Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Retrospective Database Analysis of the Clinical and Economic Outcomes Associated with Disruptive Surgical Bleeding
Authors Afolabi M, N V P, Kumar A, Danker III WA ![]() , Johnston SS
, Johnston SS
Received 30 July 2025
Accepted for publication 26 September 2025
Published 5 October 2025 Volume 2025:17 Pages 705—716
DOI https://doi.org/10.2147/CEOR.S549490
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Samer Hamidi
Mosadoluwa Afolabi,1 Prathiksha N V,2 Amitha Kumar,3 Walter A Danker III,3 Stephen S Johnston1
1Global Epidemiology, Johnson & Johnson MedTech, New Brunswick, NJ, USA; 2Decision Sciences, Mu Sigma, Bangalore, India; 3Health Economics and Market Access, Johnson & Johnson Medtech, Raritan, NJ, USA
Correspondence: Stephen S Johnston, Global Epidemiology, Johnson & Johnson MedTech, 410 George Street, New Brunswick, NJ, 08901, USA, Tel +1-443-254-2222, Email [email protected]
Background: This study evaluated the clinical and economic outcomes associated with disruptive surgical bleeding (ie, hemorrhage/hematoma that complicates a procedure despite the use of hemostatic agents) among patients with bariatric, colorectal, spine, total hip arthroplasty (THA), and total knee arthroplasty (TKA) surgery.
Methods: Premier Healthcare Database patients aged ≥ 18 with one of the five procedures and hemostatic agent use between January 1-December 31, 2019, were included. Clinical and economic outcomes (ie, operating room time, 90-day all-cause inpatient readmission, in-hospital mortality, intensive care unit [ICU] admission/duration, ventilator use, hospital costs, and length of stay [LOS]) were compared between patients with and without disruptive surgical bleeding. Multivariable analyses adjusted for differences in baseline characteristics.
Results: Among 119,994 patients meeting inclusion criteria, 10.8% had disruptive surgical bleeding despite the use of hemostatic agents (bariatric surgery 5.4%, colorectal surgery 20.0%, spine surgery 11.0%, THA 11.5%, TKA 5.6%). Disruptive bleeding was associated with significantly longer operating room times for bariatric, colorectal, and spine surgery (incremental increases 42.3– 62.4 minutes; p≤ 0.001), increased 90-day all-cause readmission risks for bariatric and spine surgery (incremental absolute risk increases 4.1% bariatric, 0.7% spine; both p=0.011), and increased inpatient mortality risk for all procedures except TKA (incremental absolute risk increases 0.2– 55.0%; p≤ 0.001). ICU admission risks were increased for all procedures except TKA (incremental absolute risk increases 3.0– 21.4%; p≤ 0.05), and ICU days were increased for bariatric, colorectal, and spine surgery (incremental increases 0.8– 2.8 days; p≤ 0.001). Risks for ventilator use were higher for all procedures except THA (incremental absolute risk increases 3.5– 25.2%; p≤ 0.05). Disruptive bleeding increased hospital costs (incremental increases $3,377–$23,346; p≤ 0.05) and LOS (incremental increases 1.0– 4.9 days; p≤ 0.05) for all five procedures.
Conclusion: The clinical and economic burden of disruptive bleeding despite hemostatic agent use among patients with bariatric, colorectal, spine, THA, and TKA surgery was substantial, highlighting the need for improved surgical bleeding interventions.
Keywords: surgical bleeding, hemostatic agent, health resource utilization, hospital costs, real-world evidence
Background
Surgical bleeding is a common intra- and post-operative surgical complication that varies in severity depending upon the type of surgery and patient, procedural, hospital, and provider characteristics.1,2 Disruptive surgical bleeding occurs when hemorrhage or hematoma complicates the procedure despite the utilization of interventions to control the bleeding.3 More severe surgical bleeding has been shown to be associated with increased mortality, increased healthcare resource utilization (ie, intensive care unit [ICU] admission, longer operating room time, longer length of stay [LOS], and reoperation), and increased healthcare costs.3–7
Hemostatic agents are sometimes used to control surgical bleeding in the United States (US) hospitals in situations where standard methods like direct pressure or suturing are insufficient or impractical. There are numerous hemostatic agents available, each with distinct mechanisms of action, forms, and applications, tailored to various bleeding scenarios in surgical, trauma, and emergency settings. Surgeons’ decisions to use or not use hemostatic agents during surgery depend on several factors, including the procedure, patient characteristics, bleeding type, site accessibility, patient coagulation status, surgeon preference, and economic considerations.
Some patients experience disruptive bleeding despite the use of hemostats.3–5 Previous contemporary studies have evaluated the clinical and economic outcomes associated with disruptive surgical bleeding despite the use of hemostatic agents among patients with coronary artery bypass grafting (CABG), cholecystectomy, cystectomy, hepatectomy, hysterectomy, lung resection, pancreatectomy, peripheral vascular procedures, and valve repair/replacement.4,5 Study findings showed that 16% of patients overall experienced disruptive bleeding (range 1.5% for cholecystectomy to 44.4% for valve repair/replacement).4 Disruptive surgical bleeding was associated with statistically significant increases in ICU admission, ICU days (except CABG), and ventilator use (p≤ 0.05) in procedures for which ICU and ventilator use was not routine. Statistically significant increases in in-hospital mortality, operating room time, LOS (except thoracic), 90-day all-cause inpatient readmission, and total hospital costs (p≤ 0.05) were also observed.
The intent of the current study was to replicate the prior methodology4 and utilize the same dataset to evaluate the clinical and economic outcomes associated with five additional high volume surgical procedures: bariatric surgery, colorectal surgery, spine surgery, and total hip arthroplasty (THA), and total knee arthroplasty (TKA). By keeping the methodology and data source consistent, comparisons across procedures would be facilitated, and the relative clinical and economic impact of disruptive bleeding across 15 surgical procedures could be better discerned.
Methods
Data Source
This retrospective, cross-sectional, real-world data study identified patients undergoing one of 5 procedures in the Premier Healthcare Database (PHD) between January 1-December 31, 2019. The PHD contains hospital discharge-level information on patient demographics, standardized clinical coding, including primary and secondary diagnosis, procedure, and hospital-prescribed medications, length of hospital stay, discharge disposition, facility and provider characteristics, and billed costs from 25% of all hospital admissions throughout the US (more than 1,300 facilities and more than 300 million unique patients since 2012).8 Hospitals included in the dataset are nationally representative based on payer distribution, geographic region, population served (urban/rural), teaching hospital status, and bed size. The New England Institutional Review Board (IRB) determined that the use of the PHD was exempt from broad IRB approval.
Patient Population
Patients were considered for inclusion in the study if they were aged ≥18 years old and had a Current Procedural Terminology (CPT) code or International Classification of Diseases, Tenth Revision (ICD-10) code indicative of one of five procedures of interest between January 1-December 31, 2019: bariatric surgery, colorectal surgery, spine surgery, THA, or TKA. The date of the first procedure was the index date. Patients were only included if their index procedure was performed at a hospital that contributed data to the PHD for at least 90 days post-discharge. Patients were excluded if their index admission occurred through transfer from a different hospital, if their discharge status or sex was missing, or if they had zero or negative billed amounts for total, room and board, and/or supply costs.
The primary analysis evaluated patients with evidence of hemostatic agent use during the index procedure. The use of a hemostatic agent was required in the primary analysis because this group reflects US patients who had all possible bleeding interventions utilized. The intent was to understand whether there is still an unmet need for addressing surgical bleeding even when currently available hemostatic agents were utilized. A sensitivity analysis evaluated all patients with the surgical procedures, whether or not they received a hemostatic agent.
Study Measures
Baseline Characteristics
Patient demographic and clinical characteristics that were evaluated included age, sex, race/ethnicity, marital status, payer category (ie, commercial, Medicare, or Medicaid health insurance), and baseline comorbidity. Baseline comorbidity (ie, comorbid conditions present prior to one of the five procedures of interest) was assessed using the Deyo-Charlson Comorbidity Index (CCI).9–11 The CCI is an aggregate measure of comorbidity associated with chronic disease (eg, heart disease, cancer) and overall health conditions created by using 17 dimensions. Prior research has shown that CCI scores are associated with increased healthcare utilization and greater risk of mortality.9–11
The baseline procedural characteristic that was evaluated was the surgical indication. Baseline provider characteristics that were evaluated included the setting of care (ie, inpatient or outpatient setting), the hospital bed size, whether the hospital was a teaching hospital, the hospital costing type (ie, procedural or ratio of cost-to-charge [RCC] costing), the provider volume for the index procedure type under evaluation, and the hospital US Census region (ie, Northeast, Midwest, South, or West).
Clinical and Economic Outcomes
Consistent with the previous published studies that evaluated the impact of disruptive surgical bleeding,3–5 patients were divided into two mutually exclusive cohorts based on whether they had evidence of disruptive bleeding at index.3 Disruptive bleeding events were identified using: (1) International Classification of Diseases, 10th Revision, Clinical Modification/Procedure Classification System (ICD-10-CM/PCS) codes for hemorrhage/hematoma complicating a procedure; (2) ICD-10-CM/PCS codes for interventions to control bleeding; (3) charges billed for use of hemovac drainage devices; (4) charges billed for use of erythropoietin; (5) charges billed for blood product transfusions; and (6) charges billed for cryoprecipitates, fresh frozen plasma, red blood cells, plasma, platelets, and whole blood. To ensure that the bleeding was not a pre-existing condition, any bleeding-related diagnoses could not be “present on admission”. The codes used for the analyses are available in Table S1.
In-hospital mortality, ICU admission and duration, use of ventilator, time in the operating room, LOS, readmission within 90 days (for any cause), and total hospital costs were the outcomes that were evaluated during the hospital visit.
Statistical Analyses
All study variables and outcomes were analyzed descriptively. Continuous variables were presented in terms of means and standard deviations (SDs) and categorical or binary variables were presented as percentages. Following the bivariate analyses, generalized linear models (GLMs) tailored to the empirical distribution of each outcome were used to adjust for all of the patient, procedure, and hospital/provider characteristics described above and test for statistically significant differences in outcomes (ie, mean operating room time, 90-day all-cause inpatient readmission rates, and inpatient mortality rates). For binary outcomes, a log link and binomial error distribution were used. For count outcomes, a log link and negative binomial error distribution were used. Finally, for total hospital costs, a log link and gamma error distribution were used. Separate models were created for bariatric surgery, colorectal surgery, spine surgery, THA, and TKA. In all analyses, a p-value <0.05 was the threshold by which differences were considered statistically significant. StataSE 16 (StataCorp, College Station, Texas, US) was used for the analyses.
Results
Patient Selection and Attrition
A total of 562,359 patients had at least one hospital discharge for a procedure of interest in 2019 and met the final patient selection criteria for the broad sensitivity analysis population (Table 1). A total of 175,384 had TKA, 165,461 had spine surgery, 109,482 had THA, 61,716 had colorectal surgery, and 50,316 had bariatric surgery. Of the 562,359 patients, 119,994 (21.3%) received a hemostatic agent and were included in the primary analysis. Bleeding agent use was most common among patients who had spine surgery (61.2%), followed by bariatric surgery (13.9%), colorectal surgery (6.7%), THA (2.9%), and TKA (2.5%).
 |
Table 1 Patient Selection |
Among 119,994 patients included in the primary analysis, 101,270 had spine surgery, 7,012 had bariatric surgery, 4,346 had TKA, 4,143 had colorectal surgery, and 3,223 had THA. The overall proportion of patients with disruptive surgical bleeding was 10.8%; the proportion of patients with disruptive surgical bleeding was 5.4% with bariatric surgery, 5.6% with TKA, 11.0% with spine surgery, 11.5% with THA, and 20.0% with colorectal surgery (Figure 1).
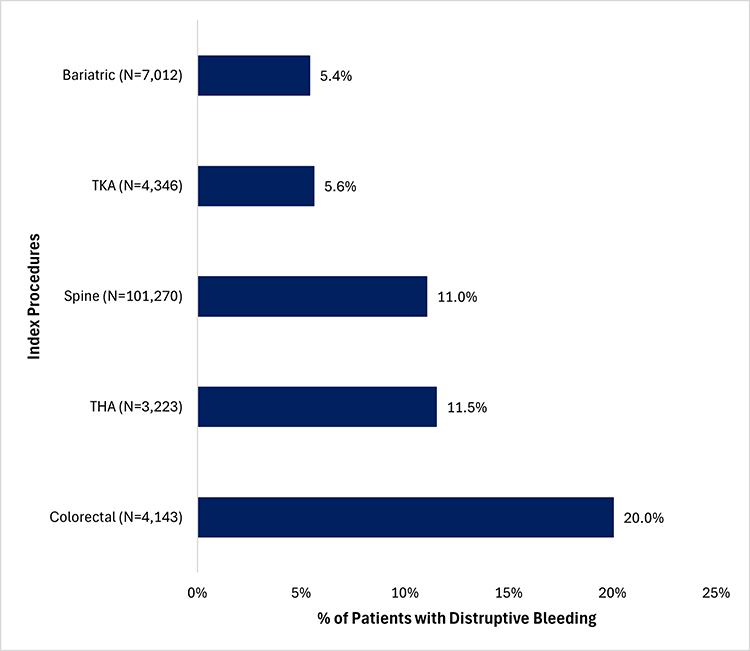 |
Figure 1 Incidence Proportion of Disruptive Bleeding. Abbreviations: THA, total hip arthroplasty; TKA, total knee arthroplasty. |
Baseline Characteristics
Patient baseline demographic and clinical characteristics are presented in Table 2. Patients with disruptive bleeding were older and greater proportions of patients with disruptive bleeding were female, African American, not Hispanic, single, had Medicare insurance, and had higher baseline comorbidity scores. Greater proportions of providers of patients with disruptive bleeding were in inpatient settings, in larger hospitals (ie, bed size and number of providers), in teaching hospitals, in hospitals with RCC costing type, and in the South region of the US (Table 3).
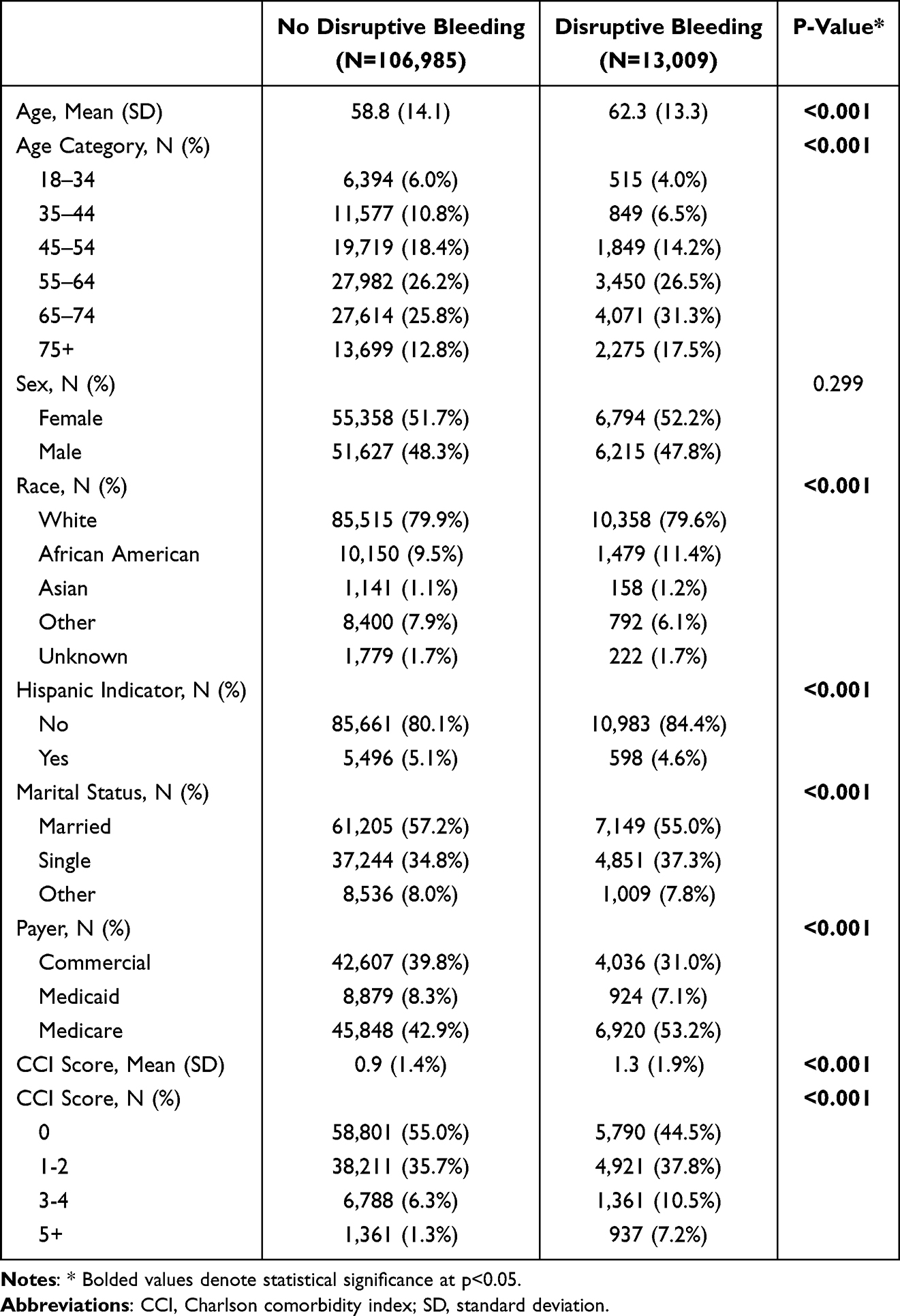 |
Table 2 Baseline Characteristics of Patients with Hemostat Use |
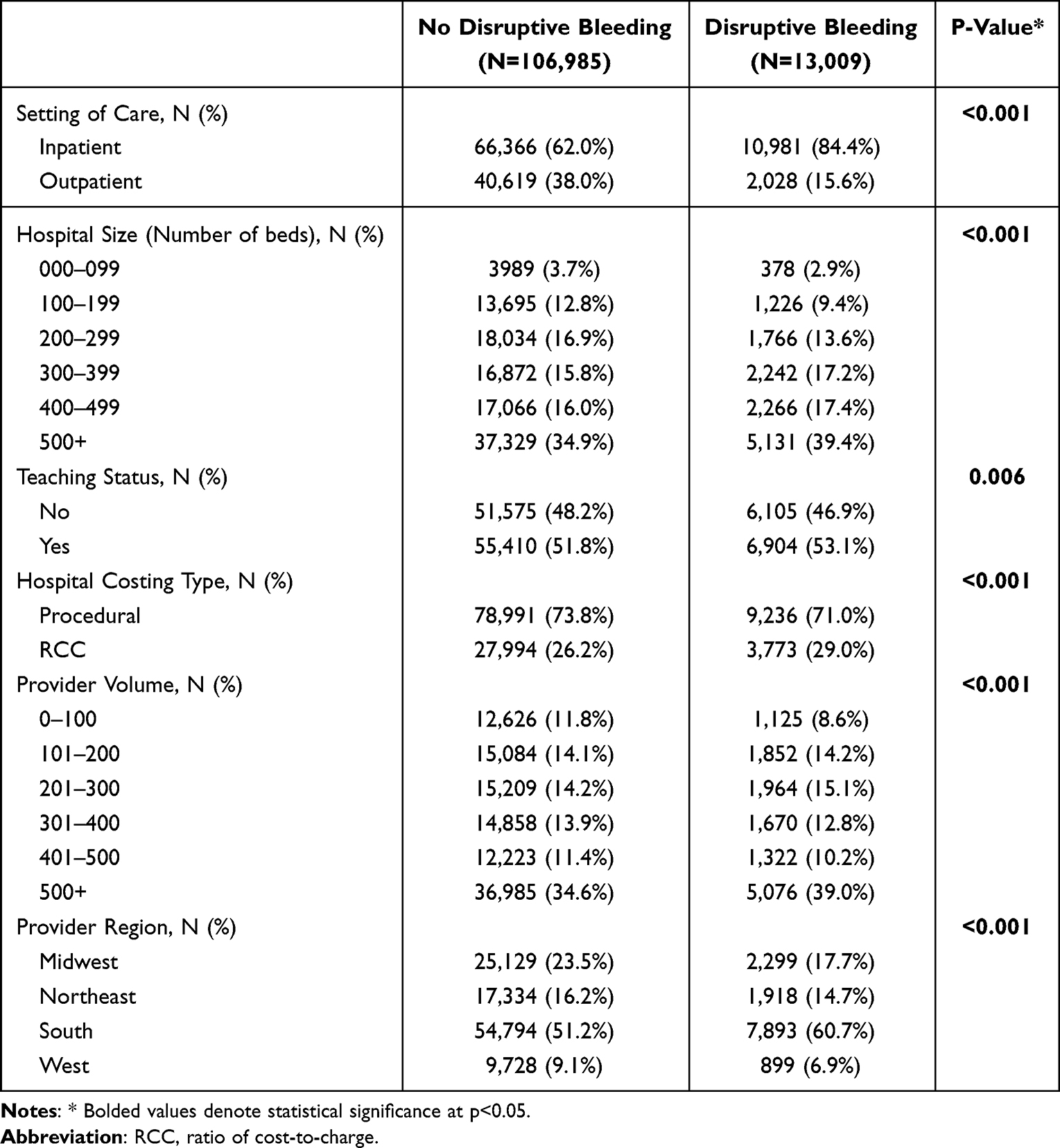 |
Table 3 Baseline Characteristics of Providers of Patients with Hemostat Use |
Adjusted Clinical and Economic Outcomes
As presented in Table 4, disruptive bleeding was associated with significantly longer operating room times for bariatric surgery (incremental increase 48.6 minutes), colorectal surgery (62.4 minutes), and spine surgery (42.3 minutes; p≤0.001); increased risks of 90-day all-cause readmission with bariatric surgery (incremental absolute risk increase 4.1%) and spine surgery (0.7%; both p=0.011); and increased risks of inpatient mortality during the index admission with bariatric surgery (incremental absolute risk increase 55.0%), colorectal surgery (3.3%), spine surgery (0.2%), and THA (2.6%; p≤0.001).
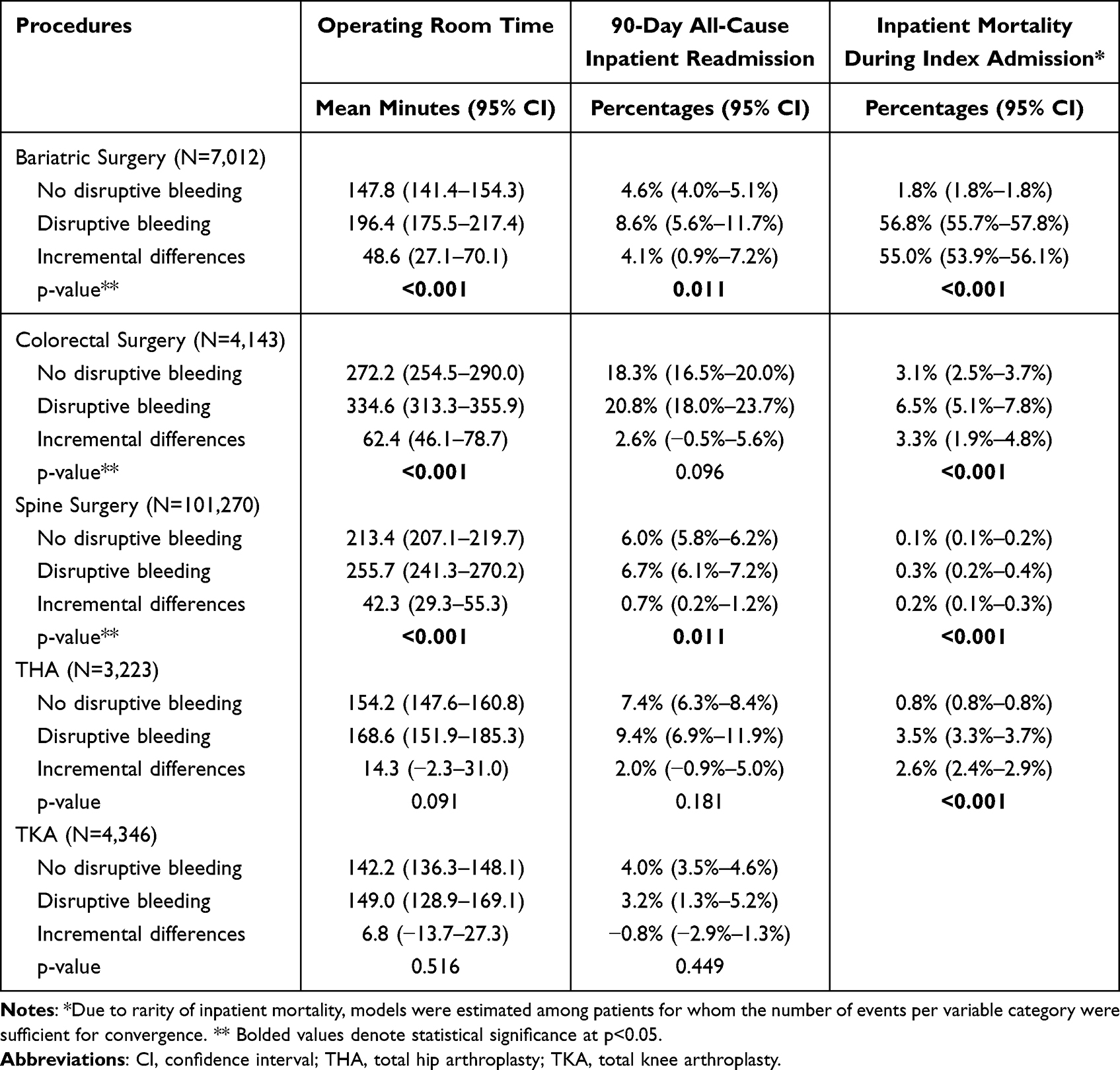 |
Table 4 Association of Disruptive Bleeding with Time in Operating Room, Readmission Within 90 Days for Any Cause, and Inpatient Mortality in Patients with Hemostat Use (Adjusted Results) |
Table 5 presents the adjusted associations of disruptive bleeding with ICU admission and duration and ventilator use. Disruptive bleeding was associated with significantly increased risks of ICU admission for all of the procedures except TKA (incremental absolute risk increase range: 3.0% THA to 21.4% for colorectal surgery; p≤0.05); ICU duration for bariatric, colorectal, and spine surgery (incremental increase range: 0.8 days spine surgery to 2.8 days colorectal surgery; p≤0.001); and increased risks of ventilator use all of the procedures except THA (incremental absolute risk increase range: 3.5% spine surgery to 25.2% TKA; p≤0.05).
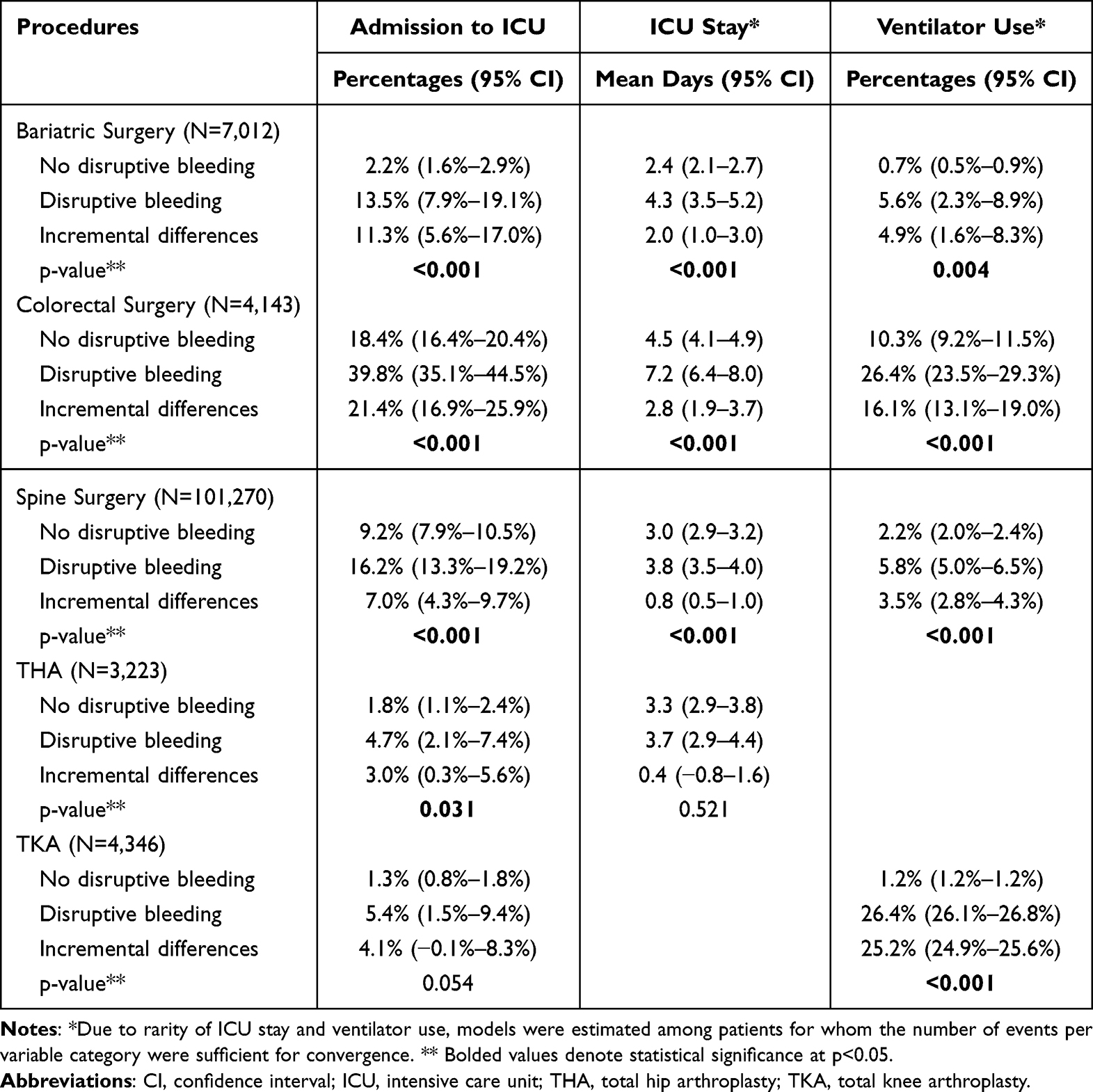 |
Table 5 Association of Disruptive Bleeding with ICU Admission and Duration and Ventilator Use in Patients with Hemostat Use (Adjusted Results) |
Total hospital costs and LOS increased with disruptive bleeding for all five procedures (total hospital cost incremental increase range: $3,377 TKA to $23,346 colorectal surgery; p≤0.05 and LOS incremental increase range: 1.0 days THA and TKA to 4.9 days colorectal surgery; p≤0.05 (Table 6).
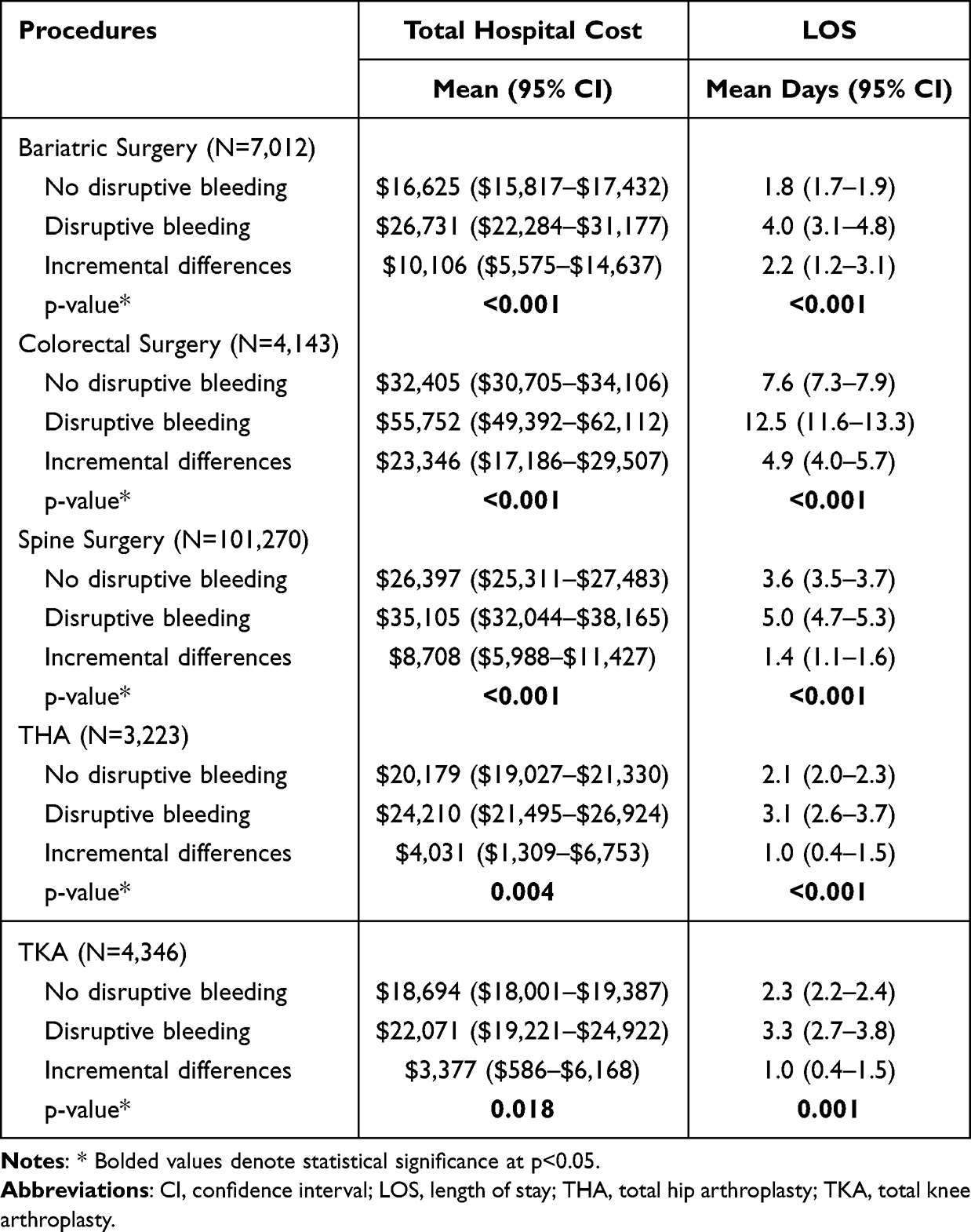 |
Table 6 Association of Disruptive Bleeding with Total Hospital Cost and Index Admission Length of Stay in Patients with Hemostat Use (Adjusted Results) |
Sensitivity Analysis of All Patients, Regardless of Hemostatic Agent Use
A sensitivity analysis evaluating all patients combined, including those with and without hemostatic agent use, was conducted (see Figure S1 and Tables S2–S4). The findings of the sensitivity analysis of the whole population were like the findings for the analyses of the population with hemostatic agent use.
Discussion
This study of nearly 120,000 patients with bariatric surgery, colorectal surgery, spine surgery, THA, and TKA found that the overall incidence proportion of disruptive surgical bleeding despite the use of hemostatic agents was 10.8%. Disruptive surgical bleeding was particularly common among patients with colorectal surgery (20.0%) and was less common among patients with bariatric surgery (5.4%) and TKA (5.6%). The study findings are consistent with the previously published analysis of CABG, cholecystectomy, cystectomy, hepatectomy, hysterectomy, lung resection, pancreatectomy, peripheral vascular procedures, and valve repair/replacement that had an overall incidence proportion of disruptive surgical bleeding of 16%, ranging from 1.5% of patients who underwent cholecystectomy to 44.4% of patients with valve procedures.4 The higher incidence of bleeding with colorectal surgery (eg, colectomy, rectal resection, hemorrhoidectomy) may be because it often involves complex procedures in a highly vascular region of the body, often in patients with predisposing conditions. Similarly, valve procedures have a higher incidence of bleeding because they involve incisions into the myocardium, aorta, or atria, which are prone to bleeding, and because they are typically done in elderly patients with comorbidities.
In alignment with the previously published study findings,4 the current study found that disruptive bleeding was associated with significantly longer operating room times for bariatric, colorectal, and spine surgery (incremental increases 42.3–62.4 minutes), increased risks of 90-day all-cause readmission for bariatric and spine surgery (incremental absolute risk increases 4.1% bariatric, 0.7% spine), and increased risk of inpatient mortality for all of the procedures except TKA (incremental absolute risk increases 0.2–55.0%). The incremental increases in operating room times in this study were greater and the increased risks of readmission in this study were lower overall compared to the previously published study findings.4
The risk of mortality with disruptive bleeding among patients with bariatric surgery observed in this study was particularly concerning (55.0%). Although disruptive surgical bleeding may not be as common among patients with bariatric surgery, the consequences can be devastating. Bariatric surgery patients may face unique risks that amplify the danger of bleeding, including cardiovascular strain from obesity-related conditions12,13 and altered coagulation profiles due to chronic inflammation or non-alcoholic fatty liver disease (NAFLD).14–16
Findings for the risks of ICU admission, ICU days, and risks for ventilator use observed in this study were similar to the previously published study.4 The range of incremental increased hospital costs with disruptive bleeding observed in this study was greater compared to the prior analysis due to the high cost of patients with disruptive bleeding from colorectal surgery ($23,346).
The findings of the current study are also mostly consistent with the previous study by Corral et al,3 which evaluated eight major surgeries deemed by surgeons to be commonly associated with major bleeding: cardiac revascularization, cardiac valve surgery, cholecystectomy, cystectomy, pancreatic, partial hepatic resection, pulmonary, and radical abdominal hysterectomy. The study used the same definition of bleeding as the current study; however, the surgeries were performed via an open surgical approach, and all of the surgeries were performed in calendar year 2012. Although their findings of significantly higher hospital costs and worse clinical outcomes with disruptive bleeding were consistent with the current study, their observed prevalences of disruptive bleeding were higher, ranging from 32% to 68%. Changes in practice patterns, including the increased availability of hemostatic agents and a shift towards minimally invasive surgeries (MIS),17–19 necessitated these more contemporary analyses.
A strength of this study is that it provided clinically and economically meaningful data originating from clinical practice for large numbers of patients. This type of real-world evidence may assist consumers, clinicians, purchasers, and policymakers in making more informed decisions and expand adoption of or optimization of topical hemostatic agents (TAHs) to potentially lower overall surgical cost by avoiding disruptive bleeding.20,21 Additionally, this study included comprehensive variables around patient, procedure, and provider characteristics in adjusting for baseline differences. Also, by keeping the methodology and data source consistent to the previously published study of CABG, cholecystectomy, cystectomy, hepatectomy, hysterectomy, lung resection, pancreatectomy, peripheral vascular procedures, and valve repair/replacement, comparisons across procedures could be facilitated, and the relative clinical and economic impact of disruptive bleeding across 15 total surgical procedures could be discerned.
However, there are limitations associated with retrospective observational and database studies that apply to this study. The PHD data were not collected specifically for research purposes; patient selection and covariate and clinical and economic outcome measurement was based on PHD diagnosis and procedure codes and could be affected by inaccuracies, temporal changes, biases, and errors.22,23 The study was designed with a maximum of 90-day follow-up and hence the clinical and economic outcomes associated with disruptive surgical bleeding despite the use of a hemostatic agent over longer periods of time are not known. The retrospective, observational study design and administrative data source make it difficult to draw causal inferences; hence, the study did not enable the evaluation of what bleeding or bleeding complications are expected, the impact of specific hemostatic agents, or the cost-effectiveness of hemostatic agent use. Another limitation is that the findings from the PHD database may not be generalizable to all hospitalized patients with the procedures of interest, particularly to patients receiving care in other countries. Nonetheless, the findings of this study contribute to the current body of evidence on the clinical and economic outcomes associated with disruptive surgical bleeding despite the use of hemostatic agents among patients with bariatric surgery, colorectal surgery, spine surgery, THA, and TKA.
Conclusions
This study of nearly 120,000 patients with bariatric surgery, colorectal surgery, spine surgery, THA, and TKA found that more than one in ten patients experienced disruptive surgical bleeding despite the use of hemostatic agents. Disruptive surgical bleeding was more common among patients with colorectal surgery (20.0%) and was less common among patients with bariatric surgery (5.4%). However, the risk of mortality with disruptive bleeding despite the use of hemostatic agents among patients with bariatric surgery in this study was 55.0%. Study findings showed that the clinical and economic burden of disruptive bleeding despite the use of hemostatic agents among these patients was substantial, with the incremental hospital cost of bleeding with colorectal surgery reaching $23,346. These findings highlight the need for improved surgical bleeding interventions and optimization of the TAH used. Continued research and analyses of bleeding interventions are required to assess their overall clinical and economic impact and efficiencies.
Ethics Approval and Consent to Participate
The use of Premier Healthcare Database was reviewed by the New England Institutional Review Board (IRB) and was determined to be exempt from broad IRB approval, as this research project did not involve human subject research and used data from an anonymous, de-identified, administrative claims database compliant with the Health Insurance Portability and Accountability Act of 1996.
Funding
This study was funded by Johnson & Johnson.
Disclosure
SSJ, AK and WAD III are employees and stockholders of Johnson & Johnson. PNV is an employee of Mu Sigma. MA and PNV provided data and analysis support under contract to Johnson & Johnson. The authors report no other conflicts of interest in this work.
References
1. Thomas AB, Shammas RL, Orr J, et al. An Assessment of Bleeding Complications Necessitating Blood Transfusion across Inpatient Plastic Surgery Procedures: a Nationwide Analysis Using the National Surgical Quality Improvement Program Database. Plast Reconstr Surg. 2019;143(5):1109e–1117e. doi:10.1097/prs.0000000000005537
2. Javed H, Olanrewaju OA, Ansah Owusu F, et al. Challenges and Solutions in Postoperative Complications: a Narrative Review in General Surgery. Cureus. 2023;15(12):e50942. doi:10.7759/cureus.50942
3. Corral M, Ferko N, Hollmann S, Broder MS, Chang E. Health and economic outcomes associated with uncontrolled surgical bleeding: a retrospective analysis of the Premier Perspectives Database. Clinicoecon Outcomes Res. 2015;7:409–421. doi:10.2147/ceor.S86369
4. Johnston SS, Afolabi M, Tewari P, Danker W. Clinical and Economic Burden Associated with Disruptive Surgical Bleeding: a Retrospective Database Analysis. Clinicoecon Outcomes Res. 2023;15:535–547. doi:10.2147/ceor.S411778
5. Afolabi M, Johnston SS, Tewari P, Danker WA. Increasing Incremental Burden of Surgical Bleeding Associated with Multiple Comorbidities as Measured by the Elixhauser Comorbidity Index: a Retrospective Database Analysis. Med Devices. 2023;16:237–249. doi:10.2147/mder.S434779
6. Johnston SS, Jamous N, Mistry S, et al. Association of In-Hospital Surgical Bleeding Events with Prolonged Hospital Length of Stay, Days Spent in Critical Care, Complications, and Mortality: a Retrospective Cohort Study Among Patients Undergoing Neoplasm-Directed Surgeries in English Hospitals. Clinicoecon Outcomes Res. 2021;13:19–29. doi:10.2147/ceor.S287970
7. Al-Attar N, Johnston S, Jamous N, et al. Impact of bleeding complications on length of stay and critical care utilization in cardiac surgery patients in England. J Cardiothorac Surg. 2019;14(1):64. doi:10.1186/s13019-019-0881-3
8. Premier I. Premier PINC AI™ Healthcare Database (PHD). Available from: https://offers.pinc-com/data?utm_source=google&utm_medium=paid_search&gad_source=1&gclid=Cj0KCQjwm7q-BhDRARIsACD6-fXkX5zX5sK8nYSBevtLAoqZFl-TUS7RyDAVmtYf9DTeajnfxy4fDL8aAkHcEALw_wcB.
9. Quan H, Li B, Couris CM, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–682. doi:10.1093/aje/kwq433
10. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
11. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
12. Aminian A, Brethauer SA, Kirwan JP, Kashyap SR, Burguera B, Schauer PR. How safe is metabolic/diabetes surgery? Diabetes Obes Metab. 2015;17(2):198–201. doi:10.1111/dom.12405
13. Poirier P, Cornier MA, Mazzone T, et al. Bariatric surgery and cardiovascular risk factors: a scientific statement from the American Heart Association. Circulation. 2011;123(15):1683–1701. doi:10.1161/CIR.0b013e3182149099
14. Samad F, Ruf W. Inflammation, obesity, and thrombosis. Blood. 2013;122(20):3415–3422. doi:10.1182/blood-2013-05-427708
15. Bladbjerg EM, Stolberg CR, Juhl CB. Effects of Obesity Surgery on Blood Coagulation and Fibrinolysis: a Literature Review. Thromb Haemost. 2020;120(4):579–591. doi:10.1055/s-0040-1702224
16. Targher G, Day CP, Bonora E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med. 2010;363(14):1341–1350. doi:10.1056/NEJMra0912063
17. Akhtar-Danseh GG, Akhtar-Danesh N, Finley C. Uptake and survival effects of minimally invasive surgery for lung cancer: a population-based study. Eur J Surg Oncol. 2021;47(7):1791–1796. doi:10.1016/j.ejso.2021.01.002
18. Williams AD, Sun T, Kakade S, Wong SL, Shulman LN, Carp NZ. Comparison of open and minimally invasive approaches to colon cancer resection in compliance with 12 regional lymph node harvest quality measure. J Surg Oncol. 2021;123(4):986–996. doi:10.1002/jso.26298
19. Unruh KR, Bastawrous AL, Bernier GV, et al. Evaluating the Regional Uptake of Minimally Invasive Colorectal Surgery: a Report from the Surgical Care Outcomes Assessment Program. J Gastrointest Surg. 2021;25(9):2387–2397. doi:10.1007/s11605-020-04875-1
20. Dreyer NA, Schneeweiss S, McNeil BJ, et al. GRACE principles: recognizing high-quality observational studies of comparative effectiveness. Am J Manag Care. 2010;16(6):467–471.
21. Schneeweiss S, Gagne JJ, Glynn RJ, Ruhl M, Rassen JA. Assessing the comparative effectiveness of newly marketed medications: methodological challenges and implications for drug development. Clin Pharmacol Ther. 2011;90(6):777–790. doi:10.1038/clpt.2011.235
22. Patel AA, Singh K, Nunley RM, Minhas SV. Administrative Databases in Orthopaedic Research: pearls and Pitfalls of Big Data. J Am Acad Orthop Surg. 2016;24(3):172–179. doi:10.5435/jaaos-d-13-00009
23. Bohl DD, Singh K, Grauer JN. Nationwide Databases in Orthopaedic Surgery Research. J Am Acad Orthop Surg. 2016;24(10):673–682. doi:10.5435/jaaos-d-15-00217
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical and Economic Burden Associated with Disruptive Surgical Bleeding: A Retrospective Database Analysis
Johnston SS, Afolabi M, Tewari P, Danker W
ClinicoEconomics and Outcomes Research 2023, 15:535-547
Published Date: 3 July 2023