")
Back to Journals » Clinical Ophthalmology » Volume 12
Retrobulbar hemodynamics and aqueous humor levels of endothelin-1 in exfoliation syndrome and exfoliation glaucoma
Authors Koukoula SC, Katsanos A , Tentes IK, Labiris G , Kozobolis VP
Received 30 October 2017
Accepted for publication 9 January 2018
Published 2 July 2018 Volume 2018:12 Pages 1199—1204
DOI https://doi.org/10.2147/OPTH.S155551
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Stavroula C Koukoula,1,2 Andreas Katsanos,2,3 Ioannis K Tentes,4 Georgios Labiris,1,2 Vassilios P Kozobolis1,2
1Department of Ophthalmology, University Hospital of Alexandroupolis, Alexandroupolis, Greece; 2Eye Institute of Thrace, Alexandroupolis, Greece; 3Ophthalmology Department, University of Ioannina, Ioannina, Greece; 4Department of Biochemistry, Medical School, Democritus University of Thrace, Alexandroupolis, Greece
Background: Endothelin-1 (ET-1) is the most potent vasoconstrictor in the body. There are reports in the literature correlating plasma levels of ET-1 and its impact on retrobulbar hemodynamics. This study evaluates aqueous humor levels of ET-1 and retrobulbar hemodynamics in patients with exfoliation syndrome (XFS) and exfoliation glaucoma (XFG).
Patients and methods: Patients scheduled for cataract surgery were included. Patients were allocated to non-exfoliation non-glaucoma group (controls), XFG and XFS groups. Peak systolic velocity (PSV), end diastolic velocity, and resistivity index of the ophthalmic artery (OA), short posterior ciliary arteries, and central retinal artery (CRA) were determined preoperatively using color Doppler imaging. Aqueous humor samples obtained at the beginning of cataract surgery were analyzed with enzyme-linked immunosorbent assay.
Results: Sixty-nine participants of similar age were included (controls: n=24, XFG: n=22, XFS: n=23). Multiple regression analysis showed that ET-1, OA-PSV, OA-resistivity index, CRA-PSV, and CRA-end diastolic velocity were influenced by group but not by sex or age. ET-1 for the XFG group (15.93±2.8 pg/mL) was significantly higher than for the XFS (8.92±2.7 pg/mL) and control (8.44±2.6 pg/mL) groups. The difference in ET-1 titers between the control and XFS groups was not statistically significant. All four hemodynamic parameters affected by group status significantly correlated with ET-1 levels in eyes with XFS. In eyes with XFG, two of the four hemodynamic parameters significantly correlated with ET-1 levels. In control eyes, no correlation between ET-1 and hemodynamic parameters affected by group status was detected.
Conclusion: ET-1 aqueous levels in eyes with XFG were significantly higher than those of age-matched controls. Reduced blood flow and increased vascular resistivity were detected in the OA and the CRA in eyes with XFG/XFS. ET-1 levels in eyes with XFG/XFS exhibit a significant correlation with hemodynamic parameters that indicate reduced perfusion.
Keywords: pseudoexfoliation, exfoliative glaucoma, color Doppler imaging
Introduction
Glaucoma is a group of optic neuropathies caused by the apoptosis of retinal ganglion cells in a characteristic pattern that might lead to blindness. Worldwide, glaucoma is a leading cause of irreversible blindness.1 Although the exact interplay of mechanisms leading to glaucoma remains a subject of investigation, it is believed that elevated intraocular pressure (IOP), vascular dysregulation, and alterations in numerous substances of the intraocular milieu are involved.1 Exfoliation (or pseudoexfoliation) syndrome (XFS) is a systemic elastosis characterized by the production and deposition of extracellular fibrillar material on several organs including the eye.2,3 Exfoliation has been linked to several systemic vascular abnormalities4 in some but not all studies.5–9 To date, exfoliation has been unequivocally associated with only ocular conditions such as exfoliation glaucoma (XFG), ischemic ocular disorders such as retinal vein occlusions, keratopathy, Zinn zonule fragility, and crystalline lens or pseudophakic dislocation.6 The obstruction of the trabecular meshwork by accumulated exfoliation material and pigment is thought to be the underlying cause of conversion from XFS to XFG. Of note, XFG is the commonest type of secondary open angle glaucoma and is characterized by unfavorable IOP characteristics and poor prognosis.3,5
Endothelin-1 (ET-1), a 21-amino acid peptide, is a member of a family of three mammalian vasoactive peptides that also includes endothelin-2 and endothelin-3.7 ET-1 is produced in lung, kidney, brain, and peripheral endocrine tissue as well as vascular endothelial cells. Being the most potent vasoconstrictor known, ET-1 induces a prolonged increase in blood pressure. In the human eye, ET-1 is actively secreted by nonpigmented ciliary epithelial cells8 and affects ocular blood flow (OBF) and IOP by several mechanisms.9,10 Experimental work has suggested that ET-1 is involved in the glaucomatous process.11 Color Doppler imaging (CDI) is a noninvasive and reproducible method that has been used for the evaluation of OBF.12–14 Previous studies with CDI have identified OBF abnormalities in patients with glaucoma and XFS.15,16 For instance, peak systolic velocity (PSV) and end diastolic velocity (EDV) in the ophthalmic artery (OA) and central retinal artery (CRA) were significantly decreased in patients with XFS and XFG.21 A significant body of evidence suggests that OBF abnormalities may be an important independent risk factor for glaucoma progression.17 However, the association between OBF characteristics and the role of ET-1 in different types of glaucoma remains unclear.
The aim of the present study was to investigate CDI-derived ocular hemodynamic parameters and aqueous humor levels of ET-1 in patients with XFS or XFG and healthy controls.
Patients and methods
This was a cross-sectional interventional study conducted at the Ophthalmology Clinic of the Democritus University of Thrace, Alexandroupolis, Greece. The study adhered to the tenets of the Declaration of Helsinki, and written informed consent was obtained from all participants. The bioethics committee of the aforementioned institution approved the investigation protocol.
The study groups consisted of cataract patients with XFS or XFG scheduled for phacoemulsification. The control group consisted of participants with no other ocular pathology except senile cataract scheduled for phacoemulsification. Patients with a family history of glaucoma were excluded from the control group. All controls had daytime IOP <21 mmHg in at least two measurements in different days.
The protocol for preoperative mydriasis was identical for all participants and included tropicamide 0.5% (Tropixal, Demo, Greece), phenylephrine hydrochloride 10% (Phenylephrine/COOPER, Cooper, Greece), cyclopentolate 1% (Cyclogyl, Bausch & Lomb U.K. Limited) and diclofenac 0.1% (Denaclof, Laboratoires Thea, France) drops, each instilled once within an hour before surgery.
Exclusion criteria for systemic conditions were history of diabetes mellitus, systemic vasculopathies, and clinically significant carotid or peripheral artery stenosis. Patients with well-controlled systemic hypertension were allowed in the study after their medication was recorded. Exclusion criteria for ophthalmic conditions were history or signs of previous ophthalmic surgery, trauma, or ocular inflammation. The use of topical antiglaucoma medications was not an exclusion criterion. However, patients in need of systemic carbonic anhydrase inhibitors were not allowed in the study.
A complete ophthalmic evaluation was performed in all patients. This included Snellen visual acuity testing, IOP measurement with a calibrated Goldmann applanation tonometer, slit lamp biomicroscopy, gonioscopy, and dilated fundoscopy. Humphrey 30-2 visual field testing was performed in all glaucoma patients (model 750; Humphrey Systems, Dublin, CA, USA). The diagnosis of XFS and XFG was made by an expert (VPK or GL) based on the European Glaucoma Society Terminology.18
Hemodynamic measurements
All CDI measurements were performed on the day before surgery by one experienced examiner (SCK) masked to the participant’s diagnosis using a 7.5 or 12 MHz linear array transducer (Philips ATL-HDI 1500; Philips Medical Systems, Eindhoven, the Netherlands). The 7.5 MHz probe was used for the assessment of the OA, whereas the 12 MHz probe was used for the assessment of the CRA and the short posterior ciliary artery (PCA). CDI was performed after the participant was allowed to rest for 10 minutes in the supine position. PSV, EDV, and resistivity index (RI) were measured in each artery (OA, CRA, and short PCA). PSV is the highest blood velocity achieved during cardiac systole and is automatically calculated from the frequency of the peak in the Doppler shifted waveform (cm/s). EDV is the lowest velocity occurring during diastole and is calculated from the frequency of the trough in the waveform (cm/s). The RI was determined according to the Pourcelot formula: RI=(PSV-EDV)/PSV. Gain and threshold were adjusted as appropriate for each participant and were kept constant during the entire examination.
ET-1 collection and measurements
At the beginning of surgery and before any tissue manipulation, a volume of aqueous humor sample ~15–30 μL was collected through a clear corneal paracentesis of the anterior chamber with a 27-G needle attached to a tuberculin syringe. Care was taken to avoid contamination of the samples with blood from limbal vessels. The sample was immediately stored in a freezer at −70°C and was analyzed within a couple of weeks in all cases. The aqueous humor concentration of ET-1 was determined with a commercially available immunoassay kit (R&D Systems Inc., Minneapolis, MN, USA). The parameter human ET-1 immunoassay is a 4.5 hours (total incubation time) solid-phase enzyme-linked immunosorbent assay designed to measure ET-1. It contains synthetic ET-1 and antibodies raised against synthetic ET-1. This immunoassay has been shown to accurately quantitate synthetic and naturally occurring human ET-1. The assay employs the quantitative enzyme immunoassay technique. An antibody specific for ET-1 has been precoated onto a microplate. Standards, samples, control, and conjugate are pipetted into the wells and any ET-1 present is sandwiched by the immobilized antibody and the enzyme-linked antibody specific for ET-1. Following a wash to remove any unbound substances and/or antibody–enzyme reagent, substrate is added to the wells and color develops in proportion to the amount of ET-1 bound. The color development is stopped, and the intensity of the color is automatically determined. All personnel involved in the biochemical analysis were masked to the patient’s group.
Data analysis
We used a multiple regression analysis model to examine whether ET-1 levels and CDI-derived hemodynamic indices differ in controls and participants with XFS or XFG. Age and sex were used as covariates. Additionally, we used Pearson product-moment correlation to assess the relationship between aqueous levels of ET-1 and hemodynamic indices in the groups. All analyses were performed using the SPSS version 21.0 software package. P-values <0.05 were considered statistically significant.
Results
Sixty-nine participants were included in the study: 24 in the control group (9 men), 22 in the XFG group (9 men), and 23 in the XFS group (12 men). The mean±SD age for the control, XFG, and XFS groups were 74.5±5.3, 76.2±4.9, and 78.3±5.6 years, respectively. There was no statistically significant difference in the participants’ age (P=0.07) and sex ratio (χ2=1.65, P=0.65) among the groups.
The multiple regression analysis model indicated that ET-1 levels and four different CDI-derived parameters (OA-PSV, OA-RI, CRA-PSV, and CRA-EDV) were influenced by group but not by sex or age (Table 1). No influence of group, age, or sex could be detected for other four parameters (OA-EDV, CRA-RI, PCA-EDV, and PCA-RI), whereas one parameter was influenced by sex (PCA-PSV: mean±standard error for men vs women: 10.6±0.2 vs 9.9±1.7 cm/s, P=0.011).
 | Table 1 ET-1 levels (in pg/mL) and retrobulbar hemodynamics results (in cm/s) for the control, XFG, and XFS groups |
A statistically significant difference in ET-1 values for the groups was detected (P<0.001). Bonferroni-adjusted pairwise comparisons indicated that the mean value of ET-1 for the XFG group (15.93±2.8 pg/mL) was significantly higher than for the XFS (8.92±2.7 pg/mL) and control (8.44±2.6 pg/mL) groups (Table 1). However, there was no statistically significant difference between the control and the XFS groups.
The relationship between those parameters affected by group status and ET-1 levels was examined with Pearson correlation analysis (Table 2). No significant correlation between ET-1 levels and hemodynamic parameters was detected for the control group. On the other hand, all four hemodynamic parameters affected by group status exhibited a significant correlation with ET-1 levels in eyes with XFS. In eyes with XFG, two of the four hemodynamic parameters significantly correlated with ET-1 levels (OA-RI: r=0.430, P=0.046; CRA-EDV: r=−0.513, P=0.015).
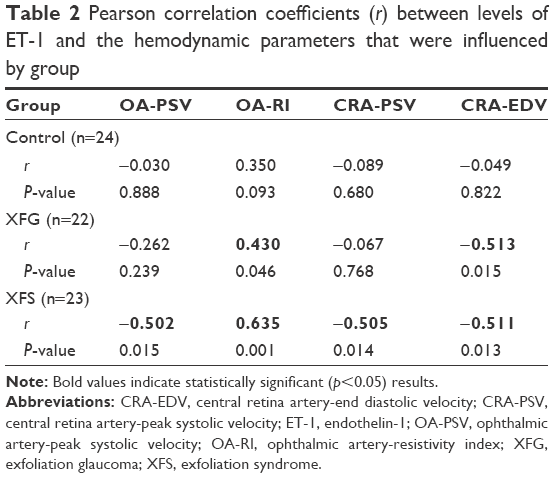 | Table 2 Pearson correlation coefficients (r) between levels of ET-1 and the hemodynamic parameters that were influenced by group |
Discussion
In the present study, the concentration of ET-1 in the aqueous humor of patients with XFG or XFS was compared to that of age-matched controls. Additionally, CDI-derived hemodynamic parameters and the possible correlation between ET-1 levels and these parameters were investigated in the three groups. To the best of our knowledge, this is the first study to investigate the relationship between aqueous humor levels of ET-1 and retrobulbar hemodynamics. We found that eyes with XFG had significantly higher aqueous humor levels of ET-1 compared with control eyes or eyes with XFS. In addition, our data suggest a general pattern of ocular hemodynamic derangement in eyes with XFS or XFG.
In the first similar study to investigate aqueous humor titers of ET-1, Koliakos et al19 reported that compared with age-matched controls, eyes with XFS had significantly higher levels of ET-1. These authors used an immunoassay kit to determine ET-1 levels in 25 participants with XFS and an equal number of age-matched controls scheduled for routine cataract surgery. In contrast to the study by Yuksel et al,24 in the present study, the difference in ET-1 levels between age-matched eyes with XFS (n=23) and controls (n=24) did not reach statistical significance (8.92±2.7 vs 8.44±2.6 pg/mL, respectively, P=1.00). The reason for this discrepancy is unclear, but a possible explanation may lie with differences in laboratory methods and study sample.
Early Doppler studies using finger capillary blood flow have shown that baseline cutaneous perfusion and its response to cold and warmth are altered in patients with XFG.20 In addition, pathological carotid artery function as well as altered parasympathetic vascular control has been described in patients with XFS or XFG.21,22 In ocular or periocular arteries, investigators using CDI have reported high values of resistivity and decreased flow velocities in the OA, CRA, and short PCA of patients with XFS or XFG.23,24 In a more recent study using CDI, Detorakis et al16 reported that the long PCAs of patients with XFS or XFG also exhibit lower flow velocities compared with controls or primary open angle glaucoma patients. The results of the current study suggest the reduction of blood flow in at least the OA and CRA of patients with XFS or XFG. Thus, our data are in accordance with previous evidence linking XFS/XFG with hemodynamic abnormalities in extraocular or ocular vessels.
The current study detected a notable pattern of correlation between ET-1 levels in the aqueous humor and hemodynamic parameters in patients with XFS/XFG. In eyes with XFG, two of the four correlations between aqueous ET-1 levels and group-dependent CDI indices exhibited statistical significance and moderate strength (OA-RI: P=0.046, r=0.430; CRA-EDV: P=0.015, r=−0.513). In eyes with XFS, all four correlations between aqueous ET-1 levels and group-dependent CDI indices exhibited statistical significance and moderate strength (Table 2). These results indicate that intraocular ET-1 may be implicated in the hemodynamic abnormalities observed with CDI in eyes with XFS/XFG.
Limitations
The current study has some limitations. First, as in all association studies, the described relationship between ET-1 and hemodynamic dysfunction in eyes with XFS or XFG does not necessarily imply causation. In other words, both hemodynamic alterations and ET-1 levels might be related to the presence of exfoliation material, or to the effects of other factors, unaccounted for in the present study. Second, our participants with XFG had been treated with antiglaucoma medications. It remains unknown if, and to what extent, IOP-lowering agents may have influenced ET-1 levels. Third, the determination of short PCA flow using CDI is inherently problematic. This happens because several of these arteries and the flow parameters we used in this study were based on the values derived from the PCAs that were technically easier to assess. Perhaps, a larger sample size would have limited measurement variability in these particular vessels.
Conclusions
Our results indicate that ET-1 aqueous levels in eyes with XFG are significantly higher than those of age-matched controls. In addition, our data portray a general pattern of reduced blood flow and increased vascular resistivity at least in the OA and in the CRA for eyes with XFG or XFS. We have also shown that ET-1 levels in eyes with XFG or XFS exhibit a significant correlation with CDI-derived hemodynamic parameters that indicate reduced perfusion.
Disclosure
The authors report no conflicts of interest in this work.
References
Yorio T, Krishnamoorthy R, Prasanna G. Endothelin: is it a contributor to glaucoma pathophysiology. J Glaucoma. 2002;1:259–270. | ||
Ritch R, Schlotzer-Schrehardt U. Exfoliation syndrome. Surv Ophthalmol. 2001;45:265–315. | ||
Holló G, Katsanos A, Konstas A. Management of exfoliative glaucoma: challenges and solutions. Clin Ophthalmol. 2015;9:907–919. | ||
Sekeroglu MA, Bozkurt B, Irkec M, Ustunel S, Orhan M, Saracbasi O. Systemic associations and prevalence of exfoliation syndrome in patients scheduled for cataract surgery. Eur J Ophthalmol. 2008;18:551–555. | ||
Andrikopoulos G, Mela EK, Georgakopoulos CD, et al. Pseudoexfoliation syndrome prevalence in Greek patients with cataract and its association to glaucoma and coronary artery disease. Eye (Lond). 2009;23:442–447. | ||
Ritch R, Prata T, Gustavo C, et al. Association of exfoliation syndrome and central retinal vein occlusion: an ultrastructural analysis. Acta Ophthalmol. 2010;88:91–95. | ||
Inoue A, Yanagisawa M, Kimura S, et al. The human endothelin family: three structurally and pharmacologically distinct isopeptides predicted by three separate genes. Proc Natl Acad Sci. 1989;86:2863–2867. | ||
Lepple-Wienhues A, Becker M, Stahl F, et al. Endothelin-like immunoreactivity in the aqueous humour and in conditioned medium from cultured ciliary epithelial cells. Curr Eye Res. 1992;11:1041–1046. | ||
Sugiyama K, Haque MS, Okada K, Taniguchi T, Kitazawa Y. Intraocular pressure response to intravitreal injection of endothelin-1 and the mediatory role of ETa receptor, ETb receptor and cyclooxygenase products in rabbits. Curr Eye Res. 1995;14:479–486. | ||
Orgul S, Cioffi GA, Bacon DR, Van Buskirk EM. An endothelin-1 induced model of chronic optic nerve ischemia in rhesus monkeys. J Glaucoma. 1996;5:135–138. | ||
Cioffi GA, Orgül S, Onda E, Bacon DR, Van Buskirk EM. An in vivo model of chronic optic nerve ischemia: the dose-dependent effects of endothelin-1 on the optic nerve microvasculature. Curr Eye Res. 1995;14:1147–1153. | ||
Williamson TH, Harris A. Color Doppler ultrasound imaging of the eye and orbit. Surv Ophthalmol. 1996;40:225–267. | ||
Quaranta L, Harris A, Donato F, et al. Color Doppler imaging of ophthalmic artery blood flow velocity: a study of repeatability and agreement. Ophthalmology. 1997;104:653–658. | ||
Giovagnorio F, Quaranta L. Power Doppler sonography enhances visualization of orbital vessels. J Ultrasound Med. 1995;14(11):837–842. | ||
Galassi F, Giambene B, Menchini U. Ocular perfusion pressure and retrobulbar haemodynamics in pseudoexfoliative glaucoma. Graefes Arch Clin Exp Ophthalmol. 2008;246:411–416. | ||
Detorakis ET, Achtaropoulos AK, Drakonaki EE, Kozobolis VP. Hemodynamic evaluation of the posterior ciliary circulation in exfoliation syndrome and exfoliation glaucoma. Graefes Arch Clin Exp Ophthalmol. 2007;245:516–521. | ||
Quaranta L, Katsanos A, Russo A, Riva I. 24-hour intraocular pressure and ocular perfusion pressure in glaucoma. Surv Ophthalmol. 2013;58:26–41. | ||
European Glaucoma Society. Terminology and Guidelines for Glaucoma. 4th ed. Savona: PubliComm; 2014. | ||
Koliakos GG, Konstas AGP, Schlotzer-Schrehardt U. Endothelin-1 concentration is increased in the aqueous humour of patients with exfoliation syndrome. Br J Ophthalmol. 2004;88:523–527. | ||
Holló G, Lakatos P, Farkas K. Cold pressor test and plasma endothelin-1 concentration in primary open-angle and capsular glaucoma. J Glaucoma. 1998;7:105–110. | ||
Visontai Z, Merisch B, Kollai M, Holló G. Increase of carotid artery stiffness and decrease of baroreflex sensitivity in exfoliation syndrome and glaucoma. Br J Ophthalmol. 2006;90:563–567. | ||
Visontai Z, Horvath T, Kollai M, Holló G. Decreased cardiovagal regulation in exfoliation syndrome. J Glaucoma. 2008;17:133–138. | ||
Repo LP, Suhonen MT, Terasvirta ME, Koivisto KJ. Color Doppler imaging of the ophthalmic artery blood flow spectra of patients who have had a transient ischemic attack. Correlations with generalized iris transluminance and exfoliation syndrome. Ophthalmology. 1995;102:1199–1205. | ||
Yuksel N, Karabas VL, Demirci A, Arslan A, Altintas O, Caglar Y. Comparison of blood flow velocities of the extraocular vessels in patients with exfoliation or primary open-angle glaucoma. Ophthalmologica. 2001;215:424–429. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.