Back to Journals » Journal of Pain Research » Volume 19
Rethinking Pain Assessment: Subjective Scales, Biomarkers, and Multimodal Integration
Authors Liu A ![]() , Zhang L
, Zhang L ![]() , Xue E, Zhang C
, Xue E, Zhang C ![]() , Guo T, Wang J, Ming D
, Guo T, Wang J, Ming D
Received 17 April 2026
Accepted for publication 1 July 2026
Published 10 July 2026 Volume 2026:19 617733
DOI https://doi.org/10.2147/JPR.S617733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Aifeng Liu,1– 3,* Longyao Zhang,2,3,* Enyan Xue,2,3,* Chao Zhang,2,3 Tianci Guo,2,3 Jida Wang,2,3 Dong Ming1
1Tianjin International Joint Research Center for Neural Engineering, Academy of Medical Engineering and Translational Medicine, Medical School, Tianjin University, Tianjin, People’s Republic of China; 2Department of Orthopedics and Traumatology, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 3Department of Orthopedics and Traumatology, National Clinical Research Center for Chinese Medicine, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jida Wang, Department of Orthopedics and Traumatology, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China, Email [email protected] Dong Ming, Tianjin International Joint Research Center for Neural Engineering, Academy of Medical Engineering and Translational Medicine, Medical School, Tianjin University, Tianjin, People’s Republic of China, Email [email protected]
Abstract: Pain assessment is fundamental in pain medicine, anesthesiology, perioperative care, and clinical trials, yet it remains difficult to standardize across diseases, populations, and care settings. This review organizes pain assessment into four interrelated layers: subjective experience, behavioral and functional proxies, mechanistic biosignals, and multimodal integration. Pain characteristics guide many clinical decisions, but they must be interpreted alongside diagnosis, imaging, laboratory findings, treatment context, and regulatory expectations for reliable and interpretable trial endpoints. Patient-reported scales remain central when feasible because they directly capture the experienced dimension of pain; however, in neonates, critically ill patients, and individuals with severe cognitive or communication impairment, behavioral and functional proxies may become the practical baseline rather than merely supplementary measures. Recent advances in observational scales, facial-expression analysis, sleep and activity monitoring, wearable sensing, electroencephalography, neuroimaging, biofluids, autonomic physiology, and artificial intelligence provide complementary information for phenotyping, monitoring, prediction, and treatment evaluation. These tools should not be treated as interchangeable measures of the same construct or as simple replacements for self-report. A task-oriented layered framework may help clarify what each indicator can and cannot answer, while emphasizing feasibility, reproducibility, effect size, external validation, interpretability, and clinical context.
Keywords: pain assessment, subjective scales, pain biomarkers, neuroimaging, multimodal integration
Introduction
Pain assessment remains central to pain medicine, anesthesiology, perioperative care, rehabilitation, and clinical trials. Pain characteristics, including intensity, quality, temporal pattern, distribution, and functional interference, guide many diagnostic and therapeutic decisions, but they must be interpreted together with the underlying diagnosis, imaging findings, laboratory results, comorbidities, treatment exposure, and clinical context.1 In translational research and clinical trials, pain endpoints must also be reliable, interpretable, and clinically meaningful rather than merely statistically significant.2 These requirements reinforce the need for assessment strategies that are communicable, reproducible, and clinically actionable.
Pain is not a simple physiological variable, but a multidimensional experience shaped by nociceptive input, emotion, cognition, prior experience, sleep, sociocultural context, and disease background.3 Therefore, no single instrument can capture all clinically relevant dimensions of pain across all settings.4 This does not diminish the practical value of simple tools. In acute postoperative pain, emergency care, and routine ward assessment, unidimensional indicators such as the numerical rating scale may provide rapid and useful information for immediate clinical decisions.5,6 However, in chronic pain, neuropathic pain, nociplastic pain, cancer pain, and communication-limited populations, a single intensity score is often insufficient to characterize mechanisms, functional burden, longitudinal trajectory, or treatment response.7 This heterogeneity is also reflected in the ICD-11 classification of chronic pain and in the growing recognition of nociplastic pain and central sensitization as clinically relevant constructs.8–10
Patient-reported scales remain central when self-report is feasible because they directly capture the experienced dimension of pain and provide a shared language for clinician–patient communication.11 Their dominance, however, reflects both conceptual and practical factors: self-report is closest to the patient’s lived experience, while currently available objective measures remain limited by reproducibility, accessibility, standardization, specificity, and interpretability.12 In neonates, critically ill patients, sedated patients, and individuals with severe cognitive or communication impairment, subjective scales may be partially or entirely unavailable. In these settings, pain assessment often depends on behavioral and physiological observation, and validated tools such as neonatal pain scales or the Critical-Care Pain Observation Tool may become the practical assessment baseline.13–15
The relationship between subjective experience and objective measurement should therefore not be framed as a simple opposition between “inferior subjectivity” and “superior objectivity”. Objective and semi-objective methods already provide value in selected clinical and research contexts. Electrophysiological paradigms can support the study of nociceptive processing in neonatal, experimental, and neuropathic pain settings.16 Neuroimaging has contributed to the identification of pain-related brain signatures, central sensitization patterns, and treatment-response phenotypes.17 Wearable sensing and activity monitoring can capture sleep, movement, and recovery trajectories that are not fully represented by a single clinic-based pain score.18 Artificial intelligence-based models may further integrate heterogeneous signals for risk prediction, phenotyping, treatment monitoring, and decision support.19 The key issue is not whether an indicator is subjective or objective, but what construct it measures, under what conditions it is valid, and which clinical decision it can support.20,21
In this review, a “robust objective marker” refers to an indicator that is reproducible across relevant settings, has adequate individual-level performance, shows interpretable thresholds or decision rules, and can support clinical judgment for a defined task.22 A “gold standard” refers to a benchmark against which other tools are calibrated, whereas “ground truth” refers here to the patient’s pain experience as the ultimate clinical reference.12 These definitions are used for clarity within this review and should not be interpreted as universally accepted terminology. We organize pain assessment into four interrelated and overlapping layers: subjective experience, behavioral and functional proxies, mechanistic biosignals, and multimodal integration. The purpose of this layered framework is not to claim methodological novelty or to replace simpler tools, but to clarify how different indicators can be selected and combined according to clinical task, feasibility, reproducibility, interpretability, and translational value.23
Literature Search and Inclusion Principles
This review was designed as a clinically oriented narrative review rather than a formal systematic review. Literature was searched in PubMed, Web of Science, and Embase through April 2026, with priority given to English-language articles, high-quality reviews, systematic reviews, meta-analyses, consensus or framework statements, and representative original studies with clear clinical or translational relevance. Search domains included pain definitions and conceptual frameworks, subjective assessment tools, behavioral and functional proxies, electrophysiology, neuroimaging, biofluids, autonomic physiology, artificial intelligence–based multimodal integration, pain phenotyping, and barriers to clinical translation.
Study selection and interpretation were guided by clinical interpretability, methodological transparency, reproducibility, and translational relevance. In evaluating the literature, we considered not only statistical significance but also the magnitude and clinical meaning of reported effects, because effect size is essential for judging whether statistically detectable findings are likely to be clinically useful in pain research.2 The clinical-maturity labels presented in Table 1 and the scenario-based minimal assessment combinations shown in Table 2 represent author-derived synthesis judgments based on evidence consistency, standardization status, external validation, and implementation feasibility; they should not be interpreted as formal evidence grades.
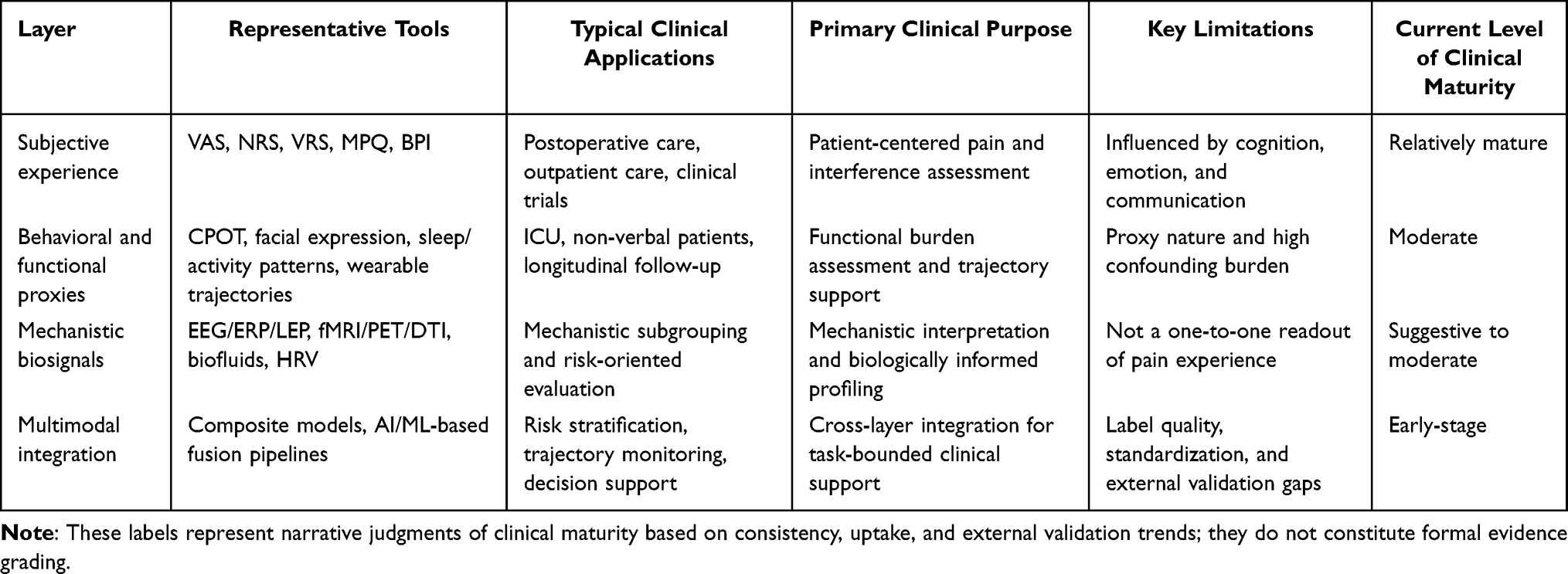 |
Table 1 Core Content of the Four-Layer Pain Assessment Framework and Current Level of Clinical Maturity |
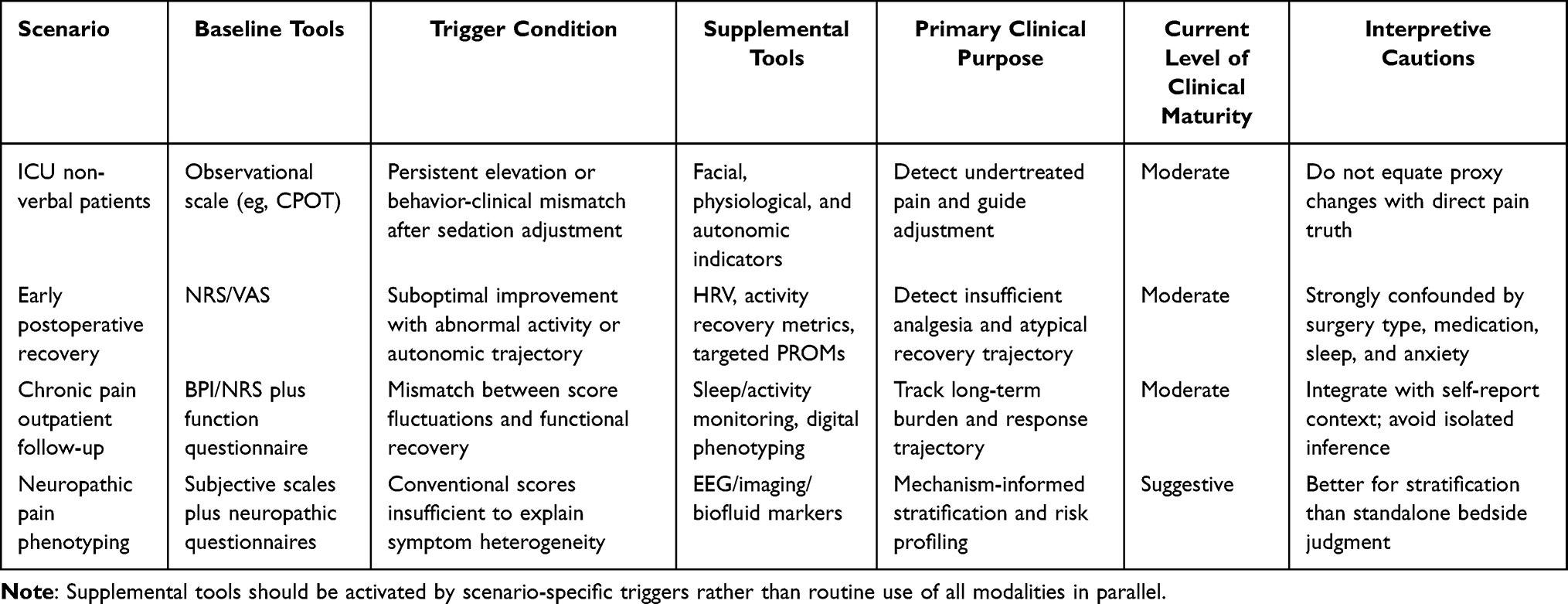 |
Table 2 Scenario-Based Suggested Minimal Assessment Combinations Across Clinical Settings |
A Clinical Layered Framework for Pain Assessment
From the perspective of pain medicine and anesthesiology, pain assessment is best understood as a coordinated set of tools operating at different levels of measurement rather than as a set of interchangeable indicators. The central value of a layered perspective is that it clarifies what each type of measure is designed to capture, thereby reducing conceptual overreach and clinical misinterpretation.21 This framework is not intended to rank subjective and objective methods hierarchically, but to match assessment tools with specific clinical tasks, patient populations, and implementation contexts.23 The overall structure of this task-oriented layered framework is summarized in Figure 1. This distinction is important because pain-related tools differ not only in objectivity, but also in measured construct, validation maturity, and workflow feasibility.24
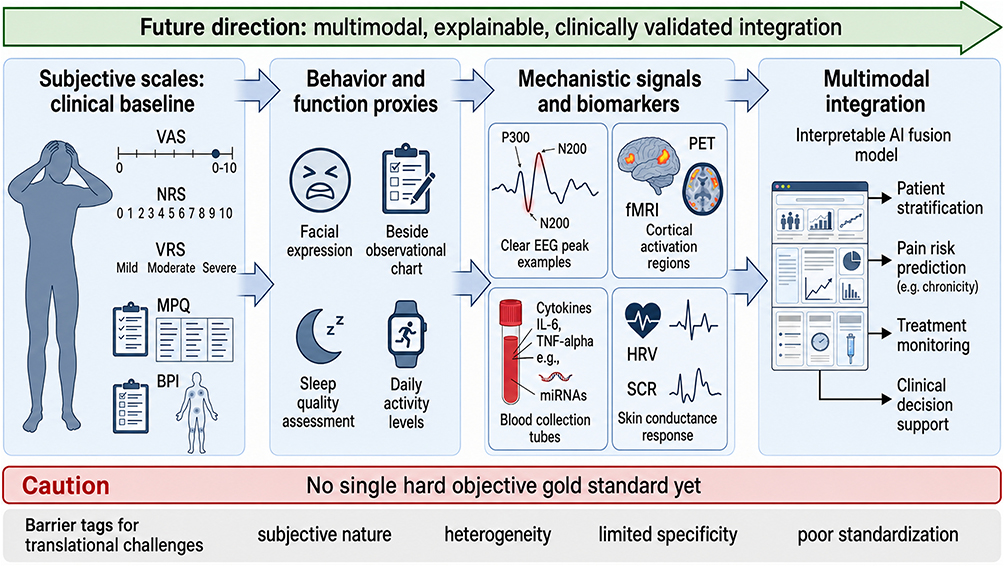 |
Figure 1 Four-layer clinical framework for pain assessment. Pain-related indicators can be grouped into four interrelated layers: subjective experience, behavioral and functional proxies, mechanistic biosignals, and multimodal integration. These layers are related but not interchangeable, and they should not be interpreted as measuring the same construct. When self-report is feasible, subjective scales remain the clinical baseline; when self-report is unavailable or unreliable, behavioral and functional proxies may become the practical baseline. Biosignal and integrative approaches provide complementary value for phenotyping, monitoring, prediction, treatment-response evaluation, and decision support. No single robust objective gold standard for pain assessment has yet emerged. |
Layer 1: Subjective Experience
The subjective experience layer centers on patient self-report and primarily includes the visual analogue scale (VAS), numerical rating scale (NRS), verbal rating scale (VRS), McGill Pain Questionnaire (MPQ), and Brief Pain Inventory (BPI).11 The selection of a self-report instrument should consider age, cognitive capacity, communication ability, and disease context, because measurement properties and usability vary across populations.25,26 When self-report is feasible, this layer remains central because it directly captures pain as experienced by the patient and provides an efficient language for clinical communication, treatment adjustment, and follow-up.5 However, its baseline role is context dependent rather than universal, because self-report may be unreliable or unavailable in neonates, critically ill patients, sedated patients, or individuals with severe cognitive or communication impairment.13,14
Layer 2: Behavioral and Functional Proxies
The behavioral and functional proxy layer includes observational pain scales, facial expression, pain-related behavior, activity monitoring, sleep rhythms, wearable devices, and digital phenotyping. These measures have been evaluated across ICU, pediatric critical care, general ward, and real-world activity-monitoring settings, supporting their role as context-specific tools rather than universally interchangeable indicators.27,28 Validated observational tools are especially relevant in critical care and other communication-limited settings, where direct self-report cannot be consistently obtained.13 Wearable sensing, sleep monitoring, and activity tracking can further capture real-world fluctuations in pain-related burden, recovery, and daily function that are not fully reflected by a single clinic-based pain score.18 This layer therefore supplements self-report when subjective scales are available and may become the practical assessment baseline when patients cannot provide stable self-report.
Layer 3: Mechanistic Biosignals
The mechanistic and biosignal layer encompasses electroencephalography (EEG), event-related potentials (ERP), laser-evoked potentials (LEP), functional magnetic resonance imaging (fMRI), positron emission tomography (PET), diffusion tensor imaging (DTI), inflammatory markers, endocrine measures, microRNAs, omics-based signatures, and heart rate variability (HRV), among others. These methods differ substantially in biological proximity to pain, ranging from stimulus-evoked neural responses and brain-network organization to immune, endocrine, molecular, and autonomic regulation.29–31 Neurophysiological paradigms can help characterize nociceptive processing and distinguish specific components of pain-related neural responses in selected experimental and clinical settings.16 Neuroimaging and biomarker studies can also support mechanistic interpretation, phenotyping, risk prediction, and treatment-response evaluation.17,22 The value of this layer lies mainly in explaining pain-related processing, disease context, systemic state, and interindividual heterogeneity rather than in producing a single biological substitute for subjective experience.
Layer 4: Multimodal Integration
The multimodal integration layer combines information from subjective scales, behavioral and functional proxies, mechanistic biosignals, and clinical context for clearly defined clinical tasks. These tasks may include patient stratification, risk identification, treatment monitoring, recovery assessment, phenotype recognition, and decision support.19 Remote wearable neuroimaging and digital monitoring approaches may further extend multimodal assessment beyond specialized laboratory settings, although their clinical maturity remains variable.32 The value of this layer is not only to prevent indicators from different sources from being treated as equivalent measures of the same construct,20 but also to identify latent or non-intuitive patterns that may not be apparent from any single modality alone.33 Broader reviews of artificial intelligence in pain medicine further support its potential for task-specific applications beyond simple data fusion.34
In practice, the four layers should be selected according to the clinical question rather than applied uniformly to every patient. Subjective scales are most useful when rapid communication and treatment adjustment are required.11 Behavioral and functional proxies are particularly important when self-report is unavailable or when real-world recovery needs to be monitored.13,18 Mechanistic biosignals are more relevant for phenotyping, mechanistic interpretation, prognostic evaluation, and treatment-response prediction.22 Multimodal integration becomes most useful when the target is risk prediction, subtype recognition, trajectory monitoring, or decision support.19 This task-specific logic is consistent with contemporary chronic pain care, in which lifestyle, rehabilitation, phenotyping, and monitoring are often combined rather than treated as isolated domains.35,36
Several dimensions should be considered when judging whether a pain indicator is clinically useful: feasibility in routine workflows;4 specificity and sensitivity in distinguishing pain-related variation from confounding factors such as sleep disturbance, anxiety, depression, fatigue, medication exposure, inflammatory activity, or disease severity;7 reproducibility and standardization of acquisition protocols, thresholds, algorithms, and cross-center performance;23 and interpretability and translational utility for stratification, monitoring, prediction, or treatment adjustment.19 Many emerging indicators remain confined to research not because they lack signal, but because these requirements are difficult to satisfy simultaneously.
Pain heterogeneity further supports a layered and task-oriented approach. Acute postoperative pain places a premium on speed, simplicity, and bedside usability, and a single intensity score may be sufficient for many immediate analgesic decisions.5 Chronic and nociplastic pain require broader coverage of functional interference, sleep, mood, central sensitization, and quality of life.37 Neuropathic pain places greater emphasis on mechanistic and phenotypic information, whereas inflammatory pain and cancer pain are often intertwined with systemic disease activity, treatment exposure, and complications.38 Because pain syndromes differ in mechanisms, trajectories, and decision priorities, indicators should be evaluated according to the clinical task, patient population, measurement context, and expected decision value.
Finally, clinical usefulness should be judged not only by statistical significance, but also by the magnitude and clinical meaning of observed effects. A statistically significant correlation does not necessarily imply clinical utility, particularly when effects are small, context dependent, or insufficiently reproducible. Current recommendations in pain research emphasize that effect size should be considered alongside statistical significance when interpreting findings and planning studies.2 Incorporating effect size can help determine whether an observed association is clinically meaningful, whether a model is likely to improve decision-making, and whether a candidate indicator is suitable for translation beyond the research setting.
Subjective Indicators
The Foundational Role of Subjective Scales
Subjective scales remain central to pain assessment because pain is ultimately experienced by the patient and cannot be fully inferred from external observation or machine-derived signals alone.3 Instruments such as the VAS, NRS, and VRS provide a simple, low-cost, and interpretable language for describing pain intensity.11 Their value is especially apparent in acute postoperative care, emergency settings, and routine ward assessment, where rapid and repeated evaluation is often required to guide analgesic adjustment.5 Similar self-report approaches have also been evaluated in dermatologic surgery, labor pain, and breastfeeding-related nipple pain, illustrating their practicality across diverse clinical contexts.39–41
The importance of subjective scales does not mean that they are universally sufficient. Their widespread use reflects both their proximity to the patient’s experience and the current limitations of alternative objective measures in accessibility, reproducibility, standardization, and interpretability.12 Multidimensional tools such as the MPQ and the BPI extend assessment beyond intensity by incorporating pain quality, emotional burden, functional interference, and impact on daily life.1 This broader coverage is particularly important in chronic pain, where clinical burden is often inadequately represented by a single intensity score. Disease- or condition-specific patient-reported tools further show that subjective assessment can be adapted to particular symptom profiles rather than limited to generic intensity scoring.42
Patient-reported measures are also closely aligned with outcomes that matter to patients and clinicians: pain severity, functional limitation, and perceived improvement after treatment. For this reason, they remain essential in pain studies and analgesic trials, even as neuroimaging, molecular biomarkers, wearable sensing, and artificial intelligence-based models continue to develop.24 The appropriate conclusion is therefore not that subjective scales are superior to all other indicators, but that they measure a clinically central dimension that other tools should complement rather than simply replace.
Common Scales and Their Clinical Applicability
Subjective assessment tools serve different clinical purposes. The VAS, NRS, and VRS are particularly useful for rapidly identifying current pain intensity and short-term change, making them suitable for repeated assessment after surgery, in emergency care, or during routine ward rounds.5 Their main strengths are speed, simplicity, familiarity, and direct relevance to immediate treatment decisions. Similar considerations have been reported in adult emergency medicine and other procedure- or condition-specific pain settings, where scale selection depends on clinical urgency, patient comprehension, and the dimension of pain being measured.6 However, these tools provide limited information about pain quality, mechanism, emotional meaning, or functional consequences.
By contrast, the MPQ emphasizes sensory and affective descriptors and is better suited to characterizing qualitative features of pain, especially in complex chronic pain states.1 The BPI combines pain severity with pain-related interference, making it more closely aligned with chronic disease management, longitudinal follow-up, and patient-reported outcomes in clinical trials.1 Condition- or context-specific assessments for labor pain, breastfeeding-related nipple pain, and movement-disorder-related pain further illustrate that subjective tools should be selected according to the clinical setting rather than treated as interchangeable scales.40–43 In practice, the key issue is whether the selected instrument matches the clinical question, patient population, and assessment setting.
Limitations of Subjective Scales and the Need for Complementation
The limitations of subjective scales define their boundaries rather than diminish their importance. In special populations, scale selection can substantially influence assessment quality. Older adults may face visual, auditory, memory, and comprehension burdens, making overly complex tools less usable in routine care.44 In neonates, verbal self-report is impossible, and assessment depends on behavioral and physiological observation; updated neonatal pain reviews further emphasize that scale choice should account for developmental stage, clinical context, and the limitations of observational items.14,45 In critically ill, mechanically ventilated, sedated, or communication-limited patients, self-report may also be unavailable or unreliable, and validated observational scales such as the Critical-Care Pain Observation Tool are often required.13
Subjective ratings are also influenced by clinically meaningful but methodologically challenging factors, including anxiety, catastrophizing, sleep disturbance, prior experience, cultural background, language, and clinician–patient interaction.25 Condition- and culture-adapted self-report instruments further show that subjective assessment may require contextual validation rather than direct transfer across populations.46 In chronic pain, reliance on a single intensity score may underestimate broader burdens involving sleep, activity, mood, social participation, and quality of life.7 Subjective scales should therefore be regarded as a necessary starting point when self-report is feasible, but not as a complete endpoint for all clinical and research questions.
A layered approach preserves the strengths of subjective scales while allowing complementary information from behavioral, functional, physiological, imaging, and molecular indicators. These tools may help identify pain when self-report is unavailable, characterize mechanisms, monitor recovery trajectories, and support phenotyping or risk prediction. The aim is not to replace subjective scales, but to compensate for their blind spots through task-specific and context-sensitive assessment.
Objective and Semi-Objective Indicators
Behavioral and Functional Proxy Measures
Behavioral and functional proxy measures are particularly important when patients cannot provide stable self-report or when continuous monitoring is needed. In critically ill, mechanically ventilated, sedated, delirious, cognitively impaired, very young, or older patients, direct pain report may be unavailable, unreliable, or difficult to interpret.44 In these contexts, tools such as the Critical-Care Pain Observation Tool (CPOT), behavioral pain scales, facial-expression analysis, actigraphy, sleep assessment, gait and activity monitoring, wearable devices, and digital phenotyping can provide information not captured by a single subjective rating.13,47
The clearest application is assessment in patients who cannot communicate pain reliably. In adult ICU patients, CPOT has shown clinically relevant diagnostic value and is widely used for nonverbal or mechanically ventilated patients.13 Similar behavioral frameworks have been evaluated in pediatric critical care and general ward settings, suggesting that observational pain assessment is not confined to a single environment.27,28 In these situations, the aim is not to infer an exact numeric pain intensity, but to reduce the risk of unrecognized suffering, guide analgesic or sedative adjustment, and monitor whether pain-related behaviors improve with clinical status.
Facial expression, pain-related behavior, activity, and movement-based measures extend assessment from verbal report to observable function. Artificial intelligence-based facial-expression analysis may help standardize visible pain-cue detection, although performance remains dependent on population, context, image quality, and training data.48 Actigraphy and movement monitoring can capture reduced mobility, avoidance behavior, gait changes, and recovery trajectories that may be missed during short clinical encounters.49 Smartphone and wearable technologies have also been applied after total knee arthroplasty and in rehabilitation settings, where activity volume, movement patterns, and adherence may help contextualize pain recovery.50 In musculoskeletal and rheumatologic populations, physical activity data may further help distinguish pain-related functional limitation from broader disability, fatigue, or disease activity.51
Sleep and circadian measures are particularly relevant in chronic pain and perioperative recovery. Pain can disturb sleep, while poor sleep may amplify pain sensitivity, emotional distress, and fatigue, creating a reciprocal cycle not captured by a single daytime score.52 Wearable and machine-learning approaches can characterize sleep–pain reciprocity and daily fluctuations in treatment response.18 Studies in temporomandibular disorders, rheumatoid arthritis, and Behçet’s syndrome further illustrate that sleep, fatigue, circadian rhythms, and pain-related burden are often interwoven across chronic inflammatory and musculoskeletal conditions.53–55 In postoperative and home-based recovery, wearable or smartphone-assisted monitoring may help identify delayed recovery, reduced activity, poor adherence, or persistent functional limitation after orthopedic procedures and exercise-based interventions.50,56,57
The main limitation of behavioral and functional proxies is limited specificity. Facial expression may be altered by sedation, fatigue, anxiety, cultural display rules, or social context; reduced activity may reflect depression, frailty, osteoarthritic degeneration, cardiopulmonary limitation, environmental restriction, or fear avoidance; and sleep fragmentation may be driven by insomnia, respiratory disturbance, medication exposure, inflammatory activity, or emotional distress.49,52 Thus, these indicators improve continuity and ecological validity but do not automatically improve specificity. Their most mature role is to identify possible pain when self-report is unavailable, characterize functional burden, and track recovery trajectories during postoperative care, chronic pain management, and rehabilitation.
EEG and Neurophysiological Indicators
EEG, ERP, and LEP are among the most developed neurophysiological approaches for studying pain because they provide millisecond-level temporal resolution and can capture neural responses close to nociceptive processing.29 Unlike behavioral proxies, these methods primarily characterize how nociceptive input is encoded, transmitted, attended to, and modulated within the nervous system. Their strongest value is mechanistic: they can help distinguish stimulus-evoked neural activity, attentional processing, affective salience, and longer-term alterations in brain rhythms or connectivity.
Different neurophysiological paradigms answer different questions. LEP is relatively close to nociceptive afferent activation and cortical processing after selective noxious stimulation, making it useful in painful radiculopathy and other neuropathic pain states.58 ERP paradigms can capture sensory, attentional, and affective-evaluative components of pain, which is particularly relevant in neonatal and experimental settings where verbal report is unavailable or limited.59 Resting-state EEG and MEG, by contrast, are more often used to examine chronic pain–related changes in oscillatory power, connectivity, vigilance, and network state rather than immediate pain intensity.60 Similar oscillatory and connectivity abnormalities have been reported in chronic low back pain with comorbid insomnia, supporting the view that resting neurophysiological signals may reflect pain-related network state, vigilance, and sleep-related modulation.61
Current evidence supports several task-specific applications. In neonates, noxious stimulus-evoked EEG or ERP responses may provide complementary physiological endpoints for analgesic efficacy, although further validation of reliability, interpretability, and clinical meaning is still required.16 In neuropathic and musculoskeletal pain, resting-state EEG findings, brain and spinal cord adaptations, and spinal cord injury–related EEG signatures suggest a role in mechanism-oriented phenotyping rather than routine diagnosis.62–64 Experimental work on nociceptive-evoked gamma-band oscillations and neurophysiological studies of analgesic interventions, such as transcutaneous electrical nerve stimulation, further indicate that these signals can be useful for probing pain modulation mechanisms and treatment-related neural responses.65,66
The limitation of EEG, ERP, and LEP is therefore not that they are unrelated to pain, but that their interpretation depends strongly on the paradigm, population, timing of assessment, and targeted outcome. A LEP abnormality may indicate altered nociceptive pathway function; an ERP change may reflect salience, attention, or affective processing; and resting EEG alterations may reflect chronic network reorganization, sleep disturbance, medication effects, or comorbidity. Routine clinical translation is further limited by heterogeneous stimulus parameters, electrode montages, preprocessing pipelines, artifact correction, frequency-band definitions, and source-localization methods.67 Even when group-level differences are statistically significant, individual-level thresholds and cross-center reproducibility often remain insufficient for bedside decision-making. In conditions such as fibromyalgia, neuromodulation studies suggest that neurophysiological and network-level measures may help evaluate treatment-related modulation, but they remain adjunctive rather than diagnostic tools.68
Neuroimaging Indicators
Neuroimaging has continued to attract attention in pain research because it can localize pain-related processing across brain networks, connectivity patterns, white-matter pathways, and neurotransmitter systems. fMRI, resting-state functional connectivity, PET, and diffusion-based MRI have shown abnormalities involving the default mode network, salience network, sensorimotor regions, limbic circuits, and descending modulatory pathways across different chronic pain conditions.17,69 These findings support the view that chronic pain is not only a peripheral sensory problem, but also a state involving central network reorganization, altered affective-salience processing, and impaired endogenous modulation.70
A key contribution of neuroimaging is that it moves pain research beyond single-region explanations. Resting-state fMRI meta-analyses have identified common neural correlates across chronic pain conditions, whereas neuropathic pain studies emphasize both regional and interregional abnormalities.71,72 PET studies extend this framework by examining neurotransmitter systems, neuroinflammation, and disease-specific tissue activity.73,74 PET-based approaches may also provide disease-context information in aging-related muscle disorders, myositis, pain states, and peripheral neuropathies.75 Other imaging approaches have been applied in musculoskeletal pain, osteoarthritis, post-traumatic headache, and migraine, illustrating that imaging findings are shaped by pain subtype, comorbidity, tissue pathology, and intervention context rather than by a uniform pain signature.76–79
It is important not to overstate the separation between neuroimaging and pain intensity. Although single imaging features rarely provide a one-to-one readout of subjective pain, multivariate predictive models and pain signatures have demonstrated meaningful associations with experimentally evoked or patient-reported pain.80 Placebo-imaging work further shows that brain signatures can be modulated by expectation, treatment context, and analgesic response, indicating that neuroimaging may capture clinically relevant components of pain modulation.81 The limitation is therefore not that neuroimaging is unrelated to pain, but that its meaning depends on task design, disease context, model construction, and the level of prediction being claimed. This context dependence is also evident in depression-related pain, where functional neuroimaging findings may reflect interactions among pain processing, affective state, and broader psychopathology.82
Neuroimaging is increasingly relevant to personalized medicine and treatment-response research. Functional connectivity and brain-network studies have been used to explore response heterogeneity after interventions such as brain stimulation, acupuncture, motor-control exercise, and rehabilitation.83–85 Changes in periaqueductal gray connectivity in knee osteoarthritis pain, altered connectivity after motor-control exercise in chronic low back pain, static and dynamic connectivity abnormalities, and resilience-related neural features in juvenile fibromyalgia all suggest that imaging may help identify mechanistic targets and response phenotypes.85–88 These applications are more clinically plausible than using neuroimaging as a universal diagnostic substitute.
At present, the strongest role of neuroimaging is mechanistic stratification, phenotype refinement, treatment-response research, and selected prediction tasks. Its routine use as a bedside pain measure remains limited by cost, workflow complexity, accessibility, protocol heterogeneity, motion and medication effects, and variable individual-level performance. Predictive models also face risks of overfitting, sampling bias, and limited external validation, especially when developed in small or single-center datasets.17 Neuroimaging should therefore be interpreted as a powerful mechanistic and predictive component within a multimodal assessment framework rather than as a stand-alone replacement for patient self-report.
Blood and Fluid Biomarkers
Blood and fluid biomarkers are attractive in pain research because they are relatively accessible and can reflect inflammatory, endocrine, neuroimmune, metabolic, and omics-level changes that are not captured by symptom ratings alone.30 Cytokines, chemokines, cortisol, neuropeptides, metabolites, microRNAs, exosomes, proteomic profiles, and metabolomic signatures have all been investigated as candidates for explaining pain mechanisms, identifying disease subtypes, or predicting pain persistence. Chemokine pathways such as CXCL13/CXCR5 further support the relevance of immune-signaling biomarkers in mechanism-oriented pain research.89 Their value is particularly apparent when pain is closely linked to systemic inflammation, immune activation, endocrine disturbance, or tissue pathology, as illustrated by immuno-inflammatory mechanisms of pain chronification and disease-specific examples such as frozen shoulder.90,91
The main limitation of a single blood or fluid marker is limited specificity. Inflammatory and endocrine mediators in endometriosis or arthritis may reflect disease activity, immune background, hormonal regulation, or tissue injury rather than pain intensity itself.92–94 Cortisol-related findings in fibromyalgia similarly point to stress-system dysregulation but cannot be interpreted as a direct measure of momentary pain severity.95 Thus, the weakness of fluid biomarkers is not the absence of biological signal, but the difficulty of assigning that signal specifically to pain rather than to comorbidity, medication exposure, systemic stress, or underlying disease activity.
Recent work has therefore shifted from single-marker interpretation toward multi-marker panels and systems-based approaches. Epigenetic and microRNA studies suggest that chronic pain states may involve broader regulatory changes rather than isolated molecular abnormalities.96 Exosome-mediated miRNA signaling, omics-based biomarker research, chronic gastrointestinal miRNA mechanisms, calcium-channel biology, and aging-related molecular findings in neuropathic pain further illustrate how molecular profiles may inform mechanisms, risk prediction, and treatment development across selected pain contexts.23,97–100
Clinically, fluid biomarkers are most useful when interpreted within disease-specific and task-specific contexts. In inflammatory pain, they may help distinguish inflammatory activity from non-inflammatory pain amplification; in neuropathic pain, they may support mechanism-oriented stratification or identify pathways relevant to chronification; and in chronic widespread, nociplastic, or aging-related pain, they may help characterize neuroimmune, stress-related, or comorbidity-linked phenotypes.91,95,101 The absence of a single robust biomarker does not preclude the objectivisation of pain, because many clinical conditions are diagnosed and monitored using combinations of clinical features, laboratory findings, imaging results, and treatment response. However, translation requires standardized sampling, validated assay platforms, defined decision rules, adequate effect-size interpretation, and external validation across disease groups and clinical settings.23,30 Blood and fluid biomarkers are therefore best positioned as mechanistic and stratification tools that add biological context to pain assessment.
Autonomic and Physiological Signals
Autonomic and physiological signals, including HRV, skin conductance, pupillary responses, respiratory patterns, microcirculatory indices, and near-infrared spectroscopy, have been increasingly used in pain research because they can be acquired continuously and are compatible with bedside monitoring and wearable devices.31 Unlike single questionnaire-based assessments, these signals can capture short-term fluctuations in arousal, autonomic regulation, stress response, and recovery state. Their relevance is particularly evident in perioperative monitoring, chronic musculoskeletal pain, neuromodulation research, and real-world rehabilitation, where pain interacts with sleep, activity, emotional state, and physiological regulation.102,103
HRV is the most frequently studied signal in this layer. Systematic reviews suggest that chronic musculoskeletal pain and low back pain are often associated with altered autonomic regulation, although the direction and magnitude of HRV changes vary across populations, protocols, and analytic methods.104,105 Exercise, rehabilitation, neuromodulation, and mind-body interventions may also influence HRV, suggesting that autonomic measures are better suited to characterizing regulatory capacity and treatment-related physiological change than to quantifying pain intensity alone.106,107 Near-infrared spectroscopy and other physiological monitoring approaches may likewise provide complementary information about pain-related cortical or systemic responses, but their interpretation remains task- and context-dependent.108
The clinical strength of this layer lies in dynamic monitoring rather than disease-specific diagnosis. In postoperative or chronic pain settings, persistent autonomic activation, reduced HRV, or sustained hyperarousal may suggest inadequate analgesia, impaired recovery, anxiety, sleep disruption, medication effects, or altered physiological regulation. Wearable HRV pipelines and autonomic measures in stress-related or visceral pain conditions illustrate that these signals can support risk identification and state monitoring when embedded in an appropriate clinical model.109,110
However, autonomic signals are strongly influenced by age, physical fitness, sleep, fatigue, medication, psychiatric comorbidity, inflammation, respiratory pattern, cardiovascular disease, and measurement conditions. HRV findings in psychiatric and substance-use populations further show that autonomic dysregulation may reflect broader stress-regulation or comorbidity states rather than pain-specific physiology.111 Therefore, autonomic and physiological signals should be interpreted as supportive indicators within continuous-monitoring and multimodal assessment frameworks. Their value is to improve temporal resolution, identify dysregulated recovery patterns, and provide physiological context for pain-related burden. Appropriate study design, repeated measurement, mathematical modeling, and integration with subjective, behavioral, and clinical data may improve diagnostic and predictive utility.112 Evidence from pediatric, adolescent, and cancer-related HRV biofeedback also suggests that autonomic measures may be useful as regulatory or intervention-related endpoints when matched to developmental context, disease state, and clinical task.113,114 These signals should not be used as independent gold standards, but they may strengthen assessment when the clinical question concerns trajectory, regulation, treatment response, or risk rather than a one-time estimate of pain intensity.
Multimodal Integration and Artificial Intelligence
Clinical Value of Multimodal Integration
The appeal of multimodal integration lies in bringing subjective scales, behavioral features, physiological signals, neuroimaging, and fluid biomarkers into a task-oriented clinical framework. Artificial intelligence and machine-learning approaches have accelerated this direction because they can extract joint patterns from multisource, weakly correlated, and high-dimensional data, making them attractive for risk prediction, subtype identification, and longitudinal trajectory analysis.19 Beyond simple data fusion, these models may also reveal latent or non-intuitive pain patterns that are difficult to identify through conventional single-modality interpretation.33
However, multimodal integration does not automatically overcome the limitations of its component modalities. Model labels are often derived from subjective ratings or broad clinical categories, meaning that label bias may be inherited rather than eliminated.115 Poorly standardized input signals may lead models to learn platform-specific noise rather than clinically meaningful structure, and models trained within a single center, disease category, or device environment may perform less well during external validation. Fairness is also a concern, because models trained on underrepresented or unbalanced populations may perform unevenly across age, sex, ethnicity, socioeconomic background, or disease subgroups.116 In addition, insufficient interpretability can limit incorporation into real-world clinical decision-making.
Current evidence suggests that multimodal models are most promising when used for specific clinical tasks rather than for generating a universal pain score. Potential applications include identifying patients at high risk of chronification, predicting response to particular treatments, tracking recovery trajectories, characterizing phenotypes, and flagging abnormal patterns that warrant further assessment.117 These advantages are clearest in settings where single indicators are insufficient: non-verbal ICU patients, where behavioral tools may help identify otherwise missed pain;47 early postoperative recovery, where sleep, activity, and wearable-derived indicators may contextualize serial pain scores;18 and chronic or neuropathic pain, where multimodal profiles may support phenotypic stratification and individualized assessment.118 These examples illustrate that multimodal integration is most useful when a single intensity scale provides limited explanatory value.
Current Limitations and Translational Preconditions
Although artificial intelligence has been increasingly applied to pain assessment and pain management, its discovery potential does not by itself guarantee clinical usefulness.33 Machine-learning and deep-learning models may identify latent phenotypes, nonlinear interactions, and non-intuitive patterns,19 but the central question is whether these patterns are reproducible, interpretable, fair, and linked to decisions that matter in clinical care.
Several recurrent limitations remain. Model labels are often derived from subjective ratings, diagnostic categories, or short-term clinical outcomes, allowing label noise and conceptual ambiguity to be inherited by the model.115 Dataset shift is common when models trained in one center, device environment, disease category, or demographic group are applied elsewhere. Fairness risks arise when underrepresented subgroups are insufficiently included in training and validation datasets.116 Model complexity may also improve predictive accuracy while reducing interpretability, creating a trade-off that is especially important when outputs are intended to guide analgesic adjustment, risk stratification, or treatment planning.
For practical translation, at least four preconditions should be met. The target task should be specific, such as risk prediction, treatment-response estimation, recovery monitoring, or subtype recognition, rather than the construction of a context-free universal pain score.117 Training labels should be clinically meaningful and, where possible, longitudinal or multidimensional rather than based only on a single pain rating at one time point. Data acquisition and preprocessing should be sufficiently standardized to permit external validation across centers and devices. Model outputs should also be interpretable enough to support clinician judgment and patient communication rather than replace them.119
Accordingly, AI-based multimodal models should be evaluated as clinical decision-support tools, not as independent arbiters of pain. Their success depends less on algorithmic novelty alone than on task definition, label quality, external validation, bias control, workflow compatibility, and evidence that the output improves decisions in real clinical settings. Without these conditions, increasingly complex models may simply repackage existing uncertainty into outputs that appear precise but remain clinically fragile.
Discussion
Why a Universal Robust Objective Marker is Still Absent
The long-standing absence of a unified, stable, and reproducible objective marker for pain should not be interpreted as the failure of a single technology. Rather, it reflects the interaction of conceptual, biological, methodological, and implementation barriers. Pain is an emergent experience arising from nociceptive input, central processing, affective appraisal, autonomic regulation, prior experience, disease context, and social meaning.3 Subjective report, behavioral expression, neural activity, inflammatory or endocrine changes, and autonomic signals are therefore related, but they operate at different levels of measurement. This makes it difficult for any single indicator to function as a universal substitute for the patient’s pain experience.21
The absence of a universal marker does not mean that objective or semi-objective indicators are unrelated to pain. In acute nociceptive pain, perioperative settings, and controlled experimental paradigms, physiological responses, evoked neurophysiological signals, and multivariate neuroimaging patterns may correlate meaningfully with pain intensity or pain-related processing.5,80 The limitation is that these associations are usually context dependent. A signal that performs reasonably well under controlled stimulation may lose specificity in chronic pain, mixed pain states, sedation, sleep disturbance, psychiatric comorbidity, medication exposure, inflammation, or advanced disease. Refractory visceral pain and complex regional pain syndrome further illustrate how peripheral pathology, central sensitization, autonomic regulation, inflammatory activity, motor changes, psychological factors, and treatment response may overlap in ways that complicate single-marker interpretation.120,121 This problem is shared across indicator classes. Behavioral tools such as CPOT are clinically useful in nonverbal or critically ill patients, but they primarily measure observable pain-related behavior.13 EEG, ERP, and LEP can identify nociceptive processing, attentional salience, and altered neural oscillations, but their interpretation depends on stimulus paradigm, analytic pipeline, and patient state.29 Neuroimaging has demonstrated pain-related signatures, network reorganization, and treatment-response phenotypes, yet individual-level prediction remains limited by heterogeneity, cost, protocol variation, and external validation challenges.17 Biofluid, endocrine, and omics-based markers may reveal inflammation, stress biology, neuroimmune activation, or risk of persistence, but they remain strongly influenced by disease activity, comorbidity, and assay platform.30 Thus, the central limitation is not the absence of pain-related signals, but the instability of signal meaning across patients, mechanisms, and clinical contexts.
Robust translation is also constrained by effect size and implementation. Many associations in pain research are small to moderate in magnitude, and even statistically reliable effects may not provide sufficient individual-level discrimination for bedside decisions.2 A group-level difference, a correlation with pain intensity, or a high internal cross-validation score does not automatically establish a clinically actionable marker. Effect size, calibration, reproducibility, external validation, workflow compatibility, and decision impact must be considered together.23 Multimodal artificial intelligence may help integrate weak-to-moderate signals and discover latent phenotypes, but it also inherits label noise, dataset shift, fairness risks, and interpretability challenges.19 Recent circuit-level evidence that chronic pain may involve bidirectional spino-brain-spinal cord loops further supports the view that pain should be interpreted as a systems-level phenomenon rather than as a single peripheral, central, or molecular signal.122 A realistic path forward is therefore not the search for one definitive pain meter, but the development of task-specific combinations of indicators for communication, detection, phenotyping, monitoring, risk stratification, and decision support.
A Task-Oriented Layered Pathway for Clinical Practice
The layered framework should be understood as a practical organization of existing assessment approaches rather than as a new diagnostic technology. Its purpose is to help clinicians and researchers decide which type of information is needed for a specific task, including rapid symptom scoring, detection of pain in nonverbal patients, monitoring of recovery, mechanistic phenotyping, prediction of treatment response, and multimodal decision support.4 In acute postoperative care, emergency settings, or routine ward rounds, a unidimensional pain intensity score may remain the most efficient and clinically appropriate option.5
A task-oriented pathway can be built around baseline assessment and selective augmentation. When patients can communicate reliably, subjective scales should usually remain the starting point because they directly capture the experienced dimension of pain and guide clinician–patient communication.11 When self-report is unavailable or unreliable, as in nonverbal ICU patients, neonates, sedated patients, or individuals with severe cognitive impairment, behavioral and functional proxies may become the practical baseline.47 When the question shifts from current pain severity to persistence, heterogeneity, treatment resistance, or prognosis, neurophysiological, imaging, autonomic, and molecular indicators may add mechanistic or predictive value.23 Recent circuit-level evidence also supports this escalation logic by suggesting that chronic pain may involve distributed spino-brain-spinal cord loops rather than a single peripheral or central signal.122
This logic differs across clinical scenarios. In ICU care, the priority is to avoid unrecognized suffering and guide analgesic or sedative adjustment, making validated behavioral tools and physiological context more useful than complex mechanistic biomarkers.47 In early postoperative recovery, repeated pain scores remain important, but activity, sleep, and wearable-derived trajectories may help identify delayed recovery or poor mobilization.18 Orthopedic perioperative pathways, such as total knee arthroplasty, further illustrate the value of interpreting pain alongside multimodal analgesia, rehabilitation progress, and functional recovery.56 In chronic, nociplastic, or neuropathic pain, assessment often expands from intensity to functional interference, mood, sleep, central sensitization, sensory profiles, imaging markers, or molecular pathways.7,38
Implementation burden should determine how many layers are added in practice. Cost, time, equipment availability, staff training, patient acceptability, data-management burden, and interpretability may limit routine use of multilayered assessment.115 For many routine decisions, additional measurements may increase complexity without improving care. Conversely, in patients with communication barriers, unexplained pain persistence, poor treatment response, or high risk of chronification, additional layers may provide information that a single score cannot capture. The clinical value of this framework therefore lies in selective escalation: beginning with the simplest valid tool for the context, adding behavioral or functional measures when communication or recovery monitoring is the priority, incorporating mechanistic biosignals when phenotyping or treatment selection is needed, and reserving multimodal artificial intelligence models for clearly defined prediction or decision-support tasks.19
Conclusion
Pain assessment is not a choice between subjective scales and objective technologies, but a layered clinical problem that requires task-oriented selection of tools. In routine settings such as acute postoperative care, emergency assessment, and ward-based follow-up, simple unidimensional scales may remain the most efficient and clinically appropriate option. In more complex contexts, including nonverbal patients, chronic or neuropathic pain, treatment-resistant pain, and research-oriented phenotyping, behavioral, functional, neurophysiological, imaging, molecular, autonomic, or artificial intelligence–based approaches may provide additional information that a single pain score cannot capture.
The value of a layered framework lies in selective escalation rather than comprehensive measurement for all patients. Cost, technological availability, staff workload, patient acceptability, data-management burden, and interpretability should determine whether additional assessment layers are justified. Standardization and validation remain essential, but their application is constrained by patient heterogeneity, disease context, psychosocial factors, cultural background, and clinical setting. Future pain assessment models should therefore be judged not only by statistical significance or prediction accuracy, but also by effect size, reproducibility, external validation, clinical usefulness, and decision impact.2 Advanced tools may improve precision and contextual interpretation, but they should support rather than replace clinical judgment.
Data Sharing Statement
No new datasets were generated or analyzed in this study. All information discussed in this review is derived from previously published articles cited in the reference list.
Ethics Approval and Consent to Participate
This article is a narrative review based on previously published literature and does not involve direct recruitment of human participants, collection of identifiable personal data, intervention, or animal experimentation by the authors. Ethics approval and informed consent were therefore not required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Natural Science Foundation of China (Grant No. 82374489) and the Tianjin Municipal Health High-Level Talent Project (Batch II; Grant No. TJSJMYXYCD2-028-2025).
Disclosure
The authors declare that they have no competing interests.
References
1. Scher C, Petti E, Meador L, Van Cleave JH, Liang E, Reid MC. Multidimensional pain assessment tools for ambulatory and inpatient nursing practice. Pain Manag Nurs. 2020;21(5):416–18. doi:10.1016/j.pmn.2020.03.007
2. Zieliński G. Getting to know pain effect sizes—guidelines for effect size and sample size in global pain research. Arch Phys Med Rehabil. 2026;107(4):726–733. doi:10.1016/j.apmr.2026.01.006
3. Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
4. Chandra SS, Pooja G, Kaur MT, Ramesh D. Current trends in modalities of pain assessment: a narrative review. Neurol India. 2024;72(5):951–966. doi:10.4103/neurol-india.Neurol-India-D-23-00665
5. Choi S, Yoon SH, Lee HJ. Beyond measurement: a deep dive into the commonly used pain scales for postoperative pain assessment. Korean J Pain. 2024;37(3):188–200. doi:10.3344/kjp.24069
6. Karcioglu O, Topacoglu H, Dikme O, Dikme O. A systematic review of the pain scales in adults: which to use? Am J Emerg Med. 2018;36(4):707–714. doi:10.1016/j.ajem.2018.01.008
7. Kaplan CM, Kelleher E, Irani A, Schrepf A, Clauw DJ, Harte SE. Deciphering nociplastic pain: clinical features, risk factors and potential mechanisms. Nat Rev Neurol. 2024;20(6):347–363. doi:10.1038/s41582-024-00966-8
8. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
9. Kosek E. The concept of nociplastic pain-where to from here? Pain. 2024;165(11S):S50–S57. doi:10.1097/j.pain.0000000000003305
10. Nijs J, Lahousse A, Kapreli E, et al. Nociplastic pain criteria or recognition of central sensitization? Pain phenotyping in the past, present and future. J Clin Med. 2021;10(15):3203. doi:10.3390/jcm10153203
11. Robinson CL, Phung A, Dominguez M, et al. Pain scales: what are they and what do they mean. Curr Pain Headache Rep. 2024;28(1):11–25. doi:10.1007/s11916-023-01195-2
12. Levitt J, Saab CY. What does a pain “biomarker” mean and can a machine be taught to measure pain? Neurosci Lett. 2019;702:40–43. doi:10.1016/j.neulet.2018.11.038
13. Zhai Y, Cai S, Zhang Y. The diagnostic accuracy of Critical Care Pain Observation Tool (CPOT) in ICU patients: a systematic review and meta-analysis. J Pain Symptom Manage. 2020;60(4):847–856.e13. doi:10.1016/j.jpainsymman.2020.06.006
14. Eriksson M, Campbell-Yeo M. Assessment of pain in newborn infants. Semin Fetal Neonatal Med. 2019;24(4):101003. doi:10.1016/j.siny.2019.04.003
15. Olsson E, Ahl H, Bengtsson K, et al. The use and reporting of neonatal pain scales: a systematic review of randomized trials. Pain. 2021;162(2):353–360. doi:10.1097/j.pain.0000000000002046
16. Baxter L, van der Vaart M, Cobo MM, et al. Is noxious stimulus-evoked electroencephalography response a reliable, valid, and interpretable outcome measure to assess analgesic efficacy in neonates? A systematic review and individual participant data (IPD) meta-analysis protocol. Syst Rev. 2025;14(1):152. doi:10.1186/s13643-025-02890-4
17. Zhang LB, Chen YX, Li ZJ, et al. Advances and challenges in neuroimaging-based pain biomarkers. Cell Rep Med. 2024;5(10):101784. doi:10.1016/j.xcrm.2024.101784
18. Kim S, Zeitzer JM, Mackey S, Darnall BD. Revealing sleep and pain reciprocity with wearables and machine learning. Commun Med. 2025;5(1):160. doi:10.1038/s43856-025-00886-8
19. Adams MCB, Bowness JS, Nelson AM, Hurley RW, Narouze S. A roadmap for artificial intelligence in pain medicine: current status, opportunities, and requirements. Curr Opin Anaesthesiol. 2025;38(5):680–688. doi:10.1097/ACO.0000000000001508
20. Djordjevic C, Saab CY. Beyond pain privacy and pain meters: a new vision for pain biomarkers. Front Pain Res Lausanne Switz. 2024;5:1397645. doi:10.3389/fpain.2024.1397645
21. Tracey I, Woolf CJ, Andrews NA. Composite pain biomarker signatures for objective assessment and effective treatment. Neuron. 2019;101(5):783–800. doi:10.1016/j.neuron.2019.02.019
22. Mackey S, Greely HT, Martucci KT. Neuroimaging-based pain biomarkers: definitions, clinical and research applications, and evaluation frameworks to achieve personalized pain medicine. Pain Rep. 2019;4(4):e762. doi:10.1097/PR9.0000000000000762
23. Mackey S, Aghaeepour N, Gaudilliere B, et al. Innovations in acute and chronic pain biomarkers: enhancing diagnosis and personalized therapy. Reg Anesth Pain Med. 2025;50(2):110–120. doi:10.1136/rapm-2024-106030
24. Verhoeff JJC. A systematic review of devices and techniques that objectively measure patients’ pain. Pain Physician. 2019;22(1):1–13. doi:10.36076/ppj/2019.22.1
25. Birnie KA, Hundert AS, Lalloo C, Nguyen C, Stinson JN. Recommendations for selection of self-report pain intensity measures in children and adolescents: a systematic review and quality assessment of measurement properties. Pain. 2019;160(1):5–18. doi:10.1097/j.pain.0000000000001377
26. Gavan SP, Chang S, Rivellese F, et al. Estimating pain visual analogue scale from health assessment questionnaire for rheumatoid arthritis with beta mixture models. Rheumatol Int. 2025;45(7):154. doi:10.1007/s00296-025-05897-1
27. Hoshino H, Ikeda M, Matsuishi Y, et al. Validity and reliability of the Critical-Care Pain Observation Tool (CPOT) for critically ill pediatric patients. PLoS One. 2025;20(4):e0320373. doi:10.1371/journal.pone.0320373
28. Wandrey JD, Behnel N, Weidner E, Dummin U, von Dincklage F, Tafelski S. Behaviour-based pain scales: validity and interrater reliability of BPS-NI and PAINAD-G on general wards. Eur J Pain. 2023;27(2):201–211. doi:10.1002/ejp.2051
29. Garcia-Larrea L, André-Obadia N. Electroencephalography, magnetoencephalography and pain: where do we stand, and where are we going. Pain. 2025;166(11S):S65–S70. doi:10.1097/j.pain.0000000000003689
30. Hutchinson MR, Barratt D, Johnston CH, et al. Biomarkers to predict, prevent, and treat persistent pain: omics. Pain. 2025;166(11S):S103–S105. doi:10.1097/j.pain.0000000000003673
31. Addleman JS, Lackey NS, Tobin MA, et al. Heart rate variability applications in medical specialties: a narrative review. Appl Psychophysiol Biofeedback. 2025;50(3):359–381. doi:10.1007/s10484-025-09708-y
32. Emish M, Young SD. Remote wearable neuroimaging devices for health monitoring and neurophenotyping: a scoping review. Biomim Basel Switz. 2024;9(4). doi:10.3390/biomimetics9040237
33. Zhang M, Zhu L, Lin SY, et al. Using artificial intelligence to improve pain assessment and pain management: a scoping review. J Am Med Inform Assoc. 2023;30(3):570–587. doi:10.1093/jamia/ocac231
34. Abd-Elsayed A, Robinson CL, Marshall Z, Diwan S, Peters T. Applications of artificial intelligence in pain medicine. Curr Pain Headache Rep. 2024;28(4):229–238. doi:10.1007/s11916-024-01224-8
35. Nijs J, Malfliet A, Roose E, et al. Personalized multimodal lifestyle intervention as the best-evidenced treatment for chronic pain: state-of-the-art clinical perspective. J Clin Med. 2024;13(3):644. doi:10.3390/jcm13030644
36. Bäckryd E, Ghafouri N, Gerdle B, Dragioti E. Rehabilitation interventions for neuropathic pain: a systematic review and meta-analysis of randomized controlled trials. J Rehabil Med. 2024;56:jrm40188. doi:10.2340/jrm.v56.40188
37. Nijs J, George SZ, Clauw DJ, et al. Central sensitisation in chronic pain conditions: latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021;3(5):e383–e392. doi:10.1016/S2665-9913(21)00032-1
38. Forstenpointner J, Sendel M, Baron R. Central and peripheral mechanisms of neuropathic pain. Neurol Clin. 2025;43(3):467–484. doi:10.1016/j.ncl.2025.04.002
39. Govas P, Ketchum A, Kazi R, Gordon BR, Carroll BT. Pain intensity assessment scales for dermatologic surgery patients: a systematic review. Dermatol Surg. 2022;48(2):232–238. doi:10.1097/DSS.0000000000003353
40. Zhang EW, Jones LE, Whitburn LY. Tools for assessing labour pain: a comprehensive review of research literature. Pain. 2023;164(12):2642–2652. doi:10.1097/j.pain.0000000000003004
41. Coca KP, Amir LH, Alves MDRDS, Barbieri M, Marcacine KO, De Vilhena Abrão ACF. Measurement tools and intensity of nipple pain among women with or without damaged nipples: a quantitative systematic review. J Adv Nurs. 2019;75(6):1162–1172. doi:10.1111/jan.13908
42. Bruno V, Achen B, Morgante F, et al. The Pain in Dystonia Scale (PIDS)-development and validation in cervical dystonia. Mov Disord. 2023;38(7):1175–1186. doi:10.1002/mds.29452
43. Blumenstock AK, Mauter D. [Pain assessment during birth: which assessment tools comprehensibly depict the labor pains during physiological birth?]. Schmerz Berl Ger. 2023;37(4):250–256. German. doi:10.1007/s00482-023-00715-8
44. Schofield P, Abdulla A. Pain assessment in the older population: what the literature says. Age Ageing. 2018;47(3):324–327. doi:10.1093/ageing/afy018
45. Maxwell LG, Fraga MV, Malavolta CP. Assessment of pain in the newborn: an update. Clin Perinatol. 2019;46(4):693–707. doi:10.1016/j.clp.2019.08.005
46. Chang HH, Hsu YC, Liao WL, et al. Translation and validation of the Chinese version of the menstrual distress questionnaire. J Obstet Gynaecol. 2024;44(1):2320844. doi:10.1080/01443615.2024.2320844
47. Afenigus AD. Evaluating pain in non-verbal critical care patients: a narrative review of the critical care pain observation tool and Its clinical applications. Front Pain Res Lausanne Switz. 2024;5:1481085. doi:10.3389/fpain.2024.1481085
48. De Sario GD, Haider CR, Maita KC, et al. Using AI to detect pain through facial expressions: a review. Bioeng Basel Switz. 2023;10(5). doi:10.3390/bioengineering10050548
49. Torres-Guzman RA, Ho OA, Borna S, Gomez-Cabello CA, Haider SA, Forte AJ. Identification of pain through actigraphy-recorded patient movement: a comprehensive review. Bioeng Basel Switz. 2024;11(9). doi:10.3390/bioengineering11090905
50. Gordon AM, Hussain A, Mont MA. Utilization of smartphone technology and wearable technology following TKA. J Knee Surg. 2025;38(8):393–396. doi:10.1055/a-2525-4672
51. Fedorchenko Y, Zimba O, Qumar AB, Yessirkepov M, Kocyigit BF. Physical activity of older patients with rheumatoid arthritis. Rheumatol Int. 2025;45(7):157. doi:10.1007/s00296-025-05901-8
52. Bjurström MF, Irwin MR. Perioperative pharmacological sleep‐promotion and pain control: a systematic review. Pain Pract. 2019;19(5):552–569. doi:10.1111/papr.12776
53. Mun CJ, Tsang S, Reid MJ, et al. Effects of sleep and circadian rest-activity rhythms on daily pain severity in women with temporomandibular disorders. Pain. 2025;166(7):1487–1496. doi:10.1097/j.pain.0000000000003578
54. Chalupczak NV, Aydemir B, Isaacs A, et al. Sleep matters: exploring the link between sleep disturbances and fatigue in rheumatoid arthritis. Arthritis Care Res. 2025;77(11):1368–1373. doi:10.1002/acr.25579
55. Colitta A, Bruno S, Cruz-Sanabria F, et al. Sleep and circadian parameters in Behçet’s syndrome: a comparative analysis using actigraphy and questionnaires. Rheumatology. 2025;64(10):5460–5470. doi:10.1093/rheumatology/keaf326
56. Zhao C, Liao Q, Yang D, Yang M, Xu P. Advances in perioperative pain management for total knee arthroplasty: a review of multimodal analgesic approaches. J Orthop Surg. 2024;19(1):843. doi:10.1186/s13018-024-05324-4
57. You M, Chen X, Liu D, Lin Y, Chen G, Li J. ChatGPT-4 and wearable device assisted intelligent exercise Therapy for co-existing Sarcopenia and Osteoarthritis (GAISO): a feasibility study and design for a randomized controlled PROBE non-inferiority trial. J Orthop Surg. 2024;19(1):635. doi:10.1186/s13018-024-05134-8
58. Hüllemann P, Von Der Brelie C, Manthey G, et al. Laser-evoked potentials in painful radiculopathy. Clin Neurophysiol. 2017;128(11):2292–2299. doi:10.1016/j.clinph.2017.09.100
59. Shiroshita Y, Kirimoto H, Ozawa M, et al. Can event-related potentials evoked by heel lance assess pain processing in neonates? A systematic review. Child Basel Switz. 2021;8(2). doi:10.3390/children8020058
60. Zebhauser PT, Hohn VD, Ploner M. Resting-state electroencephalography and magnetoencephalography as biomarkers of chronic pain: a systematic review. Pain. 2023;164(6):1200–1221. doi:10.1097/j.pain.0000000000002825
61. Chang JR, Li SX, Mei X, et al. Neural oscillations and brain connectivity in females with chronic low back pain and comorbid insomnia. J Pain. 2026;38:105485. doi:10.1016/j.jpain.2025.105485
62. Simis M, Pacheco-Barrios K, Uygur-Kucukseymen E, Castelo-Branco L, Battistella LR, Fregni F. Specific electroencephalographic signatures for pain and descending pain inhibitory system in spinal cord injury. Pain Med Malden Mass. 2022;23(5):955–964. doi:10.1093/pm/pnab124
63. Mussigmann T, Bardel B, Lefaucheur JP. Resting-state electroencephalography (EEG) biomarkers of chronic neuropathic pain. A systematic review. NeuroImage. 2022;258:119351. doi:10.1016/j.neuroimage.2022.119351
64. Ho KY, Liang JN, Budge S, Madriaga A, Meske K, Nguyenton D. Brain and spinal cord adaptations associated with patellofemoral pain: a systematic review and meta-analysis. Front Integr Neurosci. 2022;16:791719. doi:10.3389/fnint.2022.791719
65. Peng WW, Tang ZY, Zhang FR, et al. Neurobiological mechanisms of TENS-induced analgesia. NeuroImage. 2019;195:396–408. doi:10.1016/j.neuroimage.2019.03.077
66. Yue L, Bao C, Zhang L, et al. Neuronal mechanisms of nociceptive-evoked gamma-band oscillations in rodents. Neuron. 2025;113(5):769–784.e6. doi:10.1016/j.neuron.2024.12.011
67. Coll MP. Meta-analysis of ERP investigations of pain empathy underlines methodological issues in ERP research. Soc Cogn Affect Neurosci. 2018;13(10):1003–1017. doi:10.1093/scan/nsy072
68. Lopes Alves R, Zortea M, Vicuña Serrano P, et al. Modulation of neural networks and symptom correlated in fibromyalgia: a randomized double-blind multi-group explanatory clinical trial of home-based transcranial direct current stimulation. PLoS One. 2024;19(11):e0288830. doi:10.1371/journal.pone.0288830
69. Zeng X, Sun Y, Zhiying Z, Hua L, Yuan Z. Chronic pain-induced functional and structural alterations in the brain: a multi-modal meta-analysis. J Pain. 2025;28:104740. doi:10.1016/j.jpain.2024.104740
70. Kashanian A, Tsolaki E, Caruso J, Bari A, Pouratian N. Imaging as a Pain Biomarker. Neurosurg Clin N Am. 2022;33(3):345–350. doi:10.1016/j.nec.2022.02.011
71. Fiúza-Fernandes J, Pereira-Mendes J, Esteves M, Radua J, Picó-Pérez M, Leite-Almeida H. Common neural correlates of chronic pain – a systematic review and meta-analysis of resting-state fMRI studies. Prog Neuropsychopharmacol Biol Psychiatry. 2025;138:111326. doi:10.1016/j.pnpbp.2025.111326
72. El-Sayed R, Davis KD. Regional and interregional functional and structural brain abnormalities in neuropathic pain. Int Rev Neurobiol. 2024;179:91–123. doi:10.1016/bs.irn.2024.10.007
73. Garcia Guerra S, Spadoni A, Mitchell J, Strigo IA. Pain-related opioidergic and dopaminergic neurotransmission: dual meta-analyses of PET radioligand studies. Brain Res. 2023;1805:148268. doi:10.1016/j.brainres.2023.148268
74. Loggia ML. “Neuroinflammation”: does it have a role in chronic pain? Evidence from human imaging. Pain. 2024;165(11S):S58–S67. doi:10.1097/j.pain.0000000000003342
75. Katal S, Taubman K, Han J, Gholamrezanezhad A. Aging muscles, myositis, pain, and peripheral neuropathies: PET manifestations in the elderly. PET Clin. 2023;18(1):149–160. doi:10.1016/j.cpet.2022.09.009
76. Christensen RH, Al-Khazali HM, Iljazi A, Szabo E, Ashina H. Functional magnetic resonance imaging of post-traumatic headache: a systematic review. Curr Pain Headache Rep. 2025;29(1):27. doi:10.1007/s11916-024-01351-2
77. Lim M, Kim DJ, Nascimento TD, DaSilva AF. High-definition tDCS over primary motor cortex modulates brain signal variability and functional connectivity in episodic migraine. Clin Neurophysiol. 2024;161:101–111. doi:10.1016/j.clinph.2024.02.012
78. Raya JG, Duarte A, Wang N, et al. Applications of diffusion-weighted MRI to the musculoskeletal system. J Magn Reson Imaging. 2024;59(2):376–396. doi:10.1002/jmri.28870
79. Jarraya M, Roemer FW, Bäuerle T, Kogan F, Guermazi A. PET imaging in osteoarthritis. PET Clin. 2023;18(1):21–29. doi:10.1016/j.cpet.2022.09.002
80. Tracey I. Neuroimaging enters the pain biomarker arena. Sci Transl Med. 2021;13(619):eabj7358. doi:10.1126/scitranslmed.abj7358
81. Zunhammer M, Bingel U, Wager TD. Placebo imaging consortium. placebo effects on the neurologic pain signature: a meta-analysis of individual participant functional magnetic resonance imaging data. JAMA Neurol. 2018;75(11):1321–1330. doi:10.1001/jamaneurol.2018.2017
82. Tesic I, Pigoni A, Moltrasio C, Brambilla P, Delvecchio G. How does feeling pain look like in depression: a review of functional neuroimaging studies. J Affect Disord. 2023;339:400–411. doi:10.1016/j.jad.2023.07.083
83. Kong Q, Li T, Reddy S, Hodges S, Kong J. Brain stimulation targets for chronic pain: insights from meta-analysis, functional connectivity and literature review. Neurotherapeutics. 2024;21(1):e00297. doi:10.1016/j.neurot.2023.10.007
84. Liu L, Lyu TL, Fu MY, et al. Changes in brain connectivity linked to multisensory processing of pain modulation in migraine with acupuncture treatment. NeuroImage Clin. 2022;36:103168. doi:10.1016/j.nicl.2022.103168
85. Zhang C, Zhang Z, Li Y, et al. Alterations in functional connectivity in patients with non-specific chronic low back pain after motor control exercise: a randomized trial. Eur J Phys Rehabil Med. 2024;60(2):319–330. doi:10.23736/S1973-9087.24.08087-0
86. Suñol M, Pascual-Diaz S, Dudley J, et al. Neurophysiology of resilience in juvenile fibromyalgia. Pain. 2025;166(9):e200–e211. doi:10.1097/j.pain.0000000000003562
87. Zhou J, Zeng F, Cheng S, et al. Modulation effects of different treatments on periaqueductal gray resting state functional connectivity in knee osteoarthritis knee pain patients. CNS Neurosci Ther. 2023;29(7):1965–1980. doi:10.1111/cns.14153
88. Gu SY, Yao XX, Wang S, et al. Aberrant alterations of static and dynamic functional connectivity in chronic low back pain. Neuroscience. 2025;579:179–186. doi:10.1016/j.neuroscience.2025.06.011
89. Sun S, Sun Y, Shen J, et al. CXCL13/CXCR5: a new target for pain treatment. Int J Surg Lond Engl. 2025;111(9):6318–6329. doi:10.1097/JS9.0000000000002764
90. Navarro-Ledesma S. Frozen shoulder as a systemic immunometabolic disorder: the roles of estrogen, thyroid dysfunction, endothelial health, lifestyle, and clinical implications. J Clin Med. 2025;14(20):7315. doi:10.3390/jcm14207315
91. Moncada MAA, Tamayo MAN, Encinas MAN, Leoni MLG, Varrassi G. Immuno-inflammatory mechanisms in the chronification of pain. Pain Ther. 2026;15(2):443–464. doi:10.1007/s40122-026-00818-x
92. Machairiotis N, Vasilakaki S, Thomakos N. Inflammatory mediators and pain in endometriosis: a systematic review. Biomedicines. 2021;9(1):54. doi:10.3390/biomedicines9010054
93. Sarzi-Puttini P, Pellegrino G, Giorgi V, et al. Inflammatory or non-inflammatory pain in inflammatory arthritis - How to differentiate it? Best Pract Res Clin Rheumatol. 2024;38(1):101970. doi:10.1016/j.berh.2024.101970
94. Petraglia F, Vannuccini S, Dolmans MM, et al. The endocrine aspects of endometriosis. Eur J Endocrinol. 2025;193(4):R17–R30. doi:10.1093/ejendo/lvaf192
95. Úbeda-D’Ocasar E, Jiménez Díaz-Benito V, Gallego-Sendarrubias GM, Valera-Calero JA, Vicario-Merino Á, Hervás-Pérez JP. Pain and cortisol in patients with fibromyalgia: systematic review and meta-analysis. Diagnostics. 2020;10(11):922. doi:10.3390/diagnostics10110922
96. Polli A, Godderis L, Ghosh M, Ickmans K, Nijs J. Epigenetic and miRNA expression changes in people with pain: a systematic review. J Pain. 2020;21(7–8):763–780. doi:10.1016/j.jpain.2019.12.002
97. Gao H, Dong G, Yao Y, Yang H. Identification and validation of aging-related genes in neuropathic pain using bioinformatics. Front Genet. 2024;15:1430275. doi:10.3389/fgene.2024.1430275
98. Wei Z, Guo C, Zhou H, et al. Exosome-mediated miRNA delivery: a molecular switch for reshaping neuropathic pain therapy. Front Mol Neurosci. 2025;18:1625943. doi:10.3389/fnmol.2025.1625943
99. Giammona A, Galuzzi BG, Imperia E, et al. Chronic gastrointestinal disorders and miRNA-associated disease: an up-to-date. Int J Mol Sci. 2025;26(1):413. doi:10.3390/ijms26010413
100. Manzar A, Sic A, Banh C, Knezevic NN. Therapeutic potential of calcium channel blockers in neuropsychiatric, endocrine and pain disorders. Cells. 2025;14(14):1114. doi:10.3390/cells14141114
101. Sobieszczańska MI. Chronic pain in the elderly: a constant challenge. Adv Clin Exp Med. 2025;34(2):149–151. doi:10.17219/acem/200647
102. Forte G, Troisi G, Pazzaglia M, Pascalis VD, Casagrande M. Heart rate variability and pain: a systematic review. Brain Sci. 2022;12(2):153. doi:10.3390/brainsci12020153
103. Billet B, Goudman L, Rigoard P, et al. Effect of neuromodulation for chronic pain on the autonomic nervous system: a systematic review. BJA Open. 2024;11:100305. doi:10.1016/j.bjao.2024.100305
104. Rampazo ÉP, Rehder‐Santos P, Catai AM, Liebano RE. Heart rate variability in adults with chronic musculoskeletal pain: a systematic review. Pain Pract. 2024;24(1):211–230. doi:10.1111/papr.13294
105. Bandeira PM, Reis FJJ, Sequeira VCC, Chaves ACS, Fernandes O, Arruda-Sanchez T. Heart rate variability in patients with low back pain: a systematic review. Scand J Pain. 2021;21(3):426–433. doi:10.1515/sjpain-2021-0006
106. Meus T, Van Eetvelde J, Meuwissen I, et al. Exercise and heart rate variability in chronic musculoskeletal pain: a systematic review. Sports Med - Open. 2025;11(1):109. doi:10.1186/s40798-025-00916-8
107. Adler-Neal AL, Waugh CE, Garland EL, Shaltout HA, Diz DI, Zeidan F. The role of heart rate variability in mindfulness-based pain relief. J Pain. 2020;21(3–4):306–323. doi:10.1016/j.jpain.2019.07.003
108. Karunakaran KD, Peng K, Berry D, et al. NIRS measures in pain and analgesia: fundamentals, features, and function. Neurosci Biobehav Rev. 2021;120:335–353. doi:10.1016/j.neubiorev.2020.10.023
109. Guichard L, An X, Neylan TC, et al. Heart rate variability wrist-wearable biomarkers identify adverse posttraumatic neuropsychiatric sequelae after traumatic stress exposure. Psychiatry Res. 2024;342:116260. doi:10.1016/j.psychres.2024.116260
110. Nojkov B, Burnett C, Watts L, et al. The impact of transcutaneous electrical acustimulation (TEA) on rectal distension-induced pain in patients with irritable bowel syndrome (IBS)-A study to determine the optimal TEA delivery modalities and effects on rectal sensation and autonomic function. Neurogastroenterol Motil. 2024;36(7):e14799. doi:10.1111/nmo.14799
111. Moon SJE, Schlenk EA, Lee H. Heart rate variability in adults with substance use disorder: a comprehensive narrative review. J Am Psychiatr Nurses Assoc. 2024;30(2):240–251. doi:10.1177/10783903221145142
112. Fournié C, Chouchou F, Dalleau G, Caderby T, Cabrera Q, Verkindt C. Heart rate variability biofeedback in chronic disease management: a systematic review. Complement Ther Med. 2021;60:102750. doi:10.1016/j.ctim.2021.102750
113. Vermeulen N, Mejias S, Mejias S. Is heart rate variability biofeedback useful in children and adolescents? A systematic review. J Child Psychol Psychiatr. 2021;62(12):1379–1390. doi:10.1111/jcpp.13463
114. Spada GE, Masiero M, Pizzoli SFM, Pravettoni G. Heart rate variability biofeedback in cancer patients: a scoping review. Behav Sci Basel Switz. 2022;12(10). doi:10.3390/bs12100389
115. Meier TA, Refahi MS, Hearne G, et al. The role and applications of artificial intelligence in the treatment of chronic pain. Curr Pain Headache Rep. 2024;28(8):769–784. doi:10.1007/s11916-024-01264-0
116. Li H, Moon JT, Shankar V, Newsome J, Gichoya J, Bercu Z. Health inequities, bias, and artificial intelligence. Tech Vasc Interv Radiol. 2024;27(3):100990. doi:10.1016/j.tvir.2024.100990
117. Salama V, Godinich B, Geng Y, et al. Artificial intelligence and machine learning in cancer pain: a systematic review. J Pain Symptom Manage. 2024;68(6):e462–e490. doi:10.1016/j.jpainsymman.2024.07.025
118. Liang IJ, Senaratne DNS, Smith BH. Phenotyping chronic pain and neuropathic pain in population studies. Eur J Pain. 2025;29(10):e70146. doi:10.1002/ejp.70146
119. Medeiros HJS, Dabbagh A, Vlassakov K, Sabouri AS. Artificial intelligence in regional anesthesia and pain management. Anesthesiol Clin. 2025;43(3):491–505. doi:10.1016/j.anclin.2025.05.004
120. Pons T, Shipton EA, Williman J, Mulder RT. Potential risk factors for the onset of complex regional pain syndrome type 1: a systematic literature review. Anesthesiol Res Pract. 2015;2015:956539. doi:10.1155/2015/956539
121. Andrade MF, Fabris-Moraes W, Pacheco-Barrios K, Fregni F. Effect of neurostimulation on chronic pancreatic pain: a systematic review. Neuromodulation. 2024;27(8):1255–1265. doi:10.1016/j.neurom.2024.08.003
122. Wang Q, Lee JH, Nachtrab G, et al. Deconstruction of a spino-brain-spinal cord circuit that drives chronic pain. Nature. 2026. doi:10.1038/s41586-026-10296-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.