Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Rethinking Health Professionals’ Motivation to Do Research: A Systematic Review
Authors D'Arrietta LM ![]() , Vangaveti VN, Crowe MJ
, Vangaveti VN, Crowe MJ ![]() , Malau-Aduli BS
, Malau-Aduli BS ![]()
Received 1 September 2021
Accepted for publication 15 December 2021
Published 26 January 2022 Volume 2022:15 Pages 185—216
DOI https://doi.org/10.2147/JMDH.S337172
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Louisa M D’Arrietta,1,2 Venkat N Vangaveti,1 Melissa J Crowe,3 Bunmi S Malau-Aduli1
1College of Medicine and Dentistry, James Cook University, Townsville, Queensland, Australia; 2Library Services, Townsville University Hospital, Townsville Hospital and Health Service, Townsville, Queensland, Australia; 3Division of Tropical Health and Medicine, James Cook University, Queensland, Australia
Correspondence: Louisa M D’Arrietta
College of Medicine and Dentistry, James Cook University, Townsville, Queensland, 4811, Australia
Tel +61 7 4781 4060
Fax +61 7 4779 6371
Email [email protected]
Background: Health professionals’ engagement in translational health and medical research (HMR) is fundamental to evidence-based practice leading to better patient health outcomes. However, there is a decline in the number of health professionals undertaking research which has implications for patient health and the economy. Informed by the motivation-based expectancy-value-cost (EVC) and self determination theories (SDT), this systematic literature review examined the barriers and facilitators of health professionals’ (HPs) motivation to undertake research.
Methods: The literature was searched between 2011 and 2021 for relevant peer-reviewed articles written in English, using CINAHL Complete, Informit, Medline Ovid, Medline (PubMed), Scopus, Web of Science and Google Scholar databases. This systematic review was performed and reported in accordance with the PRISMA guidelines.
Results: Identified barriers to HPs’ engagement with research included the lack of knowledge, skills, and competence to conduct research, lack of protected research time, lack of funding and lack of organisational support. Integration of the findings of this review based on the EVC and SDT theories indicate that research capacity, ie, expectancy and competence is highly influenced by attitude, ie, the type of value (attainment, intrinsic or utility) and connection attributed to research. HPs who had very positive attitude towards research demonstrated all three values and were keen to take up research despite the barriers. Those who had a positive attitude were only motivated to do research because of its utility value and did not necessarily see it as having personal relevance for themselves. HPs who were unmotivated did not see any personal connection or relatedness to the research experience and saw no value in research.
Conclusion: The attitude HPs hold in their value of research is a catalyst for motivation or amotivation to engage in research as it directly influences the relevance of barriers. Facilitators that expedite the research journey have been attributed to research training, mentorship programs and supportive organisational research culture. Motivation of HPs explored through EVC and SDT is critical to the maintenance of a research culture and the clinician-researcher development pipeline.
Keywords: barriers, facilitators, expectancy-value theory, EVC, self-determination theory, SDT, health professionals, motivation
Introduction
Health professionals (HPs), including doctors, nurses, midwives, and allied health professionals (AHPs) who undertake research have been referred to in the literature under various titles including, clinician researcher1 clinician investigator2 and physician-researcher.3 This group of HPs spend time as both active clinicians and researchers and they engage in translational health and medical research (HMR) to address the issues they see in clinical practice.4 HP led research is important because it fosters evidence-based clinical practice and improved health outcomes for patients.5 For example, research on chronic diseases has significantly contributed to better health outcomes and improved quality of life for people across Australia and globally.6 In addition to the patient health benefits, employment of those engaged in HMR has resulted in continued productivity due to better health outcomes and financial benefits from new medicines and technology. HMR has helped Australia become a leading economy of the 21st century returning an increasing net benefit of $8.2 billion, returning $3.90 for every dollar invested6 and from 2000 to 2015, National Health and Medical Research Council (NHMRC)-funded research saved the Australian health system $23.4 billion.6 Despite the benefits of research to the economy and health benefits to patients there still exists a dearth of HP researchers.
There has been an ongoing global concern that the number of HPs undertaking research is declining.7 The seminal paper by Wyngaarden,8 “The clinical investigator as an endangered species” addressed this concern over 40 years ago.9,10 Recent international trends from the USA,7,11,12 Canada,13 UK,14 Sweden,15 Africa,16 Singapore,17 Pakistan18 and Saudi Arabia19 still indicate a decline in the number of young researchers replacing an aging workforce. For example, in the US, the fraction of physician-researchers has reduced from 4.7% in the 1980s to approximately 1.5% currently.20 In New Zealand (NZ) and Australia there exists a similar scenario, with the number of individuals training in medical research decreasing or stagnating over the past few decades.21–23 The Australian Institute of Health and Welfare (AIHW) reported a decline in the proportion of employed Australian doctors who identified primarily as researchers from 2.1% in 2002 to 1.5% in 2010.24,25 The 2018 Medical Deans of Australia and New Zealand (MDANZ) report indicated a further 3.9% drop in the number of physician-researchers between 2013 and 2017.26 Comparatively, of the 1346 registered doctors who self-reported as physician-researchers in 2017, 59% were males and 39% were 55 years and above.26
Decline in the number of HP researchers has largely been attributed to significant factors including lack of dedicated research time, research expertise, awareness and skills.10,27 Additionally, there has been lack of effective succession planning.12 Furthermore, younger generations of HP graduates, particularly females, are wanting more work-life balance; and this generates situations where undertaking research competes with other goals, values and career pathways.3,7,28 Reduced accessibility to research positions, particularly in rural areas has also been highlighted as a major challenge.29 Building the capacity of HPs to undertake research is considered to be an international priority in view of the increasing predominance of chronic diseases and aging world populations.30 Health organisations with strong research culture have been associated with greater service efficiencies and reduced patient mortality and morbidity, indicating that involvement in research extends beyond individual HPs’ professional development.31
Motivation to undertake or stay in HMR is a key factor in addressing the shortage of HP researchers currently being experienced.32 Motivation has largely been attributed to the opportunities and barriers HPs have experienced or expect to experience in their research journey.32 However, the number of HPs engaging in research has still not improved. Applying a theoretically informed approach to examining existing literature findings can point the way to more effective strategies to motivate HPs to do research. The Expectancy-Value-Cost (EVC) motivation theory postulates that achievement-related choices are motivated by a combination of people’s expectations for success and subjective task value in particular domains.33,34 For example, individuals are more likely to pursue an activity if they expect to do well and value the activity. The model further differentiates task value into three components: attainment value (ie, importance of doing well), intrinsic value (ie, personal enjoyment) and utility value (ie, perceived usefulness for future goals). However, motivation can be limited by potential barriers which are referred to as cost (ie, competition with other goals). According to the EVC model, expectations for success and task value are shaped by a combination of factors. These include individual characteristics (abilities, previous experiences, goals, self-concepts, beliefs, expectations, interpretations) and environmental influences (cultural milieu, socializers’ beliefs, and behaviours).35
A recurrent theme in the literature is that motivation to undertake research has largely been extrinsic, that is, to improve CVs,36 career progression37 or for academic improvement. This indicates a need for further exploration into the underlying concepts of motivational theory and its relevance to research uptake and retention by HPs. It is not surprising, therefore, that motivation is increasingly becoming a major area of interest within the field of HPs’ education38 and health research orientation,39 with a focus on Self-Determination Theory (SDT)40,41 which has special implications for HMR. Evolving from research on intrinsic and extrinsic motivations, SDT is a macro theory of human motivation that has been successfully applied to healthcare education and HMR.42,43 The focus of SDT is not on how motivation can be controlled from without, but instead on how motivation is functionally designed and experienced from within.41 SDT relates to three basic psychological needs: (1) Competence: People need to gain mastery of tasks and learn different skills. When people feel that they have the skills needed for success, they are more likely to take actions that will help them achieve their goals. (2) Connection or Relatedness: People need to experience a sense of belonging and attachment to other people. (3) Autonomy: People need to feel in control of their own behaviours and goals. This sense of being able to take direct action that will result in real change plays a major part in helping people feel self-determined.44
Rethinking HPs’ motivation to engage in research, now has immediate and wider implications for all HPs whether medical, nursing and midwifery or allied health.6 The decline in number of HP researchers comes at a critical time when medical innovations are urgently needed to combat the current global COVID-19 pandemic, other communicable diseases and the aging population crisis.2,18 The threat to individual and societal health and economic welfare requires a holistic approach to HP engagement with research and research training to ensure long-term outcomes for survival of world populations.2 Research can no longer be restricted to an elite and specialized few, it needs to be appreciated as a fundamental activity for most, if not all HPs. To foster HP engagement with research, it is important to gain deep insight and understanding of what motivates or discourages them from taking up or continuing with research along the career pipeline. Hence this systematic review utilised two theoretical frameworks (EVC33,34 and SDT40,41) to (1) examine the facilitators and barriers to health professionals’ motivation to undertake research and (2) identify current research gaps.
Methods
The systematic review was conducted and reported in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) Statement.
Inclusion and Exclusion Criteria
For the purpose of this review, the term HP researcher is defined as a medical graduate, nurse, midwife or AHP who works both clinically and in research – often varying the fractions throughout their career. The study population consisted of all HPs: AHPs, Medical, Nursing and Midwifery in hospital/research centres. Peer-reviewed articles written in English were considered if they related to HPs’ motivation, attitudes, and perceptions about undertaking research. There was no restriction on study design. Articles were excluded if they did not meet the inclusion criteria and/or they were review papers.
Search Strategy
Seven electronic databases comprising, CINAHL Complete, Informit, Medline Ovid, Medline (PubMed), Scopus, Web of Science and Google Scholar were searched. Peer reviewed primary articles, written in English and published between 2011 and 2021 (a decade of literature) were included in this review to reflect the current level of activity in the topic area.
Search terms used were research, health professionals (including physicians, AHPs, nurses, midwives), research, and motivation. The terms research capacity, attitudes and barriers were purposefully excluded as they would have limited a full exploration of the topic. The comprehensive search strategy used for this review is presented in Appendix 1. Reference lists from previous reviews and included studies were also screened for additional relevant articles.
Study Selection
All the identified articles were imported into Endnote X9 software (Clarivate, Australia), then titles and abstracts were screened. Two authors (LMDA and BSMA) independently screened the titles and abstracts of the retrieved articles and excluded those that did not meet the inclusion criteria. Subsequently, full-text articles categorised as potentially eligible for inclusion were screened and disagreements were resolved in a consensus meeting.
Data Synthesis and Analysis
Meta-analysis was not possible, due to the heterogeneous nature of the included articles. A data extraction form was developed and used to collect relevant information from all the included studies. Descriptive data including author, study year, title, country of study, research/study focus, setting – urban/rural/remote, study design, type of participants, participant numbers, gender and mean age were extracted from each of the selected studies. Elements of the Self-Determination Theory (SDT)43 and the Expectancy-Value-Cost Model of Motivation (EVC)46 were adopted to facilitate extraction of the key determinant factors to research motivation. The identified barriers and facilitators of HPs’ motivation to undertake research, as reported in each reviewed article were independently extracted and categorised by two authors (LMDA and BSMA). Conceptual content analysis47,48 was used to extract and systematically code the factors as determined by the tenets of the EVC and SDT frameworks. Rules for translation of text into codes were developed by the researchers. Coding of pre-defined concepts/sets of categories was done manually and analysis of results involved quantification of coded concepts for frequency of occurrence and determination of relationships, trends and patterns.48
Three major factors were considered namely: Research Capacity which relates to expectancy and competence; Attitude which relates to value and connection; and Barriers which relate to cost and autonomy. Research capacity was coded based on explicit/implicit statements within each reviewed article about participants’ perceived levels of confidence/ competence to participate in research. Participants’ attitude to research was underpinned by the type of value they attributed to research – attainment, intrinsic and/or utility value, as well as the connection or relatedness they expressed towards research. Participants’ attitude to research was categorised into three groups based on the frequency with which values and connections held by the study participants were openly stated or inferred. Attitude to research was coded as “very positive” if all three value types were established in a study, “positive” if only one and “negative/fear of research” if no value or connection to research was indicated. For autonomy/ cost, reported barriers in all studies were listed and grouped into categories, number of categorised barriers in each study were then quantified. LMDA and BSMA independently extracted and categorised all factors and subsequently met to check for consistency. All discrepancies were resolved through discussion.
For the purpose of this review, research capacity is defined as the ability to engage in, perform or carry out quality research.49 The expectancy and competence of individuals to carry out research activities underpins research capacity and was viewed through the EVC (expectancy) and SDT (competence) frameworks. While it is postulated that there are two types of expectancies: ability beliefs that comprise of current/immediate beliefs about being able to complete a task and expectancy beliefs that reflect being able to do the task in the future, most investigations collapse measures of ability and expectancy beliefs into a general expectancy scale.46
Attitude to undertaking research was viewed through the EVC (value) and SDT (connection) frameworks. Value is differentiated into three components: value of attainment is espoused in meeting a personal need; intrinsic value is gained through personal enjoyment or satisfaction and utility value is perceived usefulness for future goals and may be predictive of current and future interest.46 Connection or relatedness is where people need to experience a sense of belonging and attachment to other people.44
Barriers to undertaking research was also viewed through the EVC (Cost) and SDT (autonomy) frameworks where the perceived cost of undertaking research competes with other goals,44 and autonomy is seen as the need to feel in control of one’s own behaviours and goals without undue external influences.44 Cost and autonomy are largely seen as influences external to the individual although they may be encountered at the individual, organisational and/or system level.43,46
Quality Assessment of Reviewed Articles
The Quality Assessment Tool for Studies with Diverse Designs (QATSDD) was used to assess the methodological consistency and quality of the included studies.50 This tool contains 16 items and is used for examining studies with different research designs. Each of the included studies was graded on a scale of 0 to 3 for each criterion, with 0 = not at all, 1 = very slightly, 2 = moderately and 3 = complete. To assess the methodological quality of each of the included studies, the criteria scores were summed and expressed as a percentage of the maximum possible score. The percentage scores were classified into low (<50%), medium (50–80%) or high (>80%) quality evidence for easy identification. The QATSDD criteria included: (1) theoretical framework; (2) aims/objectives; (3) description of research setting; (4) sample size; (5) representative sample of target group; (6) procedure for data collection; (7) rationale for choice of data collection tool(s); (8) detailed recruitment data; (9) assessment of reliability and validity of measurement tool(s) (Quantitative only); (10) fit between research question and method of data collection (Quantitative only); (11) fit between research question and data collection method (Qualitative only); (12) fit between research question and method of analysis; (13) good justification for analytical method selected; (14) reliability of analytical process (Qualitative only); (15) evidence of user involvement in design; (16) strengths and limitations.50
Results
Included Studies
Four thousand and twenty four (4024) articles were identified from all searched databases. Ten (10) additional articles were identified through hand searching. After screening the titles and abstracts of the identified articles and reviewing 228 full texts, 46 met the inclusion criteria for this review as shown in Figure 1.
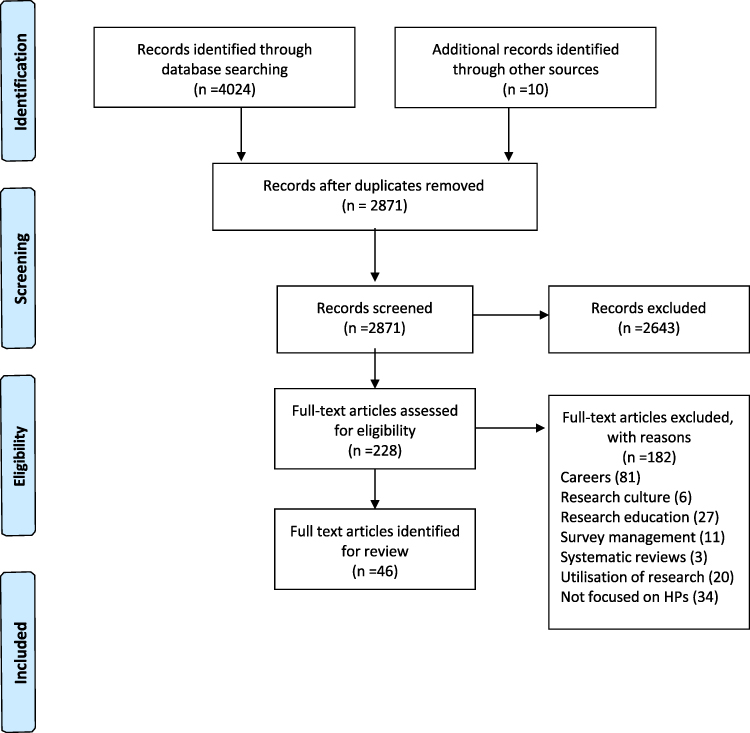 |
Figure 1 Flow chart of the study selection protocol. PRISMA figure adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 6(7):e1000097. Creative Commons45. |
Assessment of Methodological Quality
Table 1 portrays the QATSDD assessment with scores ranging from 33% to 90%. The aims and objectives, description of the research setting as well as the fit between research question and data collection method were well addressed in most studies. Strengths and limitations of the studies were also generally well addressed by most studies. Nonetheless, good justification for analytical method selected was overlooked in 14 studies and only 19 (41.3%) studies had evidence of user involvement in the design. Overall, 10 studies (22%) were rated as high quality because they were judged to be explicit in their methodology and mostly utilised theoretical frameworks. Thirty-five (76%) were medium quality studies and some of the weaknesses identified from these studies included: lack of theoretical framework, inadequate sample sizes and poor reliability. One study51 met only few quality criteria, had low rating (33%) and therefore was removed from the review.
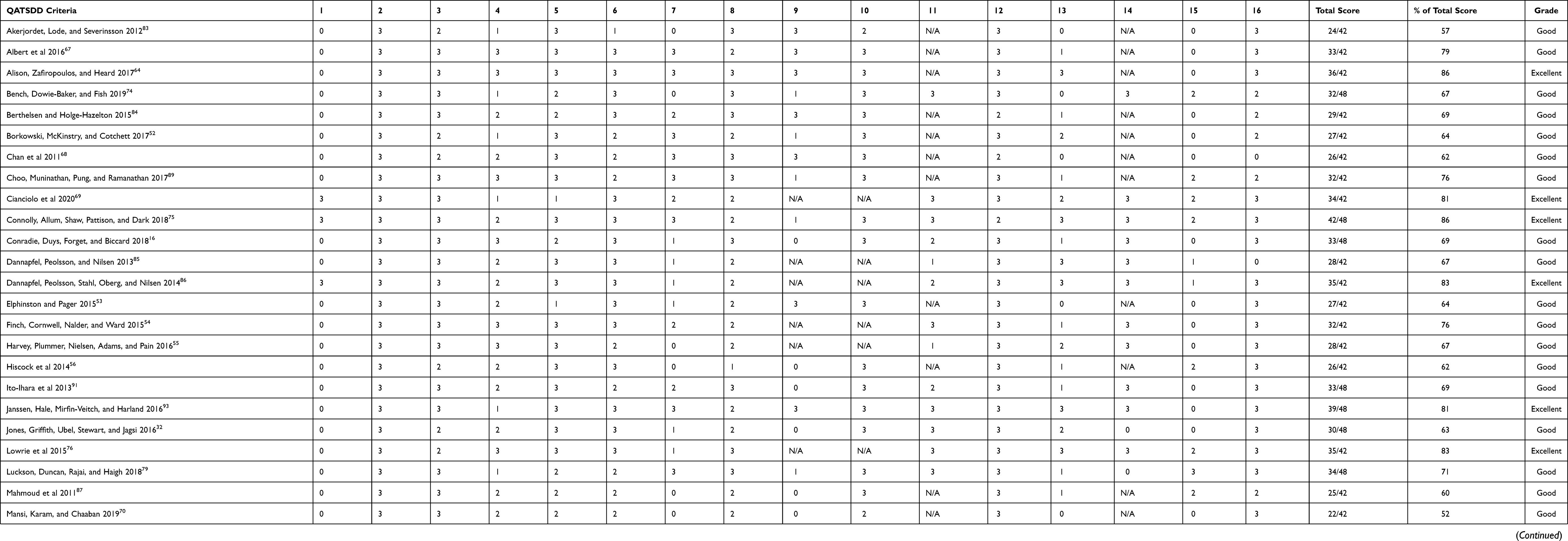 |
Table 1 Quality Assessment of the Included Studies |
Study Characteristics
A summary of the characteristics of the included 45 studies is presented in Table 2. The total number of participants was 11,438 and participant numbers per study ranged from 15 to 2052. Of the 33 studies that included both genders, 5620 (62.2%) of the 9039 participants were females. Only 19 studies indicated participants’ mean age which ranged from 34.5 ± 9.5 to 50 ± 7.7 years.
 | 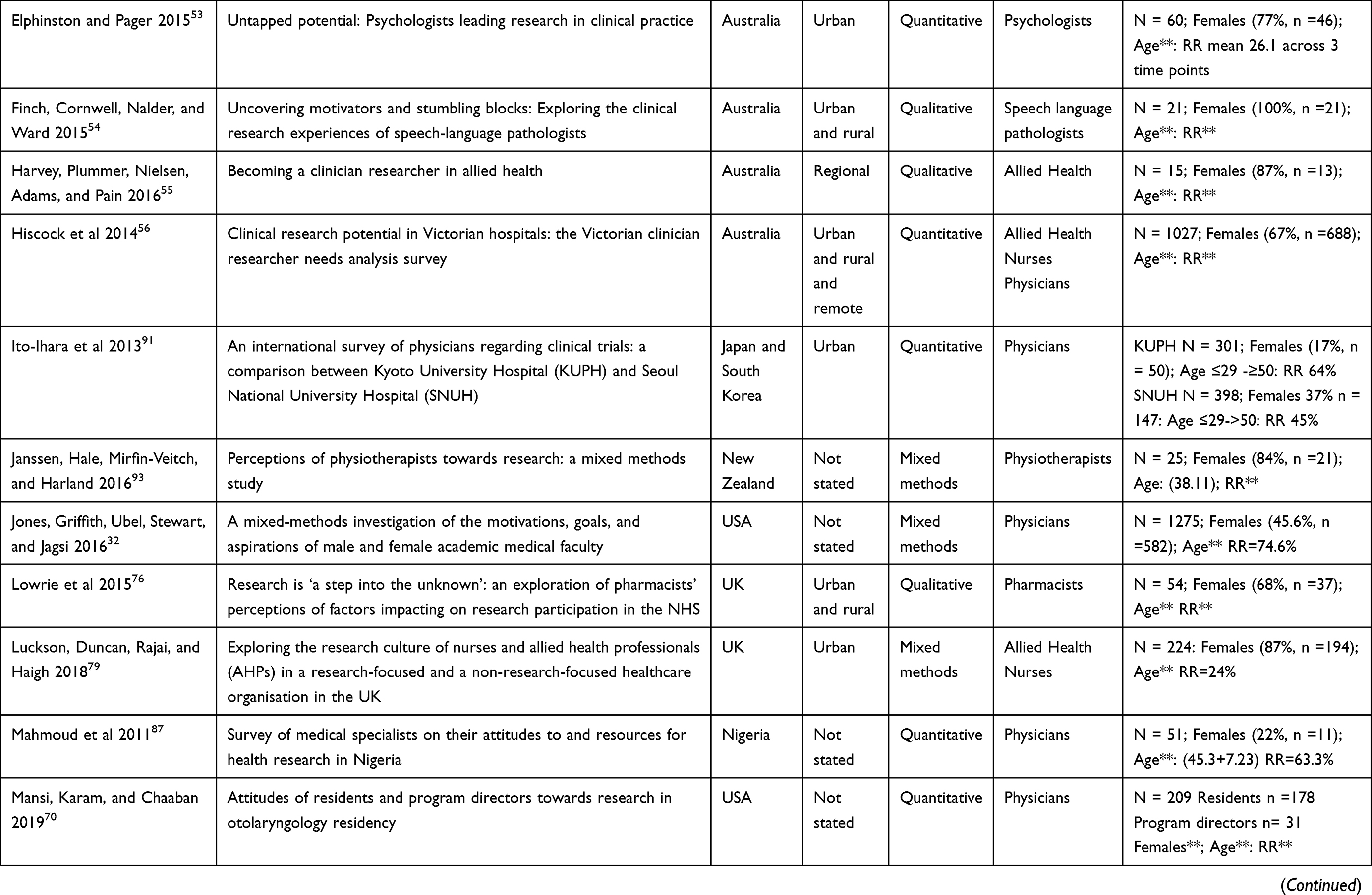 | 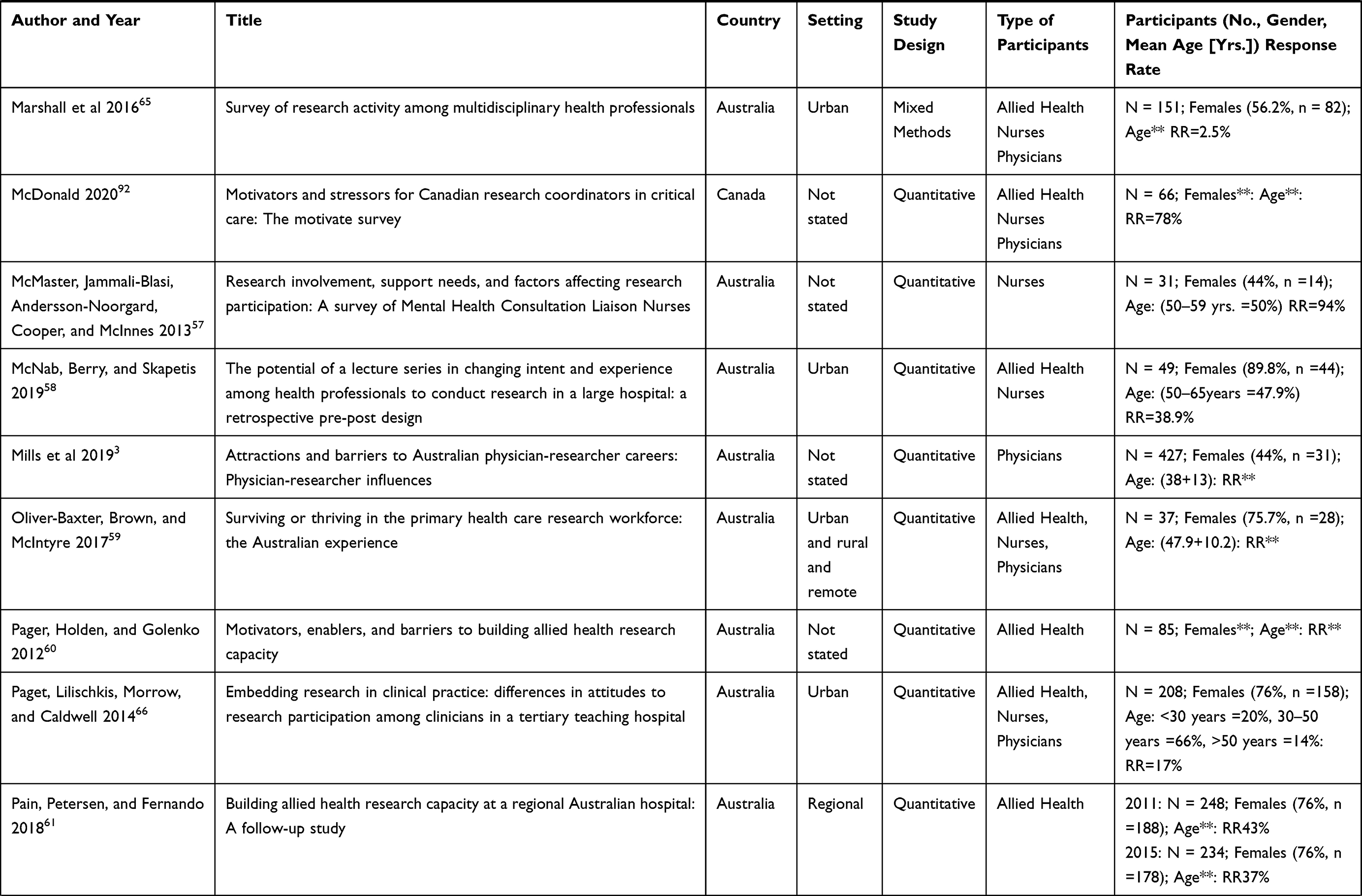 | 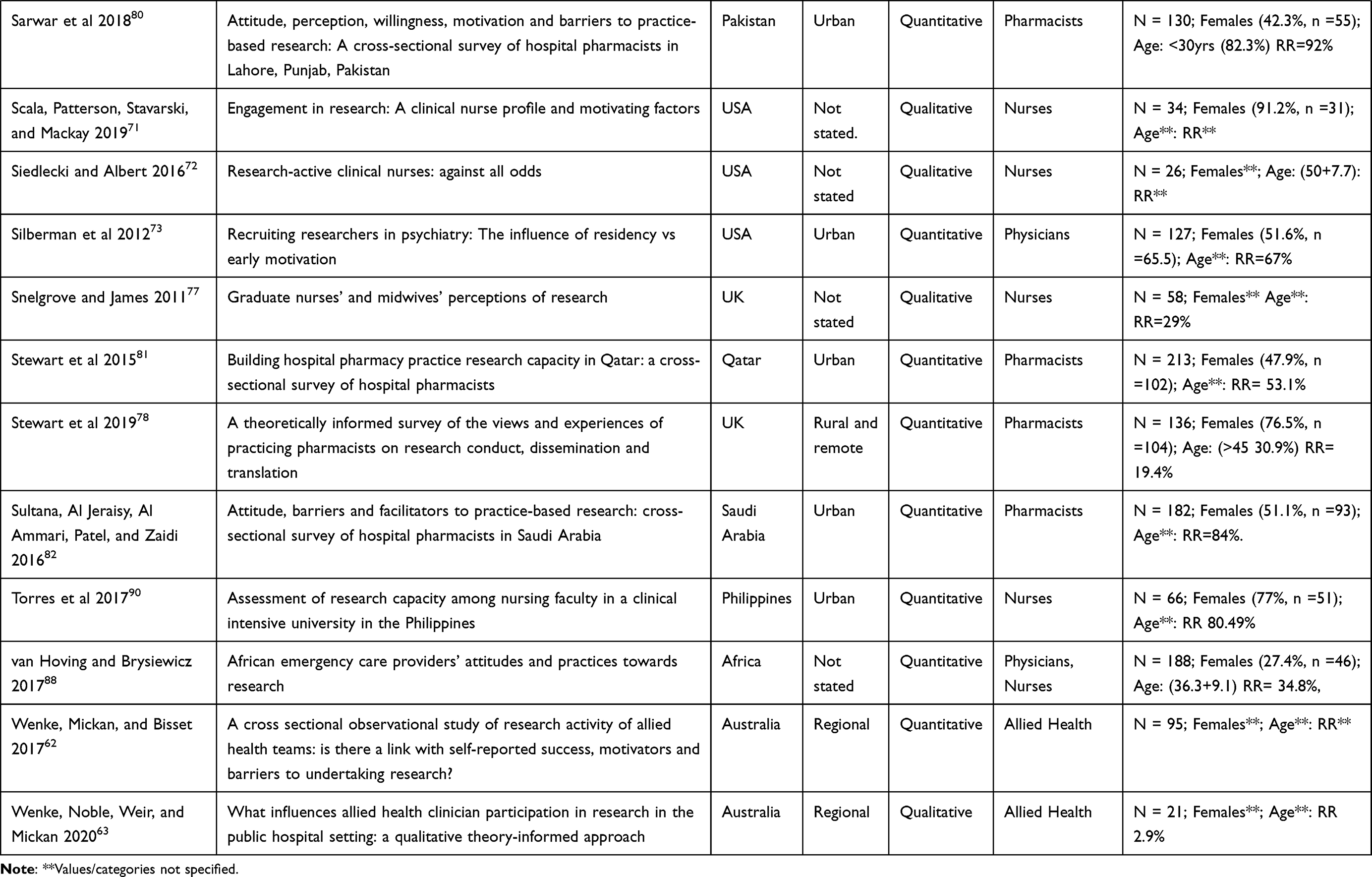 |
Table 2 Study Characteristics and Participant Demographics for Reviewed Articles |
Sixteen (16) of the studies were conducted in Australia,3,52–66 eight from USA,32,67–73 six from UK,74–79 four from the Middle East,69,80–82 four from Europe,83–86 three from Africa,16,87,88 two from South East Asia,89,90 one from Japan and South Korea91 and one each from Canada92 and New Zealand93 Study settings included 13 urban,53,58,64–67,73,79–82,90,91 six regional52,55,61–63,84 and five urban and rural settings.54,69,76,85,86 Two studies were conducted in all three settings (urban, rural and remote)56,59 while one was located in rural and remote settings.78 The setting type was not specified in 18 studies. The study designs were varied with 29 quantitative, 10 qualitative and six mixed methods studies.
Five studies focused on all HPs56,59,65,66,92 as a heterogeneous group, two on AHPs and nurses58,79 and one on nurses and physicians.88 Overall, 18 studies concentrated on AHPs with 7 of those studies considering them as a homogenous group,52,55,60–64 five studies were solely on pharmacists,76,78,80–82 four on physiotherapists75,85,86,93 and one each on psychologists53 and speech language pathologists.54 Ten studies focused on nurses57,67,68,71,72,74,77,83,84,90 and nine on physicians.3,16,32,69,70,73,87,89,91
While HPs’ motivation to do research was investigated by all 45 reviewed studies, only eight studies utilised a theoretical framework or model in their investigation. These included Self-Determination Theory (SDT),86 Social Cognitive Career Theory (SCCCT) and Professional Identity Formation as an integrated framework,69 COM-B framework,75 Vroom’s Expectancy Theory,71 Research-Active Nurse Model,72 Theoretical Domains Framework (TDF),78 Social Cognitive Theory,82 combination of TDF and COM-B.63
Factors Influencing Motivation
In relation to factors influencing motivation, all the studies in this review were appraised utilising the EVC and SDT frameworks. A summary of the findings is presented in Table 3.
 | 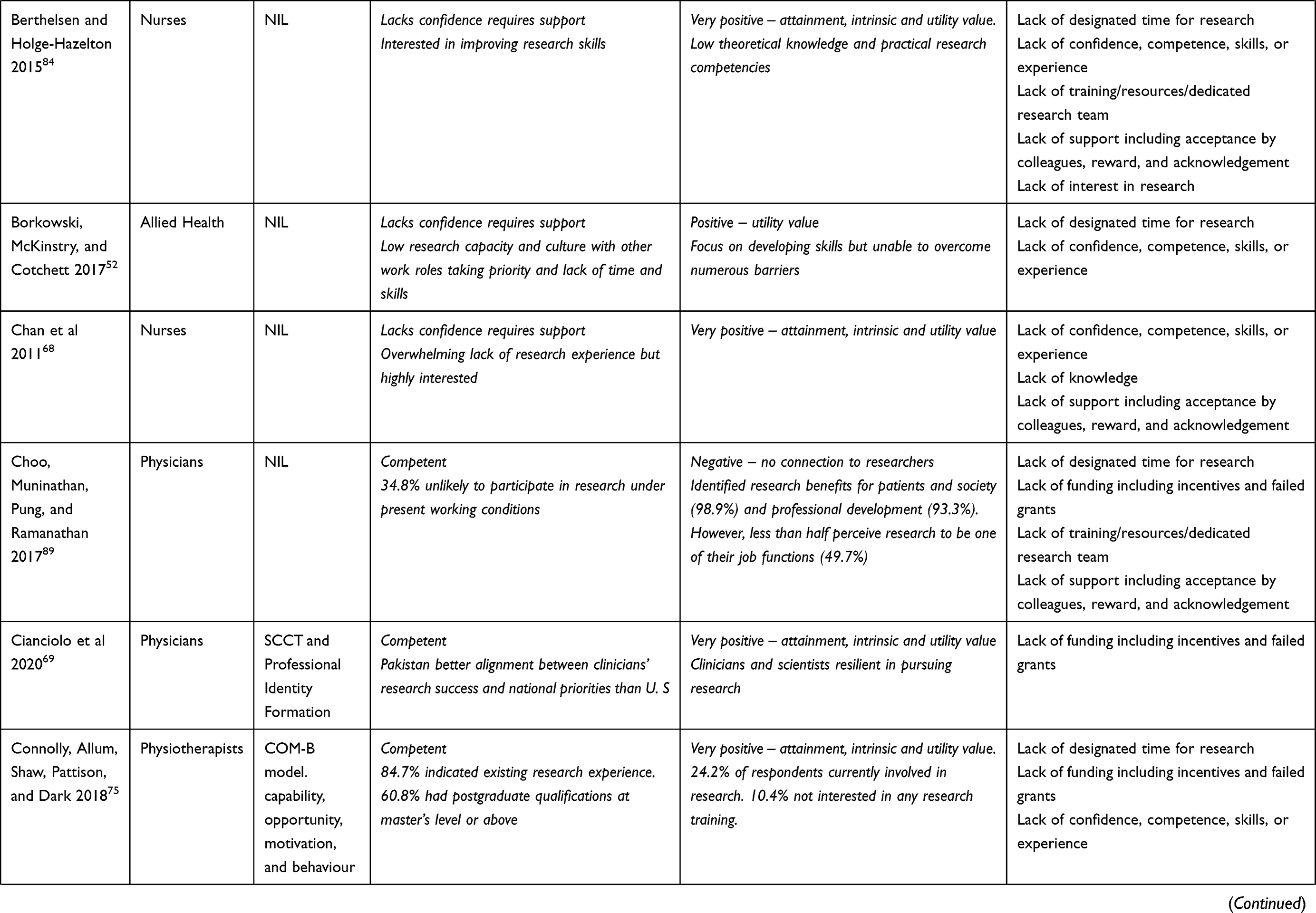 | 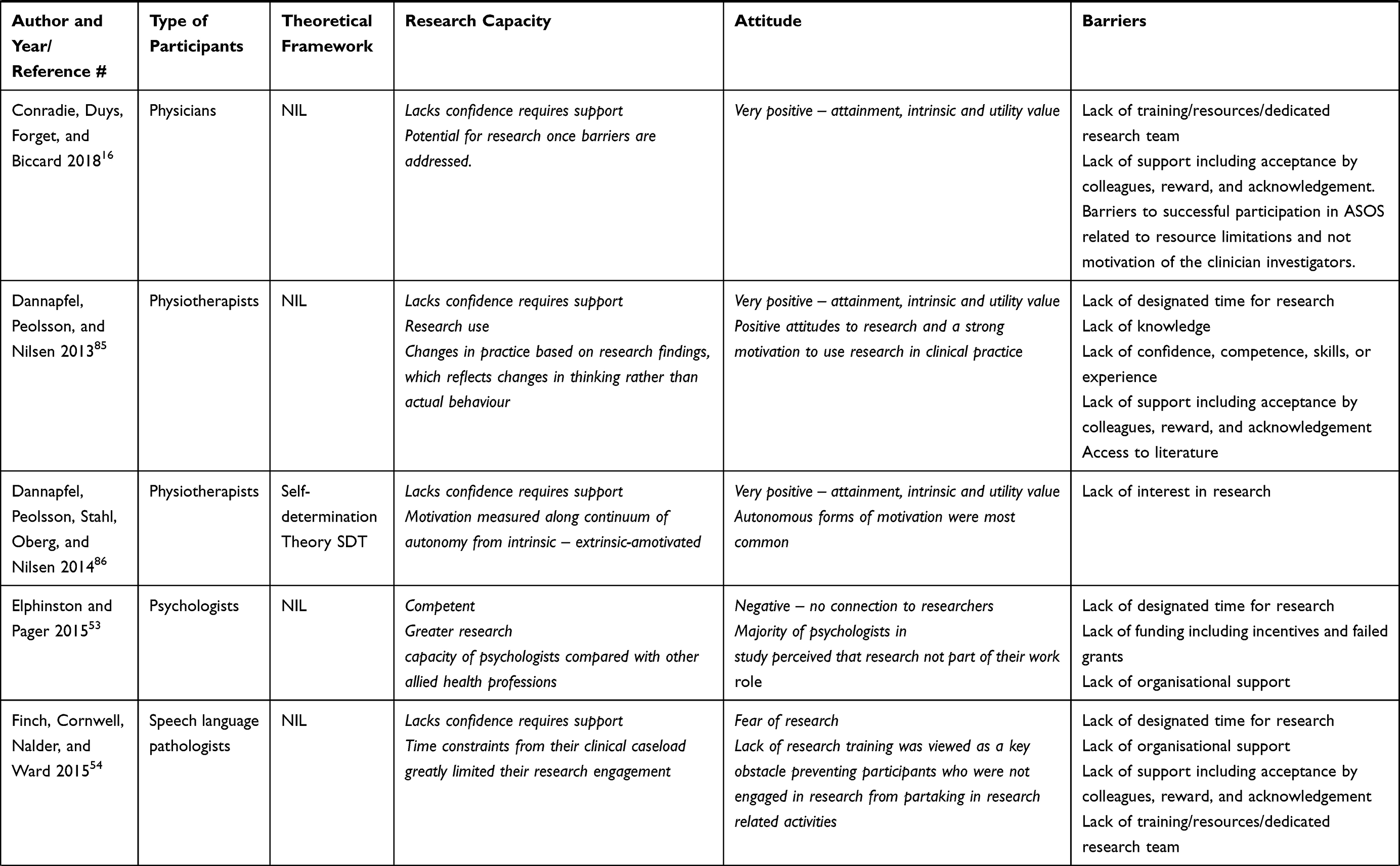 | 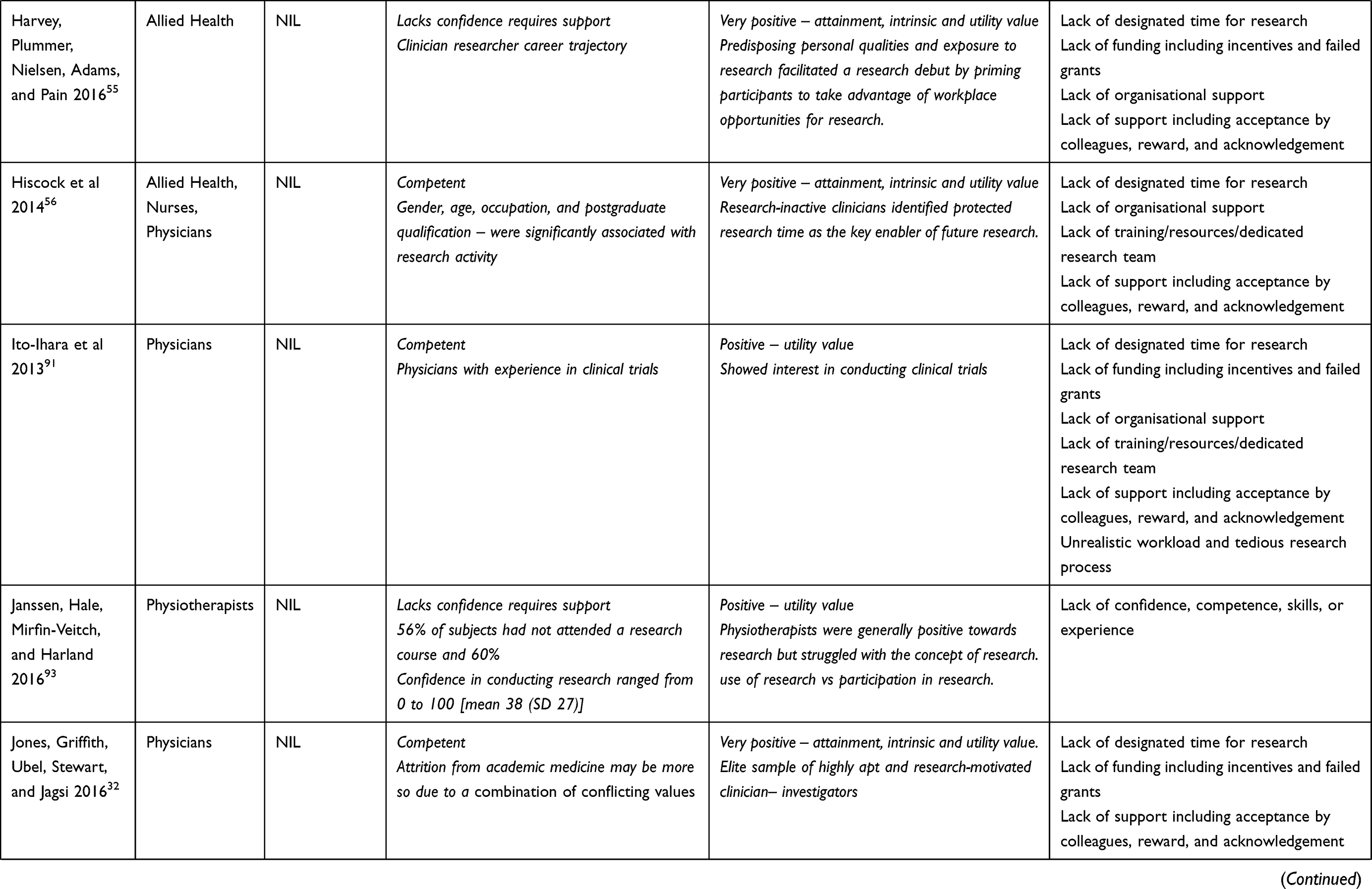 | 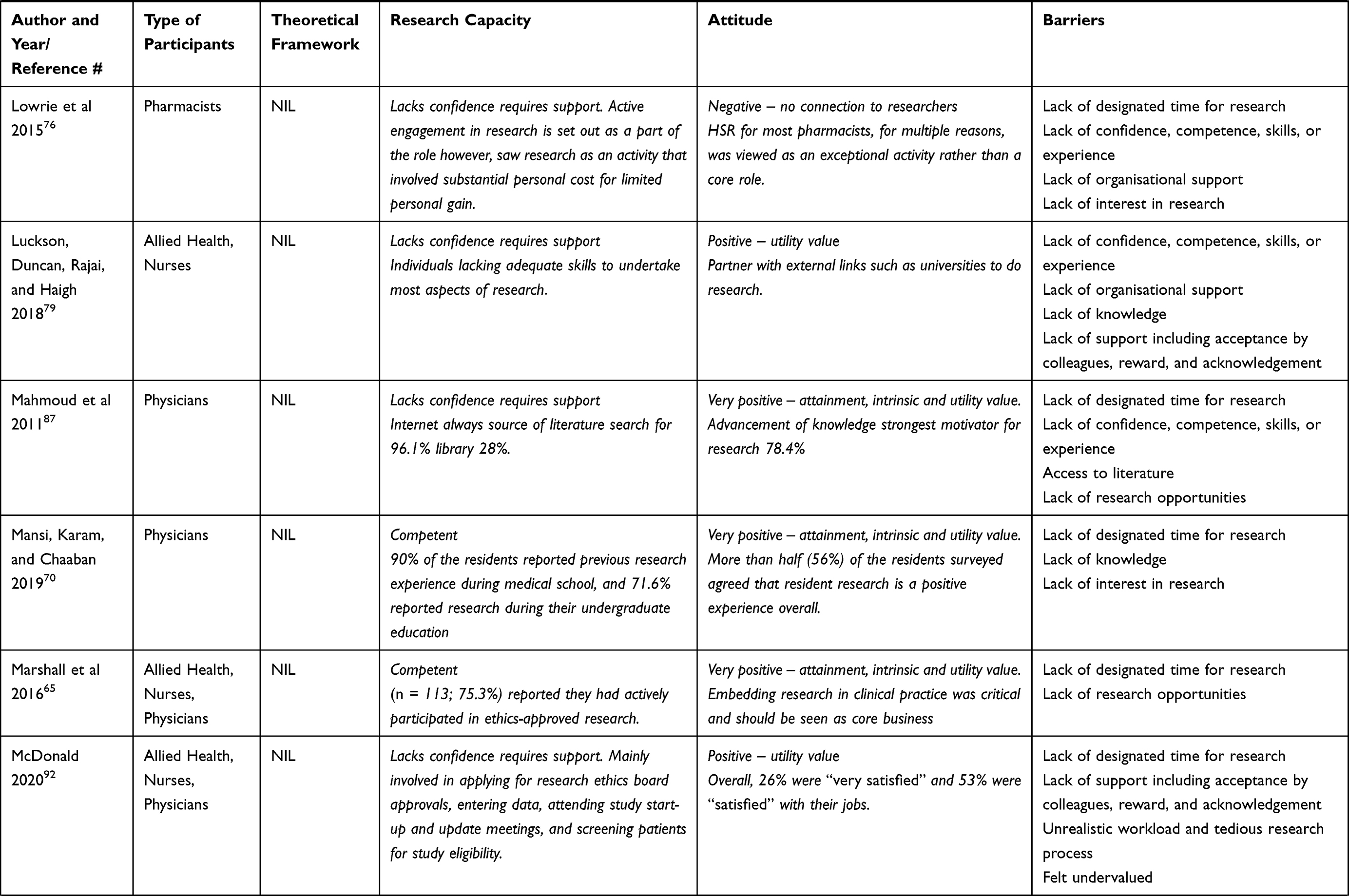 | 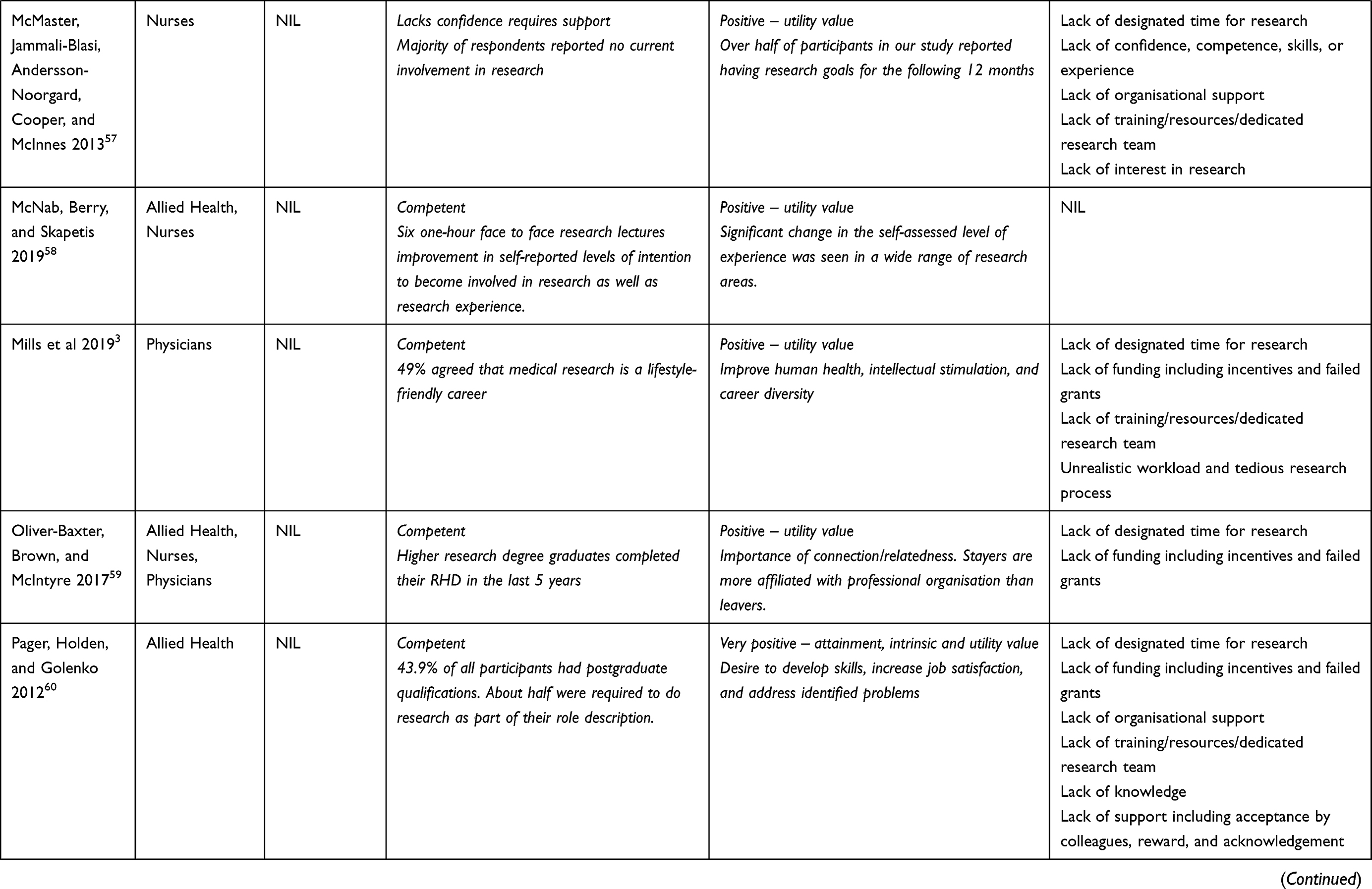 | 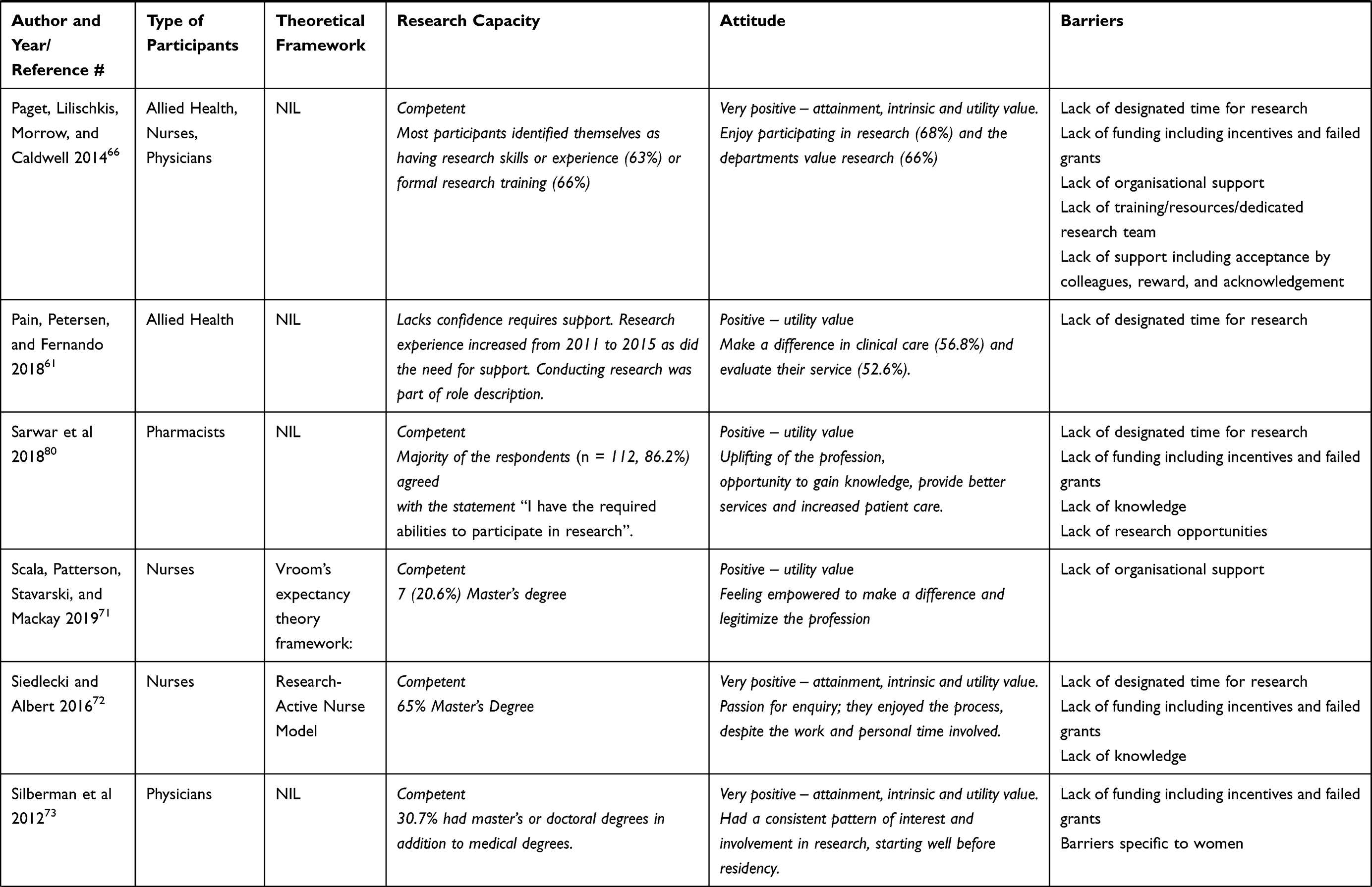 |  | 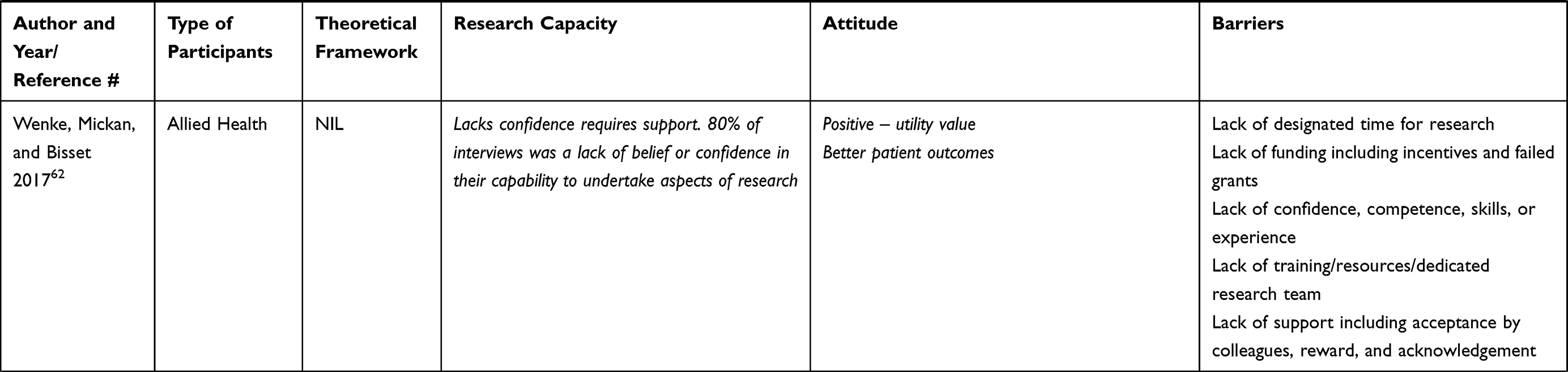 |
Table 3 Theoretical Framework Summary of Study Outcomes |
HPs’ Research Capacity
Research capacity was investigated in the studies in terms of competence/confidence and expectancy to do research. As shown in Table 3, over half 25 (56%) of the reviewed studies identified their participants as competent to undertake research, while the participants in the remaining 20 (44%) studies were identified as lacking confidence and requiring support to undertake research.
Of the 25 studies where participants were identified as competent, seven focused on physicians (medical doctors).,3,32,69,70,73,89,91 another seven on AHPs,52,55,60–64 four of which targeted pharmacists.78,80–82 Five studies focused on nurses, four on all HP groups and one each on nurse-physician group and nurse-AHP group. Most participants who felt competent perceived that they had the required abilities, skills, and knowledge to participate in research. For example, participants in one study reported high competence levels ranging from 3.14 to 4.06 on a 5-point rating scale.90 About 60–90% of participants who were identified as competent reported having prior research experience, with 66–75% confirming that they had formal training during their undergraduate education.3,58,65,66,70,75,80,82,88,90 Between 20% and 65% of this group of participants indicated that they had either completed or were undertaking a postgraduate qualification which had enhanced their research capacity.59,60,71–73,75,77,78,81,82,88
Eleven studies that targeted AHPs reported that the participants lacked competence/confidence to undertake research. Similar results were obtained for five studies focused on nurses, two on physicians and one each on all HP groups and nurse-AHP group. Common features for these studies were overwhelming poor research capacity, very little or no prior research training/experience, low research culture with other work roles taking priority and need for research support. In one study, participants indicated that they had never attended research training nor spent time on research and reported mean confidence level of 38% (SD 27).93
Overall, the results show that HPs’ confidence and expectancy to undertake research is largely dependent on research skills and experience gained through research training during their undergraduate/postgraduate education. The medical doctors were the most confident to undertake research as indicated in seven out of nine studies (77.8%) compared to nurses in five out of 11 (45.5%) studies; and AHPs in seven out of 18 (38.9%) studies. This may be attributed to the reported early exposure to research training and research experience by the medical doctors in comparison to nurses and AHPs. These findings highlight the impact of research training on perceived competence, confidence, and capability to participate in research.
HPs Attitude – This Relates to Value and Connection
As depicted in Table 3, participants’ attitude to research was assessed as very positive in 17 (38%) studies,16,32,55,56,60,65,66,68–70,72,73,75,84–87 positive in 21 (47%) studies3,52,57–59,61,62,64,67,71,78–83,88,90–93 and negative in four (9%)53,74,76,89 studies.
The 17 studies in which HPs were deemed very positive included six on medical doctors,16,32,69,70,73,87 five on AHPs,55,60,75,85,86 three on nurses55,60,75,85,86 and three on a combination of the three groups.56,65,66 The 21 studies that identified respondents as positive comprised nine on AHPs,52,61,62,64,78,80–82,93 (including four on pharmacists78,80–82 and one on physiotherapists),93 five on nurses,57,67,71,83,90 two on medical doctors3,91 and five on a combination of the HP groups – two focused on all three HP groups,59,92 two on AHPs and nurses58,79 and one on medical doctors and nurses88 The four studies in which HPs were identified as negative included two on AHPs – pharmacists76 and psychologists,53 one each on nurses74 and medical doctors.89 Another three studies reported their respondents as being afraid of research – two on AHPs54,63 and one on nurses.77
Generally, participants who demonstrated very positive attitude towards research were keen to contribute to clinical practice by engaging in collaborative research to advance clinical knowledge and improve patient health outcomes (utility value). Additionally, they were avidly interested in publishing, producing new knowledge, gaining grants and getting respect of colleagues (attainment value) as well as broadening personal scope of professional career and becoming knowledgeable researchers with genuine interest in research as a problem-solving tool32,55,69,87 (intrinsic value). This group of participants had genuine curiosity and willingness to learn, were mostly satisfied with their jobs, wanted to develop research skills so they could increase knowledge and develop cutting edge research that proffer solutions to clinical problems.55,60,75,85,86 They also felt a strong connection to research and their profession bodies. For example, research active pharmacists reported the importance of research in uplifting the pharmacy profession and enjoyed reading articles.80,82
Participants who demonstrated positive attitude mainly viewed research as beneficial for making a difference in clinical care with improved patient health outcomes and service delivery.16,70,73,91 This group focused on the utility of research and mainly focused on its benefits in improving clinical care and practice. For participants who were negative, the common attitude reported included perceived benefit only for the institution in which they worked.89 They also did not feel supported by their organisation and therefore did not consider research as part of their role. Interestingly, one study on the medical group identified its participants as negative/not involved in research and perceived the value of research as solely for the benefit of patients and the institution in which they worked.89 Nurses were negative in one study74 and found research frightening in another.77 Two studies on AHPs fell under the fear of research category.54,63 This group of participants reported minuscule63 or no value54 for research and emphasised the need for connection and relatedness. Participants in the negative/fear of research groups were of the opinion that research was a “huge undertaking” and “daunting task”.57
Overall, most of the participants in the medical group were very positive while the AHP and nursing groups were mostly in the positive category. Intrinsic value was seen as a pre-requisite for motivation, while utility value is the trigger for research to satisfy the need in clinical practice.72 The results suggest that very positive attitude towards research is based on intrinsic and attainment values and these help the HPs develop strong long-term connection with research. On the other hand, negative attitude seemed to be linked to perceived low organisational support for research. Although participants with negative attitude acknowledged that research could improve clinical practice and boost professional reputation, but feelings of poor connection to research team created disillusion or fear. These findings indicate that sense of value and connection could be paramount in determining HPs’ level of motivation to engage with research.
HPs Barriers to Undertaking Research Relates to Cost and Autonomy
Table 4 depicts the barriers identified by the participant groups. The most frequently reported barriers to undertaking research were lack of time and funding. Lack of designated time for research was reported in 32 (71%) studies3,32,52–57,59–66,70,72,74–76,78,80,82–85,87–89,91,92 while lack of funding (including incentives and failed grants) was identified as a significant barrier to conducting research in 18 (40%) studies, mostly by the medical doctors,3,32,59,66,69,73,88,89,91 followed by the AHPs53,55,60,62–64,75,80 and nurses.72,88
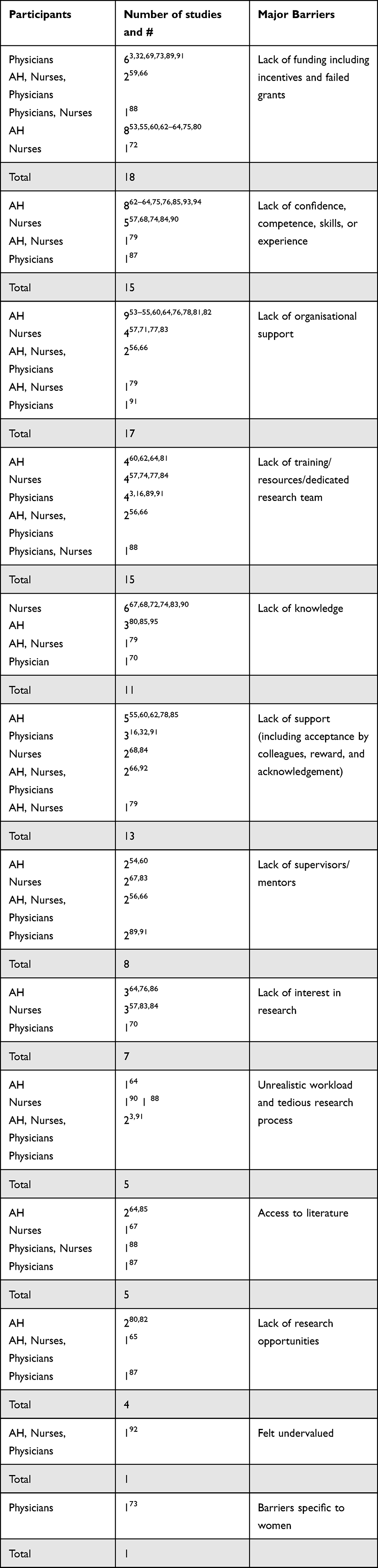 |
Table 4 Major Types of Barriers by Participant Groups |
Respondents in 15 (33%) studies reported lack of confidence, competence, skills and/or research experience,57,62–64,68,74–76,79,84,85,87,90,93,94 while 17 (38%) studies reported lack of organisational support as a significant barrier to research involvement53–57,60,64,66,71,76–79,81–83,91 Lack of research competence and organisational support were mostly flagged by the AHPs,52–55,60,62–64,75,76,78,79,81,82,85,93 followed by the nurses57,68,71,74,77,83,84,90 and only few medical doctors.87,91
Lack of training/resources/dedicated research team was mentioned by participant groups in 15 studies (33%)3,16,56,57,60,62,64,66,74,77,81,84,88,89,91 Lack of knowledge was of concern in 11 studies (24%) and mostly acknowledged by the nursing group,67,68,72,74,83,90 followed by the AHPs79,80,85,95 and the medical group.70 Lack of support (including acceptance by colleagues, reward and acknowledgement) was mentioned in 13 studies (29%) and mostly indicated by AHPs,55,60,62,78,85 and the medical group.16,32,91 Eight studies (18%) reported lack of supervision/mentors,54,56,60,66,67,83,89,91 seven studies (16%) reported lack of interest in research.57,64,70,76,83,84,86 Five studies each (11%) identified unrealistic workload/tedious research process3,64,90–92 and access to literature as barriers to research, while lack of research opportunities was reported in 4 studies (9%).65,80,82,87 Participants felt undervalued in one study92 while another study found barriers specific to women73 as a deterrent to their participation in research.
Overall, AHPs reported more barriers than nurses and medical doctors, particularly in relation to lack of organisational support, confidence, training, and acceptance by colleagues. Major barriers for nurses were lack of knowledge, training, and confidence; while for medical doctors, it was lack of funding. The results show that the AHPs and nurses were less able to demonstrate autonomy to engage with research in comparison to the medical doctors and they were mostly limited by lack of knowledge, training, and confidence which are important pre-requisites of research capability. This finding indicates that just as research knowledge and training can foster confidence and competence, lack of them can also serve as major and costly barriers that limit HPs’ capacity to participate in research.
Integration of the Elements of the Conceptual Frameworks
Integration of the findings based on the EVC33,34 and SDT40,41 theories indicate strong interactions between the three components – research capacity (expectancy and competence), attitude (value and connection), and barriers (cost and autonomy). Table 5 presents the relationship between the components that influence motivation to engage in research. Generally, HPs who were reported as competent (mostly studies on medical doctors or combination of all three groups32,56,60,65,66,69,70,72,73,75) had prior exposure to research training either in their undergraduate or postgraduate education. This boosted their confidence and facilitated interest and connection with research in their career paths. In addition, engagement with research was based on the type of value (utility, intrinsic and attainment) HPs attached to research. Those who were very positive demonstrated all three types of value, felt connected to other research colleagues and despite multiple barriers, they had genuine interest which fostered their capacity for on-going, long-term research. They viewed research as highly beneficial in advancing clinical knowledge, improving patient health outcomes (utility value), producing new knowledge, gaining recognition (attainment value) as well as broadening personal scope of professional career and building sustainable problem-solving systems to identify solutions to key clinical problems (intrinsic value). Some HPs (mostly AHPs and nurses) were competent and positive in their attitude, but they exhibited only utility value3,58,59,67,71,78,80–82,88,90,91 because connection with professional organisation was lacking.3,59 Interestingly, another group of HPs reported high confidence/competence levels, but they were negative and feared research.53,77,89 The reason for this attitude was the perception that research was not part of their job roles and there was no organisational support, so they did not see the connection with the research community.53 This same reason was observed for HPs who lacked confidence, had no prior exposure and had negative attitude towards research.54,63,74,76 They perceived that it had no value and involved a lot of personal cost for limited personal gain.76 Others lacked confidence but because of their predisposing personal qualities and exposure to research, which was facilitated by workplace research opportunities, they had positive attitude towards research.16,55,68,84–87
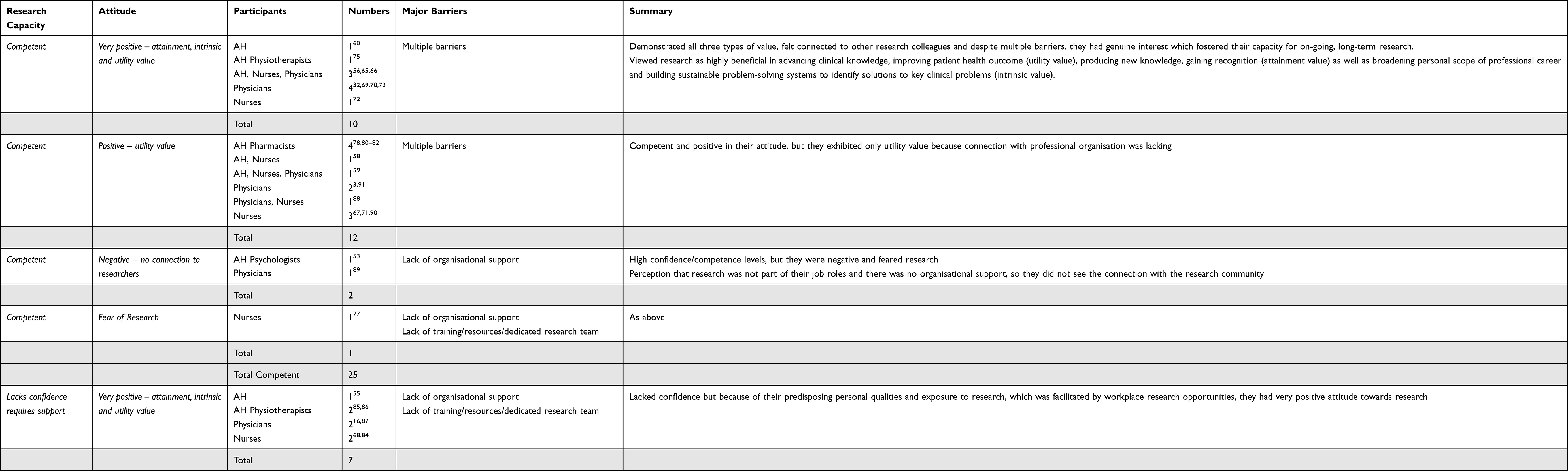 |
Table 5 Integration of Theoretical Framework Elements by Participant Groups |
Overall, the type of value attributed to research directly influenced the relevance of barriers and affected motivation to participate in research. As shown in Figure 2, participants who were very positive displayed an attitude inclusive of attainment, intrinsic and utility values as well as connectedness to research and were able to overcome the barriers relating to cost with a display of great autonomy. HPs who were positive but lacking confidence/requiring support, mainly subscribed to utility values and were limited by the burden of barriers. HPs who reported low expectancy and competence, exhibited total lack of value for research, had no sense of belonging or attachment to researchers in their organisations, focused on the barriers/ limitations and therefore had no interest to undertake research. These findings indicate that prior exposure to research training increases expectancy and confidence, but type of value placed on research determines the strength of connection to research, and ability to disregard the myriads of challenges/barriers. High values foster on-going intrinsic commitment and long-term motivation to engage with research.
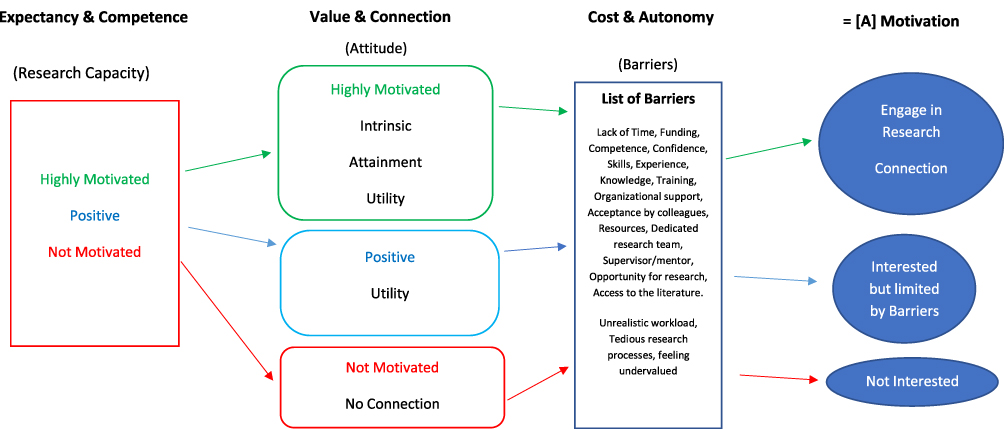 |
Figure 2 Process of motivation to do research. |
Discussion
Various strategies and assumptions have been made and tested regarding the reasons for the decline in the uptake/continuation of research by HPs and how to build research capacity among HPs.3,7,55,61,96–98 Despite these efforts, little headway has been made which necessitates taking the opportunity of examining HPs engagement in research through a different lens. This review has explored the literature with a focus on understanding HPs’ motivation to do research through the EVC33,34 and SDT40,41 theoretical constructs and an investigation of expectancy, research capacity, attitude and barriers as precursors to motivation to undertake/continue with research. The elements in these theories have been used to understand the interactions and sequence of occurrence of themes to allow for long-term motivation to do research.
Based on SDT with its elements of competence, connection, and autonomy, the review findings posit that competence is enhanced if there is prior exposure to research in undergraduate/postgraduate space and this then influences graduates when they come into the workspace as it helps them to get that connection and a sense of belonging with other research active members of the organisation and that makes them feel that they are in control and they are able to keep going.41,44 However, if HPs have not had prior exposure to research and there is no perceived organisational support, they see the barriers or limitations more and that sometimes frightens them and stops them from engaging in research.44
EVC follows a similar pattern as it considers HPs’ expectancy or anticipated ability to do research which is fostered by that confidence gained from prior exposure to research in their undergraduate/postgraduate years. Taking it one step further, EVC helps to unpack the importance of value that is attached to research. The findings from this review predicate that even when research training is strong, which is important for confidence building and expectancy to do well in research, what keeps HPs motivated and helps them to overlook or disregard the myriads of barriers is the kind of value they attach to research.
Factors which motivate and facilitate research by HPs are dependent on both extrinsic and intrinsic variables.49 These variables are dynamic in nature and are influenced at the individual, organisational and cultural level in a dynamic research ecosystem.98 In this review, in most cases those who were competent in their research capacity, with high expectations of success and had very positive attitude towards research demonstrated all three values attributed to doing research (intrinsic – personal enjoyment, utility – future usefulness and attainment – doing well). This group of HPs were keen to take up research despite the barriers. Those who had a positive attitude were only motivated to do research because of its utility value, although they did not necessarily see it as having personal relevance for themselves.57,61,88,90,93 Those who were unmotivated did not see any connection or relatedness to the research experience for themselves, felt it was too difficult and had very low ability beliefs which de-valued active participation in research.54,74,76,77 Ability beliefs have been predicted to positively impact expectancy and research capacity, while task difficulty negatively impacts expectancy.33
The barriers to involvement in research which were identified in this review corroborate previous literature findings and centre around lack of knowledge and skills to conduct research,94,97 lack of protected research time,99,100 lack of funding69,101,102 and lack of support from colleagues, and the organisation.54,74,76,77 Clinical workloads take precedence over time available for research17,56 and this was confirmed in a recent Australian study which reported that 55% of research active doctors spend most of their time on clinical activities.3 Studies have also shown that research careers pay lower salary than clinical careers3,13 and offer lower job security relative to clinical careers.3,101 These issues are compounded by the difficulty in getting research grants13,32 and the lower funding rates available for research.3,102 Lack of resources was also a deterrent for otherwise motivated medical professionals to engage in research.16,32
The lack of support, acceptance by colleagues, reward and acknowledgement highlighted in this review can be attributed to lack of organisational support. Studies have shown that organisational challenges such as lack of acknowledgement and recognition of medical professionals undertaking a research role by their peers and by the organisation for which they work are significant barriers to research involvement.32,103 Several studies found that medical professionals had difficulty finding a mentor for their research project.102,104,105 In this review, for HPs who were negative, the emphasis was on the concept of lack of mentorship which would have offered a sense of connection to inspire an attitude of value (intrinsic, attainment, and/ or utility), boosting confidence and providing support for research participation.106,107 Effective mentorship has been identified as vital for HPs undertaking research70,108,109 and an important contributor to research success.110 Mentoring programmes that support the health researcher with resources and expertise will optimise research training and research outcomes.60,111 Healthcare organisations in Australia,21 the US108,110,111 and the UK96 have been encouraged to include meaningful mentoring programmes into their research profile at all stages of the clinical academic training and career pathway from medical student, intern and pre-vocational doctor, vocational trainee, post-doctoral/early fellowships and definite appointment.21 Positive reinforcement by research active HPs is critical at all stages of the research training and career pipeline.3,112 An effective mentorship program is integral to establishing or building a research culture within the HPs’ organisation.56 Conducive organisational research culture enhances research capacity building, which is enhanced by developing organisational structure, processes and systems, developing appropriate links with external partners and research career pathways16,94 to enable health researchers to conduct research in a safe, supportive and nurturing environment where research is valued and resourced.96,113 An organisational culture that supports research and enables building research capacity through supporting research training, quarantined time for research and adequate funding espouses the value of research which engenders connection. Overall, barriers impact on attitude to conduct research66,70,80,82–84,87–89,100 and by implication affect response to the cost of doing research and significantly contribute to undervaluing research.49,65
The concept of value in research is of primary importance and is an area that needs to be focused on, particularly during training.61,64 Emphasis should be placed on the value elements of motivation, with focus on attainment and intrinsic motivation. Explaining that value goes beyond the utility of research in clinical practice, is a useful way of introducing and developing an appreciation of attainment value which is about professional gains and fostering intrinsic value, which is about being involved in finding solutions to clinical problems as such an approach may keep HPs engaged in research. This strategy may be worthy of consideration by accrediting professional bodies, educational institutions, funding bodies and workplace organisations in their endeavours to foster uptake and retention of research activities by HPs.
Of all three HP groups, AHPs were the most lacking confidence and requiring support which may be attributed to having less research training and research experience than the other groups. Nonetheless, it is interesting to note that amongst the AHPs, the pharmacists were the most confident to undertake research. The findings of this systematic review also indicate that medical professionals, possibly due to their prior exposure to research training and research experience are in a better position than AHPs and nurses to overcome the barriers. Future studies could investigate how HPs navigate their way through barriers at different career stages – early, mid-career, late career. Future explorations could also consider whether the three HP groups (AHPs, medical doctors, nurses) follow similar or dissimilar trajectories in terms of how their research values change over their career stages.
The ability to accurately inform potential researchers regarding the attractions and barriers to health research in their careers, and to implement strategies to reverse current concerning trends in the decline of health professionals engaging in research will help to ensure HPs’ leadership in HMR into the foreseeable future. Furthermore, utilisation of theoretical frameworks that inform processes and facilitate a culture of HP research would enable optimisation of health workforce research capability and high-quality care.
Strengths and Limitations
The major strength of this review is the integration of the EVC and SDT theories which offer an overarching construct that provide in-depth understanding into HPs’ motivation to do research. Additionally, the quality appraisal of the reviewed articles provides evidence for the methodological rigour of the reviewed articles and strengthens the interpretation of the findings because all the articles were assessed as medium to high-quality studies. However, interpretation of the results must be applied cautiously due to some inherent limitations of the review. Generalisation of the findings may be limited by the authors’ interpretation of the investigated research elements/domains in the reviewed papers. Other limitations of this review include the heterogeneity of the included studies and the possible exclusion of relevant studies due to the pre-set inclusion criteria.
Conclusion
Overall, this review provides good evidence for the practicality of EVC and SDT in understanding HPs’ motivation to do research. In line with SDT elements, competence is enhanced by prior exposure to research training, and this enhances autonomy and connection with other research active members of the organisation. Similarly, EVC considers HPs’ expectancy or anticipated ability to do research which is fostered by confidence gained from prior exposure to research. EVC further emphasises the impactful effect of the type of value attributed to research on the relevance HPs attach to the myriads of barriers they face and their motivation to engage in research. The findings from this systematic review indicate priority facilitators to research participation revolve around the themes of allocated time for research, funding, research training, strong organisational research culture and mentorship program. The importance of confidence building and the expectation to succeed leading to competency through research education and training is accentuated. Nonetheless, autonomy and on-going motivation to actively engage in research are mostly influenced by HPs’ attitude vis-A-vis the three value components – intrinsic attainment and utility. Therefore, emphasis on the value attributes of research may be worthy of note by accrediting professional bodies, educational institutions, funding bodies and workplace organisations as critical to the research pipeline and the motivation of HPs to undertake research.
Acknowledgments
The authors acknowledge Mr Chris Parker, Manager Library Services, the Prince Charles Hospital, Chermside, Queensland for his input in the development of the search strategy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hay-Smith EJ, Brown M, Anderson L, Treharne GJ. Once a clinician, always a clinician: a systematic review to develop a typology of clinician-researcher dual-role experiences in health research with patient-participants. BMC Med Res Methodol. 2016;16:95. doi:10.1186/s12874-016-0203-6
2. Hall AK, Mills SL, Lund PK. Clinician-investigator training and the need to pilot new approaches to recruiting and retaining this workforce. Acad Med. 2017;92(10):1382–1389. doi:10.1097/ACM.0000000000001859
3. Mills JMZ, Januszewski AS, Robinson BG, Traill CL, Jenkins AJ, Keech AC. Attractions and barriers to Australian physician-researcher careers: physician-researcher influences. Intern Med J. 2019;49(2):171–181. doi:10.1111/imj.14086
4. Pang T, Sadana R, Hanney S, Bhutta ZA, Hyder AA, Simon J. Knowledge for better health: a conceptual framework and foundation for health research systems. Bull World Health Organ. 2003;81(11):815–820.
5. Burns LJ, Clayton CP, George JN, Mitchell BS, Gitlin SD. The effect of an intense mentoring program on junior investigators’ preparation for a patient-oriented clinical research career. Acad Med. 2015;90(8):1061–1066. doi:10.1097/ACM.0000000000000742
6. Association of Australian Medical Research Institutes. Health research in Australia; 2020. Available from: https://aamri.org.au/health-medical-research/fast-facts-on-medical-research/.
7. Traill CL, Januszewski AS, Larkins R, Keech AC, Jenkins AJ. Time to research Australian physician-researchers. Intern Med J. 2016;46(5):550–558. doi:10.1111/imj.13043
8. Wyngaarden JB. The clinical investigator as an endangered species. N Engl J Med. 1979;301(23):1254–1259. doi:10.1056/NEJM197912063012303
9. Funston G, Piper RJ, Connell C, Foden P, Young AMH, O’Neill P. Medical student perceptions of research and research-orientated careers: an international questionnaire study. Med Teach. 2016;38(10):1041–1048. doi:10.3109/0142159X.2016.1150981
10. McKinney RE. The daunting career of the physician-investigator. Acad Med. 2017;92(10):1368–1370. doi:10.1097/ACM.0000000000001869
11. Deligiannidis KM. The physician-scientist workforce in the United States. Acta Psychiatr Scand. 2015;132(4):317–318. doi:10.1111/acps.12435
12. National Institutes of Health. Physician-scientist workforce working group report; 2014. Available from: https://acd.od.nih.gov/documents/reports/PSW_Report_ACD_06042014.pdf.
13. Lander B, Hanley GE, Atkinson-Grosjean J. Clinician-scientists in Canada: barriers to career entry and progress. PLoS One. 2010;5(10):04. doi:10.1371/journal.pone.0013168
14. McLean AL, Saunders C, Velu PP, Iredale J, Hor K, Russell CD. Twelve tips for teachers to encourage student engagement in academic medicine. Med Teach. 2013;35(7):549–554. doi:10.3109/0142159X.2013.775412
15. Karlsson L, Stockfelt M, Finizia C. Improved information in medical school may increase recruitment of physician-scientists. Lakartidningen. 2014;111(47):2108–2110.
16. Conradie A, Duys R, Forget P, Biccard BM. Barriers to clinical research in Africa: a quantitative and qualitative survey of clinical researchers in 27 African countries. Br J Anaesth. 2018;121(4):813–821. doi:10.1016/j.bja.2018.06.013
17. Woo KT, Wong KS, Lee EJ, Chan CM. How can we improve clinical research in clinical practice with better research outcome? Ann Acad Med Singapore. 2011;40(11):499–506.
18. Anwer LA, Anwer AN, Mahmood M, Abu-Zaid A, Shareef MA. Meeting the global need for physician-scientists: a Middle Eastern imperative. Med. 2014;19:26138.
19. Abu-Zaid A. The endangered clinician-investigator profession in Saudi Arabia: curricular attention is required. Ann Saudi Med. 2018;38(1):69–70. doi:10.5144/0256-4947.2018.69
20. Jain MK, Cheung VG, Utz PJ, Kobilka BK, Yamada T, Lefkowitz R. Saving the endangered physician-scientist - a plan for accelerating medical breakthroughs. N Engl J Med. 2019;381(5):399–402. doi:10.1056/NEJMp1904482
21. Windsor J, Garrod T, Talley NJ, et al. The clinical academic workforce in Australia and New Zealand: report on the second binational summit to implement a sustainable training pathway: sustainable clinical academic workforce. Intern Med J. 2017;47(4):394–399. doi:10.1111/imj.13356
22. Al-Busaidi IS, Tarr GP. Dissemination of results from medical student public health research training and factors associated with publication. Postgrad Med J. 2018;94(1112):330–334. doi:10.1136/postgradmedj-2017-135361
23. Al-Busaidi IS, Wells CI. Stimulating the clinical academics of tomorrow: a survey of research opportunities for medical students in New Zealand. N Z Med J. 2017;130(1462):80–88.
24. Australian Institute of Health and Welfare. Medical labor force 2002. Canberra: Australian Institute of Health and Welfare; 2004. Available from: https://www.aihw.gov.au/reports/workforce/medical-labour-force-2002/formats.
25. Australian Institute of Health and Welfare. Medical workforce 2010. Canberra: Australian institute of Health and Welfare; 2012. Available from: https://www.aihw.gov.au/getmedia/75c1aba7-71b3-4844-bd8c-9afad41e8287/14055.pdf.aspx?inline=true.
26. Medical Deans Australia and New Zealand (MDANZ). Medical schools outcomes database national data report 2013–2017. Sydney, NSW: Medical Deans Australia and New Zealand; 2018. Available from: https://medicaldeans.org.au/md/2019/09/2018-MSOD-Final-report.pdf.
27. Pain K, Hagler P, Warren S. Development of an instrument to evaluate the research orientation of clinical professionals. Can J Rehabil. 1996;9(2):93–100.
28. Traill CL, Januszewski AS, Larkins RG, Keech AC, Jenkins AJ. Time to research Australian female physician-researchers. Intern Med J. 2016;46(4):412–419. doi:10.1111/imj.12986
29. Pain T, Plummer D, Pighills A, Harvey D. Comparison of research experience and support needs of rural versus regional allied health professionals. Aust J Rural Health. 2015;23(5):277–285. doi:10.1111/ajr.12234
30. Hulcombe J, Sturgess J, Souvlis T, Fitzgerald C. An approach to building research capacity for health practitioners in a public health environment: an organisational perspective. Austr Health Rev. 2014;38(3):252–258. doi:10.1071/AH13066
31. Harding K, Lynch L, Porter J, Taylor NF. Organisational benefits of a strong research culture in a health service: a systematic review. Aust Health Rev. 2017;41(1):45–53. doi:10.1071/AH15180
32. Jones RD, Griffith KA, Ubel PA, Stewart A, Jagsi R. A mixed-methods investigation of the motivations, goals, and aspirations of male and female academic medical faculty. Acad Med. 2016;91(8):1089–1097. doi:10.1097/ACM.0000000000001244
33. Eccles JS, Adler TF, Futterman R, et al. Expectancies values and academic behaviors. In: Spence J, editor. Achievement and Achievement Motives. San Francisco, CA: W H Freeman; 1983:74–146.
34. Eccles JS, Wigfield A. Motivational beliefs, values, and goals. Annu Rev Psychol. 2002;53(1):109–132. doi:10.1146/annurev.psych.53.100901.135153
35. Wigfield A, Eccles JS. Expectancy–value theory of achievement motivation. Contemp Educ Psychol. 2000;25(1):68–81. doi:10.1006/ceps.1999.1015
36. Nikkar-Esfahani A, Jamjoom AA, Fitzgerald JE. Extracurricular participation in research and audit by medical students: opportunities, obstacles, motivation and outcomes. Med Teach. 2012;34(5):e317–24. doi:10.3109/0142159X.2012.670324
37. Griffin MF, Hindocha S. Publication practices of medical students at British medical schools: experience, attitudes and barriers to publish. Med Teach. 2011;33(1):e1–8. doi:10.3109/0142159X.2011.530320
38. Orsini C, Binnie VI, Wilson SL. Determinants and outcomes of motivation in health professions education: a systematic review based on self-determination theory. J Educ Eval Health Prof. 2016;13:19. doi:10.3352/jeehp.2016.13.19
39. Robinson GF, Switzer GE, Cohen ED, et al. Shortening the work preference inventory for use with physician scientists: WPI-10. Clin Transl Sci. 2014;7(4):324–328. doi:10.1111/cts.12132
40. Ryan R. Self determination theory and well being. Soc Psychol. 2009;84(822):848.
41. Ryan RM, Deci EL. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness. New York: Guilford Press; 2017.
42. Bernard D, Martin JJ, Kulik N. Self‐determination theory and well‐being in the health care profession. J Appl Biobehav Res. 2014;19(3):157–170. doi:10.1111/jabr.12023
43. Deci EL, Olafsen AH, Ryan RM. Self-determination theory in work organizations: the state of a science. Annu Rev Organ Psychol Organ Behav. 2017;4:19–43. doi:10.1146/annurev-orgpsych-032516-113108
44. Self-determination theory of motivation: why intrinsic motivation matters; 2019. Available from: https://positivepsychology.com/self-determination-theory/.
45. Moher D, Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration, Journal of clinical epidemiology. 2009;62(10).
46. Barron KE, Hulleman CS. Expectancy-value-cost model of motivation. In: Wright JD, editor. International Encyclopedia of the Social & Behavioral Sciences. 8.
47. Krippendorff K. Content Analysis: An Introduction to Its Methodology.
48. Allen M. The Sage Encyclopedia of Communication Research Methods. Thousand Oaks, CA: SAGE Publication; 2017.
49. Matus J, Walker A, Mickan S. Research capacity building frameworks for allied health professionals - a systematic review. BMC Health Serv Res. 2018;18. doi:10.1186/s12913-018-3518-7
50. Sirriyeh R, Lawton R, Gardner P, Armitage G. Reviewing studies with diverse designs: the development and evaluation of a new tool. J Eval Clin Pract. 2012;18(4):746–752. doi:10.1111/j.1365-2753.2011.01662.x
51. White G. Producing and utilising research: barriers for a nursing faculty in Oman. Middle East J Nurs. 2013;7(2):3–8. doi:10.5742/MEJN.2013.72223
52. Borkowski D, McKinstry C, Cotchett M. Research culture in a regional allied health setting. Aust J Prim Health. 2017;23(3):300–306. doi:10.1071/PY16085
53. Elphinston RA, Pager S. Untapped potential: psychologists leading research in clinical practice. Aust Psychol. 2015;50(2):115–121. doi:10.1111/ap.12102
54. Finch E, Cornwell P, Nalder E, Ward E. Uncovering motivators and stumbling blocks: exploring the clinical research experiences of speech-language pathologists. Int J Speech Lang Pathol. 2015;17(2):138–147. doi:10.3109/17549507.2014.930175
55. Harvey D, Plummer D, Nielsen I, Adams R, Pain T. Becoming a clinician researcher in allied health. Aust Health Rev. 2016;40(5):562. doi:10.1071/AH15174
56. Hiscock H, Ledgerwood K, Danchin M, Ekinci E, Johnson E, Wilson A. Clinical research potential in Victorian hospitals: the Victorian clinician researcher needs analysis survey. Intern Med J. 2014;44(5):477–482. doi:10.1111/imj.12396
57. McMaster R, Jammali-Blasi A, Andersson-Noorgard K, Cooper K, McInnes E. Research involvement, support needs, and factors affecting research participation: a survey of Mental Health Consultation Liaison Nurses. Int J Ment Health Nurs. 2013;22(2):154–161. doi:10.1111/j.1447-0349.2012.00857.x
58. McNab M, Berry A, Skapetis T. The potential of a lecture series in changing intent and experience among health professionals to conduct research in a large hospital: a retrospective pre-post design. BMC Med Educ. 2019;19(1):124. doi:10.1186/s12909-019-1548-4
59. Oliver-Baxter J, Brown L, McIntyre E. Surviving or thriving in the primary health care research workforce: the Australian experience. Aust J Prim Health. 2017;23(2):183–188. doi:10.1071/PY15190
60. Pager S, Holden L, Golenko X. Motivators, enablers, and barriers to building allied health research capacity. J Multidiscip Healthc. 2012;5:53–59. doi:10.2147/JMDH.S27638
61. Pain T, Petersen M, Fernando M. Building allied health research capacity at a regional Australian hospital: a follow-up study. Internet J Allied Health Sci Pract. 2018;16(4):1–10.
62. Wenke R, Mickan S, Bisset L. A cross sectional observational study of research activity of allied health teams: is there a link with self-reported success, motivators and barriers to undertaking research? BMC Health Serv Res. 2017;17:1–10. doi:10.1186/s12913-017-1996-7
63. Wenke R, Noble C, Weir KA, Mickan S. What influences allied health clinician participation in research in the public hospital setting: a qualitative theory-informed approach. BMJ Open. 2020;10(8):e036183. doi:10.1136/bmjopen-2019-036183
64. Alison JA, Zafiropoulos B, Heard R. Key factors influencing allied health research capacity in a large Australian metropolitan health district. J Multidiscip Healthc. 2017;10:277. doi:10.2147/JMDH.S142009
65. Marshall AP, Roberts S, Baker MJ, et al. Survey of research activity among multidisciplinary health professionals. Aust Health Rev. 2016;40(6):667–673. doi:10.1071/AH15156
66. Paget SP, Lilischkis KJ, Morrow AM, Caldwell PH. Embedding research in clinical practice: differences in attitudes to research participation among clinicians in a tertiary teaching hospital. Intern Med J. 2014;44(1):86–89. doi:10.1111/imj.12330
67. Albert NM, Rice KL, Waldo MJ, et al. Clinical nurse specialist roles in conducting research: changes over 3 years. Clin Nurse Spec. 2016;30(5):292–301. doi:10.1097/NUR.0000000000000236
68. Chan GK, Barnason S, Dakin CL, et al. Barriers and perceived needs for understanding and using research among emergency nurses. J Emerg Nurs. 2011;37(1):24–31. doi:10.1016/j.jen.2009.11.016
69. Cianciolo AT, Mitzelfelt J, Ghareeb A, Zahid MF, Akbar R, Ghias K. Physician-scientist or basic scientist? Exploring the nature of clinicians’ research engagement. Adv Health Sci Educ. 2020;26:353–367.
70. Mansi A, Karam WN, Chaaban MR. Attitudes of residents and program directors towards research in otolaryngology residency. Ann Otol Rhinol Laryngol. 2019;128(1):28–35. doi:10.1177/0003489418804565
71. Scala E, Patterson BJ, Stavarski DH, Mackay P. Engagement in research: a clinical nurse profile and motivating factors. J Nurses Prof Dev. 2019;35(3):137–143. doi:10.1097/NND.0000000000000538
72. Siedlecki S, Albert N. Research-active clinical nurses: against all odds. J Clin Nurs. 2016;26:766–773. doi:10.1111/jocn.13523
73. Silberman EK, Belitsky R, Bernstein CA, et al. Recruiting researchers in psychiatry: the influence of residency vs early motivation. Acad Psychiatry. 2012;36(2):85–90. doi:10.1176/appi.ap.10010010
74. Bench S, Dowie-Baker JA, Fish P. Orthopaedic nurses’ engagement in clinical research; an exploration of ideas, facilitators and challenges. Int J Orthop Trauma Nurs. 2019;35:100699. doi:10.1016/j.ijotn.2019.04.002
75. Connolly B, Allum L, Shaw M, Pattison N, Dark P. Characterising the research profile of the critical care physiotherapy workforce and engagement with critical care research: a UK national survey. BMJ Open. 2018;8(6):e020350. doi:10.1136/bmjopen-2017-020350
76. Lowrie R, Morrison G, Lees R, et al. Research is ‘a step into the unknown’: an exploration of pharmacists’ perceptions of factors impacting on research participation in the NHS. BMJ Open. 2015;5(12):e009180. doi:10.1136/bmjopen-2015-009180
77. Snelgrove S, James M. Graduate nurses’ and midwives’ perceptions of research. J Res Nurs. 2011;16(1):7–20. doi:10.1177/1744987110387484
78. Stewart D, Cunningham S, Strath A, et al. A theoretically informed survey of the views and experiences of practicing pharmacists on research conduct, dissemination and translation. Res Social Adm Pharm. 2019;15(11):1298–1308. doi:10.1016/j.sapharm.2018.12.005
79. Luckson M, Duncan F, Rajai A, Haigh C. Exploring the research culture of nurses and allied health professionals (AHPs) in a research-focused and a non-research-focused healthcare organisation in the UK. J Clin Nurs. 2018;27:E1462–E76. doi:10.1111/jocn.14264
80. Sarwar MR, Saqib A, Riaz T, Aziz H, Arafat M, Nouman H. Attitude, perception, willingness, motivation and barriers to practice-based research: a cross-sectional survey of hospital pharmacists in Lahore, Punjab, Pakistan. PLoS One. 2018;13(9):e0203568. doi:10.1371/journal.pone.0203568
81. Stewart D, Al Hail M, Abdul Rouf PV, et al. Building hospital pharmacy practice research capacity in Qatar: a cross-sectional survey of hospital pharmacists. Int J Clin Pharm. 2015;37(3):511–521. doi:10.1007/s11096-015-0087-2
82. Sultana K, Al Jeraisy M, Al Ammari M, Patel R, Zaidi STR. Attitude, barriers and facilitators to practice-based research: cross-sectional survey of hospital pharmacists in Saudi Arabia. J Pharm Policy Pract. 2016;9(1):4. doi:10.1186/s40545-016-0052-z
83. Akerjordet K, Lode K, Severinsson E. Clinical nurses’ attitudes towards research, management and organisational resources in a university hospital: part 1. J Nurs Manag. 2012;20(6):814–823. doi:10.1111/j.1365-2834.2012.01477.x
84. Berthelsen CB, Holge-Hazelton B. Orthopaedic nurses’ attitudes towards clinical nursing research - a cross-sectional survey. Int J Orthop Trauma Nurs. 2015;19(2):74–84. doi:10.1016/j.ijotn.2014.10.004
85. Dannapfel P, Peolsson A, Nilsen P. What supports physiotherapists’ use of research in clinical practice? A qualitative study in Sweden. Implement Sci. 2013;8:31. doi:10.1186/1748-5908-8-31
86. Dannapfel P, Peolsson A, Stahl C, Oberg B, Nilsen P. Applying self-determination theory for improved understanding of physiotherapists’ rationale for using research in clinical practice: a qualitative study in Sweden. Physiother. 2014;30(1):20–28.
87. Mahmoud AO, Ayanniyi AA, Lawal A, Omolase CO, Ologunsua Y, Samaila E. Survey of medical specialists on their attitudes to and resources for health research in Nigeria. Ann Afr Med. 2011;10(2):144–149. doi:10.4103/1596-3519.82078
88. van Hoving DJ, Brysiewicz P. African emergency care providers’ attitudes and practices towards research. Afr J Emerg Med. 2017;7(1):9–14. doi:10.1016/j.afjem.2017.01.003
89. Choo TL, Muninathan P, Pung CM, Ramanathan GRL. Attitudes, barriers and facilitators to the conduct of research in government hospitals: a cross-sectional study among specialists in government hospitals, northern states of Malaysia. Med J Malaysia. 2017;72(1):26–31.
90. Torres GCS, Estrada MG, Sumile EFR, Macindo JRB, Maravilla SN, Hendrix CC. Assessment of research capacity among nursing faculty in a clinical intensive university in the Philippines. Nurs Forum. 2017;52(4):244–253. doi:10.1111/nuf.12192
91. Ito-Ihara T, Hong JH, Kim OJ, et al. An international survey of physicians regarding clinical trials: a comparison between Kyoto University Hospital and Seoul National University Hospital. BMC Med Res Methodol. 2013;13:130. doi:10.1186/1471-2288-13-130
92. McDonald E, Zytaruk N, Heels-Ansdell D. Motivators and stressors for Canadian research coordinators in critical care: the motivate survey. Am J Crit Care. 2020;29(1):41–48. doi:10.4037/ajcc2020627
93. Janssen J, Hale L, Mirfin-Veitch B, Harland T. Perceptions of physiotherapists towards research: a mixed methods study. Physiotherapy. 2016;102(2):210–216. doi:10.1016/j.physio.2015.04.007
94. Borkowski D, McKinstry C, Cotchett M, Williams C, Haines T. Research culture in allied health: a systematic review. Aust J Prim Health. 2016;22(4):294–303. doi:10.1071/PY15122
95. Pager S, Pager S. A team effort: enabling rehabilitation professional research in the real world. Int J Ther Rehabil. 2014;21(3):107. doi:10.12968/ijtr.2014.21.3.107
96. Lingard L, Zhang P, Strong M, Steele M, Yoo J, Lewis J. Strategies for supporting physician-scientists in faculty roles: a narrative review with key informant consultations. Acad Med. 2017;92(10):1421–1428. doi:10.1097/ACM.0000000000001868
97. Gardner A, Smyth W, Renison B, Cann T, Vicary M. Supporting rural and remote area nurses to utilise and conduct research: an intervention study. Collegian. 2012;19(2):97–105. doi:10.1016/j.colegn.2011.09.005
98. Slade SC, Philip K, Morris ME. Frameworks for embedding a research culture in allied health practice: a rapid review. Health Res Policy Syst. 2018;16:1. doi:10.1186/s12961-018-0304-2
99. Noble C, Billett SR, Phang DTY, Sharma S, Hashem F, Rogers GD. Supporting resident research learning in the workplace: a rapid realist review. Acad Med. 2018;93:1732–1740. doi:10.1097/ACM.0000000000002416
100. Siemens DR, Punnen S, Wong J, Kanji N. A survey on the attitudes towards research in medical school. BMC Med Educ. 2010;10:4. doi:10.1186/1472-6920-10-4
101. Ganetzky RD. Becoming a physician-scientist: a view looking up from base camp. Acad Med. 2017;92(10):1373–1374. doi:10.1097/ACM.0000000000001876
102. Saeed I, Khan NF, Bari A, Khan RA. Factors contributing to the lack of interest in research activities among postgraduate medical students. Pak J Med Sci. 2018;34(4):913–917. doi:10.12669/pjms.344.15411
103. Rahman S, Majumder MAA, Shaban SF, et al.Physician participation in clinical research and trials: issues and approaches. Adv Med Educ Pract. 2011;(default):85. doi:10.2147/AMEP.S14103
104. Hirschtritt ME, Heaton PM, Insel TR. Preparing physician-scientists for an evolving research ecosystem. JAMA. 2018;320(1):31–32. doi:10.1001/jama.2018.4478
105. Kwan JM, Daye D, Schmidt ML, et al. Exploring intentions of physician-scientist trainees: factors influencing MD and MD/PhD interest in research careers. BMC Med Educ. 2017;17(1):115. doi:10.1186/s12909-017-0954-8
106. Deci EL, Ryan RM. Intrinsic Motivation and Self-Determination in Human Behavior.
107. Deci EL, Ryan RM. The ‘what’ and ‘why’ of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000;11(4):227–268. doi:10.1207/S15327965PLI1104_01
108. Byington CL, Keenan H, Phillips JD, et al. A matrix mentoring model that effectively supports clinical and translational scientists and increases inclusion in biomedical research: lessons from the university of Utah. Acad Med. 2016;91(4):497–502. doi:10.1097/ACM.0000000000001021
109. Sng JH, Pei Y, Toh YP, Peh TY, Neo SH, Krishna LKR. Mentoring relationships between senior physicians and junior doctors and/or medical students: a thematic review. Med Teach. 2017;39(8):866–875. doi:10.1080/0142159X.2017.1332360
110. Yin HL, Gabrilove J, Jackson R, et al. Sustaining the clinical and translational research workforce: training and empowering the next generation of investigators. Acad Med. 2015;90(7):861–865. doi:10.1097/ACM.0000000000000758
111. Daye D, Patel CB, Ahn J, Nguyen FT. Challenges and opportunities for reinvigorating the physician-scientist pipeline. J Clin Invest. 2015;125(3):883–887. doi:10.1172/JCI80933
112. Steer CJ, Jackson PR, Hornbeak H, McKay CK, Sriramarao P, Murtaugh MP. Team science and the physician-scientist in the age of grand health challenges. Ann N Y Acad Sci. 2017;1404(1):3–16. doi:10.1111/nyas.13498
113. Gallagher R, Sadler L, Kirkness A, Belshaw J, Roach K, Warrington D. Collaboration: a solution to the challenge of conducting nursing research in cardiac rehabilitation. Collegian. 2013;20(4):255–259. doi:10.1016/j.colegn.2012.11.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.