")
Back to Journals » International Journal of General Medicine » Volume 15
Retrospective Analysis of Sagittal Balance Parameters and Clinical Efficacy After Short-Segment Anterior Cervical Spine Surgery with Different Fusion Devices
Authors Wei Z , Zhang Y, Yang S, Cai C, Ye J, Qiu H, Hu X, Qu Y, Wen X, Chu T
Received 3 October 2021
Accepted for publication 11 March 2022
Published 22 March 2022 Volume 2022:15 Pages 3237—3246
DOI https://doi.org/10.2147/IJGM.S340877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Zihan Wei, Ying Zhang, Sizhen Yang, Chenhui Cai, Jiawen Ye, Hao Qiu, Xu Hu, Yiyun Qu, Xuan Wen, Tongwei Chu
Department of Orthopedics, Xinqiao Hospital of Chongqing, Second Affiliated Hospital of Army Medical University, Chongqing, 400037, People’s Republic of China
Correspondence: Tongwei Chu, Department of Orthopedics, Xinqiao Hospital of Chongqing, Second Affiliated Hospital of Army Medical University, Chongqing, 400037, People’s Republic of China, Tel/Fax +8613708388336, Email [email protected]
Objective: To compare the cervical sagittal balance parameters and clinical efficacy of three fusion devices after short-segment anterior cervical discectomy and fusion.
Patients and Methods: Retrospectively analyzed 516 patients with cervical spondylosis who underwent surgery at our hospital from May 2013 to May 2019. All patients had complete data and were divided into three groups according to the selected fusion cage. Neck and upper limb pain were assessed by the visual analog scale (VAS) score. Neurological function was evaluated by the modified Japanese Orthopedics Society (mJOA) score. Also, the curvature of the cervical spine and the occurrence of dysphagia were observed.
Results: There were no significant differences in the general information, thoracic inlet angle, T1 slope, or surgical data among the groups (p> 0.05). There were significant differences in the scores between pre- and postoperatively in the different groups (p< 0.05). There were no significant differences in the C2-C7 Cobb angle or C2-C7 sagittal vertebral axis before the operation among the groups (p> 0.05). There was a significant difference in the correction and loss of correction among the groups postoperatively and on follow-up (p> 0.05). Dysphagia was less likely in the Zero-P VA fusion group than in the other two groups.
Conclusion: Different fusion instruments can relieve the symptoms. In the Prodisc-C Vivo group, no significant improvement in cervical sagittal balance was achieved. A good effect on improving sagittal balance was observed in both the Zero-P VA fusion and Skyline anterior cervical titanium plate groups, but a better effect on preventing dysphagia was observed in the Zero-PVA fusion group.
Keywords: retrospective analyze, cervical spondylosis, anterior cervical discectomy and fusion, cervical sagittal balance parameters, fusion devices
Introduction
Cervical spondylosis, as a common degenerative cervical vertebra disease in middle-aged and elderly people, can result in the stimulation or compression of adjacent spinal cord tissue, blood vessels, nerves, etc., to produce neck shoulder activity limitations, soreness, numbness, weakness, hyperalgesia, paresthesia, four limbs and other clinical symptoms, seriously impacting the patient’s quality of life.1 Anterior cervical discectomy and fusion (ACDF) can adequately resolve the compression of spinal nerve roots, adjust the height of the intervertebral space and restore the physiological curvature of cervical vertebrae and is a classic surgical method for the treatment of cervical spondylosis.2 Whether using a traditional anterior cervical titanium plate as an implant, an artificial cervical disc fusion device, or the currently popular Zero-P VA anterior cervical interbody fusion and fixation system, all equipment has its own advantages and disadvantages.3 However, there has been little research on changes in short-segment cervical sagittal balance parameter changes after such procedures until now. In this paper, sagittal balance parameters after ACDF with three fixed materials were evaluated to identify the optimal method for the surgical treatment of short-segment cervical spondylosis for patients to achieve improved cervical function, sagittal balance after forward degeneration of adjacent vertebral bodies, and balance of the whole spine.
Patients and Methods
Subjects
This study retrospectively analyzed a total of 516 patients with short-segment cervical spondylosis who underwent ACDF surgery at our hospital from May 2013 to May 2019. All patients had complete preoperative and follow-up imaging data and were divided into three groups according to the selected fusion cage, patients were given detailed pre-operative communication based on Chinese Health Insurance policy and their need for cervical mobility. Patients were then divided into groups according to which type of fusion device they chose, including 182 cases in the Skyline anterior cervical titanium plate group, 163 cases in the Prodisc-C Vivo artificial cervical disc group and 171 cases in the Zero-P VA anterior cervical interbody fusion and fixation system group. All procedures were performed by one surgeon (Tongwei Chu). The protocol was approved by the Medical Ethics Committee of the Second Affiliated Hospital Army Military Medical University. We obey the principles of the 1983 Declaration of Helsinki. And all patients had obtained sufficient informed consent and signed an informed consent form.
Research Methods
Inclusion Criteria
① Obvious nerve root and/or spinal symptoms, such as neck and shoulder discomfort, paresthesia, radiating upper limb pain, gait instability, and walking difficulties, as well as imaging features conforming to the diagnostic features of cervical spondylosis; ② short-segment (<3 segments) cervical spondylosis; ③ inefficacy of conservative treatment, with indications for surgery; and ④ age between 18 and 75 years.
Exclusion Criteria
① A history of severe cervical trauma and surgery; ② poor general physical condition or absolute contraindication to surgery such as cervical vertebra tumor, cervical vertebra space infection and so on; ③ concomitant demyelinating disease, Guillain-Barre syndrome or other neurological disease; ④ concomitant mental disease or inability to cooperate; ⑤ preoperative complications, such as dysphagia; and ⑥ incomplete clinical and follow-up data.
Observation Indexes
① Statistical analysis of patient age, sex, body mass index (BMI), operation time, intraoperative blood loss and other basic information was performed. The Bazaz dysphagia score was evaluated at the last postoperative follow-up.
② Functional recovery of all patients was evaluated preoperatively and postoperatively. Neck and upper limb pain were assessed by the visual analog scale (VAS) score. Neurological function was evaluated preoperatively and postoperatively using the modified Japanese Orthopedic Society (mJOA) score.
③ Imaging observation was performed. Anteroposterior and lateral images of the cervical vertebrae were taken preoperatively, postoperatively and at the final follow-up, and the cervical curvature, fusion apparatus location, and bone graft fusion were observed. The sagittal balance of the cervical spine was evaluated by the C2-C7 Cobb angle (the angle between the vertical line of the lower endplate of C2 and the vertical line of the lower endplate of C7), C2-C7 sagittal vertebral axis (SVA, the horizontal distance between the geometric central plumb line of the C2 vertebral body and the posterior angle of the upper endplate of C7), thoracic inlet angle (TIA, the angle between the T1 midline and the T1 midpoint to the upper of the sternal border), and T1 slope (T1S, the angle between the upper edge of T1 and the horizontal plane). All X-rays are standard standing films, taken by a professional radiologist. (Figure 1).
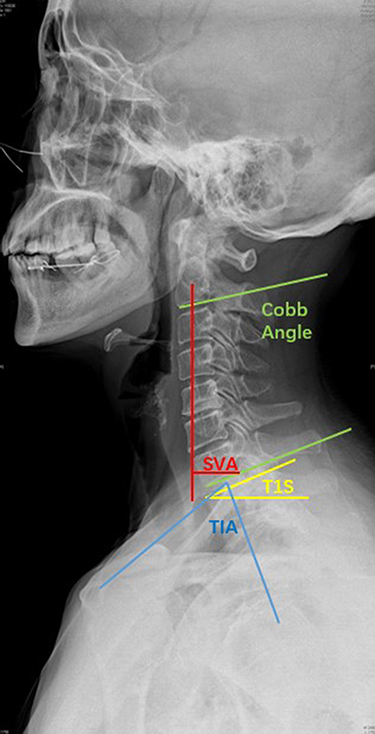 |
Figure 1 The sagittal balance of the cervical spine was evaluated by the C2-C7 Cobb angle (the angle between the vertical line of the lower endplate of C2 and the vertical line of the lower endplate of C7), C2-C7 sagittal vertebral axis (SVA, the horizontal distance between the geometric central plumb line of the C2 vertebral body and the posterior angle of the upper endplate of C7), thoracic inlet angle (TIA, the angle between the T1 midline and the T1 midpoint to the upper of the sternal border), and T1 slope (T1S, the angle between the upper edge of T1 and the horizontal plane). |
Statistical Methods
SPSS 21 was used for statistical analysis. Measurement data are presented as the mean ± standard deviation or median (interquartile range) and were analyzed by ANOVA or the rank-sum test. The measurement data are expressed as the number of cases and were analyzed by the chi-square test. P<0.05 was considered statistically significant.
Results
Comparison of Basic Patient Information Among the Groups
According to the selected fusion cage, the patients were divided into three groups: the Skyline anterior cervical titanium plate group (n=182), the Prodisc-C Vivo artificial cervical disc group (n=163), and the Zero-P VA anterior cervical interbody fusion and fixation system group (n=171). ACDF was performed in all three groups. There were no statistically significant differences in sex, age or BMI among the three groups (p>0.05), and the baseline conditions of the three groups were basically the same (Table 1).
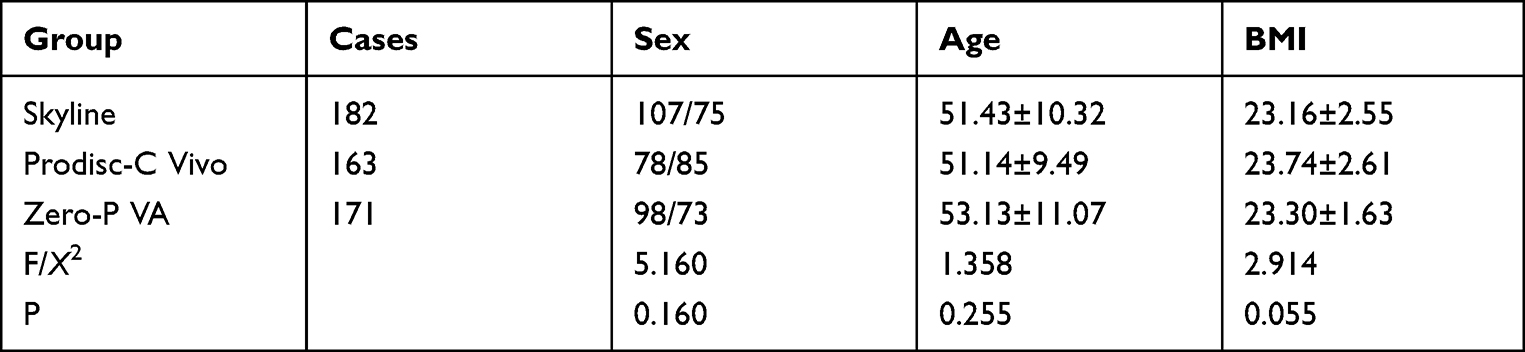 |
Table 1 Comparison of General Data Among the Three Groups |
Comparison of Operative Information Among the Groups
There was no significant difference in the operation time or blood loss among the different fusion segments groups (p>0.05) (Table 2).
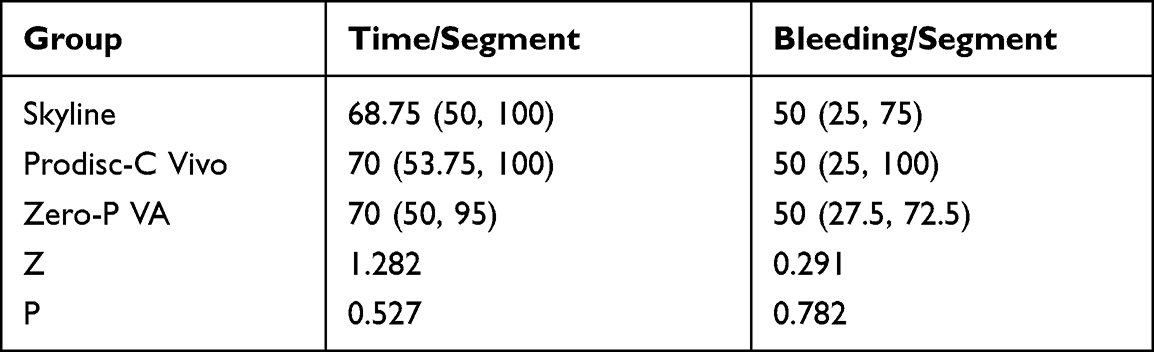 |
Table 2 Comparison of Operation Time and Blood Loss Among the Three Groups |
Comparison of mJOA and VAS Scores Among the Three Groups
The mJOA and VAS scores in each group were compared, and there was no statistical significance either before or after surgery (p>0.05). However, the postoperative scores of each group were significantly different from those before the operation (p<0.05) (Table 3).
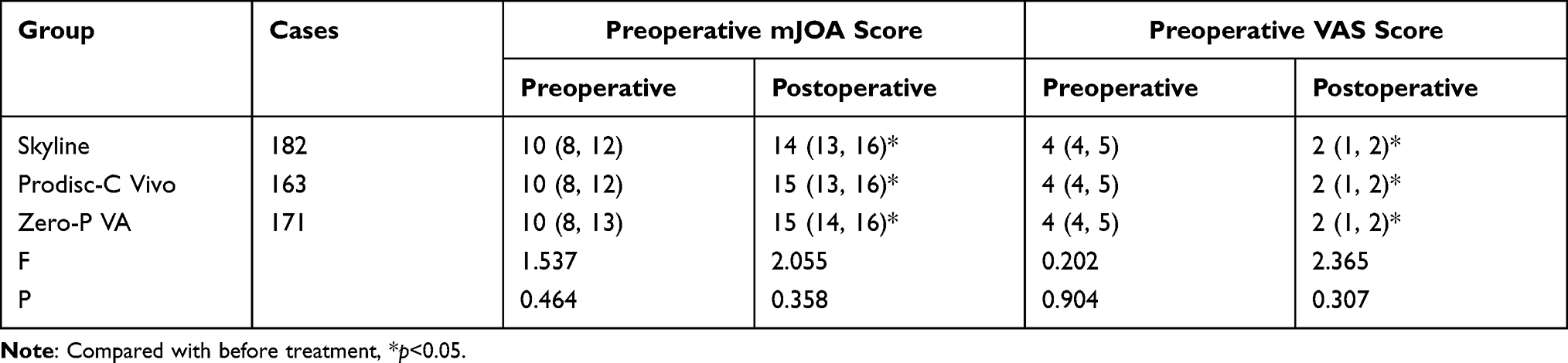 |
Table 3 Comparison of mJOA and VAS Scores Among the Three Groups |
Comparison of C2-C7 Cobb Angle and C2-C7 SVA Among the Different Groups
There were no significant differences in the C2-C7 Cobb angle or C2-C7 SVA among the groups before surgery (p>0.05). A significant difference was observed in the correction and loss of correction among the groups postoperatively and on follow-up (p<0.05). Within these groups, greater correction was clearly achieved in the low-notch Zero-P VA group than in the Skyline and Prodisc-C Vivo groups. Meanwhile, the loss of correction in these groups showed obvious differences; the values in the Zero-P VA and Skyline groups were smaller than that in the artificial disc group. Among all the groups, the Zero-P VA group showed the best correction. At the last follow-up, the Zero-P VA and Skyline groups showed significantly less loss of correction than the Prodisc-C Vivo group. The C2-C7 SVA and C2-C7 Cobb angle showed similar trends, and the greatest C2-C7 SVA correction was achieved in the Zero-P VA group among all the groups. The loss of C2-C7 SVA correction was similar in the Skyline and Zero-P VA groups and better than that in the Prodisc-C Vivo group (Tables 4 and 5).
 |
Table 4 Comparison of C2-C7 Cobb Angle (°) Among the Three Groups Before and After the Operation and at the Last Follow-Up |
 |
Table 5 Comparison of SVA (mm) Among the Three Groups Before and After Surgery and at the Last Follow-Up |
Comparison of the TIA and T1S Among the Different Groups
The TIA and T1S were compared among the groups at three time points, ie, before surgery, after surgery and at the last follow-up, with no significant differences (p>0.05) (Table 6).
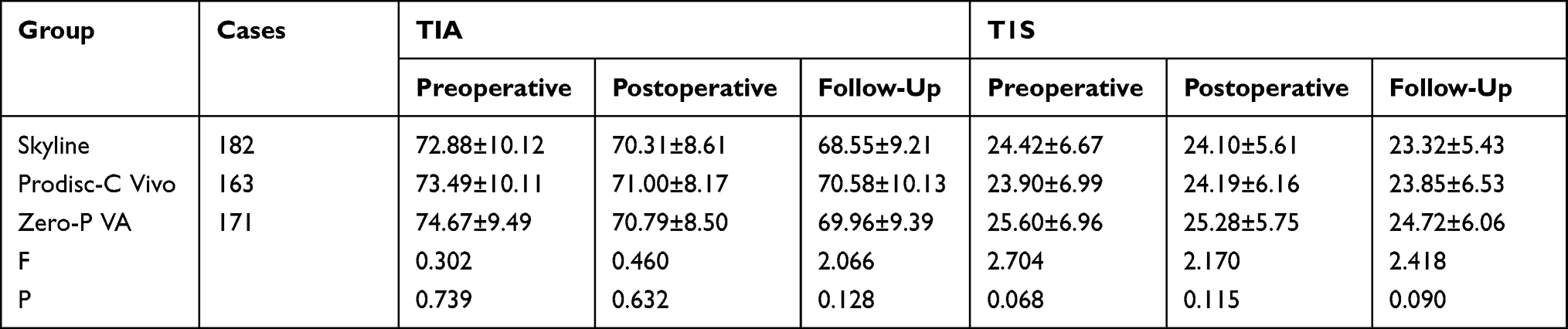 |
Table 6 Comparison of Inclination the TIA and T1S Before Surgery, After Surgery and During Follow-Up |
Occurrence of Dysphagia in Different Fusion Cage Groups
In the Zero-P VA interbody fusion group, 9 patients had mild dysphagia and 1 had moderate dysphagia; dysphagia was more common in the other two groups (Table 7).
 |
Table 7 Comparison of Dysphagia Symptoms Among the Three Groups |
Typical Case in the Skyline Group
The patient was diagnosed with cervical spondylosis. (A/B/C) Anterolateral view of the cervical spine preoperatively, postoperatively, and at the last follow-up. Before the surgery, the patient had a smaller C2-C7 Cobb angle and a larger C2-C7 SVA. After the operation, the C2-C7 Cobb angle and the C2-C7 SVA were restored immediately, and pain and neurological symptoms were significantly relieved. Meanwhile, slight loss of C2-C7 Cobb angle and C2-C7 SVA correct was observed at the last follow-up (Figure 2).
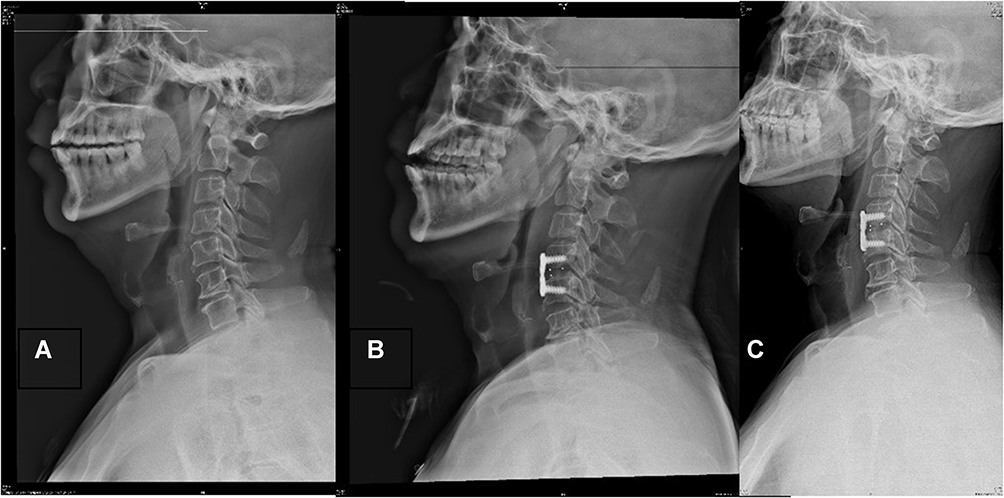 |
Figure 2 Typical case in the Skyline group. The patient was diagnosed with cervical spondylosis. (A–C) Anterolateral view of the cervical spine preoperatively, postoperatively, and at the last follow-up. Before the surgery, the patient had a smaller C2-C7 Cobb angle and a larger C2-C7 SVA. After the operation, the C2-C7 Cobb angle and the C2-C7 SVA were restored immediately, and pain and neurological symptoms were significantly relieved. Meanwhile, slight loss of C2-C7 Cobb angle and C2-C7 SVA correct was observed at the last follow-up. |
Typical Case in the Prodisc-C Vivo Group
The patient was diagnosed with cervical spondylosis. (A/B/C) Anterolateral view of the cervical spine preoperatively, postoperatively, and at the last follow-up. While there was no significant change in the sagittal balance of the cervical spine between before and after the operation, the neurological symptoms and pain were mitigated postoperatively (Figure 3).
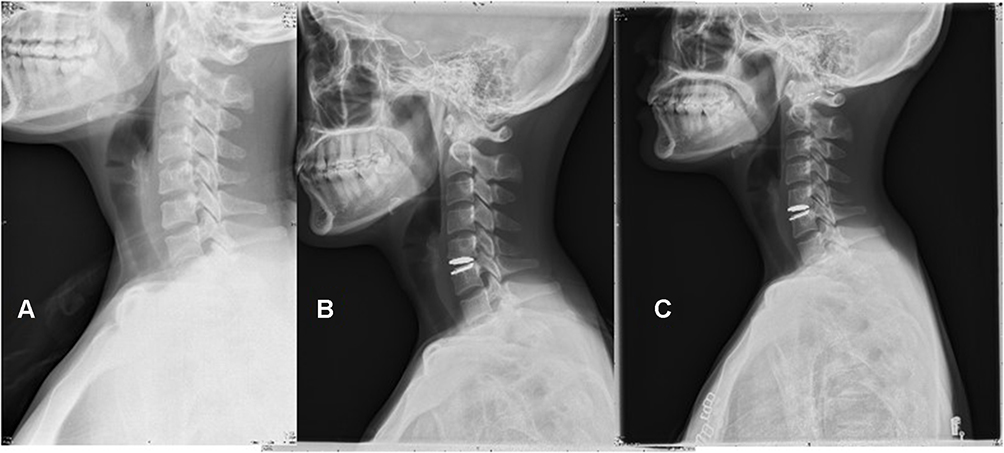 |
Figure 3 Typical case in the Prodisc-C Vivo group. The patient was diagnosed with cervical spondylosis. (A–C) Anterolateral view of the cervical spine preoperatively, postoperatively, and at the last follow-up. While there was no significant change in the sagittal balance of the cervical spine between before and after the operation, the neurological symptoms and pain were mitigated postoperatively. |
Typical Case in the Zero-P VA Group
The patient was diagnosed with cervical spondylotic radiculopathy. (A/B/C) Anterolateral view of the cervical spine preoperatively, postoperatively, and at the last follow-up. The preoperative SVA was large, and the postoperative SVA was significantly reduced. There was no significant change in other normal cervical spine parameters after the operation, and the cervical sagittal curvature was maintained over the long term (Figure 4).
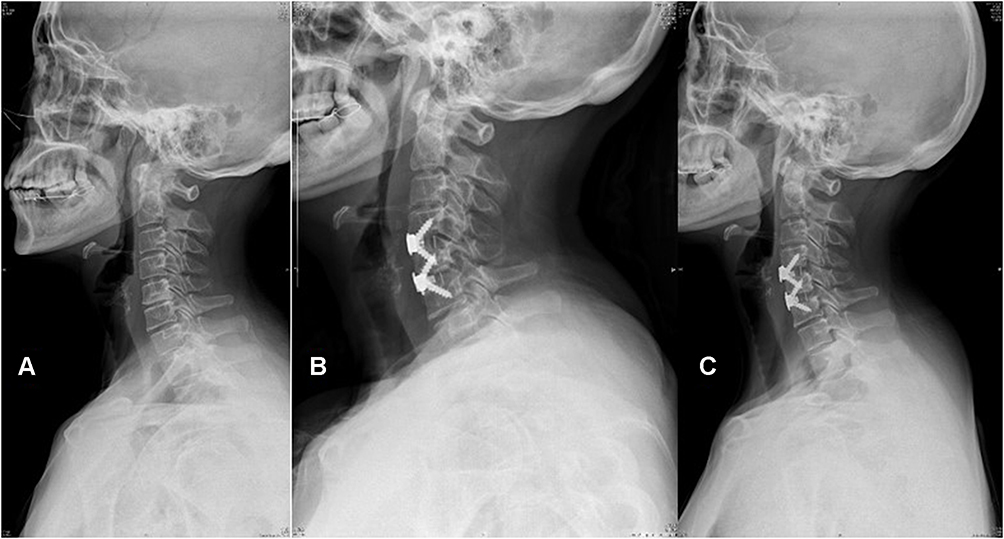 |
Figure 4 Typical case in the Zero-P VA group. The patient was diagnosed with cervical spondylotic radiculopathy. (A–C) Anterolateral view of the cervical spine preoperatively, postoperatively, and at the last follow-up. The preoperative SVA was large, and the postoperative SVA was significantly reduced. There was no significant change in other normal cervical spine parameters after the operation, and the cervical sagittal curvature was maintained over the long term. |
Discussion
ACDF was first proposed by Smith and Robinson in 1955 and has become the gold standard for the treatment of cervical spondylosis due to its satisfactory efficacy.4 To avoid the complications of autologous bone grafting, various interbody fusion cages have been gradually applied in ACDF as an alternative to autologous bone grafting. A traditional anterior titanium plate combined with an interbody fusion device can significantly improve the rate of implant subsidence, significantly reduce the incidence of secondary kyphosis, and reduce the impact on adjacent segments.5 Such plates can also improve the curvature of the cervical spine, provide immediate cervical stability during placement of the interbody bone graft, and significantly increase the interbody fusion rate.5,6 However, the combination of a titanium plate and cage can cause postoperative symptoms such as dysphagia and foreign body sensation, which affect quality of life. Therefore, an improved anterior cervical approach and bridge-shaped locking fusion method were developed. While providing sufficient stability, it avoids friction with surrounding soft tissues and reduces the incidence of postoperative foreign body sensation and swallowing disorders.7 At the same time, artificial disc replacement can retain the mobility of the replaced segment relative to that after ACDF and does not cause increased stress in adjacent segments after cervical fusion.8 This approach can retain the overall range of motion (ROM) of the cervical spine and the ROM of replaced segments, and patients have a greater chance of obtaining good segmental ROM in the long term postoperatively.9 Some studies have also demonstrated that artificial disc replacement can delay the rate of degeneration of other vertebral segments in patients.10 In conclusion, all kinds of fusion devices have unique advantages, but there has been little research on the sagittal balance of the cervical spine after ACDF.
In this study, we investigated the effects of different fusion devices on the postoperative sagittal balance parameters of the cervical spine. Regarding basic patient information, there were no significant differences in sex, age or BMI among patients in different groups, and the baseline characteristics of patients in each group were consistent and comparable. The operation time and the amount of blood loss were analyzed, and there were no statistically significant differences among the groups (p>0.05). The VAS pain score and 17 points of the Japanese Orthopaedic Society (mJOA) score were used to further analyze the three groups, and there were no significant differences in the two scores before surgery among the three groups (p>0.05), but the scores in the three groups were significantly improved postoperatively compared with preoperatively, indicating that the three surgical methods can all relieve compression of the spinal cord or nerve root and relieve symptoms, which is similar to the results of previous studies.11–13 Thus, the normal physiological curve of the cervical spine needs to be studied, especially in patients with cervical spondylosis. Improvement in cervical sagittal balance after surgery is accompanied by a reduction in neck pain14 Physiological lordosis is also closely related to degeneration of the cervical spine and affects the stability of the ligamentum flavum and the posterior longitudinal ligament.15 The present study shows that the C2-C7 Cobb angle in all three groups was significantly increased and that the C2-C7 SVA was decreased after surgery compared with that before surgery, indicating that correction of the cervical curvature of the operative segment could to achieved to some degree, which is consistent with a study by Alhashash.16 We also found a significant difference in the C2-C7 Cobb angle correction among the three groups (p<0.05). The correction was clearly greater in the Zero-P VA group than in the Skyline and Prodisc-C Vivo groups, indicating that the Zero-P VA device could be more conducive to restoring the cervical curvature of the operative segment than the other devices. We also noted that at the last follow-up, there was a significant difference in the loss of correction among these groups (p<0.05), as the value was smaller in the Zero-P VA and Skyline groups than in the artificial disc group. Regarding the C2-C7 SVA, significant differences in the correction and loss of correction were observed among the three groups (p<0.05). The greatest correction was achieved in the Zero-P VA group. The loss of C2-C7 SVA correction was similar in the Skyline and Zero-P VA groups and better than that in the Prodisc-C Vivo group. In summary, the Zero-P VA and Skyline devices can provide great correction after ACDF with relatively little loss of correction on long-term follow-up. The sagittal balance of the cervical spine is influenced by the C2-C7 Cobb and C2-C7 SVA; additionally, the TIA and T1S can also affect the curvature of the cervical vertebrae. Cervical lordosis is influenced by thoracic kyphosis; thus, the TIA and T1S have also been introduced to evaluate the stability of the cervical spine.17 Recent research has suggested that a high T1S is a potential risk factor for the development of MC due to impaired sagittal balance, especially in the C5-C6 cervical segment.18 Therefore, in this study, we performed further analysis of the preoperative, postoperative and follow-up TIA and T1S. The TIA and T1S in the groups showed no significant differences (p>0.05) at any time point. We believe this proves that for individuals, these two indicators are basically constant. Furthermore, our procedure does not directly affect the T1 vertebral body, so the effect on the TIA and T1S is negligible. Regarding postoperative complications, difficulty swallowing is conspicuous. Dysphagia is a frequent complication after ACDF. Although dysphagia usually improves over 6 months, it remains a significant and persistent problem for some patients.19 We therefore performed a long-term follow-up study of patients with postoperative dysphagia. There were 9 cases of mild dysphagia and 1 case of medium dysphagia in the Zero-P VA group, showing that dysphagia was less likely to occur in the Zero-P VA group than in the other two groups. We believe that these results can be explained by the Zero-P VA device providing better resistance to forward flexion, extension and lateral flexion and easily restoring the curvature of the cervical spine.20 The Skyline device has the same mechanism, but because the thickness and length of the Skyline titanium plate are inferior to those of the Zero-P VA device, dysphagia is more common with the Skyline device. This is consistent with a previous report that use of the Zero-P VA device avoided friction with surrounding soft tissues and reduced the rate of postoperative foreign body sensation and dysphagia21–23. Additionally, we noted that the rate of dysphagia was similar in the Prodisc-C Vivo and Skyline groups, which is not consistent with previous studies.24 As far as the Prodisc-C Vivo device is concerned, this device can maintain the adjacent-segment ROM and can reduce the incidence of radiographic adjacent-level changes in patients undergoing ACDF,25 so we hold that this device cannot restore the physiological curvature of the cervical spine very well and may result in greater loss of correction over the long term, which may be one of the causes of dysphagia, along with displacement of the prosthesis and collapse of the intervertebral space after artificial disc replacement as other possible factors. However, the data in this study are insufficient to analyze this phenomenon, so the analysis of a large number of medical records is still needed to identify the reasons for this situation.
Although some significant conclusions can be drawn from this study, there are still some limitations. This was a single-center study with a limited amount of data and a nonuniform follow-up duration. Long-term follow-up is needed for further analysis and comparison of the long-term changes in the sagittal balance among the three groups after surgery.
Conclusion
In conclusion, different fusion instruments can all provide a good surgical effect, restore the curvature of the cervical spine and correct kyphosis to some degree. However, the Prodisc-C Vivo group showed the least improvement in the cervical sagittal balance, with greater long-term loss of correction than the other two groups. Both the Zero-PVA fusion device and the Skyline anterior cervical titanium plate effectively improved sagittal balance, with little loss of correction on long-term follow-up, but because of the characteristics of the Zero-PVA fusion device, it caused less postoperative dysphagia than the other devices.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Protopsaltis T, Terran J, Soroceanu A, et al. T1 slope minus cervical lordosis (TS-CL), the cervical answer to PI-LL, defines cervical sagittal deformity in patients undergoing thoracolumbar osteotomy. Int J Spine Surg. 2018;12(3):362–370. doi:10.14444/5042
2. Liu WJ, Hu L, Chou PH, et al. Comparison of anterior cervical discectomy and fusion versus posterior cervical foraminotomy in the treatment of cervical radiculopathy: a systematic review. Orthop Surg. 2016;8(4):425–431. doi:10.1111/os.12285
3. Sala V, Lisi C, Di Natali G, et al. Functional and quality of life evaluation after single level cervical discectomy and fusion or cervical artificial disc replacement. G Ital Med Lav Ergon. 2015;37(4):239–244.
4. Donk RD, Arnts H, Verhagen WIM, et al. Cervical sagittal alignment after different anterior discectomy procedures for single-level cervical degenerative disc disease: randomized controlled trial. Acta Neurochir. 2017;159(12):2359–2365. doi:10.1007/s00701-017-3312-z
5. Oliver JD, Goncalves S, Kerezoudis P, et al. Comparison of outcomes for anterior cervical discectomy and fusion with and without anterior plate fixation: a systematic review and meta-analysis. Spine. 2018;43(7):E413–E422. doi:10.1097/BRS.0000000000002441
6. Savoldelli C, Ehrmann E, Tillier Y. Biomechanical assessment of different fixation methods in mandibular high sagittal oblique osteotomy using a three-dimensional finite element analysis model. Sci Rep. 2021;11(1):8755. doi:10.1038/s41598-021-88332-2
7. Song J, Pan F, Zhu W, et al. Characteristics of the sagittal spinal balance in the asymptomatic elderly Chinese population. Eur Spine J. 2021;31(2):233–240.
8. Mummaneni PV, Amin BY, Wu JC, et al. Cervical artificial disc replacement versus fusion in the cervical spine: a systematic review comparing long-term follow-up results from two FDA trials. Evid Based Spine Care J. 2012;3:59–66. doi:10.1055/s-0031-1298610
9. Li Y, Shen H, Khan KZ, et al. Comparison of multilevel cervical disc replacement and multilevel anterior discectomy and fusion: a systematic review of biomechanical and clinical evidence. World Neurosurg. 2018;116:94–104. doi:10.1016/j.wneu.2018.05.012
10. Wang Z, Zhou L, Lin B, et al. Risk factors for non-fusion segment disease after anterior cervical spondylosis surgery: a retrospective study with long-term follow-up of 171 patients. J Orthop Surg Res. 2018;13(1):27. doi:10.1186/s13018-018-0717-1
11. Wang Z, Wang ZW, Fan XW, et al. Assessment of spino cranial angle of cervical spine sagittal balance system after multi-level anterior cervical discectomy and fusion. J Orthop Surg Res. 2021;16(1):194. doi:10.1186/s13018-021-02353-1
12. Kwon WK, Kim PS, Ahn SY, et al. Analysis of associating factors with C2-7 sagittal vertical axis after two-level anterior cervical fusion: comparison between plate augmentation and stand-alone cages. Spine. 2017;42(5):318–325. doi:10.1097/BRS.0000000000001776
13. Lu J, Sun C, Bai J, et al. Is correction of segmental kyphosis necessary in single-level anterior cervical fusion surgery? An observational study. Ther Clin Risk Manag. 2019;15:39–44. doi:10.2147/TCRM.S177513
14. Zaidman N, De Witte O. Cervical sagittal balance: a predictor of neck pain after anterior cervical spine surgery? Br J Neurosurg. 2020;1–5. doi:10.1080/02688697.2020.1850643
15. Coric D, Nunley PD, Guyer RD, et al. Prospective, randomized, multicenter study of cervical arthroplasty: 269 patients from the Kineflex|C artificial disc investigational device exemption study with a minimum 2-year follow-up: clinical article. J Neurosurg Spine. 2011;15(4):348–358. doi:10.3171/2011.5.SPINE10769
16. Alhashash M, Shousha M, Boehm H. Adjacent segment disease after cervical spine fusion: evaluation of a 70 patient long-term follow-up. Spine. 2018;43(9):605–609. doi:10.1097/BRS.0000000000002377
17. Chen J, Wang J, Wei X, et al. The importance of preoperative T1 slope for determining proper postoperative C2-7 Cobb’s angle in patients undergoing cervical reconstruction. J Orthop Surg Res. 2020;15(1):507. doi:10.1186/s13018-020-02016-7
18. Ma Z, Liu P, Liu J, et al. Kinematic analysis of the relationship between modic changes and sagittal balance parameters in the cervical spine. Medicine. 2017;96(33):e7699. doi:10.1097/MD.0000000000007699
19. Fogel GR, McDonnell MF. Surgical treatment of dysphagia after anterior cervical interbody fusion. Spine J. 2005;5(2):140–144. doi:10.1016/j.spinee.2004.06.022
20. Sun Z, Liu Z, Hu W, et al. Zero-profile versus cage and plate in anterior cervical discectomy and fusion with a minimum 2 years of follow-up: a meta-analysis. World Neurosurg. 2018;120:e551–e561. doi:10.1016/j.wneu.2018.08.128
21. Zhang Y, Liu H, Yang H, et al. Anterior cervical corpectomy and fusion versus discectomy and fusion for the treatment of two-level cervical spondylotic myelopathy: analysis of sagittal balance and axial symptoms. Int Orthop. 2018;42(8):1877–1882. doi:10.1007/s00264-018-3804-3
22. Lan Z, Huang Y, Xu W. Relationship between T1 slope minus C2-7 lordosis and cervical alignment parameters after adjacent 2-level anterior cervical discectomy and fusion of lower cervical spine. World Neurosurg. 2019;122:e1195–e1201. doi:10.1016/j.wneu.2018.11.016
23. Katsuura Y, Lemons A, Lorenz E, et al. Radiographic analysis of cervical and spinal alignment in multilevel ACDF with lordotic interbody device. Int J Spine Surg. 2017;11:13. doi:10.14444/4013
24. Yang Y, Ma L, Liu H, et al. Comparison of the incidence of patient-reported post-operative dysphagia between ACDF with a traditional anterior plate and artificial cervical disc replacement. Clin Neurol Neurosurg. 2016;148:72–78. doi:10.1016/j.clineuro.2016.07.020
25. Hou Y, Liu Y, Yuan W, et al. Cervical kinematics and radiological changes after discover artificial disc replacement versus fusion. Spine J. 2014;14(6):867–877. doi:10.1016/j.spinee.2013.07.432
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.