")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 10
Review Of The Safety, Efficacy And Tolerability Of Fingolimod In The Treatment Of Pediatric Patients With Relapsing-Remitting Forms Of Multiple Sclerosis (RRMS)
Received 2 August 2019
Accepted for publication 16 September 2019
Published 12 November 2019 Volume 2019:10 Pages 141—146
DOI https://doi.org/10.2147/PHMT.S220817
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Video abstract presented by Jenny Feng.
Views: 509
Jenny Feng, Mary Rensel
Mellen Center for Multiple Sclerosis Treatment and Research, Cleveland Clinic, Cleveland, OH, USA
Correspondence: Mary Rensel
Mellen Center for Multiple Sclerosis Treatment and Research, Cleveland Clinic, 9500 Euclid Ave. U10, Cleveland, OH 44195, USA
Tel +1 216 444 8631
Fax +1 216 445 7013
Email [email protected]
Abstract: Pediatric-onset multiple sclerosis (POMS) is an immune-mediated, demyelinating, neurodegenerative disease that accounts for 3–5% of all multiple sclerosis (MS) cases. Although evidence suggests that it has similar risk factors and disease pathophysiology as adult-onset MS (AOMS), there are distinctive features in disease characteristics and patient demographics of POMS that require unique therapeutic development and treatment considerations. Gilenya® (Novartis International AG, Basel, Switzerland) (fingolimod) is a sphingosine-1-phosphate (S1P) receptor modulator that prevents lymphocytic outflow from peripheral lymph nodes. It has demonstrated efficacy in AOMS. In POMS, there have been three observational studies and one pivotal clinical trial evaluating the efficacy, safety, and tolerability of fingolimod. Currently, fingolimod is the only Food and Drug Administration and European Medicines Agency approved disease-modifying therapy to treat POMS. This review will critically evaluate the available evidence of fingolimod in the treatment of POMS in detail, as well as discussing its treatment implications.
Keywords: disease-modifying therapy, demyelinating disease, S1P receptor modulator, neuroimmunology, pediatric onset multiple sclerosis
Introduction
Multiple sclerosis (MS) is an immune-mediated, demyelinating, neurodegenerative disease involving the central nervous system (CNS). Typically, MS onset occurs between second and fourth decade of life, however, earlier onset of MS is becoming increasingly recognized, with 3–5% of all MS cases occurring in childhood or adolescence.1–3 Pediatric-onset multiple sclerosis (POMS) is defined as onset of disease prior to 18 years of age. Most commonly POMS is seen in adolescence, however, it has been reported in children younger than 10 years old, accounting for <1% of all MS cases.4 The estimated prevalence of POMS is 2.7–10.5%5 and estimated incidence is 0.3/100,000–1.8/100,000.6–8
Between POMS and adult-onset MS (AOMS), there are differences in non-age-related demographic characteristics, susceptibility to various risk factors, disease course, and symptomatology that warrant unique treatment considerations. It has been shown that similar genetic and environmental factors contribute to risks for both AOMS and POMS; for example, HLA-DRB1 allele, vitamin D deficiency, Epstein-Barr virus (EBV) seropositivity, and cigarette smoke exposure were associated with an increased risk for MS in numerous epidemiological studies.9,10 Unique to POMS, however, is the higher frequency of HLA-DRB alleles compared to AOMS, greater effect of environmental factors during adolescence on future MS risk (such as EBV infection, vitamin D levels and sun exposure, and obesity), and the effect of puberty on MS development.10–12 Although there is no clear evidence that POMS is an entirely distinct disease from AOMS in terms of underlying pathophysiology,13 it has been demonstrated that autoimmune responses in POMS patients may be as robust or stronger than those seen in AOMS patients.14,15 The developing nervous system in children and adolescents and immaturity of the immune system may also affect susceptibility of the pediatric population to immune-mediated diseases. The phenomenon of more prominent clinical-radiographic dissociation in POMS as compared to AOMS supports the theory that pediatric brains embody greater CNS reserve and repair capabilities.13 There is also an age-dependent positive correlation with female:male ratio in POMS, seen especially after puberty, suggestive of the hormonal changes that may affect MS risk susceptibility.16 In conclusion, the differences between POMS and AOMS pose therapeutic challenges that require modifications in both clinical trial design and treatment implementation that take into consideration the unique immune profile and developmental neurobiology of POMS patients.
Disease-modifying therapies (DMT) in MS are immunomodulatory agents that reduce relapse rate, lesion burden, and delay disability progression. Injectable therapies, which comprise of interferons and glatiramer acetate, have been approved by the European Medicines Agency (EMA) to treat POMS patients older than 12 years of age. In the United States, they are also considered as standard first-line DMTs in POMS despite lack of Food and Drug Administration (FDA) approval specifically for POMS. They have been shown to be safe and effective in POMS through results of numerous observational studies, unblinded, and small blinded randomized controlled trials.17 Gilenya® (Novartis International AG, Basel, Switzerland) (fingolimod) is an orally administered DMT that originally received FDA approval to treat relapsing AOMS in 2010. It is a sphingosine-1-phosphate (S1P) receptor modulator which promotes the entrapment of circulating peripheral lymphocytes in lymph nodes, thus effectively preventing their entry into the CNS and subsequent inflammatory action. Fingolimod received FDA approval in May 2018 to treat POMS in children 10 years and older, and EMA approval in November 2018 to treat children 10-17 years old with relapsing-remitting MS becoming the first DMT indicated specifically for POMS. The rest of this review will focus on discussing the safety, efficacy, and tolerability profile of fingolimod in the POMS population.
Fingolimod Experience In POMS
Observational Studies
Prior to the randomized controlled PARADIGMS trial,18 fingolimod experience in POMS population has been limited to small observational studies. A German study by Huppke et al, involving highly active POMS patients on either natalizumab or fingolimod published in 2017, analyzed relapse rate and MRI data (including T2-weighted and gadolinium-enhancing lesion number) prior to therapy initiation and at follow-up visits in 6-month intervals up to 18 months post-treatment.19 There were a total of 23 POMS patients in the fingolimod group with available data. Compared to the general POMS population, the 23 patients in this study had clinical characteristics indicative of more highly active disease (greater number of T2 and/or gadolinium-enhancing lesions, more frequent relapses). Compared to pre-treatment, there was 75% reduction in relapse rate, 81% reduction in new T2 lesion formation, and 93% reduction in new gadolinium-enhancing lesions post-treatment. There were 7 patients who did experience increase in disease activity after switching to fingolimod, however, they were all younger patients with more aggressive disease at onset and were only switched from natalizumab to fingolimod due to prolonged treatment duration and John Cunningham Virus (JCV) seropositivity. There were no adverse cardiac events or any serious side effects while on fingolimod reported in this cohort. Of the side effects that were observed, there were transient cases of lymphopenia and cough, as well as urinary tract infection and leg paresthesia. Compared to a historical cohort from 2005, the combined group comprised of POMS patients on either natalizumab or fingolimod in this more contemporary cohort experienced lower relapse rate (46% reduction) and had lower Expanded Disability Status Scale (EDSS) scores (44% reduction, lower scores confer less disability).
The other observational study of fingolimod in POMS was published by Fragoso et al in 2015.20 Descriptive data from 17 POMS patients who were treated with fingolimod before the age of 18 were reported. The POMS patients were treated with fingolimod for an average of 8.6 months (range 1–18 months). A majority of patients (94%, or 16/17 patients) did not experience further relapses either clinically or radiographically. Only 1 patient experienced a clinical relapse and had 1 new cerebellar lesion on MRI 14 months post-treatment-initiation. In this group, there was an improvement in average EDSS score compared to pre-treatment data, with 8 patients maintaining the same EDSS score and 9 patients with improved EDSS scores (range of change −3 to −0.5). No adverse cardiac events were observed with first dose and no lymphopenia or macular edema were reported during periods of treatment. There were single cases of genital herpes and upper respiratory infection, and 2 cases of urinary tract infection.
Most recently Egyptian registry data of 186 POMS patients were published by Hamdy et al in 2018.21 In this registry, there were a total of 8 patients treated with fingolimod (3 treated within 1 year of symptom onset and 6 treated after more than a year of symptoms since onset). 2 of the 8 patients had altered liver function tests leading to 1 patient eventually discontinuing fingolimod, and 2 patients had abnormal blood counts with 1 patient discontinuing fingolimod as well.
Case Report
Rebound of disease activity following fingolimod discontinuation has been reported in AOMS.22–24 To date, there is 1 case report of disease rebound post-fingolimod-discontinuation in POMS. The patient in the case report was diagnosed with POMS at age 11, and had breakthrough disease activity on interferon beta. After switching to fingolimod, she continued to have clinical and radiographic relapses, resulting in fingolimod discontinuation for lack of efficacy. Fifty days following fingolimod discontinuation, she experienced a more severe relapse with significantly increased number of enhancing and non-enhancing lesions on MRI of brain and spinal cord.25
Clinical Trial
Currently, there is only 1 published pivotal trial which evaluated efficacy of fingolimod in POMS. The PARADIGMS study is a randomized, multicenter, double-blind, double-dummy, active-controlled, parallel-group trial that compared efficacy of fingolimod against interferon beta-1a in POMS.18 Patients enrolled in PARADIGMS had confirmed POMS, were 10–17 years old, with EDSS scores ranging from 0.0 to 5.5. They had at least 1 or 2 relapses 1 or 2 years prior to screening visit, respectively, or at least 1 gadolinium-enhancing lesion 6 months prior to randomization.
Patients were randomly assigned to receive either fingolimod (oral 0.25 mg – 0.5 mg capsule once daily depending on body weight), or interferon beta-1a (intramuscular injection 30 µg once weekly) for up to 24 months with matching placebo capsules or syringes as part of the double-dummy trial design.
Primary end-point was annualized relapse rate (average number of confirmed relapses/year/treatment period). Secondary end-points included annualized rate of new or enlarged T2-weighted MRI lesions compared to baseline (average lesion number/year/treatment period), time to first confirmed relapse, percentage of patients free of relapse or lesions, number of gadolinium-enhancing lesions, lesion volume, and the safety and tolerability profile of both drugs in this trial. The effect of fingolimod on time to 3-month sustained and confirmed disability worsening from baseline was assessed in a post hoc analysis. Several exploratory end-points in MRI imaging metrics were also included in the trial.
A total of 348 patients were screened, from which 215 patients were enrolled, and 107 patients were randomly assigned to fingolimod and 108 to interferon beta-1a. Trial completion rates were 93.5% in fingolimod group and 81.5% in interferon beta-1a group. The demographic spread of recruited patients in the PARADIGMS trial was similar to that of the general POMS population, with age ranging from 10–18 years old, 62.3% female sex, and disease duration of 0.1–8.2 years. A majority (63.3%) of the patients had not been on any DMTs prior to the trial; of the remaining previously-treated patients, a majority were on interferon (32.1%).
For primary end-point, results from the PARADIGMS trial favored fingolimod. Fingolimod group had significantly lower annualized relapse rate (0.12) compared to interferon beta-1a (0.67). Similar favorable trends for fingolimod were found in secondary end-points as well, including time to first relapse (fingolimod 720 days vs. interferon beta-1a 488 days), percentage of patient free of relapse at 24 months (fingolimod group 85.7% vs. interferon beta-1a 38.8%), annualized rate of new or enlarging T2-weighted MRI lesions (fingolimod 4.39 vs. interferon beta-1a 9.27), gadolinium-enhancing lesions (fingolimod 0.44 vs. interferon beta-1a 1.28). Exploratory analysis involving brain volume change, T2-weighted MRI lesion and gadolinium-enhancing lesion volumes also favored fingolimod. Finally, post hoc analysis of time to confirmed 3-month disability worsening showed that fingolimod significantly delayed its onset compared to interferon beta-1a.
Overall adverse events incidence for fingolimod (88.8%) was comparable to that of interferon beta-1a (95.3%). Fingolimod group experienced more adverse events that led to discontinuation (5.6% vs interferon beta-1a 0.9%). There were more serious adverse events in the fingolimod group (16.8%) compared to interferon beta-1a (6.5%). In the fingolimod group, there were 6 patients who had convulsions compared to 1 patient with convulsions in the interferon beta-1a group. Out of the 6 patients with convulsions in fingolimod group, 2 were categorized as having serious adverse events. There were also single cases of agranulocytosis, second-degree atrioventricular block, elevated alanine aminotransferase and γ-glutamyltransferase levels, autoimmune uveitis, gastrointestinal necrosis, and macular edema reported, among others. Serious infections occurred in 4 fingolimod patients (3.7%) compared to 2 patients in the interferon beta-1a group (1.9%), the infections included appendicitis, cellulitis, gastrointestinal infection, oral abscess, and respiratory tract infection. There were no reports of opportunistic infections, cancer, or death in either group.
Discussion
Fingolimod is an oral DMT for the treatment of relapsing-remitting multiple sclerosis. It was approved in September 2010 by FDA to treat AOMS. For POMS, there were no FDA-approved therapies until May 2018. Based on the results of the PARADIGMS trial,18 both FDA and EMA have approved fingolimod use in POMS population. Results from the PARADIGMS trial demonstrated that fingolimod, compared to interferon beta-1a, significantly reduced annualized relapse rate (82% reduction), annualized rate of new or enlarged lesion formation (53% reduction), and mean number of gadolinium enhancing lesions (63% reduction). Furthermore, fingolimod also significantly delayed time to first relapse and 3-month confirmed disability worsening. Effects reported from the clinical trial were echoed in the limited number of previously published observational studies involving fingolimod in POMS.19–21
Based on safety and tolerability data from both observational studies and the PARADIGMS trial, fingolimod appeared to be well-tolerated in POMS. Adverse events from aforementioned studies are summarized in Table 1. While there were no serious adverse events reported in observational studies, there were a few cases of seizures and leukopenia among others in the PARADIGMS trial. In terms of mild adverse events, lymphopenia and mild infectious complications were most commonly reported. It is believed that leukopenia and lymphopenia, as a result of fingolimod’s mechanism of action, increase infection risks. Discontinuation rate of fingolimod was less than 6% in PARADIGMS. Despite only 1 case of macular edema reported in the PARADIGMS trial, similar screening measures for macular edema, as well as for bradyarrythmia and herpes virus infection should be applied when prescribing fingolimod for POMS as per protocol in AOMS. There was 1 case report of rebound disease activity in a POMS patient following fingolimod discontinuation.25 Therefore, strict adherence should be emphasized to patients when prescribing fingolimod. There is a theoretical risk of PML with fingolimod in POMS, as there have been 19 AOMS patients diagnosed with PML as of May 7, 2018. No POMS patients with PML have been reported to date and JCV serostatus is not required currently prior to prescribing fingolimod.
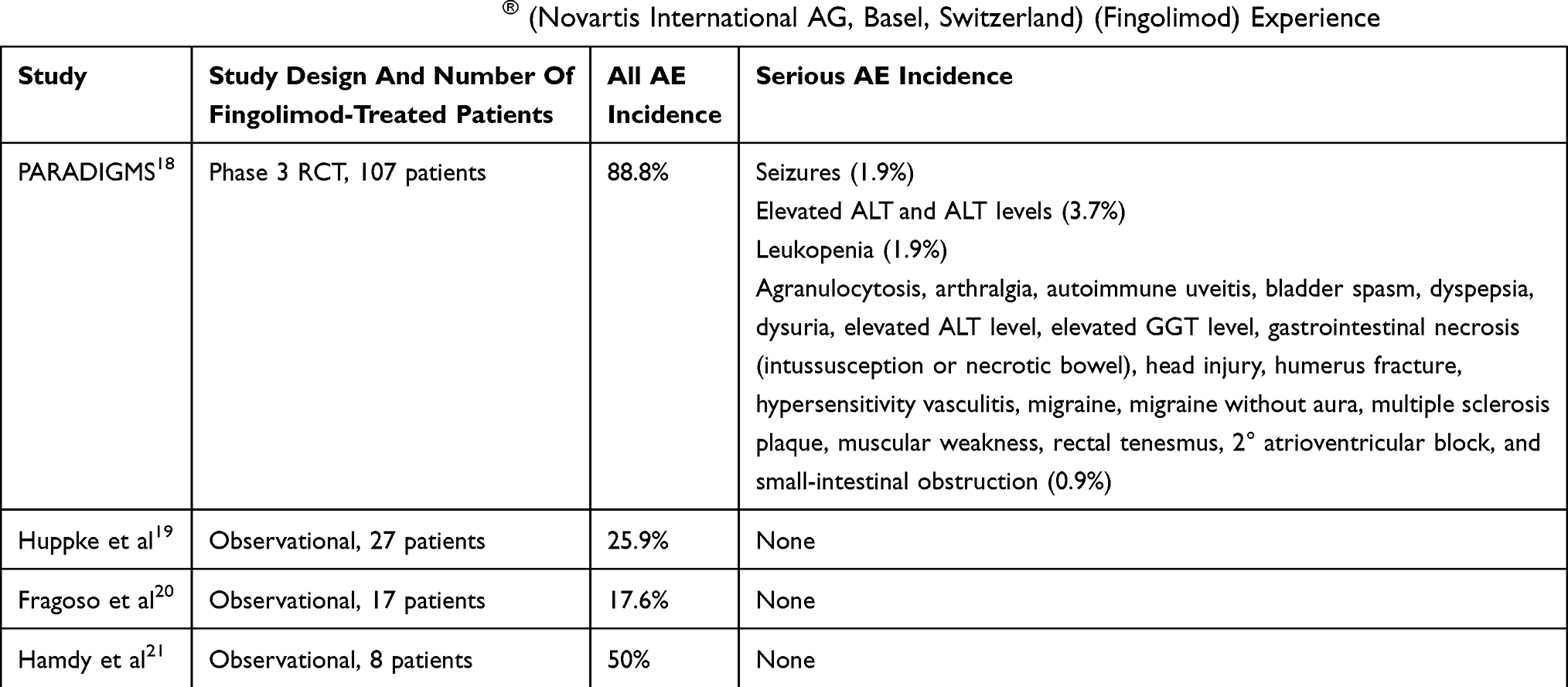 |
Table 1 Adverse Events In POMS Gilenya® (Novartis International AG, Basel, Switzerland) (Fingolimod) Experience |
Lastly, it is important to emphasize that POMS occurs in the setting of actively developing neurological and immunological systems. The long-term neurodevelopmental effects of fingolimod in POMS is unknown, due to lack of longitudinal data. However, it has been reported that POMS patients experience more cognitive deficits in the setting of slowed whole brain and regional volume growth as well as increased lesion burden in posterior fossa compared to age-matched controls.26 The benefit of early effective treatment in POMS may be argued based on fingolimod’s effect on delaying disability worsening.18 The unique lymphocytic sequestration mechanism of fingolimod should also be taken into consideration when prescribing fingolimod in POMS patients with maturing adaptive immune systems. The thymus and bone marrow play major roles in the maturation of lymphocytes in the setting of repeated immune challenges.13 Therefore, the potential long-term effects of fingolimod on the development of comprehensive adaptive immune defense system in POMS need to be carefully weighed.
Conclusion
Fingolimod has demonstrated efficacy in key end-points in POMS population including relapse rate, radiographic lesion changes, and disability. It is well tolerated with mostly mild adverse events such as blood count and liver function test abnormalities and mild infectious events. Limited number of serious adverse events were identified in 16.8% of fingolimod-treated patients in the PARADIGMS trial. It is currently the only FDA and EMA-approved DMT to treat POMS and offers improved disease control compared to current first-line injectable therapies.
Disclosure
Dr. Jenny Feng receives funding via a Sylvia Lawry Physician Fellowship Grant through the National Multiple Sclerosis Society (#FP-1707-28-768), and has received personal fees for speaking for Sanofi/Genzyme and serving on an advisory board for Sanofi/Genzyme.
Dr. Mary Rensel serves on the advisory board or panel for Serono and Biogen, received consulting fees from Biogen, Teva, Genzyme and Novartis, commercial research support from Medimmune and Genentech, foundation/society research support from the National Multiple Sclerosis Society, and educational grants from Genzyme. She is on speaker’s bureau for Novartis, Genzyme, Biogen, and Multiple Sclerosis Association of America. The authors report no other conflicts of interest in this work.
References
1. Boiko A, Vorobeychik G, Paty D, Devonshire V, Sadovnick D. Early onset multiple sclerosis: a longitudinal study. Neurology. 2002;59(7):1006–1010. doi:10.1212/wnl.59.7.1006
2. Harding KE, Liang K, Cossburn MD, et al. Long-term outcome of paediatric-onset multiple sclerosis: a population-based study. J Neurol Neurosurg Psychiatry. 2013;84(2):141–147. doi:10.1136/jnnp-2012-303996
3. Chitnis T, Glanz B, Jaffin S, Healy B. Demographics of pediatric-onset multiple sclerosis in an MS center population from the Northeastern United States. Mult Scler. 2009;15(5):627–631. doi:10.1177/1352458508101933
4. Waldman A, Ness J, Pohl D, et al. Pediatric multiple sclerosis: clinical features and outcome. Neurology. 2016;87(9 Suppl 2):S74–S81. doi:10.1212/WNL.0000000000003028
5. Chitnis T. Disease-modifying therapy of pediatric multiple sclerosis. Neurotherapeutics. 2013;10:89–96. doi:10.1007/s13311-012-0158-1
6. Langer-Gould A, Zhang JL, Chung J, Yeung Y, Waubant E, Yao J. Incidence of acquired CNS demyelinating syndromes in a multiethnic cohort of children. Neurology. 2011;77(12):1143–1148. doi:10.1212/WNL.0b013e31822facdd
7. Pohl D, Hennemuth I, von Kries R, Hanefeld F. Paediatric multiple sclerosis and acute disseminated encephalomyelitis in Germany: results of a nationwide survey. Eur J Pediatr. 2007;166(5):405–412. doi:10.1007/s00431-006-0249-2
8. Banwell B, Kennedy J, Sadovnick D, et al. Incidence of acquired demyelination of the CNS in Canadian children. Neurology. 2009;72(3):232–239. doi:10.1212/01.wnl.0000339482.84392.bd
9. Banwell B, Bar-Or A, Arnold DL, et al. Clinical, environmental, and genetic determinants of multiple sclerosis in children with acute demyelination: a prospective national cohort study. Lancet Neurol. 2011;10(5):436–445. doi:10.1016/S1474-4422(11)70045-X
10. Olsson T, Barcellos LF, Alfredsson L. Interactions between genetic, lifestyle and environmental risk factors for multiple sclerosis. Nat Rev Neurol. 2017;13(1):25–36. doi:10.1038/nrneurol.2016.187
11. Chitnis T, Graves J, Weinstock-Guttman B, et al. Distinct effects of obesity and puberty on risk and age at onset of pediatric MS. Ann Clin Transl Neurol. 2016;3(12):897–907. doi:10.1002/acn3.365
12. Verhey LH, Shroff M, Banwell B. Pediatric multiple sclerosis: pathobiological, clinical, and magnetic resonance imaging features. Neuroimaging Clin N Am. 2013;23(2):227–243. doi:10.1016/j.nic.2012.12.004
13. Bar-Or A, Hintzen RQ, Dale RC, Rostasy K, Bruck W, Chitnis T. Immunopathophysiology of pediatric CNS inflammatory demyelinating diseases. Neurology. 2016;87(9 Suppl 2):S12–S19. doi:10.1212/WNL.0000000000002821
14. McLaughlin KA, Chitnis T, Newcombe J, et al. Age-dependent B cell autoimmunity to a myelin surface antigen in pediatric multiple sclerosis. J Immunol. 2009;183(6):4067–4076. doi:10.4049/jimmunol.0801888
15. Banwell B, Bar-Or A, Cheung R, et al. Abnormal T-cell reactivities in childhood inflammatory demyelinating disease and type 1 diabetes. Ann Neurol. 2008;63(1):98–111. doi:10.1002/ana.21244
16. Bove R, Chitnis T. The role of gender and sex hormones in determining the onset and outcome of multiple sclerosis. Mult Scler. 2014;20(5):520–526. doi:10.1177/1352458513519181
17. Ghezzi A, Amato MP, Makhani N, Shreiner T, Gartner J, Tenembaum S. Pediatric multiple sclerosis: conventional first-line treatment and general management. Neurology. 2016;87(9 Suppl 2):S97–s102. doi:10.1212/WNL.0000000000002823
18. Chitnis T, Arnold DL, Banwell B, et al. Trial of fingolimod versus interferon beta-1a in pediatric multiple sclerosis. N Engl J Med. 2018;379(11):1017–1027. doi:10.1056/NEJMoa1800149
19. Huppke P, Huppke B, Ellenberger D, et al. Therapy of highly active pediatric multiple sclerosis. Mult Scler. 2019;25(1):72–80. doi:10.1177/1352458517732843
20. Fragoso YD, Alves-Leon SV, Barreira AA, et al. Fingolimod prescribed for the treatment of multiple sclerosis in patients younger than age 18 years. Pediatr Neurol. 2015;53(2):166–168. doi:10.1016/j.pediatrneurol.2015.03.024
21. Hamdy SM, Abdel-Naseer M, Shalaby NM, et al. Pediatric-onset multiple sclerosis in Egypt: a multi-center registry of 186 patients. Neuropsychiatr Dis Treat. 2018;14:631–640. doi:10.2147/NDT.S160060
22. Ghezzi A, Rocca MA, Baroncini D, et al. Disease reactivation after fingolimod discontinuation in two multiple sclerosis patients. J Neurol. 2013;260(1):327–329. doi:10.1007/s00415-012-6744-7
23. Hakiki B, Portaccio E, Giannini M, Razzolini L, Pasto L, Amato MP. Withdrawal of fingolimod treatment for relapsing-remitting multiple sclerosis: report of six cases. Mult Scler. 2012;18(11):1636–1639. doi:10.1177/1352458512454773
24. Havla JB, Pellkofer HL, Meinl I, Gerdes LA, Hohlfeld R, Kumpfel T. Rebound of disease activity after withdrawal of fingolimod (FTY720) treatment. Arch Neurol. 2012;69(2):262–264. doi:10.1001/archneurol.2011.1057
25. Piscolla E, Hakiki B, Pasto L, Razzolini L, Portaccio E, Amato MP. Rebound after Fingolimod suspension in a pediatric-onset multiple sclerosis patient. J Neurol. 2013;260(6):1675–1677. doi:10.1007/s00415-013-6933-z
26. McGinley M, Rossman IT. Bringing the HEET: the argument for high-efficacy early treatment for pediatric-onset multiple sclerOSIS. Neurotherapeutics. 2017;14:985–998. doi:10.1007/s13311-017-0568-1
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.