Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Retinal Microvascular Diameters are Associated with Diabetic Kidney Disease in Patients with Type 2 Diabetes Mellitus
Authors Feng J, Xie X, Teng Z, Fei W, Zhen Y ![]() , Liu J, Yang L
, Liu J, Yang L ![]() , Chen S
, Chen S
Received 4 April 2023
Accepted for publication 13 June 2023
Published 21 June 2023 Volume 2023:16 Pages 1821—1831
DOI https://doi.org/10.2147/DMSO.S415667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Jing Feng,1– 3 Xiaohua Xie,4 Zhenjie Teng,4,5 Wenjie Fei,1,2 Yunfeng Zhen,2 Jingzhen Liu,2 Liqun Yang,2 Shuchun Chen1– 3
1Department of Endocrinology, Hebei Medical University, Shijiazhuang, Hebei Province, People’s Republic of China; 2Department of Endocrinology, Hebei General Hospital, Shijiazhuang, Hebei Province, People’s Republic of China; 3Hebei Key Laboratory of Metabolic Disease, Shijiazhuang, Hebei Province, People’s Republic of China; 4Department of Neurology, Hebei General Hospital, Shijiazhuang, Hebei Province, People’s Republic of China; 5Department of Neurology, Hebei Medical University, Shijiazhuang, Hebei Province, People’s Republic of China
Correspondence: Shuchun Chen, Department of Endocrinology, Hebei General Hospital, 348 Heping West Road, Shijiazhuang, Hebei Province, 050051, People’s Republic of China, Tel/Fax +86 31185988406, Email [email protected]
Objective: To investigate the association between retinal microvascular diameters and diabetic kidney disease (DKD) in patients with type 2 diabetes mellitus (T2DM).
Methods: A total of 690 patients with T2DM were included in this retrospective study. Patients were divided into DKD and non-DKD groups according to urine microalbumin/creatinine ratio and estimated glomerular filtration rate. Retinal microvascular diameters were measured by the automated retinal image analysis system. Multivariate logistic regression analysis and restricted cubic splines were used to assess the relationships between the retinal microvascular diameters and DKD in patients with T2DM.
Results: Multivariate logistic regression showed that widened diameters of retinal venules and narrowed diameters of retinal arterioles were associated with DKD after adjusting for potential confounding variables. There was a significant linear trend between the diameters of superior temporal retinal venula (P for trend < 0.001, P for non-linearity = 0.080), inferior temporal retinal venula (P for trend < 0.001, P for non-linearity = 0.111) and central retinal venular equivalent (CRVE) (P for trend < 0.001, P for non-linearity = 0.392) and risk of DKD in patients with T2DM. The restricted cubic splines showed that narrowed retinal arteriolar diameters, superior and inferior nasal retinal venulas were associated with the risk of DKD in a non-linear fashion (all P for non-linearity < 0.001).
Conclusion: Wider retinal venular diameters and narrower retinal arteriolar diameters were associated with an increased risk of DKD in patients with T2DM. Widened retinal venular diameters, especially CRVE, superior and inferior temporal retinal venula, were positively associated with an increased risk of DKD in a linear fashion. In contrast, narrowed retinal arteriolar diameters were associated with the risk of DKD in a non-linear fashion.
Keywords: diabetic kidney disease, type 2 diabetes mellitus, retinal venules, retinal arterioles, diameter
Introduction
Type 2 diabetes mellitus (T2DM) and its complications are a growing global public health problem.1 Approximately 537 million adults around the world have diabetes, and this number is expected to increase to a staggering 783 million by 2045.1,2 Diabetic kidney disease (DKD), a common and serious microvascular complication of diabetes, affects about 40% of people with diabetes.3,4 DKD is the leading cause of chronic kidney disease and end-stage renal disease and increases the risk of cardiovascular disease and mortality.3,5 Although the pathogenesis of DKD remains incompletely understood, damage to microvascular components, such as endothelial cells and podocytes, seems to be a pivotal factor.3,6
Researchers are working to reduce the global burden of DKD - a goal that depends on early detection of the disease.7 However, as the onset of DKD is asymptomatic and poor available biomarkers, early diagnosis is challenging.7,8 Like DKD, diabetic retinopathy (DR) is a primary microvascular complication of T2DM.9,10 The co-occurrence of DR and DKD suggests that the same risk factors and mechanisms, such as microvascular damage, may underlie the development of ocular and renal complications of T2DM.11–13 Moreover, as the eye shares strikingly similar structural, functional, developmental and genetic pathways with the kidney,13 DKD and DR may be closely related. Retinal microvascular visualization offers the possibility to study the systemic microvasculature in a non-invasive way. Retinal microvascular diameters are the most commonly and easily observed retinal microvascular parameters and may be early predictors of a microvascular disease.14
A meta-analysis has suggested that retinal microvascular diameters may predict future risk for chronic kidney disease development and progression.15 However, few studies have explored the relationship between retinal microvascular diameters and DKD. Therefore, this study aimed to explore the association of retinal microvascular diameters and DKD and to evaluate whether retinal microvascular diameter is a potential biomarker for the early detection of DKD in patients with T2DM.
Materials and Methods
Participants
The retrospective study included 690 eligible patients with T2DM who were admitted to Hebei General Hospital from January 2020 to December 2021. DKD was defined as estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 and/or urine microalbumin/creatinine ratio (UACR) ≥30 mg/g based on American Diabetes Association criteria.16 Inclusion criteria were as follows: diagnosis of T2DM based on World Health Organization criteria17 and completed more than one colour fundus photography in which the four main retinal venular or arteriolar trunks at the optic disc could be clearly defined. We excluded those with glaucoma, ametropia, uveitis, macular degeneration, cataract, diabetic ketoacidosis, diabetic hyperglycemic hyperosmolar state, acute cardiovascular and cerebrovascular diseases and end-stage renal disease. The process for patient selection is shown in Figure 1.
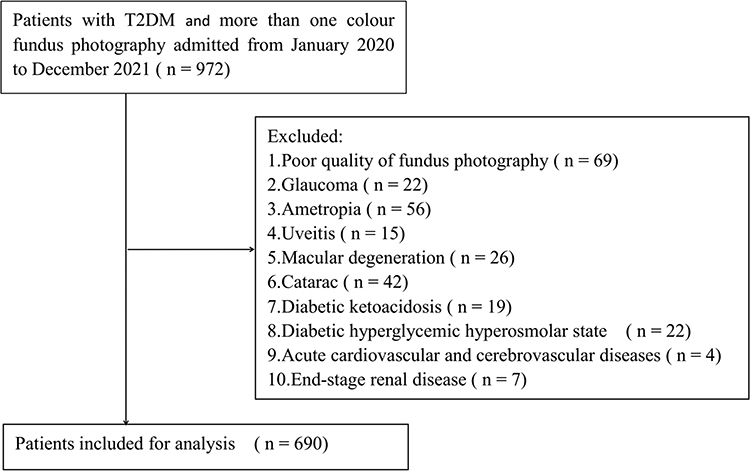 |
Figure 1 Flow chart of patient selection. Abbreviation: T2DM, type 2 diabetes mellitus. |
Clinical and Laboratory Assessments
Demographic characteristics (age, sex and body mass index) and medical history (hypertension and duration of T2DM) were collected from electronic databases or by interviewing patients. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured in a quiet environment. Hypertension was defined as SBP ≥140 mmHg or DBP ≥90 mmHg, previous diagnosis of hypertension or antihypertensive treatment. Fasting plasma glucose (FPG), blood urea nitrogen (BUN), serum creatinine (Scr), uric acid (UA), urine microalbumin, urine creatinine, total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C) and glycosylated haemoglobin (HbA1c) were measured in all patients after 8 hours of overnight fasting within two days of admission.
Measurement of Retinal Microvascular Diameters
A 45°Colour fundus photograph centred on the optic disc was taken in both eyes of all patients using a digital retinal camera (Canon CR-2 AF, Japan). Retinal microvascular diameters were measured from a fundus photograph of the right eye of each patient using an automated retinal image analyser (ARIA 1.0). The left eye was measured if the photograph of the right eye was ungradable. ARIA is software designed for the automated detection and measurement of retinal blood vessels. Retinal microvascular diameters were measured between one optic disc diameters and two optic disc diameter away from the central optic disc by two trained researchers who were blinded to the study. The diameters of the superior and inferior temporal retinal arterioles, superior and inferior nasal retinal arterioles, superior and inferior temporal retinal venulas, and superior and inferior nasal retinal venulas were recorded. Central retinal arteriolar equivalent (CRAE) and central retinal venular equivalent (CRVE) were calculated using the modified Knudtson-Parr-Hubbard formula.18,19
Statistical Analysis
Statistical analyses were performed using SPSS 26.0 (IBM Corporation, Armonk, NY) and R, version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were expressed as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables were expressed as the number of cases (percentage). Shapiro–Wilk test was used to test whether the variables were normally distributed. t-tests, Mann–Whitney U-tests, or chi-squared tests were used for different variables, as appropriate. Multivariate binary logistic regression models were used to investigate the association between retinal microvascular diameter and DKD in patients with T2DM. Tests for trend were conducted with using the quartiles of the retinal microvascular diameters as continuous variables by assigning the median values of the quartiles to the variable. The restricted cubic splines with four knot were used to test for possible non-linear relationships between the retinal microvascular diameters and DKD. P<0.05 was considered to be statistically significant.
Results
Participant Characteristics
A total of 690 eligible participants (435 males and 255 females) were included in this retrospective study. The median age of the enrolled participants was 57 years. All participants were stratified into two groups in accordance with the American Diabetes Association criteria:16 non-DKD group (n = 424) and DKD group (n = 266).
Table 1 shows the clinical and laboratory characteristics of participants between non-DKD group and DKD group. Participants in the DKD group had significantly longer duration of T2DM and more frequent hypertension than those in the non-DKD group (P<0.05). The DKD group presented higher SBP, body mass index, BUN, Scr, UA, and TG levels, but lower HDL-C than the non-DKD group (P<0.05).
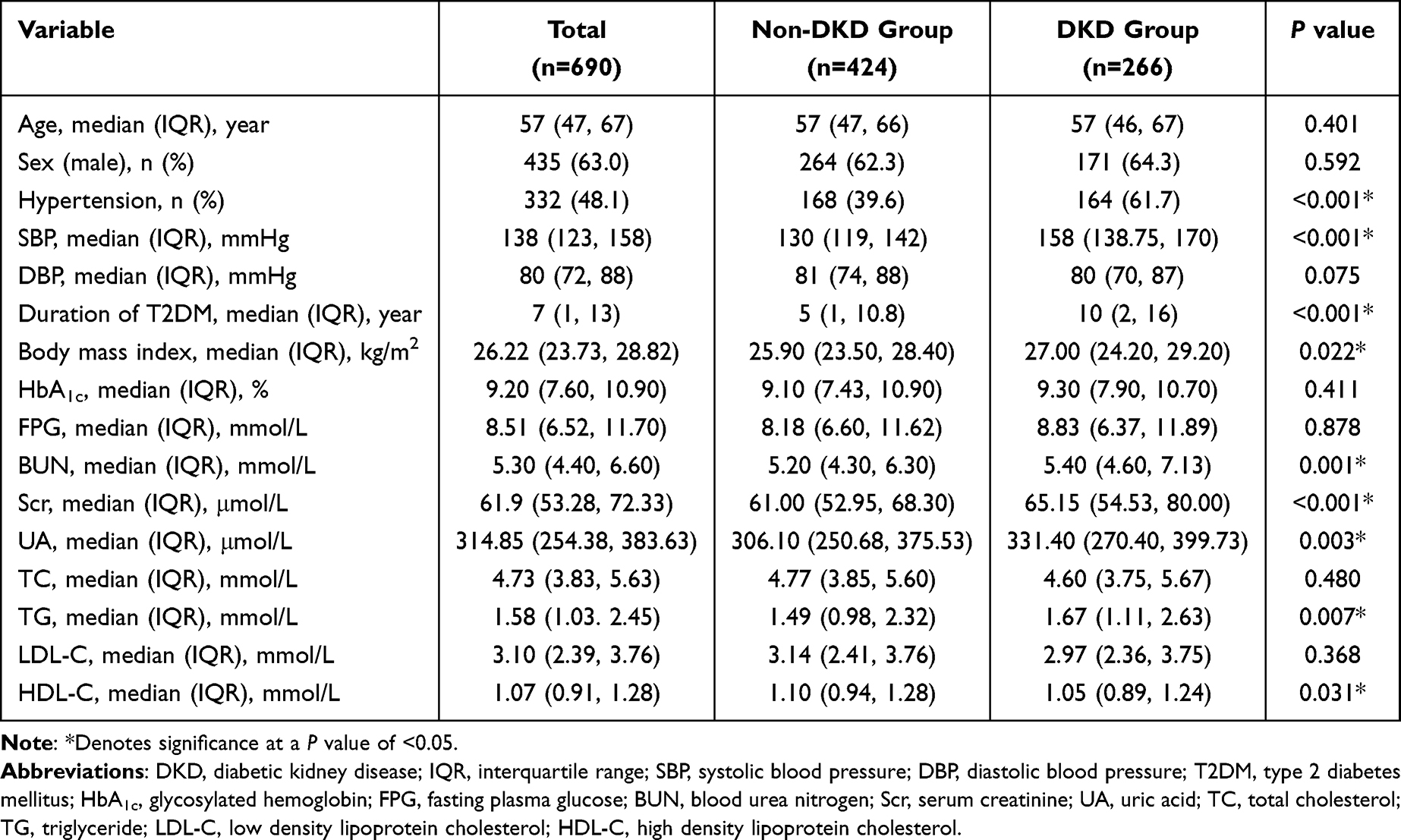 |
Table 1 Clinical and Laboratory Characteristics of Participants Between Non-DKD Group and DKD Group |
Retinal Venular Diameters and DKD
Participants with DKD showed significantly wider retinal venular diameters at the temporal superior, temporal inferior, nasal superior, nasal inferior and CRVE compared to the participants without DKD (P < 0.001) (Table 2). In univariate analysis, the widened diameters of all four retinal venules and CRVE were associated with DKD (odds ratio [OR]: 1.023, 95% confidence interval [CI]: 1.015 to 1.031, P<0.001; OR: 1.037, 95% CI: 1.028 to 1.046, P<0.001; OR: 1.038, 95% CI: 1.027 to 1.050, P<0.001; OR: 1.030, 95% CI: 1.019 to 1.041, P<0.001; OR: 1.041, 95% CI: 1.032 to 1.051, P<0.001; respectively) (Table 3). This trend remained statistically significant after adjusting for duration of T2DM, hypertension, SBP, DBP, BMI, TG, HDL-C, BUN, Scr and UA (temporal superior OR: 1.026, 95% CI: 1.016 to 1.036, P<0.001; temporal inferior OR: 1.034, 95% CI: 1.023 to 1.045, P<0.001; nasal superior OR: 1.029, 95% CI: 1.016 to 1.042, P<0.001; nasal inferior OR: 1.024, 95% CI: 1.012 to 1.038, P<0.001; CRVE OR: 1.038, 95% CI: 1.026 to 1.050, P<0.001) (Table 3).
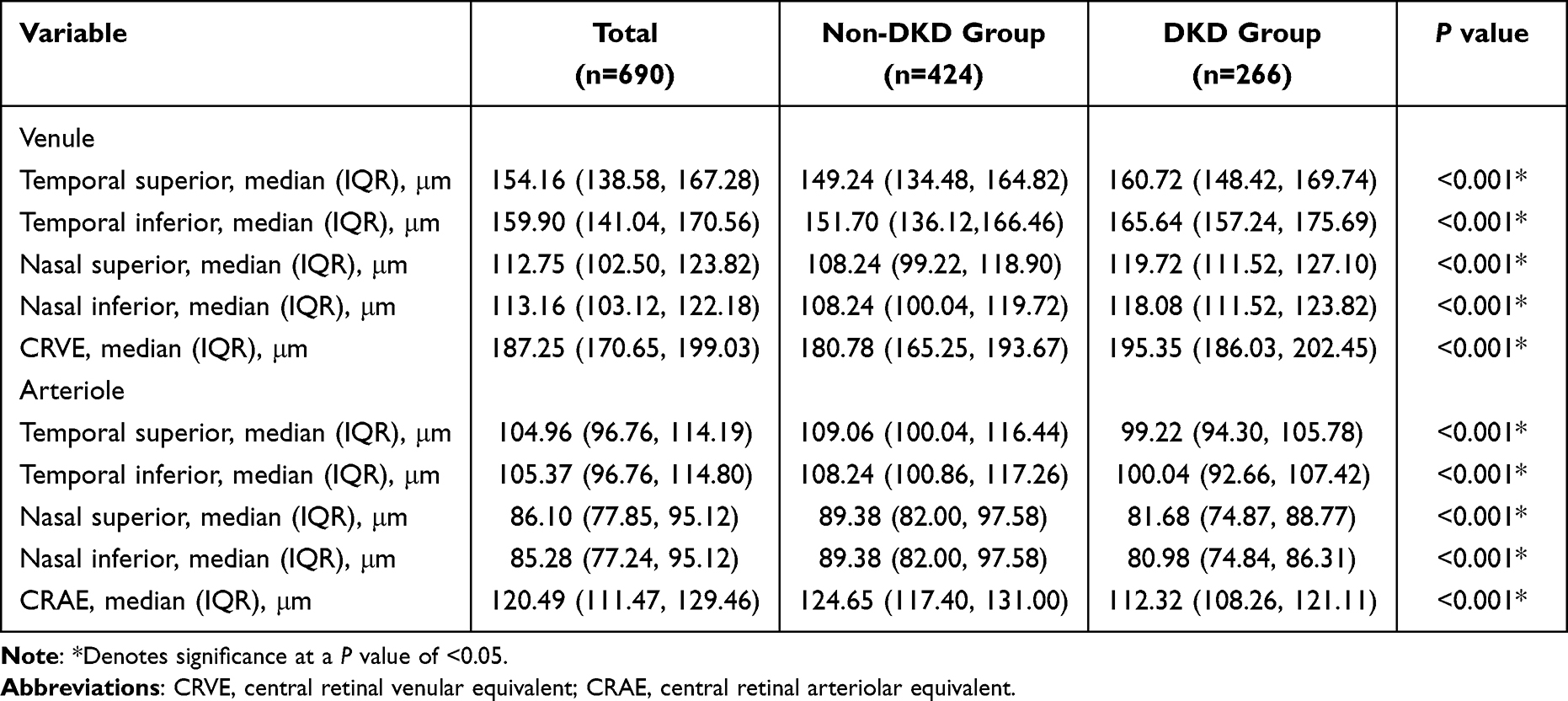 |
Table 2 Comparison of the Retinal Microvascular Diameters Between Non-DKD Group and DKD Group |
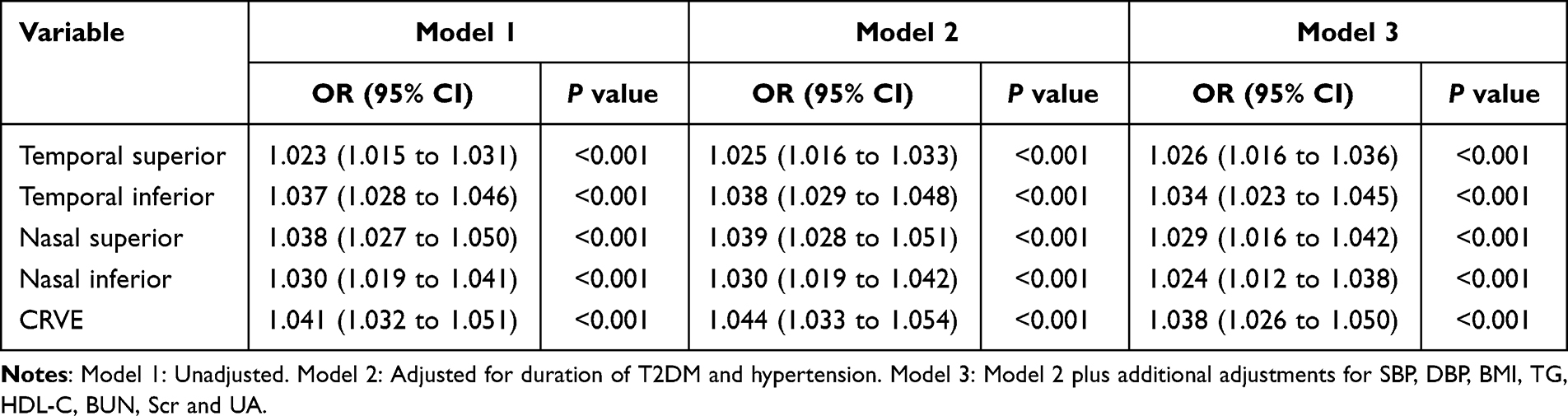 |
Table 3 The Logistic Regression Analyses Between Retinal Venular Diameters and DKD |
There was a significant linear trend between the diameters of superior temporal retinal venula (P for trend < 0.001, P for non-linearity = 0.080), inferior temporal retinal venula (P for trend < 0.001, P for non-linearity = 0.111) and CRVE (P for trend < 0.001, P for non-linearity = 0.392) and risk of DKD in patients with T2DM after adjusting for duration of T2DM, hypertension, SBP, DBP, BMI, TG, HDL-C, BUN, Scr and UA (Table 4 and Figure 2). The ORs of DKD of the highest quartile of superior temporal retinal venula, inferior temporal retinal venula and CRVE compared with the lowest were 3.831 (95% CI: 2.131 to 6.884), 6.936 (95% CI: 3.704 to 12.987) and 8.367 (95% CI: 4.379 to 15.988), respectively (Table 4). Figure 2C and D shows there was a nonlinear association between superior or inferior nasal retinal venulas and risk of DKD (P for non-linearity < 0.001). The ORs of DKD increased rapidly between around 113 and 134 µm of the diameters of superior nasal retinal venula and then plateaued thereafter (Figure 2C). The ORs of DKD increased rapidly between around 113 and 128 µm of the diameters of inferior nasal retinal venula and then decreased thereafter (Figure 2D).
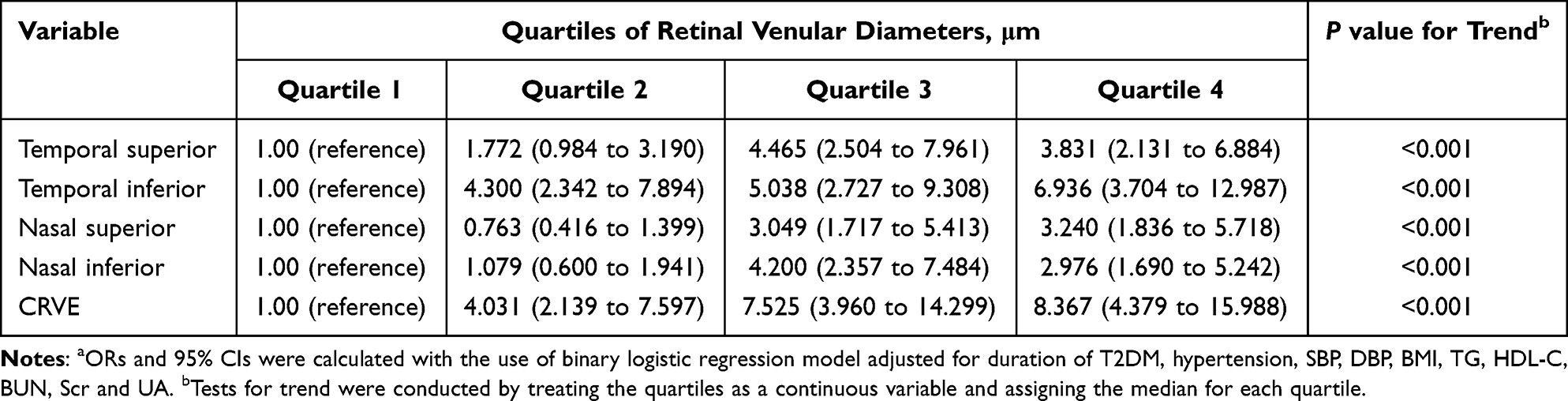 |
Table 4 ORs (and 95% CIs) of DKD According to Quartiles of Retinal Venular Diameter Levelsa |
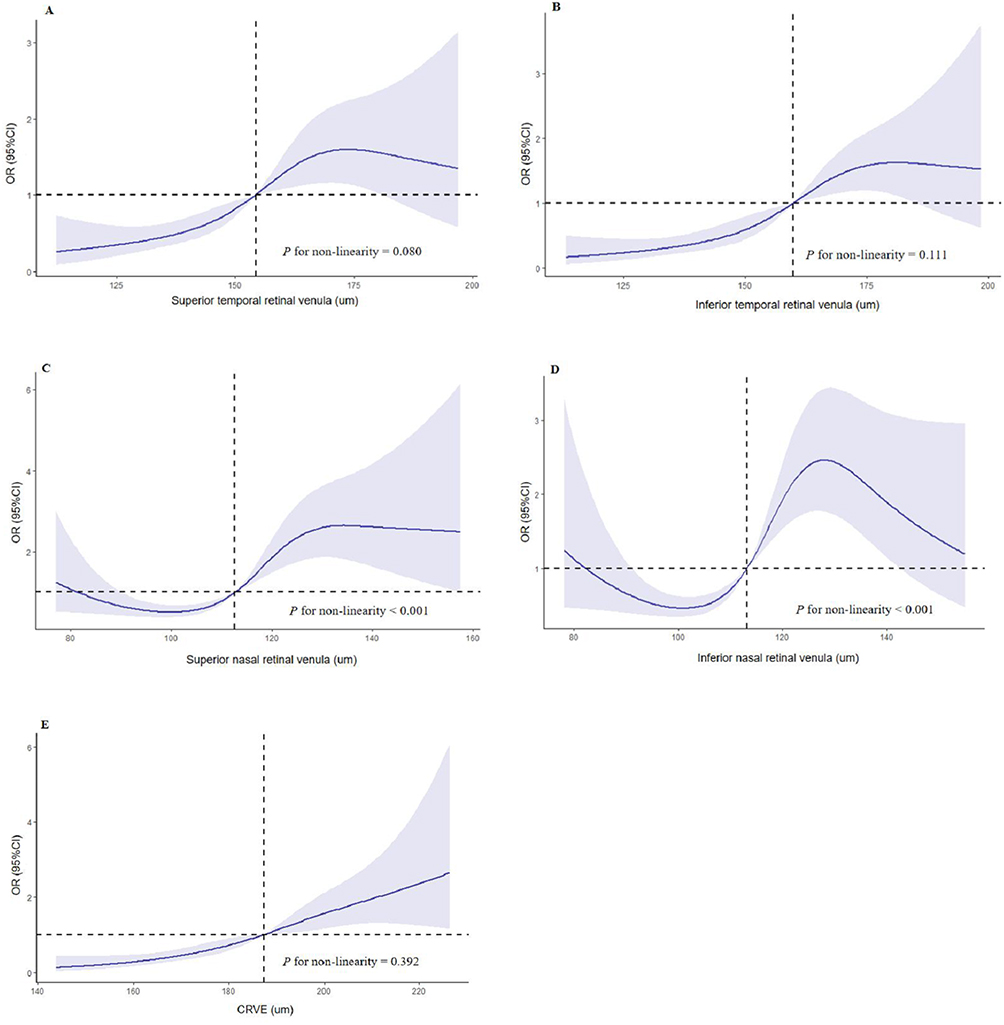 |
Figure 2 Restricted cubic splines for the association between retinal venular diameters and DKD. OR of DKD by the diameters of superior temporal retinal venula (A), inferior temporal retinal venula (B), superior nasal retinal venula (C), inferior nasal retinal venula (D) and CRVE (E) with the use of restricted cubic splines. The analysis was adjusted for duration of T2DM, hypertension, SBP, DBP, BMI, TG, HDL-C, BUN, Scr and UA. Abbreviation: CRVE, central retinal venular equivalent. |
Retinal Arteriolar Diameters and DKD
Participants with DKD had narrower retinal arteriolar diameters at the temporal superior, temporal inferior, nasal superior, nasal inferior and CRAE than participants without DKD (P < 0.001) (Table 2). In unadjusted logistic regression analysis, the narrowed diameters of all four retinal arterioles and CRAE were associated with DKD (P<0.001) (Table 5). This trend remained statistically significant after adjusting for duration of T2DM, hypertension, SBP, DBP, BMI, TG, HDL-C, BUN, Scr and UA (temporal superior OR: 0.984, 95% CI: 0.972 to 0.997, P = 0.015; temporal inferior OR: 0.986, 95% CI: 0.974 to 0.999, P = 0.035; nasal superior OR: 0.978, 95% CI: 0.964 to 0.993, P = 0.005; nasal inferior OR: 0.966, 95% CI: 0.951 to 0.981, P<0.001; CRAE OR: 0.971, 95% CI: 0.956 to 0.986, P<0.001) (Table 5).
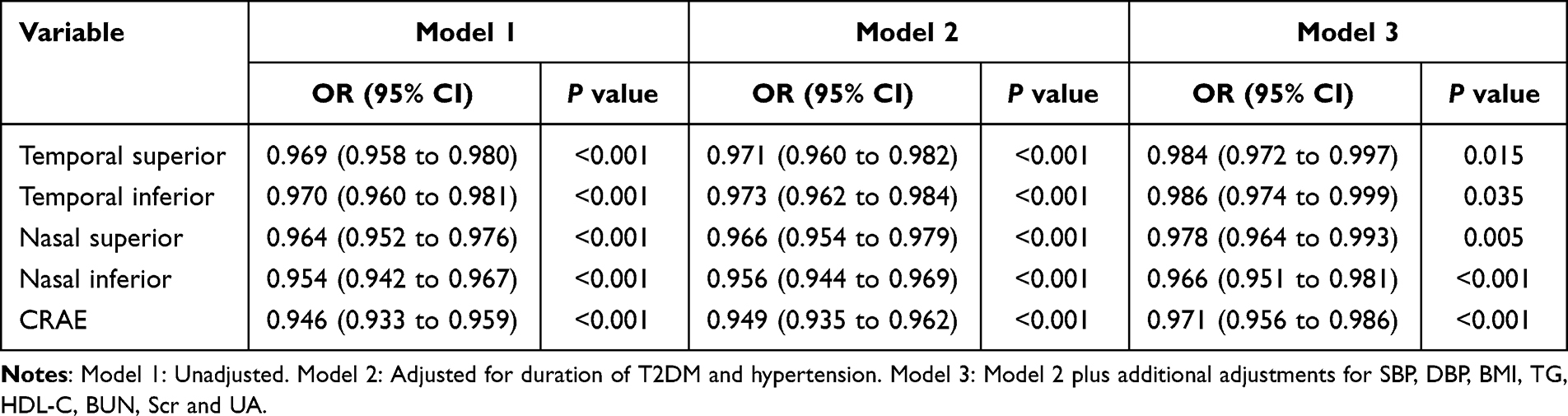 |
Table 5 The Logistic Regression Analyses Between Retinal Arteriolar Diameters and DKD |
Table 6 and Figure 3 show the association between retinal arteriolar diameters and DKD. The multivariable adjusted models showed the U-shaped relation between retinal arteriolar diameters (all P for non-linearity < 0.001) and DKD after adjusting for duration of T2DM, hypertension, SBP, DBP, BMI, TG, HDL-C, BUN, Scr and UA. The risk of DKD was increased when the diameters of superior nasal retinal arteriole was less than 105 µm after adjustment of potential confounders (Figure 3A). A similar nonlinear shape was also seen for the inferior temporal retinal arteriole (less than 105 µm, Figure 3B), superior nasal retinal arteriole (less than 86 µm, Figure 3C), inferior nasal retinal arteriole (less than 85 µm, Figure 3D) and CRAE (less than 120 µm, Figure 3E) association.
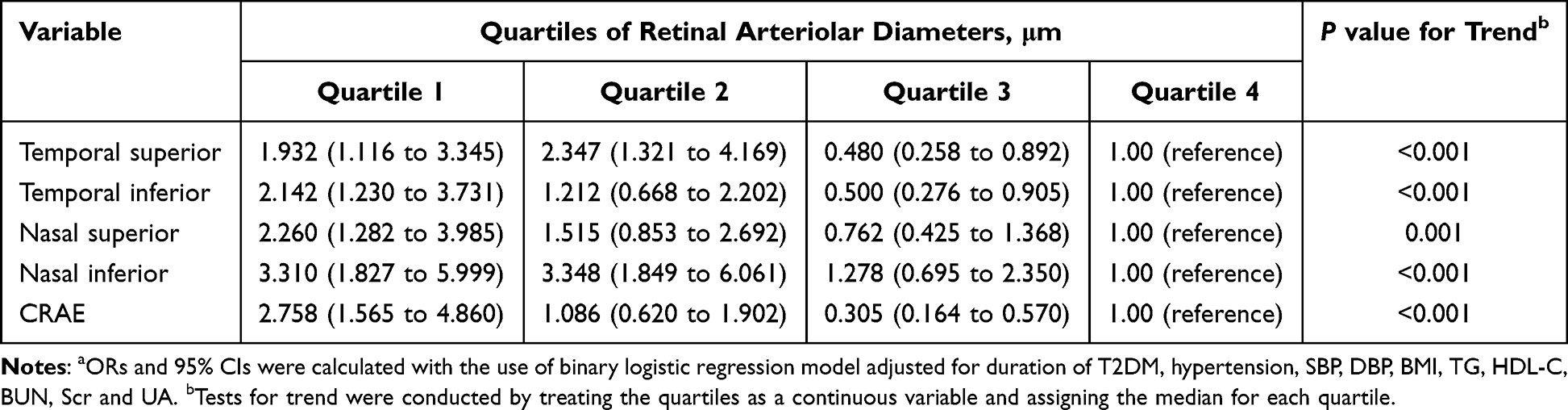 |
Table 6 ORs (and 95% CIs) of DKD According to Quartiles of Retinal Arteriolar Diameter Levelsa |
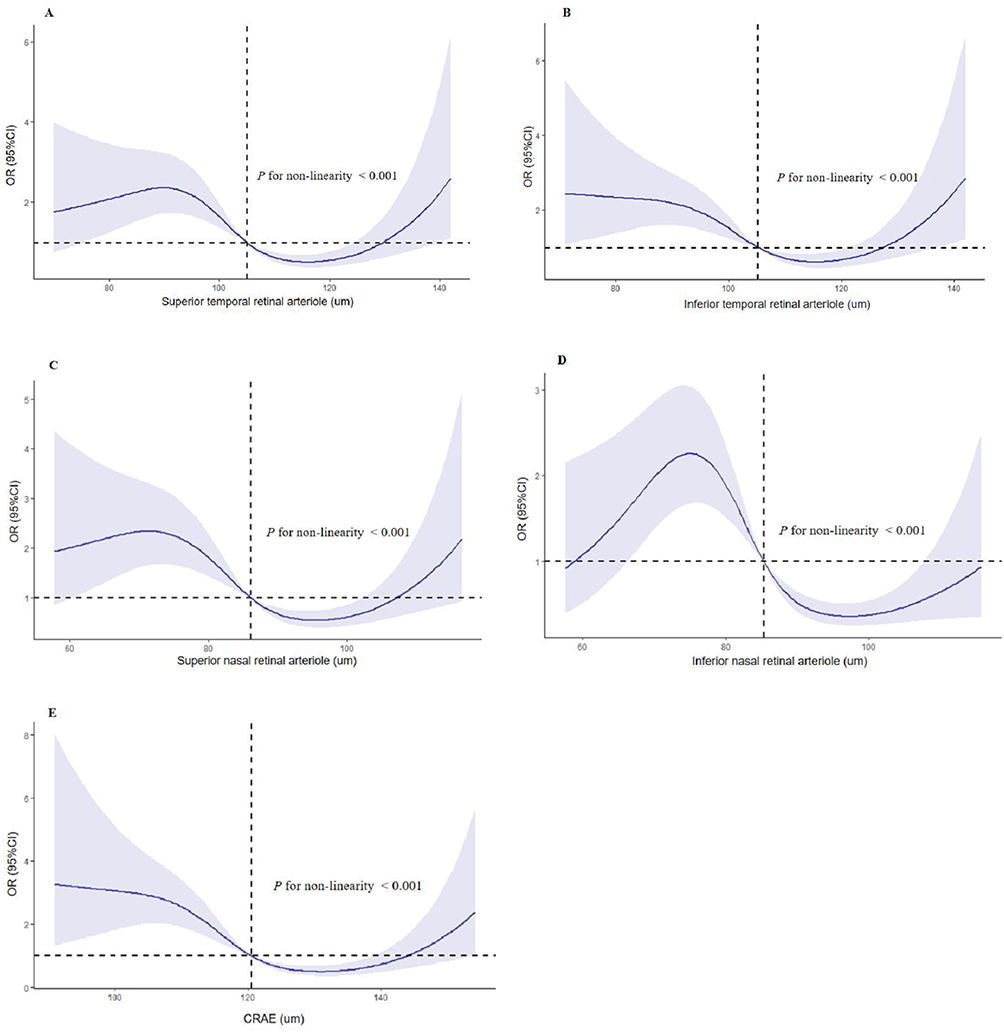 |
Figure 3 Restricted cubic splines for the association between retinal arteriolar diameters and DKD. OR of DKD by the diameters of superior temporal retinal arteriole (A), inferior temporal retinal arteriole (B), superior nasal retinal arteriole (C), inferior nasal retinal arteriole (D) and CRAE (E) with the use of restricted cubic splines. The analysis was adjusted for duration of T2DM, hypertension, SBP, DBP, BMI, TG, HDL-C, BUN, Scr and UA. Abbreviation: CRAE, central retinal arteriolar equivalent. |
Discussion
In this study, we investigated the association between retinal microvascular diameters and DKD in patients with T2DM. We found that wider retinal venular diameters and narrower retinal arteriolar diameters were associated with an increased risk of DKD. After adjustment for potential confounders, these associations remained significant. Furthermore, widened diameters of the superior temporal retinal venula, inferior temporal retinal venula and CRVE were positively associated with the risk of DKD in a linear manner. In contrast, narrowed retinal arteriolar diameters were associated with the risk of DKD in a non-linear manner, such that an exposure-response association was observed within a range of relatively small retinal arteriolar diameters.
Endothelial dysfunction is a key event in the pathogenesis of DKD.3,20 Exposure of endothelial cells to high glucose can activate the deleterious pathways, such as the polyol pathway, the protein kinase C pathway and the hexosamine pathway, leading to overproduction of endogenous reactive oxygen species and a worsening vicious cycle of inflammation, which play a direct role in DKD.3,20–22 It seems obvious to assess endothelial function in an accessible part of the microcirculation, as 90% of endothelial cells are located in the microcirculation.14 Importantly, the retina provides a unique window to non-invasively monitor microcirculation in vivo and is easy to visualize noninvasively.23,24 Changes in retinal microvascular diameter may be quantified as a subclinical marker of microvascular remodelling and dysfunction before clinical manifestation of DKD, as the retinal and renal microvasculature share similar anatomic and physiologic features.13,25
Retinal venular widening is a marker of retinal ischemia26 and may be mediated by endothelial dysfunction27 and increased inflammatory stress.28,29 Previous studies have suggested that wider CRVE was associated with incident chronic kidney disease30,31 and DKD.32,33 However, the population-based prospective study (BDES) found that chronic kidney disease was associated with a greater decrease rather than an increase in CRVE over time.34 Similarly, in another study, the CRVE was found to be negatively correlated with kidney function in a population without chronic kidney disease.35 In addition, some reported that CRVE were not associated with CKD.36–38 In our study, we found that wider CRVE was associated with an increased risk of DKD in patients with T2DM, consistent with a population-based prospective study.32 Moreover, we found a stronger association in the highest quartile of CRVE levels compared with the lowest and the levels of CRVE were positively associated with DKD in a linear manner, which suggested that increased diameter of the CRVE may accelerate the progression of DKD.
Retinal arteriolar narrowing is an indicator of microvascular dysfunction caused by aging, T2DM, hypertension, inflammation and other processes.39,40 Histopathologically, it is characterised by intimal thickening, medial hyperplasia, hyalinisation and sclerosis.41 The association between retinal arteriolar diameter and kidney disease is controversial. A prospective population-based study indicated that CRVE, but not CRAE, was associated with 14-year incidence of DKD.32 In contrast, a population-based study suggested that reduced CRAE, but not CRVE, was associated with chronic kidney disease.37 In addition, a recent meta-analysis found CRAE was associated with chronic kidney disease (OR: 1.41, 95% CI: 1.09 to 1.82).15 However, a risk estimation in previous studies depends on the assumption of a linear association. In our study, we observed that the OR for DKD was 2.758 for the lowest quartile of CRAE levels, but 0.305 for the third quartile compared with the highest. This observed pattern was further confirmed by our analysis of the association shape, which showed a U-shaped relation between CRAE levels and DKD. The result suggested that only the lower level of CRAE (less than 120 µm) was associated with an increased risk of DKD in patients with T2DM, which may partly explain the heterogeneity of previous studies.
Another major strength of our study, in comparison with previous studies, was the evaluation of the relationship between retinal branch microvascular diameter and the risk of DKD in patients with T2DM. To our knowledge, few studies have done this. In our study, we found that similar to CRVE, superior and inferior temporal retinal venular diameters were positively associated with the DKD in a linear manner, whereas superior and inferior nasal retinal venulas were associated with the DKD in a non-linear manner. Similar to CRAE, we found that a U-shaped relationship between four retinal branch arteriolar diameters and DKD. The results suggested that the smaller level of inferior temporal retinal arteriole (less than 105 µm), inferior temporal retinal arteriole (less than 105 µm), superior nasal retinal arteriole (less than 86 µm) and inferior nasal retinal arteriole (less than 85 µm) were associated with an increased risk of DKD in patients with T2DM. In conclusion, changes in retinal branch microvascular diameter may have potential clinical relevance for the risk of DKD.
The strength of our study is that we used retinal photography, a convenient and non-invasive technique, to explore the association between retinal microvascular diameters (including branch vessels) and DKD in patients with T2DM. There are several limitations in our study. First, it is a retrospective analysis. A cause–effect relationship could not be established. Longitudinal follow-up is desirable in the future to better understand the pathophysiological mechanisms of the early stages of DKD. Second, vascular geometry, such as arteriolar and venular fractal dimensions and vessel tortuosity, was not considered. However, the aim of this study is to evaluate whether retinal microvascular diameter is a potential biomarker for the detection of DKD in patients with T2DM. Third, the single-center design of our study may lead to a source of potential selection bias due to differences in ethnic factors. Large-scale longitudinal studies of retinal vessel diameter and DKD are warranted to address these issues.
Conclusions
In summary, our study demonstrated that widened retinal venular diameters, especially CRVE, superior and inferior temporal retinal venula, were positively associated with an increased risk of DKD in a linear fashion. In contrast, narrowed retinal arteriolar diameters are associated with the risk of DKD in a non-linear fashion, suggesting that only the lower level of retinal arteriolar diameters was associated with an increased risk of DKD in patients with T2DM. Our study supports that changes in retinal microvascular diameters (including branch vessels) were potential biomarkers for DKD in patients with T2DM. Retinal imaging may provide a non-invasive tool to identify patients with T2DM at risk for DKD.
Ethical Approval
The study followed the principles in the Declaration of Helsinki and was approved by the Ethical Committees of Hebei General Hospital (No.2022131). We promised that the data of the participants were anonymized or maintained with confidentiality, and the rights or interests of participants were not invaded. Therefore, the requirement for informed consent in this study was waived in accordance with the national legislation and the institutional requirements.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ahmad E, Lim S, Lamptey R, et al. Type 2 diabetes. Lancet. 2022;400(10365):1803–1820. doi:10.1016/S0140-6736(22)01655-5
2. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
3. Mohandes S, Doke T, Hu H, et al. Molecular pathways that drive diabetic kidney disease. J Clin Invest. 2023;133(4):e165654. doi:10.1172/JCI165654
4. Johansen KL, Chertow GM, Foley RN, et al. US renal data system 2020 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. 2021;77(4 Suppl 1):A7–A8. doi:10.1053/j.ajkd.2021.01.002
5. Tuttle KR, Jones CR, Daratha B, et al. Incidence of chronic kidney disease among adults with diabetes, 2015–2020. N Engl J Med. 2022;387(15):1430–1431. doi:10.1056/NEJMc2207018
6. Forbes JM, Cooper ME. Mechanisms of diabetic complications. Physiol Rev. 2013;93(1):137–188. doi:10.1152/physrev.00045.2011
7. Schmidt C. Confronting racial and ethnic disparities in diabetic kidney disease. Nature. 2023;615(7951):S8–S9. doi:10.1038/d41586-023-00651-8
8. Niewczas MA, Pavkov ME, Skupien J, et al. A signature of circulating inflammatory proteins and development of end-stage renal disease in diabetes. Nat Med. 2019;25(5):805–813. doi:10.1038/s41591-019-0415-5
9. Stitt AW, Curtis TM, Chen M, et al. The progress in understanding and treatment of diabetic retinopathy. Prog Retin Eye Res. 2016;51:156–186. doi:10.1016/j.preteyeres.2015.08.001
10. Mishriky BM, Cummings DM, Powell JR. Diabetes-related microvascular complications - a practical approach. Prim Care. 2022;49(2):239–254. doi:10.1016/j.pop.2021.11.008
11. Cankurtaran V, Inanc M, Tekin K, et al. Retinal microcirculation in predicting diabetic nephropathy in type 2 diabetic patients without retinopathy. Ophthalmologica. 2020;243(4):271–279. doi:10.1159/000504943
12. Wong TY, Coresh J, Klein R, et al. Retinal microvascular abnormalities and renal dysfunction: the atherosclerosis risk in communities study. J Am Soc Nephrol. 2004;15(9):2469–2476. doi:10.1097/01.ASN.0000136133.28194.E4
13. Wong CW, Wong TY, Cheng CY, et al. Kidney and eye diseases: common risk factors, etiological mechanisms, and pathways. Kidney Int. 2014;85(6):1290–1302. doi:10.1038/ki.2013.491
14. Hanssen H, Streese L, Vilser W. Retinal vessel diameters and function in cardiovascular risk and disease. Prog Retin Eye Res. 2022;91:101095. doi:10.1016/j.preteyeres.2022.101095
15. Aronov M, Allon R, Stave D, et al. Retinal vascular signs as screening and prognostic factors for chronic kidney disease: a systematic review and meta-analysis of current evidence. J Pers Med. 2021;11(7):665. doi:10.3390/jpm11070665
16. American Diabetes Association. Microvascular complications and foot care: standards of medical care in diabetes-2021. Diabetes Care. 2021;44(Suppl 1):S151–S167. doi:10.2337/dc21-S011
17. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
18. Knudtson MD, Lee KE, Hubbard LD, et al. Revised formulas for summarizing retinal vessel diameters. Curr Eye Res. 2003;27(3):143–149. doi:10.1076/ceyr.27.3.143.16049
19. Wong TY, Knudtson MD, Klein R, et al. Computer-assisted measurement of retinal vessel diameters in the Beaver Dam Eye Study: methodology, correlation between eyes, and effect of refractive errors. Ophthalmology. 2004;111(6):1183–1190. doi:10.1016/j.ophtha.2003.09.039
20. Lassen E, Daehn IS. Molecular mechanisms in early diabetic kidney disease: glomerular endothelial cell dysfunction. Int J Mol Sci. 2020;21(24):9456. doi:10.3390/ijms21249456
21. Jourde-Chiche N, Fakhouri F, Dou L, et al. Endothelium structure and function in kidney health and disease. Nat Rev Nephrol. 2019;15(2):87–108. doi:10.1038/s41581-018-0098-z
22. Salvatore T, Galiero R, Caturano A, et al. Coronary microvascular dysfunction in diabetes mellitus: pathogenetic mechanisms and potential therapeutic options. Biomedicines. 2022;10(9):2274. doi:10.3390/biomedicines10092274
23. Chaikijurajai T, Ehlers JP, Tang W. Retinal microvasculature: a potential window into heart failure prevention. JACC Heart Fail. 2022;10(11):785–791. doi:10.1016/j.jchf.2022.07.004
24. Liew G, Mitchell P, Wong TY, et al. Retinal microvascular signs are associated with chronic kidney disease in persons with and without diabetes. Kidney Blood Press Res. 2012;35(6):589–594. doi:10.1159/000339173
25. Lai S, Perrotta AM, Bagordo D, et al. Literature review on the cross-link between ocular and renal disease: renin angiotensin aldosterone system is a main actor. Eur Rev Med Pharmacol Sci. 2022;26(13):4774–4788. doi:10.26355/eurrev_202207_29203
26. de Jong FJ, Schrijvers EM, Ikram MK, et al. Retinal vascular caliber and risk of dementia: the Rotterdam study. Neurology. 2011;76(9):816–821. doi:10.1212/WNL.0b013e31820e7baa
27. Ikram MK, de Jong FJ, Vingerling JR, et al. Are retinal arteriolar or venular diameters associated with markers for cardiovascular disorders? The Rotterdam Study. Invest Ophthalmol Vis Sci. 2004;45(7):2129–2134. doi:10.1167/iovs.03-1390
28. Wong TY, Islam FM, Klein R, et al. Retinal vascular caliber, cardiovascular risk factors, and inflammation: the multi-ethnic study of atherosclerosis (Mesa). Invest Ophthalmol Vis Sci. 2006;47(6):2341–2350. doi:10.1167/iovs.05-1539
29. Klein R, Klein BE, Knudtson MD, et al. Are inflammatory factors related to retinal vessel caliber? The Beaver Dam Eye Study. Arch Ophthalmol. 2006;124(1):87–94. doi:10.1001/archopht.124.1.87
30. Yip W, Ong PG, Teo BW, et al. Retinal vascular imaging markers and incident chronic kidney disease: a prospective cohort study. Sci Rep. 2017;7(1):9374. doi:10.1038/s41598-017-09204-2
31. Grunwald JE, Pistilli M, Ying GS, et al. Retinopathy and the risk of cardiovascular disease in patients with chronic kidney disease (from the Chronic Renal Insufficiency Cohort study). Am J Cardiol. 2015;116(10):1527–1533. doi:10.1016/j.amjcard.2015.08.015
32. Klein R, Klein BE, Moss SE, et al. Retinal vessel caliber and microvascular and macrovascular disease in type 2 diabetes: XXI: the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Ophthalmology. 2007;114(10):1884–1892. doi:10.1016/j.ophtha.2007.02.023
33. Broe R, Rasmussen ML, Frydkjaer-Olsen U, et al. Retinal vessel calibers predict long-term microvascular complications in type 1 diabetes: the Danish Cohort of Pediatric Diabetes 1987 (DCPD1987). Diabetes. 2014;63(11):3906–3914. doi:10.2337/db14-0227
34. Myers CE, Klein R, Knudtson MD, et al. Determinants of retinal venular diameter: the Beaver Dam Eye Study. Ophthalmology. 2012;119(12):2563–2571. doi:10.1016/j.ophtha.2012.06.038
35. Daien V, Kawasaki R, Villain M, et al. Retinal vascular caliber is associated with renal function in apparently healthy subjects. Acta Ophthalmol. 2013;91(4):e283–e288. doi:10.1111/aos.12094
36. Sabanayagam C, Shankar A, Klein BE, et al. Bidirectional association of retinal vessel diameters and estimated GFR decline: the Beaver Dam CKD Study. Am J Kidney Dis. 2011;57(5):682–691. doi:10.1053/j.ajkd.2010.11.025
37. Sabanayagam C, Shankar A, Koh D, et al. Retinal microvascular caliber and chronic kidney disease in an Asian population. Am J Epidemiol. 2009;169(5):625–632. doi:10.1093/aje/kwn367
38. Keel S, Itsiopoulos C, Koklanis K, et al. Retinal vascular caliber and kidney function in children and adolescents with type 1 diabetes. Ophthalmic Epidemiol. 2017;24(3):204–208. doi:10.1080/09286586.2016.1267230
39. Sabanayagam C, Tai ES, Shankar A, et al. Retinal arteriolar narrowing increases the likelihood of chronic kidney disease in hypertension. J Hypertens. 2009;27(11):2209–2217. doi:10.1097/HJH.0b013e328330141d
40. Wong TY, Klein R, Klein BE, et al. Retinal microvascular abnormalities and their relationship with hypertension, cardiovascular disease, and mortality. Surv Ophthalmol. 2001;46(1):59–80. doi:10.1016/s0039-6257(01)00234-x
41. Wong TY, Klein R, Sharrett AR, et al. Retinal arteriolar narrowing and risk of coronary heart disease in men and women. The Atherosclerosis Risk in Communities Study. JAMA. 2002;287(9):1153–1159. doi:10.1001/jama.287.9.1153
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Serum Albumin Level and Microvascular Complications of Type 2 Diabetes Mellitus
Zhang J, Deng Y, Wan Y, He S, Cai W, Xu J
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2173-2182
Published Date: 23 July 2022
Effects of Glycemic Variability on Regulatory T Cells in Patients with Type 2 Diabetes and Kidney Disease
Gu QW, Sun Q, Wang J, Gu WS, Wang W, Mao XM
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2365-2375
Published Date: 8 August 2023
Sex Difference in the Association Between Serum Versican and Albuminuria in Patients with Type 2 Diabetes Mellitus
Li S, Li N, Li L, Zhan J
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3631-3639
Published Date: 11 November 2023
Association Between GGT/HDL-C Ratio and Diabetic Kidney Disease in Patients with Type-2 Diabetes Mellitus
Teng C, Lin H, Xu J, Wu X
Diabetes, Metabolic Syndrome and Obesity 2025, 18:4859-4871
Published Date: 31 December 2025