Back to Journals » Vascular Health and Risk Management » Volume 18
Reversal and Remission of T2DM – An Update for Practitioners
Authors Shibib L ![]() , Al-Qaisi M, Ahmed A, Miras AD, Nott D, Pelling M, Greenwald SE
, Al-Qaisi M, Ahmed A, Miras AD, Nott D, Pelling M, Greenwald SE ![]() , Guess N
, Guess N
Received 29 October 2021
Accepted for publication 10 May 2022
Published 14 June 2022 Volume 2022:18 Pages 417—443
DOI https://doi.org/10.2147/VHRM.S345810
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Konstantinos Tziomalos
Lina Shibib,1 Mo Al-Qaisi,1 Ahmed Ahmed,1 Alexander D Miras,2 David Nott,1 Marc Pelling,1 Stephen E Greenwald,3 Nicola Guess4
1Department of Surgery and Cancer, Imperial College London, London, UK; 2Department of Metabolism, Digestion and Reproduction, Imperial College London, London, UK; 3Blizard Institute, Barts and the London School of Medicine and Dentistry, Queen Mary, University of London, London, UK; 4School of Life Sciences, Westminster University, London, UK
Correspondence: Mo Al-Qaisi, Imperial Weight Centre, Imperial College Healthcare NHS Trust, Praed Street, London, W2 1NY, UK, Tel +44 7968 016315, Email [email protected]
Abstract: Over the past 50 years, many countries around the world have faced an unchecked pandemic of obesity and type 2 diabetes (T2DM). As best practice treatment of T2DM has done very little to check its growth, the pandemic of diabesity now threatens to make health-care systems economically more difficult for governments and individuals to manage within their budgets. The conventional view has been that T2DM is irreversible and progressive. However, in 2016, the World Health Organization (WHO) global report on diabetes added for the first time a section on diabetes reversal and acknowledged that it could be achieved through a number of therapeutic approaches. Many studies indicate that diabetes reversal, and possibly even long-term remission, is achievable, belying the conventional view. However, T2DM reversal is not yet a standardized area of practice and some questions remain about long-term outcomes. Diabetes reversal through diet is not articulated or discussed as a first-line target (or even goal) of treatment by any internationally recognized guidelines, which are mostly silent on the topic beyond encouraging lifestyle interventions in general. This review paper examines all the sustainable, practical, and scalable approaches to T2DM reversal, highlighting the evidence base, and serves as an interim update for practitioners looking to fill the practical knowledge gap on this topic in conventional diabetes guidelines.
Keywords: weight loss, very low energy, very low calorie, bariatric surgery, orlistat, electrical muscle stimulation, low carbohydrate, behaviour change, diabetes reversal, diabetes remission
Introduction: The Ever-Growing Pandemic of T2DM
Type 2 diabetes mellitus (T2DM) is a complex, multifactorial, metabolic disease provoked by chronic overconsumption of unhealthy calories in those with a sedentary lifestyle and genetic predisposition, although no specific important risk gene(s) has been identified yet. It is preceded by a variable period of pre-diabetes during which time the body tries to compensate for blood glucose level spikes coinciding with increasing insulin resistance and attenuation of insulin production, but which ultimately progresses if the diet is left unchecked, resulting in a chronic state of elevated blood glucose level. Combined with increasingly sedentary lifestyles, T2DM is on course to be the largest non-communicable pandemic in human history. It has been estimated that the world prevalence of diabetes among adults (aged 20–79 years) in 2010 was 6.4%, affecting 285 million people, and this is projected to increase to 7.7%, or approximately 642 million adults, by 2030.1 Although the prevalence of T2DM is higher in developed than in developing countries,2,3 between 2010 and 2030, there is expected to be a 69% increase in the number of adults with diabetes in the developing world compared to a 20% increase in the West.4
Since the advent of processed food in the 1950s, unhealthy constituents (refined sugars and saturated fats) have increasingly become the dominant part of total calorie intake in the developed world, whilst consumption of natural fibres from organic, fresh whole foods has fallen. The calorie-dense, widely available, and addictive menus touted to a poorly informed public have no doubt played a part in an obesity pandemic – facilitated by underlying epigenetic and genetic factors that are common. As Figure 1 reveals, the T2DM pandemic appears to be preceded by, and then moves in lockstep with, an underlying obesity pandemic.5,6
 |
Figure 1 BMI and risk of diabetes rise in lockstep. Note: Data from Chan JM, Rimm EB, Colditz GA, Stampfer MJ, Willett WC. Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care. 1994;(9):961–969.6 |
The annual cost of diabetes in the US has been estimated to have risen from US $245 billion in 2012 to US $327 billion in 2017 – that is a 33% increase, in just five years.7 For the UK, the costs of diabetes to the National Health Service (NHS) have also risen, reaching a staggering US $15 billion in 2017. Some 80% of the cost of diabetes is spent on treating complications.8 Successful reversal of T2DM would relieve health-care systems and societies around the world from a substantial, and increasingly unsustainable socio-economic burden.9 This review paper gives the practitioner an update about the reversibility of T2DM, which is still an emerging area of practice.
Can T2DM Really Be Reversed?
T2DM has long been regarded as a chronic, irreversible illness, requiring a continuous titration of add-on pharmacotherapy, and which inexorably progresses in over 50% of patients to insulin dependence within 9–10 years.10 However, many studies and reports have emerged that challenge that narrative with new approaches to managing the disease which prioritize reversal and remission.11,12 Respected organizations like the World Health Organization and Diabetes UK now openly acknowledge that diabetes is metabolically reversible – at least for a period of time. Four approaches are detailed on the Diabetes UK website: low carbohydrate diets, very low-calorie diets, exercise, and bariatric surgery.13,14
As a result of the debate around and interest in diabetes remission, a joint consensus statement has emerged around the definition of diabetes remission from the American Diabetes Association (ADA), the Endocrine Society, the European Association for the Study of Diabetes (EASD) and Diabetes UK. The consensus position now defines remission as being a return to below the World Health Organization (WHO)/American Diabetes Association (ADA) original diagnostic thresholds for diabetes and this return should be maintained for 3 months without any glucose-lowering pharmacotherapy (see Table 1). Measurement of either HbA1c or blood glucose can be used to confirm remission. Patients in remission should thereafter be kept under regular review with annual testing as a minimum. It is important to note that the term “cure” has not been applied to T2DM, as weight regain is always a risk factor for its re-occurrence.15 Although the terms “reversal” and “remission” are used interchangeably, recent consensus supports the use of “remission” in the context of T2DM. Furthermore, a distinction could be made between mere reversal (return to normoglycaemia) and true remission (normoglycaemia maintained for at least 3 months in the absence of glucose-lowering drugs).16
 |
Table 1 Published Criteria for T2DM in Remission15 |
Surgical Reversal and Remission of T2DM
It has been known for over 30 years that bariatric surgery can reverse T2DM and change outcomes for obese patients with T2DM.12 Systematic reviews showed that bariatric surgery could initially reverse T2DM for 58% to 95% of patients.17–20
In one long-term study, T2DM patients who had undergone bariatric surgery had a reversal rate of over 51% at 12 years, with an average of 35kg weight loss, representing a reduction of 26.9% weight from baseline. The long-term studies of bariatric surgery have been usually in a group of patients who have BMIs of 35 or more.21,22 Another long-term prospective study of outcomes after bariatric surgery reported a 10-year remission rate from T2DM of just 36%.23 Long-term outcomes from bariatric surgery of course depend on multiple factors, including type of surgery, patient baseline co-morbidities, patient willingness to engage with lifelong lifestyle change, and the quality of ongoing surveillance. Whilst these studies are encouraging, more long-term studies are required to be certain about the true outcomes of glucose homeostasis after bariatric surgery. Initial data suggested that gastric bypass is the most effective at inducing diabetes remission in T2DM patients, followed by sleeve gastrectomy, and then gastric banding.24 Longer term data (5-year) reveal that remission rates for T2DM patients after sleeve gastrectomy are nearly as good as those for gastric bypass.25,26 Laparoscopic gastric banding and gastric balloons are often adjuncts to weight loss, and have good short-term results in type 2 diabetes, however data on their long-term impact on T2DM are scant. Recently “pill balloons” which do not require any procedure have become available.27
In diabetic obese adolescents who have had bariatric surgery, the remission rate of T2DM after the surgery was 82% (95% CI: 66–94%) for the first year, 82% (95% CI: 60–98%) for the second year, 98% (95% CI: 83–100%) for the third year, and 99% (95% CI: 82–100%) >5 years after surgery. Other long-term data suggest remission rates settling at around 85% at 5 years.28,29 Interestingly, after gastric bypass surgery, one study with 5 years of data suggested that adolescents appear to have similar weight loss to adults but do better than adults when it comes to remission of T2DM. However, this advantage comes at the possibly unacceptable cost of a high rate of abdominal re-operations and nutritional deficiencies in the adolescent group.30,31 These undesirable side effects have led some to question whether adolescents should wait until they are adults before undergoing bariatric surgery.32
More than 25% of T2DM patients require insulin. Those already on insulin have a lower diabetes remission rate after bariatric surgery than those on oral hypoglycemics only. In those T2DM patients already on insulin, 62% who underwent gastric bypass were off insulin at 12 months. Gastric bypass was a weight-independent predictor of insulin therapy cessation early after surgery, even before significant weight loss.33 Thus, the beneficial effects of surgical intervention could not be entirely due to weight loss alone, and the metabolic nature of the surgery itself was likely also playing an, as yet, poorly understood part.34
It was only in 2016 that the second Diabetes Surgery Summit produced recommendations, endorsed by 45 national medical societies worldwide, to use bariatric surgery as a treatment for T2DM in adults with body mass index >40, or >35 kg/m2 in those with obesity-related co-morbidities.35 These guidelines were based on the observation that there was uniform improvement in glycemic control after any bariatric operation.36 In addition to early and dramatic post-operative improvement in glycaemia and insulin sensitivity, bariatric surgery causes alterations in gastrointestinal hormone release, including ghrelin, leptin, cholecystokinin, peptide YY, and in particular, glucagon-like peptide 1 (GLP-1), which may correct feeding behavior via the gut-brain axis in addition to sustaining euglycaemia.37 Studies have shown that postprandial levels of endogenous GLP-1 after bariatric surgery can be 10 to 20 times higher compared with before surgery.38
Interestingly, bariatric surgery has been associated with dramatic changes in the gut microbiome, with reversion from an “obesogenic” to a “lean” profile.39–44 The exact neuroendocrine mechanisms by which bariatric surgery effects all these improvements in glycemic profile are not yet fully understood, although it appears that a combination of sudden, sharp energy reduction,45 changes in vagal tone,46 gut hormones in particular GLP-1,47 bile acid metabolism,48 reprogramming of intestinal glucose metabolism and the colonic microbiome49 have all been implicated.
Like all surgeries, there is a risk of complications, although this is small in bariatric surgery. In randomized clinical trials, the mortality rate within 30 days was 0.08% (95% CI, 0.01–0.24%) and the mortality rate after 30 days was 0.31% (95% CI, 0.01–0.75%). The complication rate was 17% (95% CI, 11–23%), and the reoperation rate was 7% (95% CI, 3–12%).50 Patients who require reoperation for either revision or complete reversal of their initial bariatric surgery have further attendant risk, the magnitude of which is still under investigation. Individually, rates of major adverse events in the first 30 days were 5.0% for roux-en-y gastric bypass (RYGB), 2.6% for sleeve gastrectomy, and 2.9% for laparoscopic adjustable gastric banding (LAGB).51 Significant complications include anastomotic leak or hemorrhage, dumping syndrome, worsening acid reflux, marginal ulceration, and micronutrient deficiencies.52–56 For each patient, these risks must be weighed up against the risks associated with leaving their morbid obesity untreated. Interestingly, recent studies have shown that bariatric surgery for T2DM is of benefit even to lower BMI groups.57 In non-obese (BMI <30) type 2 diabetes, remission rates for bariatric surgery have been reported to range from 13.3% to 90.2%, depending on the type of procedure, with the longest study having a three-year follow-up.58–60
Even after remission following surgical intervention, T2DM patients can still relapse. The prospective Swedish Obese Subjects study reported remission rates of T2DM at 2, 10 and 15 years of follow-up as 72.3%, 38.1% and 30.4%, respectively.61 These results were mirrored in a retrospective cohort study including 4434 obese patients with diabetes who underwent gastric bypass. The average remission time after bypass was 8.3 years, with 35.1% suffering from T2DM relapse by year 5.62 Revisional bariatric surgery has been shown to have utility for recurrent metabolic disease, especially T2DM. Depending on the index surgery and subsequent reconstruction, improvement of diabetes was seen in 65–100% of patients. Gazda et al63 retrospectively studied the use of GLP-1 receptor agonist-based weight-loss programs for recidivism after bariatric surgery as an alternative to revisional surgery. They found that GLP-1-based programs to be superior to non-GLP-1 programs and intensive lifestyle modification alone for treating post-bariatric surgery weight regain, regardless of surgery type.
Further mechanistic research and much larger prospective randomized studies would be needed to identify the optimal treatment strategies for post-bariatric weight regain and relapse of T2DM with residual or recurrent metabolic disease.64
Predicting Remission Outcomes After Surgery
With an increasing quantity of data available for analysis, a long list of pre-operative clinical and biochemical factors has been identified as being potentially predictive of T2DM remission and relapse after bariatric surgery, including the surgical procedure, insulin sensitivity, weight regain, bile acids, changes of gut microbiota, gastrointestinal hormones, particularly ghrelin, glucagon‐like‐peptide‐1, gastric inhibitory polypeptide and peptide YY, as well as a large number of inflammatory markers.65 These predictors may be classified into two broad groups based on their mechanism of action. The first group includes indices for preserved pancreatic beta-cell function, including younger age, shorter duration of diabetes, and lack of insulin dependency. The second group tracks insulin resistance, including baseline BMI and amount of visceral fat. Several validated prediction models for diabetes remission have been produced to help guide clinicians. However, the precise utility of these models still needs further verification in prospective, randomized controlled studies and long‐term follow-up.66 So, whilst bariatric surgery has been shown unequivocally to reverse T2DM and to be of great benefit in obese patients, further studies are under way to pinpoint more effective patient selection and post-operative follow-up to mitigate the risk of complications and increase or optimize the levels of long-term benefit and remission.
Taylor Twin Cycle Theory
Blood glucose levels return to normal within a week of bariatric surgery. Initially, it was postulated that bariatric surgery produces this early normoglycemia via a direct effect on incretin hormones. However, incretin hormones are secondary regulatory hormones, and are less likely to be the driver of an almost immediate change in fasting plasma glucose. A careful review of the data from Guidone et al67 begins to shed more light on what could be happening in the body after bariatric surgery. In patients who elect to undergo bariatric surgery, there is an obvious and stark change in calorific intake following the procedure. The immediate consequence is negative calorie balance, and the body has to use its energy reserves. Instead of an abundance of post-prandial fatty acid intermediates (that inhibit glucose metabolism) being left to accumulate in the cytoplasm,68 they are urgently taken up by the mitochondria for oxidation. Diacylglycerol, the product of removing one of the three fatty acids from triacylglycerol (ie, triglyceride), rapidly decreases in concentration and suddenly cells are left with a normal choice of fuel—either glucose or fat, depending upon needs. This postulated sequence of events has been drawn together as the Taylor Twin Cycle Hypothesis,69 which is a considered attempt to explain why T2DM could be reversible.70
According to the Taylor Twin Cycle Hypothesis, during chronic over-consumption of energy-dense sugary foods, the excess carbohydrate is removed by lipogenesis, and this particularly promotes fat accumulation in the liver. As insulin promotes this lipogenesis, individuals with a predisposition for, or a pre-existing degree of insulin resistance (determined by genetics or lifestyle factors) will accumulate liver fat more easily than others because of the higher plasma insulin levels. Fat deposition in the liver, trackable by rising serum ALT levels, will cause resistance to insulin suppression of hepatic glucose production. If left unchecked over many years, the resulting hyperinsulinemia will accelerate the conversion of excess calories into liver fat. This creates a vicious cycle of insulin resistance, hyperinsulinemia, and fat deposition in the liver.71 To deal with the fat, a fatty liver increases its export of VLDL triacylglycerol,72 which adds to the problem of elevated levels of free fatty acids in the blood from any unhealthy diet. This fat can be taken up by B islets in the pancreas. Eventually, the twin process of fatty acid uptake in the islet cells and insulin resistance will reach a threshold level, causing B cell dysfunction, and precipitating impaired glycemic control followed by frank T2DM.73 After bariatric surgery, this whole mechanism could be thrown into reverse because of the stark change in calorie balance. The excess toxic fat in the pancreas is quickly eliminated, and B cell function appears to be re-established. A recent study has suggested that as little as 0.5g of excess fat can cause severe dysfunction in the pancreas. A mere 0.5g can quickly be eliminated, possibly explaining why normoglycemia is established so astonishingly quickly – with the caveat that such a small amount is also very easy to re-accumulate. So, whilst reversal might be very quick, maintaining reversal for longer periods (ie, long-term remission), will require a further period of dietary restriction.74 The Taylor Twin Cycle Theory will allow scientists to study further how medical interventions might be designed to have similar beneficial effects to bariatric surgery without the need for the invasive anatomic rearrangement. Figure 2 depicts the main processes of the Twin Cycle Theory and how they could combine to effect T2DM remission.69
 |
Figure 2 The Taylor twin cycle theory. Abbreviation: HPG, hepatic glucose production. Notes: This bicycle is controlled by handlebars representing chronic, excess (XS) calorie intake in the presence of muscle insulin resistance. Raised plasma insulin levels will expedite chronic excess calorie storage from carbohydrate via de novo lipogenesis, and hence promote liver fat storage. This will cause the liver to become relatively resistant to insulin and a small increase in plasma glucose will occur. In turn, insulin secretion will increase to reduce plasma glucose. The further increased insulin levels will bring about a self-reinforcing cycle. Excess fat will result in increased export of VLDL triglyceride from the liver, uptake by islets and inhibition of meal insulin secretion. At a personal threshold, the level of pancreatic fat imposes too great a load and plasma glucose levels will then rise relatively rapidly.69 Adapted from Taylor R. Banting Memorial lecture 2012: reversing the twin cycles of T2DM. Diabet Med. 2013;30(3):267–275. © 2012 The Author. Diabetic Medicine © 2012 Diabetes UK. |
Pharmacotherapy for T2DM- from Reversal to Remission
Most T2DM guidelines have focused on the pharmacological management of hyperglycemia, rather than weight loss, which was always a part of core management.75 The increasing use of hyperphagic drugs like insulin and sulphonylureas was a further contradiction.
It is a sensible view that pharmacotherapy alone cannot address underlying unhealthy lifestyles leading to overweight. Overweight/obesity is strongly driven by genetic factors that makes it a chronic problem with a high risk of relapse. Compounding this state of affairs is an obesogenic environment within which sugar and the pleasure of eating can be addictive. Even if medication could solve lifestyle disease on its own, the prospect of medicating the majority of the population is not one that can be entertained without considering all the side effects and cost.76 A recent analysis reported that between 2011 and 2017, additional benefits from the diabetes drugs approved by regulators were found in only 16% of patients.77 If conventional glucose-lowering pharmacotherapy is used without considering an individual strategy for reversal, T2DM is usually a progressive disease.10 This disappointing state of affairs is at least partly because conventional pharmacotherapy has been developed to treat the levels of blood glucose, whilst the underlying etiology of T2DM is, in reality, much more complex, and for example, associated with visceral fat.78,79 It is a sobering fact that increased US expenditure on conventional diabetes care has not improved outcomes.80 Perhaps, the most depressing data come from a major study by Kaiser Permanente that found only a 0.23% remission rate with best practice standard care.81
However, revisiting the literature around pharmacotherapy for T2DM more carefully reveals that these otherwise depressing trends even with “best practice” were not left unchecked by pioneering researchers who prioritized exploring interventions that could be effective for remission.
In fact, the feasibility of reversing T2DM with pharmacotherapy has been demonstrated in numerous studies and with different medications – therapeutic strategies that have not been adopted as first-line. Studies have shown that, when implemented early in the course of T2DM (ideally less than 2 years), intensive insulin therapy for 2–3 weeks can induce a glycemic remission, wherein patients are able to maintain normoglycaemia without any anti-diabetic medication. When followed-up in a meta-analysis, short-term intensive insulin therapy was found to significantly improve islet function and induce remission in 46% of patients at 12 months, and 42% at 24 months. This effect is not weight-loss dependent, and patients were not administered with VLEDs or LCDs. Beta-cell redifferentiation was considered the important underlying mechanism for the treatment effect. Short-term intensive insulin therapy can improve the underlying pathophysiology in early T2DM, and this approach clearly provides one treatment strategy for modifying the natural history of the disease.82–87
Jennings et al found a triple therapy of metformin, pioglitazone and repaglinide to be effective for reversing newly diagnosed T2DM patients. The drugs were given at maximum tolerated doses and then tapered according to results.88
Panikar et al found a multidrug therapy consisting of metformin, pioglitazone, and gliclazide effective for reversal in a population of T2DM patients of less than 24 months duration.89
Even for T2DM patients who have had the disease for 5 years and progressed to insulin (but before the advent of any serious co-morbidities), add-on drug therapy with metformin, glibenclamide, and pioglitazone saw 43% lose their requirement for insulin altogether at 6 months.90
Elsewhere, there is the anti-obesity drug orlistat, which has been available for over 2 decades. It is a peripheral lipase inhibitor which has virtually no systemic absorption and an excellent safety profile, despite initial (unfounded) fears about liver injury.91 Orlistat could be considered a calorie restriction mimetic (CRM), a type of drug that otherwise mimics the mechanism of action, effects, and long-term outcome noted with calorie restriction, without actually causing calorie restriction or lack of food intake.92 Interventions that can mimic energy deficit can drive similar beneficial effects on T2DM as bariatric surgery.
Orlistat is often overlooked by practitioners because of its gastrointestinal side effects (oily stools, soiling), causing poor patient compliance. However, gastrointestinal side effects can be greatly mitigated by careful patient selection, giving clear instructions to patients on how to follow a low-fat diet, and starting with a lower dose (60mg capsule instead of 120mg). The horror stories about oily stool are associated with starting on the higher dose (120mg) and poorly informed patients who use the orlistat inadvertently when on an ad libitum diet or with fried food, despite dietary advice.
If prescribed with due care and patients can tolerate the drug, then the improvements in glycemic profile seen in orlistat-treated diabetic patients93,94 are comparable to those on antidiabetic medications95–97 Orlistat also improves glycemic control and reduces insulin requirements when it is added to insulin monotherapy in T2 diabetes.98 Similar results were found in those treated with oral hypoglycemics.99–101 In one of the largest studies of its kind on diabetes prevention, orlistat was found to prevent and delay pre-diabetes from progressing to frank T2 diabetes.102
The improvements with orlistat can be seen both in the long and short term. In the long term, orlistat improves glycemic control by effecting accelerated weight loss103 even with diabetic patients, a group who are known to have particular difficulty losing weight when compared to non-diabetics.104 In addition, orlistat improves glycemic control more than would be predicted by equivalent weight loss through diet and exercise programs.98,105–107 And interestingly, if we look more closely at the literature, in the short term we see that many studies have even reported that improvements in glycemic control and insulin sensitivity are seen very shortly after orlistat is started, before any weight loss has occurred.108,109 These observations tie in with the results of other research on T2DM and body fat. If we look at weight distribution in T2DM patients, they are more likely than non-diabetics to have an increased abdominal circumference. Increased intra-abdominal adiposity is often a surrogate for visceral fat deposition around the liver and pancreas, which in turn is closely associated with T2DM risk.110,111 Visceral fat is a source of several pro-inflammatory cytokines that increase insulin resistance112 and reduce the survival of pancreatic B cells.113 Orlistat selectively reduces visceral fat rather than other body fat stores, and therefore attenuates the harmful cytokine production, whilst boosting adiponectin.93,114–119 It has long been known that free fatty acids increase peripheral and hepatic insulin resistance, inhibiting whole body glucose utilization and oxidation, thereby increasing hepatic glucose output, and affecting virtually all major pathways involved in glucose metabolism.120–127 HbA1c levels are also positively associated with total fat intake.128 Orlistat blocks the digestion (and therefore absorption) of free fatty acids from the diet. Patients treated with orlistat recover much greater insulin sensitivity than patients who are given behavioral interventions plus placebo, even when the reduction in hepatic steatosis, loss of skeletal muscle fat content, changes in visceral fat tissue, and amount and rate of weight loss remain unchanged.106 Improvements in insulin sensitivity are therefore not modulated by weight loss alone, and plasma free fatty acid levels could in fact be a much stronger and more immediate correlate of insulin sensitivity both at baseline and after weight loss. In obese individuals, levels of free fatty acids are elevated, especially after unhealthy meals, and this is associated with their state of increased insulin resistance.129,130 Reduction in the levels of free fatty acids in obese individuals with pre-diabetes or diabetes improves their glycemic control.124 Not surprisingly, obese type 2 diabetics have consistently shown improvements in glycemic control with orlistat use.93,101,118,119 Orlistat has positive effects on gut peptide hormones, resulting in an incretin-like response. The increase in the passage of intestinal fat content due to orlistat blockade stimulates increased secretion of two gut hormones, GLP-1 and GIP,131 which in turn boost insulin secretion.132,133 GLP-1 secretion is also associated with accelerated weight loss.134
In practice, orlistat is often overlooked by clinicians due to its socially embarrassing side effects. However, given its proven benefits, more effort should be made to overcome this barrier. Greater attention when giving appropriate low fat dietary advice, and perhaps considering starting on lower dose (60mg) of orlistat, would greatly mitigate any embarrassing side effects. Making the drug more socially acceptable by removing the greatest barrier to its more widespread use would greatly benefit T2DM patients. Interestingly, studies of orlistat with a modified-release version of alpha-glucosidase inhibitor acarbose showed much improved tolerability of orlistat. Data on weight loss outcomes with the combination are still awaited.135,136
Kalra et al92 elaborate on glucose-lowering drugs that are CRMs. Of the various anti-diabetic medications, four classes are identified: insulin sensitizers (pioglitazone, metformin), the alpha-glucosidase inhibitors, GLP-1 agonists, and SGLT2 inhibitors, as summarized in Table 2.
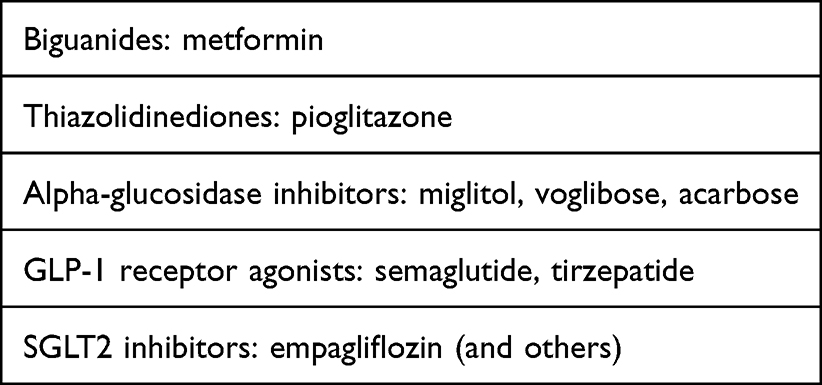 |
Table 2 Examples of Glucose-Lowering CRM Drugs |
A study in Japanese patients found the alpha-glucosidase inhibitors effective for reversal in obese type 2 diabetics, with miglitol most effective (followed by voglibose, whilst acarbose did not accrue benefits in the study timeframe of 12 weeks). Interestingly, the vast majority of patients in this study were on a number of concomitant medications, and the beneficial effects likely resulted from the inadvertent multi-drug therapy administered by the authors, aided by the CRM. The authors postulated that acarbose required more than 12 weeks use to accrue reversal benefits. The authors did not mention how long the patients had had T2DM.137
Since 2021, it has been seen from Phase 3 trials that high dose GLP-1 analogues (like semaglutide) or GLP-1/GIP dual analogues (like tirzepatide) can deliver stunning results and promise to be game-changers in the realm of T2DM reversal. In the SURPASS-1 study of tirzepatide, treatment differences for two estimands – efficacy and treatment-regimens – were evaluated for the three tirzepatide doses (5 mg, 10 mg and 15 mg) compared to placebo for 40 weeks. Astonishingly, 51.7% of participants assigned the highest dose (Eli Lilly; 15mg) achieved an HbA1c of 5.7%, which is considered a nondiabetic level. Average weight loss was 9.5 kg (11.0%) at 40 weeks. Participants had a mean diabetes duration of 4.7 years and baseline HbA1c and weight of 7.9% and 85.9kg respectively. There were no events of severe hypoglycemia or severe hyperglycemia in the tirzepatide treatment arms. The most commonly reported adverse events were gastrointestinal-related and these were mild to moderate in severity, usually occurring during the dose-escalation period. Treatment discontinuation rates due to adverse events were less than 7% in each tirzepatide treatment arm.138 Tirzepatide has been shown to be as effective for type 2 diabetics on insulin with up to 62.4% of treated participants using the highest dose (Eli Lilly; 15mg) achieving an HbA1c level of less than 5.7% at 40 weeks.139 In a 68-week study of semaglutide in type 2 diabetes, subjects on a high dose of the drug (Novo Nordisk; 2.4 mg) lost an average 9.6% of their body weight, compared with an average weight loss of 7% on 1mg of the drug, and 3.4% with the placebo. At the higher dose, more than a quarter of the participants lost over 15% of their weight, almost half lost 10%, and two-thirds lost at least 5%. The average reduction in body weight with high dose semaglutide was 10kg. These results have been hailed as among the best ever seen with any weight loss medication in patients with T2DM. At the end of the trial, participants on the high dose had an average HbA1c of 6.4%, which is just in the prediabetes range, and therefore below the threshold to diagnose T2DM. This compared with 6.6% on a 1 mg dose (still diabetic) and 7.8% on placebo. The most commonly reported side effects with high dose semaglutide were gastrointestinal issues including nausea, vomiting, diarrhea, and constipation, which 88% of participants reported.140
It should be cautioned that there are no data yet to see if reversal mediated by GLP-1/GIP analogue drugs can be maintained long term without dependency on the drugs. Under the strict ADA definition of remission, reversal of T2DM dependent on continued use of GLP-1/GIP analogue drugs might not be regarded as remission if the drugs are considered to be glucose-lowering drugs rather than weight loss agents.
Dutta et al141 point out that when it comes to using pharmacotherapy for weight loss, especially in type 2 diabetics who are more brittle slimmers, combination therapy rather than monotherapy will be the only feasible strategy to achieve the required weight reduction required for reversal and remission. The kind of weight loss required for successful reversal and remission, as has been keenly observed by Dutta et al, is much more likely with combination pharmacotherapy.
The observations of Dutta et al141 about the need for multi-drug therapy is supported by almost all studies of combination pharmacotherapy for weight loss, wherever data is available, especially in the context of T2DM reversal and remission, albeit at a cost of a theoretically increased risk of side effects. Unfortunately, studies with comprehensive data on all the permutations of multi-drug therapy for weight loss and reversal in T2DM are scant – for example, there are no data on the combination of orlistat with the other alpha-glucosidase inhibitors like miglitol or voglibose, themselves on their own, or in combination;137 and very little data on orlistat with GLP-1 agonists or orlistat with SGLT2 inhibitors- to name a few gaps in the literature.141,142
Notwithstanding, new studies (even if anecdotal or case reports) are being published all the time about multi-drug combinations – for example, Chua’s paper on high dose liraglutide (a type of GLP-1 agonist) and SGLT2 inhibitor.143 With each new publication, we have a slightly clearer picture of which combinations of drugs can be used, and in which circumstances.
Very Low Energy Diets (VLEDs)
When it comes to the nutrition therapy of T2DM, standard practice has been kept in alignment with generic public health advice and health promotion targets, without specifically aiming to achieve remission. Nutritional management of T2DM is focused on improving glycemic control through moderate weight loss.75,144 Moderate weight loss (ie, 5% body weight) improves glycaemic control significantly, but is usually not sufficient to achieve remission. A retrospective cohort study of T2DM patients receiving standard ADA care (including dietary advice) found a 7-year cumulative remission rate of just 0.14%.81
Born out of this depressing state of affairs, researchers have been exploring different approaches to the nutritional management of T2DM for a long time. Early, dramatic improvements in fasting plasma glucose, prior to significant weight loss, have been observed with VLEDs long ago in the overweight or obese T2DM patient, even in the absence of any pharmacotherapy.145 Although achieving normoglycemia was easy, maintaining it as a durable remission required sustained weight loss in overweight type 2 diabetes. And it should be noted that some 90% of adults in the UK with T2DM are overweight or obese.146 In 1976, Bistrian et al reported a small study with seven T2DM patients with obesity on insulin demonstrating that a very low energy diet rapidly eliminated the need for insulin in all participants. This was achieved in an average of just 6.5 days, with the longest taking 19 days.147 Bauman et al showed that a low energy diet led to significant improvements in glycemic control.148 Another study showed that low energy dieting and gastric bypass in type 2 diabetes could be equally effective in improving glycemic profile in the short term.149 However, the diet group only maintained weight loss for the first 3 months on average, confirming the difficulty of long-term maintenance using dietary approaches, reported in many other studies.23,150–153
For individuals with diabetes, the Look AHEAD (Action for Health in Diabetes) study showed that a loss of 5–10% of body weight could improve fitness, reduce HbA1c levels, improve cardiovascular disease (CVD) risk factors, and decrease use of diabetes, hypertension, and lipid-lowering medications,154 however the idea that weight loss as a potential approach for long-term remission was not considered at the time. The conventional wisdom was not seriously questioned until the seminal DiRECT study, which demonstrated that T2DM can be successfully reversed for the long term with a very low energy diet. In fact, 50% of the participants had long-term reversal with a weight loss of 10kg, and 90% with 15kg provided that this was achieved within 6 years of their diagnosis. After 6 years, or if already on insulin, T2DM was still potentially reversible, but remission was more difficult, took longer, and was more fragile.155 On average, the participants in DiRECT had achieved 10–15kg of weight loss, translating to remission for 46% of their patients at 1 year, and 36% at 2 years follow-up.156 The DiRECT trial used a structured approach with evidence-based (entirely non-surgical non-pharmaceutical) behavior change interventions to deliver the initial weight loss, a result all the more worthy of admiration as all treatment was delivered via routine care in general practice. This was despite the fact that GP clinics are given few resources to attend to challenging areas of practice such as weight management. In a further study, the number of participants has been expanded to 5000 and follow-up extended for a further 3 years, to assess the long-term outcome of diet-induced weight loss on remission.157 The DiRECT authors surmised that remission (or significant improvement in glycemic control) would be maintained long term by careful weight maintenance or perhaps further weight loss at a later stage.158 The DiRECT approach and impressive results (61% remission rate at 12 months) were replicated in the DIADEM-1 study in Qatar, in a totally different Middle Eastern and North African population, showing that the DiRECT approach could work equally well outside of a UK population.296
Researchers have analysed the profiles of those patients who were able to achieve remission. Those who had positive outcomes were male, younger, with good mental health, on fewer medications, had shorter duration of T2DM (less than 6 years and ideally less than 2 years), higher fasting insulin, and lower fasting glucose at baseline. Importantly, they had less pancreatic and total body fat, although there was no difference in hepatic triglyceride content. Interestingly, the key feature distinguishing responders from non-responders was the return of the first-phase insulin response. Responders showed an improvement in first-phase insulin response, whereas non-responders showed little or no change. Combining these data, there seems to be a point at which B-cell function declines to such a degree that it cannot recover from lifestyle interventions alone, even though those interventions can still induce significant clinical improvements.159,160
The Role of Counselling and Behavior Change
The American Heart Association (AHA) recommends the implementation of behavior change techniques for promoting lifestyle change.161
A study published in the Journal of Human Nutrition found that weight regain (after initial rapid weight loss) can be significantly slowed down, but not eliminated, once a normal diet is restarted, if there is structured psychological support using cognitive behavior therapy.162 Over the past 3 years, a frenzy of health-care start-ups have launched digital (online) solutions and apps focused on delivering weight loss through digital behavior change techniques, and it is interesting to note that these psychological approaches do indeed deliver modest results for weight loss much more than would be expected from an entirely non-surgical and non-pharmaceutical intervention. Perhaps, the most thorough evidence-based digital behavior change program of its kind is that of Changing Health based on the Southampton POWeR (Positive Online Weight Reduction) study, which has partnered with the NHS in the UK.163 The evidence from the POWeR study suggests that this approach – digital written content with occasional brief nurse follow-up – could be a very scalable model that improves outcomes from dietary approaches to weight loss, and by extension, should contribute to better outcomes if combined with all approaches to T2DM reversal.164,165
Further research needs to be done on the extension of digital behavior change outside of dietary approaches to reversal, but the results are already highly anticipated. For example, Novo Nordisk has already partnered with Noom to deliver behavior change to those using its ground breaking GLP-1 pharmacotherapy.166
There is also a lack of studies directly comparing delivery methods for counselling (eg, individual vs group-based, face-to-face vs online) with a counsellor. Some studies have used intensive lifestyle interventions whilst others have had the minimum of contact time. The online methods allow an increase in intensity of the intervention using automated reminders and intelligent-driven personalized content with only minimal contact time. Interestingly, simply increasing contact time with a counsellor did not improve outcomes.167,168
In vitro Studies and Remission of T2DM After VLED’s
In vitro studies have provided parallel evidence that remission from T2DM really is possible at a cellular level. A study published in Cell Metabolism showed that the B-cells of the pancreas can indeed recover their ability to synthesize insulin after remission through weight loss.169 The restoration of B-cell function and the resumption of exports of very low-density lipoprotein from the liver were salient features of the cellular remission seen.169–173
All of this adds to the feasibility and validity of VLEDs for reversing T2DM. For T2DM patients who are of normal weight or are underweight, it is still thought that weight loss can bring about remission, albeit by a much smaller amount. The DiRECT authors are already studying this group and more data will be available soon.174 As noted by others, Newcastle University found that it was as little 0.5g of excess toxic fat in the pancreas that was causing insulin production failure in B-cells, which might explain how those of normal weight could still have the problem.74,175
Despite the optimism generated by the DiRECT trial results, a feature of studies of all VLEDs not to be forgotten is that remission is not universal. Less than 40% of participants have good long-term outcomes. VLEDs can only be prescribed for 12 weeks by practitioners, and the main challenge now is to improve long-term remission rates after initial reversal using this dietary approach. Weight maintenance interventions have yet to definitively tackle all the issues around appetite resurgence once a normal diet is reintroduced. A major criticism of VLEDs (like the one used in the DiRECT trial) is that they do not rely on meals made from natural whole foods, but instead opt for processed, total diet replacement drinks176 and this also could put patients at risk of micronutrient deficiencies, requiring preventive supplementation with multi-vitamins.177
Low Carbohydrate Diets (LCDs)
There are several different definitions of a low carbohydrate diet (LCD) based broadly on restricting carbohydrate intake to anywhere between 20g–130g of carbohydrates per day (equating to 6–26% of total energy intake).178 The Scottish Intercollegiate Guidelines Network (SIGN) suggests that “a minimum of 50g of carbohydrates per day appears safe for up to six months” for type 2 diabetics.179 The classification of LCDs by Feinman et al180 has become the most popular definition among dietetic practitioners, as summarized in Table 3.
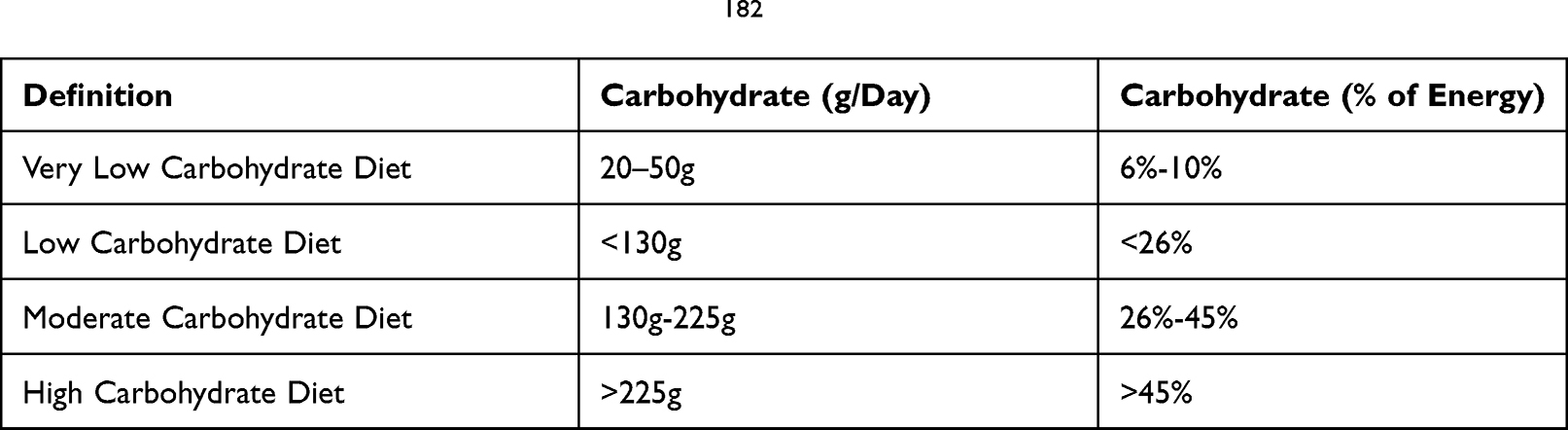 |
Table 3 Definition of LCDs After Feinman et al182 |
Before the discovery of insulin in 1921, LCDs were the default dietetic approach to diabetes.181,182 In fact, LCDs are not new and have been promoted for cardiovascular health since at least the time of William Banting in 1863.183 However, the advent of injectable insulin and oral hypoglycemics led to a paradigm shift in the dietetic management of T2DM. Around the world, drug companies drove the strategy of relatively higher carbohydrate, lower fat diets, with the aim of controlling sugars with the use of their medications – not a surprising strategy, assuming the principal aim of drug companies is to promote strategies that sell their medications.184,185 In the 1980s, public health advice in the UK was pushing the “low fat” and “low cholesterol” message, whilst staying silent on the consumption of refined carbohydrates,186 facilitating the trend of increased consumption of low fat, high carbohydrate processed foods. In fact, between 1961 and 2011, the same trend was seen in the USA where 90% of the increase in calorie intake came from carbohydrates and polyunsaturated vegetable oils.187 The meteoric rise in diabesity over the past decade in the UK and USA, following an increase in the consumption of refined carbohydrates, makes it unlikely that it was entirely coincidental, but more likely that the increased consumption of refined carbohydrates was one of the aggravating causes of the diabesity problem that we face today. It is paradoxical that the poorly educated Queen Marie Antoinette of France has been vilified for generations for allegedly proposing to let the masses “eat cake” to satisfy their hunger- an attribution that most historians now think was part of revolutionary propaganda and not actually factual;188 yet this seems very similar to what policy makers in the West were happy to recommended to the public for several decades, whilst food manufacturers took advantage of the liberal regulations to flood the marketplace with processed, calorie-dense foods using highly refined sugars. Today, the recommended NHS guidelines in the UK allow the daily consumption of 30g of “free sugars” (added sugars plus naturally-occurring sugars in certain foods) as being within normal limits for normal adults, equating to no more than 5% of total energy intake. However, this UK government recommendation does not include the sugars found naturally in milk, fruit or vegetables, which are included in total carbohydrate counts elsewhere.189 Public health advice about carbohydrate consumption is changing. A report by the Scientific Advisory Committee on Nutrition in May 2021 sets out a body of evidence that low carbohydrate diets have a role to play in T2DM management and reversal, a role that requires further study in order to be optimized and individualized.190
The “high carbohydrate low fat” approach of previous decades was challenged with the popular re-discovery of LCDs by Dr Atkins in 1972.191 Sceptics of the conventional approach to carbohydrates like Dr Atkins pointed out that there was no evidence of a dietary or biological requirement for so much sugar in the human diet. Added sugar had no obvious nutritional value. Dietary fructose or sucrose were not known to be an essential part of any biochemical process in the human body. No studies have demonstrated the health benefit of consuming sugar.192 Today, some authors question whether consuming carbohydrate (excluding fibre) is essential for human function at all.193 The scientific ambivalence about dietary sugar has been growing, especially over the past decade.194 Excessive refined and starchy carbohydrates have been found to increase the risk of developing poorly controlled blood glucose levels, and therefore the chances of progressing to T2DM and its morbid complications, and these food choices could increase the risks independent of calories or weight gain.195–197 The underlying mechanisms for the harm caused by unhealthy carbohydrates are no longer obscure. For example, it has been found that the plasma level of the saturated fat palmitic acid, linked to the consumption of starch, sugar, and alcohol, is strongly associated with T2DM.198,199 The same calories from different foods can have very different metabolic impacts on the body, and it has been suggested that, after digestion and absorption, some foods are metabolized in such a way that they may promote metabolic disease, an effect that is over and above merely measuring the impact of their calorific content. Isocaloric portions of sugar, alcohol, meat or olive oil have very different effects on thermogenesis, insulin resistance, appetite regulation, and the gut microbiome – a situation which becomes even more complex when we add the interaction with an individual’s genetics.200 It appears that calories are not the only variable to consider, even though recent messaging from some clinical academics has been focused on the point that “diabetes is caused by chronic calorie excess”,157 whilst remaining silent on the additional deleterious role of carbohydrates within that excess of calories. A recent review in the BMJ explicitly discussed the importance of the quality of carbohydrates and their links to developing a multitude of chronic diseases. Whilst the consumption of refined sugars has been linked to the etiology of chronic disease, on the other hand, highly viscous plant fibres which, paradoxically, are also carbohydrates, are the diametric opposite, helping to reverse type 2 diabesity and reducing the risk of morbid cardiovascular complications. This reinforces the concept of high-quality versus low-quality carbohydrates, based on their glycemic index and glycemic load, which are the two key empirical metrics to rank foods according to their effects on blood glucose.201
At the same time, much evidence has been published on restricting carbohydrate intake–not just sugars, but also grains and starchy vegetables–and has found that T2DM can improve dramatically or disappears with this approach.168,202–235 One review concluded that restricting dietary carbohydrates was the “single most effective intervention for reducing all the features of metabolic syndrome” and should therefore be the first approach in diabetes management. The greatest reductions in HbA1c and diabetic medication use were seen when carbohydrates were restricted to <10% of calorie intake.236 The evidence includes a number of short-term studies, including a meta-analysis, all of which found that low carbohydrate diets are highly therapeutic for diabetes.42,168,203,207,213,218,223,236–238 The improvements in glycemic control usually appear early and before significant weight loss.224 An advantage is seen in glycemic control in trials where a low-carbohydrate group is compared to a control group for a given weight loss.168,217,233 Another interesting feature of low carbohydrate diets is that, even if prescribed ad libitum to the participants with no obligation to restrict calorie intake in the study protocol, a spontaneous calorie restriction is quite often seen,239,240 perhaps suggesting that intake of unhealthy carbohydrates is associated with increased appetite. Evidence from short-term studies suggests that low carbohydrate diets produce greater (or at least the same) weight loss as traditional low fat (and low calorie) diets.240–250 2-year results from a recent ad libitum low-carbohydrate T2DM trial, which included patients with a longer duration of diabetes (8.4 years on average) and which did not exclude any patients on insulin, were very surprising. Normoglycaemia (off medications other than metformin) was achieved in 54% of those completing the study, and 74% were able to maintain the diet and complete the study, suggesting retention was higher than with normal diets. Typically, weight loss of 10% was recorded despite no calorie restriction.232
Adding to the general cause of LCDs, few of the studies have accounted for the withdrawal of drugs much more rapidly in the carbohydrate restriction arms than in control arms, perhaps underestimating the benefits of LCDs in some instances.
Dr David Unwin, an innovative GP expert in diabetes, has published evidence of the cost-benefits of low carbohydrate diet promotion in general practice, demonstrating significant savings from curtailed prescriptions. If all 9400 GPs in the UK chose to replicate Dr Unwin’s approach, the immediate savings could reach £423m annually for the NHS. This does not take into account the long-term savings in human and financial terms of preventing morbid complications of diabetes like blindness, strokes, peripheral arterial disease, renal failure, and heart attacks.156,251 It should be noted that attention from a long-time primary care practitioner might induce a motivating factor for patients out of loyalty and attachment that skews the data about LCDs from primary care practitioners- the so-called “practitioner effect”.
Low carbohydrate diets may also have an advantage for long-term weight maintenance. A variety of powerful epigenetic and genetic factors will drive weight regain after all types of successful weight loss program, usually as a result of a surge in appetite. Interestingly, participants assigned to a low carbohydrate diet after losing weight had significantly higher energy expenditure and lower levels of ghrelin (higher levels of which are presumed to lower energy expenditure and increase rebound appetite) than those assigned to a high carbohydrate diet. Total energy expenditure after weight loss was increased in those assigned a low carbohydrate diet with a linear trend of 52kcal per day (95% CI 23 to 82) for every 10% decrease in the calorific contribution of carbohydrate to total energy intake during weight maintenance.252
Low carbohydrate diets have been endorsed as an appropriate diet pattern by the ADA and the European Association for the Study of Diabetes (EASD).253,254 The WHO has published the LIMIT recommendations on dietary carbohydrates,255 and the introduction of sugar taxes in the UK (and elsewhere) could be followed by further policy measures if the results are positive.256
It is not known if restricting carbohydrates is easier for some patients than others, compared to reducing calories in general. Carbohydrates are addictive and quitting unhealthy sugars may be as difficult as smoking cessation.257 Dr Michael Mosley, another GP expert in low carbohydrate slimming, clearly alludes to the challenges of carbohydrate restriction for some patients in his articles, although he does not try to quantify or measure this aspect.258
A major limitation of the LCD literature base is that there are few studies of LCDs showing T2DM remission without also reporting weight loss. It is difficult to attribute pure causality to the LCD as a result. The underlying T2DM pathophysiology may still be intact, although not being fueled, unless there is weight loss. As soon as normal dietary patterns return, so could the T2DM. The other limitation of LCD literature is the lack of long-term studies, partly because it might be difficult to maintain a pure LCD for the long term. However, in practical terms, if the patient is able to maintain carbohydrate restriction appropriate for their personal threshold for euglycemia, it makes little difference to their continued enjoyment of euglycemia.
A major complication of the story of LCDs is that some advocates of these diets have advanced very controversial versions, in particular those which include a high fat intake,259 causing debate and paradoxically probably slowing down their more widespread adoption by health-care practitioners.260 It should be the common sense position that there is no one-size-fits-all prescriptive approach to making food choices, including restricting carbohydrates. Food choices should be underpinned by scientific evidence with the aim of achieving treatment goals, improving health, and quality of life. To improve compliance, they should also be acceptable and enjoyable. An individualized approach will need to be taken to some degree when practitioners want to advise on restricting unhealthy carbohydrates. Whilst the tolerance threshold for consumption of refined and starchy carbohydrates in patients with pre-diabetes and T2DM is a personal threshold, it is still likely to be much less than the average in normal individuals. In any single individual patient, the personal tolerance level for unhealthy carbohydrate intake will to some degree be moderated by other factors like exercise and genetics. More longer-term studies of LCDs with standardized definitions and comparable methodology will be required to determine and classify the optimum approach in patients and to maximize the duration of the associated metabolic benefits. Studies are still required to elucidate any long-term side effects and how to mitigate them.
Which Diet is Superior?
The published papers and real-world examples for both VLEDs and LCDs vary tremendously with respect to quality, robustness, numbers enrolled, counselling intervention strategy, intensity, and length of follow-up. With no direct, high-quality comparison of VLEDs and LCDs, it is not possible to say which is superior for T2DM remission. Like for pharmacotherapy, it would not be surprising if some combination of both approaches might be best of all. There is no evidence to suggest that it is not feasible to combine the approaches.
Even if a study were designed to compare VLEDs and LCDs, like all dietary research, it would not be realistic to expect participants to adhere purely to any dietary recommendation over a long period, effectively meaning that dietary trials are not randomized. This is apart from the fact that it is difficult to control carbohydrates as sugars are addictive.
It should also be remembered that not everybody with T2DM is overweight or obese. More research is needed to elucidate what dietary approach is most appropriate for this group. It might be that LCDs are more appropriate in patients who are normal weight as calorie restriction would not be required.
Exercise
For over 10 years, there has been a general consensus that exercise improves glycemic control.261,262 However, many people with diabesity are unable or unwilling to take exercise. Obesity alone can discourage exercise, for example if there are concomitant joint problems.263–266 Many diabetic patients who could take exercise, still choose not to, for many reasons, and until now, no behavioral interventions have been successful in reversing this problem.267 Therefore, prescribing sudden exercise on its own is less likely to be an effective first-line treatment to achieve remission of T2DM. There is little evidence that there is sufficient compliance with prescription exercise by T2DM patients to make a significant impact on diabetes in the population. However, thoughtfully structured exercise as an add-on, when prescribed carefully and in consideration of the context of the patient’s behavioral/psychological, musculoskeletal and cardiovascular status, can only accelerate and improve outcomes when combined with other approaches. As a minimum, practitioners should remember to advise the maintenance of usual physical activity, whilst avoiding any sudden surges, during dietary interventions for weight loss.268
Where it is possible to prescribe it (and some compliance is forthcoming), the impact of exercise in T2DM reversal might be maximized in the maintenance phase when restrictive diets are stopped and calorific intake increases. The Nutrition Practice Guideline (NPG) sets out an individualized exercise plan for diabetes. This guideline suggests aiming for >150 min/week of moderate-intensity (50–70% maximum heart rate) aerobic physical activity, divided between 3 days per week, and with no gap of more than two consecutive days without exercise.269 Daily physical activity is known to be an essential component of long-term weight control.270
It should come as no surprise to practitioners that there are many forms of exercise that can be prescribed. Numerous studies confirm that all kinds of physical activity and exercise results in immediate improvements in glycemic control. However, the types of exercise that appear most beneficial for reducing post-prandial glycaemia and insulin resistance appear to be pre-prandial resistance training and high-intensity interval exercise.270,271 Interestingly, some authors have conceded that prescribing voluntary exercise successfully is fraught for the majority of diabetic patients and that a completely different approach to prescription exercise in the sedentary needs to be taken. These authors have suggested that neuromuscular electrical stimulation (NMES) devices can deliver exercise in a sedentary population crucially without requiring any substantial patient movement at equivalent (or even faster) rates to voluntary aerobic exercise. A fit or obese person using an NMES system while watching television for 6 hours could burn over 2000 kcal - an impressive addition to non-exercise activity thermogenesis (NEAT). NMES devices are already widely used and available in rehabilitation and sports medicine for a range of indications. Exercising with NMES systems appears to improve both the strength as well as aerobic capacity of muscle – similar to vigorous voluntary exercise.272 Another attraction of modern NMES devices is that they are able to exercise big muscle groups directly without loading any joints, and without the need for extensive back, hip or knee movements – as these joints are often painful or at risk in diabetics.272–278
There is evidence that NMES can play an important role in controlling T2DM.279 Studies of NMES devices in diabetics have shown improvements in HbA1c equivalent to, or better than, taking real exercise.280 The average improvement in HbA1c of 0.8 ± 0.7% with NMES therapy is clinically significant and compares well with lifestyle intervention studies where an exercise effect of 0.62% improvement can be expected. Like most exercise modalities, improvement is seen even after short-term use.281,282 Of particular interest, there may be unexpected metabolic advantages of using NMES for type 2 diabetes, over and above voluntary exercise. Kimura et al283 have proposed the benefits of targeting type 2b muscle fibres in exercise for T2DM, as this is associated with a shift towards oxidative metabolism. NMES is thought to preferentially recruit these type 2b fibres when compared to voluntary exercise.284,285 When using NMES, it appears that the muscle is preferentially metabolizing carbohydrate as a substrate. This has been reported in healthy subjects273,286 but has also been noted in a small study with just nine obese patients.280 Consistent with this observation is the finding of high lactate levels, up to 15.3 mmol/L in two studies on healthy volunteers.273,287 Sola-Penna et al288 argue that lactate is probably ‘a regulatory molecule that modulates the integration of metabolism’ including glucose.
Much further research is needed to elucidate the basic metabolic mechanisms and to optimize exercise prescription with NMES therapy for type 2 diabetes. Commercial, patient-friendly, personal use devices specifically for type 2 diabetes have yet to emerge, although Slendertone has launched evidence-based NMES belts for general personal wellness.289 Practitioners working with type 2 diabetics need to keep abreast of advances in exercise science that could unlock the hugely beneficial role of exercise for an otherwise frequently sedentary population of patients.
Computer Modelling Reversal and Remission
Ha et al290 have explored and extended a mathematical model of the pathogenesis, prevention, and reversal of T2DM first envisaged by Topp et al.291 Simulations based on the model by Ha et al offer a mathematical explanation of how a moderate, gradual program of weight loss and exercise could be effective for preventing but not reversing diabetes, and diabetes of longer duration would be more difficult to reverse. Also, the model predicts that standard glucose-lowering drugs like metformin on their own could help with the prevention but never the reversal of established T2DM. On the other hand, acute caloric restrictions – whether via VLEDs or bariatric surgery – show immediate improvements in glycemic control, long before any weight loss, and are the interventions most likely to generate reversal and remission of T2DM. Further work on computer modelling would greatly assist clinical researchers, especially if it was possible to simulate whether interventions on their own or in novel combinations could reach the required threshold for remission.
Does Remission Translate into Better Long-Term Outcomes for T2DM Patients?
Whilst practitioners are still considering the many very positive results that upset the conventional wisdom and show T2DM to be reversible, the big questions for the future are how to convert reversal into a durable remission, and whether long-term remission can translate into the prevention of any (further) macrovascular, and more importantly, microvascular damage caused by the T2DM. Only long-term follow-up of patients in remission can unequivocally answer these questions.292 Interestingly, from long-term studies of remission after bariatric surgery, some predictors of remission have already been identified. These include diabetes duration, degree of medication use, glycemic control, BMI, manifestation and severity of co-morbidities, C-peptide levels (lower levels being a proxy marker of poor endogenous insulin production), and age.293 Further focus and study into the heterogeneity of these predictors will help practitioners optimize and personalize the approach for each T2DM patient and provide a framework for targeting and personalizing more effective support for remission to take place in addition to making it more durable.
Conclusions and Recommendations for Further Study
Multiple, disparate therapeutic interventions (from dietary to surgical) confirm that T2DM patients can become normoglycemic again, and early results suggest that this reversal could be maintained in the long term. Just as we struggle to untangle the complex role of diet in the pathogenesis and prevention of T2DM,294 we can postulate that, despite the variety of interventions, the underlying mechanisms of reversal in each therapeutic approach could have some pathway(s) in common – and some of these phenomena might be explained by the Taylor Twin Cycle Theory. This may seem paradoxical, because there is no obvious connection between, say, taking exercise and bariatric surgery, using orlistat or a GLP-1 agonist, but some shared underlying mechanisms or pathways should not come as a complete surprise. There is much underlying pathophysiological complexity, with many unknowns, but it is interesting that these widely disparate methods appear to boil down to metabolic interventions that can fix the pathophysiology from very different starting points. It is not yet known if the progression of macrovascular and microvascular disease in T2DM patients is prevented by long-term reversal or remission. Further studies are needed to address these points.
As the cost of diabetes has escalated, society can no longer afford to ignore the pandemic of lifestyle diseases, so understanding T2DM remission becomes more of a priority. Whereas the current standard of care still needs to be followed carefully, many practitioners might choose to promote reversal/remission to their patients based on the latest evidence. The current standard of care has done little to check the pandemic of diabetes. Therefore, this review has highlighted for the practitioner the various approaches to reversing T2DM. Table 4 summarizes some of those approaches.
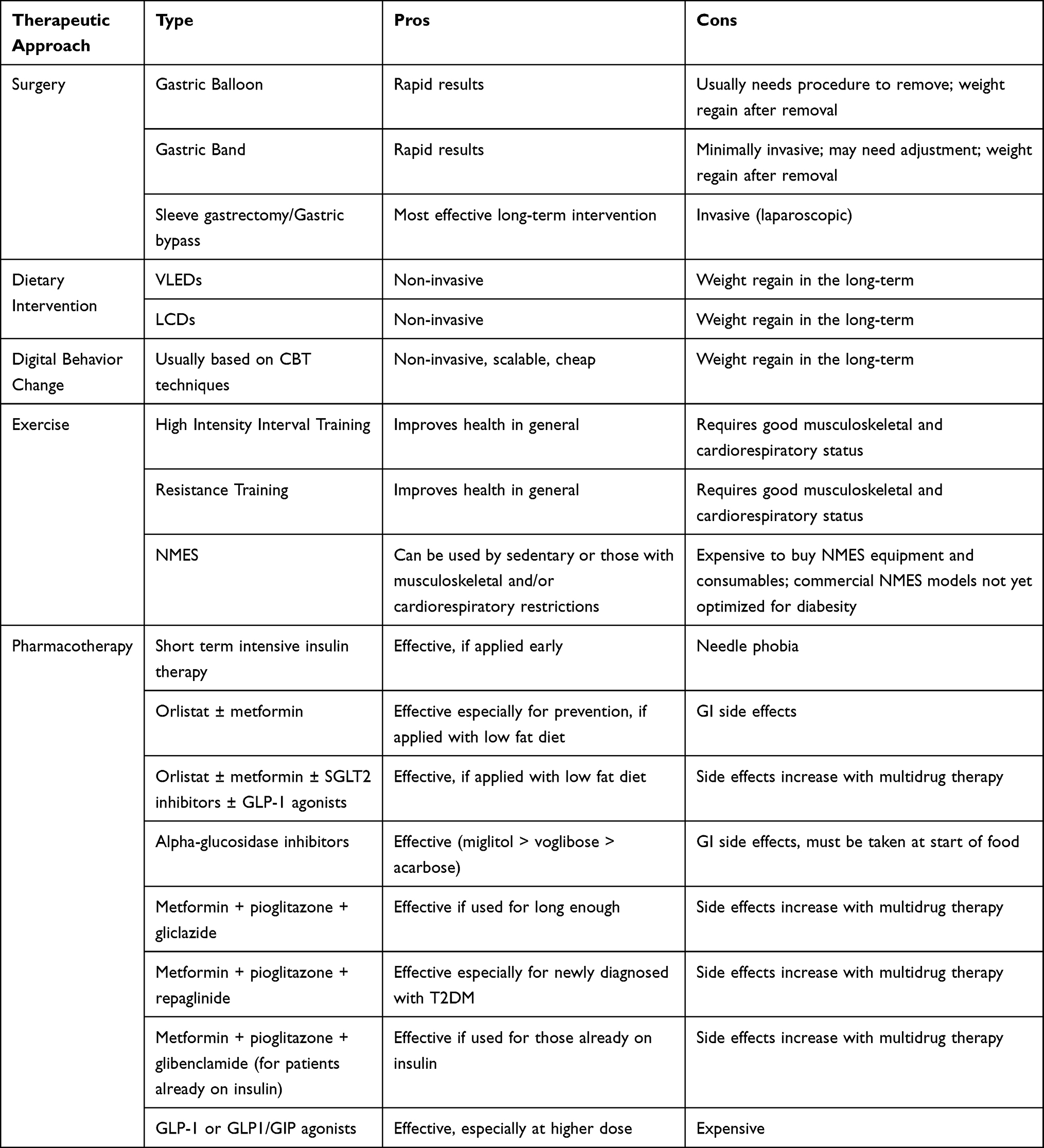 |
Table 4 A Summary of the Most Promising Therapeutic Approaches for Reversing T2DM |
The future is likely to present a stepwise approach to T2DM reversal and remission based on the patient’s metabolic baseline and background profile. Combination therapy – including possibly multi-drug therapy – rather than monotherapy will be the key feature of successful reversal and remission. Remission will be seen as the primary aim especially for pre-diabetes and newly diagnosed T2DM patients, who are the two groups most likely to go into long-term remission with the least effort.
Remission-focused services for T2DM are an emerging area and not a part of routine diabetes care. Formal remission services may not be feasible until long-term studies elucidate the efficacy of different approaches and also their optimum combination. Consequently, the field is left to opportunistic evidence-based practice. There is little consensus and few guideline recommendations regarding the optimum timing, combination, and mode of delivery of intervention components to help people achieve T2DM remission. Researchers will surely need to test many combinations – for example, whether there is added value from a very low calorie diet that is low carb at the same time. Reversal can now be supported by scalable digital behavior change, and practitioners can then pick from multi-drug pharmacotherapy (with or without a bariatric intervention) in a personalized way in order to truly move the T2DM needle from reversal onto long-term remission. The fact that a personalized, multi-disciplinary, and combination, step-wise approach is required for reversing T2DM should come as no surprise – in the same way that oncology patients are managed with a carefully filtered, personalized mix of surgery, radiotherapy, and chemotherapy based on sensitive, specific evidence-based markers (wherever possible) of their baseline disease status, disease profile, and response.
Practitioners should therefore see the various different approaches to T2DM reversal as entirely complementary to each other with common mechanistic pathways. There is already a large volume of (unhelpfully competing) literature available regarding the various strategies, medications, and interventions for reversing T2DM when used alone, and sometimes when used in dual or triple combinations – and studies are already emerging that many of these approaches can be combined safely and effectively, with some data on patient selection.
Data on all the different permutations of multi-drug combinations with all the other strategies and their impact on weight loss and glycemic control are not available yet. But the evidence that triple drug therapy is much more efficacious than mono or dual therapy is already emerging. Only much further study can give practitioners the bigger picture. A truly rationalized approach to T2DM reversal will come when all the numerous permutations of intervention available are studied in detail, providing the evidence base for practitioners to optimally combine all these therapies in a stepwise fashion that is personalized to patient baselines and profiles. For now, practitioners will have to rely on the available evidence and to be open-eyed about the possibilities of achieving better outcomes for their type 2 diabetic patients with combination approaches and aiming for remission more often, and earlier in the course of the disease.
This paper captures some of the exciting details about the possibilities of reversing T2DM – a disease that has always been viewed as chronic and progressive. It has tried to pick up the available evidence and fill in gaps as much as possible where guidelines fall silent. In particular, remission should be a treatment goal for those who are still pre-diabetic, newly diagnosed type 2 diabetics, and type 2 diabetics of less than 6 years duration – although that is not to rule out those who have had T2DM for longer – and practitioners should remember the main driver and predictor of long-term remission is weight loss of 15kg or more.17,18,160,295
The authors of this review paper propose that remission of T2DM should be the primary clinical goal in the management of T2DM. There is an abundance of options that have potential to effect T2DM remission, nearly all of which require weight loss. Although incurable, diabetes prevention, delay in onset, and reversal are real-world possibilities. When it comes to healthcare, one size does not fit all, and a mixture of different approaches and at different intensities is likely necessary to maximize remission rates. Patients will need to be offered a menu of options to choose from, and to be involved in this “mix and match” from the start. This review offers practitioners a practical, evidence-based approach in order for them to provide individualized care in a clinical setting on an informed basis. A lot more could be said about how to motivate people, society, and policy makers to understand the true impact of the diabesity pandemic. Prioritizing a wholesale change in our approach to T2DM is essential, because if the status quo is maintained, individuals, society at large, and our precious environment will pay an unacceptably high price.
Disclosure
Dr Mo Al-Qaisi reports involvement in the innovation start up Ziro Fibre Ltd, which is focused on diabesity reversal using functional appetite quenching drinks and digital behaviour change. The remaining authors report no conflicts of interest in this work.
References
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2013;380:2095–2128. doi:10.1016/S0140-6736(12)61728-0
2. Ma RC, Chan JC. T2DM in East Asians: similarities and differences with populations in Europe and the United States. Ann NY Acad Sci. 2013;1281:64–91. doi:10.1111/nyas.12098
3. Zimmet PZ, Magliano DJ, Herman WH, Shaw JE. Diabetes: a 21st century challenge. Lancet Diabetes Endocrinol. 2014;2:56–64. doi:10.1016/S2213-8587(13)70112-8
4. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14. doi:10.1016/j.diabres.2009.10.007
5. Colditz GA, Willett WC, Rotnitzky A, Manson JE. Weight gain as a risk factor for clinical diabetes mellitus in women. Ann Intern Med. 1995;122(7):481–486. doi:10.7326/0003-4819-122-7-199504010-00001
6. Chan JM, Rimm EB, Colditz GA, Stampfer MJ, Willett WC. Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care. 1994;17(9):961–969. doi:10.2337/diacare.17.9.961
7. American Diabetes Association. The cost of diabetes; 2018. Available from: https://www.diabetes.org/resources/statistics/cost-diabetes#:~:text=The%20American%20Diabetes%20Association%20(ADA,the%20cost%20was%20last%20examined).
8. Diabetes UK. The cost of diabetes report; 2017. Available from: https://www.diabetes.org.uk/resources-s3/201711/diabetes%20uk%20cost%20of%20diabetes%20report.pdf.
9. Kones R, Rumana U. Cardiometabolic diseases of civilization: history and maturation of an evolving global threat. An update and call to action. Ann Med. 2017;49(3):260–274. doi:10.1080/07853890.2016.1271957
10. UK prospective Diabetes Study Group. U.K. prospective diabetes study 16. Overview of 6 years’ therapy of type II diabetes: a progressive disease. Diabetes. 1995;44(11):1249–1258. doi:10.2337/diab.44.11.1249
11. Hallberg SJ, Gershuni VM, Hazbun TL, Athinarayanan SJ. Reversing T2DM: a narrative review of the evidence. Nutrients. 2019;11(4):E766. doi:10.3390/nu11040766
12. Taylor R. Reversing the irreversible: T2DM and you; 2014. Available from: https://campus.recap.ncl.ac.uk/Panopto/Pages/Embed.aspx?id=c3bef819-e5f4-4a55-876f-0a23436988ed.
13. Diabetes UK. Reversing T2DM; 2019. Available from: https://www.diabetes.co.uk/reversing-diabetes.html.
14. World Health Organization. Global report on diabetes; 2016. Available from: https://www.who.int/publications/i/item/9789241565257.
15. Riddle MC, Cefalu WT, Evans PH, et al. Consensus report: definition and interpretation of remission in type 2 diabetes. Diabetes Care. 2021;44(10):2438–2444. doi:10.2337/dci21-0034
16. Kalra S, Singal A, Lathia T. What’s in a name? Redefining type 2 diabetes remission. Diabetes Ther. 2021;12:647–654. doi:10.1007/s13300-020-00990-z
17. Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta‐analysis. Am J Med. 2009;122(3):248–256. doi:10.1016/j.amjmed.2008.09.041
18. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery. A systematic review and metaanalysis. JAMA. 2004;292(14):1724–1737. doi:10.1001/jama.292.14.1724
19. Pories WJ, MacDonald KG, Morgan EJ, et al. Surgical treatment of obesity and its effect on diabetes: 10-y follow-up. Am J Clin Nutr. 1992;55(2 Suppl):582S–585S. doi:10.1093/ajcn/55.2.582s
20. Taylor R. Type 2 diabetes: etiology and reversibility. Diabetes Care. 2013;36(4):1047–1055. doi:10.2337/dc12-1805
21. Mayor S. Obesity surgery achieves long term weight loss and prevents T2DM, study finds. BMJ. 2017;358:j4376. doi:10.1136/bmj.j4376
22. Wu G, Cai B, Yu F, et al. Meta-analysis of bariatric surgery versus non-surgical treatment for T2DM mellitus. Oncotarget. 2016;7(52):87511–87522. doi:10.18632/oncotarget.11961
23. Sjostrom L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683–2693. doi:10.1056/NEJMoa035622
24. Vetter ML, Ritter S, Wadden TA, Sarwer DB. Comparison of bariatric surgical procedures for diabetes remission: efficacy and mechanisms. Diabetes Spectr. 2012;25(4):200–210. doi:10.2337/diaspect.25.4.200
25. Salminen P, Helmiö M, Ovaska J, et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic Roux-en-Y gastric bypass on weight loss at 5 years among patients with morbid obesity: the SLEEVEPASS randomized clinical trial. JAMA. 2018;319(3):241–254. doi:10.1001/jama.2017.20313
26. Peterli R, Wölnerhanssen BK, Peters T, et al. Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Roux-en-Y Gastric Bypass on Weight Loss in Patients With Morbid Obesity: the SM-BOSS Randomized Clinical Trial. JAMA. 2018;319(3):255–265. doi:10.1001/jama.2017.20897
27. Ienca R, Al Jarallah M, Caballero A, et al. The procedureless elipse gastric balloon program: multicenter experience in 1770 consecutive patients. Obes Surg. 2020;30(9):3354–3362. doi:10.1007/s11695-020-04539-8
28. Qi L, Guo Y, Liu CQ, Huang ZP, Sheng Y, Zou DJ. Effects of bariatric surgery on glycemic and lipid metabolism, surgical complication and quality of life in adolescents with obesity: a systematic review and meta-analysis. Surg Obes Relat Dis. 2017;13(12):2037–2055. doi:10.1016/j.soard.2017.09.516
29. Ruiz-Cota P, Bacardí-Gascón M, Jiménez-Cruz A. Long-term outcomes of metabolic and bariatric surgery in adolescents with severe obesity with a follow-up of at least 5 years: a systematic review. Surg Obes Relat Dis. 2018;15:S1550.
30. Inge TH, Courcoulas AP, Jenkins TM, et al. Five-year outcomes of gastric bypass in adolescents as compared with adults. N Engl J Med. 2019;380(22):2136–2145. doi:10.1056/NEJMoa1813909
31. Olbers T, Beamish AJ, Gronowitz E, et al. Laparoscopic Roux-en-Y gastric bypass in adolescents with severe obesity (AMOS): a prospective, 5-year, Swedish nationwide study. Lancet Diabetes Endocrinol. 2017;5(3):174–183. doi:10.1016/S2213-8587(16)30424-7
32. Adams TD. In teens with severe obesity, can bariatric surgery wait until adulthood? N Engl J Med. 2019;380(22):2175–2177. doi:10.1056/NEJMe1905778
33. Ardestani A, Rhoads D, Tavakkoli A. Insulin cessation and diabetes remission after bariatric surgery in adults with insulin-treated T2DM. Diabetes Care. 2015;38(4):659–664. doi:10.2337/dc14-1751
34. Scheen AJ, De Flines J, De Roover A, et al. Bariatric surgery in patients with T2DM: benefits, risks, indications and perspectives. Diabetes Metab. 2009;35:537–543. doi:10.1016/S1262-3636(09)73463-9
35. Rubino F, Nathan D, Eckel RH, et al. Delegates of the 2nd Diabetes Surgery Summit. Metabolic surgery in the treatment algorithm for T2DM: a joint statement by International Diabetes Organizations. Diabetes Care. 2016;39:861–877. doi:10.2337/dc16-0236
36. Steven S, Carey PE, Small PK, Taylor R. Reversal of T2DM after bariatric surgery is determined by the degree of achieved weight loss in both short- and long-duration diabetes. Diabet Med. 2015;32:47–53. doi:10.1111/dme.12567
37. Federico A, Dallio M, Tolone S, et al. Gastrointestinal hormones, intestinal microbiota and metabolic homeostasis in obese patients: effect of bariatric surgery. In vivo. 2016;30:321–330.
38. Larraufie P, Roberts GP, McGavigan AK, et al. Important role of the GLP-1 axis for glucose homeostasis after bariatric surgery. Cell Rep. 2019;26(6):1399–1408.e6. doi:10.1016/j.celrep.2019.01.047
39. Anhe FF, Varin TV, Schertzer JD, Marette A. The gut microbiota as a mediator of metabolic benefits after bariatric surgery. Can J Diabetes. 2017;41:439–447. doi:10.1016/j.jcjd.2017.02.002
40. Medina DA, Pedreros JP, Turiel D, et al. Distinct patterns in the gut microbiota after surgical or medical therapy in obese patients. PeerJ. 2017;5:e3443. doi:10.7717/peerj.3443
41. Murphy R, Tsai P, Jullig M, Liu A, Plank L, Booth M. Differential changes in gut microbiota after gastric bypass and sleeve gastrectomy bariatric surgery vary according to diabetes remission. Obes Surg. 2017;27:917–925. doi:10.1007/s11695-016-2399-2
42. Sweeney TE, Morton JM. The human gut microbiome: a review of the effect of obesity and surgically induced weight loss. JAMA Surg. 2013;148:563–569. doi:10.1001/jamasurg.2013.5
43. Peat CM, Kleiman SC, Bulik CM, Carroll IM. The intestinal microbiome in bariatric surgery patients. Eur Eat Disord Rev. 2015;23:496–503. doi:10.1002/erv.2400
44. Sweeney TE, Morton JM. Metabolic surgery: action via hormonal milieu changes, changes in bile acids or gut microbiota? A summary of the literature. Best Pract Res Clin Gastroenterol. 2014;28:727–740. doi:10.1016/j.bpg.2014.07.016
45. Jackness C, Karmally W, Febres G, et al. Very low calorie diet mimics the early beneficial effect of Roux‐en‐Y gastric bypass on insulin sensitivity and β‐cell function in type 2 diabetic patients. Diabetes. 2013;62(9):3027–3032. doi:10.2337/db12-1762
46. Tadross JA, le Roux CW. The mechanisms of weight loss after bariatric surgery. Int J Obes. 2009;33(Suppl 1):S28–S32. doi:10.1038/ijo.2009.14
47. Cummings DE. Endocrine mechanisms mediating remission of diabetes after gastric bypass surgery. Int J Obes. 2009;33(Suppl 1):S33–40. doi:10.1038/ijo.2009.15
48. Noel OF, Still CD, Argyropoulos G, Edwards M, Gerhard GS. Bile acids, FXR, and metabolic effects of bariatric surgery. J Obes. 2016;2016:4390254. doi:10.1155/2016/4390254
49. Saeidi N, Meoli L, Nestoridi E, et al. Reprogramming of intestinal glucose metabolism and glycemic control in rats after gastric bypass. Science. 2013;341(6144):406–410. doi:10.1126/science.1235103
50. Chang SH, Stoll CR, Song J, Varela JE, Eagon CJ, Colditz GA. The effectiveness and risks of bariatric surgery: an updated systematic review and meta-analysis, 2003–2012. JAMA Surg. 2014;149(3):275–287. doi:10.1001/jamasurg.2013.3654
51. Arterburn D, Wellman R, Emiliano A, et al. Comparative effectiveness and safety of bariatric procedures for weight loss: a PCORnetCohort study. Ann Intern Med. 2018;169(11):741–750. doi:10.7326/M17-2786
52. Ma IT, Madura JA. Gastrointestinal complications after bariatric surgery. Gastroenterol Hepatol. 2015;11:526–535.
53. Rubino F, Schauer PR, Kaplan LM, Cummings DE. Metabolic surgery to treat T2DM: clinical outcome and mechanisms of action. Annu Rev Med. 2010;61:393–411. doi:10.1146/annurev.med.051308.105148
54. Abraham A, Ikramuddin S, Jahansouz C, Arafat F, Hevelone N, Leslie D. Trends in bariatric surgery: procedure selection, revisional surgeries, and readmissions. Obes Surg. 2016;26:1371–1377. doi:10.1007/s11695-015-1974-2
55. Tack J, Deloose E. Complications of bariatric surgery: dumping syndrome, reflux and vitamin deficiencies. Best Pract Res Clin Gastroenterol. 2014;28:741–749. doi:10.1016/j.bpg.2014.07.010
56. Eisenbarg D, Azagury DE, Ghiassi S, Grover BT, Ki JJ. ASMBS position statement on postprandial hyperinsulinemic hypoglycemia after bariatric surgery. Surg Obes Relat Dis. 2017;13:371–378. doi:10.1016/j.soard.2016.12.005
57. Science Daily. Bariatric surgery is safe option for managing T2DM in overweight or mildly obese patients; 2015. Available from: www.sciencedaily.com/releases/2015/11/151105160525.htm.
58. Huang ZP, Guo Y, Liu CQ, Qi L, Zou DJ, Zhou WP. The effect of metabolic surgery on nonobese patients (BMI<30 kg/m2) with t2dm: a systematic review. Surg Obes Relat Dis. 2018;14(6):810–820. doi:10.1016/j.soard.2018.02.013
59. Rubio-Almanza M, Hervás-Marín D, Cámara-Gómez R, Caudet-Esteban J, Merino-Torres JF. Does metabolic surgery lead to diabetes remission in patients with BMI < 30 kg/m2?: A meta-analysis. Obes Surg. 2019;29:1105–1116. doi:10.1007/s11695-018-03654-x
60. Goh YM, Toumi Z, Date RS. Surgical cure for T2DM by foregut or hindgut operations: a myth or reality? A systematic review. Surg Endosc. 2017;31(1):25–37. doi:10.1007/s00464-016-4952-4
61. Sjostrom L, Peltonen M, Jacobson P, et al. Association of bariatric surgery with long‐term remission of T2DM and with microvascular and macrovascular complications. JAMA. 2014;311:2297–2304. doi:10.1001/jama.2014.5988
62. Arterburn DE, Bogart A, Sherwood NE, et al. A multisite study of long‐term remission and relapse of T2DM mellitus following gastric bypass. Obes Surg. 2013;23:93–102. doi:10.1007/s11695-012-0802-1
63. Gazda CL, Clark JD, Lingvay I, Almandoz JP. Pharmacotherapies for post-bariatric weight regain: real-world comparative outcomes. Obesity. 2021;29(5):829–836. doi:10.1002/oby.23146
64. Daigle CR, Chaudhry R, Boules M, et al. Revisional bariatric surgery can improve refractory metabolic disease. Surg Obes Relat Dis. 2016;12(2):392–397. doi:10.1016/j.soard.2015.07.004
65. Haluzik M, Kratochvilova H, Haluzikova D, Mraz M. Gut as an emerging organ for the treatment of diabetes: focus on mechanism of action of bariatric and endoscopic interventions. J Endocrinol. 2018;237:R1–R17. doi:10.1530/JOE-17-0438
66. Park JY. Prediction of T2DM remission after bariatric or metabolic surgery. J Obes Metab Syndr. 2018;27(4):213–222. doi:10.7570/jomes.2018.27.4.213
67. Guidone C, Manco M, Valera-Mora E, et al. Mechanisms of recovery from T2DM after malabsorptive bariatric surgery. Diabetes. 2006;55:2025–2031. doi:10.2337/db06-0068
68. Samuel VT, Petersen KF, Shulman GI. Lipid-induced insulin resistance: unravelling the mechanism. Lancet. 2010;375:2267–2277. doi:10.1016/S0140-6736(10)60408-4
69. Taylor R. Banting memorial lecture 2012: reversing the twin cycles of T2DM. Diabet Med. 2013;30(3):267–275. doi:10.1111/dme.12039
70. Taylor R. Pathogenesis of T2DM: tracing the reverse route from cure to cause. Diabetologia. 2008;51:1781–1789. doi:10.1007/s00125-008-1116-7
71. Sattar N, McConnachie A, Ford I, et al. Serial metabolic measurements and conversion to T2DM in the west of Scotland coronary prevention study: specific elevations in alanine aminotransferase and triglycerides suggest hepatic fat accumulation as a potential contributing factor. Diabetes. 2007;56:984–991. doi:10.2337/db06-1256
72. Adiels M, Taskinen MR, Packard C, et al. Overproduction of large VLDL particles is driven by increased liver fat content in man. Diabetologia. 2006;49:755–765. doi:10.1007/s00125-005-0125-z
73. White MG, Shaw JA, Taylor R. T2DM: the pathologic basis of reversible β-cell dysfunction. Diabetes Care. 2016;39(11):2080–2088. doi:10.2337/dc16-0619
74. Neuffer P. Key to T2DM remission may be loss of half a gram of pancreas fat; 2019. Available from: https://www.healio.com/endocrinology/diabetes/news/online/%7B3262844a-137c-4cbc-a1d3-aba49b0f378b%7D/key-to-type-2-diabetes-remission-may-be-loss-of-half-a-gram-of-pancreas-fat.
75. Dyson PA, Twenefour D, Breen C, et al. Diabetes UK evidence‐based nutrition guidelines for the prevention and management of diabetes. Diabet Med. 2018;35(5):541–547. doi:10.1111/dme.13603
76. Godlee F. Pills are not the answer to unhealthy lifestyles. BMJ. 2018;362:k3046. doi:10.1136/bmj.k3046
77. Wieseler B, McGauran N, Kaiser T. New drugs: where did we go wrong and what can we do better? BMJ. 2019;366:l4340. doi:10.1136/bmj.l4340
78. Diabetes remission- “treating blood glucose, when the disease process is to do with body fat” [podcast on the Internet]. BMJ talk medicine; 2018. Available from: https://soundcloud.com/bmjpodcasts/diabetes-remission-treating-blood-glucose-when-The-disease-process-is-to-do-with-body-fat.
79. Prasad V. Rosiglitazone, medical reversal, and back to basics for diabetes. Am Fam Physician. 2014;90(6):368, 370.
80. Kazemian P, Shebl FM, McCann N, Walensky RP, Wexler DJ. Evaluation of the cascade of diabetes care in the United States, 2005–2016. JAMA Intern Med. 2019;179(10):1376–1385. doi:10.1001/jamainternmed.2019.2396
81. Karter AJ, Nundy S, Parker MM, Moffet HH, Huang ES. Incidence of remission in adults with T2DM: the diabetes & aging study. Diabetes Care. 2014;37:3188–3195. doi:10.2337/dc14-0874
82. Weng J, Li Y, Xu W, et al. Effect of intensive insulin therapy on beta-cell function and glycaemic control in patients with newly diagnosed type 2 diabetes: a multicentre randomised parallel-group trial. Lancet. 2008;371(9626):1753–1760. doi:10.1016/S0140-6736(08)60762-X
83. Chen A, Huang Z, Wan X, et al. Attitudes toward diabetes affect maintenance of drug-free remission in patients with newly diagnosed type 2 diabetes after short-term continuous subcutaneous insulin infusion treatment. Diabetes Care. 2012;35(3):474–481. doi:10.2337/dc11-1638
84. Kramer CK, Zinman B, Retnakaran R. Short-term intensive insulin therapy in type 2 diabetes mellitus: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2013;1(1):28–34. doi:10.1016/S2213-8587(13)70006-8
85. Wang H, Kuang J, Xu M, et al. Predictors of long-term glycemic remission after 2-week intensive insulin treatment in newly diagnosed type 2 diabetes. J Clin Endocrinol Metab. 2019;104(6):2153–2162. doi:10.1210/jc.2018-01468
86. McInnes N, Hall S, Sultan F, et al. Remission of type 2 diabetes following a short-term intervention with insulin glargine, metformin, and dapagliflozin. J Clin Endocrinol Metab. 2020;105(8):dgaa248. doi:10.1210/clinem/dgaa248
87. Kramer CK, Zinman B, Choi H, Retnakaran R. Predictors of sustained drug-free diabetes remission over 48 weeks following short-term intensive insulin therapy in early type 2 diabetes. BMJ Open Diabetes Res Care. 2016;4(1):e000270. doi:10.1136/bmjdrc-2016-000270
88. Jennings AS, Lovett AJ, George TM, Jennings JS. Getting to goal in newly diagnosed type 2 diabetes using combination drug “subtraction therapy”. Metabolism. 2015;64(9):1005–1012. doi:10.1016/j.metabol.2015.04.008
89. Panikar V, Joshi SR, Bukkawar A, Nasikkar N, Santwana C. Induction of long-term glycemic control in type 2 diabetic patients using pioglitazone and metformin combination. J Assoc Physicians India. 2007;55:333–337.
90. Panikar V, Chandalia HB, Joshi SR, Fafadia A, Santvana C. Beneficial effects of triple drug combination of pioglitazone with glibenclamide and metformin in type 2 diabetes mellitus patients on insulin therapy. J Assoc Physicians India. 2003;51:1061–1064.
91. Wilding J. Orlistat: should we worry about liver inflammation? BMJ. 2013;346:f2777. doi:10.1136/bmj.f2777
92. Kalra S, Jacob JJ, Gupta Y. Newer antidiabetic drugs and calorie restriction mimicry. Indian J Endocrinol Metab. 2016;20(1):142–146. doi:10.4103/2230-8210.172242
93. Halpern A, Mancini MC, Suplicy H, et al. Latin-American trial of orlistat for weight loss and improvement in glycemic profile in obese diabetic patients. Diabetes Obes Metab. 2003;5(3):180–188. doi:10.1046/j.1463-1326.2003.00262.x
94. Didangelos TP, Thanopoulou AK, Bousboulas SH, et al. The ORLIstat and CArdiovascular risk profile in patients with metabolic syndrome and T2DM (ORLICARDIA) study. Curr Med Res Opin. 2004;20(9):1393–1401. doi:10.1185/030079904125004466
95. Hoffmann J, Spengler M. Efficacy of 24-week monotherapy with acarbose, glibenclamide, or placebo in NIDDM patients. The Essen study. Diabetes Care. 1994;17(6):561–566. doi:10.2337/diacare.17.6.561
96. Hoffmann J, Spengler M. Efficacy of 24-week monotherapy with acarbose, metformin, or placebo in dietary-treated NIDDM patients: the Essen-II Study. Am J Med. 1997;103(6):483. doi:10.1016/S0002-9343(97)00252-0
97. Johansen K. Efficacy of metformin in the treatment of NIDDM. Meta-analysis. Diabetes Care. 1999;22(1):33–37. doi:10.2337/diacare.22.1.33
98. Kelley DE, Bray GA, Pi-Sunyer FX, et al. Clinical efficacy of orlistat therapy in overweight and obese patients with insulin-treated T2DM. A 1-year randomized controlled trial. Diabetes Care. 2002;25:1033–1041. doi:10.2337/diacare.25.6.1033
99. Miles JM, Leiter L, Hollander P, et al. Effect of orlistat in overweight and obese patients with T2DM treated with metformin. Diabetes Care. 2002;25(7):1123–1128. doi:10.2337/diacare.25.7.1123
100. Hollander PA, Elbein SC, Hirsch IB, et al. Role of orlistat in the treatment of obese patients with T2DM. A 1-year randomized double-blind study. Diabetes Care. 1998;21:1288–1294. doi:10.2337/diacare.21.8.1288
101. Berne C. A randomized study of orlistat in combination with a weight management programme in obese patients with T2DM treated with metformin. Diabet Med. 2005;22:612–618. doi:10.1111/j.1464-5491.2004.01474.x
102. Torgerson JS, Hauptman J, Boldrin MN, Sjostrom L. XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of T2DM in obese patients. Diabetes Care. 2004;27(1):155–161. doi:10.2337/diacare.27.1.155
103. Williamson DA, Bray GA, Ryan DH. Is 5% weight loss a satisfactory criterion to define clinically significant weight loss? Obesity. 2015;23(12):2319–2320. doi:10.1002/oby.21358
104. Wing RR, Marcus MD, Epstein LH, Salata R. Type II diabetic subjects lose less weight than their overweight nondiabetic spouses. Diabetes Care. 1987;10:563–566. doi:10.2337/diacare.10.5.563
105. Lindgarde F; on behalf of the orlistat Swedish multimorbidity study group. The effect of orlistat on bodyweight and coronary heart disease risk profile in obese patients: the Swedish Multimorbidity study. J Intern Med. 2000;248:245–254. doi:10.1046/j.1365-2796.2000.00720.x
106. Kelley DE, Kuller LH, McKolanis TM, Harper P, Mancino J, Kalhan S. Effects of moderate weight loss and orlistat on insulin resistance, regional adiposity, and fatty acids in T2DM. Diabetes Care. 2004;27:33–40. doi:10.2337/diacare.27.1.33
107. Jacob S, Meier MK, Rabbia M, Hauptman J. Orlistat has positive effects on glycemic control in T2DM beyond the improvements produced by weight loss alone. Obes Rev. 2006;7(Suppl 2):336.
108. Jacob S, Rabbia M, Meier MK, Hauptman J. Orlistat 120 mg improves glycemic control in type 2 diabetic patients with or without concurrent weight loss. Diabetes Obes Metab. 2009;11(4):361–371. doi:10.1111/j.1463-1326.2008.00970.x
109. Rowe R, Cowx M, Poole C, McEwan P, Morgan C, Walker M. The effects of orlistat in patients with diabetes: improvement in glycemic control and weight loss. Curr Med Res Opin. 2005;21(11):1885–1890. doi:10.1185/030079905X74943
110. Kissebah AH, Krakower GR. Regional adiposity and morbidity. Physiol Rev. 1994;74(4):761–811. doi:10.1152/physrev.1994.74.4.761
111. Boyko EJ, Fujimoto WY, Leonetti DL, Newell-Morris L. Visceral adiposity and risk of T2DM: a prospective study among Japanese Americans. Diabetes Care. 2000;23(4):465–471. doi:10.2337/diacare.23.4.465
112. Calles-Escandon J, Cipolla M. Diabetes and endothelial dysfunction: a clinical perspective. Endocr Rev. 2001;22(1):36–52. doi:10.1210/edrv.22.1.0417
113. Eldor R, Raz I. Lipotoxicity versus adipotoxicity-The deleterious effects of adipose tissue on beta cells in the pathogenesis of T2DM. Diabetes Res Clin Pract. 2006;74(2 Suppl):S3–S8. doi:10.1016/j.diabres.2006.06.004
114. Mancini MC, Halpern A. Orlistat in the prevention of diabetes in the obese patient. Vasc Health Risk Manag. 2008;4(2):325–336. doi:10.2147/VHRM.S6808
115. Brandberg J, Lönn L, Peltonen M, et al. Body composition changes during 4 years of treatment with orlistat vs placebo (The XENDOS study). Int J Obes. 2003;27(Suppl 1):S100.
116. Tiikkainen M, Bergholm R, Rissanen A, et al. Effects of equal weight loss with orlistat and placebo on body fat and serum fatty acid composition and insulin resistance in obese women. Am J Clin Nutr. 2004;79:22–30. doi:10.1093/ajcn/79.1.22
117. Mendoza-Guadarrama LG, Lopez-Alvarenga JC, Castillo-Martinez L, et al. Orlistat reduces visceral fat independent of weight changes in obese diabetics type 2. Int J Obes. 2000;24(Suppl 1):S167.
118. Hanefeld M, Sachse G. The effects of orlistat on body weight and glycemic control in overweight patients with T2DM: a randomized, placebo-controlled trial. Diabetes Obes Metab. 2002;4:415–423. doi:10.1046/j.1463-1326.2002.00237.x
119. Shi YF, Pan CY, Hill J, Gao Y. Orlistat in the treatment of overweight or obese Chinese patients with newly diagnosed T2DM. Diabet Med. 2005;22:1737–1743. doi:10.1111/j.1464-5491.2005.01723.x
120. Ferrannini E, Barrett EJ, Bevilacqua S, et al. Effect of fatty acids on glucose production and utilization in man. J Clin Invest. 1983;72:1737–1747. doi:10.1172/JCI111133
121. Piatti PM, Monti LD, Davis SN, et al. Effects of an acute decrease in non-esterified fatty acid levels on muscle glucose utilization and forearm indirect calorimetry in lean NIDDM subjects. Diabetologia. 1996;103–112. doi:10.1007/BF00400420
122. Randle PJ. Regulatory interactions between lipids and carbohydrates: the glucose fatty acid cycle after 35 years. Diabetes Metab Rev. 1998;14:263–283. doi:10.1002/(SICI)1099-0895(199812)14:4<263::AID-DMR233>3.0.CO;2-C
123. Santomauro AT, Boden G, Silva ME, et al. Overnight lowering of free fatty acids with Acipimox improves insulin resistance and glucose tolerance in obese diabetic and nondiabetic subjects. Diabetes. 1999;48:1836–1841. doi:10.2337/diabetes.48.9.1836
124. Kelley DE, Williams K, Price J, et al. Plasma fatty acids, adiposity and variance of skeletal muscle insulin resistance in T2DM mellitus. J Clin Endocrinol Metab. 2001;86:5412–5419. doi:10.1210/jcem.86.11.8027
125. Boden G, Chen X. Effects of fat on glucose uptake and utilization in patients with non-insulin-dependent diabetes. J Clin Invest. 1995;96:1261–1268. doi:10.1172/JCI118160
126. Carpentier A, Mittelman SD, Lamarche B, Bergman RN, Giacca A, Lewis GF. Acute enhancement of insulin secretion by FFA in humans is lost with prolonged FFA elevation. Am J Physiol. 1999;276:E1055–E1066. doi:10.1152/ajpendo.1999.276.6.E1055
127. Carpentier A, Mittelman SD, Bergman RN, Giacca A, Lewis GF. Prolonged elevation of plasma free fatty acids impairs pancreatic b-cell function in obese nondiabetic humans but not in individuals with T2DM. Diabetes. 2000;49:399–408. doi:10.2337/diabetes.49.3.399
128. Harding A-H, Sargeant LA, Welch A, et al. Fat consumption and HbA1c levels. The EPIC-Norfolk Study. Diabetes Care. 2001;24:1911–1916. doi:10.2337/diacare.24.11.1911
129. Boden G. Free fatty acids – the link between obesity and insulin resistance. Endocr Pract. 2001;7:44–51. doi:10.4158/EP.7.1.44
130. Roust LR, Jensen MJ. Postprandial free fatty acid kinetics are abnormal in upper body obesity. Diabetes. 1993;42:1567–1573. doi:10.2337/diab.42.11.1567
131. Thomsen C, Storm H, Holst JJ, et al. Differential effects of saturated and monounsaturated fats on postprandial lipemia and glucagon-like peptide 1 responses in patients with T2DM. Am J Clin Nutr. 2003;77:605–611. doi:10.1093/ajcn/77.3.605
132. Vilsboll T, Krarup T, Sonne J, et al. Incretin secretion in relation to meal size and body weight in healthy subjects and people with type 1 and T2DM mellitus. J Clin Endocrinol Metab. 2003;88:2706–2713. doi:10.1210/jc.2002-021873
133. Zander M, Madsbad S, Madsen JL, Holst JJ. Effect of 6-week course of glucagon-like peptide 1 on glycemic control, insulin sensitivity, and beta-cell function in T2DM: a parallel-group study. Lancet. 2002;359:824–830. doi:10.1016/S0140-6736(02)07952-7
134. Damci T, Yalin S, Balci H, et al. Orlistat augments postprandial increases in glucagon-like peptide 1 in obese type 2 diabetic patients. Diabetes Care. 2004;27:1077–1080. doi:10.2337/diacare.27.5.1077
135. Grudén S, Forslund A, Alderborn G, Söderhäll A, Hellström PM, Holmbäck U. Safety of a novel weight loss combination product containing orlistat and acarbose. Clin Pharmacol Drug Dev. 2021;10(10):1242–1247. doi:10.1002/cpdd.920
136. Holmbäck U, Forslund A, Grudén S, et al. Effects of a novel combination of orlistat and acarbose on tolerability, appetite, and glucose metabolism in persons with obesity. Obes Sci Pract. 2020;6(3):313–323. doi:10.1002/osp4.405
137. Sugihara H, Nagao M, Harada T, et al. Comparison of three α-glucosidase inhibitors for glycemic control and bodyweight reduction in Japanese patients with obese type 2 diabetes. J Diabetes Investig. 2014;5(2):206–212. doi:10.1111/jdi.12135
138. Lilly. Lilly’s SURPASS-1 results published in The Lancet show tirzepatide’s superior A1C and body weight reductions versus placebo in adults with T2DM; 2021. Available from: http://lilly.mediaroom.com/2021-06-26-Lillys-SURPASS-1-results-published-in-The-Lancet-show-tirzepatides-superior-A1C-and-body-weight-reductions-versus-placebo-in-adults-with-type-2-diabetes.
139. Lilly. Tirzepatide significantly reduced A1C and body weight in people with T2DM in two phase 3 trials from Lilly’s SURPASS program; 2021. Available from: https://investor.lilly.com/news-releases/news-release-details/tirzepatide-significantly-reduced-a1c-and-body-weight-people.
140. Everyday Health. More evidence once-weekly semaglutide injection helps people with diabetes lose weight; 2021. Available from: https://www.everydayhealth.com/type-2-diabetes/more-evidence-once-weekly-semaglutide-injection-helps-people-with-diabetes-lose-weight/.
141. Dutta D, Jaisani R, Khandelwal D, Ghosh S, Malhotra R, Kalra S. Role of metformin, Sodium-Glucose Cotransporter-2 (SGLT2) inhibitors, Glucagon-Like Peptide-1 (GLP-1) receptor agonists, and orlistat based multidrug therapy in glycemic control, weight loss, and euglycemia in diabesity: a real-world experience. Indian J Endocrinol Metab. 2019;23(4):460–467. doi:10.4103/ijem.IJEM_185_19
142. Vickers SP, Cheetham SC, Headland KR, et al. Combination of the sodium-glucose cotransporter-2 inhibitor empagliflozin with orlistat or sibutramine further improves the body-weight reduction and glucose homeostasis of obese rats fed a cafeteria diet. Diabetes Metab Syndr Obes. 2014;7:265–275. doi:10.2147/DMSO.S58786
143. Chua MWJ. High-dose liraglutide and SGLT2 inhibitor: a promising combination. Clin Pract. 2021;12(1):1–7. doi:10.3390/clinpract12010001
144. American Diabetes Association. Nutrition recommendations and interventions for diabetes. A position statement of the American Diabetes Association. Diabetes Care. 2008;31(Suppl 1):S61–78. doi:10.2337/dc08-S061
145. Wilding JP. The importance of weight management in T2DM mellitus. Int J Clin Pract. 2014;68(6):682–691. doi:10.1111/ijcp.12384
146. Public Health England. Adult obesity and T2DM; 2014. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/338934/Adult_obesity_and_type_2_diabetes_.pdf.
147. Bistrian BR, Blackburn GL, Flatt JP, Sizer J, Scrimshaw NS, Sherman M. Nitrogen metabolism and insulin requirements in obese diabetic adults on a protein-sparing modified fast. Diabetes. 1976;25:494–504. doi:10.2337/diab.25.6.494
148. Bauman WA, Schwartz E, Rose HG, Eisenstein HN, Johnson DW. Early and long term effects of acute caloric deprivation in obese diabetic patients. Am J Med. 1988;85:38–46. doi:10.1016/0002-9343(88)90500-1
149. Hughes TA, Gwynne JT, Switzer BR, Herbst C, White G. Effects of caloric restriction and weight loss on glycemic control, insulin release and resistance, and atherosclerotic risk in obese patients with type II diabetes mellitus. Am J Med. 1984;77:7–17. doi:10.1016/0002-9343(84)90429-7
150. Hammer S, Snel M, Lamb HJ, et al. Prolonged caloric restriction in obese patients with T2DM mellitus decreases myocardial triglyceride content and improves myocardial function. J Am Coll Cardiol. 2008;52:1006–1012. doi:10.1016/j.jacc.2008.04.068
151. Snel M, Jonker JT, Hammer S, et al. Long-term beneficial effect of a 16-week very low calorie diet on pericardial fat in obese T2DM mellitus patients. Obesity. 2012;20:1572–1576. doi:10.1038/oby.2011.390
152. Paisey RB, Harvey P, Rice S, et al. An intensive weight loss programme in established T2DM and controls: effect on weight and atherosclerosis risk factors at 1 year. Diabet Med. 1998;15:73–79. doi:10.1002/(SICI)1096-9136(199801)15:1<73::AID-DIA516>3.0.CO;2-F
153. Wing RR, Blair E, Marcus M, Epstein LH, Harvey J. Year-long weight loss treatment for obese patients with type II diabetes: does including an intermittent very-low-calorie diet improve outcome? Am J Med. 1994;97:354–362. doi:10.1016/0002-9343(94)90302-6
154. van Gaal L, Scheen A. Weight management in T2DM: current and emerging approaches to treatment. Diabetes Care. 2015;38(6):1161–1172. doi:10.2337/dc14-1630
155. Kmietowicz Z. GP based weight loss programme can reverse T2DM. BMJ. 2017;359:j5641. doi:10.1136/bmj.j5641
156. Lean MEJ, Leslie WS, Barnes AC, et al. Durability of a primary care-led weight-management intervention for remission of T2DM: 2-year results of the DiRECT open-label, cluster-randomised trial. Lancet Diabetes Endocrinol. 2019;7(5):344–355. doi:10.1016/S2213-8587(19)30068-3
157. Feinmann J. Low calorie and low carb diets for weight loss in primary care. BMJ. 2018;360:k1122. doi:10.1136/bmj.k1122
158. Feinmann J. T2DM: 5000 patients to test feasibility of “remission service”. BMJ. 2018;363:k5114. doi:10.1136/bmj.k5114
159. Steven S, Hollingsworth KG, Al‐Mrabeh A, et al. Very low‐calorie diet and 6 months of weight stability in type 2 diabetes: pathophysiological changes in responders and nonresponders. Diabetes Care. 2016;39(5):808–815. doi:10.2337/dc15-1942
160. Thom G, Messow C‐M, Leslie WS, et al. Predictors of type 2 diabetes remission in the Diabetes Remission Clinical Trial (DiRECT). Diabet Med. 2020;21:e14395.
161. Artinian NT, Fletcher GF, Mozaffarian D, et al. Interventions to promote physical activity and dietary lifestyle changes for cardiovascular risk factor reduction in adults: a scientific statement from the American Heart Association. Circulation. 2010;122(4):406–441. doi:10.1161/CIR.0b013e3181e8edf1
162. McCombie L, Brosnahan N, Ross H, Bell‐Higgs A, Govan L, Lean MEJ. Filling the intervention gap: service evaluation of an intensive nonsurgical weight management programme for severe and complex obesity. J Hum Nutr Diet. 2019;32(3):329–337. doi:10.1111/jhn.12611
163. Changing Health. Changing health appointed by NHS to deliver national T2DM programme. 2020. Available from: https://www.changinghealth.com/article/changing-health-appointed-by-nhs-to-deliver-national-type-2-diabetes-programme/.
164. Little P, Stuart B, Hobbs FR, et al. An internet-based intervention with brief nurse support to manage obesity in primary care (POWeR+): a pragmatic, parallel-group, randomised controlled trial. Lancet Diabetes Endocrinol. 2016;4(10):821–828. doi:10.1016/S2213-8587(16)30099-7
165. Spahn JM, Reeves RS, Keim KS, et al. State of the evidence regarding behavior change theories and strategies in nutrition counseling to facilitate health and food behavior change. J Am Diet Assoc. 2010;110(6):879–891. doi:10.1016/j.jada.2010.03.021
166. Novo Nordisk. Novo Nordisk and Noom to partner around digital health solutions to help people with obesity lose weight and keep it off; 2019. Available from: https://mL-eu.globenewswire.com/Resource/Download/353ec32a-cdea-4f9e-ba99-05a4cd1fabe5.
167. Ried‐Larsen M, Johansen MY, MacDonald CS, et al. Type 2 diabetes remission 1 year after an intensive lifestyle intervention: a secondary analysis of a randomized clinical trial. Diabetes Obes Metab. 2019;21(10):2257–2266. doi:10.1111/dom.13802
168. Saslow LR, Daubenmier JJ, Moskowitz JT, et al. Twelve-month outcomes of a randomized trial of a moderate-carbohydrate versus very low-carbohydrate diet in overweight adults with T2DM mellitus or prediabetes. Nutr Diabetes. 2017;7:304. doi:10.1038/s41387-017-0006-9
169. Taylor R, Al-Mrabeh A, Zhyzhneuskaya S, et al. Remission of human T2DM requires decrease in liver and pancreas fat content but is dependent upon capacity for β cell recovery. Cell Metab. 2018;28(4):547–556.e3. doi:10.1016/j.cmet.2018.07.003
170. McInnes N, Smith A, Otto R, et al. Piloting a remission strategy in type 2 diabetes: results of a randomized controlled trial. J Clin Endocrinol Metab. 2017;102(5):1596–1605. doi:10.1210/jc.2016-3373
171. Al‐Mrabeh A, Zhyzhneuskaya SV, Peters C, et al. Hepatic lipoprotein export and remission of human type 2 diabetes after weight loss. Cell Metab. 2020;31(2):233–249. doi:10.1016/j.cmet.2019.11.018
172. Bhatt AA, Choudhari PK, Mahajan RR, et al. Effect of a low-calorie diet on restoration of normoglycemia in obese subjects with type 2 diabetes. Indian J Endocrinol Metab. 2017;21(5):776–780. doi:10.4103/ijem.IJEM_206_17
173. Lim EL, Hollingsworth KG, Aribisala BS, Chen MJ, Mathers JC, Taylor R. Reversal of type 2 diabetes: normalisation of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia. 2011;54(10):2506–2514. doi:10.1007/s00125-011-2204-7
174. University of Oxford Diabetes Trials Unit. Reversal of T2DM upon normalisation of energy intake in the non-obese. 2018. Available from: https://www.dtu.ox.ac.uk/OurTrials/ReTune.php.
175. Taylor R. Key to T2DM remission may be loss of half a gram of pancreas fat. 2019. Available from: https://www.healio.com/news/endocrinology/20190427/key-to-type-2-diabetes-remission-may-be-loss-of-half-a-gram-of-pancreas-fat.
176. Mathew R. Liquid diets offer promise, but we still need upstream solutions. BMJ. 2019;364:k5340. doi:10.1136/bmj.k5340
177. Gardner CD, Kim S, Bersamin A, et al. Micronutrient quality of weight-loss diets that focus on macronutrients: results from the A to Z study. Am J Clin Nutr. 2010;92:304–312. doi:10.3945/ajcn.2010.29468
178. Low carb diets – a balanced approach. [document on the Internet]. Cambridge: Cambridgeshire and Peterborough NHS Foundation Trust; 2019. Available from: https://www.cambridgeshireandpeterboroughccg.nhs.uk/easysiteweb/getresource.axd?assetid=17806&type=0&servicetype=1https://www.cambridgeshireandpeterboroughccg.nhs.uk/easysiteweb/getresource.axd?assetid=17806&type=0&servicetype=1.
179. Quality and outcomes framework (QOF) indicator development programme. [document on the Internet]. London: National Institute for Health and Clinical Excellence; 2004. Available from: https://www.nice.org.uk/Media/Default/standards-and-indicators/qof%20indicator%20key%20documents/NM28%20briefing%20paper%20to%20the%20Advisory%20Committee%20on%20diabetes%20mellitus.pdf.
180. Feinman RD, Pogozelski WK, Astrup A, et al. Dietary carbohydrate restriction as the first approach in diabetes management: critical review and evidence base. Nutrition. 2015;31(1):1–13. doi:10.1016/j.nut.2014.06.011
181. Campbell WR. Dietetic treatment in diabetes mellitus. Can Med Assoc J. 1923;13:487–492.
182. Westman EC, Yancy WS, Humphreys M. Dietary treatment of diabetes mellitus in the pre-insulin era (1914–1922). Perspect Biol Med. 2006;49:77–83. doi:10.1353/pbm.2006.0017
183. Diabetes UK. William Banting; 2019. Available from: https://www.diabetes.co.uk/pioneers/william-banting.html.
184. Arky R, Wylie-Rosett J, El-Beheri B. Examination of current dietary recommendations for individuals with diabetes mellitus. Diabetes Care. 1982;5:59–63. doi:10.2337/diacare.5.1.59
185. Anderson JW, Geil PB. New perspectives in nutrition management of diabetes mellitus. Am J Med. 1988;85:159–165. doi:10.1016/0002-9343(88)90410-X
186. National Advisory Committee on Nutritional Education (NACNE). Proposals for nutritional guidelines for health education in Britain. Extracts from a consultative document prepared for the National Advisory Committee on Nutrition Education (NACNE). Lancet. 1983;2(8352):719–721.
187. Credit Suisse Research Institute. Fat: the new health paradigm; 2015. Available from: https://research-doc.credit-suisse.com/docView?language=ENG&source=ulg&format=PDF&document_id=1053247551&serialid=MFT6JQWS%2B4FvvuMDBUQ7v9g4cGa84/gpv8mURvaRWdQ%3D.
188. Britannica. Did Marie-Antoinette really say “let them eat cake”? Date unknown. Available from: https://www.britannica.com/story/did-marie-antoinette-really-say-let-them-eat-cake.
189. Sugar: the facts; 2020. Available from: https://www.nhs.uk/live-well/eat-well/how-does-sugar-in-our-diet-affect-our-health/.
190. Scientific Advisory Committee on Nutrition (SACN). Lower carbohydrate diets for adults with T2DM; 2021. Available from: https://www.gov.uk/government/groups/scientific-advisory-committee-on-nutrition.
191. Atkins RC. Dr Atkins Diet Revolution.
192. Credit Suisse Research Institute. Sugar consumption at a crossroads; 2013. Available from: http://archive.wphna.org/wp-content/uploads/2014/01/13-09_Credit_Suisse_Sugar_crossroads.pdf.
193. Westman EC. Is dietary carbohydrate essential for human nutrition? Am J Clin Nutr. 2002;75(5):951–953. doi:10.1093/ajcn/75.5.951a
194. Malhotra A. The dietary advice on added sugar needs emergency surgery. BMJ. 2013;346:f3199. doi:10.1136/bmj.f3199
195. Lustig RH. Sickeningly sweet: does sugar cause T2DM? Yes. Can J Diab. 2016;40(4):282–286. doi:10.1016/j.jcjd.2016.01.004
196. Lustig RH, Mulligan K, Noworolski SM, et al. Isocaloric fructose restriction and metabolic improvement in children with obesity and metabolic syndrome. Obesity. 2016;24(2):453–460. doi:10.1002/oby.21371
197. Yang Q, Zhang Z, Gregg EW, Flanders WD, Merritt R, Hu FB. Added sugar intake and cardiovascular diseases mortality among US adults. JAMA Intern Med. 2014;174(4):516–524. doi:10.1001/jamainternmed.2013.13563
198. Taubes G. What if sugar is worse than just empty calories? BMJ. 2018;360:j5808. doi:10.1136/bmj.j5808
199. Russell W, Baka A, Björck I, et al. Impact of diet composition on blood glucose regulation. Crit Rev Food Sci Nutr. 2016;56(4):541–590. doi:10.1080/10408398.2013.792772
200. San-Cristobal R, Navas-Carretero S, Martínez-González M, et al. Contribution of macronutrients to obesity: implications for precision nutrition. Nat Rev Endocrinol. 2020;16:305–320. doi:10.1038/s41574-020-0346-8
201. Ludwig DS, Hu FB, Tappy L, Brand-Miller J. Dietary carbohydrates: role of quality and quantity in chronic disease. BMJ. 2018;361:k2340. doi:10.1136/bmj.k2340
202. Leonetti F, Campanile FC, Coccia F, et al. Very low-carbohydrate ketogenic diet before bariatric surgery: prospective evaluation of a sequential diet. Obes Surg. 2015;25:64–71. doi:10.1007/s11695-014-1348-1
203. Stern L, Iqbal N, Seshadri P, et al. The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: one-year follow-up of a randomized trial. Ann Intern Med. 2004;140:778–785. doi:10.7326/0003-4819-140-10-200405180-00007
204. Miyashita Y, Koide N, Ohtsuka M, et al. Beneficial effect of low carbohydrate in low calorie diets on visceral fat reduction in type 2 diabetic patients with obesity. Diabetes Res Clin Pract. 2004;65:235–241. doi:10.1016/j.diabres.2004.01.008
205. Jönsson T, Granfeldt Y, Ahren B, et al. Beneficial effects of a Paleolithic diet on cardiovascular risk factors in T2DM: a randomized cross-over pilot study. Cardiovasc Diabetol. 2009;8:3. doi:10.1186/1475-2840-8-35
206. Davis NJ, Tomuta N, Schechter C, et al. Comparative study of the effects of a 1-year dietary intervention of a low- carbohydrate diet versus a low-fat diet on weight and glycemic control in T2DM. Diabetes Care. 2009;32:1147–1152. doi:10.2337/dc08-2108
207. Daly ME, Paisey R, Paisey R, et al. Short-term effects of severe dietary carbohydrate-restriction advice in T2DM: a randomized controlled trial. Diabet Med. 2006;23:15–20. doi:10.1111/j.1464-5491.2005.01760.x
208. Dyson PA, Beatty S, Matthews DR. A low-carbohydrate diet is more effective in reducing body weight than healthy eating in both diabetic and non-diabetic subjects. Diabet Med. 2007;24:1430–1435. doi:10.1111/j.1464-5491.2007.02290.x
209. Wolever TM, Gibbs AL, Mehling C, et al. The Canadian trial of carbohydrates in diabetes (CCD), a 1-yr controlled of low-glycemic index dietary carbohydrate in T2DM: no effect on glycated hemoglobin but reduction in C-reactive protein. Am J Clin Nutr. 2008;87:114–125. doi:10.1093/ajcn/87.1.114
210. Iqbal N, Vetter ML, Moore RH, et al. Effects of a low-intensity intervention that prescribed a low-carbohydrate vs. a low-fat diet in obese, diabetic participants. Obesity. 2010;18:1733–1738. doi:10.1038/oby.2009.460
211. Goday A, Bellido D, Sajoux I, et al. Short-term safety, tolerability and efficacy of a very low-calorie ketogenic diet interventional weight loss program versus hypocaloric diet in patients with T2DM mellitus. Nutr Diabetes. 2016;6:e230. doi:10.1038/nutd.2016.36
212. Saslow LR, Mason AE, Kim S, et al. An online intervention comparing a very low-carbohydrate ketogenic diet and lifestyle recommendations versus a plate method diet in overweight individuals with T2DM: a randomized controlled trial. J Med Int Res. 2017;19:e36.
213. Yamada Y, Uchida J, Izumi H, et al. A non-calorie-restricted low-carbohydrate diet is effective as an alternative therapy for patients with T2DM. Int Med. 2014;53:13–19. doi:10.2169/internalmedicine.53.0861
214. Guldbrand H, Dizdar B, Bunjaku B, et al. In T2DM, randomisation to advice to follow a low-carbohydrate diet transiently improves glycemic control compared with advice to follow a low-fat diet producing a similar weight loss. Diabetologi. 2012;55:2118–2127. doi:10.1007/s00125-012-2567-4
215. Westman EC, Yancy WS, Mavropoulos JC, Marquart M, McDuffie JR. The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in T2DM mellitus. Nutr Metab. 2008;19:36. doi:10.1186/1743-7075-5-36
216. Haimoto H, Iwata M, Wakai K, Umegaki H. Long-term effects of a diet loosely restricting carbohydrates on HbA1c levels, BMI and tapering of sulfonylureas in T2DM: a 2-year follow-up study. Diabetes Res Clin Pract. 2008;79:350–356. doi:10.1016/j.diabres.2007.09.009
217. Tay J, Thompson CH, Luscombe-Marsh ND, et al. Effects of an energy-restricted low-carbohydrate, high unsaturated fat/low saturated fat diet versus a high-carbohydrate, low-fat diet in T2DM: a 2-year randomized clinical trial. Diabetes Obes Metab. 2018;20:858–871. doi:10.1111/dom.13164
218. Wang LL, Wang Q, Hong Y, et al. The effect of low-carbohydrate diet on glycemic control in patients with T2DM mellitus. Nutrients. 2018;10:661. doi:10.3390/nu10060661
219. Larsen RN, Mann NJ, Maclean E, Shaw JE. The effect of high-protein, low-carbohydrate diets in the treatment of T2DM: a 12 month randomised controlled trial. Diabetologia. 2011;54:731–740. doi:10.1007/s00125-010-2027-y
220. Sato J, Kanazawa A, Makita S, et al. A randomized controlled trial of 130g/day low-carbohydrate diet in T2DM with poor glycemic control. Clin Nutr. 2017;36:992–1000. doi:10.1016/j.clnu.2016.07.003
221. Sanada M, Kabe C, Hata H, et al. Efficacy of a moderately low carbohydrate diet in a 36-month observational study of Japanese patients with T2DM. Nutrients. 2018;10:528. doi:10.3390/nu10050528
222. Boden G, Sargrad K, Homko C, Mozzoli M, Stein TP. Effect of a low carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with T2DM. Ann Intern Med. 2005;142:403–411. doi:10.7326/0003-4819-142-6-200503150-00006
223. Gannon MC, Nuttall FQ. Effect of a high-protein, low-carbohydrate diet on blood glucose control in people with T2DM. Diabetes. 2004;53:2375–2382. doi:10.2337/diabetes.53.9.2375
224. Hallberg SJ, McKenzie AL, Williams PT, et al. Effectiveness and safety of a novel care model for the management of T2DM at 1 year: an open-label, non-randomized, controlled study. Diabetes Ther. 2018;9:583–612. doi:10.1007/s13300-018-0373-9
225. Krebs JD, Bell D, Hall R, et al. Improvements in glucose metabolism and insulin sensitivity with a low-carbohydrate diet in obese patients with T2DM. J Am Coll Nutr. 2013;32:11–17. doi:10.1080/07315724.2013.767630
226. Hussain TA, Matthew TC, Dashti AA, Asfar S, Al-Zaid N, Dashti HM. Effect of low-calorie versus low-carbohydrate ketogenic diet in T2DM. Nutrition. 2012;28:1016–1021. doi:10.1016/j.nut.2012.01.016
227. Sasakabe T, Haimoto H, Umegaki H, Wakai K. Effects of a moderate low-carbohydrate diet on preferential abdominal fat loss and cardiovascular risk factors in patients with T2DM. Diabetes Metab Syndr Obes. 2011;4:167–174. doi:10.2147/DMSO.S19635
228. Nielsen JV, Joensson EA. Low carbohydrate diet in T2DM: stable improvement of bodyweight and glycemic control during 44 months follow-up. Nutr Metab. 2008;5:14. doi:10.1186/1743-7075-5-14
229. Dashti HM, Mathew TC, Khadada M, et al. Beneficial effects of ketogenic diet in obese diabetic subjects. Mol Cell Biochem. 2007;302:249–256. doi:10.1007/s11010-007-9448-z
230. Yancy WS, Foy M, Chalecki AM, Vernon AC, Westman EC. A low carbohydrate, ketogenic diet to treat T2DM. Nutr Metab. 2005;2:34. doi:10.1186/1743-7075-2-34
231. Dashti HM, Mathew TC, Hussein T, et al. Long-term effects of a ketogenic diet in obese patients. Exp Clin Cardiol. 2004;9:200–205.
232. Shai I, Schwarzfuchs D, Henkin Y, et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N Engl J Med. 2008;359:229–241.
233. Elhayany A, Lustman A, Abel R, Attal-Singer J, Vinker S. A low carbohydrate Mediterranean diet improves cardiovascular risk factors and diabetes control among overweight patients with T2DM mellitus: a 1-year prospective randomized intervention study. Diabetes Obes Metab. 2010;12:204–209. doi:10.1111/j.1463-1326.2009.01151.x
234. Athinarayanan SJ, Adams RN, Hallberg SJ, et al. Long-term effects of a novel continuous remote care intervention including nutritional ketosis for the management of T2DM: a 2-year non-randomized clinical trial. Front Endocrinol. 2019;10:348. doi:10.3389/fendo.2019.00348
235. Snorgaard O, Poulsen GM, Andersen HK, Astrup A. Systematic review and meta-analysis of dietary carbohydrate restriction in patients with T2DM. BMJ Open Diabetes Res Care. 2017;5(1):e000354. doi:10.1136/bmjdrc-2016-000354
236. Kaska L, Sledzinski T, Chomiczewska A, Dettlaff-Pokora A, Swierczynski J. Improved glucose metabolism following bariatric surgery is associated with increased circulating bile acid concentrations and remodeling of the gut microbiome. World J Gastroenterol. 2016;22:8698–8719. doi:10.3748/wjg.v22.i39.8698
237. Penney NC, Kinross J, Newton RC, Purkayastha S. The role of bile acids in reducing the metabolic complications of obesity after bariatric surgery: a systematic review. Int J Obes. 2015;39:1565–1574. doi:10.1038/ijo.2015.115
238. Ajala O, English P, Pinkney J. Systematic review and meta-analysis of different dietary approaches to the management of T2DM. Am J Clin Nutr. 2013;97:505–516. doi:10.3945/ajcn.112.042457
239. Brehm BJ, Seeley RJ, Daniels SR, D’Alessio DA. A randomized trial comparing a very low carbohydrate diet and a calorie-restricted low fat diet on body weight and cardiovascular risk factors in healthy women. J Clin Endocrinol Metab. 2003;88:1617–1623. doi:10.1210/jc.2002-021480
240. Nordmann AJ, Nordmann A, Briel M, et al. Effects of a low-carbohydrate vs. low-fat diets on weight loss and cardiovascular risk factors. Arch Intern Med. 2006;166:285–293. doi:10.1001/archinte.166.3.285
241. Bueno NB, de Melo IS, de Oliveira SL, da Rocha Ataide T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. Br J Nutr. 2013;110:1178–1187. doi:10.1017/S0007114513000548
242. Mancini JG, Filion KB, Atallah R, Eisenberg MJ. Systematic review of the Mediterranean diet for long term weight loss. Am J Med. 2016;129:407–415.e4. doi:10.1016/j.amjmed.2015.11.028
243. Mansoor N, Vinknes KJ, Veierød MB, Retterstøl K. Effects of low-carbohydrate diets v. low-fat diets on body weight and cardiovascular risk factors: a meta-analysis of randomised controlled trials. Br J Nutr. 2016;115:466–479. doi:10.1017/S0007114515004699
244. Sackner-Bernstein J, Kanter D, Kaul S. Dietary intervention for overweight and obese adults: comparison of low-carbohydrate and low-fat diets. a meta-analysis. PLoS One. 2015;10:e0139817. doi:10.1371/journal.pone.0139817
245. Tobias DK, Chen M, Manson JE, Ludwig DS, Willett W, Hu FB. Effect of low-fat diet interventions versus other diet interventions on long-term weight change in adults: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2015;3:968–979. doi:10.1016/S2213-8587(15)00367-8
246. Naude CE, Schoonees A, Senekal M, et al. Low carbohydrate versus isoenergetic balanced diets for reducing weight and cardiovascular risk: a systematic review and meta-analysis. PLoS One. 2014;9:e100652. doi:10.1371/journal.pone.0100652
247. Johnston BC, Kanters S, Bandayrel K, et al. Comparison of weight loss among named diet programs in overweight and obese adults: a meta-analysis. JAMA. 2014;312:923–933. doi:10.1001/jama.2014.10397
248. Hu T, Mills KT, Yao L, et al. Effects of low-carbohydrate diets versus low-fat diets on metabolic risk factors: a meta-analysis of randomized controlled clinical trials. Am J Epidemiol. 2012;176(Suppl 7):S44–54. doi:10.1093/aje/kws264
249. Hession M, Rolland C, Kulkarni U, et al. Systematic review of randomized controlled trials of low-carbohydrate vs. low-fat/low-calorie diets in the management of obesity and its comorbidities. Obes Rev. 2009;10:36–50. doi:10.1111/j.1467-789X.2008.00518.x
250. Santos FL, Esteves SS, Da Costa PA, et al. Systematic review and meta-analysis of clinical trials of the effects of low carbohydrate diets on cardiovascular risk factors. Obes Rev. 2012;13:1048–1066. doi:10.1111/j.1467-789X.2012.01021.x
251. Unwin D, Unwin J. Low carbohydrate diet to achieve weight loss and improve HbA1c in T2DM and pre-diabetes: experience from one general practice. Practical Diabetes. 2014;31(2):76–79. doi:10.1002/pdi.1835
252. Ebbeling CB, Feldman HA, Klein GL, et al. Effects of a low carbohydrate diet on energy expenditure during weight loss maintenance: randomized trial. BMJ. 2018;363:k4583. doi:10.1136/bmj.k4583
253. Davies MJ, D’Alessio DA, Fradkin J. Management of hyperglycemia in T2DM, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41:2669–2701. doi:10.2337/dci18-0033
254. American Diabetes Association. Summary of revisions: standards of medical care in diabetes-2019. Diabetes Care. 2019;42:S4–S6. doi:10.2337/dc19-Srev01
255. World Health Organisation. WHO calls on countries to reduce sugars intake among adults and children; 2015. Available from: https://www.who.int/news/item/04-03-2015-who-calls-on-countries-to-reduce-sugars-intake-among-adults-and-children.
256. Pym H. Sugar tax is already producing results; 2018. Available from: https://www.bbc.com/news/health-43372295.
257. Kliff S. Ending junk food: the harder addiction to quit; 2011 Available from: https://www.washingtonpost.com/blogs/ezra-klein/post/ending-junk-food-The-harder-addiction-to-quit/2011/09/27/gIQAlbAh2K_blog.html?utm_term=.b5442739d737.
258. Mosley M. Eat to beat diabetes and week by week watch the weight fall off! Dr Michael Mosley explains the changes you will experience if you follow his 800-calorie diet. 2016. Available from: http://www.dailymail.co.uk/health/article-3407500/Eat-beat-diabetes-week-week-watch-weight-fall-Dr-Michael-Mosley-explains-changes-experience-follow-800-calorie-diet.html.
259. National Obesity Forum. Eat fat, cut the carbs and avoid snacking to reverse obesity and T2DM; 2016. Available from: https://phcuk.org/wp-content/uploads/2016/05/Eat-Fat-Cut-The-Carbs-and-Avoid-Snacking-To-Reverse-Obesity-and-Type-2-Diabetes-National-Obesity-Forum-Public-Health-Collaboration.pdf.
260. BBC. National obesity forum campaigners quit over low-fat report; 2016. Available from: https://www.bbc.com/news/uk-36447808.
261. Alberti KG, Zimmet P, Shaw J. International Diabetes Federation: a consensus on T2DM prevention. Diabet Med. 2007;24:451e63. doi:10.1111/j.1464-5491.2007.02157.x
262. Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycaemia in T2DM mellitus: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia. 2009;52:17e30. doi:10.1007/s00125-008-1157-y
263. Korkiakangas EE, Alahuhta MA, Laitinen JH. Barriers to regular exercise among adults at high risk or diagnosed with T2DM: a systematic review. Health Promot Int. 2009;24:416e27. doi:10.1093/heapro/dap031
264. Ball K, Crawford D, Owen N. Too fat to exercise? Obesity as a barrier to physical activity. Aust N Z J Public Health. 2000;24:331e3. doi:10.1111/j.1467-842X.2000.tb01579.x
265. Hootman JM, Macera CA, Ham SA, et al. Physical activity levels among the general US adult population and in adults with and without arthritis. Arthritis Rheum. 2003;49:129e35. doi:10.1002/art.10911
266. Sallis JF, Hovell MF. Determinants of exercise behavior. Exerc Sport Sci Rev. 1990;18:307e30. doi:10.1249/00003677-199001000-00014
267. Varo JJ, Martinez-Gonzalez MA, De Irala-Estevez J, et al. Distribution and determinants of sedentary lifestyles in the European Union. Int J Epidemiol. 2003;32:138e46. doi:10.1093/ije/dyg116
268. Taylor R, Barnes AC. Can type 2 diabetes be reversed and how can this best be achieved? James Lind Alliance research priority number one. Diabet Med. 2019;36:308–315. doi:10.1111/dme.13851
269. Franz MJ, MacLeod J, Evert A, Brown C, Gradwell E. Academy of nutrition and dietetics nutrition practice guideline for type 1 and type 2 diabetes in adults: systematic review of evidence for medical nutrition therapy effectiveness and recommendations for integration into the nutrition care process. J Acad Nutr Diet. 2017;117:1659–1679. doi:10.1016/j.jand.2017.03.022
270. Bittel AJ, Bittel DC, Mittendorfer B, et al. A single bout of premeal resistance exercise improves postprandial glucose metabolism in obese men with prediabetes. Med Sci Sports Exerc. 2021;53(4):694–703. doi:10.1249/MSS.0000000000002538
271. Eichner NZM, Gaitán JM, Gilbertson NM, Khurshid M, Weltman A, Malin SK. Postprandial augmentation index is reduced in adults with prediabetes following continuous and interval exercise training. Exp Physiol. 2019;104(2):264–271. doi:10.1113/EP087305
272. Banerjee P, Caulfield B, Crowe L, et al. Prolonged electrical muscle stimulation exercise improves strength, peak VO2, and exercise capacity in patients with stable chronic heart failure. J Card Fail. 2009;15:319e26. doi:10.1016/j.cardfail.2008.11.005
273. Crowe L, Caulfield B. Pushing out the limits of electrical stimulation. A case study in the aggressive use of an alternative to voluntary exercise. BMJ Case Rep. 2011;bcr0620114343. doi:10.1136/bcr.06.2011.4343
274. Crognale D, Crowe L, Devito G, et al. Neuro-muscular electrical stimulation training enhances maximal aerobic capacity in healthy physically active adults. Conf Proc IEEE Eng Med Biol Soc. 2009;2009:2137e40.
275. Banerjee P, Caulfield B, Crowe L, et al. Prolonged electrical muscle stimulation exercise improves strength and aerobic capacity in healthy sedentary adults. J Appl Physiol. 2005;99:2307e11. doi:10.1152/japplphysiol.00891.2004
276. Caulfield B, Crowe L, Minogue C, et al. The use of electrical muscle stimulation to elicit a cardiovascular exercise response without joint loading: a case study. J Exerc Physiol. 2004;7:84e8.
277. Crognale D, Vito GD, Grosset JF, Crowe L, Minogue C, Caulfield B. Neuromuscular electrical stimulation can elicit aerobic exercise response without undue discomfort in healthy physically active adults. J Strength Cond Res. 2013;27(1):208–215. doi:10.1519/JSC.0b013e318252f5e5
278. Grosset JF, Crowe L, de Vito G, O’Shea D, Caulfield B. Comparative effect of a 1 h session of electrical muscle stimulation and walking activity on energy expenditure and substrate oxidation in obese subjects. Appl Physiol Nutr Metab. 2013;38(1):57–65. doi:10.1139/apnm-2011-0367
279. Jabbour G, Belliveau L, Probizanski D, et al. Effect of low frequency neuromuscular electrical stimulation on glucose profile of persons with T2DM: a pilot study. Diabetes Metab J. 2015;39(3):264–267. doi:10.4093/dmj.2015.39.3.264
280. Crowe L, Caulfield B. Aerobic neuromuscular electrical stimulation–an emerging technology to improve haemoglobin A1c in T2DM mellitus: results of a pilot study. BMJ Open. 2012;2(3):e000219. doi:10.1136/bmjopen-2011-000219
281. Thomas DE, Elliott EJ, Naughton GA. Exercise for T2DM mellitus. Cochrane Database Syst Rev. 2006;(3):CD002968. doi:10.1002/14651858.CD002968.pub2
282. Sanz C, Gautier JF, Hanaire H. Physical exercise for the prevention and treatment of T2DM. Diabetes Metab. 2010;36(5):346–351. doi:10.1016/j.diabet.2010.06.001
283. Kimura T, Matsumoto K, Kameda N, et al. Percutaneous electrical muscle stimulation attenuates postprandial hyperglycemia in obese and pre-obese Japanese men. Int J Sports Health Sci. 2010;8:1e6.
284. Gregory CM, Bickel CS. Recruitment patterns in human skeletal muscle during electrical stimulation. Phys Ther. 2005;85:358e64. doi:10.1093/ptj/85.4.358
285. Gondin J, Brocca L, Bellinzona E, et al. Neuromuscular electrical stimulation training induces atypical adaptations of the human skeletal muscle phenotype: a functional and proteomic analysis. J Appl Physiol. 2011;110:433e50. doi:10.1152/japplphysiol.00914.2010
286. Crowe L, Caulfield B. Towards creating a super-stimulus to normalise glucose metabolism in the pre-diabetic; a case study in the feast-famine and activity-rest cycle. BMJ Case Rep. 2012;2012:bcr0320113939. doi:10.1136/bcr.03.2011.3939
287. Hamada T, Hayashi T, Kimura T, et al. Electrical stimulation of human lower extremities enhances energy consumption, carbohydrate oxidation, and whole body glucose uptake. J Appl Physiol. 2004;96:911e16. doi:10.1152/japplphysiol.00664.2003
288. Sola-Penna M. Metabolic regulation by lactate. Life. 2008;60:605e8.
289. Why slendertone [webpage on the internet]; 2021. Available from: https://us.slendertone.com/pages/why-slendertone.
290. Ha J, Satin LS, Sherman AS. A mathematical model of the pathogenesis, prevention, and reversal of type 2 diabetes. Endocrinology. 2016;157(2):624–635. doi:10.1210/en.2015-1564
291. Topp B, Promislow K, deVries G, Miura RM, Finegood DT. A model of β-cell mass, insulin, and glucose kinetics: pathways to diabetes. J Theor Biol. 2000;206(4):605–619. doi:10.1006/jtbi.2000.2150
292. Lean M. BMJ talk medicine. Diabetes remission- treating blood glucose, when the disease process is to do with body fat; 2017. Available from: https://soundcloud.com/bmjpodcasts/diabetes-remission-treating-blood-glucose-when-The-disease-process-is-to-do-with-body-fat?utm_source=clipboard&utm_campaign=wtshare&utm_medium=widget&utm_content=https%253A%252F%252Fsoundcloud.com%252Fbmjpodcasts%252Fdiabetes-remission-treating-blood-glucose-when-The-disease-process-is-to-do-with-body-fat.
293. Min T, Barry JD, Stephens JW. Predicting the resolution of T2DM after bariatric surgical procedures: a concise review. J Diabetes Metab. 2015;6:617.
294. Neuenschwander M, Ballon A, Weber KS, et al. Role of diet in T2DM incidence: umbrella review of meta-analyses of prospective observational studies. BMJ. 2019;366:l2368. doi:10.1136/bmj.l2368
295. Lean ME, Leslie WS, Barnes AC, et al. Primary care‐led weight management for remission of type 2 diabetes (DiRECT): an open‐label, cluster‐randomised trial. Lancet. 2018;391(10120):541–551. doi:10.1016/S0140-6736(17)33102-1
296. Taheri S, Zaghloul H, Chagoury O, et al. Effect of intensive lifestyle intervention on bodyweight and glycaemia in early type 2 diabetes (DIADEM-I): an open-label, parallel-group, randomised controlled trial. Lancet Diabetes Endocrinol. 2020;8(6):477–489. doi:10.1016/S2213-8587(20)30117-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.