Back to Journals » Infection and Drug Resistance » Volume 16
Retrospective Analysis of Azithromycin-Resistant Ureaplasma urealyticum and Mycoplasma hominis Cervical Infection Among Pregnant Women
Authors Zhang S ![]() , Xu K
, Xu K ![]() , Liu SX
, Liu SX ![]() , Ye XL
, Ye XL ![]() , Huang P, Jiang HJ
, Huang P, Jiang HJ ![]()
Received 18 January 2023
Accepted for publication 31 May 2023
Published 5 June 2023 Volume 2023:16 Pages 3541—3549
DOI https://doi.org/10.2147/IDR.S405286
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Su Zhang,1 Ke Xu,2 Su-Xiao Liu,3 Xiao-Lan Ye,1 Ping Huang,1 Hong-Juan Jiang1
1Center for Clinical Pharmacy, Cancer Center, Department of Pharmacy, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China; 2Laboratory Medicine Center, Department of Clinical Laboratory, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China; 3Center for Reproductive Medicine, Department of Obstetrics, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Hong-Juan Jiang, Center for Clinical Pharmacy, Cancer Center, Department of Pharmacy, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China, Tel +86 571 85893143, Fax +86 571 87666666, Email [email protected]
Purpose: Ureaplasma urealyticum and Mycoplasma hominis began to show resistance to azithromycin, a macrolide antibiotic commonly used in pregnancy. Unfortunately, there are few effective and safe drugs in the clinic for genital mycoplasmas in pregnant women. In the present study, we investigated the prevalence of azithromycin-resistant U. urealyticum and M. hominis infections in pregnant women. The secondary research objects were possible influencing factors and consequences of insensitive Mycoplasma infection.
Patients and methods: A retrospective analysis was carried out in pregnant women who underwent cervical Mycoplasma culture between October 2020 and October 2021 at a large general hospital in eastern China. The sociological characteristics and clinical information of these women were collected and analyzed.
Results: A total of 375 pregnant women were enrolled, and 402 cultured mycoplasma specimens were collected. Overall, 186 (49.60%) patients tested positive cervical Mycoplasma infection, and 37 (9.87%) had infections caused by azithromycin-resistant Mycoplasma. In total, 39 mycoplasma samples were insensitive to azithromycin in vitro, also showing extremely high resistance to erythromycin, roxithromycin, and clarithromycin. Azithromycin was the only antibiotic used in women with Mycoplasma cervical infection, regardless of azithromycin resistance in vitro. Statistical results showed that azithromycin-resistant cervical Mycoplasma infection in pregnant women was unrelated to age, body mass index (BMI), gestational age, number of embryos, and assisted reproductive technology (ART) use, but led to a significantly increased incidence of adverse pregnancy outcomes (spontaneous abortion (SA), preterm birth (PTB), preterm prelabor rupture of membranes (PPROM), and stillbirth).
Conclusion: Azithromycin-resistant U. urealyticum and M. hominis cervical infections are relatively common during pregnancy, and can increase the risk of adverse pregnancy outcomes; however, there is currently a lack of safe and effective drug treatments. Herein, we show that azithromycin-resistant mycoplasma infection requires timely intervention.
Keywords: azithromycin resistance, Ureaplasma urealyticum, Mycoplasma hominis, pregnant women
Introduction
Mycoplasma are a form of small, free-living microorganism.1 The mycoplasma species Ureaplasma urealyticum, Mycoplasma hominis, Ureaplasma parvum, and Mycoplasma genitalium are the most common mycoplasma associated with urogenital tract infections.1 These microbes, particularly U. urealyticum, commonly colonize the urogenital tract without causing symptoms or harmful effects in nonpregnant women.2,3 However, several studies have reported that post-pregnancy mycoplasma infection in the genital tract is associated with adverse pregnancy outcomes, including preterm birth (PTB), preterm prelabor rupture of membranes (PPROM), low birth weight (LBW), spontaneous abortion (SA), and stillbirth.4–6 Other studies have suggested that, in conjunction with bacterial vaginosis (BV), mycoplasma infection plays a role in causing adverse pregnancy outcomes.7,8 M. hominis infection was identified as a potential risk factor for SA, stillbirth, and PPROM in a meta-analysis in 2021.9 However, the latest meta-analysis data shows that the currently available literature does not allow conclusions about the role of mycoplasmas in adverse pregnancy outcomes, alone or coexisting with BV due to strong data bias.10 Nevertheless, the clinical consensus is that gestational women with symptoms of threatened abortion, threatened premature delivery, or suspected intrauterine infection should undergo active intervention for cervical mycoplasma infection.1,3,11
Given the teratogenic risk of tetracycline and quinolone antibiotics, pregnant women are almost exclusively administered macrolides to fight mycoplasma infection, of which the most commonly used varieties are azithromycin and erythromycin.1,3,9 However, the problem of mycoplasma macrolide resistance has become increasingly serious in recent years. The prevalence of mutations associated with macrolide resistance among M. genitalium samples increased from 10% before 2010 to 51.4% between 2016–2017.12 The resistance rates of U. urealyticum and M. hominis to azithromycin were found to be 65.79% and 88.89%, respectively, in a 2021 study conducted in central China.13 As a result, the drug choice for azithromycin-resistant mycoplasma infection in pregnant women is increasingly difficult.3
To date, only U. urealyticum and M. hominis can be detected by culture and drug sensitivity tests because U. parvum and M. genitalium require harsh in vitro growth environments.1,14 However, there is still a relative paucity of data on azithromycin-resistant U. urealyticum and M. hominis cervical infections in pregnant women. Therefore, this retrospective study was conducted to clarify the prevalence of azithromycin resistance in U. urealyticum and M. hominis among pregnant women. The possible influencing factors and consequences of this insensitive Mycoplasma infection were investigated as the secondary research goals.
Methods
Study Population and Information Collection
This study was approved by the institutional review board of the host institution. The B-ultrasound results from the hospital information system (HIS) were used as the judging criteria for pregnancy in the present study. All pregnant women who underwent cervical mycoplasma (U. urealyticum and M. hominis) culture between October 2020 and October 2021 at Zhejiang Provincial People’s Hospital (Hangzhou, eastern China) were selected as the study population. Patients who did not meet the inclusion criteria were excluded. The pregnant women included in this study were renumbered with Arabic numerals according to the sequence of Mycoplasma culture times to ensure patient confidentiality. Sociological and clinical information at the time of mycoplasma culture, including age, height, weight, gestational age, embryo number, gestation method (spontaneous conception or pregnancy by assisted reproductive technology [ART]), cervical mycoplasma infection, drug susceptibility results, and anti-mycoplasma drug usage, was collected by querying the HIS. We further recorded the subsequent mycoplasma culture re-examination results and the occurrence of adverse pregnancy outcomes, including SA, PTB, PPROM, and stillbirth, in these women using the HIS. Some missing data in the HIS, primarily delivery information among women who did not give birth in the hospital, were collected via telephone inquiries. We further analyzed the risk factors for azithromycin-resistant cervical mycoplasma infection and their correlation with adverse pregnancy outcomes.
The identity and antibiotic susceptibility of U. urealyticum and M. hominis were determined using the Mycoplasma Ies Test kit (ZHUHAI DL BIOTECH Co., Ltd., Zhuhai, China) according to the manufacturer’s guidelines, which provides information on susceptibility to 12 antibiotics. Each drug has two sensitivity test holes with different drug concentrations in the Mycoplasma culture plate. After confirming mycoplasma growth in isolated culture holes, drug-sensitive holes were used to further analyze resistance: the absence of mycoplasma growth in both high and low concentration test holes indicated susceptibility (S); mycoplasma growth at low drug concentration and no growth at high drug concentration was considered as intermediate (I), and mycoplasma growth in both 2 holes indicated resistance (R). The breakpoints of the 12 antibiotics were as follows: tetracycline S≤4 mg/L, R≥8 mg/L; levofloxacin S≤1 mg/L, R≥4 mg/L; erythromycin S≤1 mg/L, R≥4 mg/L; josamycin S≤2 mg/L, R≥8 mg/L; doxycycline S≤4 mg/L, R≥8 mg/L; ciprofloxacin S≤1 mg/L, R≥2 mg/L; ofloxacin S≤1 mg/L, R≥4 mg/L; minocycline S≤4 mg/L, R≥8 mg/L; roxithromycin S≤1 mg/L, R≥4 mg/L; azithromycin S≤0.12 mg/L, R≥4 mg/L; clarithromycin S≤1 mg/L, R≥4 mg/L; spaflexacin S≤1 mg/L, R≥4 mg/L. Intermediate and resistant test kit results were redefined as broader resistance to further calculate the antimicrobial resistance rates. The standard operating procedure was as follows: A clinical specimen swab was inserted into a Mycoplasma culture flask and mixed with the medium; 100 μL medium was then added into each hole of the test plate which was cultured in an incubator at 35–37°C. U. urealyticum and M. hominis were observed after 24 and 48 hours, respectively. All surgeries were performed under sterile conditions.
Data Analysis
Categorical variables were expressed as frequencies and percentages, and continuous variables were expressed as mean and standard deviation (SD). The body mass index (BMI) of patients was calculated from the height and weight data. Pregnant women were divided into two groups based on whether they were infected with azithromycin-resistant Mycoplasma. The Independent-samples T-test or Mann–Whitney U-test was used to analyze comparisons between groups of continuous variables, and the Fisher’s exact test or χ2 test was used to compare frequency data. The 95% Confidence Interval (CI) for the drug resistance rate was calculated using the approximately normal method or the Clopper-Pearson method, based on sample size and incidence. The Statistical Package for Social Science (SPSS) (version 26.0) was used for data analysis, and a p value <0.05 was considered statistically significant.
Results
Sociological and Clinical Characteristics of the Study Population
A total of 375 pregnant women were included in the study, with a mean age of 30.40±4.46 years in this study. A total of 186 (49.60%) patients had cervical mycoplasma (U. urealyticum and/or M. hominis), of whom 37 (9.87% of total) were infected with azithromycin-resistant strains. The overall incidence of adverse pregnancy outcomes (SA, PTB, PPROM, and stillbirth) was 33.87% (Table 1).
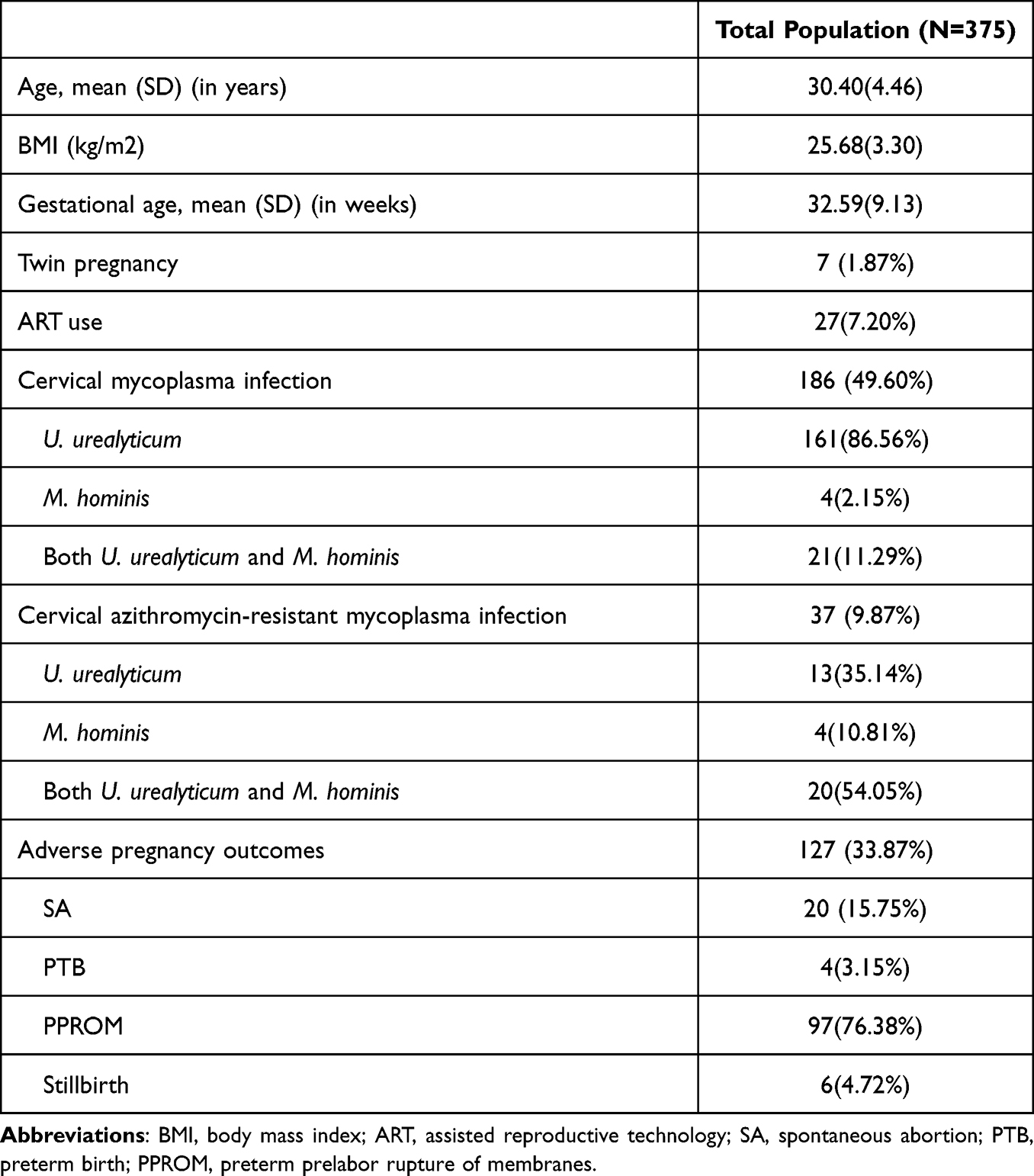 |
Table 1 Sociological and Clinical Characteristics of 375 Pregnant Women |
Mycoplasma Drug Resistance in Positive Cervical Secretions in vitro
A total of 402 cervical specimens were cultured from these 375 women. Two hundred samples tested positive for Mycoplasma, including 174 (87.00%) for U. urealyticum, four (2.00%) for M. hominis, and 22 (11.00%) mixed infection samples. In general, U. urealyticum and M. hominis showed high resistance to quinolones, moderate resistance to macrolide antibiotics (except josamycin), and low resistance to tetracycline (Table 2).
 |
Table 2 Mycoplasma Drug Resistance in 200 Positive Cervical Secretions in vitro |
Azithromycin-Resistant Mycoplasma and Their Resistance to Other Macrolides in vitro
Further analysis found that the resistance rate of pure U. urealyticum to azithromycin was 8.05%. All four M. hominis samples collected in the present study were azithromycin resistant. The 22 mixed mycoplasma samples also showed high azithromycin resistance (Table 3).
 |
Table 3 Mycoplasma Azithromycin Resistance in 200 Positive Cervical Secretions in vitro |
The 39 azithromycin-resistant Mycoplasma strains discovered in this study showed extremely high resistance to erythromycin, roxithromycin, and clarithromycin, with resistance rates above 90%. Of note, mycoplasmas showed good sensitivity to josamycin, regardless of azithromycin resistance (Table 4).
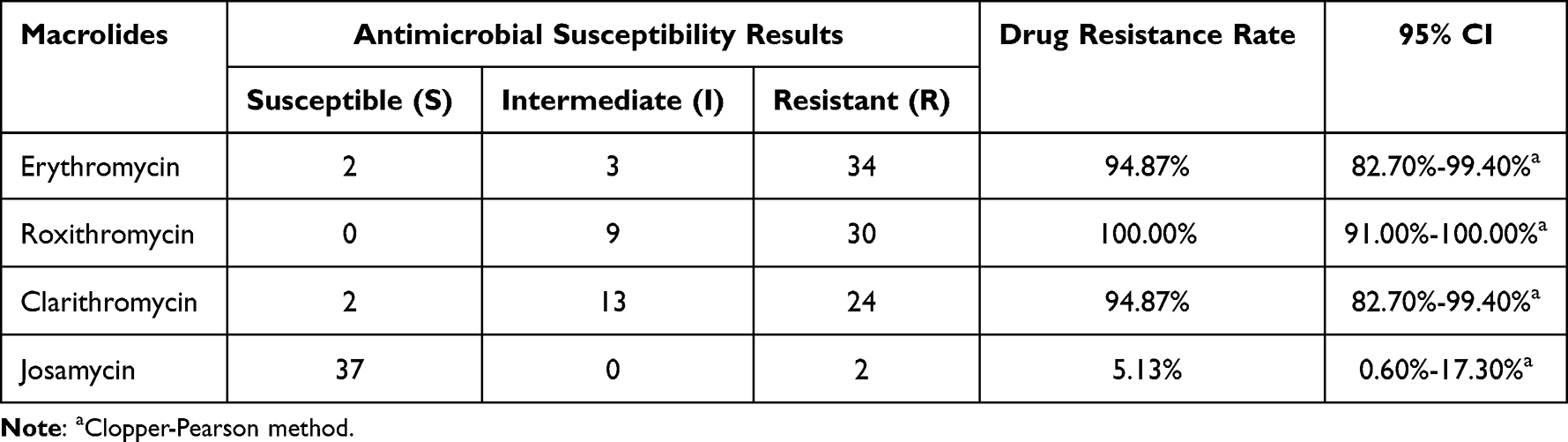 |
Table 4 Resistance of 39 Azithromycin-Resistant Mycoplasma to Other Macrolides in vitro |
Antibiotic Therapy and Subsequent Culture Reexamination in Women with Mycoplasma Infection
Among the 186 pregnant women with Mycoplasma infections, 84 (45.16%) received antibiotic therapy. Azithromycin was the only drug used, but differences were observed in usage: 54 (64.29%) patients were treated with a single dose of 1 g azithromycin orally, 23 (27.38%) with 0.5 g dose for 3 days orally, 2 (2.38%) with 0.25 g dose for 6 days orally and 5 (5.95%) with 0.5 g dose for 3 days intravenously. Of the 37 women infected with azithromycin-resistant strains, 10 (27.03%) were still treated with azithromycin, and a single oral dose of 1 g was the most commonly used (7/10). The remaining 27 patients (72.97%) did not receive drug treatment during pregnancy.
Mycoplasma results were reviewed in only 13 (15.48%) medicated women who received drug therapy. Patients No.3 and No.283 were reviewed twice with review intervals of 22, 98 days, and 14, 26 days, respectively. The remaining 11 patients were reexamined once each, at intervals of 11, 22, 97, 38, 27, 7, 186, 55, 72, 43, and 20 days.
Risk Factors for Azithromycin-Resistant Cervical Mycoplasma Infection and Its Correlation with Adverse Pregnancy Outcomes
Statistical analysis revealed that infection with azithromycin-resistant mycoplasma occurred independently of age, BMI, gestational age, number of embryos, and ART use (all p > 0.05). The incidence of adverse pregnancy outcomes was 51.35% in women infected with azithromycin-resistant mycoplasma, which was significantly higher than in women with no azithromycin-resistant mycoplasma (31.95%) (p=0.018) (Table 5).
 |
Table 5 Risk Factors for Azithromycin-Resistant Cervical Mycoplasma Infection and Its Correlation with Adverse Pregnancy Outcomes |
Discussion
This is among the first studies to investigate the situation of azithromycin resistance in U. urealyticum and M. hominis in pregnant women. Existing research data show that the resistance rate of mycoplasma to macrocyclic lipid antibiotics increases rapidly due to key mutations in the 23s ribosomal RNA gene.12,15 Most studies on mycoplasma resistance have focused on M. genitalium.11,12,15 Similar to M. genitalium, U. urealyticum and M. hominis also showed resistance to typical macrocyclic lipids, including azithromycin, erythromycin, roxithromycin, and clarithromycin, and the drug resistance rates in vitro were 19.50%, 47.00%, 40.50%, and 28.00%, respectively, in this study. This is similar to the data published in 2021 in central China: U. urealyticum and M. hominis showed varying degrees of resistance to the majority of macrocyclic lipids.13 Erythromycin and azithromycin, two classic macrocyclic lipids, are recommended by guidelines for the treatment of mycoplasma infection in pregnancy.1,3,11 Azithromycin is more commonly used clinically than erythromycin due to its similar antibacterial profiles but longer half-life.16 This study found that azithromycin-insensitive mycoplasma (U. urealyticum or/and M. hominis) also exhibited extremely high resistance to other macrolides, including erythromycin, roxithromycin and clarithromycin. Considering the reproductive toxicity of quinolones and tetracyclines, almost no drugs are available for azithromycin-resistant Mycoplasma infections during pregnancy.
Several researchers have postulated that the rapidly increasing prevalence of macrolide resistance in Mycoplasma is most likely due to the widespread use of azithromycin as a 1 g single dose without follow-up efficacy test.11,17 A similar phenomenon was observed in the present study. Among 84 pregnant women treated with azithromycin, 54 (64.29%) received a single dose of 1 g orally. In addition, the guideline clearly recommends that patients with confirmed urogenital Mycoplasma infection should be reviewed 2 weeks after drug withdrawal by culture test.1 However, only 13 (15.48%) patients in the present study were reviewed for Mycoplasma results, and most of the follow-up intervals did not meet the 2 week time requirement in this study. Inadequate drug therapy may exacerbate the selection of drug-resistant Mycoplasma. As such, more attention should be paid to the prescribing behavior of clinicians to delay Mycoplasma resistance to macrocyclic lipids. Compared with an azithromycin regimen of a single dose of 1 g, using a 2 g dose administered over 3 days (1 g followed by 0.5 g for 2 days) may improve microbiological cure rate and reduce the risk of macrolide resistance developing in mycoplasma.3 Further, a review of the existing mycoplasma after drug therapy is necessary.1
In the present study, 186 women (49.60%) had cervical mycoplasmas (U. urealyticum and/or M. hominis). In a 2014 study of 5377 pregnant patients at 25–37 weeks of gestation, 2259 (42%) had a positive culture for Ureaplasma spp. and/or M. hominis.18 These data suggest that Mycoplasma infection during pregnancy is a common clinical phenomenon. As the rate of azithromycin resistance in mycoplasma increases, an increasing number of pregnant women will inevitably become infected with this resistant microorganism. In the present study, 9.87% of the pregnant women investigated were infected with azithromycin-resistant U. urealyticum and/or M. hominis. Statistical analysis showed that resistant Mycoplasma infection was unrelated to age, BMI, gestational age, embryo number, or ART use. Women with twin pregnancies appeared to have a higher cervical mycoplasma detection rate in this study, which is consistent with current medical cognition. Compared with single pregnancies, women with twin pregnancies tend to have shorter cervical lengths due to fetal weight, meaning that the mycoplasma colonizing the vagina might have relatively easy access to the cervix.19 This fact suggests that obstetricians should pay more attention to mycoplasma infections in women with twin pregnancies. Another interesting finding was that woman with resistant Mycoplasma infections had a lower rate of ART use, although this difference was not statistically significant. Transvaginal procedures are usually performed during ART, and examination of reproductive tract mycoplasmas is required before operation. Thus, if drug-resistant Mycoplasma colonizes the reproductive tract, sensitive antibacterial drugs can be freely used prior to embryo implantation. This suggests that pre-pregnancy screening and necessary interventions for Mycoplasma infection may be useful in reducing resistant Mycoplasma infections during pregnancy.
The overall incidence of adverse pregnancy outcomes (SA, PTB, PPROM, and stillbirth) was 33.87%. This figure is higher than 15% in a 2020 study of 4285 pregnant women in Yunnan Province, China.20 This may be because Mycoplasma cervical culture is not part of routine pregnancy check-up, and obstetricians in this hospital would consider this test only if the pregnant women have related clinical symptoms, such as threatened abortion, threatened premature delivery, or suspected intrauterine infection in the clinic. Further analysis found that approximately half of the pregnant women with azithromycin-resistant Mycoplasma infection had adverse pregnancy outcomes, which was significantly higher than in women without. These data highlighted the serious consequences of azithromycin-resistant Mycoplasma infections during pregnancy. We further observed that 10 (27.03%) patients were still treated with azithromycin, although their in vitro drug sensitivity was low. The reasons for this may be as follows: some obstetricians in this hospital believed that although commonly used macrolides were resistant in vitro, they may be beneficial in reducing adverse pregnancy outcomes by downgrading the mycoplasma titer in pregnant women with clinical symptoms. Azithromycin is safer during pregnancy than roxithromycin and clarithromycin, and seems to be a relatively good choice for this drug choice predicament. Together, these data indicate that there is an urgent need to curb mycoplasma azithromycin resistance and to find safe and effective drugs during pregnancy.
Prior reports have indicated differences in drug resistance between U. urealyticum and M. hominis in vitro.1,21,22 U. urealyticum is sensitive to erythromycin, whereas M. hominis is naturally resistant.1,21 Erythromycin and azithromycin have similar antibacterial profiles owing to their similar chemical structures.16 Similar results were obtained in this study: only 8.05% of U. urealyticum strains showed azithromycin resistance, whereas all four M. hominis strains identified were insensitive, while the azithromycin resistance rate reached 95.45% for U. urealyticum and M. hominis mixed strains. Some studies have found that M. hominis is susceptible to 16-membered macrolides (josamycin and miocamycin) and lincomycin in vitro.21,22 This study verified the effectiveness of josamycin against mycoplasma, regardless of azithromycin resistance. Josamycin therefore appears to be a good option for treating Mycoplasma infections. However, there are limited data on the safety of josamycin during pregnancy. Furthermore, it has not yet been approved by the United States Food and Drug Administration (FDA) for sale in United States. Medical facilities in some provinces in China are also unable to obtain josamycin owing to differences in drug purchase lists among the provinces. In Zhejiang Province, where this hospital is located, doctors are unable to prescribe josamycin because of drug supply restrictions. These barriers limit the use of josamycin during pregnancy. Clindamycin, a derivative of lincomycin, has a similar antibacterial profile to lincomycin, and has been widely used in pregnant women for many years.23 Although lincomycin and clindamycin do not appear on the drug list in mycoplasma culture, it has been reported that M. hominis is sensitive to clindamycin, while U. urealyticum is moderately sensitive in vitro.1 A 2014 study proved that clindamycin could reduce the rates of premature labor and neonatal complications in pregnant women with mycoplasma infection with symptoms of potential obstetric complications at 25–37 weeks of gestation.18 These data suggest that clindamycin may be a potential choice for azithromycin-resistant mycoplasma infection in pregnant women. However, further in vitro and human trials are required to confirm the efficacy of clindamycin against urogenital tract mycoplasmas. Based on the above data, we can conclude that all M. hominis and a small portion of U. urealyticum together constitute azithromycin-resistant mycoplasma in the urogenital tract, and that josamycin and clindamycin might be potential research targets for this resistant mycoplasma infection during pregnancy.
Limitations
This study had several limitations. First, only pregnant women with related obstetric symptoms were tested for mycoplasma culture. As a result, the positive rates of U. urealyticum and M. hominis in cervical secretions and the incidence of adverse pregnancy outcomes in this retrospective study may theoretically deviate from the actual situation. On the premise of ethical approval, prospective studies should theoretically obtain more realistic results. Secondly, 375 pregnant women were enrolled in this study, and 37 were infected with azithromycin-resistant mycoplasma. Only four culture samples tested positive for M. hominis. This sample size may be insufficient for an accurate analysis of the composition and characteristics of azithromycin-resistant mycoplasma. Further studies with an increased sample size should be performed in the future.
Conclusion
Cervical infections caused by azithromycin-resistant U. urealyticum and M. hominis can occur in pregnant women. Infection with these resistant organisms can increase the incidence of adverse pregnancy outcomes; however, there is currently a lack of effective and safe drug treatments for pregnant women. Infection with azithromycin resistant U. urealyticum and M. hominis is of great concern, particularly in pregnant women.
Ethics Approval
This study has been approved by Ethics Committee of the Zhejiang Provincial People’s Hospital (ZJPPHEC2022O (375)). The women in this study were encrypted into a new patient serial number to protect privacy according to the sequence of mycoplasma culture time. All procedures performed in this study involving human participants were in accordance with the Ethical Standards of the Institutional Ethics Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Since this was a retrospective analysis and patient information was encrypted, the ethics Committee exempted the informed consent of the patients. Personal information and medical information of a specific patient will not be disclosed in this article.
Funding
This study was supported by Zhejiang Provincial Natural Science Foundation of China (LQ21H310004), Special scientific research fund project of Hospital Pharmacy of Zhejiang Pharmaceutical Association (2021ZYY30) and Zhejiang Medical and Health Science and Technology Project (2022KY024).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dai L, Chaohui L. Consensus on the diagnosis and treatment of mycoplasma infection in genital tract. Chin J Hum Sex. 2016;25(3):80–82. doi:10.3969/j.issn.1672-1993.2016.03.026
2. Plummer EL, Vodstrcil LA, Bodiyabadu K, et al. Are Mycoplasma hominis, Ureaplasma urealyticum and Ureaplasma parvum associated with specific genital symptoms and clinical signs in nonpregnant women. Clin Infect Dis. 2021;73(4):659–668. doi:10.1093/cid/ciab061
3. Soni S, Horner P, Rayment M, et al. British association for sexual health and HIV national guideline for the management of infection with mycoplasma genitalium (2018). Int J STD AIDS. 2019;30(10):938–950. doi:10.1177/0956462419825948
4. Oliveira CNT, Oliveira MTS, Oliveira HBM, et al. Association of spontaneous abortion and Ureaplasma parvum detected in placental tissue. Epidemiol Infect. 2020;148:e126. doi:10.1017/S0950268820001302
5. Luton D, Ville Y, Luton-Sigy A, et al. Prevalence and influence of Mycoplasma hominis and Ureaplasma urealyticum in 218 African pregnant women and their infants. Eur J Obstet Gynecol Reprod Biol. 1994;56(2):95–101. doi:10.1016/0028-2243(94)90263-1
6. Farhadifar F, Khodabandehloo M, Ramazanzadeh R, et al. Survey on association between Mycoplasma hominis endocervical infection and spontaneous abortion using polymerase chain reaction. Int J Reprod Biomed. 2016;14(3):181–186.
7. Taylor-Robinson D. The role of mycoplasmas in pregnancy outcome. Best Pract Res Clin Obstet Gynaecol. 2007;21(3):425–438. doi:10.1016/j.bpobgyn.2007.01.011
8. Donders GGG, Ruban K, Bellen G, et al. Mycoplasma/Ureaplasma infection in pregnancy: to screen or not to screen. J Perinat Med. 2017;45(5):505–515. doi:10.1515/jpm-2016-0111
9. Ma C, Du J, Dou Y, et al. The associations of genital mycoplasmas with female infertility and adverse pregnancy outcomes: a systematic review and meta-analysis. Reprod Sci. 2021;28(11):3013–3031. doi:10.1007/s43032-020-00399-w
10. Jonduo ME, Vallely LM, Wand H, et al. Adverse pregnancy and birth outcomes associated with Mycoplasma hominis, Ureaplasma urealyticum and Ureaplasma parvum: a systematic review and meta-analysis. BMJ Open. 2022;12(8):e062990. doi:10.1136/bmjopen-2022-062990
11. Jensen JS, Cusini M, Gomberg M, et al. 2016 European guideline on Mycoplasma genitalium infections. J Eur Acad Dermatol Venereol. 2016;30(10):1650–1656. doi:10.1111/jdv.13849
12. Machalek DA, Tao Y, Shilling H, et al. Prevalence of mutations associated with resistance to macrolides and fluoroquinolones in Mycoplasma genitalium: a systematic review and meta-analysis. Lancet Infect Dis. 2020;20(11):1302–1314. doi:10.1016/S1473-3099(20)30154-7
13. Zhang Y, Fan DS, Fan LJ, et al. Detection and drug resistance of Mycoplasma in 850 patients with genitourinary system infection. Eval Anal Drug Use Hosp China. 2021;21(5):620–623. doi:10.14009/j.issn.1672-2124.2021.05.025
14. Leli C, Mencacci A, Latino MA, et al. Prevalence of cervical colonization by Ureaplasma parvum, Ureaplasma urealyticum, Mycoplasma hominis and Mycoplasma genitalium in childbearing age women by a commercially available multiplex real-time PCR: an Italian observational multicentre study. J Microbiol Immunol Infect. 2018;51(2):220–225. doi:10.1016/j.jmii.2017.05.004
15. Laumen JGE, van Alphen LB, Maduna LD, et al. Molecular epidemiological analysis of Mycoplasma genitalium shows low prevalence of azithromycin resistance and a well-established epidemic in South Africa. Sex Transm Infect. 2021;97(2):152–156. doi:10.1136/sextrans-2019-054371
16. Bakheit AH, Al-Hadiya BM, Abd-Elgalil AA. Azithromycin. Profiles Drug Subst Excip Relat Methodol. 2014;39:1–40. doi:10.1016/B978-0-12-800173-8.00001-5
17. de Salazar A, Barrientos-Durán A, Espadafor B, et al. Macrolide and fluoroquinolone resistance of Mycoplasma genitalium in southern Spain, 2018–2019. Sex Transm Infect. 2021;97(1):8–10. doi:10.1136/sextrans-2019-054386
18. Vouga M, Greub G, Prod’hom G, et al. Treatment of genital mycoplasma in colonized pregnant women in late pregnancy is associated with a lower rate of premature labour and neonatal complications. Clin Microbiol Infect. 2014;20(10):1074–1079. doi:10.1111/1469-0691.12686
19. Khalil A, Prasad S. Screening and prevention of preterm birth in twin pregnancies. Best Pract Res Clin Obstet Gynaecol. 2022;84:179–193. doi:10.1016/j.bpobgyn.2022.08.008
20. Yang Y, Yang JY, Du YL, et al. The survey of the correlation between adverse pregnancy outcomes of women and their menstrual history and birth history in Baoshan city of Yunnan Province. Chin J Fam Plann. 2020;28(9):1342–1345. doi:10.3969/j.issn.1004-8189.2020.09.003
21. Furneri PM, Rappazzo G, Musumarra MP, et al. Genetic basis of natural resistance to erythromycin in Mycoplasma hominis. J Antimicrob Chemother. 2000;45(4):547–548. doi:10.1093/jac/45.4.547
22. Waites KB, Katz B, Schelonka RL. Mycoplasmas and ureaplasmas as neonatal pathogens. Clin Microbiol Rev. 2005;18(4):757–789. doi:10.1128/CMR.18.4.757-789.2005
23. Bookstaver PB, Bland CM, Griffin B, et al. A review of antibiotic use in pregnancy. Pharmacotherapy. 2015;35(11):1052–1062. doi:10.1002/phar.1649
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.