")
Back to Journals » Clinical Epidemiology » Volume 9
Return to work for patients with diffuse large B-cell lymphoma and transformed indolent lymphoma undergoing autologous stem cell transplantation
Authors Arboe B , Olsen MH , Goerloev JS, Duun-Henriksen AK, Johansen C , Dalton SO , Brown PDN
Received 14 February 2017
Accepted for publication 5 April 2017
Published 6 June 2017 Volume 2017:9 Pages 321—329
DOI https://doi.org/10.2147/CLEP.S134603
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Irene Petersen
Bente Arboe,1,2 Maja Halgren Olsen,2 Jette Soenderskov Goerloev,1 Anne Katrine Duun-Henriksen,2 Christoffer Johansen,2,3 Susanne Oksbjerg Dalton,2 Peter de Nully Brown1
1Department of Hematology, Copenhagen University Hospital, Rigshospitalet, 2Unit of Survivorship Research, The Danish Cancer Society Research Center, 3Department of Oncology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
Background: Autologous stem cell transplantation (ASCT) is the standard treatment for patients with relapsed diffuse large B-cell lymphoma (DLBCL) or transformed indolent lymphoma (TIL). The treatment is mainly considered for younger patients still available for the work market. In this study, social outcomes after ASCT in terms of return to work (RTW) are described.
Patients and methods: Information from national administrative registers was combined with clinical information on patients, who received ASCT for relapse of DLBCL or TIL between 2000 and 2012. A total of 164 patients were followed until RTW, disability or old-age pension, death, or December 31, 2015, whichever came first. A total of 205 patients were followed with disability pension as the event of interest. Cox models were used to determine cause-specific hazards.
Results: During follow-up, 82 (50%) patients returned to work. The rate of returning to work in the first year following ASCT was decreased for patients being on sick leave at the time of relapse (hazard ratio [HR] 0.3 [0.2;0.5]) and increased for patients aged ≥55 years (HR 1.9 [1.1;3.3]). In all, 56 (27%) patients were granted disability pension. Being on sick leave at the time of relapse was positively associated with receiving a disability pension in the first 2 years after ASCT (HR 3.7 [1.8;7.7]).
Conclusion: Patients on sick leave at the time of relapse have a poorer prognosis regarding RTW and have a higher rate of disability pension. Furthermore, patients >55 are more likely to RTW compared to younger patients. These results indicate an unmet need for focused social rehabilitation.
Keywords: social outcomes, chemotherapy, relapse treatment, disability pension, epidemiology
Introduction
All cancer patients are at risk of developing health impairments that result in a decrease in their ability to work.1,2 This may lead to a loss of identity and affect self-esteem, and it may also, even in tax-funded, free-of-charge health systems, give rise to financial concerns.3,4 Social involvement and income levels improve the quality of life of cancer survivors,5–7 and studies have shown that patients often regard returning to work as indicative of complete recovery and regained normality.8,9 Previous studies have found that cancer patients have impaired work market affiliation10,11 and a higher risk of taking a disability pension in the years after diagnosis.12
Denmark has a wide-ranging tax-financed welfare system and a high level of social security covering all citizens. If a person is not able to work due to sickness, the state is obligated to support the individual financially through welfare benefits, such as sick leave benefits. If a person is not able to work due to permanent disability, the person can receive a disability pension, and hence be financially compensated, although not equivalent to a full salary. Since the ability to work is positively associated with quality of life, there might be a negative impact of taking a disability pension on the person’s social function and self-esteem.12 How receiving a disability pension affects quality of life has been evaluated in a study among 1143 persons followed for 1 year after the start of the disability pension. It was found that quality of life increased during the first year, but persons who were re-employed had an even higher quality of life than those who stayed retired.13 However, in Denmark, it is a rare event to become re-employed on a disability pension.
High-dose chemotherapy with autologous stem cell transplantation (ASCT) is the standard therapy for patients with primary refractory or relapsed diffuse large B-cell lymphoma (DLBCL), as well as for patients with transformed indolent lymphoma (TIL).14 This potentially curative treatment is toxic with many side effects and is mostly considered for younger patients without major comorbidities.15 This young patient group is still eligible for the work market. Quality of life after ASCT has been shown to be associated with employment status and to be decreased compared to the general population.16–18
The aim of this study was to describe the rate of return to work (RTW) and of taking a disability pension in patients receiving ASCT as relapse treatment, and to evaluate the influence of comorbidity, socioeconomic, and clinical factors on these social outcomes. If patients at risk of not returning to work could be identified, early targeted interventions could be initiated for those at the highest risk of developing work-related problems.
Patients and methods
Patients
A population-based nationwide cohort study using the clinical Danish National Lymphoma Registry (LYFO) was conducted to identify patients with relapsed B-cell lymphoma in Denmark in the period 2000–2012, who underwent ASCT. The LYFO includes data on all lymphoma patients who have been treated at hematological departments in Denmark since 2000.19,20 Furthermore, medical records were reviewed for clinical, pathological, and treatment information. Patients with DLBCL and TIL aged ≥18 at the time of diagnosis were included. Patients undergoing ASCT as part of first-line treatment, patients with primary or secondary central nervous system lymphomas, and patients with Richter transformation were excluded.
All Danish residents are assigned a unique Central Person Registry (CPR) number at birth or at the time of commencing residence in Denmark. Linkage to The Civil Registration System tracks changes in the vital status and residential area daily, and the CPR number allows linkage between national administrative registries and clinical databases in Denmark.21,22
Covariates
Information on clinical factors was obtained from the individual medical records. Disease-specific variables such as lymphoma subtype, primary refractory disease, and international prognostic index (IPI) were analyzed in order to consider disease burden. To evaluate the treatment toxicity, information on days of admission during salvage therapy and performance status on the day of admission for high-dose therapy were obtained. In addition, the patient-specific variables such as sex and age were also analyzed, with an age cut-off of 55 years.
Comorbidity
Information on comorbidity was obtained from the Danish National Patient Registry (DNPR), which includes information on all hospitalizations since 1978 and, from 1995, also on outpatient visits.23 To estimate the burden of comorbidity, all somatic diagnoses other than lymphoma were retrieved from the DNPR. Comorbidity was measured as the number of comorbidities, using the 19 disorders specified in the Charlson comorbidity index, grouped into no comorbidities, one, and two or more. In the RTW analysis, comorbidity was grouped into no comorbidities and one or more due to small numbers.
Socioeconomic factors
Information on socioeconomic factors was obtained via data linkage to various population-based administrative registers operated by Statistics Denmark that contain annually updated data on a broad range of socioeconomic factors.24,25 Information on the highest attained educational level by October 1 the year before relapse was obtained, and this was categorized as short (mandatory school, 7 or 9 years depending on the year of birth), medium (youth or vocational education, 10–12 years of education), and higher education (>12 years of education). Disposable income the year before relapse was grouped into quintiles based on the population of the same sex and birth cohort, calculated per person after taxation and interest. Disposable income was categorized as low (first quintile), medium (second to third quintile), and high (fourth to fifth quintile). Information on cohabitation status was obtained by January 1 of the year of relapse and was defined as living alone or with an adult partner.
Work market affiliation
Information on welfare benefits and work market affiliation was obtained from the Danish Register for Evaluation of Marginalization (DREAM). DREAM includes data on all Danish residents who have received any social transfer payments or welfare benefits since 1991. Each person is registered weekly, with a code representing the type of social transfer payment received.26,27 Patients were included in the RTW analysis, if they were registered with sick leave at the time of stem cell reinfusion. RTW was defined as the first period of four consecutive weeks without receiving any welfare benefits.26,28 Patients were included in the disability pension analysis, if they were not registered with a disability or old-age pension at the time of relapse. Information on disability pension was available from DREAM. Permanent withdrawal from the work market was defined as taking a disability pension (including wage-diminished employment, so-called flex jobs) and old-age pension or age >65 years.
Statistical analysis
Patient baseline characteristics were analyzed descriptively and compared by chi-square test. Patients were followed from the day of stem cell reinfusion until an event of interest (disability pension or RTW), death, old-age pension or age 65 years, or 31 December 2015, whichever came first. Cumulative incidences were estimated for each event type. Cox proportional hazard models were used to determine cause-specific hazards for RTW within the first year after ASCT and disability pension within the first 2 years accounting for competing risks (death, old-age pension, or age 65 years); all of the variables listed in Tables 1 and 2 were tested one at a time. The proportional hazards assumption was tested and fulfilled for all models in the disability pension analysis. For the RTW analysis on sex and performance status, hazards were not proportional, but graphical control showed no crossing of curves. Due to multiple testing on a small patient cohort, the p-values were adjusted by the Bonferroni method. Factors that remained significant were included in a fully adjusted model, taking into account age, sex, and period. All analyses were conducted using R 3.2.2, using packages “Surv” and “cmprsk.”29,30
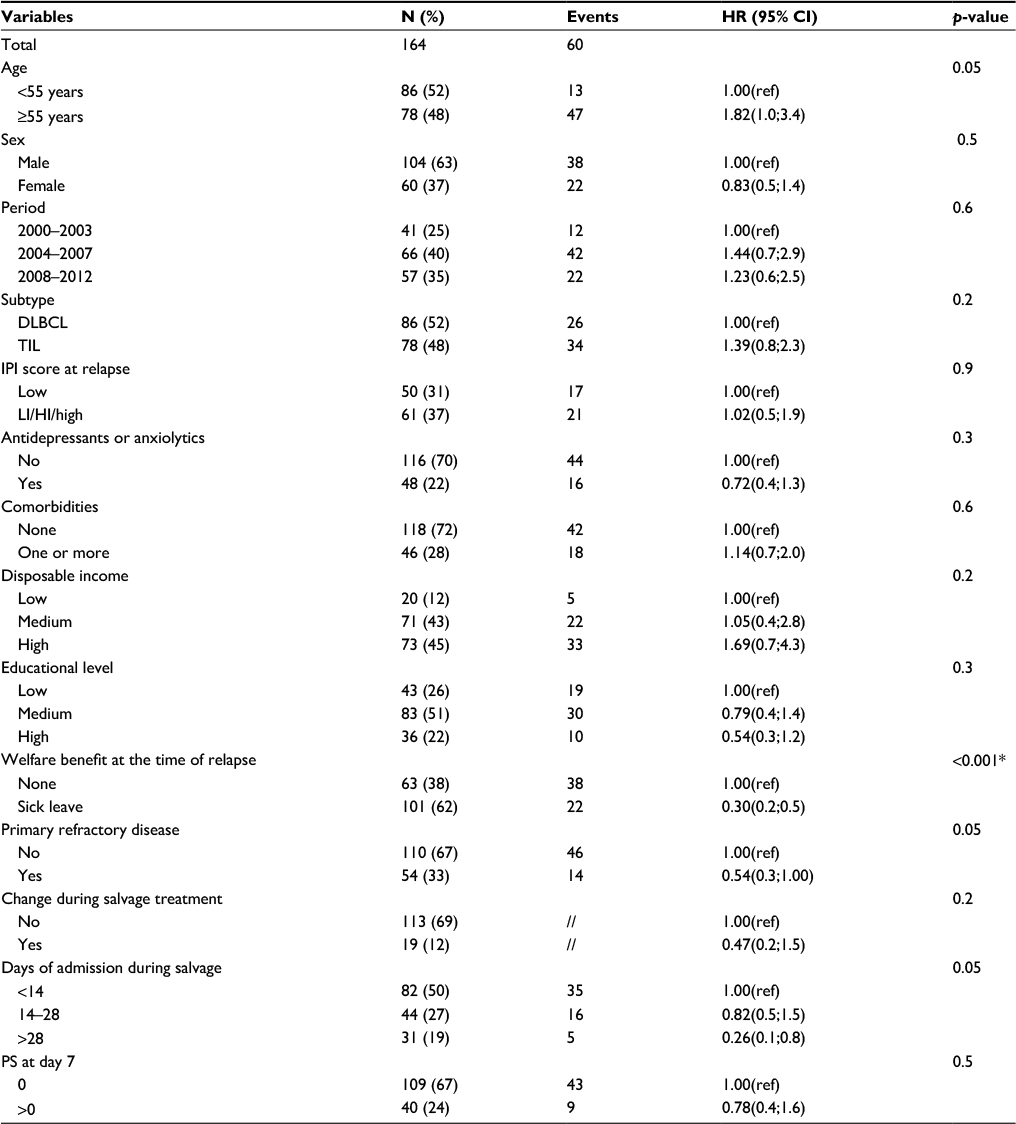 | Table 1 Baseline characteristics and HRs (with accompanying 95% CIs) for returning to work within the first year after ASCT for the 164 patients with diffuse large B-cell lymphoma or transformed indolent lymphoma in Denmark in 2000–2012 included in the analysis on return to work Notes: *p-values significant after Bonferroni adjustment; //, ≤5 events; Numbers may not add up to 164 due to missing data. Abbreviations: ASCT, autologous stem cell transplantation; CI, confidence interval; DLBCL, diffuse large B-cell lymphoma; HI, high intermediate; HRs, hazard ratios; IPI score, international prognostic index score; LI, low-intermediate; PS, performance status; ref, reference; TIL, transformed indolent lymphoma. |
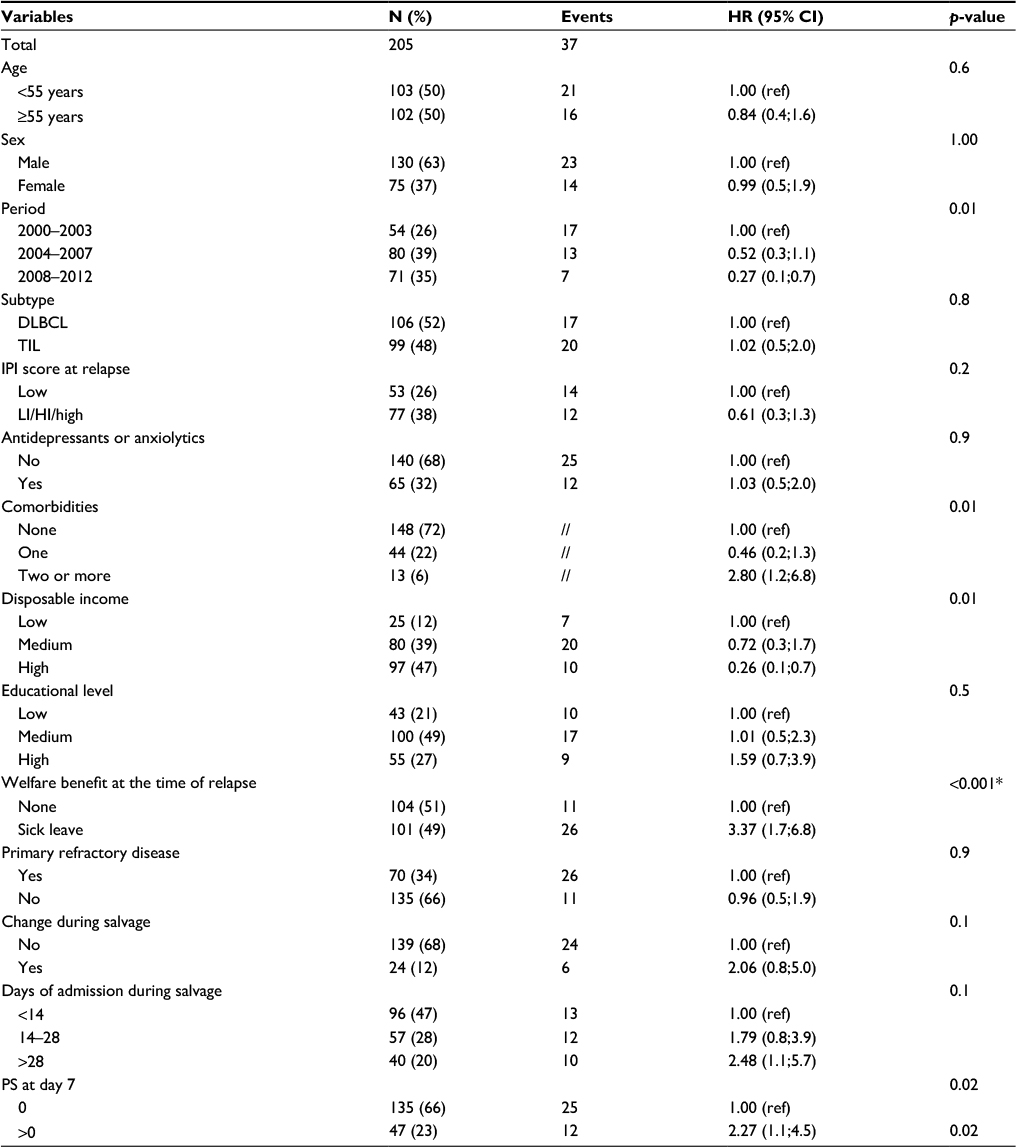 | Table 2 Baseline characteristics and HRs (with accompanying 95% 95% CIs) for taking disability pension within the first 2 years after ASCT for the 205 patients with diffuse large B-cell lymphoma or transformed indolent lymphoma in Denmark in 2000–2012 included in the analysis on disability pension^ Notes: *p-values significant after Bonferroni adjustment; //, ≤5 events; ^, numbers may not add up to 205 due to missing data. Abbreviations: ASCT, autologous stem cell transplantation; CI, confidence interval; DLBCL, diffuse large B-cell lymphoma; HI, high intermediate; HRs, hazard ratios; IPI score, international prognostic index score; LI, low-intermediate; PS, performance status; ref, reference; TIL, transformed indolent lymphoma. |
Ethics
The study was approved by the Danish Data Protection Agency (30-1251) and the Danish Patient Safety Authority (3-3013-574/1). The study is register based, and according to approval from the Danish Patient Safety Authority, informed consent from participants was not required.
Results
A total of 369 patients, who received ASCT for primary refractory or relapsed DLBCL or TIL in Denmark in the period 2000–2012, were identified. The median age was 58 years (range 22–73), and 60% were male. At the time of stem cell reinfusion, 164 patients were on sick leave, a total of 163 had permanently withdrawn from the work market (61 patients received some kind of disability pension and 102 patients obtained old-age pension), and 41 patients did not receive any welfare benefits (Figure 1).
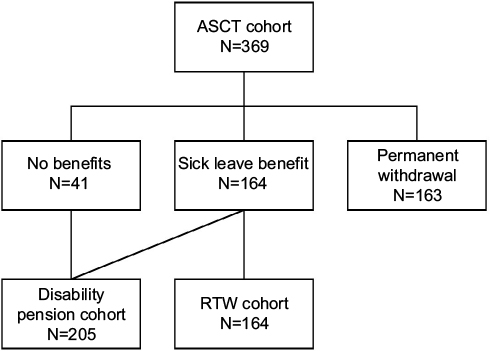 | Figure 1 Flowchart of the study population. Patients with diffuse large B-cell lymphoma or transformed indolent lymphoma in Denmark in 2000–2012 included in the analyses on return to work and disability pension. Abbreviations: ASCT, autologous stem cell transplantation; RTW, return to work. |
Return to work analysis
For the 164 patients included in the RTW analysis, the median age was 54 years (range 25–65) (Table 1), 78 (48%) had TIL, 86 (52%) had DLBCL, and 54 patients (33%) had primary refractory disease. At time of relapse, 50 patients (31%) had a low IPI score, 61 patients (37%) had an intermediate or high IPI score, and IPI score was missing for the remaining patients. During salvage therapy, 31 patients (19%) had prolonged admission >28 days, and 40 patients (24%) had a performance status above 0 at the time of ASCT (Table 1). A total of 153 patients received etoposide, cytarabine, and melphalan (BCNU) as conditioning regimens, and 11 received TBI.
Median time to RTW was 420 days, ranging from 13 to 914 days. Sixty (37%) patients returned to work within the first year after ASCT, 16 (10%) received disability pension, and 7 (4%) were retired. A total of 49 (30%) were still on sick leave after the first year, and 32 (20%) died within the first year without returning to work. After Bonferroni adjustment, only sick leave at the time of relapse maintained significance (p<0.001) (Table 1). In a fully adjusted model taking into account sex, period, and age, sick leave at the time of relapse was associated with a significantly poorer RTW prognosis with a hazard ratio (HR) of 0.31 (0.2;0.6). Age ≥55 years was associated with a better RTW prognosis with a HR of 1.90 (1.1;3.3), although this diminished over time (Figure 2). Of the 48 patients still on sick leave 1 year after ASCT, five (10%) had developed a subsequent relapse. Of the 86 patients under the age of 55, 59 patients were on sick leave at time of relapse, and 27 patients were not on sick leave. Of the patients on sick leave, 12 (20%) returned to work within the first year after ASCT, whereas 12 (44%) of the patients not on sick leave returned to work within the first year. For the 78 patients aged ≥55, 42 patients were on sick leave at time of relapse, and 10 (22%) returned to work within the first year after ASCT, and 26 (72%) of the 36 patients not on sick leave had returned to work.
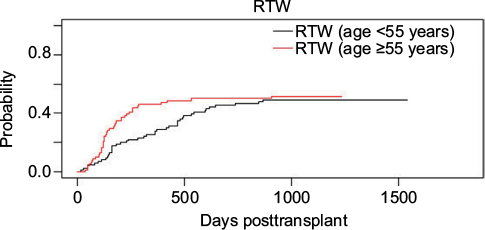 | Figure 2 Cumulative incidence curves for return to work within the first five years following ASCT for the 164 patients with diffuse large B-cell lymphoma or transformed indolent lymphoma in Denmark in 2000–2012 included in the return to work analysis, stratified on age. Abbreviation: RTW, return to work. |
Disability pension analysis
A total of 205 patients were eligible for the analysis on disability pension (Figure 1). The median age was 54 years (range 25–66), and time to receiving a disability pension ranged from 42 days to 2911 days. Among the 205 patients included, a total of 56 (27%) received a disability pension in the study period. Of the 205 patients included, 99 (48%) had TIL, 70 patients (34%) had primary refractory disease, 53 patients (26%) had a low IPI score at time of relapse, and 77 (38%) had an intermediate or high IPI score. A total of 40 patients (20%) had prolonged admission during salvage therapy (>28 days), and 40 (20%) had a performance status >0 at the time of ASCT (Table 2).
Within the first 2 years after ASCT, 37 (18%) patients were granted a disability pension, 16 (8%) were retired, 100 (49%) were still available for work, and 52 (25%) had died. After Bonferroni adjustment, the period and sick leave at the time of relapse were significantly associated with outcome (Table 2). In the fully adjusted model, age, sex, and period were taken into account. Sick leave at the time of relapse was associated with a worse disability pension prognosis (HR 3.72 [1.8;7.7]). Fewer were granted a disability pension in the later part of the study, the HR decreasing from 0.47 (0.2;1.0) in the period 2000–2003 to 0.24 (0.1;0.6) in 2004–2007 compared to 2008–2012. Of the 37 patients, who received a disability pension within the first 2 years after ASCT, 11 (30%) had developed a subsequent relapse. Of the 103 patients <55, 59 patients were on sick leave at time of relapse, and of them 15 (25%) received disability pension within the first 2 years after ASCT. Of the 44 patients not on sick leave at the time of relapse, 6 (14%) patients received disability pension. For the 102 patients aged ≥55, 42 patients were on sick leave at the time of relapse, of whom 11 (26%) received disability pension, and 5 (8%) of the 60 patients not on sick leave received disability pension.
Discussion
In this nationwide cohort study, it was found that being on sick leave at the time of relapse was associated with an impaired work market affiliation in the years after ASCT. This was true for both RTW and disability pension. Furthermore, age >55 years was positively associated with RTW.
The findings of this study are consistent with a Norwegian register study matching 2008 cancer survivors with a cancer-free control group. In the Norwegian study, they found that sick leave in the year before the cancer diagnosis predicted sick leave 5 years after.10 In a Danish population-based study among 3194 patients with hematological malignancies, Horsboel et al found that sick leave in the second year before diagnosis was positively associated with the risk of taking a disability pension.2
A study on RTW prognosis included 1741 patients with hematological malignancies <55 years. They found younger age to be associated with an improved RTW rate.28 A recent Norwegian cross-sectional study on 312 long-term lymphoma survivors treated with ASCT between 1987 and 2008 showed that older age was associated with a higher risk of having a not-employed status (odds ratio 1.04 [1.0;1.1]).18 In the Norwegian study, the not-employed status covered sick leave, disability pension, and old-age pension. Since they included old-age pension as not employed, it is not surprising that older age is associated with higher risk of being not employed. Here, it was found found that an age ≥55 years was associated with an improved RTW prognosis within the first year after undergoing ASCT. One reason might be that for patients ≥55 years, the risk of unemployment after a longer period of sick leave might be higher, motivating a faster RTW. Furthermore, older patients may have a more established work life and a higher influence on the work tasks when returning to work, thereby making it possible to work fewer hours or having flexible working hours. Both the Danish and the Norwegian studies included a more heterogeneous patient group, whereas, in the present study, only lymphoma patients receiving ASCT as relapse treatment were included. Therefore, the patient population in this study is older. Furthermore, the follow-up in this analysis is long, and, due to the historical cohort design, the authors were able to study cause-specific hazards for RTW, considering disability and old-age pension as competing events. The risk of having to take a disability pension is not only associated with the ability to work, but also with the demands of the specific job. People with high-strain jobs (defined as high demands and low decision latitude) have a higher risk of receiving a disability pension.31 The same associations might be seen regarding RTW, but the authors were not able to control for this.
An association between comorbidity and RTW or receiving a disability pension was not found. This is consistent with the results reported by Horsboel et al, where comorbidity was not found to be associated with RTW.28 In another study among 3194 patients with hematological malignancies, Horsboel et al found that comorbidity was positively associated with the risk of receiving a disability pension among both patients and the reference group.2 This is consistent with the results from a Danish study evaluating the risk of taking a disability pension among 44,905 cancer patients, where comorbidity was found to be positively associated with the risk of receiving a disability pension (relative risk [RR] 1.60 [1.55;1.65] and RR 1.55 [1.46;1.65] for women and men, respectively).12 The study population is small, and since patients with severe comorbidities are normally not considered for ASCT, only a few patients have comorbidities (n=57). The small sample size might explain why a significant association was not found.
In this study, both RTW and taking a disability pension were chosen as outcomes. Using data from DREAM, RTW can only be evaluated for patients on sick leave at the time of stem cell reinfusion, whereas disability pension can be evaluated for all patients not receiving a pension at the time of stem cell reinfusion. However, the age distribution in the entire cohort (N=369) shows that a large group of the patients were aged ≥60 years. For these patients, a disability pension may not be considered due to the long processing time. The authors chose to include all patients regardless of age due to the small sample size, and by accounting for competing events the authors have tried to minimize this bias. Furthermore, disability pension 2 years after ASCT was examined in order to account for the time it takes to be granted a disability pension. All possible efforts must have been made for a person to be able to RTW before a disability pension can be granted, and the time from application to final decision may be a lengthy process.
It has been investigated whether rehabilitation programs can improve RTW prognosis and quality of life, and results are not consistent. However, in a recent Cochrane review, there is moderate evidence that rehabilitation programs do improve RTW prognosis, whereas no difference was found regarding the quality of life.32 Future rehabilitation programs might benefit from a tailored approach,33 also considering social position.
Strengths and limitations
The strengths of this study include the nationwide patient inclusion; all relevant patients receiving ASCT in the study period are included. Due to the toxicity of ASCT and the risk of treatment-related mortality, patients undergo clinical evaluation before being offered the treatment. Therefore, the patient cohort is homogeneous. Furthermore, the exclusion of patients receiving ASCT as part of first-line treatment and patients with Richter transformation ensures that the included patients are comparable regarding disease status and future treatment. The use of population-based registries ensures complete follow-up. In addition, this study investigated the effect of a variety of variables regarding clinical status, disease status, treatment, comorbidity, and socioeconomic position; thereby, the risk of confounding was minimized. The fact that information on all variables was obtained from medical record review for each case combined with data from registries reduced the risk of recall and selection bias. Furthermore, the risk of misclassification of outcome is limited regarding disability pension, since it was assumed that DREAM has a 100% coverage.34 The LYFO database has a high coverage and all patients identified with the inclusion criteria from the LYFO were included. Although there might be a few patients not registered in the LYFO, the study group is believed to be representative and it is also believed that an eventual bias would be non-differential. Although patients from all centers performing ASCT in Denmark were included, the authors were not able to analyze data on center level due to Danish regulations; hence any potential differences in the RTW rate between the included centers in the study could not be ruled out.
One of the limitations is that only RTW as a parameter for not receiving sick leave benefits in four consecutive weeks was investigated. This definition may have caused misclassification of the outcome RTW, since patients as having returned to work could have been misclassified, if they were financially supported by a partner or parents. This is considered to be a rare scenario, but it might have caused an overestimation of RTW in the study. Moreover, some patients may have started a new job with less demanding tasks, and perhaps lower salary. Therefore, RTW cannot be used as a measure of having obtained the same capacity to work. Furthermore, the registries used are designed for administrative purposes, which limited the possibility for us to obtain more detailed information. There is no information on self-reported symptoms like quality of life or physical impairments, which have been shown to be associated with work market affiliation after ASCT.16,18 Future studies might combine register data with questionnaires in order to explore the association between these factors. Furthermore, it could be of interest to investigate the effect of special social rehabilitation programs addressed at patient groups at risk of not returning to work in order to improve the quality of life and social reintegration for patients receiving ASCT.
Acknowledgments
The abstract of this paper was presented at the American Society of Hematology Annual Meeting 2016 as a conference talk with interim findings. The presentation’s abstract was published in “The Abstract & Meeting Program Book” in Blood, Vol 128, Issue 22: 92–5969.
Disclosure
The authors report no conflicts of interest in this work.
References
de Boer AG, Taskila T, Ojajärvi A, van Dijk FJH, Verbeek JHAM. Cancer survivors and unemployment: a meta-analysis and meta-regression. JAMA. 2009;301(7):753–762. | ||
Horsboel TA, Nielsen CV, Andersen NT, Nielsen B, de Thurah A. Risk of disability pension for patients diagnosed with haematological malignancies: a register-based cohort study. Acta Oncol. 2014;53(6):724–734. | ||
Kennedy F. Returning to work following cancer: a qualitative exploratory study into the experience of returning to work following cancer. Eur J Cancer Care (Engl). 2007;16(16):17–25. | ||
Horsboel TA, De Thurah A, Nielsen B, Nielsen CV. Factors associated with work outcome for survivors from haematological malignancies–a systematic literature review. Eur J Cancer Care (Engl). 2012;21(4):424–435. | ||
Roelen CA, Koopmans PC, Groothoff JW, van der Klink JJ, Bültmann U. Sickness absence and full return to work after cancer: 2-year follow-up of register data for different cancer sites. Psychooncology. 2011;20(9):1001–1006. | ||
Mols F, Vingerhoets AJ, Coebergh JW, van de Poll-Franse LV. Quality of life among long-term breast cancer survivors: a systematic review. Eur J Cancer. 2005;41(17):2613–2619. | ||
Greenwald HP, Dirks SJ, Borgatta EF, McCorkle R, Nevitt MC, Yelin EH. Work disability among cancer patients. Soc Sci Med. 1989;29(11):1253–1259. | ||
Spelten ER, Sprangers MAG, Verbeek JHAM. Factors reported to influence the return to work of cancer survivors: a literature review. Psychooncology. 2002;11(2):124–131. | ||
Wells M, Williams B, Firnigl D, et al. Supporting “work-related goals” rather than “return to work” after cancer? A systematic review and meta-synthesis of 25 qualitative studies. Psychooncology. 2013;22(6):1208–1219. | ||
Torp S, Nielsen RA, Gudbergsson SB, Fosså SD, Dahl AA. Sick leave patterns among 5-year cancer survivors: a registry-based retrospective cohort study. J Cancer Surviv. 2012;6(3):315–323. | ||
Syse A, Tretli S, Kravdal Ø. Cancer’s impact on employment and earnings – a population-based study from Norway. J Cancer Surviv. 2008;2(3):149–158. | ||
Carlsen K, Oksbjerg Dalton S, Frederiksen K, Diderichsen F, Johansen C. Cancer and the risk for taking early retirement pension: a Danish cohort study. Scand J Public Health. 2008;36(2):117–125. | ||
Pattani S, Constantinovici N, Williams S. Predictors of re-employment and quality of life in NHS staff one year after early retirement because of ill health; a national prospective study. Occup Environ Med. 2004;61:572–576. | ||
Philip T, Guglielmi C, Hagenbeek A, et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin’s lymphoma. N Engl J Med. 1995;333(23):1540–1545. | ||
Gisselbrecht C. Is there any role for transplantation in the rituximab era for diffuse large B-cell lymphoma? Hematology Am Soc Hematol Educ Program. 2012;2012:410–416. | ||
Hensel M, Egerer G, Schneeweiss A, Goldschmidt H, Ho AD. Quality of life and rehabilitation in social and professional life after autologous stem cell transplantation. Ann Oncol. 2002;13(2):209–217. | ||
Andresen S, Brandt J, Dietrich S, Memmer M-L, Ho AD, Witzens-Harig M. The impact of high-dose chemotherapy, autologous stem cell transplant and conventional chemotherapy on quality of life of long-term survivors with follicular lymphoma. Leuk Lymphoma. 2012;53:386–393. | ||
Kiserud CE, Fagerli U-M, Smeland KB, et al. Pattern of employment and associated factors in long-term lymphoma survivors 10 years after high-dose chemotherapy with autologous stem cell transplantation. Acta Oncol. 2016;55(5):547–553. | ||
Arboe B, Josefsson P, Jørgensen J, et al. Danish National Lymphoma Registry. Clin Epidemiol. 2016; 8:577–581. | ||
Arboe B, El-Galaly TC, Clausen MR, et al. The Danish National Lymphoma Registry: coverage and data quality. In: Chu P-Y, editor. PLoS One. 2016;11(6):e0157999. | ||
Pedersen CB. The Danish Civil Registration System. Scand J Public Health. 2011;39:22–25. | ||
Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. | ||
Schmidt M, Schmidt S, Sandegaard J, Eherenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. | ||
Kragholm K, Wissenberg M, Mortensen RN, et al. Return to work in out-of-hospital cardiac arrest survivors: a nationwide register-based follow-up study. Circulation. 2015;131(19):1682–1690. | ||
Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39(7 Suppl):103–105. | ||
Biering K, Hjøllund NH, Lund T. Methods in measuring return to work: a comparison of measures of return to work following treatment of coronary heart disease. J Occup Rehabil. 2013;23(3):400–405. | ||
Hjollund NH, Larsen FB, Andersen JH. Register-based follow-up of social benefits and other transfer payments: accuracy and degree of completeness in a Danish interdepartmental administrative database compared with a population-based survey. Scand J Public Health. 2007;35:497–502. | ||
Horsboel TA, Nielsen CV, Nielsen B, Jensen C, Andersen NT, de Thurah A. Type of hematological malignancy is crucial for the return to work prognosis: a register-based cohort study. J Cancer Surviv. 2013;7(4):614–623. | ||
Ripley B, Venables W. Modern Applied Statistics with S. 4th ed. New York: Springer; 2002. Available from: http://www.stats.ox.ac.uk/pub/MASS4. Accessed November 21, 2016. | ||
Therneau TM. A Package for Survival Analysis in R; 2015. Available from: https://cran.r-project.org/package=survival. Accessed November 21, 2016. | ||
Canivet C, Choi B, Karasek R, Moghaddassi M, Staland-Nyman C, Östergren PO. Can high psychological job demands, low decision latitude, and high job strain predict disability pensions? A 12-year follow-up of middle-aged Swedish workers. Int Arch Occup Environ Health. 2013;86(3):307–319. | ||
de Boer AG, Taskila TK, Tamminga SJ, Feuerstein M, Frings-Dresen MH, Verbeek JH. Interventions to enhance return-to-work for cancer patients. In: Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd; 2015. | ||
Zaman AGNM, Tytgat KMAJ, Klinkenbijl JHG, Frings-Dresen MHW, de Boer AG. Design of a multicentre randomized controlled trial to evaluate the effectiveness of a tailored clinical support intervention to enhance return to work for gastrointestinal cancer patients. BMC Cancer. 2016;16(1):303. | ||
Christensen KB, Feveile H, Labriola M, Lund T. The impact of psychosocial work environment factors on the risk of disability pension in Denmark. Eur J Public Health. 2008;18(3):235–237. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.