8Department of Biotechnology, SSET, Sharda University, Greater Noida, 201306, India; 9Pennsylvania State University Hershey Medical Center, 500 University Dr, Heshey, PA, USA
*These authors contributed equally to this work
Correspondence: Chaitenya Verma; Vinay Kumar, Email [email protected]; [email protected]
Abstract: The CAR-T cell therapy has marked the dawn of new era in the cancer therapeutics and cell engineering techniques. The review emphasizes on the challenges that obstruct the therapeutic efficiency caused by cell toxicities, immunosuppressive tumor environment, and decreased T cell infiltration. In the interest of achieving the overall survival (OS) and event-free survival (EFS) of patients, the conceptual background of potential target selection and various CAR-T cell design techniques are described which can minimize the off-target effects, reduce toxicity, and thus increase the resilience of CAR-T cell treatment in the haematological malignancies as well as in solid tumors. Furthermore, it delves into cutting-edge technologies like gene editing and synthetic biology, providing new opportunities to enhance the functionality of CAR-T cells and overcome mechanisms of immune evasion. This review provides a comprehensive understanding of the complex and diverse aspects of CAR-T cell-based gene treatments, including both scientific and clinical aspects. By effectively addressing the obstacles and utilizing the capabilities of cutting-edge technology, CAR-T cell therapy shows potential in fundamentally changing immunotherapy and reshaping the approach to cancer treatment.
Keywords: CAR-T cells, immune checkpoint inhibitors, gene therapies, gene editing, predictive biomarkers
Introduction
Chimeric Antigen Receptor (CAR)-T cell therapies have emerged as a viable strategy for the treatment of many forms of cancer. CAR-T cell therapy is categorized as an ex vivo gene therapy, wherein the patient’s T cells are genetically altered outside the body prior to reinfusion into the patient’s system, with the purpose of specifically targeting and eliminating cancer cells.1 This process enhances the immune system’s effectiveness in fighting against the disease.2 The efficacy of CAR-T cell therapy has facilitated the progress of other advanced therapy medical goods, showcasing the potential of gene therapy in the treatment of diverse disorders.3 The clinical studies of this groundbreaking therapy have demonstrated exceptional efficacy, especially in patients with hematologic malignancies.4 In addition, CAR-T cell therapy has demonstrated potential in the treatment of hematological malignancies, specifically B cell malignancies such relapsed or refractory diffuse large B cell lymphoma (DLBCL).5 The therapy possesses the capacity to produce enduring remission and potentially even eradicate specific forms of cancer, thereby presenting a newfound sense of optimism for patients with few treatment alternatives. The emergence of CAR-T cell treatments signifies a notable progression in the realm of cancer treatment, holding the capacity to fundamentally transform our approach to and control of the disease. CAR-T cell therapies utilize the immune system and genetic engineering to provide a customized and focused method for treating cancer, overcoming the constraints of conventional treatments.2 Moreover, the effectiveness of the therapy in addressing blood cancers has opened up possibilities for investigating its use in solid tumors, which pose a more intricate difficulty due to the diverse conditions within the tumor and its surroundings.4 This therapy seeks to augment the effectiveness of CAR-T cells by modifying the tumor microenvironment through the use of tumor-targeting nanozymes. These nanozymes have the ability to boost immune activation and improve the overall therapeutic efficacy of the treatment.6 Nevertheless, the broad implementation of CAR-T cell treatment is hindered by notable barriers, including immunity-related side events and prognostic heterogeneity.7 These tasks involve the management of potential negative effects like cytokine release syndrome and neurotoxicity, the improvement of manufacturing methods to guarantee consistent and high-quality cell products, and the resolution of the high cost and limited availability of these advanced medicines.2 Despite these obstacles, CAR-T cell therapy has exhibited notable advancements in the treatment of liquid malignancies, with a complete remission rate above 57%.8 Within the realm of gene therapy, CAR-T cell therapy signifies a notable progression in the discipline. Furthermore, current research is concentrated on improving the effectiveness of CAR-T cell therapy in solid tumors, addressing the immunosuppressive mechanisms present in the tumor microenvironment, and devising techniques to counteract antigen escape and tumor relapse.4 CAR-T cell therapy, utilized in oncology, may treat autoimmune diseases. CAR-T cells targeting specific antigens show potential in systemic lupus erythematosus.9 In 2021, CAR-T therapy helped SLE patients achieve sustained remission. This therapy targets and depletes autoreactive B cells, where traditional treatments fail. Successful treatment of SLE implies implications in other autoimmune disorders, a major therapeutic development.10 Figure 1 represents the significant discoveries in the field of CAR-T cell therapies.
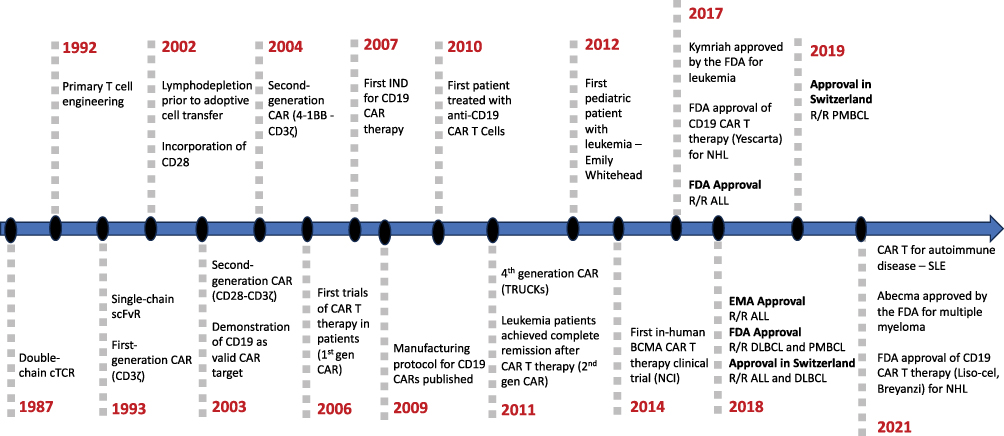 |
Figure 1 Timeline of the development of CAR-T cell therapies. |
Emerging Targets for CAR-T Cell Therapy and Next-Generation CAR-T Engineering
The immunotherapies centered on the application of triggered and genetically persuaded T cells have transfigured the area of superior precision targeting in cancer treatment. Among the various forms of T cell transfer strategies, the CAR-T cells provoke an intention of targeting cell death with the help of single-chain variable fragment (scFv) that aim at tumors.11 This strategy causes the abolition of supposedly indistinguishable malignant cells, thereby resulting in tremendous improvements in cancer subjects.12 CAR-T cells possess the capability of navigating the T cell specificity towards the antigens by means of fusing the binding domains of antibodies towards T cell CD3-like signaling proteins.13 CAR-T cell immunotherapy, notably with the use of anti-CD19 CAR-T cells, has been proven to be effective in treating various hematological cancers.14 At present, American and European Drug Agencies (Food and Drugs Administration and European Medicines Agency) have permitted four distinctive CD19-targeting, as well as one BCMA-targeting CAR-T product, respectively.15,16 These treatments are implemented to cure abnormal B cell malignancies.17–19
In the field of leukemia, targeting CD19 was efficacious because of the effortless approachability to cancerous targets as well as the uniform expression of CD19 on the expendable population of B cells. In 2017, US FDA approved Kymriah™ (Tisagenlecleucel) and Tecartus™ (Brexucabtagene autoleucel), the first cell-based therapeutic treatment in the form of CD19-targeted CAR-T cells against B cell malignancies.20 Despite its terrific attainments in B cell malignancies, the immune-refereed toxicities inside the TME can cause morbidity and mortality, which sublimit the prevalent use of this therapy in solid tumors. One of the barriers is linked through the loss of tumor-associated antigens (TAAs).21 In 1993, Eshhar described the earliest CARs, which were comprised of scFv joined solitary to the CD3 complex. These “first generation” CAR-T cells proliferated poorly and were unable to facilitate complete tumor remission. Eventually, CAR-T schemes involved the merging of the scFv to a T cell receptor (TCR) domain, CD28 or CD137 Endo domains.14 An assimilation of costimulatory domains with the CD3ξ signaling tail circumvents the requisite for outward primary and secondary commencement indicators, which begin cytotoxicity and cytokine emission upon T cell engagement.11,14,21 The finest molecular strategies of the CARs can be accomplished by the virtue of conceivable variability of modular protein domain constituents. Over the period, the evolution in protein engineering of CARs caused significant improvements in its designs with respect to adaptation in the ectodomain, transmembrane domain, linker and hinge regions for better efficacy at treating various cancers.22
Despite attaining the beneficial stimulatory effects in the patients of various malignancies, the application of CAR-T therapy could not be achieved in a wider range of treatments due to its associated toxicity, safety issues and obstructed programmability.23–26 These limitations can be relieved by means of engineering strategies to build better CAR-T cells by implanting array of antigen detection capabilities and engineering adaptor reliant approaches.25 CAR protein expression can be regulated with the help of protease-based apparatuses. A protease merged to the CAR severs the target spot in cis position to detach a degron. This process brings stability to the structure of a CAR protein, which leads to the ON state of its expression.27,28 Whereas the presence of the protease inhibitor foils elimination of degron, that initiates CAR degradation and switches OFF the system.28,29 The CAR protein can be divided into two domains.21
To acquire the complete functionality of CAR-T activity, dimerizing remedies are required. Its activity and specificity can be coordinated with the help of diverse protein toggles. For example, the switchable CARs (sCARs) hold a bi-orthogonal tag, like peptide neoepitope (PNE), that can be steered to tumor antigens by supplementing an antigen-binding fragment exclusively for a tumor antigen.30 The synthetic Notch receptor method involves identification of numerous TAAs to stimulate CAR-T system.31 The attachment of an antigen causes structural modification in the synNotch receptor that triggers the delivery of transcription factor to initiate expression of another antigen of interest with respect to CAR protein.32 The inhibitory CAR (iCAR) technique obliges detection of a TAA in the absenteeism of a healthy-tissue antigen to gain necessary CAR-T cell stimulation.33 Fei et al evaluated a PD-1-founded anti-HLA-DR iCAR, which regulated inhibition of NK cells against HLA-DR expression for various malignancies.34 Zhang et al reported the development of a novel BAFF-R CAR-T cell product based on single-domain antibody.35 Bangayan et al developed a dual-inhibitory domain CAR (DiCAR) that integrates two immune cell inhibitory signaling domains to selectively control CAR-T cell cytotoxicity and enhance inhibition effectiveness in comparison to an iCAR containing only a single PD1 domain.36 The tandem bispecific CARs involve dual extracellular antigen-binding domains.37 The broad TAA specificity biotinylated epitopes can be targeted with the help of Universal adaptor receptors. Here, distinctive antibodies or the adaptor molecules of antigen-binding system can be dispensed to readdress specificity of CAR-T cell.38–40
To elevate the plasticity of CARs, a split, universal, and programmable (SUPRA) CAR method was developed.41 It constitutes two modules that harbor a universal receptor along with leucine zipper adaptor (zipCAR) expressed on T cells. It also contains a distinct scFv associated with leucine zipper adaptor molecule (zipFv).42 To enhance the safety aspect of CAR-T cell system, the T cell incidence as well as expression of CAR can be controlled using various methods. The dimerizing drugs elicit downstream signaling pathways to stimulate apoptosis.43 The truncated epidermal growth factor receptor serves as the suicide tag when expressed simultaneously on the CAR-T cell.44 Upon administration of antibodies, like cetuximab, the exclusive epitope identifier generates in-house antibody-dependent cell-mediated cytotoxicity (ADCC) and complement-dependent cytotoxicity (CDC) apparatuses to produce CAR-T cell apoptosis.45 To abolish CAR-T cells, the interruption of DNA synthesis can be achieved by means of CAR-T cells tagged with herpes simplex virus thymidine kinase (HSV-TK), which possess the capacity of transforming ganciclovir into a cytotoxic molecule.46,47
Combination Immunotherapies: Synergizing CAR-T with Checkpoint Inhibitors
Combining CAR-T cell therapy with immune checkpoint inhibitors is being researched in order to improve the efficacy of CAR-T cell treatments and overcome their limitations. Targeting non-solid tumors has proven to be successful for CAR-T cell therapy; however, its efficacy against solid tumors is restricted. Furthermore, questions concerning long-term impacts and safety still exist. Checkpoint inhibitors, including PD-1/PD-L1 blockade, have been approved for use in a variety of solid tumors and have revolutionized the treatment of cancer. While some combinations of checkpoint inhibitors and targeted therapy have shown synergistic effects, not all of these combinations have proven to be effective. Research has demonstrated that the use of checkpoint inhibitors in combination with targeted drugs such as PARP inhibitors, EGFR/HER2 inhibitors, and angiogenesis inhibitors can enhance clinical results. In preclinical models, combining checkpoint inhibitors with CAR-T cell therapy showed potential in improving T cell infiltration and intra-tumoral performance. Checkpoint inhibitors have demonstrated encouraging preclinical evidence in cancer immunotherapy.48–50 These inhibitors, such as PD-1/PD-L1 and LAG-3, have been validated as targets in oncology and have shown efficacy in varied tumor types.51 Small-molecule PD-L1 inhibitors have been developed with a novel mechanism of action, favorable pharmacokinetics, and in vivo efficacy in mice models. Combination therapy with checkpoint inhibitors has been showed to improve antitumor activity when compared to individual blockade of receptors. Preclinical studies show that blocking the interaction between LAG-3 and its ligands can reverse LAG-3-mediated suppression of T cell function. These findings offer a biological rationale for combining LAG-3 inhibitors with other checkpoint inhibitors as an efficient cancer immunotherapy strategy. Additionally, positive results from clinical studies have been observed in patients with advanced cancers seeing better progression-free survival when CAR-T cell therapy and immune checkpoint inhibitors are combined.52
The complimentary mechanisms of action of these therapies provide a rationale for this approach. Immune checkpoint inhibitors strengthen the immune system’s defense against cancer, while CAR-T cell therapy directly targets cancer cells. Preclinical research has shown the advantages of this combination, such as decreased tumor burden, increased objective response rate, and enhanced long-term protection.53 NK cells created with CARs have benefits over CAR-T cells in terms of specific killing, cell source, and efficiency against solid tumors.54 Immune checkpoint inhibitors, which are used in cancer treatment, may influence the function of CAR-NK cell therapy.55 Furthermore, combining CAR-T cell therapy with immune checkpoint inhibitors has demonstrated promise for boosting CAR-T cell function, antitumor effects, and minimizing toxicity in patients with lymphoid B cell malignancies.56 Additionally, in metastatic clear cell renal cell carcinoma, the combination of cabozantinib, an inhibitor of the VEGF-VEGFR and Gas6-AXL/TYRO3/MER (TAM) axes, with PD1 inhibitors showed synergistic antitumor activity.57 Preclinical evidence of their synergistic interaction is driving research into the integrating of immune checkpoint inhibitors and radiotherapy for the treatment of advanced or metastatic solid cancers.
The T cell infiltrates developed during various cancerous stages are capable of determining the diagnosis, the disease progression and the anticipation of clinical response to respective immunotherapies. In this regard, various subsets of T cells such as NKT cells, γδT cells and mucosa-associated invariant T cells (MAITs) have exhibited encouraging results.58–60 The NKT cell subsets consist of a Type I: Vα14Jα18 invariant TCR α-chain, which identifies the glycosphingolipid α-galactosylceramide (α-GalCer) and correlates via CD1d molecules, and type II: non-α-GalCer molecules. The Type I-NKT cells secret IFN-γ and TNF-α enhance the antitumor effect and modulate the tumor niche.61 Heczey et al produced anti-GD2 CAR-NK T cells that showcased higher tumor infiltration capacity that regulated better tumor regression response minus dose-limiting toxicities.62 MAIT, another contender for CAR-T cells, has shown excellent expression of the Vα7.2–Jα33 invariant TCR α-chain that can perfoliate solid tumours.63 Mikail et al developed anti-Her2 CAR-MAIT that showed higher efficiency against breast tumors and also B cell lymphoma.64,65 The γδT cell subset is characterized by γδT cell receptors that are not MHC restricted. It holds the potential to cure solid tumor with less graft-versus-host disease (GvHD) risk. In addition, their capability to direct antigen-independent cytotoxicity restricts the getaway of heterogeneous tumour cells.66,67
Checkpoint inhibitors have demonstrated efficacy in many clinical trials when used with standard of care chemotherapy for diverse types of malignancies. Possible synergistic mechanisms include immunogenic tumor cell death, anti-angiogenesis, selective depletion of myeloid immunosuppressive cells, and lymphopenia. Lymphopenia reduces regulatory T cells and generates room for effector T cell growth.68 However, the complicated tumor microenvironment (TME) and the dearth of preclinical models that can replicate this complexity have made the use of CAR-T cell therapy in solid tumors difficult. Combining CAR-T therapy with checkpoint inhibitors, such γδT cells treatment, may enhance infiltration and efficacy in solid tumors, according to recent preclinical findings.69 Clinical trials have demonstrated the promise of combining immune checkpoint inhibitors (ICIs) with CAR-T cell treatment. By overcoming immunosuppression and modulating immune responses in the tumor microenvironment, the synergy of CAR-T cells with ICIs can improve the therapeutic outcomes of CAR-T cell therapy.70 These findings emphasize the combinatorial approach’s potential to improve cancer treatment efficacy and serve as a basis for future research and development in this field. Nevertheless, additional investigation is required to maximize the efficacious combination of checkpoint inhibitors and CAR-T cells for cancer therapy.
CAR-T in Solid Tumor Therapy: Progress and Hurdles
CAR-T cell therapy has proven exceptional success in hematological malignancies, but solid tumors present unique obstacles. The immunosuppressive tumor microenvironment (TME), insufficient tumor infiltration, and unreliable tumor-specific antigens are the main barriers.71–73 Hypoxic cores, aberrant vascularization, and increased reactive oxygen species in solid tumors prevent CAR-T cell trafficking and infiltration.74,75 Tumor antigens are heterogeneously expressed and present in healthy tissues, making target antigen selection difficult.76 Additionally, antigen escape, which refers to tumor cells that fail to express the antigen, and heterogeneity resulting from the expression of different tumor-associated antigens (TAAs) in solid cancers serve as challenge. On-target/off-tumor toxicity occurs when antigens are strongly expressed in both healthy cells and tumor cells.77,78 To address this, researchers are looking into bystander effects, such as antigen spreading, when CAR-T cells activate other CD8 T cells against non-targeted antigens.79 Innovative models, such as solid tumor-on-chip, have been developing to predict the safety and efficacy of CAR-T cell therapy in clinical settings.72 In addition to lack of reliable tumor-associated antigens, solid tumors also present challenges such as an immunosuppressive tumor environment and decreased T cell infiltration.75 The efficacy of CAR-T therapy in solid tumors is restricted by immunosuppressive tumor environments and a deficiency of reliable tumor-associated antigens.72 The intricate microenvironments of solid tumors prevent CAR-T cells from infiltrating and functioning.73 In order to address these issues, scientists are investigating into methods like using chemokine receptors to increase the functioning and specificity of CAR-T cells, combining immune checkpoint inhibitors, and developing cost-effective, tumor microenvironment-specific CAR-T cells.75 Additional immune cells, including macrophages and NK cells, are also being researched as potential alternatives for solid tumor immunotherapy.74 CAR-T therapy with radiation can also improve the TME and expand CAR-T cells.80 Moreover, CAR-NK and CAR-M cells may have clinical benefits, including decreased toxicity and better infiltration.81 Moreover, efforts are being explored to promote tumor infiltration and boost anticancer efficaciousness through the regional administration of CAR-T cells via hydrogel platforms.71 Despite these efforts, CAR-T cells typically exhibit exhaustion and need combo therapies like PD-1 blocking to persist and anti-tumor activity. CAR-T cell therapy for solid tumors is difficult, but new approaches may make it more effective. Figure 2 depicts a typical image illustrating the obstacles faced by CAR-T cell therapy when targeting solid tumors.
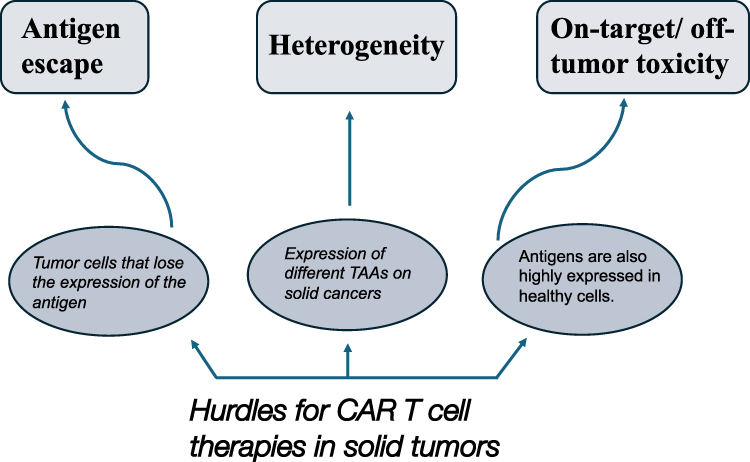 |
Figure 2 Image illustrating the obstacles faced by CAR-T cell therapy when targeting solid tumors. |
Overcoming the above-mentioned limitations requires discovering reliable tumor-associated antigens as well as developing tumor microenvironment-specific CAR-T cells.73 Molecular imaging and cell tracking can provide light on the therapeutic hurdles associated with solid tumors while also aiding in the effective delivery of CAR-T cells. Overall, more investigation and development are required to maximize the success of CAR-T cell therapy in treating solid tumors, even though it has demonstrated promise in treating hematological cancers. Furthermore, axicabtagene ciloleucel and tisagenlecleucel, two CAR T-cell therapies for relapsed or refractory B-cell lymphomas, have significantly boosted cure rates.82 However, real-world application differ greatly from randomized controlled trials (RCTs). RCTs, the gold standard for therapy efficacy evaluation, generally use highly selected patient populations that do not fully represent routine clinical practice’s more diverse patient demographics.83,84 For instance, real-world patients are older, have more comorbidities, and have worse functional status than trial participants, which can affect clinical outcomes.85,86 Real-world evidence (RWE) from electronic health records and disease registries serves to fill this gap by revealing CAR T-cell therapies’ safety, effectiveness, and wider application in more heterogeneous populations of patients.87 Real-world data can validate RCT efficacy, as proven by German claims data resembling CHAARTED trial outcomes in metastatic hormone-sensitive prostate cancer.88 Moreover, real-world studies have shown the viability and limitations of CAR T-cell therapy in trial-ineligible patients, emphasizing the necessity to address side effects like cytokine release syndrome and neurotoxicity.89,90 RWE must evolve to evaluate and optimize CAR T-cell therapies to fulfill the demands of a broader population of patients and handle regulatory and economic constraints.91 Thus, RWE and RCT data must be integrated to improve CAR T-cell therapy and patient outcomes in real-world. Table 1 summarizes the aggregation of clinical trials progress on CAR-T Cell Immunotherapy.
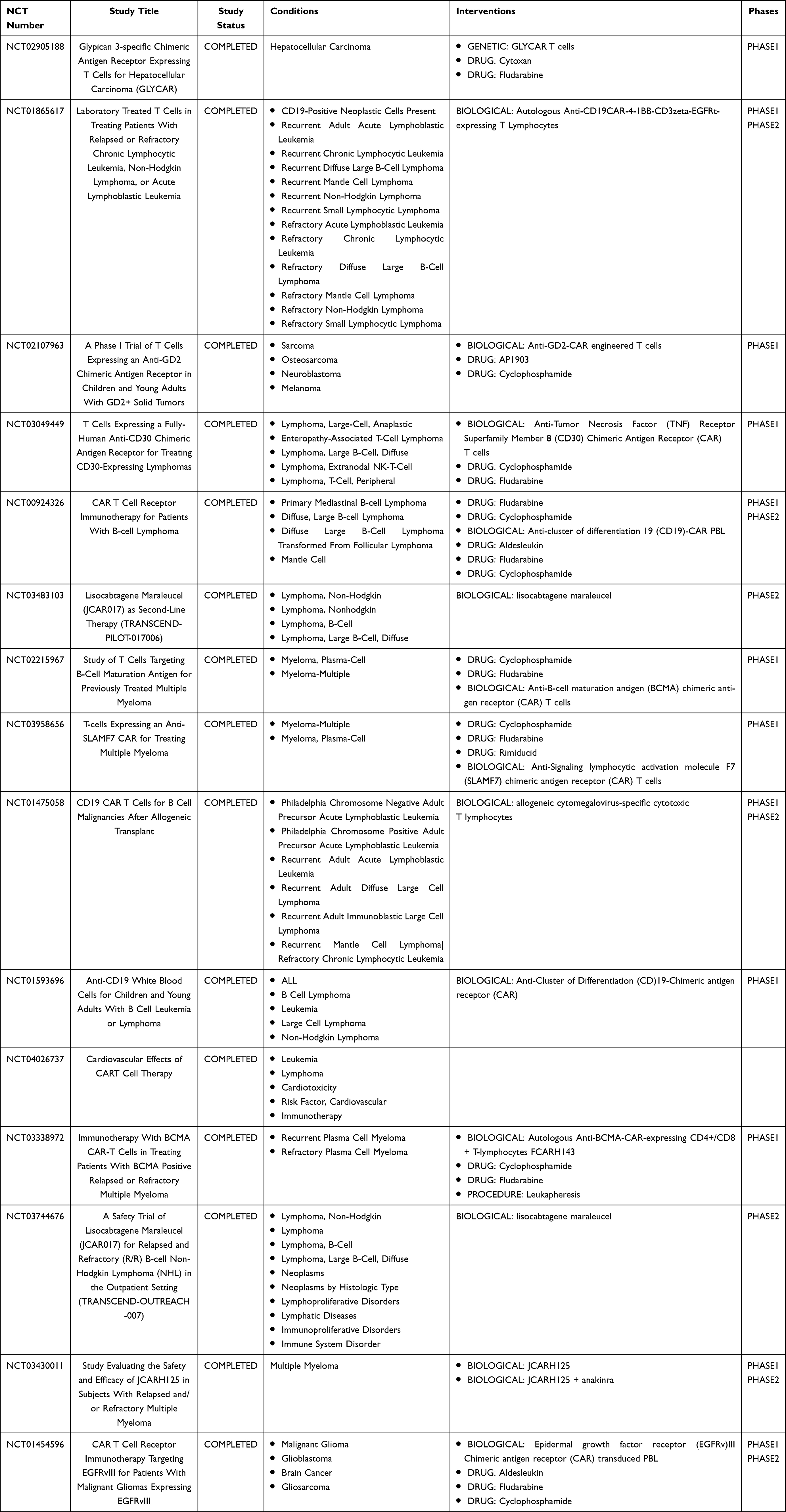 |
Table 1 Compilation of Clinical Trial Status on CAR-T Cell Immunotherapy (Information Based on Study Records Available on “Clinicaltrials.gov”) |
Gene Editing Technologies in CAR-T: CRISPR and Beyond
Gene editing technologies, such as CRISPR-Cas9, have shown potential in improving CAR-T cell therapy by providing targeted modifications to genes for enhanced efficacy and durability.92–94 Conventional gene editing tools based on nuclease activity, such as CRISPR-Cas9, can cause undesired genomic alterations and genotoxicity. The Pin-point™ base editing technology uses modular RNA aptamers to achieve high editing efficiency and purity at target sites, resulting in reduced chromosomal translocations.95 CRISPR-based gene editing and screening have enabled the direct genomic manipulation of immune cells, contributing to the discovery of novel factors that reprogram and regulate immune responses.96 Non-viral CRISPR/Cas9 nano-formulations were developed as well to improve the safety, efficiency, and specificity of cancer gene editing. Furthermore, precision genome engineering techniques like Cas9 RNP-mediated gene editing have been employed to produce PD-1-deficient CAR-T cells, resulting in greater tumor cell killing and improved CAR-T cell immunotherapy efficacy.
However, recent gene editing tools like Base and Prime Editing minimize the risk of harmful events, but their ability to make edits is limited.97 High-frequency gene editing in primary immune cells, including T cells, has been demonstrated by novel gene-editing systems based on metagenomic data, with insignificant impact on cell viability.95 CRISPR-Cas9 technology can be applied to engineer allogeneic CAR-T cells, target inhibitors of T lymphocyte function, and maximize the efficacy and safety of CAR-T therapy.98 These developments in gene editing technology could enhance CAR-T immunotherapy’s effectiveness, safety, and accessibility for the treatment of different cancers.
For CAR-T cell therapy, CRISPR-Cas9 technology has several advantages. Effective and controllable genetic modification has become possible, enabling the knockout of genes that inhibit T cell function and the regulation of CAR-T cell activity within the tumor microenvironment.99,100 Multiple T cell exhaustion pathways can be targeted simultaneously using CRISPR-Cas9, resulting in CAR-T cells with increased effector activity and enhanced tumor cell killing.101 Furthermore, CRISPR-Cas9 can be applied to effective gene silencing and non-viral gene transfer, minimizing the possibility of genomic rearrangements, and facilitating the development of safer and more potent CAR-T cell therapies.102,103 However, using CRISPR-Cas9 for CAR-T cell therapy has several drawbacks as well. During the genome editing process, off-target effects, such as unexpected genetic modifications, might happen. The safety and potential long-term repercussions of CRISPR-edited CAR-T cells are called questionable by this. It is imperative to cautiously analyze and tackle these possible limitations to ensure the efficaciousness, safety, and accessibility of CRISPR-edited CAR-T cell therapies.
Biomarkers and Predictive Indicators Associated with Response to CAR-T Cell Therapies
Genetically manipulated allogeneic and autologous CAR-T cell therapy has been one of the most promising immunotherapies for cancer treatment, particularly in hematological malignancies of the current decade. Seven CAR-T cell immunotherapies have been approved by the FDA for treating lymphocytic leukemia, including B cell malignancies and multiple myeloma. Tisagenlecleucel (Kymriah®), an anti-CD19 CAR-T cell therapy, was the first FDA-approved treatment for B cell precursor acute lymphoblastic leukemia patients with evidence of non-response to conventional therapy or who had relapsed more than twice.104–106 Subsequently, four more axicabtagene ciloleucel (Yescarta®), brexucabtagene autoleucel (Tecartus®), lisocabtagene maraleucel (Breyanzi®), and relmacabtagene autoleucel (Relma-cel; brand name Carteyva® in China only) CD19-specific CAR-T cell therapies for the treatment of various B cell malignancies were approved. Later, idecabtagene vicleucel (Abecma™) and ciltacabtagene autoleucel (Carvykti®), BCMA-specific CAR-T cell therapies for multiple myeloma, were also approved in February 2022.105,107–110
The recent advancements and ongoing improvement of CAR-T therapies arose as a potent method for treating hematological malignancies.111 The treatment of B-cell acute lymphoblastic leukemia (B-ALL) with CD19 CAR-T cells showed tremendous efficacy, with a complete remission of 70–90%.18,112 However, several obstacles are still present to hinder the treatment outcomes and utility of CAR-T cell therapy, including life-threatening CAR-T cell-associated toxicities, inhibition and resistance in B cell malignancies, limited efficacy against solid tumors, antigen escape, poor trafficking, limited persistence, infiltration, and the immunosuppressive microenvironment. Biomarkers could play a prime role in personalized cancer care regarding the prediction of CAR-T-related toxicity, efficacy, and relapse of CAR-T therapy. It is crucial to prioritize the development of new biomarkers and the validation of current ones in order to incorporate them into cancer care practice. In order to make CAR-T cell treatment more widely available to a larger number of patients, it is crucial to speed up the clinical implementation of modified CAR-T products and personalized management strategies.
Predictive Biomarkers for Therapeutic Response in CAR-T Cell Therapy
The principal goal of cancer treatment is the overall survival (OS) and event-free survival (EFS) of patients. There is an urgent need for feasible predictive biomarkers for long-term and short-term CAR-T therapy outcomes. Several studies reported that patients’ baseline characteristics, T cell functionality of constructed CAR-T cells, and minimal residual diseases post-CAR-T therapy could be strongly associated with therapeutic response. Prior to CAR-T therapy, various patient-related factors, including gender, age, treatment history, p53 status, tumor burden, immunoglobulin heavy chain variable region gene IGH variable (IGHV) mutation status, and chromosome 17p deletions, were found to have no significant correlation with the response to CAR-T cell therapy.17,113–115 Some studies have found no direct effect of these factors on therapeutic outcomes, whereas others imply potential indirect effects or within specific subgroups. TP53 mutations are linked to poor prognosis and therapy resistance in lymphomas such as DLBCL and B-ALL.116,117 In DLBCL, TP53 mutations were associated with inferior complete response (CR) and overall survival (OS) rates, suggesting that TP53 status could be a useful biomarker for CAR-T risk stratification.118 In another study, TP53 mutation status did not significantly affect outcomes in DLBCL patients treated with CAR-T cells, emphasizing the need for bigger cohort validation.119 Age and gender also have conflicting results. Some studies reported no significant impact on leukemia-free survival (LFS) and OS in B-ALL patients treated with CAR-T cells, while others suggested that older age could be associated with less favorable outcomes due to higher toxicity and lesser efficacy.120,121 For high tumor burden patients, dose fractionation of CAR-T cells is recommended to reduce toxicity, indirectly suggesting that patient-specific factors like tumor burden may affect therapeutic outcomes.122 CAR-T cell kinetics, which vary by patient and tumor type, may also affect therapeutic efficacy and toxicity.123 Thus, a more nuanced discussion that takes into account these contradicting evidences would provide a balanced view, noting that some patient-related factors may not have a direct correlation but may still affect CAR-T therapy outcomes in specific contexts or subgroups.
Elevated levels of serum LDH (lactate dehydrogenase) have been observed in cancer patients; this could be associated with high tumor burden, proliferation in B cell malignancies, and disease progression. The increased serum LDH levels were correlated with a poor prognosis and a negative therapeutic outcome in most cancer patients.124 Serum LDH levels in CAR-T therapy could be a potentially negative prognostic biomarker in cancer. An investigation conducted on adult patients with B-ALL indicated that a decreased pre-lymphodepletion LDH level and an elevated platelet count were distinct factors linked to improved EFS. Furthermore, it has been proposed that patients exhibiting elevated pre-lymphodepletion LDH levels and a decreased platelet count may necessitate systemic treatment prior to CAR-T cell infusion. However, LDH levels are not directly linked to the immune system, making them less promising for predictive biomarkers for CAR-T therapy responses.125 In non-small cell lung cancer (NSCLC) and large B cell lymphoma, serum LDH levels have been associated with treatment response and overall survival.126,127 In CAR T cell therapy, LDH levels are critical to assessing treatment response, although they have limited effect on the immune system.128 Combining LDH levels with additional biomarkers like carcinoembryonic antigen (CEA) can help predict clinical outcomes and guide treatment decisions in CAR T cell therapy patients.129 Routine monitoring of LDH levels can improve early therapy response assessment and patient outcomes in immune-related therapies like CAR T cell therapy. It was observed that elevated CRP at baseline was associated with poor treatment outcomes of CAR-T therapy, and the presence of circulating tumor DNA (ctDNA) in peripheral blood samples at the first week of CAR-T infusion was also correlated with poor response to CAR-T therapy. Both baseline CRP and the presence of ctDNA during the initial stage of CAR-T cell therapy could be reliable predictive biomarkers for CAR-T therapy response.130,131 A study conducted in B-ALL and B cell non-Hodgkin lymphoma (NHL) patients with CAR19/22-T cell therapy reported that macrophage inflammatory protein (MIP)-3α is a highly sensitive and specific prognostic predictor for non-response (NR) and early relapse (ER) to therapies. Extensive clinical validation of biomarkers like CD19 has led to their successful use in CAR T-cell therapies for B-cell malignancies.132 GPC3 and TGF-b have been quantified using advanced image analysis in preclinical models and demonstrate high correlation with pathologist assessment, suggesting a robust preclinical validation stage.133 CAR T-cell detection and quantification technologies including flow cytometry and quantitative PCR are well-established, but study application varies, affecting comparability and reproducibility.134 Despite advances like droplet digital PCR, NanoString, and single-cell RNA sequencing, detection timepoint and frequency remain a challenge.134,135 Reproducibility across studies and clinical trials requires standardized reporting and validation protocols.136,137 In addition, molecular assays and imaging technologies for in vivo CAR T-cell tracking and visualization are improving, but they need thorough validation to prove their clinical utility.138 Some biomarkers and detection technologies are well-validated, but others are still in preclinical or early clinical trials, requiring more research to demonstrate their reliability and reproducibility.
Patients with higher MIP3α levels after sequential CAR19/22 T cell infusion had much better progression-free survival (PFS) outcomes than patients with lower MIP3α levels. This study suggested that MIP3α could be a promising prognostic biomarker for the post-CAR-T therapy treatment response in terms of a prognostic predictor for NR/ER to therapies.139 Researchers had reported that the epigenetic characteristics of leukemia cells, such as hypermethylation of DNA, a stem cell-like phenotype and inherent plasticity, and decreased antigen presentation, were independent of CD19 status, and the leukemia subtype could be playing a crucial role in developing resistance to CAR-T therapy in AL patients. Moreover, the epigenetic status of leukemia cells may be used as a potential early predictive biomarker for resistance to CAR-T cell therapy.140,141 It was observed that significantly higher numbers of “exhausted” T cells (differentiated CD3+CD27-CD28-T cells) in lymphoma patients were associated with a low response to CAR-T cell therapy. Therefore, the low frequency of “exhausted” T at leukapheresis could be a potential pre-infusion predictive biomarker for the responsiveness of CAR-T cell therapy.142 In solid tumors, exhausted T cells with inhibitory receptors such as PD-1, LAG-3, and TIM-3 prevent CAR-T cell therapy. These markers are associated with reduced proliferative capacity, impaired anti-tumor activity, and attenuated persistence of CAR-T cells.143 Chronic antigen stimulation and the immunosuppressive tumor microenvironment (TME) cause substantial transcriptional, epigenetic, and metabolic reprogramming, exhausting T cells.144,145 For instance, PD-1, LAG-3, and TIM-3 are highly expressed in tumor-infiltrating lymphocytes (TILs) and are linked to T-cell activation, but also with a proapoptosis, suggesting a complicated interplay between exhaustion and activation.146 To alleviate T-cell exhaustion, numerous therapies have been explored. Immune checkpoint blockade (ICB) targeting these inhibitory receptors has showed promise in reinvigorating exhausted T cells, however not all patients respond durably.147 Cytokine therapy and metabolic pathway modifications targeting the TME are also being investigated to improve CAR-T cell efficacy.148 Regulatory T cells (Tregs) also show exhaustion-like phenotypes under persistent stimulation, which may restrict their therapeutic potential in autoimmunity and transplantation. This suggests that comparable mechanisms may be at play across different T cell subsets.149 A unified exhaustion definition incorporating metabolic, epigenetic, transcriptional, and activation-based markers (M.E.T.A.) could improve understanding and improve targeted interventions. T-cell exhaustion can be addressed by ICB, metabolic reprogramming, and TME regulation to improve cancer CAR-T cell therapy outcomes.146
CAR-T cell therapies' efficacy and safety depend on epigenetic modifications that affect T-cell differentiation, exhaustion, and tumor infiltration. Cancer stem cells (CSCs) promote their initiation and maintenance by aberrant epigenetic reprogramming, allowing them to evade immune defenses and resist therapies. Targeting these epigenetic modifications can improve CAR-T therapy outcomes.150 Integrating omics technologies like epigenomics has helped discover tumor-specific antigens and molecular characteristics linked with CAR-T cell therapy’s anti-tumor effects and toxicity.151 CAR-T cells’ in vivo performance is affected by epigenetic regulation, which may improve memory phenotype, trafficking, and fitness, leading to more effective immunotherapies.152 Modulating epigenetic factors such as DNA methylation, histone modification, and chromatin remodeling may improve CAR-T therapy's safety and efficacy.35 Epigenetic modifications could improve targeting mechanisms for CAR-T therapies in hematologic malignancies, reducing side effects and off-target effects.153 Understanding epigenomic events within the tumor immune microenvironment (TIME) is essential for exploiting epigenetic modification reversibility for cancer diagnosis, progression tracking, and treatment.154 CAR-T therapy combined with other treatments, such as radiation, may benefit from epigenetic insights to overcome solid tumor therapeutic limits.155 Overall, epigenetic biomarkers have the potential to improve CAR-T therapy’s predictive and therapeutic efficiency, making them a promising research and clinical application.
Biomarkers for CAR-T Cell Functionality
The study found that the specific characteristics of T cells, including the presence of immune checkpoints like TIM-3, PD-1, and LAG-3, as well as the immune microenvironment, can affect the effectiveness and behavior of CAR-T cells in fighting tumors. However, the proper functions of CAR-T cells are essential for their effective therapeutic response and durable remission.129,156 Numerous previous studies have reflected that the less differentiated T cells were strongly correlated with the expansion, persistence, and tumor-killing ability of CAR-T cells.114,157 A mouse model study on B-ALL revealed that the functionally modified CAR-T product with CD8+ Tscm cells is more effective in terms of prolonged antitumor activity and survival.158 It was also suggested that the number of CD8+CD45RA+CCR7+ Tscm cells in CAR-T cell products was linked to the speed at which CAR-T cells grew.159 Furthermore, in vivo investigations indicated that the presence of Tscm cells in the final CAR-T cell product was a favorable indicator for the expansion of CAR-T cells. Conversely, the presence of Tem cells and CD57+ cells in the final product had a detrimental effect on CAR-T cell proliferation and the effectiveness of anti-tumor activity.160
Biomarkers for Immune Checkpoints
It was also observed that the high-level expression of immune checkpoint proteins such as LAG-3, PD-1, and T cell immunoglobulin-3 (TIM-3) was associated with T cell exhaustion and could be associated with a lower response to anti-CD19 and CAR-T cell therapies.19 PD-1 expression on activated T cells, NK cells, and B cells can inhibit the growth of T cells, the production of cytokines, and the cytotoxicity that could result in tumor cells evading the immune system.161 Similarly, TIM-3 and LAG-3 have a role in exerting negative regulation on T cell activation.162 A study indicated that the dysfunctional response group had a considerably larger number of LAG-3+ T cells and TIM-3+ T cells compared to the functional response group. However, both groups had equal frequencies of PD-1+ CD4+ CAR-T cells and PD-1+ CD8+ CAR-T cells. Higher numbers of PD-1+ CD4+ T cells and PD-1+LAG-3+ CD8+T cells were seen in the group with trouble responding. Moreover, the findings also revealed that more expression of LAG-3 together with low secretion of TNF-α was correlated with early therapeutic failure, and the low frequency of TNF-α+/TIM-3-CD8+ T cells in CD19 CAR-T cell products may be a risk factor for low persistence of CAR-T cells and early relapse.140 So, having too much PD-1, LAG-3, and TIM-3 on immune cells could be a way to tell early on how well a CAR-T treatment will work.
Biomarkers for the Immune Microenvironment
The suppressive immune microenvironment status could be unfavourable for T cell function and associated with inferior survival. The activated myeloid and lymphoid lineages of immune cells can indicate a lower immune-suppressed environment, which could be suitable for the expansion and persistence of CAR-T cells. A study observed that the B cell lymphoma patients treated with CD19 CAR-T cells had low monocytic myeloid-derived suppressor cell counts (CD14+ CD33+ HLA-DR cells) and showed a better response. Also, patients who had more expression of myeloid activation markers (IL-12, DC-Lamp) and lymphocyte effector markers (Fas ligand, TRAIL) had a longer overall survival.163 Furthermore, polyfunctional T cells produce cytokines and chemokines such as IFN-γ, MIP-1, IL-8, granzyme-B, IL-17A, and IL-5, which can reduce immunosuppression caused by the tumor microenvironment and could enhance clinical outcomes in CD19 CAR-T cell therapy. The increased serum levels of IL-15, MCP-1, and IL-7, which are associated with CAR-T cell expansion, could also impact the positive outcome of CD19 CAR-T cells.164,165 IL-12 is produced by immune cells (T cells, NK cells, dendritic cells, and macrophages), which induces the secretion of several inflammatory cytokines, including IL-6, IL-8, IL-15, IL-18, IFN-ϒ, TNF-α, and GM-CSF. It also increases the cytotoxic functions of T cells and NK cells.166 Similarly, IL-18, which activates monocytes and lymphocytes, could enhance the antitumor activity of CAR-T cells as well as decrease the number of immunosuppressive cells.167–169
Future Prospects and Challenges
The potential of CAR-T cell-based gene therapies to transform cancer treatment is highly promising. Although CAR-T cell therapy has achieved significant success in treating hematological malignancies, there are still difficulties and opportunities that need to be addressed. Comprehending the immunological characteristics and surroundings of solid tumors is essential for enhancing the effectiveness of immunotherapies. Furthermore, improvements in the accuracy and selectivity of CAR-T cell identification by flow cytometry and PCR are crucial for boosting the accuracy and surveillance of CAR-T cell treatment. CAR-T therapy has revolutionized cancer treatment, especially for hematologic malignancies, although it presents technological and logistical obstacles. Antigen escape, when tumor cells evade the target antigen, and the immunosuppressive tumor microenvironment, which reduces CAR-T cell efficacy in solid tumors, are technical hurdles.170–172 Technical challenges include improving CAR-T cell persistence and overcoming drug-resistant relapse.173,174 The necessity for specialist institutes with excellent processes and the high expense and complexity of producing patient-specific CAR-T cells limit accessibility.175–177 Different national and supranational interpretations of CAR-T products, as shown in the Russian Federation, exacerbate regulatory issues.178 Technical solutions like engineering CAR-T cells to better infiltrate tumors and resist immunosuppressive environments and logistical solutions like decentralized manufacturing models and regulatory harmonization to reduce costs and improve access are needed to address these issues.179 As required by the European Medicines Agency, CAR-T cell efficacy and safety must be monitored over time. By systematically addressing these obstacles, CAR-T therapy can be made more effective and accessible to more patients.
Ensuring broader accessibility and affordability of novel cellular and immunotherapy treatments requires careful consideration of quality, cost, and access during their delivery. Optimizing the safety and tolerability of CAR-T cell therapy requires the careful management of adverse effects, including cytokine release syndrome and immune effector cell-associated neurotoxicity syndrome. The relapse mechanism and treatment method following CAR-T cell therapy in B cell hematological malignancies are currently being actively researched. The goal is to tackle the obstacles of disease recurrence and improve therapeutic techniques. In addition, the investigation of several categories of T cells, such as memory cells and effector cells, along with the development of advanced CAR-T immunotherapy, presents potential avenues for improving the effectiveness and long-lasting effects of CAR-T cell treatment. The advancement of immunotherapy, specifically the production of CD8+ T cells from hematopoietic stem cells, is a notable achievement in cellular immunotherapy. This has the potential to broaden the scope of these treatments, making them more applicable. The critical focus lies in surmounting challenges and applying coping mechanisms for CAR-T cell immunotherapy in solid tumors. This endeavor holds substantial potential for expanding the advantages of CAR-T cell therapy to a wider array of cancer types. Ensuring the long-term effectiveness of CAR-T cell therapy relies on the persistence and development of memory cells. CAR-T cell therapy has been successful in treating hematological malignancies such B-cell acute lymphoblastic leukemia and non-Hodgkin’s lymphoma, earning FDA approval.72,180,181 Its efficacy in solid tumors is restricted by the lack of reliable tumor-specific antigens, poor T-cell infiltration, and immunosuppressive tumor microenvironments.73,182,183 Antigen escape, T-cell exhaustion, and severe toxicities such cytokine release syndrome and neurotoxicity hamper CAR-T cell therapy’s use.184–186 Using bi-specific chimeric antigen receptors, immune checkpoint inhibitors, and immuno-PET/-SPECT for better monitoring and optimization are among the innovative ways to improve CAR-T cell efficacy.187 CAR-Treg therapies for autoimmune disorders and CAR-T cell applications beyond oncology suggest a promising future for this technology. However, the high cost and complexity of CAR-T cell manufacture require cost-effective production methods and improved clinical application approaches. The future for CAR-T cell therapy is optimistic, but these complex issues must be addressed to maximize its potential across cancer types and other diseases. Thus, CAR-T cell therapy has considerable potential, but its efficacy and future applications should be examined in light of its existing limits and ongoing advances. Ongoing research endeavors to tackle these obstacles and enhance the durability of CAR-T cell therapy. Moreover, comprehending the role of tumor cell dedifferentiation in promoting immune evasion and immunotherapy resistance offers valuable knowledge for developing strategies to overcome resistance mechanisms and improve treatment results. The engineering of CAR-T cells for the treatment of solid tumors and the advancement of immunotherapies that activate T cells demonstrate the ongoing progress of CAR-T cell technology and its ability to fulfill medical demands that have not been met in cancer treatment. Utilizing combinatorial methods to enhance the effectiveness of CAR-T cell therapy in hematological malignancies, along with investigating single-cell imaging of T cell immunotherapy responses in living organisms, are novel strategies aimed at further improving the efficacy of CAR-T cell therapy. CAR-T cell therapy has revolutionized the course of therapy of hematological malignancies by targeting CD-19 and B-cell maturation antigens in B-cell acute lymphoblastic leukemia and large B-cell lymphoma.72,73 Extending this achievement to solid tumors is difficult. The TME of solid tumors is complicated and immunosuppressive, with dense extracellular matrices, hypoxic cores, and inhibitory cytokines that impede CAR-T cell infiltration and function.74,75,188 CAR-T cells’ efficacy in solid tumors is further complicated by tumor antigen heterogeneity and antigen escape.189–191 To overcome these obstacles, researchers are augmenting CAR-T cells with chemokine receptors, combining CAR-T therapy with immune checkpoint inhibitors, and establishing dual-target CARs to enhance specificity and limit off-target effects.192,193 Alternative immune cells such CAR-NK and CAR-M cells are being studied for tumor infiltration and decreased toxicity. Advanced methods like single-cell RNA sequencing and artificial intelligence are identifying solid tumor biomarkers to refine CAR-T cell design and predict therapy responses. Despite these advances, multicenter clinical trials are needed to confirm the efficacy and safety of combinatorial and novel solid tumor treatments. In solid tumors, CAR-T cell therapy poses considerable challenges, although ongoing research and technical improvements may improve patient outcomes.
Overall, the future outlook for CAR-T cell-based gene therapies is marked by continuous progress in comprehending the tumor microenvironment, enhancing methods for detection and monitoring, mitigating side effects, optimizing treatment approaches, and broadening the scope of cellular immunotherapy. These combined efforts contribute to the ongoing development and improvement of CAR-T cell therapy, leading to its wider and more efficient use in treating different types of cancer.
Conclusions
To summarize, CAR-T cell therapy has emerged as a viable treatment method for hematological malignancies, specifically B cell malignancies. In addition, CAR-T cell-based gene therapies are an innovative method in the field of cancer treatment, providing new opportunities for patients with resistant or recurring malignancies. Despite the presence of obstacles such as adverse events and prognostic heterogeneity, the distinctiveness and strength of CAR-T cells have demonstrated notable therapeutic efficacy. Continuous research and clinical trials are crucial in advancing the field of CAR-T cell therapies. These efforts aim to enhance the effectiveness and widen the range of cancer treatments, ultimately leading to improved outcomes. CAR-T cell therapy is a sort of gene therapy that is a major breakthrough in the industry. It provides new optimism for patients with hematological malignancies that are resistant to treatment or have relapsed.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Cesur-Ergün B, Demir-Dora D. Gene therapy in cancer. J Gene Med. 2023;25(11). doi:10.1002/jgm.3550
2. Oaklander AL, Lunn MPT, Hughes RA, van Schaik IN, Frost C, Chalk CH. Treatments for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP): an overview of systematic reviews. Cochrane Database Syst Rev. 2017;2017(1). doi:10.1002/14651858.CD010369.pub2
3. Aiuti A, Roncarolo MG, Naldini L. Gene therapy for ADA-SCID, the first marketing approval of an ex vivo gene therapy in Europe: paving the road for the next generation of advanced therapy medicinal products. EMBO Mol Med. 2017;9(6):737–740. doi:10.15252/emmm.201707573
4. Thomson D, Foisy M, Oleszczuk M, Wingert A, Chisholm A, Hartling L. Overview of reviews in child health: evidence synthesis and the knowledge base for a specific population. Evid Based Child Health. 2013;8(1):3–10. doi:10.1002/ebch.1897
5. Hopfinger G, Rupp B, Greil R. Barriers to patient access of CAR T cell therapies in Austria. memo. 2023;16(1):79–90. doi:10.1007/s12254-022-00859-w
6. Zhu L, Liu J, Zhou G, et al. Remodeling of tumor microenvironment by tumor-targeting nanozymes enhances immune activation of CAR T cells for combination therapy. Small. 2021;17(43). doi:10.1002/smll.202102624
7. Wu J, Tang L, Du M, et al. Plasma proteomic and metabolomic signatures of B‐ALL patients during CAR‐T cell therapy. Clin Transl Med. 2023;13(3). doi:10.1002/ctm2.1225
8. Montalvo M, Bandey I, Rezvan A, et al. 402 T cell killing is facilitated by multiple cytotoxic pathways. BMJ Spec J. 2022. doi:10.1136/jitc-2022-sitc2022.0402
9. Schett G, Mackensen A, Mougiakakos D. CAR T-cell therapy in autoimmune diseases. Lancet. 2023;402(10416):2034–2044. doi:10.1016/S0140-6736(23)01126-1
10. Phillips R. CAR T cells induce drug-free SLE remission. Nat Rev Rheumatol. 2022;18(12):671–671. doi:10.1038/s41584-022-00865-6
11. Ochi T, Maruta M, Tanimoto K, et al. A single-chain antibody generation system yielding CAR-T cells with superior antitumor function. Commun Biol. 2021;4(1). doi:10.1038/s42003-021-01791-1
12. Jayaraman J, Mellody MP, Hou AJ, et al. CAR-T design: elements and their synergistic function. EBioMedicine. 2020:58. doi:10.1016/j.ebiom.2020.102931
13. Abbasi S, Totmaj MA, Abbasi M, et al. Chimeric antigen receptor T (CAR-T) cells: novel cell therapy for hematological malignancies. Cancer Med. 2023;12(7):7844–7858. doi:10.1002/cam4.5551
14. Abbott RC, Cross RS, Jenkins MR. Finding the keys to the CAR: identifying novel target antigens for t cell redirection immunotherapies. Int J Mol Sci. 2020;21(2):515. doi:10.3390/ijms21020515
15. Prasad V. Tisagenlecleucel - The first approved CAR-T-cell therapy: implications for payers and policy makers. Nat Rev Clin Oncol. 2018;15(1):11–12. doi:10.1038/nrclinonc.2017.156
16. Mullard A. FDA approves first BCMA-targeted CAR-T cell therapy. Nat Rev Drug Discov. 2021;20(5). doi:10.1038/d41573-021-00063-1
17. Neelapu SS, Locke FL, Bartlett NL, et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large B-cell lymphoma. N Engl J Med. 2017;377(26):2531–2544. doi:10.1056/nejmoa1707447
18. Maude SL, Laetsch TW, Buechner J, et al. Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N Engl J Med. 2018;378(5):439–448. doi:10.1056/nejmoa1709866
19. Schuster SJ, Svoboda J, Chong EA, et al. Chimeric antigen receptor T cells in refractory B-cell lymphomas. N Engl J Med. 2017;377(26):2545–2554. doi:10.1056/nejmoa1708566
20. Awasthi R, Maier HJ, Zhang J, Lim S. Kymriah® (tisagenlecleucel)–An overview of the clinical development journey of the first approved CAR-T therapy. Hum Vaccin Immunother. 2023;19(1). doi:10.1080/21645515.2023.2210046
21. Lu J, Jiang G. The journey of CAR-T therapy in hematological malignancies. Mol Cancer. 2022;21(1). doi:10.1186/s12943-022-01663-0
22. Maus MV. A decade of CAR T cell evolution. Nat Cancer. 2022;3(3):270–271. doi:10.1038/s43018-022-00347-4
23. Ragoonanan D, Sheikh IN, Gupta S, et al. The evolution of chimeric antigen receptor T-cell therapy in children, adolescents and young adults with acute lymphoblastic leukemia. Biomedicines. 2022;10(9):2286. doi:10.3390/biomedicines10092286
24. Baker DJ, Arany Z, Baur JA, Epstein JA, June CH. CAR T therapy beyond cancer: the evolution of a living drug. Nature. 2023;
25. Daei Sorkhabi A, Mohamed khosroshahi L, Sarkesh A, et al. The current landscape of CAR T-cell therapy for solid tumors: mechanisms, research progress, challenges, and counterstrategies. Front Immunol. 2023:14. doi:10.3389/fimmu.2023.1113882
26. Yu S, Yi M, Qin S, Wu K. Next generation chimeric antigen receptor T cells: safety strategies to overcome toxicity. Mol Cancer. 2019;18(1). doi:10.1186/s12943-019-1057-4
27. Jan M, Scarfò I, Larson RC, et al. Reversible ON- And OFF-switch chimeric antigen receptors controlled by lenalidomide. Sci Transl Med. 2021;13(575). doi:10.1126/SCITRANSLMED.ABB6295
28. Carbonneau S, Sharma S, Peng L, et al. An IMiD-inducible degron provides reversible regulation for chimeric antigen receptor expression and activity. Cell Chem Biol. 2021;28(6):802–812.e6. doi:10.1016/j.chembiol.2020.11.012
29. Richman SA, Wang LC, Moon EK, Khire UR, Albelda SM, Milone MC. Ligand-induced degradation of a CAR permits reversible remote control of CAR T cell activity in vitro and in vivo. Mol Ther. 2020;28(7):1932. doi:10.1016/j.ymthe.2020.06.004
30. Rodgers DT, Mazagova M, Hampton EN, et al. Switch-mediated activation and retargeting of CAR-T cells for B-cell malignancies. Proc Natl Acad Sci U S A. 2016;113(4). doi:10.1073/pnas.1524155113
31. Morsut L, Roybal KT, Xiong X, et al. Engineering customized cell sensing and response behaviors using synthetic notch receptors. Cell. 2016;164(4):780–791. doi:10.1016/j.cell.2016.01.012
32. Choe JH, Watchmaker PB, Simic MS, et al. SynNotch-CAR T cells overcome challenges of specificity, heterogeneity, and persistence in treating glioblastoma. Sci Transl Med. 2021;13(591). doi:10.1126/scitranslmed.abe7378
33. Li Y, Basar R, Wang G, et al. KIR-based inhibitory CARs overcome CAR-NK cell trogocytosis-mediated fratricide and tumor escape. Nat Med. 2022;28(10):2133–2144. doi:10.1038/s41591-022-02003-x
34. Fei F, Rong L, Jiang N, Wayne AS, Xie J. Targeting HLA-DR loss in hematologic malignancies with an inhibitory chimeric antigen receptor. Mol Ther. 2022;30(3):1215–1226. doi:10.1016/j.ymthe.2021.11.013
35. Zhang X. The application of epigenetics in CAR-T therapy. Advan Engin Technol Res. 2023;1(3):604. doi:10.56028/aetr.3.1.604
36. Bangayan NJ, Wang L, Sojo GB, et al. Dual-inhibitory domain iCARs improve the efficiency of the AND-NOT gate CAR T strategy. Proc Natl Acad Sci U S A. 2023;120(47). doi:10.1073/pnas.2312374120
37. Ghamari A, Pakzad P, Majd A, Ebrahimi M, Hamidieh AA. Design and production an effective bispecific tandem chimeric antigen receptor on T cells against CD123 and folate receptor ß towards B-acute myeloid leukaemia blasts. Cell J. 2021;23(6):650–657. doi:10.22074/cellj.2021.7314
38. Ruffo E, Butchy AA, Tivon Y, et al. Post-translational covalent assembly of CAR and synNotch receptors for programmable antigen targeting. Nat Commun. 2023;14(1). doi:10.1038/s41467-023-37863-5
39. Kvorjak M, Ruffo E, Tivon Y, et al. Conditional Control of Universal CAR T Cells by Cleavable OFF-Switch Adaptors. ACS Synth Biol. 2023;12(10):2996–3007. doi:10.1021/acssynbio.3c00320
40. Arndt C, Fasslrinner F, Loureiro LR, Koristka S, Feldmann A, Bachmann M. Adaptor car platforms—next generation of T cell-based cancer immunotherapy. Cancers. 2020;12(5):1302. doi:10.3390/cancers12051302
41. Cho JH, Collins JJ, Wong WW. Universal chimeric antigen receptors for multiplexed and logical control of T cell responses. Cell. 2018;173(6):1426–1438.e11. doi:10.1016/j.cell.2018.03.038
42. Zhao J, Lin Q, Song Y, Liu D. Universal CARs, universal T cells, and universal CAR T cells. J Hematol Oncol. 2018;11(1). doi:10.1186/s13045-018-0677-2
43. Caulier B, Enserink JM, Wälchli S. Pharmacologic control of car t cells. Int J Mol Sci. 2021;22(9):4320. doi:10.3390/ijms22094320
44. Do MH, Thanh HD, To PK, Kim MS, Moon C, Jung C. CD46 protects the bladder cancer cells from cetuximab-mediated cytotoxicity. Sci Rep. 2022;12(1). doi:10.1038/s41598-022-27107-9
45. Paszkiewicz PJ, Fräßle SP, Srivastava S, et al. Targeted antibody-mediated depletion of murine CD19 CAR T cells permanently reverses B cell aplasia. J Clin Investig. 2016;126(11):4262–4272. doi:10.1172/JCI84813
46. Andrea AE, Chiron A, Bessoles S, Hacein-Bey-abina S. Engineering next-generation car-t cells for better toxicity management. Int J Mol Sci. 2020;21(22):8620. doi:10.3390/ijms21228620
47. Kalinin RS, Petukhov AV, Knorre VD, Maschan MA, Stepanov AV, Gabibov AG. Molecular approaches to safe and controlled engineered T-cell therapy. Acta Naturae. 2018;10(2):16–23. doi:10.32607/2075851-2018-10-2-16-23
48. Thi EP, Cole AG, Heffernan G, et al. Preclinical anti-tumor activity of small-molecule oral PD-L1 checkpoint inhibitors. J Clin Oncol. 2022;40(16_suppl):e14558–e14558. doi:10.1200/jco.2022.40.16_suppl.e14558
49. Kasichayanula S, Mandlekar S, Shivva V, Patel M, Girish S. Evolution of preclinical characterization and insights into clinical pharmacology of checkpoint inhibitors approved for cancer immunotherapy. Clin Transl Sci. 2022;15(8):1818–1837. doi:10.1111/cts.13312
50. Jacoberger-Foissac C, Allard B, Allard D, Stagg J. Assessing the efficacy of immune checkpoint inhibitors in preclinical tumor models. Methods Mol Biol. 2023;2614. doi:10.1007/978-1-0716-2914-7_11
51. Thudium K, Selby M, Zorn JA, et al. Preclinical characterization of relatlimab, a human LAG-3-blocking antibody, alone or in combination with nivolumab. Cancer Immunol Res. 2022;10(10):1175–1189. doi:10.1158/2326-6066.CIR-22-0057
52. Hovhannisyan L, Riether C, Aebersold DM, Medová M, Zimmer Y. CAR T cell-based immunotherapy and radiation therapy: potential, promises and risks. Mol Cancer. 2023;22(1). doi:10.1186/s12943-023-01775-1
53. Ghareghani M, Rivest S. The synergistic potential of combining PD-1/PD-L1 immune checkpoint inhibitors with NOD2 agonists in alzheimer’s disease treatment. Int J Mol Sci. 2023;24(13):10905. doi:10.3390/ijms241310905
54. Yang K, Zhao Y, Sun G, et al. Clinical application and prospect of immune checkpoint inhibitors for CAR-NK cell in tumor immunotherapy. Front Immunol. 2023:13. doi:10.3389/fimmu.2022.1081546
55. Mohty R, Gauthier J. Current combinatorial CAR T cell strategies with Bruton tyrosine kinase inhibitors and immune checkpoint inhibitors. Bone Marrow Transplant. 2021;56(11):2630–2636. doi:10.1038/s41409-021-01420-9
56. Durán I, Castellano D, Puente J, et al. Exploring the synergistic effects of cabozantinib and a programmed cell death protein 1 inhibitor in metastatic renal cell carcinoma with machine learning. Oncotarget. 2022;13:13. doi:10.18632/ONCOTARGET.28183
57. Rajeev-Kumar G, Pitroda SP. Synergizing radiotherapy and immunotherapy: current challenges and strategies for optimization. Neoplasia. 2023;36. doi:10.1016/j.neo.2022.100867
58. Li YR, Zhou Y, Yu J, et al. Generation of allogeneic CAR-NKT cells from hematopoietic stem and progenitor cells using a clinically guided culture method. Nat Biotechnol. 2024. doi:10.1038/s41587-024-02226-y
59. van der Leun AM, Thommen DS, Schumacher TN. CD8+ T cell states in human cancer: insights from single-cell analysis. Nat Rev Cancer. 2020;20(4):218–232. doi:10.1038/s41568-019-0235-4
60. Moreno M, Molling JW, von Mensdorff-Pouilly S, et al. IFN-γ-producing human invariant NKT cells promote tumor-associated antigen-specific cytotoxic T cell responses. J Immunol. 2008;181(4):2446–2454. doi:10.4049/jimmunol.181.4.2446
61. Cortés-Selva D, Dasgupta B, Singh S, Grewal IS. Innate and innate-like cells: the future of chimeric antigen receptor (CAR) cell therapy. Trends Pharmacol Sci. 2021;42(1):45–59. doi:10.1016/j.tips.2020.11.004
62. Heczey A, Xu X, Courtney AN, et al. Anti-GD2 CAR-NKT cells in relapsed or refractory neuroblastoma: updated Phase 1 trial interim results. Nat Med. 2023;29(6):1379–1388. doi:10.1038/s41591-023-02363-y
63. Zhou Y, Li M, Zhou K, et al. Engineering-Induced Pluripotent Stem Cells for Cancer Immunotherapy. Cancers. 2022;14(9). doi:10.3390/cancers14092266
64. Dogan M, Karhan E, Kozhaya L, et al. Engineering human MAIT cells with chimeric antigen receptors for cancer immunotherapy. J Immunol. 2022;209(8):1523–1531. doi:10.4049/jimmunol.2100856
65. Bohineust A, Tourret M, Derivry L, Caillat-Zucman S. Mucosal-associated invariant T (MAIT) cells, a new source of universal immune cells for chimeric antigen receptor (CAR)-cell therapy. Bull Cancer. 2021;108(10):S92–S95. doi:10.1016/j.bulcan.2021.07.003
66. Rozenbaum M, Meir A, Aharony Y, et al. Gamma-Delta CAR-T Cells Show CAR-Directed and Independent Activity Against Leukemia. Front Immunol. 2020;11:11. doi:10.3389/fimmu.2020.01347
67. Dwivedi A, Fu L, Chien CD, Pouzolles M, Shah NN, Taylor N. Engineering off-the-shelf gamma delta CAR T cells for the treatment of acute myeloid leukemia. Blood. 2023;142(Supplement 1):4827–4827. doi:10.1182/blood-2023-190357
68. Becker WJ, Olkhanud PB, Berzofsky JA. Triple synergy between vaccine and checkpoint inhibitors in a pre-clinical tumor model. J Immunol. 2022;208(1_Supplement):118.14–118.14. doi:10.4049/jimmunol.208.supp.118.14
69. Guha R, Waddell J, Banerjee A. Commentary on: pre-clinical platforms to study therapeutic efficacy of human γδ T cells. Clin Translat Discov. 2022;2(2). doi:10.1002/ctd2.74
70. Jiang M, Fiering S, Shao Q. Combining energy-based focal ablation and immune checkpoint inhibitors: preclinical research and clinical trials. Front Oncol. 2023;13. doi:10.3389/fonc.2023.1153066
71. Wu S, Ji F, Xu B, Wu F. Delivering CAR‐T cells into solid tumors via hydrogels. Med Comm Oncol. 2023;2(2). doi:10.1002/mog2.40
72. Dagar G, Gupta A, Masoodi T, et al. Harnessing the potential of CAR-T cell therapy: progress, challenges, and future directions in hematological and solid tumor treatments. J Transl Med. 2023;21(1). doi:10.1186/s12967-023-04292-3
73. Zheng J. CAR T-cell therapy in solid tumors: current review and future perspectives. Highligh Sci Enginee Technol. 2023;54. doi:10.54097/hset.v54i.9841
74. Shin MH, Oh E, Kim Y, et al. Recent Advances in CAR-based solid tumor immunotherapy. Cells. 2023;12(12):1606. doi:10.3390/cells12121606
75. Kheyrolahzadeh K, Tohidkia MR, Tarighatnia A, Shahabi P, Nader ND, Aghanejad A. Theranostic chimeric antigen receptor (CAR)-T cells: insight into recent trends and challenges in solid tumors. Life Sci. 2023;328. doi:10.1016/j.lfs.2023.121917
76. Newick K, Moon E, Albelda SM. Chimeric antigen receptor T-cell therapy for solid tumors. Mol Ther Oncolytics. 2016;3. doi:10.1038/mto.2016.6
77. Ponterio E, De Maria R, Haas TL, Qiu L, Zhu L. Identification of targets to redirect CAR T cells in glioblastoma and colorectal cancer: an arduous venture. Front Immunol. 2020;11:11. doi:10.3389/fimmu.2020.565631
78. Kara E, Jackson TL, Jones C, McGee RL, Sison R. Mathematical modeling insights into improving CAR T cell therapy for solid tumors: antigen heterogeneity and bystander effects. arXiv preprint, arXiv. 2023;2023:1.
79. Tengku Ibrahim Maulana CT, MCLL FE van den H. Solid tumor-on-chip model for efficacy and safety assessment of CAR-T cell therapy. bioRxiv. 2023;2023:7.
80. Sailer CJ, Hong Y, Dahal A, et al. PD-1Hi CAR-T cells provide superior protection against solid tumors. Front Immunol. 2023:14. doi:10.3389/fimmu.2023.1187850
81. Adachi K, Tamada K. Development of CAR-T cells effective against solid tumors. Gan To Kagaku Ryoho. 2023;50(5):1.
82. Tang M, Pearson SA, Simes RJ, Chua BH. Harnessing real-world evidence to advance cancer research. Current Oncol. 2023;30(2):1844–1859. doi:10.3390/curroncol30020143
83. Usmanova TA, Verbitskaya EV. Combining real-world data with randomized controlled trials results in better information oncology decision making. Real World Data Eviden. 2022;2(2):21–31. doi:10.37489/2782-3784-myrwd-14
84. Vitale C, Strati P, Bi S, Xie S. CAR T-Cell Therapy for B-cell non-Hodgkin lymphoma and chronic lymphocytic leukemia: clinical trials and real-world experiences. Front Oncol. 2020;10:10. doi:10.3389/fonc.2020.00849
85. Chen D. Real-world studies: bridging the gap between trial-assessed efficacy and routine care. J Biomed Res. 2022;36(3):147. doi:10.7555/JBR.36.20220040
86. Asai N, Shibata Y, Hirai J, et al. A gap of patients with infective endocarditis between clinical trials and the real world. J Clin Med. 2023;12(4):1566. doi:10.3390/jcm12041566
87. Ghiani M, Maywald U, Wilke T, Heeg B. Bridging the gap between oncology clinical trials and real-world data: evidence on replicability of efficacy results using German claims data. J Comp Eff Res. 2022;11(7):513–521. doi:10.2217/cer-2021-0224
88. Bethge W. CAR-T-Zelltherapie bewährt sich in Real-World-Szenario. Transfusionsmedizin. 2022;12(03). doi:10.1055/a-1856-6141
89. Yang DD, Nguyen PL. The increasing importance of rigorous real-world evidence. JNCI Cancer Spectr. 2022;6(4). doi:10.1093/jncics/pkac051
90. Azam U, Sridharan K. CAR-T cell clinical trials experience – past, present and future. Second Generat Cell Gene Bas Therap. 2020. doi:10.1016/B978-0-12-812034-7.00012-1
91. Barros LRC, Couto SCF, da Silva Santurio D, et al. Systematic review of available CAR-T cell trials around the world. Cancers. 2022;14(11):2667. doi:10.3390/cancers14112667
92. Porreca I, Blassberg R, Harbottle J, et al. An aptamer-mediated base editing platform for simultaneous knock-in and multiple gene knockout for allogeneic CAR-T cells generation. bioRxiv. 2023;2023:1.
93. Zhou X, Renauer PA, Zhou L, Fang SY, Chen S. Applications of CRISPR technology in cellular immunotherapy. Immunol Rev. 2023;320(1):199–216. doi:10.1111/imr.13241
94. Yi K, Kong H, Lao YH, et al. Engineered nanomaterials to potentiate CRISPR/Cas9 gene editing for cancer therapy. Adv Mater. 2023. doi:10.1002/adma.202300665
95. Li Z. Trends for CRISPR and CAR-T in the future medical field. Highligh Sci Enginee Technol. 2023;2023:54. doi:10.54097/hset.v54i.9780
96. Iqbal F. Enhancing the effectiveness of Chimeric Antigen Receptor (CAR) T cells against tumors through CRISPR/Cas9-mediated PD-1 disruption. Int J Health Sci (Qassim). 2023;7(S1). doi:10.53730/ijhs.v7ns1.14397
97. Hendel A, Bak RO. Editorial: CRISPR and beyond: cutting-edge technologies for gene correction in therapeutic applications. Front Genome Ed. 2023;5. doi:10.3389/fgeed.2023.1203864
98. Lamothe RC, Storlie MD, Espinosa DA, et al. Novel CRISPR-associated gene-editing systems discovered in metagenomic samples enable efficient and specific genome engineering. CRISPR J. 2023;6(3):243–260. doi:10.1089/crispr.2022.0089
99. Naeem M, Hazafa A, Bano N, et al. Explorations of CRISPR/Cas9 for improving the long-term efficacy of universal CAR-T cells in tumor immunotherapy. Life Sci. 2023:316. doi:10.1016/j.lfs.2023.121409
100. Sergeeva O, Fearnley A, Chin SS, et al. Abstract 4094: enhanced CRISPR-Cas9 edited CAR-T cells through simultaneous inactivation of multiple T cell exhaustion pathways. Cancer Res. 2023;83(7_Supplement):4094–4094. doi:10.1158/1538-7445.am2023-4094
101. Ajavavarakula T. CRISPR-edited CAR-T cells: using CRISPR-Cas9 to Improve CAR-T Therapy. Highligh Sci Enginee Technol. 2022;14. doi:10.54097/hset.v14i.1846
102. Glaser V, Flugel C, Kath J, et al. Combining different CRISPR nucleases for simultaneous knock-in and base editing prevents translocations in multiplex-edited CAR T cells. Genome Biol. 2023;24(1). doi:10.1186/s13059-023-02928-7
103. Galvin B, Zheng G, Moot R, et al. 332 CRISPR/Cas9-based integration of a large and modular cassette into a safe harbor site to improve CAR T cell therapy efficacy and safety. BMJ Spec J. 2022. doi:10.1136/jitc-2022-sitc2022.0332
104. Ni B. First-Ever CAR T-cell therapy approved in U.S. Cancer Discov. 2017;7(10). doi:10.1158/2159-8290.CD-NB2017-126
105. Li Y, Ming Y, Fu R, et al. The pathogenesis, diagnosis, prevention, and treatment of CAR-T cell therapy-related adverse reactions. Front Pharmacol. 2022:13. doi:10.3389/fphar.2022.950923
106. Mitra A, Barua A, Huang L, Ganguly S, Feng Q, He B. From bench to bedside: the history and progress of CAR T cell therapy. Front Immunol. 2023;14. doi:10.3389/fimmu.2023.1188049
107. Munshi NC, Anderson LD, Shah N, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. 2021;384(8):705–716. doi:10.1056/nejmoa2024850
108. Wang M, Munoz J, Goy A, et al. KTE-X19 CAR T-cell therapy in relapsed or refractory mantle-cell lymphoma. N Engl J Med. 2020;382(14):1331–1342. doi:10.1056/nejmoa1914347
109. Abramson JS, Palomba ML, Gordon LI, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet. 2020;396(10254):839–852. doi:10.1016/S0140-6736(20)31366-0
110. Locke FL, Ghobadi A, Jacobson CA, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1–2 trial. Lancet Oncol. 2019;20(1):31–42. doi:10.1016/S1470-2045(18)30864-7
111. Majzner RG, Mackall CL. Clinical lessons learned from the first leg of the CAR T cell journey. Nat Med. 2019;25(9):1341–1355. doi:10.1038/s41591-019-0564-6
112. Park JH, Rivière I, Gonen M, et al. Long-Term Follow-up of CD19 CAR Therapy in Acute Lymphoblastic Leukemia. N Engl J Med. 2018;378(5):449–459. doi:10.1056/nejmoa1709919
113. Porter DL, Hwang WT, V. FN, et al. Chimeric antigen receptor T cells persist and induce sustained remissions in relapsed refractory chronic lymphocytic leukemia. Sci Transl Med. 2015;7(303). doi:10.1126/scitranslmed.aac5415
114. Fraietta JA, Lacey SF, Orlando EJ, et al. Determinants of response and resistance to CD19 chimeric antigen receptor (CAR) T cell therapy of chronic lymphocytic leukemia. Nat Med. 2018;24(5):563–571. doi:10.1038/s41591-018-0010-1
115. Schuster SJ, Bishop MR, Tam CS, et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med. 2019;380(1):45–56. doi:10.1056/nejmoa1804980
116. Porpaczy E, Wohlfarth P, Königsbrügge O, et al. Influence of TP53 mutation on survival of diffuse large B-cell lymphoma in the CAR T-cell era. Cancers. 2021;13(22):5592. doi:10.3390/cancers13225592
117. Shouval R, Tomas AA, Fein JA, et al. Impact of TP53 genomic alterations in large B-cell lymphoma treated with CD19-chimeric antigen receptor T-cell therapy. J Clin Oncol. 2022;40(4):369–381. doi:10.1200/JCO.21.02143
118. Rotte A, Frigault MJ, Ansari A, Gliner B, Heery C, Shah B. Dose-response correlation for CAR-T cells: a systematic review of clinical studies. J Immunother Cancer. 2022;10(12):e005678. doi:10.1136/jitc-2022-005678
119. Coelho A, Nogueira A, Soares S, et al. TP53 Arg72Pro polymorphism is associated with increased overall survival but not response to therapy in Portuguese/caucasian patients with advanced cervical cancer. Oncol Lett. 2018;15(5):8165–8171. doi:10.3892/ol.2018.8354
120. Smith FM, Stephens RB, Kennedy MJ, Reynolds JV. P53 abnormalities and outcomes in colorectal cancer: a systematic review [1]. Br J Cancer. 2005;92(9):1813–1813. doi:10.1038/sj.bjc.6602589
121. Zhang X, Yang J, Li J, et al. Factors associated with treatment response to CD19 CAR-T therapy among a large cohort of B cell acute lymphoblastic leukemia. Cancer Immunol Immunother. 2022;71(3):689–703. doi:10.1007/s00262-021-03009-z
122. Liu C, Ayyar VS, Zheng X, et al. Model-based cellular kinetic analysis of chimeric antigen receptor-T cells in humans. Clin Pharmacol Ther. 2021;109(3):716–727. doi:10.1002/cpt.2040
123. Frigault M, Rotte A, Ansari A, Gliner B, Heery C, Shah B. Dose fractionation of CAR-T cells. A systematic review of clinical outcomes. J Exp Clin Cancer Res. 2023;42(1). doi:10.1186/s13046-022-02540-w
124. Claps G, Faouzi S, Quidville V, et al. The multiple roles of LDH in cancer. Nat Rev Clin Oncol. 2022;19(12):749–762. doi:10.1038/s41571-022-00686-2
125. Hay KA, Gauthier J, Hirayama AV, et al. Factors associated with durable EFS in adult B-cell ALL patients achieving MRD-negative CR after CD19 CAR T-cell therapy. Blood. 2019;133(15):1652–1663. doi:10.1182/blood-2018-11-883710
126. Good Z, Spiegel JY, Sahaf B, et al. Post-infusion CAR TReg cells identify patients resistant to CD19-CAR therapy. Nat Med. 2022;28(9):1860–1871. doi:10.1038/s41591-022-01960-7
127. de Jong C, Deneer VHM, Kelder JC, Ruven H, Egberts TCG, Herder GJM. Association between serum biomarkers CEA and LDH and response in advanced non-small cell lung cancer patients treated with platinum-based chemotherapy. Thorac Cancer. 2020;11(7). doi:10.1111/1759-7714.13449
128. Du M, Hari P, Hu Y, Mei H. Biomarkers in individualized management of chimeric antigen receptor T cell therapy. Biomark Res. 2020;8(1). doi:10.1186/s40364-020-00190-8
129. Mirzaei HR, Mirzaei H, Namdar A, Rahmati M, Till BG, Hadjati J. Predictive and therapeutic biomarkers in chimeric antigen receptor T-cell therapy: a clinical perspective. J Cell Physiol. 2019;234(5):5827–5841. doi:10.1002/jcp.27519
130. Frank MJ, Hossain NM, Bukhari A, et al. Monitoring of circulating tumor DNA Improves early relapse detection after axicabtagene ciloleucel infusion in large B-cell lymphoma: results of a prospective multi-institutional trial. J Clin Oncol. 2021;39(27):3034–3043. doi:10.1200/JCO.21.00377
131. Rabinovich E, Pradhan K, Sica RA, et al. Elevated LDH greater than 400 U/L portends poorer overall survival in diffuse large B-cell lymphoma patients treated with CD19 CAR-T cell therapy in a real world multi-ethnic cohort. Exp Hematol Oncol. 2021;10(1). doi:10.1186/s40164-021-00248-9
132. Turicek DP, Giordani VM, Moraly J, Taylor N, Shah NN. CAR T-cell detection scoping review: an essential biomarker in critical need of standardization. J Immunother Cancer. 2023;11(5):e006596. doi:10.1136/jitc-2022-006596
133. Turicek D, Giordani V, Taylor N, Shah N. 289 Clinical expansion and persistence of CAR T-cells: an essential biomarker in need of standardization. BMJ Spec J. 2022. doi:10.1136/jitc-2022-sitc2022.0289
134. Magee MS, Abraham TS, Baybutt TR, et al. Human GUCY2C-targeted chimeric antigen receptor (CAR)-expressing T cells eliminate colorectal cancer metastases. Cancer Immunol Res. 2018;6(5):509–516. doi:10.1158/2326-6066.CIR-16-0362
135. Harder N, Schick M, Sontakke P, et al. 339 Quantitative assessment of CAR-T cell therapy targets using computational pathology. BMJ Spec J. 2022. doi:10.1136/jitc-2022-sitc2022.0339
136. Los-Arcos I, Iacoboni G, Aguilar-Guisado M, et al. Recommendations for screening, monitoring, prevention, and prophylaxis of infections in adult and pediatric patients receiving CAR T-cell therapy: a position paper. Infection. 2021;49(2):215–231. doi:10.1007/s15010-020-01521-5
137. Townsend MH, Shrestha G, Robison RA, O’Neill KL. The expansion of targetable biomarkers for CAR T cell therapy. J Exp Clin Cancer Res. 2018;37(1). doi:10.1186/s13046-018-0817-0
138. Hu Y, Huang J, Hu L, Qiu L, Zhu L. The chimeric antigen receptor detection toolkit. Front Immunol. 2020;11:11. doi:10.3389/fimmu.2020.01770
139. Jin J, Liu T, Cheng J, et al. MIP3α as an early prognostic predictor for patients with B-cell malignancies receiving CD19/CD22-redirected CAR-T cell cocktail therapy. Cancer Immunol Immunother. 2023;72(7):2245–2256. doi:10.1007/s00262-023-03418-2
140. Finney OC, Brakke H, Rawlings-Rhea S, et al. CD19 CAR T cell product and disease attributes predict leukemia remission durability. J Clin Investig. 2019;129(5):2123–2132. doi:10.1172/JCI125423
141. Singh N, Lee YG, Shestova O, et al. Impaired death receptor signaling in leukemia causes antigen-independent resistance by inducing CAR T-cell dysfunction. Cancer Discov. 2020;10(4):552–567. doi:10.1158/2159-8290.CD-19-0813
142. Worel N, Grabmeier-Pfistershammer K, Kratzer B, et al. The frequency of differentiated CD3+CD27-CD28- T cells predicts response to CART cell therapy in diffuse large B-cell lymphoma. Front Immunol. 2023:13. doi:10.3389/fimmu.2022.1004703
143. Jenkins E, Whitehead T, Fellermeyer M, Davis SJ, Sharma S. The current state and future of T-cell exhaustion research. Oxf Open Immunol. 2023;4(1). doi:10.1093/oxfimm/iqad006
144. Lamarche C, Ward-Hartstonge K, Mi T, et al. Tonic-signaling chimeric antigen receptors drive human regulatory T cell exhaustion. Proc Natl Acad Sci U S A. 2023;120(14). doi:10.1073/pnas.2219086120
145. Brunell AE, Lahesmaa R, Autio A, Thotakura AK. Exhausted T cells hijacking the cancer-immunity cycle: assets and liabilities. Front Immunol. 2023;14. doi:10.3389/fimmu.2023.1151632
146. Datar I, Sanmamed MF, Wang J, et al. Expression analysis and significance of PD-1, LAG-3, and TIM-3 in human non-small cell lung cancer using spatially resolved and multiparametric single-cell analysis. Clin Cancer Res. 2019;25(15):4663–4673. doi:10.1158/1078-0432.CCR-18-4142
147. Yin X, He L, Guo Z. T-cell exhaustion in CAR-T -cell therapy and strategies to overcome it. Immunology. 2023;169(4):400–411. doi:10.1111/imm.13642
148. Guan Q, Han M, Guo Q, et al. Strategies to reinvigorate exhausted CD8+ T cells in tumor microenvironment. Front Immunol. 2023:14. doi:10.3389/fimmu.2023.1204363
149. Zhu X, Li Q, Zhu X. Mechanisms of CAR T cell exhaustion and current counteraction strategies. Front Cell Dev Biol. 2022;10. doi:10.3389/fcell.2022.1034257
150. Veschi V, Turdo A, Stassi G. Novel insights into cancer stem cells targeting: CAR-T therapy and epigenetic drugs as new pillars in cancer treatment. Front Molecul Med. 2023;3. doi:10.3389/fmmed.2023.1120090
151. Yang J, Chen Y, Han L. A multi‐omics perspective of CAR T cell therapy. Clin Transl Med. 2023;13(5). doi:10.1002/ctm2.1274
152. Alvanou M, Lysandrou M, Christophi P, et al. Empowering the Potential of CAR-T Cell Immunotherapies by Epigenetic Reprogramming. Cancers. 2023;15(7):1935. doi:10.3390/cancers15071935
153. He R, Huang Y, Qian R. Principle and Application of CAR-T Cell Therapy for Cancer. Theoret Nat Sci. 2023;4(1):545–553. doi:10.54254/2753-8818/4/20220646
154. Lin HY, Chan MWY, Lui VWY, Kuppen PJK, Hung SK. Editorial: the role of epigenetic modification in radiotherapy and immuno-oncology in cancer: from bench to clinical application. Front Oncol. 2023;13. doi:10.3389/fonc.2023.1213513
155. Keshari S, Barrodia P, Singh AK. Epigenetic Perspective of Immunotherapy for Cancers. Cells. 2023;12(3):365. doi:10.3390/cells12030365
156. Chen GM, Azzam A, Ding YY, Barrett DM, Grupp SA, Tan K. Dissecting the tumor–immune landscape in chimeric antigen receptor T-cell therapy: key challenges and opportunities for a systems immunology approach. Clin Cancer Res. 2020;26(14):3505–3513. doi:10.1158/1078-0432.CCR-19-3888
157. Wang X, Popplewell LL, Wagner JR, et al. Phase 1 studies of central memory-derived CD19 CAR T-cell therapy following autologous HSCT in patients with B-cell NHL. Blood. 2016;127(24):2980–2990. doi:10.1182/blood-2015-12-686725
158. Sabatino M, Hu J, Sommariva M, et al. Generation of clinical-grade CD19-specific CAR-modified CD81 memory stem cells for the treatment of human B-cell malignancies. Blood. 2016;128(4):519–528. doi:10.1182/blood-2015-11-683847
159. Xu Y, Zhang M, Ramos CA, et al. Closely related T-memory stem cells correlate with in vivo expansion of CAR.CD19-T cells and are preserved by IL-7 and IL-15. Blood. 2014;123(24):3750–3759. doi:10.1182/blood-2014-01-552174
160. Arcangeli S, Falcone L, Camisa B, et al. Next-generation manufacturing protocols enriching TSCM CAR T cells can overcome disease-specific t cell defects in cancer patients. Front Immunol. 2020;11:11. doi:10.3389/fimmu.2020.01217
161. Tunger A, Sommer U, Wehner R, et al. The evolving landscape of biomarkers for anti-pd-1 or anti-pd-l1 therapy. J Clin Med. 2019;8(10):1534. doi:10.3390/jcm8101534
162. Qin S, Xu L, Yi M, Yu S, Wu K, Luo S. Novel immune checkpoint targets: moving beyond PD-1 and CTLA-4. Mol Cancer. 2019;18(1). doi:10.1186/s12943-019-1091-2
163. Enblad G, Karlsson H, Gammelgård G, et al. A Phase I/IIa trial using CD19-targeted third-generation CAR T cells for lymphoma and leukemia. Clin Cancer Res. 2018;24(24):6185–6194. doi:10.1158/1078-0432.CCR-18-0426
164. Hirayama AV, Gauthier J, Hay KA, et al. The response to lymphodepletion impacts PFS in patients with aggressive non-Hodgkin lymphoma treated with CD19 CAR T cells. Blood. 2019;133(17):1876–1887. doi:10.1182/blood-2018-11-887067
165. Rossi J, Paczkowski P, Shen YW, et al. Preinfusion polyfunctional anti-CD19 chimeric antigen receptor T cells are associated with clinical outcomes in NHL. Blood. 2018;132(8):804–814. doi:10.1182/blood-2018-01-828343
166. Berraondo P, Etxeberria I, Ponz-Sarvise M, Melero I. Revisiting interleukin-12 as a cancer immunotherapy agent. Clin Cancer Res. 2018;24(12):2716–2718. doi:10.1158/1078-0432.CCR-18-0381
167. Chmielewski M, Abken H. CAR T cells releasing IL-18 Convert to T-bethigh foxo1low effectors that exhibit augmented activity against advanced solid tumors. Cell Rep. 2017;21(11):3205–3219. doi:10.1016/j.celrep.2017.11.063
168. Hu B, Ren J, Luo Y, et al. Augmentation of antitumor immunity by human and mouse CAR T cells secreting IL-18. Cell Rep. 2017;20(13):3025–3033. doi:10.1016/j.celrep.2017.09.002
169. Dinarello CA, Novick D, Kim S, Kaplanski G. Interleukin-18 and IL-18 binding protein. Front Immunol. 2013;4(OCT). doi:10.3389/fimmu.2013.00289
170. Donnadieu E, Dupré L, Pinho LG, Cotta-de-Almeida V. Surmounting the obstacles that impede effective CAR T cell trafficking to solid tumors. J Leukoc Biol. 2020;108(4):1067–1079. doi:10.1002/JLB.1MR0520-746R
171. Bailey SR, Berger TR, Graham C, Larson RC, Maus MV. Four challenges to CAR T cells breaking the glass ceiling. Eur J Immunol. 2023;53(11). doi:10.1002/eji.202250039
172. Wang CY, Ting Cheung SP, Sugimura R. Combating challenges in CAR-T cells with engineering immunology. Front Cell Dev Biol. 2022;10. doi:10.3389/fcell.2022.969020
173. Kansagra A, Farnia S, Majhail N. Expanding access to chimeric antigen receptor T-cell therapies: challenges and opportunities. Am Soc Clin Oncol Educat Book. 2020;e27–e34. doi:10.1200/edbk_279151
174. Arnaudo L. On CAR-Ts, decentralized in-house models, and the hospital exception. Routes for sustainable access to innovative therapies. J Law Biosci. 2022;9(2). doi:10.1093/jlb/lsac027
175. McGrath E, Chabannon C, Terwel S, Bonini C, Kuball J. Opportunities and challenges associated with the evaluation of chimeric antigen receptor T cells in real-life. Curr Opin Oncol. 2020;32(5):427–433. doi:10.1097/CCO.0000000000000665
176. Bachmeier CA, Kurian TJ, Davila ML. Regulatory challenges and considerations for the clinical application of CAR T cell therapy. Expert Opin Biol Ther. 2021;21(5):549–552. doi:10.1080/14712598.2021.1887130
177. Lu X. Structural and Research Advances in CAR-T Cell Therapy. Theoret Nat Sci. 2023;3(1):200–205. doi:10.54254/2753-8818/3/20220232
178. Roselli E, Faramand R, Davila ML. Insight into next-generation CAR therapeutics: designing CAR T cells to improve clinical outcomes. J Clin Investig. 2021;131(2). doi:10.1172/JCI142030
179. Drokov MY, Gaponova TV, Gubenko TY, et al. Organisational and methodological challenges of CAR-T manufacturing in the Russian Federation. Biolog Prod Prev Diagn Treat. 2023;23(2):162–172. doi:10.30895/2221-996x-2023-23-2-162-172
180. Li Q, Wang K, Zhou J. Comprehensive Overview of CAR-T cell therapy, engineering process and future prospects. Highligh Sci Enginee Technol. 2023;36:376–384. doi:10.54097/hset.v36i.5706
181. Abraham AR, Maghsoudlou P, Copland DA, Nicholson LB, Dick AD. CAR-Treg cell therapies and their future potential in treating ocular autoimmune conditions. Frontiers in Ophthalmol. 2023;3. doi:10.3389/fopht.2023.1184937
182. Mulgaonkar A, Udayakumar D, Yang Y, et al. Current and potential roles of immuno-PET/-SPECT in CAR T-cell therapy. Front Med Lausanne. 2023:10. doi:10.3389/fmed.2023.1199146
183. Padmanjali DS, Revathi B, Jalaiah M. Revealing facts about CAR-T cell therapy. Immuno Analysis. 2022;2. doi:10.34172/ia.2022.06
184. Liu Q, Liu Z, Wan R, Huang W. Clinical strategies for enhancing the efficacy of CAR T-cell therapy for hematological malignancies. Cancers. 2022;14(18). doi:10.3390/cancers14184452
185. Ansah EO, Baah A, Agyenim EB. Vaccine boosting CAR-T cell therapy: current and future strategies. Adv Cell Gene Ther. 2023;2023:1–9. doi:10.1155/2023/8030440
186. Chen L, Chen F, Li J, et al. CAR-T cell therapy for lung cancer: potential and perspective. Thorac Cancer. 2022;13(7):889–899. doi:10.1111/1759-7714.14375
187. Chen H, Han Y, Liu K. CAR T-Cell Therapy: current Progress, Challenges and potential Strategies. Highligh Sci Enginee Technol. 2023;36:1001–1005. doi:10.54097/hset.v36i.6161
188. Kulczycka M, Derlatka K, Tasior J, Lejman M, Zawitkowska J. CAR T-Cell Therapy in Children with Solid Tumors. J Clin Med. 2023;12(6):2326. doi:10.3390/jcm12062326
189. Zhang K, Chen H, Li F, Huang S, Chen F, Li Y. Bright future or blind alley? CAR-T cell therapy for solid tumors. Front Immunol. 2023;14. doi:10.3389/fimmu.2023.1045024
190. Liu S, Zhang Y, Zhang Y. Challenges and interventions of chimeric antigen receptor-T cell therapy in solid tumors. Chin J Cancer Res. 2023;35(3):239. doi:10.21147/j.issn.1000-9604.2023.03.03
191. Yin L, Wan Z, Sun P, Shuai P, Liu Y. Time to abandon CAR-T monotherapy for solid tumors. Biochim Biophys Acta Rev Cancer. 2023;1878(4):188930. doi:10.1016/j.bbcan.2023.188930
192. Maalej KM, Merhi M, Inchakalody VP, et al. CAR-cell therapy in the era of solid tumor treatment: current challenges and emerging therapeutic advances. Mol Cancer. 2023;22(1). doi:10.1186/s12943-023-01723-z
193. Klobuch S, Seijkens TTP, Haanen JBAG. The emerging role for CAR T cells in solid tumor oncology. Chin Clin Oncol. 2023;12(2):19–19. doi:10.21037/cco-22-125
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.