")
Back to Journals » Infection and Drug Resistance » Volume 16
Retrospective Evaluation of Nosocomial Bacterial Infections and Their Antimicrobial Resistance Patterns Among Hospitalized Patients in Mogadishu, Somalia
Authors Sheikh Omar NM, Erismis B, Muse Osman M , Garba B , Hassan MA , Akuku IG
Received 20 November 2022
Accepted for publication 22 January 2023
Published 1 February 2023 Volume 2023:16 Pages 705—720
DOI https://doi.org/10.2147/IDR.S398387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Nasteho Mohamed Sheikh Omar,1 Betul Erismis,2 Marian Muse Osman,1 Bashiru Garba,3,4 Mohamed Abdulahi Hassan,3 Isaiah G Akuku5
1University of Health Sciences Turkey, Mogadishu Somalia-Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 2University of Health Sciences, Bakirkoy Dr Sadi Konuk Education and Research Hospital, Istanbul, Turkey; 3Dr Sumait Hospital, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, 2526, Somalia; 4Department of Veterinary Public Health and Preventive Medicine, Faculty of Veterinary Medicine, Usmanu Danfodiyo University, Sokoto, Sokoto State, Nigeria; 5Institutes of Tropical and Infectious Diseases, University of Nairobi, Nairobi, Kenya
Correspondence: Mohamed Abdulahi Hassan, Tel + 252 61 5987780, Email [email protected]
Background: Nosocomial infection constitutes a significant public health challenge globally, with resource-limited countries bearing the greatest burden. Sadly, the emergence of drug-resistant strains of these pathogens have worsened the already precarious situation.
Methods: This study aimed to determine the incidence of nosocomial infections, the causative agents, and their antimicrobial susceptibilities among patients admitted to a tertiary hospital in Mogadishu, Somalia. The study included patients who had positive cultures 48 hours after admission. Abstracted data include the patient’s demographic, infection outcome, the agents involved, and the site of infection.
Results: A total of 330 patients were found to have acquired nosocomial infection, comprising 100 (30%) patients from the ICU department. The median age for the patients in this study was 36 years. Patients who died of all-cause mortality were older than those discharged. Most of the bacteria were collected from sepsis/bloodstream infections (34%) dominated by Staphylococcus aureus (42.1%), Acinetobacter baumannii (14.0%), Escherichia coli (14.0%), and Klebsiella spp. (7.0%). Urinary tract infections were mainly associated with Escherichia coli (37.5%), Staphylococcus aureus (18.8%), and Klebsiella spp. 50% of all microorganisms were multidrug-resistant.
Conclusion: The findings of this study suggested that hospital infection control and prevention strategies need to be strengthened to improve the quality of care among hospitalized patients.
Keywords: healthcare-associated infections, multi-drug resistant, infectious diseases, Somalia, nosocomial infection
Introduction
Nosocomial infections (NI) also referred to as hospital-acquired infections are common disease conditions that follow hospital admissions that lasted 48–72 hours.1 It is estimated that 1 out of every ten patients admitted to a hospital for more than 48 hours could acquire it and that most patients with a hospital-acquired infection spend 2.5 times longer in the hospital.2 The most prevalent nosocomial infection is caused by bacterial pathogens with the Gram-positive bacteria Staphylococcus aureus being the most common.3,4 Recently, the rate of antibiotic-resistant bacteria associated with nosocomial infections in the ICU is increasing.4 The rapid rate at which bacterial pathogens acquire resistance is driven by the unregulated sale, prescription, and usage of antibiotics.5–7
Hospital acquired infections (HAI) are among the major causes of increased mortality, morbidity, length of stay, and cost in the world. Although the number of patients in intensive care units is smaller compared to the number of patients in other clinics, the rate of HAI is significantly higher in ICU than in other units.4 Several factors are believed to be responsible for this high number of ICU-related NI including, invasive therapeutic measures or diagnostic interventions, administration of wide-spectrum antibiotics, presence of underlying diseases and mechanical ventilation, as well as central venous catheterization.8,9 It is generally believed that the majority of NI occurring in intensive care units are associated with invasive device usage.10
A recent World Health Organization report indicates that annually, hundreds of millions of people acquire nosocomial infections including from the most advanced countries.11 The report also revealed that 15 patients out of every 100 will acquire at least one nosocomial infection in resource-poor countries while 1 out of every 10 infected patients will die because of the hospital-acquired infection.11 This report shows that the risk to acquire HAI is universal and pervades every healthcare facility and system worldwide, however, while the true burden remains unknown, particularly in developing countries, the incidence of the condition is 2–3 times higher in lower-middle income countries compared to high-income countries.11
Investigations have been undertaken in many African countries to determine surgical and other hospital-related infections including Kenya, Nigeria, Tanzania, Ethiopia, and Burkina Faso.4,12–15 The findings from these studies demonstrate similar patterns of pathogens which have also been incriminated as the major causes of NI including staphylococci, Enterobacteriaceae and Pseudomonas spp., with high levels of antimicrobial resistance. However, most of the research could only be conducted in hospitals that have an operating microbiology unit, with adequate resources and well-trained staff. Limited resources have led to the identification of only the noticeable culturable bacteria while providing a partial picture of the test while the antimicrobial resistance patterns of pathogens have not been adequately studied.11
Till now, only a little information about the burden of HAI is available in the Republic of Somalia due to many factors that range from limited resources, funding, and commitments from the research community.16,17 Therefore, this study aimed to determine the prevalence of bacterial pathogens causing nosocomial infections, as well as their antimicrobial resistance profile across all the departments in the Tertiary Somali-Turkish Training and Research Hospital, Mogadishu, Somalia.
Materials and Methods
Study Design and Location
This was a retrospective study conducted to evaluate the nosocomial infections in the Somali-Turkey Recep Tayyip Erdogan Training and Research Hospital, Somalia between January 1, 2018, and December 31, 2020. The hospital is the largest tertiary referral hospital in the region with a more than 250-bed capacity serving about 327,000 patients annually.
Inclusion Criteria
All the wards in all the departments of the hospital were surveyed except the outpatient and emergency departments. Patients’ demographic characteristics (age, gender), and the results of the culture tests were retrieved through the computerized database of the hospital. Patients who were tested during the study period and diagnosed with nosocomial infections (growth after 48 hours of admission) in inpatient departments were enrolled in the study.
Bacterial Culture and Isolation
According to hospital policy, a single culture test is mandatory for all hospitalized patients. This is a routine practice that follows clinical sample collection, bacterial culture, identification, and then antimicrobial susceptibility assay. All forms of clinical specimens including morning midstream urine, peritoneal and pleural fluids, blood, stool, respiratory secretions, and wound discharge, were aseptically collected, and sent to the microbiology laboratory for culture and identification of bacteria based on colony morphology, gram reaction, and biochemical characterizations.18 The BBL Crystal enteric/non-fermenter identification system (Becton Dickinson, Sparks, MD, USA) was used for the identification of bacterial isolates. Briefly, samples were plated on selective media including blood agar, mannitol salt agar, and MacConkey agar. The choice of growth media used was based on the clinical specimen in accordance with the instructions of the system. Presumptive bacterial isolates were then subjected to the system which is designed to identify members of the family Enterobacteriaceae as well as common isolates of clinically significant glucose-nonfermenting gram-negative bacilli, including biochemical tests like citrate, sulphide, indole, and triple sugar iron for confirmation. The reaction patterns for the substrates were then interpreted with the BBL Crystal auto-reader (Becton Dickinson).19
Antibiotic Susceptibility Assay
Confirmed isolates after biochemical screening were subjected to antibiotic susceptibility tests using the Kirby Bauer disk diffusion method based on the clinical and laboratory standards institute guidelines (CLSI).20 In brief, the bacterial isolates were suspended to a density equivalent to 0.5 McFarland standard and then used to inoculate a petri dish containing solidified Mueller–Hinton agar (Himedia, India) by covering the entire surface, then applying the antimicrobial disks on the seeded plates with the aid of dispenser and incubated at 35°C for 18 hours according to the CLSI protocol. The panel of antimicrobial impregnated discs (Oxoid, USA) include aminoglycosides, ansamycins, carbapenems, cephalosporins, cephalosporins+beta lactamase inhibitors, fluoroquinolones, folate pathway inhibitor, fucidanes, glycopeptides, glycylcyclines, lincosamides, nitrofuran, oxazolidinones, penicillin, penicillin+beta lactamase inhibitors, phosphonic acids, polymyxins, streptogramins, and tetracyclines to determine resistance or susceptibility of the isolates to the drugs.21 To avoid overestimation, the isolates with the zone of inhibition within the intermediate range were susceptible. Escherichia coli ATCC 25922 was used as a control according to the CLSI standard.20
Data Analysis
All statistical analyses were carried out in R (Version 4.1.2) for Windows software. Descriptive analyses were presented using mean (± Standard Deviation) or median with interquartile range (IQR). The proportions were presented using frequencies and percentages. The Chi-square test or Fisher’s exact test was performed where appropriate. A P-value <0.05 was considered statistically significant.
Results
Characteristics of the Study Population
Retrospective data of the 330 patients retrieved from the hospital’s database were analyzed for nosocomial infections. Most of the patients were male (n = 208) amounting to 63% while 122 were female (37%). The median age of the patients was 36.5 (interquartile range, 42.8). Patients who died of all-cause mortality were older than those discharged (median greater dimension, 45.0 vs 32.0, p = 0.029).
The intensive care units (ICUs) had the largest number of patients studied, with the adult ICU having 98 (29.7%), while the newborn ICU (NICU) had 31 (9.4%). This was followed by the internal medicine ward which had 69 (20.9%) and the pediatric ward with 33 (10.0%) patients. Microbiological examination revealed that most of the bacterial cultures were obtained from clinical blood samples (34.2%) followed by wound cultures (23.6%). The most common comorbidities observed among the patients were renal failure (41.4%), diabetes (20.0%), and stroke (12.9%).
About half of the patients (50.9%) had stayed in the hospital for not more than 15 days, that is, a median total length of stay of 15 (IQR, 15.0), while 229 (69.4%) were discharged from the hospital. Of all the deaths, 81 (80.2%) occurred not more than 30 days after admission. All-cause mortality was also common in patients in the fourth quartile of the length of hospital stay (36.7%). The groups by the 15-days-interval length of stay in the hospital were statistically indifferent as regards demographics (Table 1).
 |
Table 1 Characteristics of Patients with Nosocomial Infections |
Bacterial Isolates from Patients with Nosocomial Infections
Among the bacteria isolated, 240 (73.0%) were Gram-negative bacteria. The bacterial isolates were mainly Escherichia coli (26.3%), Staphylococcus aureus (24.0%), Acinetobacter baumannii (14.7%), and Klebsiella spp. (13.2%). Of all studied patients, the case fatality rate or death by a fatal diagnosis was 30.6%. The case fatality rate was high for Acinetobacter baumannii (50.0%), Pseudomonas spp. (48.4%), Klebsiella spp. (38.6%), Escherichia coli (25.3%), and Staphylococcus aureus (14.1%). The bacterial isolates associated with higher case fatality rates also had infected patients that stayed much longer in hospital with a median of 21.0 (IQR, 21.5) days for Acinetobacter baumannii, 18.0 (IQR, 16.2) days for Pseudomonas spp. and 14.0 (IQR, 13.0) days for Klebsiella spp (Table 2). Although Escherichia coli had the highest infection rate, it was associated with a relatively lower median hospital stay (13.5 [IQR, 14.8]) compared to the other isolates with higher case fatality rates.
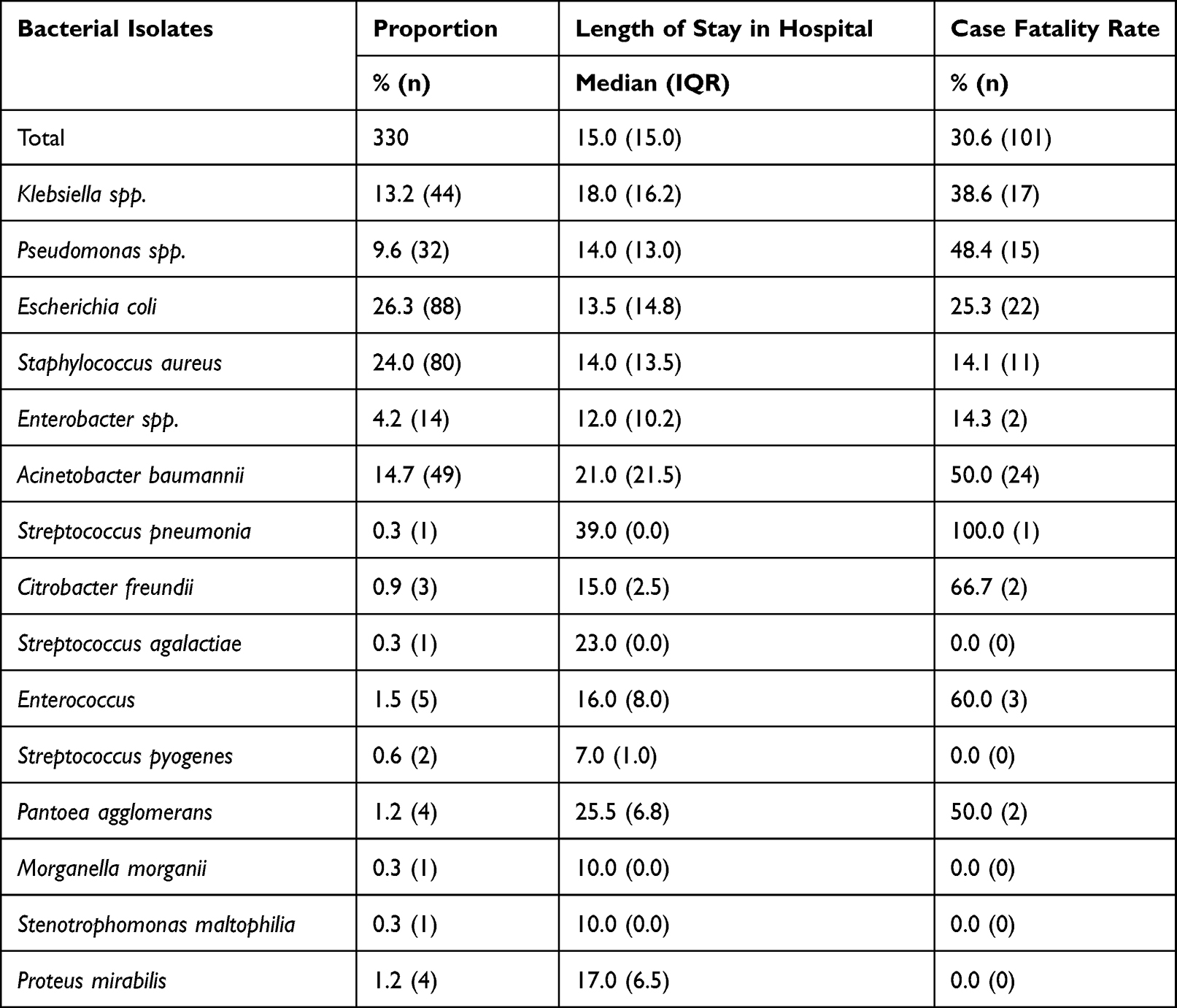 |
Table 2 Nosocomial Infections Concerning the Length of Stay in Days and Case Fatality Rate |
Acinetobacter baumannii, Klebsiella spp., Pseudomonas spp., Escherichia coli, and Staphylococcus aureus were the dominant bacterial isolates in all the departments/wards. Of all the nosocomial infections in the ICU and NICU, 16% and 35.5%, respectively were for Staphylococcus aureus. Notably, apart from Streptococcus agalactiae, all the bacteria were isolated from cultures from the department of internal medicine (Table 3).
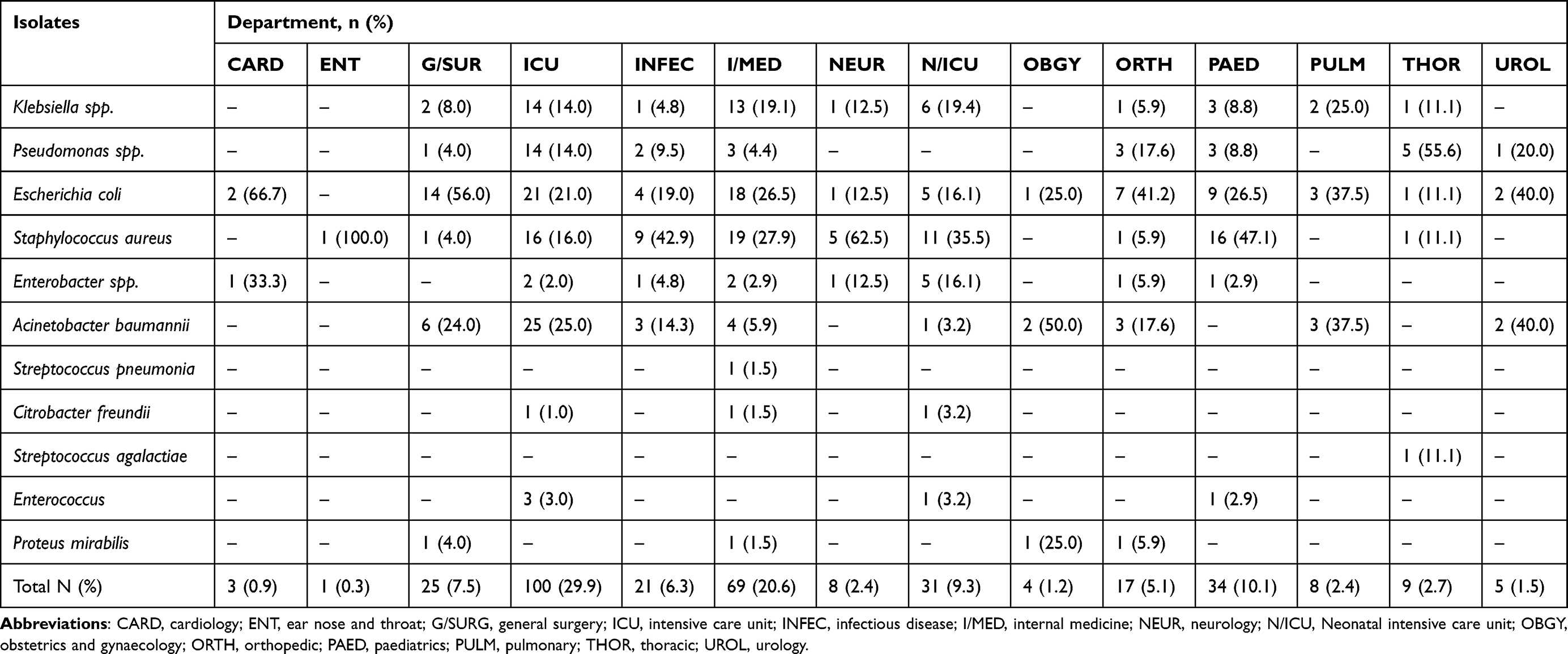 |
Table 3 Frequency Distribution of Bacterial Isolates from Patients with Nosocomial Infections from Various Departments |
Most of the bacteria isolated were from sepsis/bloodstream infections (34%) dominated by Staphylococcus aureus (42.1%), followed by Acinetobacter baumannii (14.0%), Escherichia coli (14.0%) and Klebsiella spp. (7.0%). On the other hand, urinary tract infections were mainly Escherichia coli (37.5%), Staphylococcus aureus (18.8%) and Klebsiella spp. (15.6%) (Table 4).
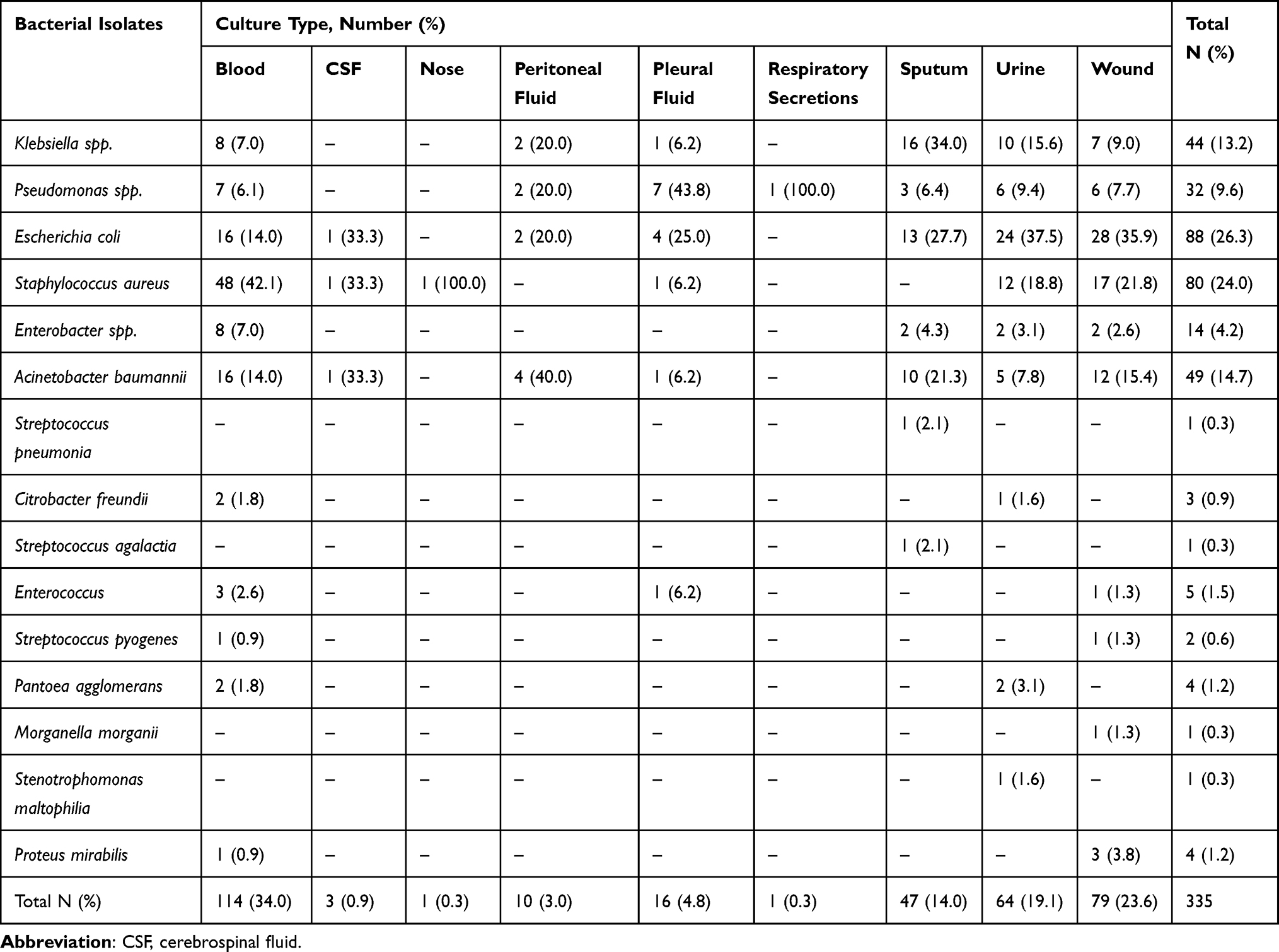 |
Table 4 Frequency Distribution of Bacterial Isolates from Patients with Nosocomial Infections Based on a Clinical Sample |
The Pattern of Antimicrobial Susceptibility
This study observed that the bacterial isolates obtained exhibited resistance to 50.1% of the antibiotics tested. This comprises 28.7% of Gram-positive bacteria, while the majority (58.9%) of the bacterial isolates with resistance belonged to the Gram-negative bacteria (Table 5).
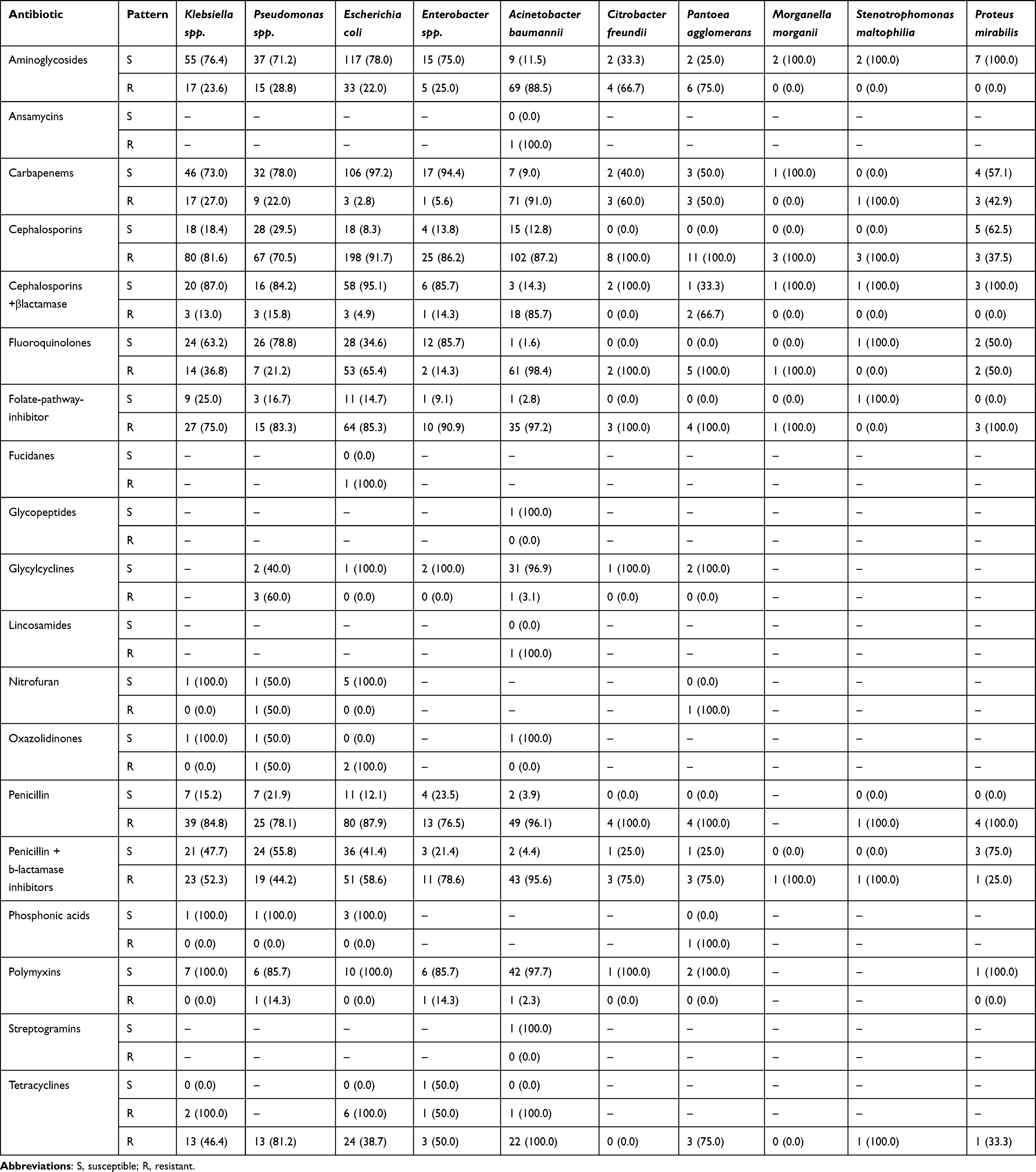 |
Table 5 Pattern of Antimicrobial Susceptibility for Gram-Negative Bacterial Isolates from Patients with Nosocomial Infections |
For the Gram-negative bacterial isolates, the percentage of resistance to aminoglycosides was 88.5% for Acinetobacter baumannii. Resistance to cephalosporins was high for Klebsiella spp., Pseudomonas spp., Escherichia coli, Enterobacter spp., Acinetobacter baumannii. For the Gram-negative bacteria, resistance ranged from 0.0% to 100% for cephalosporins (Table 5).
For the Gram-positive bacteria, most of the cultures were for Staphylococcus aureus. Resistance was mostly against tetracyclines (46.7%) and macrolides (46.2%). The resistance pattern to the antibiotic agents is summarized in Table 6.
 |
Table 6 Pattern of Antimicrobial Susceptibility for Gram-Positive Bacterial Isolates from Patients with Nosocomial Infections |
Nosocomial Infections and the Effect of Antibiotic Resistance on Length of Stay and Likelihood of Death
As shown in Table 7, for the mortality outcome, for every one-unit increase in resistance to antibiotic class, the odds of mortality increased by 4% (adjusted odds ratio of 1.04). However, the finding was not statistical (p = 0.535). The only covariates used to adjust the effect of multi-drug resistance that were statistically significant were age and ward/department type (ICU/NICU compared to other departments/wards). In this case, a one-year increase in age increased the odds of mortality by 2% (AOR 1.02; 95% CI 1.01–1.03; p <0.001). There were 14-fold odds increase in the odds of death for the patients from ICU/NICU compared to all other departments (AOR 14.0; 95% CI 7.71–26.4; p=<0.001). For every one-unit increase in resistance to an antibiotic class, there was a 15% increase in days for length of stay in the hospital (AOR 1.15; 95% CI 1.06–1.25; p = 0.001). All the other covariates (age, sex, co-morbidities, department/ward) were not statistically significant.
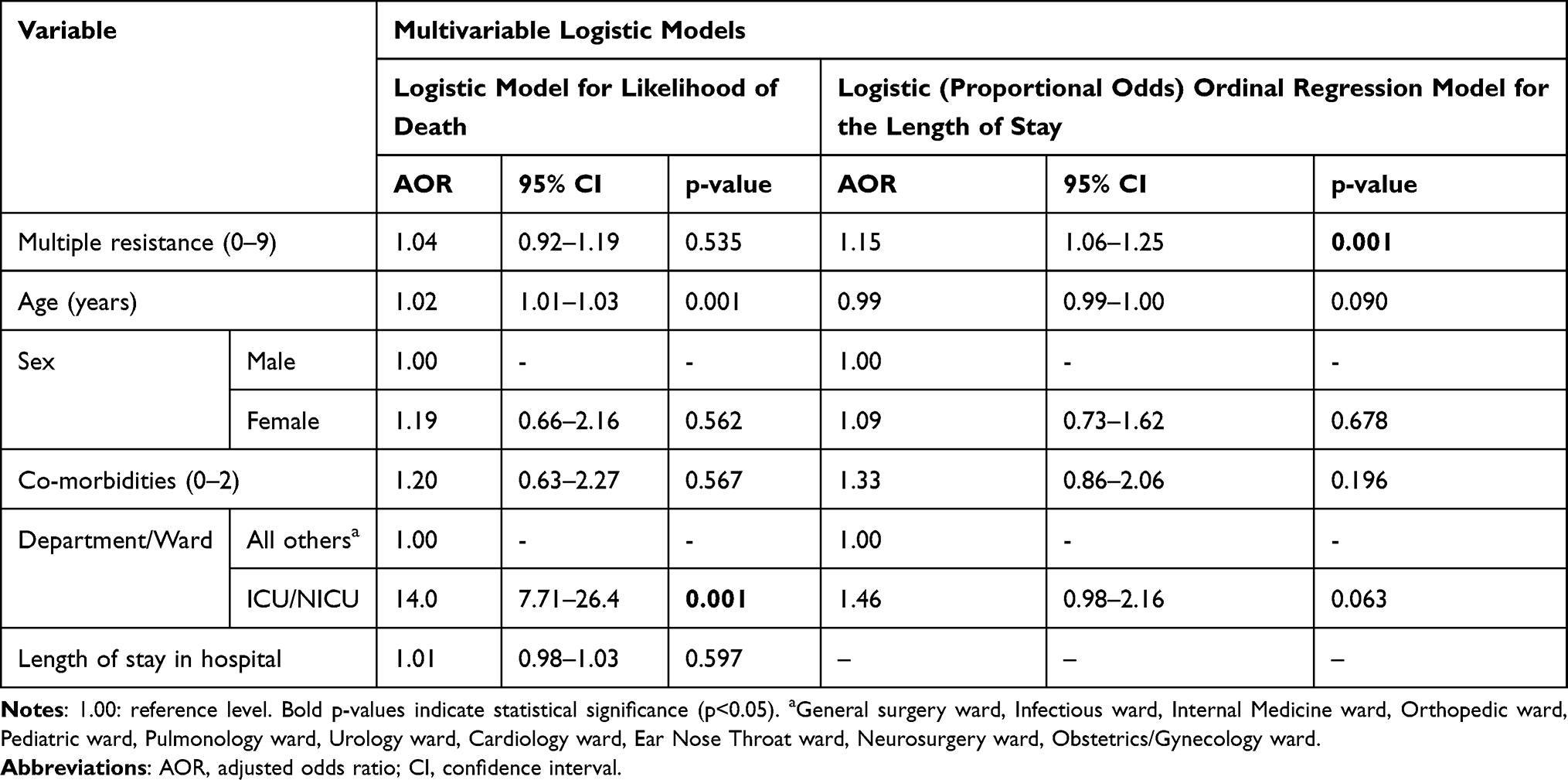 |
Table 7 Multivariable Adjusted Regression Models for the Effect of Multidrug Resistance on the Likelihood of Death and Length of Stay at the Hospital |
Discussion
Hospital-acquired infection is a health complication that usually occurs during health service delivery common in both developed and resource-poor countries. Although, reports have shown that the incidence of NI is 2–3 times higher among lower/middle-income countries compared to high-income countries.11 Also, the impact of these infections is not only restricted to individuals but also the larger community settings having been associated with multidrug-resistant infections.22 Hence, understanding the endemic NIs and the antimicrobial resistance characteristics of the causative agents is vital, and forms part of the core component of infection prevention and control measures globally.23
The prevalence of culture-positive HAI in our study was 34.2% for blood samples, while wound swab cultures have 23.6%. Some of the common means by which hospitalized patients acquire infection are due to cross-contamination from other infected patients and health workers, diminished immune responses which tend to increase susceptibility, as well as infections following surgical site contamination, implants, and central line-associated bloodstream infections.24,25 Among the positive isolates, 58.9% were Gram-negative bacteria. This is similar to a report by Allegranzi et al who reported that gram-negative bacilli were the most common hospital isolates.26 It is thought that in recent years, changes in health care, infection prevention and control practices at hospitals, and antimicrobial usage and resistance are among the major factors driving the frequency of NI caused by these gram-negative organisms.27 Between 2009 and 2018, a total of 22 studies have conducted including countries like Tunisia, Algeria, Madagascar, Uganda, South Africa, Egypt, Senegal, Benin, Gambia, and Tanzania. All these investigations observed that the most prevalent conditions associated with NI were bacteremia (32%), pneumonia (19%), and urinary tract infections (13%).28–31 In this study, bacteremia was also the illness with the highest isolation (34.2%), followed by wound infections (23.6%), and UTIs (19.1%). Nosocomial bacteremia is one of the common indicators of trends in overall nosocomial infection frequently used in developed countries because of the availability of clear definitions and clinical relevance.32
In a previous study conducted in Tunisia, 67 ICU patients were found to develop HAI, among which 67.2% were male and 32.8% were female. In this study, the intensive care units (ICUs) also had the largest number of patients with NI, with the adult ICU having 29.7% of the cases while the newborn ICU (NICU) had 9.4%. ICU patients are vulnerable because their immune system does not function normally due to the critical nature of their illnesses. Hence, the body’s natural defenses are not working properly. Secondly, invasive devices such as needles and tubes are routinely used as part of the regular treatments of the ICU patients. These devices bypass the body’s normal defenses such as the outer layers of skin, and where aseptic devices are not used, during these invasive treatments, infection usually occurs as commonly seen in respiratory infection following airway intubation to assist breathing; septicemia due to intravenous lines to administer medications; or urinary tract infection due to catheterization to drain the bladder.33–35
The rate of NI for the other departments was internal medicine at 20.9%, and the pediatric ward at 10.0%. Intensive care units have been reported to have a higher rate of NI because of the specific setting in which it is operated. The high rate of ICU infections recorded in this study is consonant with reports in Serbia.36 A related study of 63 ICU patients conducted in Tunisia to determine the epidemiological and predisposing factors associated with NI, the endemic bacterial species and their drug resistance profiles, as well as their roles in the morbidity and mortality of infected patients, found that the mean age of the patients was 51, which was significantly higher when compared to our study (42).37 The study also reported the most common bacteria during hospitalization, was Acinetobacter with 87.5% of the isolates being sensitive to colistin. In our study, Acinetobacter was also among the highest bacterial isolates (97.7%) and these isolates were also found to be susceptible to colistin. However, a retrospective cross-sectional study conducted among pediatrics in Kenya revealed that Klebsiella was the most common bacterial pathogen associated with NI, while S. aureus and E. coli were the most reported in Gabon.15,38 These goes to show the diversity of bacterial pathogens usually incriminated in NI infections in most sub-Saharan African countries. On the other hand, while the mortality rate due to NI was found to be 36.6% in Tunisia study, the mortality rate in our study was found to be slightly lower at 30.6%. This may be related to the fact that only ICU patients were included in the referred study and the number of patients was less compared to our study. Similarly, in a related study that included 238 newborns in the neonatal ICU in Egypt, a total of 51 NIs were recorded from 49 patients. The most common condition was pneumonia with 11.3%, followed by bacteremia with 8.8%.30 In addition, the most frequently isolated bacteria were Klebsiella with a rate of 33.3%, followed by E. coli with a rate of 21.6%. In our study, the most common cause among newborns was S. aureus, followed by Klebsiella and E. coli. The findings in our study agree with a 2-year multi-center retrospective study conducted in the Hubei Province, China where E. coli, S. aureus and K. pneumoniae were found to be the most common pathogens responsible for nosocomial bloodstream infections.39 Studies have shown that patients in the intensive care unit and surgical service patients are more prone to acquiring NI, with catheterization being the most common source of infections (28.81%), followed by bacteremia (20.34%), and then skin and soft tissue infections with a rate of 20.34%.29 The severity of the hospital-acquired infection and its incidence is reported to be directly proportional to patients’ immunological status, thereby making patients in the burn, and intensive care units including neonates to be the most affected groups.40
Length of stay and presence of indwelling urinary catheter as well as the history of recent surgery have been reported as significant risk factors associated with HAI.41–43 In our study, prolonged hospitalization was also found to be a risk factor for acquiring NI where we observed that hospitalization for more than ten days increased the chances of getting NI as well as the risk of mortality, and this finding was found to be statistically significant. This study also observed 14-fold odds increase in odds of death for the patients from ICU/NICU who developed NI (AOR 14.0; 95% CI 7.71–26.4; p=<0.001). Duration of 10 days and more have previously been reported to have a significant association with mortality in NI.44
The findings of the present study demonstrated a major problem with the antimicrobial resistance rate among the bacterial isolates obtained from the hospital, similar to the global trends.45–47 This goes to show the urgent need for hospitals to recognize antimicrobial resistance as a major concern and develop a measure to control its emergence and spread.48 Overall, 50.1% of all bacterial isolates exhibited resistance against the drugs tested with 28.7% being Gram-positive bacteria, while the majority (58.9%) of the bacterial isolates belonged to Gram-negative bacteria. In our study, ampicillin-clavulanic acid resistance among Pseudomonas was 88.2%, and TMP-SX resistance was 83.3%. The Acinetobacter in the study was found to exhibit multi-drug resistance to ampicillin-clavulanic acid, ceftriaxone, cefotaxime, ciprofloxacin, and tetracycline. This investigation also found out that for every unit increase in resistance to an antibiotic class, there was a 15% increase in days for length of stay in hospital (AOR 1.15; 95% CI 1.06–1.25; p = 0.001). Our findings are indicating that A. baumannii, Klebsiella spp., Pseudomonas spp., and Escherichia coli are the major health problem in the clinical area in the hospital and likely to be the case in most healthcare institutions in the country. In addition, in this study, all the isolates were found to be sensitive to vancomycin. This may be related to the fact that approximately 60% of the patients in our study were ward patients, who mostly do not have an invasive catheter before, and they could not easily access antibiotics due to their low socioeconomic status. This is similar to reports from Ethiopia where 58.8% of enterococci were susceptible to vancomycin.49 Furthermore, 27% of Klebsiella, 2.8% of E. coli, and 5.6% of enterobacteria were found to be carbapenem-resistant. In total, 11.05% of 190 HAIs belonging to Enterobacteriaceae were found to have carbapenem resistance. This may be related to the small number of patients – not only intensive care patients but also both service and intensive care patients – in our study.50 Another interesting finding in this study is that while all the Klebsiella cases were susceptible to colistin and piperacillin-tazobactam, 85.7% were ceftriaxone resistant, 25% were ceftazidime resistant, 17.1% were imipenem resistant, 38.7% were ciprofloxacin-resistant, and 3.3% were amikacin resistant. In a previous study, 73.81% ceftriaxone resistance, 61.54% ciprofloxacin resistance, 17.36% imipenem resistance, 16.67% amikacin resistance, and 6.38% colistin resistance were found for E. coli.51 However, all the isolates were resistant to ceftriaxone, while 69.4% were resistant to ciprofloxacin. This is also in agreement with Rosenthal et al who reported 40.28% ciprofloxacin resistance from clinical samples obtained from patients with HAI.51 Ciprofloxacin resistance among major causes of HAI including E. coli has been on the increase due to the frequent misuse of this antimicrobial agent as empirical therapy.52
Limitations
It is a single-center study, and in terms of NIs, not only surgical site infections but all wound infections were included in the study. Sputum cultures were taken from patients with pneumonia, but it could not be determined whether they were connected to the mechanical ventilator due to the deficiencies in the records. Also, because the data were collected over a 3-year period, discrepancies may exist in terms of patient records and test results.
Conclusion
In conclusion, NIs were common in our setup with blood stream infection as the commonest followed by wound infections. Therefore, infection prevention and control efforts should prioritize these cases. Moreover, despite the discrepancies regarding the number of isolates subjected to each of the drugs tested, we were still able to identify multidrug resistant organisms with Acinetobacter baumannii being resistant to third generation cephalosporins. Hence, we have an idea about the nature of resistant bacteria associated with NIs in the study location. These findings can be useful for NI surveillance and will also guide antimicrobial stewardship program in the hospital as well as other healthcare institutions in the country to enhance their infection prevention and control efforts as well as promoting appropriate usage of antimicrobials.
Data Sharing Statement
All data related to the study is contained within this manuscript.
Ethics Approval
This study was approved by the Research Ethics Committee of the Somali-Turkey Recep Tayyip Erdogan Training and Research Hospital (17.05.2021-MSTH/6199). Database management complies with legislation on privacy, and this research followed the ethical principles of the Helsinki Declaration. Also, written informed consent was obtained from each participant or their parents indicating their willingness to participate in the study.
Funding
This study did not receive any financial support from any individual or organization.
Disclosure
The authors declare that they have no competing interests.
References
1. Sadeghi H, Khoei SG, Bakht M, et al. A retrospective cross-sectional survey on nosocomial bacterial infections and their antimicrobial susceptibility patterns in hospitalized patients in northwest of Iran. BMC Res Notes. 2021;14(1):1–7. doi:10.1186/S13104-021-05503-0/TABLES/2
2. Stewart S, Robertson C, Pan J, et al. Impact of healthcare-associated infection on length of stay. J Hosp Infect. 2021;114:23–31. doi:10.1016/J.JHIN.2021.02.026
3. Nimer NA. Nosocomial infection and antibiotic-resistant threat in the Middle East. Infect Drug Resist. 2022;15:631. doi:10.2147/IDR.S351755
4. Alemu AY, Endalamaw A, Belay DM, Mekonen DK, Birhan BM, Bayih WA. Healthcare-associated infection and its determinants in Ethiopia: a systematic review and meta-analysis. PLoS One. 2020;15(10):e0241073. doi:10.1371/JOURNAL.PONE.0241073
5. Ventola CL. The antibiotic resistance crisis: part 1: causes and threats. Pharmacol Ther. 2015;40(4):277.
6. Ayukekbong JA, Ntemgwa M, Atabe AN. The threat of antimicrobial resistance in developing countries: causes and control strategies. Antimicrob Resist Infect Control. 2017;6(1):1–8. doi:10.1186/S13756-017-0208-X/TABLES/2
7. Karim MR, Zakaria Z, Hassan L, Ahmad NI, Faiz NM, Garba B. Rapid detection of colistin-resistant Enterobacterales using the resazurin reduction-based assay. J Glob Antimicrob Resist. 2021;26:154–156. doi:10.1016/J.JGAR.2021.05.012
8. Effatpanah M, Effatpanah H, Geravandi S, et al. The prevalence of nosocomial infection rates and needle sticks injuries at a teaching hospital, during 2013–2014. Clin Epidemiol Glob Health. 2020;8(3):785–790. doi:10.1016/j.cegh.2020.01.020
9. Sikora A, Zahra F. Nosocomial Infections. StatPearls; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559312/.
10. Dereli N, Ozayar E, Degerli S, Sahin S, Koç F. Three-year evaluation of nosocomial infection rates of the ICU. Braz J Anesthesiol. 2013;63(1):73–84. doi:10.1016/S0034-7094(13
11. World Health Organization. WHO’s Infection prevention & control department. WHO report on member states information session on infection prevention and control (IPC); 2022. Available from: https://www.who.int/teams/integrated-health-services/infection-prevention-control.
12. Nejad SB, Allegranzi B, Syed SB, Ellisc B, Pittetd D. Health-care-associated infection in Africa: a systematic review. Bull World Health Organ. 2011;89(10):757. doi:10.2471/BLT.11.088179
13. Gosling R, Mbatia R, Savage A, Mulligan JA, Reyburn H. Prevalence of hospital-acquired infections in a tertiary referral hospital in northern Tanzania. Ann Trop Med Parasitol. 2003;97(1):69–73. doi:10.1179/000349803125002724
14. Abubakar U. Point-prevalence survey of hospital acquired infections in three acute care hospitals in Northern Nigeria. Antimicrob Resist Infect Control. 2020;9(1):1–7. doi:10.1186/S13756-020-00722-9/TABLES/4
15. Patil RK, Kabera B, Muia CK, Ale BM. Hospital acquired infections in a private paediatric hospital in Kenya: a retrospective cross-sectional study. PAMJ. 2022;41:28. doi:10.11604/PAMJ.2022.41.28.25820
16. Aden MA, Bashiru G. How misuse of antimicrobial agents is exacerbating the challenges facing somalia’s public health. Afr J Infect Dis. 2022;16(2):26. doi:10.21010/AJID.V16I2S.4
17. Moussa AA, Abdi AA, Awale MA, Garba B. Occurrence and phenotypic characterization of multidrug-resistant bacterial pathogens isolated from patients in a public hospital in Mogadishu, Somalia. Infect Drug Resist. 2021;14:825–832. doi:10.2147/IDR.S275090
18. Giuliano C, Patel CR, Kale-Pradhan PB. A guide to bacterial culture identification and results interpretation. Pharmacol Ther. 2019;44(4):192. doi:10.1017/ice.2016.82
19. Lo-Ten-Foe JR, Ververs MAC, Buiting AGM. Comparative evaluation of automated reading versus visual interpretation with the BBL Crystal enteric/nonfermenter identification system in a clinical setting. Eur J Clin Microbiol Infect Dis. 2007;26(6):443. doi:10.1007/S10096-007-0317-1
20. Wayne PA. CLSI Performance Standards for Antimicrobial Susceptibility Testing Performance Standards for Antimicrobial Susceptibility Testing.
21. Zakaria Z, Hassan L, Ahmad N, et al. Discerning the antimicrobial resistance, virulence, and phylogenetic relatedness of salmonella isolates across the human, poultry, and food materials sources in Malaysia. Front Microbiol. 2021;1:2513. doi:10.3389/FMICB.2021.652642
22. Monegro AF, Muppidi V, Regunath H. Hospital Acquired Infections. Cambridge Handbook of Psychology, Health and Medicine.
23. Murhekar MV, Kumar CG. Health-care-associated infection surveillance in India. Lancet Glob Health. 2022;10(9):e1222–e1223. doi:10.1016/S2214-109X(22)00317-5
24. Haque M, Sartelli M, McKimm J, Bakar MA. Health care-associated infections – an overview. Infect Drug Resist. 2018;11:2321. doi:10.2147/IDR.S177247
25. Narayana JL, Huang HN, Wu CJ, Chen JY. Efficacy of the antimicrobial peptide TP4 against Helicobacter pylori infection: in vitro membrane perturbation via micellization and in vivo suppression of host immune responses in a mouse model. Oncotarget. 2015;6(15):12936. doi:10.18632/ONCOTARGET.4101
26. Allegranzi B, Nejad SB, Combescure C, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011;377(9761):228–241. doi:10.1016/S0140-6736(10)61458-4
27. Gaynes R, Edwards JR. Overview of nosocomial infections caused by gram-negative bacilli. Clin Infect Dis. 2005;41(6):848–854. doi:10.1086/432803/2/41-6-848-FIG005.GIF
28. Dell AJ, Navsaria PH, Gray S, Kloppers JC. Nosocomial infections: a further assault on patients in a high-volume urban trauma centre in South Africa. SAMJ. 2020;110(2):123–125. doi:10.7196/SAMJ.2020.V110I2.14243
29. Nouetchognou JS, Ateudjieu J, Jemea B, Mesumbe EN, Mbanya D. Surveillance of nosocomial infections in the yaounde university teaching hospital, Cameroon. BMC Res Notes. 2016;9(1):1–8. doi:10.1186/S13104-016-2310-1/FIGURES/1
30. Abdel-Wahab F, Ghoneim M, Khashaba M, El-Gilany AH, Abdel-Hady D. Nosocomial infection surveillance in an Egyptian neonatal intensive care unit. J Hosp Infect. 2013;83(3):196–199. doi:10.1016/J.JHIN.2012.10.017
31. Rejeb M, Sahli J, Chebil D, et al. Mortality Among Patients with Nosocomial Infections in Tertiary Intensive Care Units of Sahloul Hospital, Sousse, Tunisia. Archives of Iranian Medicine; 2016.
32. Hongsuwan M, Srisamang P, Kanoksil M, et al. Increasing incidence of hospital-acquired and healthcare-associated bacteremia in northeast Thailand: a multicenter surveillance study. PLoS One. 2014;9:10. doi:10.1371/JOURNAL.PONE.0109324
33. Baviskar AS, Khatib KI, Rajpal D, Dongare HC. Nosocomial infections in surgical intensive care unit: a retrospective single-center study. Int J Crit Illn Inj Sci. 2019;9(1):16. doi:10.4103/IJCIIS.IJCIIS_57_18
34. Wang L, Zhou KH, Chen W, Yu Y, Feng SF. Epidemiology and risk factors for nosocomial infection in the respiratory intensive care unit of a teaching hospital in China: a prospective surveillance during 2013 and 2015. BMC Infect Dis. 2019;19:1. doi:10.1186/S12879-019-3772-2
35. Esfahani BN, Basiri R, Mirhosseini SMM, Moghim S, Dolatkhah S. Nosocomial infections in intensive care unit: pattern of antibiotic-resistance in Iranian community. Adv Biomed Res. 2017;6:54. doi:10.4103/2277-9175.205527
36. Despotovic A, Milosevic B, Milosevic I, et al. Hospital-acquired infections in the adult intensive care unit—Epidemiology, antimicrobial resistance patterns, and risk factors for acquisition and mortality. Am J Infect Control. 2020;48(10):1211–1215. doi:10.1016/J.AJIC.2020.01.009
37. Trifi A, Abdellatif S, Oueslati M, et al. Infections nosocomiales: état des lieux dans un service de réanimation nosocomial infections: current situation in a resuscitation-unit. Tunis Med. 2017;95:3.
38. Scherbaum M, Kösters K, Mürbeth RE, et al. Incidence, pathogens and resistance patterns of nosocomial infections at a rural hospital in Gabon. BMC Infect Dis. 2014;14(1):124. doi:10.1186/1471-2334-14-124
39. Tian L, Sun Z, Zhang Z. Antimicrobial resistance of pathogens causing nosocomial bloodstream infection in Hubei Province, China, from 2014 to 2016: a multicenter retrospective study. BMC Public Health. 2018;18(1):1–8. doi:10.1186/S12889-018-6013-5/FIGURES/6
40. Avershina E, Shapovalova V, Shipulin G. Fighting antibiotic resistance in hospital-acquired infections: current state and emerging technologies in disease prevention, diagnostics and therapy. Front Microbiol. 2021;12:2044. doi:10.3389/FMICB.2021.707330/BIBTEX
41. Ali S, Birhane M, Bekele S, et al. Healthcare associated infection and its risk factors among patients admitted to a tertiary hospital in Ethiopia: longitudinal study. Antimicrob Resist Infect Control. 2018;7:2. doi:10.1186/S13756-017-0298-5
42. Labi AK, Obeng-Nkrumah N, Owusu E, et al. Multi-centre point-prevalence survey of hospital-acquired infections in Ghana. J Hosp Infect. 2019;101(1):60–68. doi:10.1016/J.JHIN.2018.04.019
43. Bunduki GK, Feasey N, Henrion MYR, Noah P, Musaya J. Healthcare-associated infections and antimicrobial use in surgical wards of a large urban central hospital in Blantyre, Malawi: a point prevalence survey. Infect Prevent Pract. 2021;3:3. doi:10.1016/J.INFPIP.2021.100163
44. Ketata N, Ben Ayed H, Ben Hmida M, et al. Point prevalence survey of health-care associated infections and their risk factors in the tertiary-care referral hospitals of Southern Tunisia. Infect Dis Health. 2021;26(4):284–291. doi:10.1016/J.IDH.2021.06.004
45. Abdulhaleem N, Garba B, Younis H, et al. Current trend on the economic and public health significance of salmonellosis in Iraq. Adv Anim Vet Sci. 2019;7(6):484–491. doi:10.17582/journal.aavs/2019/7.6.484.491
46. Gaddafi MS, Yakubu Y, Garba B, Bello MB, Musawa AI, Lawal H. Occurrence and antimicrobial resistant patterns of methicillin resistant staphylococcus aureus (MRSA) among practicing veterinarians in Kebbi State, Nigeria. Folia Vet. 2020;64(4):55–62. doi:10.2478/FV-2020-0038
47. D’accolti M, Soffritti I, Mazzacane S, Caselli E. Fighting amr in the healthcare environment: microbiome-based sanitation approaches and monitoring tools. Int J Mol Sci. 2019;20:7. doi:10.3390/ijms20071535
48. Bubonja-Sonje M, Matovina M, Skrobonja I, Bedenic B, Abram M. Mechanisms of carbapenem resistance in multidrug-resistant clinical isolates of pseudomonas aeruginosa from a Croatian hospital. Microb Drug Resist. 2015;21(3):261–269. doi:10.1089/MDR.2014.0172
49. Ashagrie D, Genet C, Abera B. Vancomycin-resistant enterococci and coagulase-negative staphylococci prevalence among patients attending at felege hiwot comprehensive specialized hospital, Bahir Dar, Ethiopia. PLoS One. 2021;16(4):e0249823. doi:10.1371/JOURNAL.PONE.0249823
50. Kotb S, Lyman M, Ismail G, et al. Epidemiology of carbapenem-resistant Enterobacteriaceae in Egyptian intensive care units using national healthcare-associated infections surveillance data, 2011-2017. Antimicrob Resist Infect Control. 2020;9:1. doi:10.1186/S13756-019-0639-7
51. Rosenthal VD, Duszynska W, Ider BE, et al. International Nosocomial Infection Control Consortium (INICC) report, data summary of 45 countries for 2013-2018, adult and pediatric units, device-associated module. Am J Infect Control. 2021;49(10):1267–1274. doi:10.1016/J.AJIC.2021.04.077
52. Fasugba O, Gardner A, Mitchell BG, Mnatzaganian G. Ciprofloxacin resistance in community- and hospital-acquired Escherichia coli urinary tract infections: a systematic review and meta-analysis of observational studies. BMC Infect Dis. 2015;15(1):1–16. doi:10.1186/S12879-015-1282-4/FIGURES/6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.