")
Back to Journals » International Journal of General Medicine » Volume 15
Revising Vital Signs Criteria for Accurate Triage of Older Adults in the Emergency Department
Authors Su YC, Chien CY , Chaou CH , Hsu KH , Gao SY, Ng CJ
Received 4 May 2022
Accepted for publication 8 July 2022
Published 20 July 2022 Volume 2022:15 Pages 6227—6235
DOI https://doi.org/10.2147/IJGM.S373396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yi-Chia Su,1,2 Cheng-Yu Chien,1– 5 Chung-Hsien Chaou,1,2 Kuang-Hung Hsu,1,2,6,7 Shi-Ying Gao,1 Chip-Jin Ng1,2
1Department of Emergency Medicine, Chang Gung Memorial Hospital, Taoyuan, Taiwan; 2College of Medicine, Chang Gung University, Taoyuan, Taiwan; 3Department of Emergency Medicine, Ton-Yen General Hospital, Zhubei, Taiwan; 4Graduate Institute of Management, Chang Gung University, Taoyuan, Taiwan; 5Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taipei, Taiwan; 6Laboratory for Epidemiology, Chang Gung University, Taoyuan, Taiwan; 7Department of Urology, Chang Gung Memorial Hospital, Taoyuan, Taiwan
Correspondence: Chip-Jin Ng, Department of Emergency Medicine, Chang Gung Memorial Hospital Linkou, No. 5 Fushing St., Gueishan Dist., Taoyuan, 333, Taiwan, Tel +886-3-3281200 # 2505, Fax +886-3-3287715, Email [email protected]
Objective: Because of physiologic changes in older adults, their vital signs need to be assessed differently. This study aimed to determine appropriate vital sign cut points for triage designation in older patients presented to the emergency department (ED).
Patients and Methods: Data from 78,524 ED visits of patients aged ≥ 65 years in Linkou Chang Gung Memorial Hospital (LCGMH) between 2016 and 2017 were collected. New cut points for vital signs (systolic blood pressure [SBP], heart rate [HR], body temperature [BT], and Glasgow Coma Scale [GCS]) were determined using the critical event rate (the composite of admission to ICU and mortality in hospital) for each vital sign. The newly proposed triage scale was then validated using two other databases (Chang Gung Research Database [CGRD] and Taipei City Hospital [TPECH] database). The Taiwan Triage and Acuity Scale (TTAS) was used in this study.
Results: In the LCGMH derivation group, older patients presenting with SBP < 80 mmHg, HR < 40 or > 140 beats per minute (bpm), BT < 35°C, and GCS score 3– 8 had a critical event rate of > 20% and were proposed to be uptriaged to TTAS level 1. Following a reclassification, a portion of older patients are uptriaged by the newly proposed TTAS, and increase in the critical event rate in TTAS level 1 and level 2 groups compared to the existing TTAS. The newly proposed TTAS exhibited comparable discriminatory ability for triage in older patients compared to the existing TTAS (the area under the receiver operating characteristics curve: CGRD, 0.76 vs 0.62; TPECH, 0.71 vs 0.59).
Conclusion: Revising the vital signs triage criteria for older patients could be a way to improve the identification of patients with critical event outcomes in high TTAS level, thereby improving triage accuracy among older patients visiting the ED.
Keywords: older patients, emergency department, triage, vital signs, decision-making
Introduction
The proportion and frequency of older adults (age ≥ 65 years)1–3 visiting the emergency Department (ED) has been increasing.4–6 Moreover, they have longer ED stays and higher readmission rates than the general adult population.7 These patients have various comorbidities and varying degrees of cognitive impairment and disability, thereby necessitating special and additional attention in the ED.4
In the ED, triage is a process of prioritising patients based on the urgency of care required.8 In the Canadian Triage and Acuity Scale (CTAS), CTAS-based triage systems such as Japanese TAS (JTAS) and Taiwan TAS (TTAS),8–11 triage assignment is mainly based on the presenting complaint along with a specific set of first- and second-order modifiers to accurately determine the triage acuity level. Vital signs are common first-order modifiers in triage systems. Traditional vital signs include blood pressure (BP), body temperature (BT), heart rate (HR), and respiratory rate. However, other factors crucial for determining the patients’ well-being can be considered vital signs, including the Glasgow Coma Scale (GCS) score and pain severity.12
As objective measures of physiological function, vital signs are used to monitor acute and chronic diseases and thus serve as a universal communication tool about patient status.13 However, normal vital signs are subjective and vary with age and many other factors.12 In older patients, homeostatic mechanisms change with age, leading to difficulties in maintaining internal physiological consistency.4,13 Consequently, vital sign changes in older patients may be subtle because of reduced physiological ranges and inability to respond appropriately to stressors.13 When overlooked or misinterpreted, older patients are at a higher risk of undertriage and delay in intervention, potentially causing deterioration of their condition.14 Therefore, vital signs in older patients should be carefully interpreted.
Our recent study has found that the capacity of TTAS to predict mortality in hospitals was less accurate for older adults than for general adult population.3 As we attempt to improve our overall ED care for older patients, triage is the first critical step in that process. Few studies have compared the cut points of vital signs between older adults and the general adult population, especially in Asian populations. This database study aimed to determine new vital sign thresholds as first modifiers for an improved triage in older ED patients. This would identify those who are at risk of deterioration during prolonged waiting, so that early intervention could be given promptly by uptriaging them.
Materials and Methods
Study Setting and Databases
This retrospective cohort study was conducted between January 2016 and December 2017. The study was reviewed and approved by the Institutional Review Boards of Chang Gung Memorial Hospital (CGMH) (202000012BOC503) and Taipei City Hospital (TPECH) (TCHIRB-10911003-E), and the need for informed consent was waived. This study was conducted in compliance with the principles of the Declaration of Helsinki.
Data from two databases, the Chang Gung Research Database (CGRD) and the TPECH database, were used. The CGRD contains the multi-institutional standardised electronic medical records (EMRs) from seven CGMHs, namely two medical centres, two regional hospitals, and three district hospitals in Taiwan, of which Linkou branch of CGMH (LCGMH) is the largest.15 LCGMH is a multispecialty medical centre accredited by Joint Commission International and has a 3600-bed capacity and approximately 180,000 ED patient visits per year. TPECH is a municipal hospital with ten branches in Taipei city; of them, two tertiary and three community general hospitals provide emergency services with an average annual number of ED visits of approximately 220,000. Both the TPECH database and the CGRD regularly collect basic information and medical records from ED patients and provide deidentified data for research use.
For model derivation, we used the deidentified data obtained from the EMRs of the ED of the LCGMH, Taiwan, stored in the CGRD. While deidentified data from the EMRs of the ED from the other six CGMHs stored in the CGRD were used for model internal validation.
For model external validation, deidentified data from the EMRs of the ED of TPECH, Taiwan, were used. Our study used data from the two tertiary hospitals in the TPECH network, which account for 60% of TPECH emergency visits.
TTAS
The TTAS is a validated five-level triage system developed based on CTAS.8 It has been modified from the CTAS by shortening the reassessment time, dividing the chief complaint list into two domains (non-trauma and trauma), and further categorising the complaint using anatomical region and environmental injury. Vital sign ranges for hemodynamic stability and pain severity ratings have also been modified. The computerised TTAS (eTTAS) links the standardised list of presenting complaints to the relevant triage scale modifiers and supports the user in assigning the appropriate triage score based on the complaint selected. In the TTAS, triage levels are categorised as follows: level 1, resuscitation; level 2, emergency; level 3, urgent; level 4, less urgent; and level 5, nonurgent. Patients are evaluated and then assigned a triage level by a triage nurse.8,16 In the current TTAS, patients presenting with SBP < 70 mmHg, BT < 32 °C or > 41 °C, and GCS score of 3–8 are to be triaged as TTAS level 1; patients presenting with SBP < 90 mmHg, HR < 50 bpm or >140 bpm, and GCS score of 9–13 are to be triaged as TTAS level 2 (see Supplementary Table 1).
Patient Inclusion, Data Collection, and Outcome Measurement
Older patients (age ≥ 65 years) presenting to the ED between January 2016 and December 2017 were selected. Patients whose vital sign measurement values seemed implausible or to be outliers (0.05% of the data at the tails) were excluded. We also excluded those with out-of-hospital cardiac arrest. The same inclusion and exclusion criteria were applied to the derivation (LCGMH) and validation (CGRD and TPECH) groups.
Patient demographic data (eg, sex and age), vital signs at triage (eg, systolic BP [SBP], HR, BT, respiratory rate, blood oxygen saturation, and GCS), and triage assignments based on the TTAS were collected. The outcome measurements were composite of direct admission to ICU from ED and mortality in hospital following the ED visit (referred to as a critical event as a whole). An expert panel consisting of three senior emergency physicians and two statisticians was formed to discuss the analytic process and the cut points derived.
Statistical Analysis
Categorical variables were presented as counts and percentages and were compared using the chi-squared test or Fisher’s exact test, as appropriate. Continuous variables were presented as means and standard deviations (SDs). Student’s t-test and the Mann–Whitney U-test were used for normally and nonnormally distributed continuous variables, respectively. For model derivation using the LCGMH group, bar charts were used to display the distributions of critical event rates in every category within modifiers, including SBP, HR, BT, and GCS, to determine the new cut points for these modifiers in triage of older patients.
In general, the cut points for the modifiers were decided as follows based on the results of distribution of critical events in each vital sign parameter in the LCGMH derivation group and past studies: (1) an identified critical event rate of 20% or above was proposed to be classified to TTAS level 1; (2) an identified critical event rate of approximately 10–20% was proposed to be classified to TTAS level 2; and (3) a major elevation or drop of the critical event rate or admission rate may be considered as a cut point under the expert panel consensus.4,8,9,16
Subsequently, the validity of the revised TTAS was examined using the CGRD and TPECH validation groups. A reclassification concept was applied which we re-triaged the patients using the newly proposed cut points for vital signs determined in our study. Bar charts were used to compare the difference in the critical event rate between the current TTAS and newly proposed TTAS (reclassification). The area under the receiver operating characteristic curve (AUROC) with 95% confidence interval (CI) was determined to evaluate the discriminative ability of the current TTAS and newly proposed TTAS in predicting critical events in older patients.
Results with p < 0.05 were considered statistically significant. The data were analysed using SAS software (version 9.4 for Windows, SAS Institute, Cary, North Carolina, USA). Missing data was not imputed and was not included in analyses.
Results
Figure 1 depicts the case selection flow diagram of the LCGMH derivation group. The LCGMH derivation group comprised 357,715 ED presentations between January 2016 and December 2017. After excluding patients aged <65 years and those with vital sign outliers, 78,524 cases were included for analysis. The patient characteristics of the LCGMH derivation group were as follows: 50.9% were male; mean (SD) age was 76.69 (8.17) years; 7.2% were TTAS level 1, 26.8% were TTAS level 2, and 59.8% were TTAS level 3; and 48.3% were admitted to general wards (Table 1). The validation groups comprised 54,541 cases from CGRD and 41,174 cases from TPECH under the same eligibility criteria as the LCGMH derivation group; Table 1 presents their baseline characteristics.
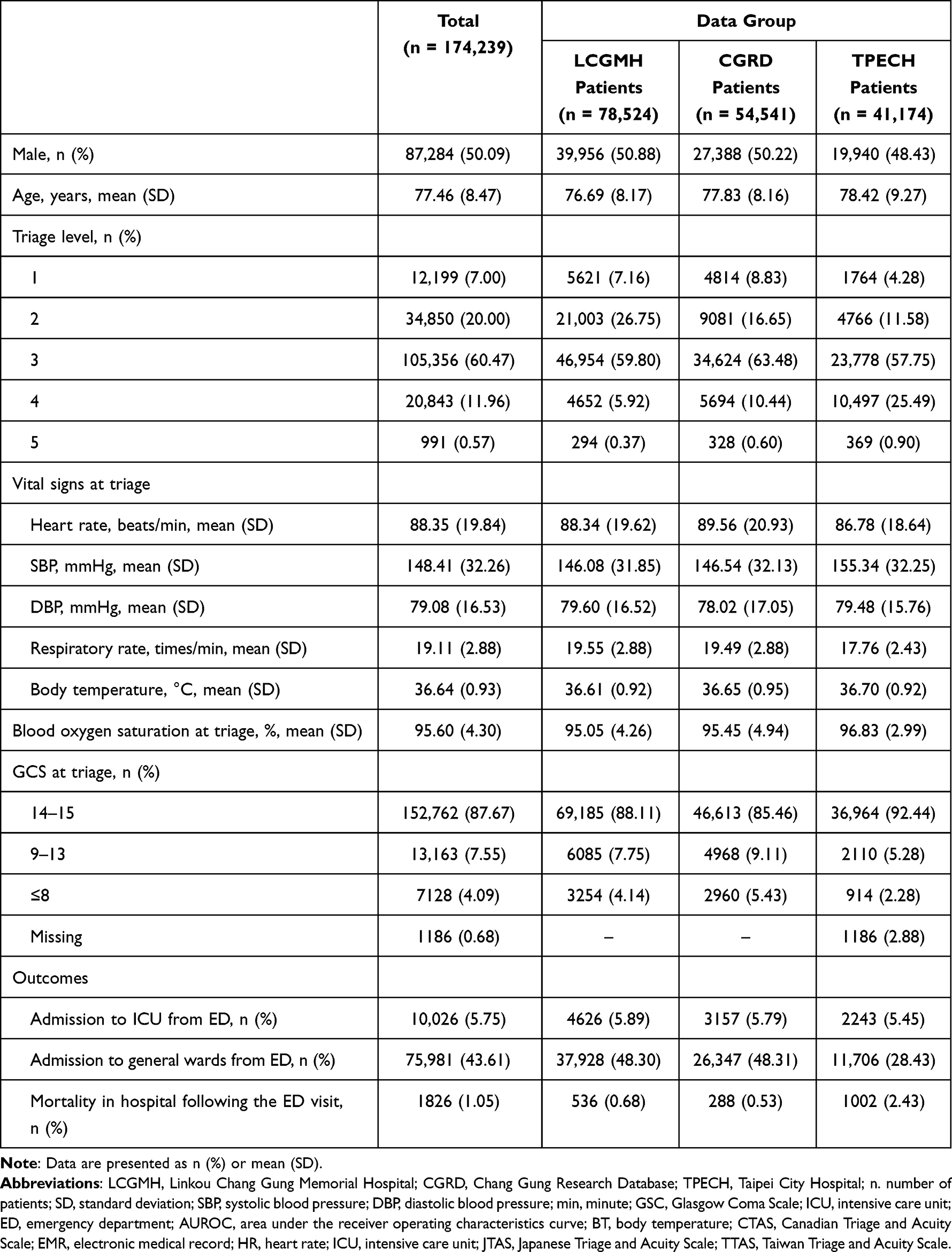 |
Table 1 Baseline Characteristics of the Patients |
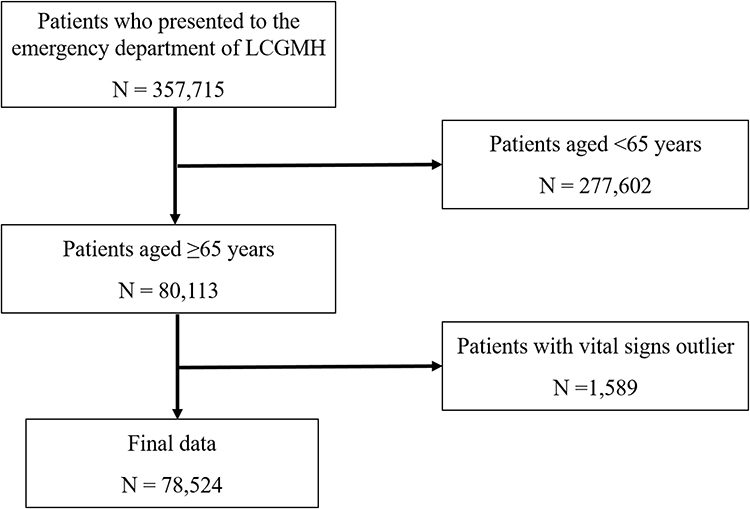 |
Figure 1 Flow diagram of patient selection in the LCGMH derivation group. Abbreviation: LCGMH, Linkou Chang Gung Memorial Hospital. |
Figure 2 illustrates the changes in the distribution of the critical event rate in every category for SBP, HR, BT, and GCS, in the LCGMH derivation group. The critical event rate was >50% when the patients presented with BT < 32 °C and GCS score of 3. The critical event rate was >20% when the patients presented with SBP < 80 mmHg, HR < 40 or > 140 bpm, BT < 35 °C, and GCS score of 3–8. A superimposed line graph represented the logged incidence rate of each interval category.
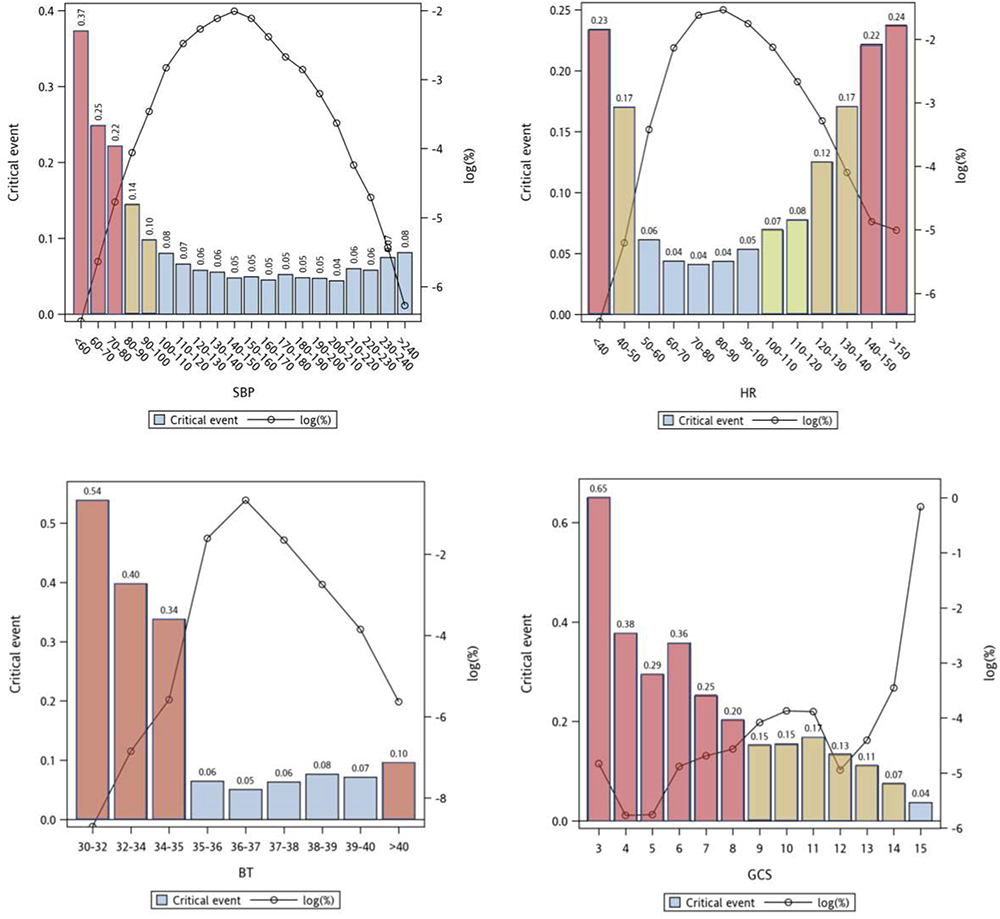 |
Figure 2 Critical event rate in every category for SBP, HR, BT, and GCS in the LCGMH derivation group. The vertical bars were critical event rates (the composite of admission to ICU and mortality in hospital). The superimposed line graph represented the logged incidence rate in each category. Red bar (TTAS 1); Brown bar (TTAS 2); Green bar (TTAS 3). Abbreviations: SBP, systolic blood pressure; HR, heart rate; BT, body temperature; GCS, Glasgow Coma Scale; ICU, intensive care unit; LCGMH, Linkou Chang Gung Memorial Hospital. |
On the basis of Figure 2, new cut points for the first-order modifiers were proposed for triage in older patients (Supplementary Table 1). For the newly proposed TTAS, patients presenting with SBP < 80 mmHg, HR < 40 bpm or >140 bpm, BT < 35 °C, and GCS score of 3–8 were classified as TTAS level 1; patients presenting with SBP 80–100 mmHg, HR of 40–50 bpm or 120–140 bpm, BT of > 40 °C, and GCS score of 9–14 were classified as TTAS level 2. The critical event rate under the existing TTAS and the newly proposed TTAS in the LCGMH group after reclassification is shown in Supplementary Figure 1.
The critical event rate and AUROC were compared between the existing TTAS and newly proposed TTAS for triage in older patients using the CGRD (Figure 3) and TPECH (Figure 4) validation groups after reclassification. The newly proposed TTAS increase in the critical event rate in both triage levels 1 (current vs newly proposed: CGRD, 23% vs 26%; TPECH, 20% vs 21%) and 2 (CGRD, 8% vs 12%; TPECH, 9% vs 11%) compared to the current TTAS. The critical event rate in triage levels 3–5 was comparable between the newly proposed TTAS and the current TTAS. The AUROC for critical events was comparable between the newly proposed TTAS and the current TTAS in both CGRD (0.62 [95% CI: 0.61–0.63] vs 0.76 [95% CI: 0.75–0.77], p = 0.0006) and TPECH (0.59 [95% CI: 0.58–0.60] vs 0.71 [95% CI: 0.70–0.72], p < 0.0001) validation groups.
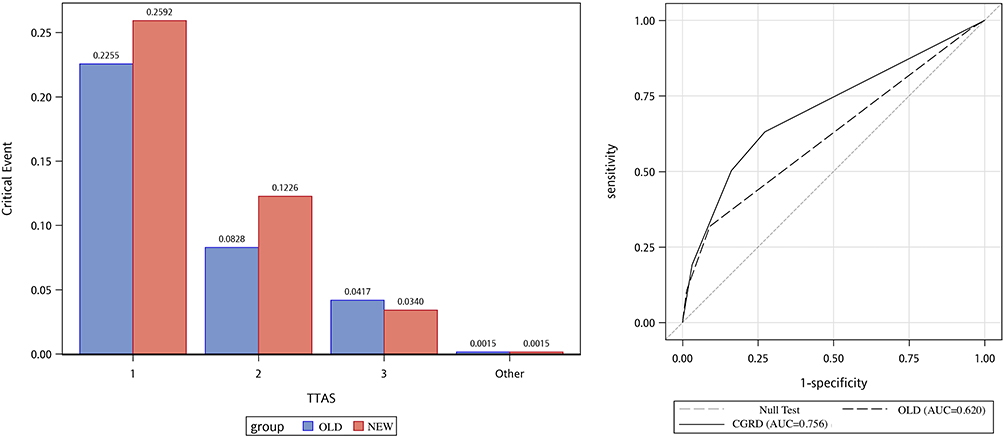 |
Figure 3 Comparisons of critical event rate (the composite of admission to ICU and mortality in hospital) and ROC curve for predicting critical event between the existing TTAS and the newly proposed TTAS in the CGRD validation group. Abbreviations: TTAS, Taiwan Triage and Acuity Scale; CGRD, Chang Gung Research Database; ICU, intensive care unit; ROC, receiver operating characteristics curve. |
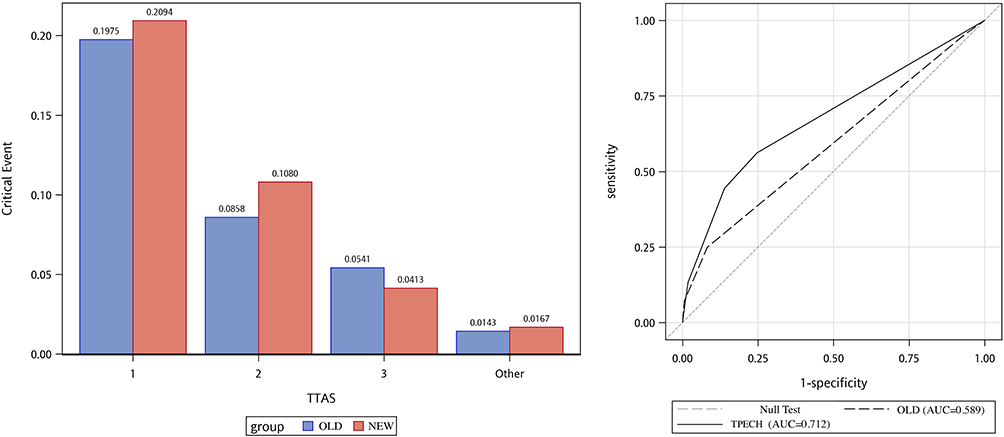 |
Figure 4 Comparisons of critical event rate (the composite of admission to ICU and mortality in hospital) and ROC curve for predicting critical event between the existing TTAS and the newly proposed TTAS in the TPECH validation group. Abbreviations: TTAS, Taiwan Triage and Acuity Scale; TPECH, Taipei City Hospital; ROC, receiver operating characteristics curve; ICU, intensive care unit. |
Discussion
This study determined newer cut points for vital signs, thereby improving triage accuracy in older patients. Following a reclassification using the newly proposed TTAS, a portion of older patients are uptriaged, and increase in the critical event rate in TTAS levels 1 and 2 groups compared to the existing TTAS. The newly proposed TTAS demonstrate a notable improvement in the discriminative ability for critical events and avoid under-triage initially in older patients.
Overall, triage systems are designed to screen all adult patients evenly, despite heterogeneity. However, older patients have a higher mortality rate across all triage levels, and the association with age was stronger in the lowest triage (ie, nonurgent) group.17 Another study using JTAS reported that its discriminative ability decreased with an increase in patient age (AUROC from 0.85 to 0.71).18 The validation study of JTAS in older patients reported an AUROC of 0.69 for overall admission.11 In our study, the discriminative ability of the existing TTAS for critical events as measured using AUROC was 0.59–0.62 in older patients. After revising the cut points for vital signs, approximately 10% of the older patients were uptriaged to TTAS level 1 or 2, and the discriminative ability of the newly proposed TTAS for critical events in older patients showed trend of improvement to 0.71–0.76. Our study uptriage older patients using newly proposed TTAS due to high critical event rate in high TTAS level. This suggests that vital signs modifiers may help improve the triage accuracy. Other factors, such as frailty status,4,9 should be taken into consideration when trying to improve triage for older people.
Age-related molecular changes cumulatively result in altered sensitivity, reliability, and normative ranges of cardiovascular vital signs (ie, SBP and HR).13 A 5-year review of presenting physiology demonstrated an inflection point for the association between the risk of death and SBP at 110 mmHg in older patients.5 Using SBP < 110 mmHg as a criterion greatly reduced under-triage in older patients.19 Our study found that the critical event rate was more than 10% in older patients with SBP < 100 mmHg, revealing that low BP in older patients may be more critical than previously considered and should be given special attention. This finding is supported by a study reporting that low BP was independently associated with mortality and admission in older patients.20 Therefore, we proposed to revise the SBP cut points of <80 mmHg and 80–100 mmHg as TTAS level 1 and 2 criteria, respectively, according to their associated rate of critical events. We also proposed revising the HR cut points of <40 or >140 bpm and 40–50 or 120–140 bpm as TTAS level 1 and 2 criteria, respectively, according to their associated rate of critical events. The newly proposed TTAS criteria of HR < 40 bpm and 40–50 bpm is consistent with the National Early Warning Score.21
Ageing causes changes in the thermoregulatory system.13 Because of decreased metabolic rates and alterations to the hypothalamus, older people tend to have lower core BT and altered thermoregulatory response.4,13 Fever (defined as an oral temperature of ≥ 37.8 °C) is often absent in benign infections, and temperature is lower in severe infections of approximately 25% of older adults compared with the general population.22 Therefore, a subtle increase in BT could be as significant a finding as fever and is associated with increased rates of serious clinical outcomes in older patients.13 The present study revealed that the critical event rate was more than 30% for BT < 35 °C. We proposed revising the BT cut points of < 35 °C and > 40°C as TTAS level 1 and 2 criteria, respectively, according to their associated rate of critical events.
The critical event rate was >60% in patients with GCS scores of 3. A gradual decrease in the critical event rates (from 65% to 20%) was observed when the GCS score was increased from 3 to 8. According to their associated rate of critical events, we proposed to maintain the GCS score cut points of 3–8 as TTAS level 1 and revising the GCS score cut points of 9–14 as TTAS level 2 criteria. These revisions are in agreement with the results of previous studies.23–25 The modified JTAS considers GCS ≤ 9 as level 1.23 The Ohio emergency medical service system changed its trauma triage cutoff for older adults from a GCS score of 13 to 14.24 Revising GCS scores from 13 to 14 for older patients may improve the identification of those with serious injuries.25
Respiratory rate is a significant vital sign. In the current TTAS, patients with a respiratory rate of <10 times per minute are to be triaged as level 1. Our result of respiratory rate and critical event rate (Supplementary Figure 2) supported the current cut point and hence did not propose to revise it. In addition, patients with an oxygen saturation of <90% are to be triaged as level 1 in the current TTAS. Our result of oxygen saturation and critical event rate (Supplementary Figure 3) supported the current cut point and hence did not propose to revise it.
Strengths and Limitations
The major strength of this study was the number of patients included and the validation of its results by using two multicentre cohort databases. Nonetheless, our study had some limitations. First, selection bias may have been introduced due to its retrospective nature. The generalizability of the study results may be limited due to the varying baseline characteristics of ED patients in other settings or countries, as well as different hospital levels and low-volume hospitals. Second, the main purpose of the TTAS is to identify medical urgency among ED patients but not to predict critical event outcomes, such as admission to ICU, and mortality. However, validating a triage system is difficult because no gold standard exists for assessing the degree of medical urgency.26 Therefore, in this study, a surrogate marker, namely the critical event rate, was used to assess the validity of the TTAS in older patients. Third, respiratory rate is measured through direct observation by the triage nurse and may often be inaccurate due to subjective judgment and vary in respiratory pattern.27 Fourth, the revised triage system enables uptriage of older ED patients using the new vital signs modifiers to prevent or improve clinical outcomes due to possible under-triage by the current triage system. However, there is a possibility that some older ED patients assigned with a lower triage level (particularly levels 4–5) based on chief complaints and could not be uptriaged using the vital signs modifier are at risk of clinical deterioration and need for critical care. Fifth, longitudinal vital-sign data were not used in the present study; the added value of trajectories of vital signs on triage or critical event prediction is yet to be characterized.28
Conclusions
Our study demonstrated a process to renew the cut points of vital signs within a triage system and proposed new triage criteria for older patients. The newly proposed TTAS uptriages older ED patients and therefore enable them to access early medical intervention and prevents them from further clinical deterioration, thereby improving waiting time and the critical event rate. Revising vital signs criteria seems to be a pragmatic way to improve the triage of older ED patients by resolving under-triage issues in the existing triage system.
Data Sharing Statement
All data relevant to the study are included in the article or uploaded as Supplementary Information.
Ethics Approval and Consent to Participate
The study was reviewed and approved by the Institutional Review Board of Chang Gung Memorial Hospital (202000012BOC503) and Taipei City Hospital (TCHIRB-10911003-E), and the need of informed consent was waived.
Acknowledgments
We would like to thank Wallace Academic Editing for proofreading this manuscript. Cheng-Yu Chien contributed equally to this article with Chip-Jin Ng.
Disclosure
The authors report no conflicts of interest in this work.
References
1. United Nations, Department of Economic and Social Affairs. World population ageing 2019 highlights. Available from: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf.
2. Lee SB, Oh JH, Park JH, Choi SP, Wee JH. Differences in youngest-old, middle-old, and oldest-old patients who visit the emergency department. Clin Exp Emerg Med. 2018;5(4):249–255. doi:10.15441/ceem.17.261
3. Chien CY, Chaou CH, Yeh CC, Hsu KH, Gao SY, Ng CJ. Using mobility status as a frailty indicator to improve the accuracy of a computerised five-level triage system among older patients in the emergency department. BMC Emerg Med. 2022;22(1):86. doi:10.1186/s12873-022-00646-0
4. Bullard MJ, Melady D, Emond M, et al. Guidance when applying the Canadian Triage and Acuity Scale (CTAS) to the geriatric patient: executive summary. CJEM. 2017;19(Suppl 2):S28–S37. doi:10.1017/cem.2017.363
5. Heffernan DS, Thakkar RK, Monaghan SF, et al. Normal presenting vital signs are unreliable in geriatric blunt trauma victims. J Trauma. 2010;69(4):813–820. doi:10.1097/TA.0b013e3181f41af8
6. Pham KD, Lim FA. The impact of geriatric-specific triage tools among older adults in the emergency department. Crit Care Nurs Q. 2020;43(1):39–57. doi:10.1097/CNQ.0000000000000290
7. Šteinmiller J, Routasalo P, Suominen T. Older people in the emergency department: a literature review. Int J Older People Nurs. 2015;10(4):284–305. doi:10.1111/opn.12090
8. Ng CJ, Yen ZS, Tsai JC, et al. Validation of the Taiwan triage and acuity scale: a new computerised five-level triage system. Emerg Med J. 2011;28(12):1026–1031. doi:10.1136/emj.2010.094185
9. Bullard MJ, Musgrave E, Warren D, et al. Revisions to the Canadian Emergency Department Triage and Acuity Scale (CTAS) guidelines 2016. CJEM. 2017;19(Suppl 2):S18–S27. doi:10.1017/cem.2017.365
10. Bullard MJ, Unger B, Spence J, Grafstein E. Revisions to the Canadian Emergency Department Triage and Acuity Scale (CTAS) adult guidelines. CJEM. 2008;10(2):136–151. doi:10.1017/S1481803500009854
11. Kuriyama A, Kaihara T, Ikegami T. Validity of the Japan acuity and triage scale in elderly patients: a cohort study. Am J Emerg Med. 2019;37(12):2159–2164. doi:10.1016/j.ajem.2019.03.006
12. Hong W, Earnest A, Sultana P, Koh Z, Shahidah N, Ong ME. How accurate are vital signs in predicting clinical outcomes in critically ill emergency department patients. Eur J Emerg Med. 2013;20(1):27–32. doi:10.1097/MEJ.0b013e32834fdcf3
13. Chester JG, Rudolph JL. Vital signs in older patients: age-related changes. J Am Med Dir Assoc. 2011;12(5):337–343. doi:10.1016/j.jamda.2010.04.009
14. Wolf L. How normal are “normal vital signs”? Effective triage of the older patient. J Emerg Nurs. 2007;33(6):587–589. doi:10.1016/j.jen.2007.09.006
15. Shao SC, Chan YY, Kao Yang YH, et al. The Chang Gung Research Database-A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol Drug Saf. 2019;28(5):593–600. doi:10.1002/pds.4713
16. Ng CJ, Chien CY, Seak JC, et al. Validation of the five-tier Taiwan triage and acuity scale for prehospital use by emergency medical technicians. Emerg Med J. 2019;36(8):472–478. doi:10.1136/emermed-2018-207509
17. Ruge T, Malmer G, Wachtler C, et al. Age is associated with increased mortality in the RETTS-A triage scale. BMC Geriatr. 2019;19(1):139. doi:10.1186/s12877-019-1157-4
18. Kuriyama A, Ikegami T, Nakayama T. Impact of age on the discriminative ability of an emergency triage system: a cohort study. Acta Anaesthesiol Scand. 2019;63(6):781–788. doi:10.1111/aas.13342
19. Brown JB, Gestring ML, Forsythe RM, et al. Systolic blood pressure criteria in the National Trauma Triage Protocol for geriatric trauma: 110 is the new 90. J Trauma Acute Care Surg. 2015;78(2):352–359. doi:10.1097/TA.0000000000000523
20. Morrissey Y, Bedford M, Irving J, Farmer CK. Older people remain on blood pressure agents despite being hypotensive resulting in increased mortality and hospital admission. Age Ageing. 2016;45(6):783–788. doi:10.1093/ageing/afw120
21. Kim I, Song H, Kim HJ, et al. Use of the National early warning score for predicting in-hospital mortality in older adults admitted to the emergency department. Clin Exp Emerg Med. 2020;7(1):61–66. doi:10.15441/ceem.19.036
22. Blatteis CM. Age-dependent changes in temperature regulation - a mini review. Gerontology. 2012;58(4):289–295. doi:10.1159/000333148
23. Funakoshi H, Shiga T, Homma Y, et al. Validation of the modified Japanese triage and acuity scale-based triage system emphasizing the physiologic variables or mechanism of injuries. Int J Emerg Med. 2016;9(1):1. doi:10.1186/s12245-015-0097-9
24. Caterino JM, Raubenolt A, Cudnik MT. Modification of Glasgow coma scale criteria for injured elders. Acad Emerg Med. 2011;18(10):1014–1021. doi:10.1111/j.1553-2712.2011.01164.x
25. Newgard CD, Richardson D, Holmes JF, et al. Physiologic field triage criteria for identifying seriously injured older adults. Prehosp Emerg Care. 2014;18(4):461–470. doi:10.3109/10903127.2014.912707
26. Kuriyama A, Urushidani S, Nakayama T. Five-level emergency triage systems: variation in assessment of validity. Emerg Med J. 2017;34:703–710. doi:10.1136/emermed-2016-206295
27. Kallioinen N, Hill A, Christofidis MJ, Horswill MS, Watson MO. Quantitative systematic review: sources of inaccuracy in manually measured adult respiratory rate data. J Adv Nurs. 2021;77(1):98–124. doi:10.1111/jan.14584
28. Naemi A, Schmidt T, Mansourvar M, Naghavi-Behzad M, Ebrahimi A, Wiil UK. Machine learning techniques for mortality prediction in emergency departments: a systematic review. BMJ Open. 2021;11(11):e052663. doi:10.1136/bmjopen-2021-052663
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.