Back to Journals » Nature and Science of Sleep » Volume 18

Restoring Physiological Normoxia as an Adjuvant Strategy to Improve Cancer Treatment Outcomes
Authors Mas Bermejo C ![]() , Mas Gómez C
, Mas Gómez C ![]() , Sevilla-García-MA, O'Connor-Reina C, Falardo Ramos S
, Sevilla-García-MA, O'Connor-Reina C, Falardo Ramos S ![]() , Alonso-Romero JL, Bravo-González LA
, Alonso-Romero JL, Bravo-González LA ![]()
Received 14 January 2026
Accepted for publication 23 March 2026
Published 19 May 2026 Volume 2026:18 593331
DOI https://doi.org/10.2147/NSS.S593331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah L Appleton
Carlos Mas Bermejo,1 Carlos Mas Gómez,1 Ma-Agustina Sevilla-García,2 Carlos O’Connor-Reina,3 Susana Falardo Ramos,4 José Luis Alonso-Romero,5 Luis-Alberto Bravo-González6
1Center of Integrated Adult Dentistry, Murcia, Spain; 2Department of Otolaryngology, Hospital Universitario Virgen de la Arrixaca, Murcia, Spain; 3Department of Otolaryngology, Hospital Quirón-Salud Marbella, Marbella, Spain; 4Sleep Medicine Program, Universidade Católica Portuguesa, Porto, Portugal; 5Department of Medical Oncology, Hospital Clínico Universitario Virgen de la Arrixaca, Murcia, Spain; 6Department of Orthodontics and Dentofacial Orthopedics, University of Murcia, Murcia, Spain
Correspondence: Carlos Mas Bermejo, Email [email protected]
Abstract: Hypoxia is a central driver of cancer progression, immune evasion, and resistance to anticancer therapies. While hypoxia has traditionally been considered an intrinsic feature of the tumor microenvironment, growing evidence indicates that chronic intermittent hypoxia—particularly that occurring during sleep—represents a systemic and potentially modifiable contributor to hypoxia-driven oncogenic signaling. Sleep-disordered breathing is the most prevalent cause of nocturnal intermittent hypoxia and induces oxidative stress, inflammation, metabolic reprogramming, and immune dysregulation through mechanisms that overlap with those observed in hypoxic tumors.This narrative review synthesizes current experimental, translational, and clinical evidence supporting the concept that restoration of physiological normoxia, especially during sleep, may attenuate hypoxia-mediated cancer biology and improve responsiveness to standard anticancer therapies. We examine the biological effects of normoxia restoration on hypoxia-inducible signaling, redox homeostasis, tumor metabolism, and antitumor immunity, highlighting its potential role as a host-directed, adjuvant strategy rather than a direct tumor-targeting intervention.We further review sleep and airway-centered therapeutic approaches capable of reducing nocturnal hypoxic burden, including continuous positive airway pressure, mandibular advancement devices, upper airway surgery, myofunctional therapy, and respiratory physiotherapy. Although these interventions are not cancer-specific, their ability to stabilize nocturnal oxygenation positions them as clinically relevant tools within a multidisciplinary framework aimed at hypoxia normalization.Collectively, the evidence suggests that nocturnal normoxia is a biologically meaningful and clinically actionable target. Integrating sleep and airway interventions into cancer care pathways may represent a novel avenue to mitigate hypoxia-driven treatment resistance and enhance therapeutic outcomes. Prospective clinical studies incorporating objective measures of hypoxic burden are warranted to validate this integrative approach.Restoration of physiological normoxia is therefore proposed as a host-directed, adjuvant strategy aimed at mitigating hypoxia-driven oncogenic pathways and improving responsiveness to standard anticancer therapies.
Keywords: hypoxia, normoxia, sleep-disordered breathing, intermittent hypoxia, cancer, treatment resistance, CPAP, upper airway therapy
Introduction
Hypoxia is a well-established hallmark of cancer biology, playing a central role in tumor initiation, progression, immune escape, and resistance to anticancer therapies. Within the tumor microenvironment, hypoxic conditions promote angiogenesis, metabolic reprogramming, epithelial–mesenchymal transition, and genomic instability, largely through the activation of hypoxia-inducible factors (HIFs). These adaptive mechanisms provide tumor cells with a selective advantage, facilitating survival, invasiveness, and therapeutic resistance. Consequently, hypoxia has traditionally been regarded as an intrinsic tumor feature and a major obstacle to effective cancer treatment.
In the context of this review, physiological normoxia refers to systemic oxygenation levels compatible with normal tissue metabolism and homeostatic regulation, typically characterized by stable arterial oxygen saturation and the absence of chronic or intermittent hypoxic burden.
In clinical practice, systemic hypoxemia is commonly categorized according to arterial oxygen saturation levels.1 Oxygen saturation values between 91–94% are generally considered mild hypoxia, values between 86–90% moderate hypoxia, and values below 86% severe hypoxia, while oxygen saturation below 90% is widely regarded as clinically significant hypoxemia.1,2 Repeated episodes of desaturation within these ranges during sleep may generate a substantial cumulative hypoxic burden.
However, emerging evidence indicates that hypoxia is not exclusively confined to the tumor microenvironment. Chronic intermittent hypoxia, particularly when occurring systemically and repeatedly during sleep, represents a distinct and clinically relevant biological stressor. Sleep-related breathing disorders, such as obstructive sleep apnea, constitute the most prevalent cause of nocturnal intermittent hypoxia in adults.3 In these conditions, recurrent oxygen desaturation–reoxygenation cycles induce oxidative stress, inflammation, sympathetic activation, and immune dysregulation, thereby creating a systemic milieu that may favor carcinogenesis and tumor progression.
Recent narrative and experimental studies have begun to elucidate mechanistic links between chronic intermittent hypoxia and cancer biology, demonstrating that nocturnal hypoxic burden can activate pro-oncogenic pathways similar to those observed in hypoxic tumor regions. These include HIF-1α stabilization, enhanced glycolytic metabolism, increased expression of immune checkpoint molecules such as PD-L1, and impaired antitumor immune surveillance. Importantly, such processes appear to be temporally patterned, with hypoxia-related signaling peaks occurring predominantly during sleep, suggesting that tumor adaptation and progression may be reinforced during nocturnal periods.
In parallel, anatomical and functional factors contributing to sleep-related hypoxia have gained increasing attention. Altered craniofacial development, maxillary growth deficiency, ankyloglossia, and chronic mouth breathing are increasingly recognized as contributors to upper airway collapse and nocturnal hypoxia. These observations support the concept that systemic hypoxia may precede and facilitate malignant transformation long before the emergence of clinically detectable tumors.
While the deleterious effects of hypoxia on cancer biology are increasingly well characterized, comparatively little attention has been devoted to the potential biological consequences of restoring physiological normoxia. Rather than viewing oxygen solely as a tumor-directed intervention, restoring stable normoxic conditions—particularly during sleep—may represent a strategy to counteract hypoxia-driven oncogenic pathways at the host level. By attenuating HIF-mediated signaling, reducing oxidative stress, improving immune surveillance, and normalizing metabolic homeostasis, physiological normoxia could enhance the effectiveness of standard anticancer therapies without directly targeting tumor cells.
Importantly, several non-pharmacological interventions routinely used in sleep medicine and airway management—including continuous positive airway pressure (CPAP), mandibular advancement devices, myofunctional therapy, speech therapy, and respiratory physiotherapy—have demonstrated efficacy in reducing nocturnal hypoxic burden. These interventions provide a unique opportunity to explore whether normalization of oxygenation can modulate tumor biology and improve treatment outcomes when used as adjuncts to conventional oncologic care. In addition, otorhinolaryngologic interventions aimed at improving upper airway patency may play an important role in selected patients by addressing anatomical contributors to nocturnal hypoxia.
Therefore, the aim of this narrative review is to synthesize current experimental, translational, and clinical evidence addressing the role of physiological normoxia as a potential modulator of hypoxia-driven cancer biology. We focus on the biological mechanisms through which restoration of normoxia—particularly nocturnal normoxia—may enhance antitumor immunity, reduce treatment resistance, and improve the efficacy of standard anticancer therapies. By reframing oxygenation as a systemic and circadian-modulated determinant of cancer behavior, this review seeks to propose a novel integrative perspective linking sleep, airway physiology, and oncology.
Within this framework, nocturnal oxygenation emerges as a potentially overlooked systemic determinant of tumor biology. Recurrent episodes of sleep-related hypoxia may act as a circadian amplifier of hypoxia-driven oncogenic signaling, whereas restoration of stable nocturnal normoxia could represent a biologically plausible strategy to mitigate these effects and enhance responsiveness to anticancer therapies.
Accordingly, this review does not propose normoxia restoration as a tumor-targeted treatment, but rather as a host-directed, adjuvant strategy aimed at mitigating hypoxia-driven mechanisms that influence cancer progression and treatment responsiveness.
An overview of the proposed biological relationships between sleep-related intermittent hypoxia and cancer treatment responsiveness is summarized in Figure 1 while the systemic biological mechanisms linking chronic intermittent hypoxia to tumor behavior are illustrated in Figure 2.
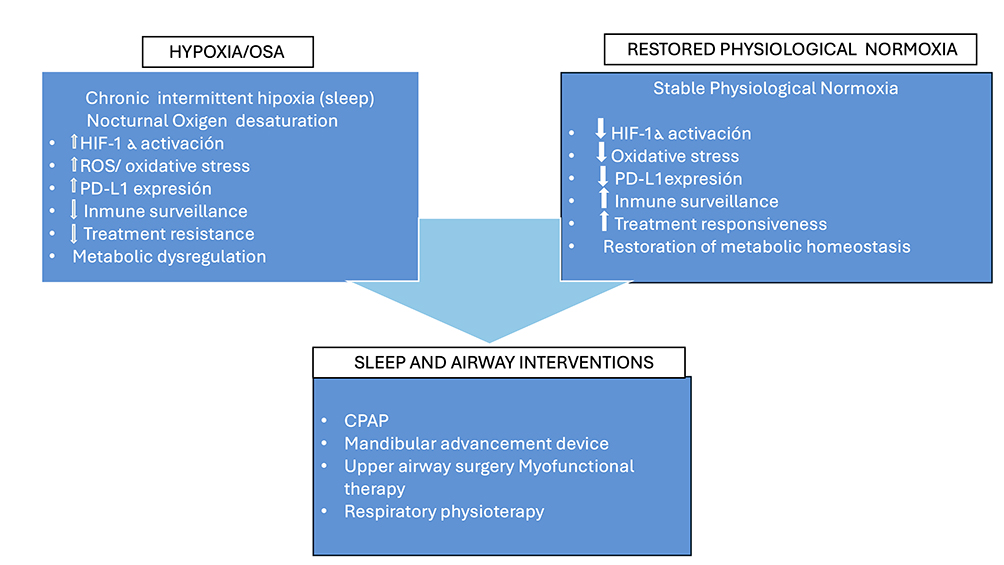 |
Figure 1 Conceptual framework linking sleep-related intermittent hypoxia and cancer treatment responsiveness.Sleep-disordered breathing may generate chronic intermittent hypoxia during sleep, producing repeated cycles of oxygen desaturation and reoxygenation. These oscillatory hypoxic signals activate hypoxia-inducible pathways, oxidative stress responses, inflammatory signaling, and immune modulation. Together, these mechanisms may influence tumor–host interactions and contribute to resistance to anticancer therapies. |
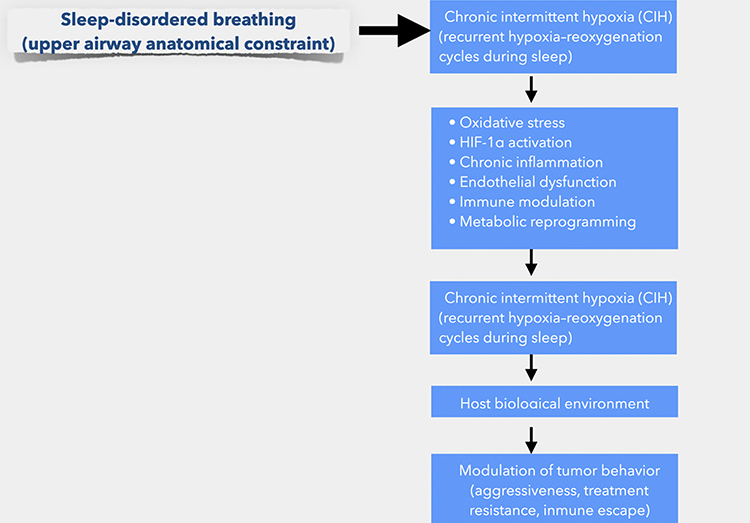 |
Figure 2 Proposed biological relationship between chronic intermittent hypoxia and systemic modulation of tumor biology.Chronic intermittent hypoxia associated with sleep-disordered breathing may influence multiple biological processes relevant to cancer progression, including HIF-1α activation, oxidative stress, metabolic reprogramming, endothelial dysfunction, and immune dysregulation. These systemic alterations may contribute to a tumor-supportive microenvironment and reduce responsiveness to conventional anticancer therapies. |
Narrative Review Methodology
This article was conducted as a narrative review integrating experimental, translational, and clinical evidence related to tumor hypoxia, chronic intermittent hypoxia, and sleep-disordered breathing. Relevant literature was identified through searches of PubMed, Scopus, and Google Scholar using combinations of the following keywords: “hypoxia”, “intermittent hypoxia”, “sleep-disordered breathing”, “obstructive sleep apnea”, “cancer biology”, and “tumor microenvironment”. Priority was given to mechanistic studies, translational research, and clinical investigations addressing hypoxia-related oncogenic pathways.
Chronic Intermittent Hypoxia as a Driver of Treatment Resistance
Chronic intermittent hypoxia (CIH) represents a biologically distinct form of hypoxic stress characterized by repetitive cycles of oxygen desaturation and reoxygenation, most commonly occurring during sleep in individuals with sleep-related breathing disorders. Unlike sustained tumor hypoxia, CIH generates oscillatory hypoxic signals that combine activation of hypoxia-responsive pathways with recurrent oxidative stress, leading to maladaptive cellular responses rather than stable metabolic adaptation.4,5
A growing body of experimental and translational evidence indicates that CIH promotes resistance to anticancer therapies. Intermittent stabilization of hypoxia-inducible factor-1α (HIF-1α) under CIH conditions enhances the transcription of genes involved in angiogenesis, glucose transport, cell survival, and invasion, while reoxygenation phases induce bursts of reactive oxygen species (ROS) that contribute to genomic instability and activation of DNA damage response pathways.6,7 Together, these mechanisms may paradoxically protect tumor cells from cytotoxic injury induced by chemotherapy and radiotherapy.1
Radiotherapy efficacy is highly dependent on oxygen availability, as molecular oxygen acts as a radiosensitizer by stabilizing radiation-induced DNA damage. CIH reduces effective tissue oxygenation during nocturnal periods and may impair the radiosensitizing effect of oxygen, thereby contributing to radioresistance. Preclinical studies have demonstrated that fluctuating hypoxic conditions enhance tumor cell survival following irradiation, partly through upregulation of antioxidant defenses and hypoxia-responsive survival pathways.8,9
Chemotherapy resistance has also been linked to hypoxia-induced alterations in drug transport, metabolism, and apoptotic signaling. CIH promotes the expression of multidrug resistance proteins, anti-apoptotic factors, and metabolic adaptations favoring glycolysis over mitochondrial respiration.10,11 These changes reduce susceptibility to chemotherapy-induced cell death and may be particularly relevant in tumors exposed to systemic hypoxia over prolonged periods.
Immunotherapy resistance represents another critical dimension of CIH-driven treatment failure. Hypoxic signaling enhances the expression of immune checkpoint molecules, including programmed death-ligand 1 (PD-L1), on tumor cells and tumor-associated macrophages, thereby suppressing cytotoxic T-cell and natural killer cell activity.12,13 In addition, CIH-induced inflammation and sympathetic activation impair effective antitumor immune surveillance, potentially reducing responsiveness to immune checkpoint inhibitors.14
Beyond direct effects on tumor cells, CIH exerts systemic influences that indirectly shape the tumor microenvironment. Endothelial dysfunction, vascular remodeling, and impaired perfusion further exacerbate intratumoral hypoxia, creating a feed-forward loop that reinforces therapeutic resistance.15 Collectively, these findings support the concept that CIH functions as a host-level amplifier of hypoxia-driven treatment resistance, extending the impact of hypoxia beyond the tumor itself.
Biological Effects of Restoring Physiological Normoxia
Restoration of physiological normoxia represents a potential means to counteract multiple hypoxia-driven oncogenic pathways activated under chronic intermittent hypoxia. Unlike hyperoxic interventions, which may exacerbate oxidative stress, normoxia aims to re-establish stable tissue oxygenation within physiological ranges, thereby attenuating maladaptive cellular responses without inducing redox imbalance.
One of the most immediate biological consequences of normoxia restoration is the downregulation of hypoxia-inducible factor signaling. Under normoxic conditions, HIF-1α undergoes prolyl hydroxylation and proteasomal degradation, resulting in reduced transcription of genes involved in angiogenesis, glycolysis, cell survival, and invasion.15,16 Experimental studies demonstrate that normalization of oxygen availability suppresses HIF-mediated expression of VEGF, GLUT1, and LDHA, thereby limiting angiogenic drive and metabolic reprogramming associated with tumor aggressiveness.17
Normoxia also exerts a stabilizing effect on cellular redox homeostasis. Chronic intermittent hypoxia is characterized by repeated hypoxia–reoxygenation cycles that generate bursts of reactive oxygen species18 contributing to DNA damage, genomic instability, and activation of stress-response pathways.7 By minimizing oxygen fluctuations, normoxia reduces oxidative stress burden and may limit the accumulation of mutations that favor malignant progression. In experimental models, sustained normoxic conditions are associated with decreased ROS production and improved mitochondrial function, supporting cellular metabolic stability.19
Importantly, restoration of normoxia has significant implications for antitumor immunity. Hypoxic signaling suppresses immune surveillance by impairing cytotoxic T lymphocyte and natural killer cell function while promoting immune checkpoint expression within the tumor microenvironment. In contrast, normoxic conditions favor immune effector cell activity, enhance antigen presentation, and reduce hypoxia-induced PD-L1 expression on tumor cells and tumor-associated macrophages.12,13,20 These effects suggest that normoxia may indirectly potentiate immunotherapy by restoring immune competence rather than directly targeting tumor cells.
Metabolic plasticity is another domain in which normoxia may exert protective effects. Hypoxia-driven metabolic reprogramming toward aerobic glycolysis confers survival advantages to tumor cells and contributes to treatment resistance. Restoration of physiological oxygen levels promotes oxidative phosphorylation, improves mitochondrial efficiency, and reduces reliance on glycolytic pathways.21,22 By attenuating metabolic stress and lactate accumulation, normoxia may limit tumor invasiveness and reduce selection pressure for aggressive phenotypes.
Collectively, these biological effects indicate that normoxia acts as a systemic modulator capable of counterbalancing hypoxia-driven oncogenic signaling. Rather than functioning as a direct anticancer therapy, restoration of physiological normoxia may improve the host environment in which tumors develop and are treated, thereby enhancing responsiveness to conventional anticancer modalities.
Sleep and Airway Interventions as Normoxia-Restoring Strategies
Given the central role of chronic intermittent hypoxia in driving hypoxia-dependent oncogenic pathways, interventions aimed at restoring physiological normoxia—particularly during sleep—emerge as biologically plausible adjunctive strategies in cancer care. Importantly, these approaches do not target tumor cells directly but act at the host level by stabilizing oxygenation, reducing hypoxic burden, and modulating systemic physiological stressors that influence tumor behavior.
Continuous positive airway pressure (CPAP) remains the gold standard treatment for obstructive sleep apnea and is the most effective intervention for eliminating nocturnal oxygen desaturation.23 By preventing upper airway collapse, CPAP abolishes intermittent hypoxia, reduces oxidative stress, and normalizes sympathetic activity.24,25 Experimental and clinical studies have shown that CPAP therapy attenuates HIF-1α activation, decreases systemic inflammation, and improves endothelial function, thereby mitigating several biological processes implicated in cancer progression and treatment resistance.26,27
Mandibular advancement devices (MADs) represent an alternative therapeutic option for patients with mild to moderate sleep-disordered breathing or for those intolerant to CPAP. By advancing the mandible and enlarging the upper airway, MADs improve nocturnal oxygenation and reduce hypoxic burden.28 Although their impact on cancer-related outcomes has not been directly studied, their demonstrated efficacy in reducing intermittent hypoxia suggests a potential role in modulating hypoxia-driven biological pathways.
In selected patients, otorhinolaryngologic interventions aimed at improving upper airway patency may also contribute to the restoration of physiological normoxia. Surgical or medical management of nasal obstruction, turbinate hypertrophy, septal deviation, oropharyngeal collapse, or adenotonsillar hypertrophy has been shown to reduce airflow limitation and improve nocturnal oxygenation. Although these interventions are not cancer-directed therapies, their ability to alleviate anatomical contributors to sleep-related hypoxia supports their inclusion within a multidisciplinary framework focused on hypoxia normalization.29,30
Beyond mechanical airway stabilization, functional interventions targeting orofacial and respiratory physiology may further contribute to normoxia restoration. Myofunctional therapy, speech therapy, and oropharyngeal exercises have been shown to improve tongue posture, nasal breathing, and upper airway muscle tone, leading to reductions in sleep-disordered breathing severity and nocturnal hypoxia.31,32 These approaches are particularly relevant in individuals with craniofacial growth alterations, maxillary deficiency, or ankyloglossia, where structural and functional factors converge to impair airway patency.
Respiratory and postural physiotherapy may also play a complementary role by enhancing ventilatory mechanics, thoracic mobility, and diaphragmatic function. Improved ventilation efficiency can reduce nocturnal hypoventilation and oxygen fluctuations, further contributing to stable oxygenation during sleep.33 While evidence linking these interventions directly to cancer outcomes is currently limited, their capacity to reduce systemic hypoxic stress supports their inclusion within an integrative normoxia-restoration framework.
Collectively, sleep and airway interventions represent a spectrum of non-pharmacological strategies capable of reducing chronic intermittent hypoxia and restoring physiological normoxia. When considered in the context of cancer biology, these interventions may function as modulators of the tumor–host interaction, potentially enhancing the efficacy of standard anticancer therapies by alleviating hypoxia-driven resistance mechanisms.
Clinical Implications and Future Directions
The recognition of chronic intermittent hypoxia as a modifiable contributor to cancer progression and treatment resistance carries important clinical implications. Rather than positioning normoxia restoration as a standalone anticancer therapy, the evidence reviewed here supports its potential role as an adjuvant strategy aimed at optimizing the biological context in which conventional oncologic treatments are delivered. Importantly, normoxia-restoring interventions should not be interpreted as direct anticancer therapies, but as adjunctive measures intended to optimize the physiological environment in which standard oncologic treatments are delivered.
One of the most relevant clinical implications relates to treatment responsiveness. Hypoxia is a well-established determinant of resistance to chemotherapy, radiotherapy, and immunotherapy. By reducing nocturnal hypoxic burden, interventions that restore physiological normoxia may enhance oxygen-dependent radiosensitivity, improve drug-induced cytotoxicity, and facilitate antitumor immune responses. This host-centered approach aligns with the growing emphasis on precision oncology, where modifiable systemic factors are increasingly recognized as determinants of treatment efficacy.34
From a translational perspective, sleep-related breathing disorders represent an underdiagnosed and potentially actionable source of systemic hypoxia in cancer patients.35 Routine screening for sleep-disordered breathing, particularly in individuals with head and neck, colorectal, breast, and lung cancers, could identify patients at risk of sustained nocturnal hypoxia. In such cases, implementation of airway and sleep interventions may help stabilize oxygenation and reduce hypoxia-driven signaling during critical periods of tumor growth and therapeutic exposure.36,37
The concept of hypoxic burden—rather than isolated hypoxic events—emerges as a promising biomarker for risk stratification and therapeutic monitoring.38 Metrics integrating the depth, duration, and frequency of oxygen desaturation episodes may provide a more accurate reflection of biologically relevant hypoxic stress than conventional indices such as apnea–hypopnea index alone. Incorporating hypoxic burden into oncologic assessment could facilitate personalized intervention strategies and improve outcome prediction.35
In sleep medicine, commonly used metrics of nocturnal hypoxic burden include the cumulative time spent below 90% oxygen saturation (T90) and the oxygen desaturation index (ODI), which quantify the duration and frequency of oxygen desaturation events during sleep and provide clinically meaningful measures of systemic intermittent hypoxia.
Importantly, restoration of normoxia may also influence treatment tolerance and quality of life. Improved sleep quality, reduced sympathetic activation, and enhanced cardiopulmonary function associated with effective management of sleep-related hypoxia may increase patients’ capacity to tolerate intensive anticancer therapies. These benefits, while indirect, may contribute meaningfully to overall treatment success and patient-centered outcomes.3,39
Despite these promising implications, several limitations must be acknowledged. Direct clinical evidence linking normoxia-restoring interventions to improved cancer survival remains limited, and most available data are derived from experimental models or observational studies. Prospective clinical trials specifically designed to evaluate the impact of hypoxia normalization on oncologic outcomes are needed. Such studies should incorporate objective measures of nocturnal oxygenation, treatment response, immune function, and long-term survival.
Future research should also explore optimal timing, duration, and patient selection for normoxia-restoring interventions. Given the circadian modulation of immune and metabolic pathways, targeting nocturnal hypoxia may prove particularly relevant. Multidisciplinary collaboration between oncologists, sleep specialists, pulmonologists, and dental professionals will be essential to translate this integrative framework into clinical practice.
Limitations
Several limitations of the present narrative review should be acknowledged. First, although substantial experimental and translational evidence supports the role of chronic intermittent hypoxia in cancer biology, direct clinical trials evaluating the impact of normoxia-restoring interventions on cancer outcomes remain scarce. Most available data are derived from preclinical models, observational studies, or indirect clinical associations, which limits causal inference.
Second, the assessment of physiological normoxia remains challenging. Conventional measures such as peripheral oxygen saturation do not fully capture tissue-level oxygenation or temporal hypoxic burden, particularly during sleep. Standardized and clinically accessible biomarkers capable of quantifying biologically relevant hypoxia are still under development.
Third, heterogeneity in cancer types, stages, and treatments complicates the generalization of findings. The extent to which normoxia restoration may influence tumor behavior likely varies across malignancies and patient populations. Additionally, excessive oxygen supplementation carries potential risks, underscoring the importance of distinguishing physiological normoxia from hyperoxia.
Finally, sleep-related breathing disorders are frequently underdiagnosed in oncologic populations. Without systematic screening, the contribution of nocturnal hypoxia to cancer progression and treatment resistance may be underestimated, limiting opportunities for timely intervention.
Conclusions
Hypoxia is a central driver of cancer progression, therapeutic resistance, and immune evasion. While hypoxia has traditionally been considered an intrinsic feature of the tumor microenvironment, growing evidence indicates that chronic intermittent hypoxia—particularly during sleep—represents a systemic and potentially modifiable contributor to oncogenic signaling.
This narrative review proposes that restoration of physiological normoxia, especially nocturnal normoxia, may attenuate hypoxia-driven cancer biology and enhance the efficacy of standard anticancer therapies. Rather than acting as a direct antitumor treatment, normoxia restoration should be viewed as an adjuvant strategy aimed at optimizing the host environment in which cancer develops and is treated.
Sleep and airway interventions such as continuous positive airway pressure, mandibular advancement devices, myofunctional therapy, and respiratory physiotherapy offer practical means to reduce hypoxic burden and stabilize oxygenation. Integrating these approaches into multidisciplinary cancer care pathways may represent a novel and clinically relevant avenue for improving treatment outcomes.
Future prospective studies incorporating objective measures of hypoxic burden, immune function, and treatment response are needed to validate this integrative framework. By reframing oxygenation as a dynamic, circadian-modulated determinant of cancer behavior, this work highlights normoxia restoration as a promising and underexplored dimension of precision oncology.
Data Sharing Statement
Data sharing is not applicable to this article as no data were created or analysed in this study.
Ethical Considerations
This article is a narrative review of previously published studies and does not involve human participants, patient data, or animal research. Ethical approval and informed consent were therefore not required.
Author Contributions
Carlos Mas Bermejo: Conceptualization, Investigation, Supervision, Methodology, Writing – original draft, Writing – review & editing
Carlos Mas Gomez: Data curation, Investigation, Methodology, Validation, Writing – reviewing & editing
Maria Agustina Sevilla Garcia: Supervision, Visualization, Writing – review & editing
Carlos O’Connor-Reina: Data curation, Visualization, Validation, Formal analysis, Writing – reviewing & editing
Dr. Susana Falardo: Validation, Visualization, Writing – reviewing & editing
Jose Luis Alonso-Romero: Conceptualization, Investigation, Supervision, Writing – review & editing
Luis Alberto Bravo Gonzalez: Methodology, Supervision, Validation, Writing – review & editing
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mottram CD. Ruppel’s Manual of Pulmonary Function Testing.
2. West JB. Respiratory Physiology: The Essentials.
3. Zhang L, Liu F, Li J. Obstructive sleep apnea and lung cancer: molecular underpinnings and clinical translational prospects. Front Cell Dev Biol. 2026;14:1764594.PMID: 41768993; PMCID: PMC12946056. doi:10.3389/fcell.2026.1764594
4. Prabhakar NR, Semenza GL. Oxygen sensing and homeostasis. Physiology. 2015;30(5):340–9. doi:10.1152/physiol.00022.2015
5. Ryan S, McNicholas WT, McNicholas WT. Intermittent hypoxia and activation of inflammatory molecular pathways in obstructive sleep apnea. Thorax. 2009;64(7):631–636. doi:10.1136/thx.2008.105494
6. Semenza GL. Targeting HIF-1 for cancer therapy. Nat Rev Cancer. 2003;3(10):721–732. doi:10.1038/nrc1187
7. Lavie L. Oxidative stress in obstructive sleep apnea and intermittent hypoxia—revisited. Sleep Med Rev. 2015;20:27–45. doi:10.1016/j.smrv.2014.07.003
8. Brown JM. Tumor hypoxia in cancer therapy. Methods Enzymol. 2007;435:297–321. doi:10.1016/S0076-6879(07)35015-5
9. Wouters BG, Brown JM. Cells at intermediate oxygen levels can be more important than the hypoxic fraction in determining tumor response to fractionated radiotherapy. Radiat Res. 1997;147(5):541–550. doi:10.2307/3579620
10. Rohwer N, Cramer T. Hypoxia-mediated drug resistance: novel insights on the functional interaction of HIFs and cell death pathways. Drug Resist Updat. 2011;14(3):191–201. doi:10.1016/j.drup.2011.03.001
11. Wilson WR, Hay MP. Targeting hypoxia in cancer therapy. Nat Rev Cancer. 2011;11(6):393–410. doi:10.1038/nrc3064
12. Huang MH, Zhang XB, Wang HL, et al. Intermittent hypoxia enhances tumor programmed death ligand 1 expression in a mouse model of sleep apnea. Ann Transl Med. 2019;7(5):97. doi:10.21037/atm.2019.01.44
13. Cui Z, Ruan Z, Li M, et al. Intermittent hypoxia inhibits anti-tumor immune response via regulating PD-L1 expression in lung cancer cells and tumor-associated macrophages. Int Immunopharmacol. 2023;122:110652. doi:10.1016/j.intimp.2023.110652
14. Noman MZ, Hasmim M, Lequeux A, et al. Improving cancer immunotherapy by targeting hypoxia. Cancer Res. 2014;74(21):665–671. doi:10.1158/0008-5472.CAN-13-3045
15. Jain RK. Normalization of tumor vasculature: an emerging concept in antiangiogenic therapy. Science. 2005;307(5706):58–62. doi:10.1126/science.1104819
16. Semenza GL. Hypoxia-inducible factors in physiology and medicine. Cell. 2012;148(3):399–408. doi:10.1016/j.cell.2012.01.021
17. Rankin EB, Giaccia AJ. Hypoxic control of metastasis. Science. 2016;352(6282):175–180. doi:10.1126/science.aaf4405
18. Lavalle S, Masiello E, Iannella G, et al. Unraveling the complexities of oxidative stress and inflammation biomarkers in obstructive sleep apnea syndrome: a comprehensive review. Life. 2024;14:425. doi:10.3390/life14040425
19. Chandel NS. Mitochondria and cancer. Cancer Metab. 2014;2:8. doi:10.1186/2049-3002-2-8
20. Barsoum IB, Smallwood CA, Siemens DR, Graham CH. A mechanism of hypoxia-mediated escape from adaptive immunity in cancer cells. Cancer Immunol Res. 2014;2(4):362–371. doi:10.1158/2326-6066.CIR-13-0225
21. Almendros I, Montserrat JM, Torres M, et al. Intermittent hypoxia increases melanoma metastatic growth in a mouse model of sleep apnea. Eur Respir J. 2012;39(1):215–217. doi:10.1183/09031936.00104411
22. Pavlova NN, Thompson CB. The emerging hallmarks of cancer metabolism. Cell Metab. 2016;23(1):27–47. doi:10.1016/j.cmet.2015.12.006
23. Srivali N, De Giacomi F. Does CPAP increase or protect against cancer risk in OSA: a systematic review and meta-analysis. Sleep Breath. 2025;29(2):175.PMID: 40310575. doi:10.1007/s11325-025-03345-9
24. Marín JM, Carrizo SJ, Vicente E, Agustí AG. Long-term cardiovascular outcomes in men with obstructive sleep apnea–hypopnea with or without treatment with CPAP. Lancet. 2005;365(9464):1046–1053. doi:10.1016/S0140-6736(05)71141-7
25. McNicholas WT, Bonsignore MR. Sleep apnea as an independent risk factor for cardiovascular disease. Eur Respir J. 2007;29(1):156–178. doi:10.1183/09031936.00027406
26. Ryan S, Taylor CT, McNicholas WT. Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation. 2005;112(17):2660–2667. doi:10.1161/CIRCULATIONAHA.105.556746
27. Campos-Rodriguez F, Martinez-Garcia MA, Martinez M, et al. Association between obstructive sleep apnea and cancer incidence in a large multicenter clinical cohort. Am J Respir Crit Care Med. 2013;187(1):99–105. doi:10.1164/rccm.201209-1671OC
28. Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy. J Clin Sleep Med. 2015;11(7):773–827. doi:10.5664/jcsm.4858
29. Caples SM, Rowley JA, Prinsell JR, et al. Surgical modifications of the upper airway for obstructive sleep apnea in adults: a systematic review and meta-analysis. Sleep. 2010;33(10):1396–1407. doi:10.1093/sleep/33.10.1396
30. Weaver EM, Kapur VK. Surgical treatment of obstructive sleep apnea. Otolaryngol Clin North Am. 2007;40(4):745–768. doi:10.1016/j.otc.2007.03.003
31. Camacho M, Certal V, Abdullatif J, et al. Myofunctional therapy to treat obstructive sleep apnea: a systematic review and meta-analysis. Sleep. 2015;38(5):669–675. doi:10.5665/sleep.4652
32. Guimarães KC, Drager LF, Genta PR, Marcondes BF, Lorenzi-Filho G. Effects of oropharyngeal exercises on patients with moderate obstructive sleep apnea syndrome. Am J Respir Crit Care Med. 2009;179(10):962–966. doi:10.1164/rccm.200806-981OC
33. Courtney R, Noël E, Lieutaud A, d’Alessio P. Breathing retraining and respiratory efficiency. J Bodyw Mov Ther. 2009;13(3):239–248. doi:10.1016/j.jbmt.2008.03.003
34. Horsman MR, Overgaard J, Mayer IA, Sanders ME, Gianni L. The impact of hypoxia on radiotherapy of tumors. Nat Rev Clin Oncol. 2016;13(11):674–687. doi:10.1038/nrclinonc.2016.66
35. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173–178. doi:10.1513/pats.200708-119MG
36. Martinez-Garcia MA, Campos-Rodriguez F, Barbé F. Cancer and obstructive sleep apnea: implications for pathogenesis and treatment. Am J Respir Crit Care Med. 2014;190(9):1029–1036.
37. Azarbarzin A, Sands SA, Stone KL, et al. The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: the osteoporotic fractures in men study and the sleep heart health study. Eur Heart J. 2019;40(14):1149–1157.PMID: 30376054; PMCID: PMC6451769. doi:10.1093/eurheartj/ehy624
38. Campos-Rodriguez F, Martinez-Garcia MA, Barbé F. Obstructive sleep apnea and cancer: epidemiologic and mechanistic insights. Am J Respir Crit Care Med 2023. 207(1):20–31. doi:10.1164/rccm.202204-0725PP
39. Ferreira PM, Carvalho I, Redondo M, van Zeller M, Drummond M. The role of obstructive sleep apnea and nocturnal hypoxia as predictors of mortality in cancer patients. Sleep Med. 2024;121:258–265.PMID: 39029304. doi:10.1016/j.sleep.2024.07.017
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hypoxia Effects in Intervertebral Disc-Derived Stem Cells and Discus Secretomes: An in vitro Study
Romaniyanto, Mahyudin F, Prakoeswa CRS, Notobroto HB, Tinduh D, Ausrin R, Rantam FA, Suroto H, Utomo DN, Rhatomy S
Stem Cells and Cloning: Advances and Applications 2022, 15:21-28
Published Date: 27 May 2022