")
Back to Journals » International Journal of General Medicine » Volume 14
Resting Dead Space Fraction as Related to Clinical Characteristics, Lung Function, and Gas Exchange in Male Patients with Chronic Obstructive Pulmonary Disease
Authors Chuang ML , Hsieh BYT , Lin IF
Received 11 November 2020
Accepted for publication 30 December 2020
Published 3 February 2021 Volume 2021:14 Pages 169—177
DOI https://doi.org/10.2147/IJGM.S291555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ming-Lung Chuang,1,2 Benjamin Yung-Thing Hsieh,3 I-Feng Lin4
1Division of Pulmonary Medicine and Department of Internal Medicine, Chung Shan Medical University Hospital, Taichung, Taiwan, 40201, Republic of China; 2School of Medicine, Chung Shan Medical University, Taichung, Taiwan, 40201, Republic of China; 3School of Medicine, National Yang Ming University, Taipei, Taiwan, 11221, Republic of China; 4Institute of Public Health, National Yang Ming University, Taipei, Taiwan, 11221, Republic of China
Correspondence: Ming-Lung Chuang
Division of Pulmonary Medicine and Department of Internal Medicine, Chung Shan Medical University Hospital, #110, Section 1, Chien-Kuo North Road, South District, Taichung, 40201, Taiwan, Republic of China
Tel +886-4-2473-9595 ext. 34718
Email [email protected]
I-Feng Lin
Institute of Public Health, National Yang Ming University, 155, Sec 2, LihNong Street, ShiPai, Taipei, Taiwan, 11221, Republic of China
Email [email protected]
Background: Measures of forced expired volume in one second % predicted (FEV1%), residual volume to total lung capacity ratio (RV/TLC) and diffusing capacity for carbon monoxide measurements (DLCO) are the standard lung function test for evaluating patients with chronic obstructive pulmonary disease (COPD). The dead space fraction (VD/VT) has been shown to be a robust marker of gas exchange abnormality. However, the use of VD/VT has gradually become less common. As VD/VT measured at rest (VD/VTR) has been successfully used in non-COPD conditions, it was hypothesized that in COPD the VD/VTR was more sensitive than the standard lung function test in correlation with clinical characteristics and gas exchange. This study aimed to test the hypothesis and to identify the variables relevant to VD/VTR.
Methods: A total of 46 male subjects with COPD were enrolled. Clinical characteristics included demographic data, oxygen-cost diagram (OCD), and image studies for pulmonary hypertension. The standard lung function was obtained. To calculate VD/VT, invasive arterial blood gas and pulmonary gas exchange (PGX) were measured. The variables relevant to VD/VTR were analyzed by multiple linear regression.
Results: Compared to lung function, VD/VTR was more frequently and significantly related to smoking, carboxyhemoglobin level, pulmonary hypertension and PaCO2 (all p < 0.05) whereas FEV1% was more related to lung function test, PaO2 and OCD score. VD/VTR and FEV1% were highly related to resting gas exchange but RV/TLC and DLCO% were not. Cigarette consumption, the equivalent for CO2 output, arterial oxyhemoglobin saturation, and the product of tidal volume and inspiratory duty cycle were identified as the parameters relevant to VD/VTR with a power of 0.72.
Conclusion: Compared to lung function test, VD/VTR is more related to clinical characteristics and is a comprehensive marker of resting gas exchange. Further studies are warranted to provide a noninvasive measurement of VD/VTR.
Registration Number: MOST 106– 2314-B-040-025 and CSH-2019-C-30.
Keywords: obstructive airway disease, residual volume and total lung capacity ratio, diffusing capacity of lung, dead space and tidal volume ratio, cigarette consumption, carboxyhemoglobin, pulmonary hypertension
Background
The severity of chronic obstructive pulmonary disease (COPD) is usually graded by forced expired volume in one second % predicted (FEV1%).1 Despite mMRC and acute exacerbation being related to the risk assessment of COPD, the power of correlations of FEV1% with the clinical outcomes is not robust,2–4 and lung volume such as the residual volume to total lung capacity ratio (RV/TLC) and diffusing capacity measurements (DLCO) provide additional information.5–8
The dead space to tidal volume ratio at rest or at peak exercise or change during exercise (VD/VTR, -P, and -C) indicating the severity of ventilation/perfusion (V/Q) mismatch9 can serve as a marker of physiological change in patients with COPD in a various clinical conditions.8,10–15 However, exercise testing is labor consuming and costly and in diseases other than COPD, the VD/VT has been successfully used in non-exercise conditions.16–20
It was hypothesized that the VD/VTR was more significant than the standard lung function test in correlation with clinical characteristics and gas exchange (ie, all variables relevant to oxygen and CO2 tensions and their differences in arterial blood and alveoli) in patients with COPD. This study aimed to test the hypothesis by correlation analysis and to identify variables of demographics, symptom scores, images for pulmonary hypertension, lung function, and gas exchange relevant to VD/VTR by multiple regression analysis.
Methods
Study Design
In this observational cross-sectional study, we measured demographic characteristics, cigarette smoking history, functional activity and pulmonary hypertension determined by image studies, and lung function in subjects with COPD at a university teaching hospital. Resting pulmonary gas exchange (PGX) and arterial blood gas (ABG) were measured simultaneously. The local Institutional Review Board of Chung Shan Medical University Hospital (CS16174) approved this study. This study was conducted in compliance with the Declaration of Helsinki.
Subjects
Subjects aged ≥40 years with COPD were enrolled. Anthropometric measurements, cigarette consumption, and functional activity were recorded. Male adult subjects who underwent lung function testing were enrolled if their forced expired volume in one second (FEV1)/forced vital capacity (FVC) was <0.7.1 The diagnosis of COPD was made according to the Global Initiative for Chronic Lung Disease (GOLD) criteria.1 As few female subjects met the criteria of COPD in Taiwan (4%),2 for simplicity they were not included in this study. Subjects with a body mass index ≤18 kg·m−2 or ≥32 kg·m−2, any other chronic diseases including uncontrolled diabetes mellitus, uncontrolled hypertension, anemia (hemoglobin <13 g·dL−1 in males), or with laboratory findings of cardiovascular, hematological, metabolic or neuromuscular diseases or acute illnesses in the recent 1 month were not enrolled. Uncontrolled hypertension means having hypertension but no or inadequate treatment so that the blood pressure remained high (ie, >140/90 mm Hg).21 Signed informed consent was obtained from each participant. Some of the participants were enrolled in other studies.22,23
Measurements
Demographic Data and Functional Activity
Age, height, weight, body mass index, triceps skinfold, mid-arm circumference, and cigarette consumption were recorded. The oxygen cost diagram (OCD) was used to evaluate the participants’ functional activity. The OCD a 100-mm long vertical line with everyday activities listed alongside the line, above which breathlessness limited the participants. The distance from zero was measured and scored.
Image Study
Chest radiography was obtained within one month of enrolling in the study. The hila thoracic ratio (HTR), cardiac thoracic ratio, and the diameter of anterior descending pulmonary artery (ADPA) on the standing posterior-anterior chest radiograph were measured as these variables were reported to represent pulmonary hypertension.24 The chest radiographs were evaluated by an experienced pulmonologist without knowing the clinical information and the average values were recorded for analysis.
Two-dimensional echocardiography was performed by an experienced cardiologist who was unaware of the clinical data and lung function. Parasternal, apical, and subcostal studies were conducted.25,26
Pulmonary Function Testing
Pre-test preparation was followed the standard guide and bronchodilators were not administered within 3 h for short-acting beta-agonists and 12 h for long-acting beta-agonists before the tests.27–29 FEV1, FVC, TLC, RV, and DLCO were measured using spirometry, body plethysmography, and the single-breath technique (MasterScreenTM Body; Carefusion, Wuerzburg, Germany), respectively, in accordance with the currently recommended standards by ATS/ERS task force.30,31 The best of three technically satisfactory readings was used.30,32,33 All of the spirometry data were obtained before and after inhaling a standard dose of fenoterol HCl. Post-dose measurements were performed 15 minutes after inhalation. Static lung volume data and DLCO data were obtained before inhaling fenoterol.
Maximum inspiratory pressure at the mouth indicating inspiratory muscle strength and maximum expiratory pressure indicating expiratory muscle strength at the mouth were measured.34
Pulmonary Gas Exchange and VD/VT Measurement
Each subject completed PGX measured at a 2-min complete rest. VO2 (mL/min), CO2 output (VCO2) (mL/min), and minute ventilation (VE) were continuously measured and the data at the last 15 seconds were averaged and reported (MasterScreen CPX™, Carefusion, Wuerzburg, Germany). The physiological VD/VT was measured (VD/VT) using a standard formula as follows:35

where PaCO2 was arterial PCO2 and  and PB was barometric pressure measured daily and VDm was the dead space of mouth piece and pneumotachograph as the manufacture reported.36 Artery blood samples were drawn at the brachial artery and heparinized at rest. The sample was immediately placed on ice and then analyzed for pH, PCO2, and PO2 with body temperature correction (model 278, CIBA-Corning, Medfield, MA, USA).
and PB was barometric pressure measured daily and VDm was the dead space of mouth piece and pneumotachograph as the manufacture reported.36 Artery blood samples were drawn at the brachial artery and heparinized at rest. The sample was immediately placed on ice and then analyzed for pH, PCO2, and PO2 with body temperature correction (model 278, CIBA-Corning, Medfield, MA, USA).
Statistical Analysis
Data were summarized as mean ± standard deviation. Pearson’s or Spearman correlation coefficients were used when appropriate for quantifying the pair-wise relationships among the variables of interest. Multiple linear regression analysis was used to select important parameters of VD/VTR. All possible regression algorithms were performed using the candidate variables with p values < 0.35 in univariate analysis. The Student’s t-test was used for comparisons between two groups. The chi-square test or Fisher exact test was used to compare the proportions between the two groups. All statistical analyses were performed using SAS statistical software (SAS Institute Inc., Cary, NC, USA). Statistical significance was set at p < 0.05. Marginal significance was set at 0.05 ≤ p ≤ 0.1.
Results
Fifty-seven patients were enrolled, of whom 10 were excluded because two subjects did not meet the inclusion criteria and another two met the exclusion criteria and six subjects declined to participate (Figure 1). The remaining 46 male subjects with COPD were enrolled after excluding one subject whose arterial blood gas analysis was not obtained (mean age 65.2 ± 5.8 years) (Tables 1–3). In Tables 1–3, some data were missing in one to six subjects because of technical failure or no measurements. Most of the patients had GOLD stages II and III, hyperinflation of lung and static air trapping, high VD/VTR, and impaired diffusing capacity, inspiratory muscle strength and peak flow, and hyperventilation with normoxemia and normocapnia.
 |
Table 1 Demographic Data, Symptom Score, Blood Tests, Chest Radiography, and Echocardiography (n = 46) |
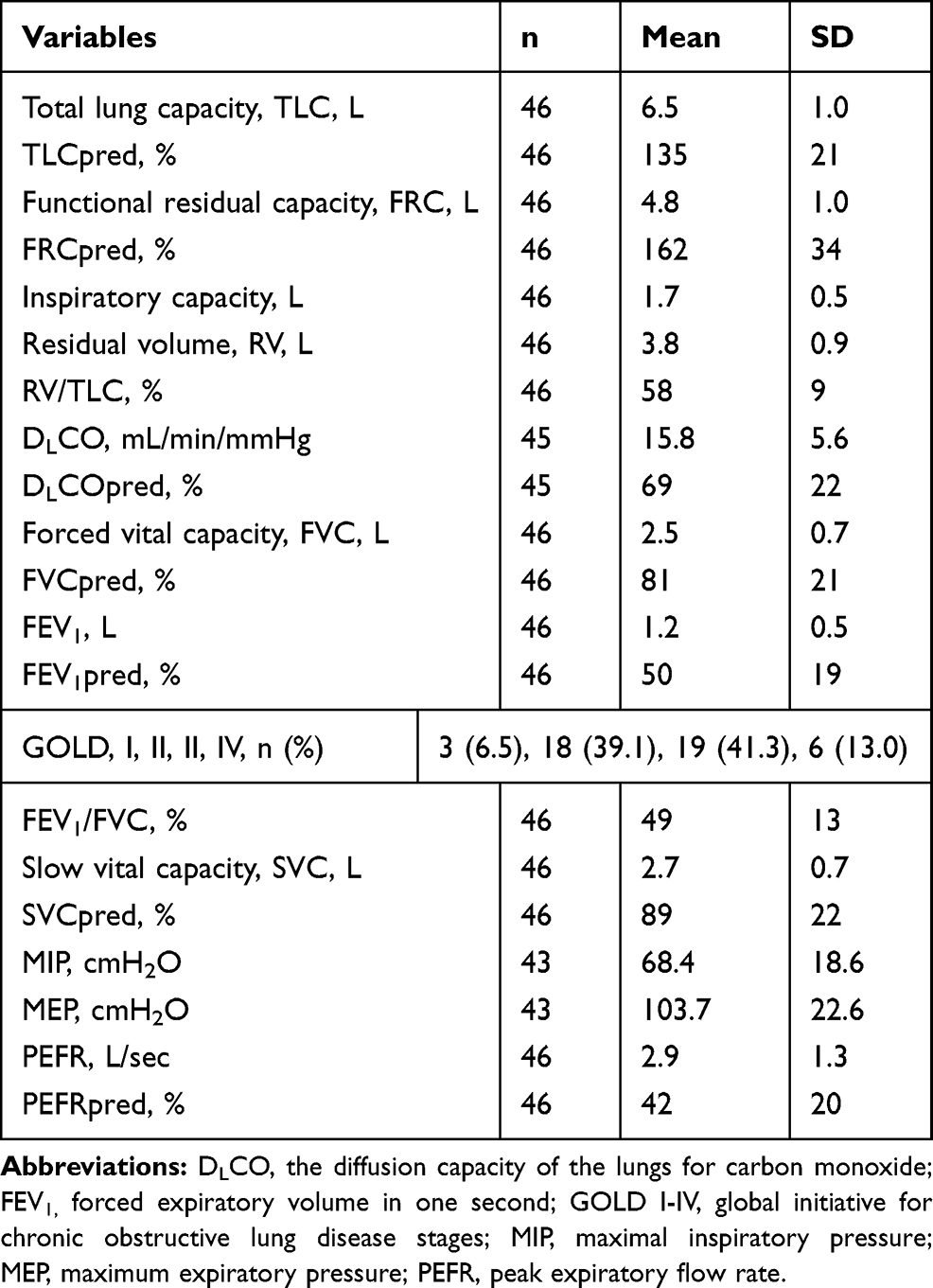 |
Table 2 Lung Function |
 |
Table 3 Cardiopulmonary Physiological Data, Arterial Blood Gases, Carboxyhemoglobin and Plasma Lactate Concentrations at Rest |
 |
Figure 1 Flow diagram. A total of 57 subjects with chronic obstructive pulmonary disease were screened. After excluding 10 subjects, the remaining 46 were retained for analysis after further excluding another one subject whose arterial blood gas data was not obtained. |
Compared to the standard lung function test, VD/VTR was more frequently (Table 4, p <0.0001) and significantly related to cigarette consumption, carboxyhemoglobin level, and pulmonary hypertension (all p <0.05) and these associated factors were not related to FEV1%, RV/TLC, and DLCO% (all p = NS). In contrast, FEV1% and RV/TLC were more related to lung function as expected and DLCO% was singly and mildly related to RV/TLC. VD/VTR and FEV1% were correlated with the resting gas exchange whereas RV/TLC and DLCO% were not.
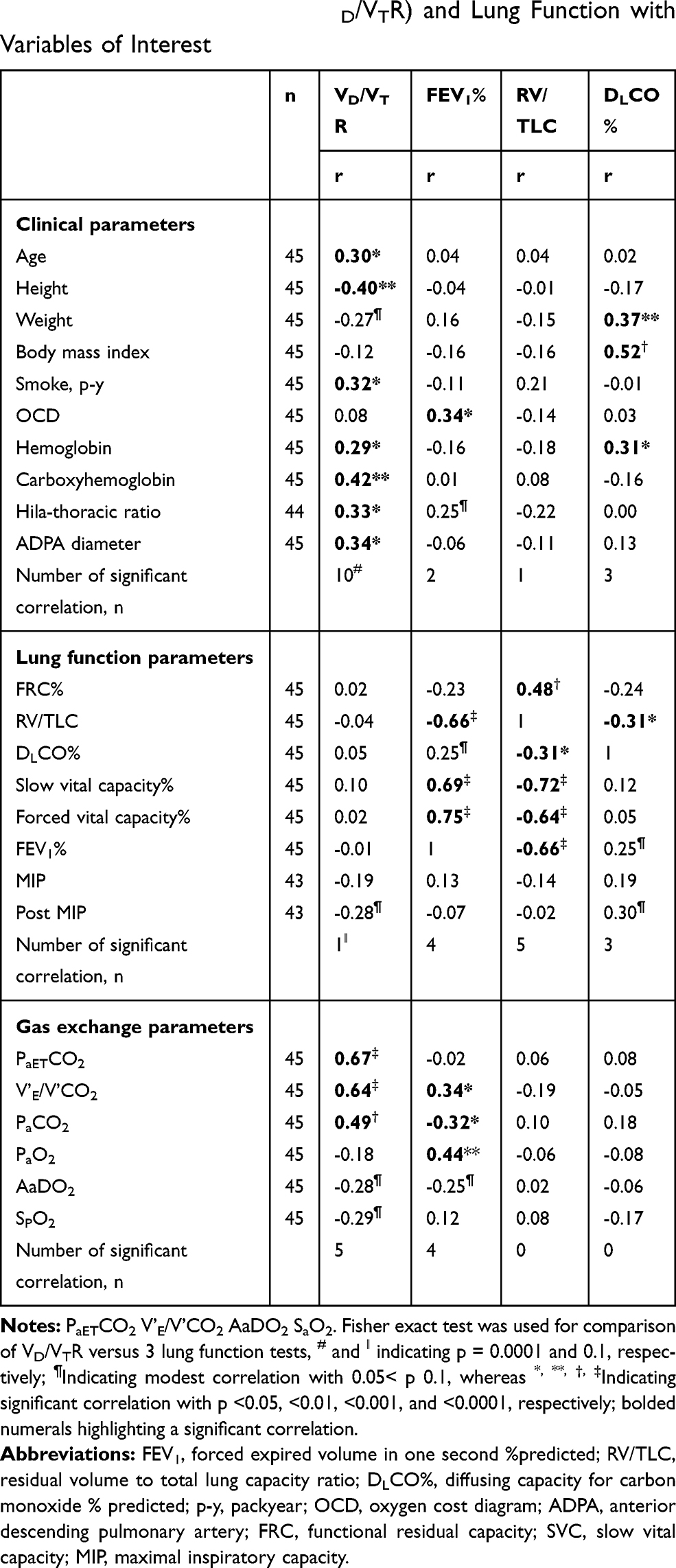 |
Table 4 Comparison of Correlation Coefficient (r) Between Resting Dead Space Fraction (VD/VTR) and Lung Function with Variables of Interest |
Multiple linear regression analysis revealed that cigarette consumption and HTR were positively related to VD/VTR whereas the height was negatively related to VD/VTR (Table 5). When PGX data were added in analysis, the HTR and height were replaced by VE/VCO2, the product of VT and inspiratory duty cycle (VTIDC), and SPO2 where VE/VCO2 was positively related to VD/VTR whereas VTIDC and SPO2 were negatively related to VD/VTR. Cigarette consumption and the three PGX variables were highly related to VD/VTR with a power of 0.72.
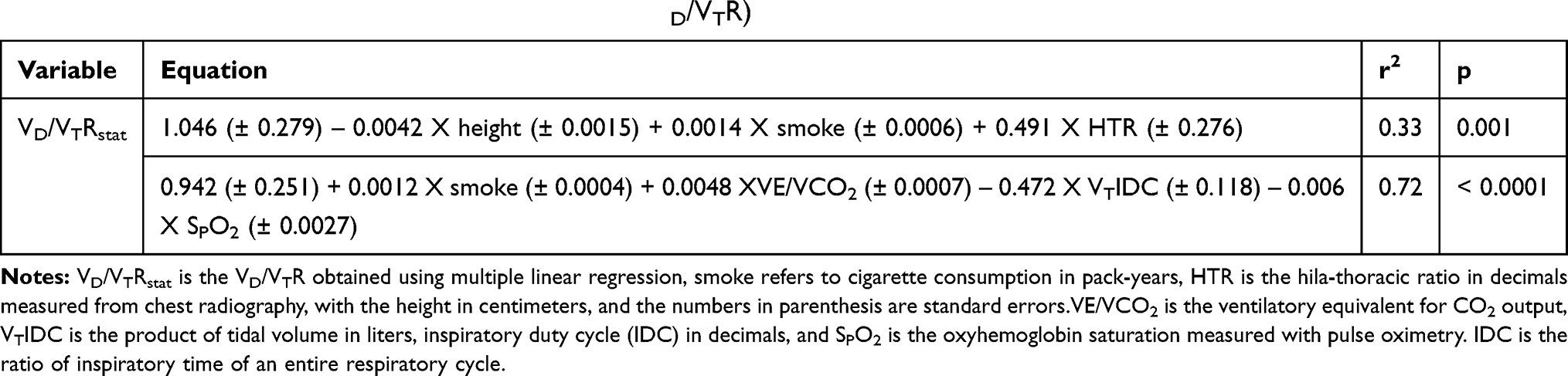 |
Table 5 Risk Factors of Dead Space Fraction at Rest (VD/VTR) |
Discussion
In this study, compared to FEV1%, RV/TLC, and DLCO%, VD/VTR was a unique marker for male patients with COPD (Table 4). VD/VTR was related to cigarette consumption, carboxyhemoglobin, and pulmonary hypertension, whereas the standard lung function was not. Using statistical technique for evaluation of VD/VTR, cigarette consumption, VE/VCO2, VTIDC and SPO2 were the four contributors (Table 5, r2 = 0.72).
Regarding lung function, DLCO%, KCO, and VA/TLC have been related to VD/VTR and VD/VTP in the literature (r = –0.20-–0.60, p < 0.05 - <0.01) where KCO is DLCO divided by alveolar volume (VA).7 The VA and VA/TLC were related to lung volumes and airway obstruction, respectively (all p < 0.05 - <0.01),7 suggesting that DLCO, KCO, and VA are related to poor communication of airways “that would be indicative of high ventilation-perfusion areas (~alveolar dead space)”.7 Hence, it was expected that RV/TLC was related to VD/VTR and thus measuring VD/VTR is redundant. However, in this study, VD/VTR was not correlated with the lung function variables suggesting that VD/VT and lung hyperinflation, air trapping or diffusing capability might be different components in physiology.22 VD/VTR was correlated with cigarette consumption, carboxyhemoglobin, and pulmonary hypertension measured by chest radiography (Table 4). Thus, VD/VTR may offer additional information to lung function test, whereas FEV1%, RV/TLC, and DLCO% were more related to lung function test (Table 4).
Tobacco smoking is the key preventable risk factor for the development of COPD and the pathogenesis of emphysema. The duration of cigarette consumption associated with the development of COPD is considered to be ≥20 pack-years.1,37 Emphysema with a tissue-to-airway progression pattern37 was related to an increased VD/VT.15 Although cigarette consumption is thought to contribute to an increased VD/VT as found in this study, their relationship may not be necessary through the mechanism of emphysema. This was noted that RV/TLC was not related to VD/VTR in this study. Further studies are warranted to elucidate the relationship between cigarette consumption, emphysema, and VD/VT. Furthermore, carboxyhemoglobin level is modestly related to cigarette smoking (r = 0.28, p = 0.06) and was mildly correlated with VD/VTR (r = 0.35, p = 0.02) in the current study. It was consistent with a previous report that carboxyhemoglobin was positively correlated with VE/VCO2 and rapid breathing and inversely with VO2max% and expandable volume excursion.38 Of note, carboxyhemoglobin level and VD/VTR were not in a cause–effect relationship and that carboxyhemoglobin was not correlated with DLCO% in the current study does not exclude that carboxyhemoglobin can affect DLCO in normal subjects. The findings indicate that the lung pathology of COPD plays a more important role than carboxyhemoglobin in relation to DLCO.
Regarding chest radiography, a HTR ≥0.36 and diameter of the right ADPA ≥1.8 cm have been reported to be markers of pulmonary hypertension in COPD.24 COPD is usually complicated with pulmonary hypertension in the later stages. Although there was discordance between radiographic and hemodynamic measures of pulmonary arterial pressure, HTR and diameter of the right ADPA were modestly correlated with increased VD/VTR in this study (Table 4, r = 0.33 and 0.34, both p <0.05).
In normal subjects, age and height have been positively related to VD/VTR whereas weight has been negatively related to VD/VTR, and VD/VTR has been reported to be smaller in females.39 However, in this study, in subjects with COPD, height was negatively related to VD/VTR. The reason for this discrepancy is not clear, but it is probably due to the high correlation between height and weight in this study in an analysis a posteriori (r = 0.51, p = 0.0003). A higher weight is probably beneficial against the development of emphysema and stage 4 disease of COPD40 and thus negatively related to VD/VT (Table 4, r = –0.27, p = 0.08), while sarcopenia or low lean body mass may predispose to the development of emphysema (multi-organ loss of tissue, MOLT phenotype).41 Another possible reason is that the lung pathology of COPD outweighs the contribution of height to VD/VTR as normal subjects do.
VE/VCO2 has been reported to be strongly related to VD/VT when the data involve healthy subjects and those with COPD at rest and during submaximal exercise.7 This is attributed to the Bohr-Enghoff equation in which VE/VCO2 and VD/VT are mathematically related at a given level of PaCO2. A high VE/VCO2 and high Pa–ETCO2 explain 40–50% of high VD/VTR in this study (Table 4, r = 0.64 and 0.67, both p < 0.0001) compatible with that Lewis et al and Liu et al reported that VD/VT and Pa-ETCO2 were highly correlated (r = 0.76–0.88, p < 0.001).42,43 Compared to FEV1% in this study, VD/VTR was more related to PaCO2 at rest (r2 = 0.24 versus 0.10) whereas FEV1% was more related to PaO2 and OCD.
Despite A-aDO2 and SPO2 being marginally correlated with VD/VT (Table 4, r = −0.28 to −0.29, both p = 0.06), SPO2 was selected in multiple regression analysis. However, in COPD even in subjects with mild severity A-aDO2 was positively related to VD/VT.10 The discrepancy between these two studies in the VD/VTR versus A-aDO2 relationship might be due to poor correlation of VD/VTR with PaO2 where A-aDO2 was highly negatively related to PaO2 in this study (r = −0.66, p < 0.0001).
VTIDC probably represents expandable tidal volume excursion in a timely manner. When both VT and IDC are large, the mean inspiratory flow (VT/inspiratory time) can be favorably generated by the force of the inspiratory muscles. On the other hand, when VT is large and IDC is small, the mean inspiratory flow is extremely high and would be not biologically plausible. VTIDC is a variable firstly reported in the literature and its importance needs to be confirmed.
Study Limitations
The number of cases in this study was small; however, it may be inevitable for an invasive study. The small number of cases may have caused insufficient power when performing correlation coefficient analysis on VD/VTR. However, the sample size of 46 achieved a power of 80% to detect a difference between a correlation of 0.4 and the null (no correlation) using a two-sided test with a significance level of 0.05.23 As the power is related to type II error, nonsignificant test results should be interpreted more conservatively. All of the participants in this study were male, so using the results applied to females should be cautious. To investigate the relationship between two or more variables, it is usually to adjust known factors that influence the dependent variables. We used % predicted of lung function variables instead of using the absolute measured values because lung function variables are obviously influenced by anthropometrics. In this context, the unwanted influences by anthropometrics were avoided and highlight the important factors. This issue has been strongly recommended in a previous report that TLC, FRC, IC, IRV, ERV, RV, FVC, SVC, and FEV1 in liters and DLCO in mL/min/mmHg were omitted from correlation analysis.27 As transcutaneous PCO2 (PtcCO2) is a noninvasive measurement, it warrants further study to compare the study with that using PtcCO2.7,44 Although using radioisotopes or applying the multiple inert gas elimination technique (MIGET) is the standard of measuring V/Q mismatch, these techniques are costly and the latter is not common in clinical practice whereas VD/VT measurement is practical and high VD/VT is consistent with high V/Q mismatch.9
Clinical Implication
Compared to lung function test, VD/VTR was more related to cigarette consumption and pulmonary hypertension and was a comprehensive variable of resting PGX. Whether or not it can serve as a prognosticator or can be applied in smoking cessation strategy warrants further studies.
Conclusion
Compared to FEV1%, RV/TLC, and DLCO%, VD/VTR is more related to smoking, carboxyhemoglobin, pulmonary hypertension, and PaCO2 whereas FEV1% is more related to PaO2 and oxygen-cost diagram score and thus should be considered when evaluating patients with COPD. Further studies are warranted to provide a noninvasive measurement of VD/VTR.
Author Contributions
MLC: initiated and designed the study, analyzed and interpreted the data, wrote and revised the manuscript, and approved the version to be published in Inter J Gen Med. and take responsibility and is accountable for the contents of the article. BYTH: analyzed and interpreted the data, critically reviewed the manuscript and approved the version to be published in Inter J Gen Med. and take responsibility and is accountable for the contents of the article. IFL: analyzed and interpreted the data and revised and critically reviewed the manuscript and approved the version to be published in Inter J Gen Med. and take responsibility and is accountable for the contents of the article.
Funding
Chung Shan Medical University Hospital (CS16174).
Disclosure
The authors declare that there are no competing interests.
References
1. GOLD Committees. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. disclosure forms for GOLD Committees are posted on the GOLD Website, www.goldcopd.org. 2020
2. Huang TH, Hsiue TR, Lin SH, Liao XM, Su PL, Chen CZ. Comparison of different staging methods for COPD in predicting outcomes. Eur Respir J. 2018;51(3):
3. Jones PW. Health status measurement in chronic obstructive pulmonary disease. Thorax. 2001;56(11):880–887. doi:10.1136/thorax.56.11.880
4. Oga T, Nishimura K, Tsukino M, Sato S, Hajiro T. Analysis of the factors related to mortality in chronic obstructive pulmonary disease: role of exercise capacity and health status. Am J Respir Crit Care Med. 2003;167(4):544–549. doi:10.1164/rccm.200206-583OC
5. Casanova C, Cote C, de Torres JP, et al. Inspiratory-to-total lung capacity ratio predicts mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(6):591–597. doi:10.1164/rccm.200407-867OC
6. Martinez FJ, Foster G, Curtis JL, et al. Predictors of mortality in patients with emphysema and severe airflow obstruction. Am J Respir Crit Care Med. 2006;173(12):1326–1334. doi:10.1164/rccm.200510-1677OC
7. Mahut B, Chevalier-Bidaud B, Plantier L, et al. Diffusing capacity for carbon monoxide is linked to ventilatory demand in patients with chronic obstructive pulmonary disease. COPD. 2012;9(1):16–21. doi:10.3109/15412555.2011.630700
8. Sue DY, Oren A, Hansen JE, Wasserman K. Diffusing capacity for carbon monoxide as a predictor of gas exchange during exercise. N Engl J Med. 1987;316(21):1301–1306. doi:10.1056/NEJM198705213162103
9. Wasserman K, Hansen JE, Sue DY, Stringer WW, Whipp BJ. Physiology of exercise. In: Wasserman K, editor. Principles of Exercise Testing and Interpretation. Philadelphia: Lippicott Williams & Wilkins; 2005:10–65.
10. Elbehairy AF, Ciavaglia CE, Webb KA, et al. Pulmonary gas exchange abnormalities in mild chronic obstructive pulmonary disease. implications for dyspnea and exercise intolerance. Am J Respir Crit Care Med. 2015;191(12):1384–1394. doi:10.1164/rccm.201501-0157OC
11. Benditt JO, Lewis S, Wood DE, Klima L, Albert RK. Lung volume reduction surgery improves maximal O2 consumption, maximal minute ventilation, O2 pulse, and dead space-to-tidal volume ratio during leg cycle ergometry. Am J Respir Crit Care Med. 1997;156(2 Pt 1):561–566. doi:10.1164/ajrccm.156.2.9611032
12. Elbehairy AF, Webb KA, Laveneziana P, et al. Acute bronchodilator therapy does not reduce wasted ventilation during exercise in COPD. Respir Physiol Neurobiol. 2018;252–253:64–71. doi:10.1016/j.resp.2018.03.012
13. Rocha A, Arbex FF, Sperandio PA, et al. Excess ventilation in chronic obstructive pulmonary disease-heart failure overlap. implications for dyspnea and exercise intolerance. Am J Respir Crit Care Med. 2018;196(10):1264–1274. doi:10.1164/rccm.201704-0675OC
14. Wasserman K, Hansen JE, Sue DY, Casaburi R, Whipp BJ. Measurements during integrative cardiopulmonary exercise testing. In: Wasserman K, editor. Principles of Exercise Testing and Interpretation. Philadelphia: Lea & Febiger; 1994:53–78.
15. Yamasawa W, Tasaka S, Betsuyaku T, Yamaguchi K. Correlation of a decline in aerobic capacity with development of emphysema in patients with chronic obstructive pulmonary disease: a prospective observational study. PLoS One. 2015;10(4):e0125053. doi:10.1371/journal.pone.0125053
16. Beitler JR, Thompson BT, Matthay MA, et al. Estimating dead-space fraction for secondary analyses of acute respiratory distress syndrome clinical trials. Crit Care Med. 2015;43(5):1026–1035. doi:10.1097/CCM.0000000000000921
17. González-Castro A, Suárez-Lopez V, Gómez-Marcos V, et al. Utility of the dead space fraction (Vd/Vt) as a predictor of extubation success. Med Intensiva. 2011;35(9):529–538. doi:10.1016/j.medin.2011.05.016
18. Meyer K, Görnandt L, Schwaibold M, et al. Predictors of response to exercise training in severe chronic congestive heart failure. Am J Cardiol. 1997;80(1):56–60. doi:10.1016/S0002-9149(97)00283-X
19. Rodger MA, Bredeson CN, Jones G, et al. The bedside investigation of pulmonary embolism diagnosis study: a double-blind randomized controlled trial comparing combinations of 3 bedside tests vs ventilation-perfusion scan for the initial investigation of suspected pulmonary embolism. Arch Intern Med. 2006;166(2):181–187. doi:10.1001/archinte.166.2.181
20. Sinha P, Calfee CS, Beitler JR, et al. Physiologic analysis and clinical performance of the ventilatory ratio in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2019;199(3):333–341. doi:10.1164/rccm.201804-0692OC
21. Gebremichael GB, Berhe KK, Zemichael TM. Uncontrolled hypertension and associated factors among adult hypertensive patients in Ayder comprehensive specialized hospital, Tigray, Ethiopia, 2018. BMC Cardiovasc Disord. 2019;19(1):121. doi:10.1186/s12872-019-1091-6
22. Chuang ML. Combining dynamic hyperinflation with dead space volume during maximal exercise in patients with chronic obstructive pulmonary disease. J Clin Med. 2020;9(10):1127. doi:10.3390/jcm9041127
23. Chuang ML. Mechanisms affecting exercise ventilatory inefficiency-airflow obstruction relationship in male patients with chronic obstructive pulmonary disease. Respir Res. 2020;21(1):206. doi:10.1186/s12931-020-01463-4
24. Chetty KG, Brown SE, Light RW. Identification of pulmonary hypertension in chronic obstructive pulmonary disease from routine chest radiographs. Am Rev Respir Dis. 1982;126(2):338–341. doi:10.1164/arrd.1982.126.2.338
25. Bertoli L, Mantero A, Cicero SL, Alpago R, Rizzato G, Belli C. Usefulness of two-dimentional echocardiography in the assessment of right heart in chronic obstructive lung disease. Progress Respiration Res Basel: Karger. 1985;91–100.
26. Danchin N, Cornette A, Henriquez A, et al. Two-dimensional echocardiographic assessment of the right ventricle in patients with chronic obstructive lung disease. Chest. 1987;92(2):229–233. doi:10.1378/chest.92.2.229
27. Chuang ML, Lin IF. Investigating the relationships among lung function variables in chronic obstructive pulmonary disease in men. Peer J. 2019;7:e7829. doi:10.7717/peerj.7829
28. Chuang ML, Lin IF, Hsieh MJ. More impaired dynamic ventilatory muscle oxygenation in congestive heart failure than in chronic obstructive pulmonary disease. J Clin Med. 2019;8(10):E1641. doi:10.3390/jcm8101641
29. Chuang ML, Lin IF, Wasserman K. The body weight-walking distance product as related to lung function, anaerobic threshold and peak VO2 in COPD patients. Respir Med. 2001;95(7):618–626. doi:10.1053/rmed.2001.1115
30. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
31. Wanger J, Clausen JL, Coates A, et al. Standardisation of the measurement of lung volumes. Eur Respir J. 2005;26(3):511–522.
32. ATS/ERS S. ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166(4):518–624.
33. Miller MR, Crapo R, Hankinson J, et al. General considerations for lung function testing. Eur Respir J. 2005;26(1):153–161. doi:10.1183/09031936.05.00034505
34. Chuang ML, Lin IF. Clinical characteristics and lung function in chronic obstructive pulmonary disease complicated with impaired peripheral oxygenation. Intern Emerg Med. 2014;9(6):633–640. doi:10.1007/s11739-013-0989-8
35. Wasserman K, Hansen JE, Sue DY, Stringer WW, Whipp BJ. Calculations, formulas, and examples. In: Wasserman K, editor. Principles of Exercise Testing and Interpretation. Philadelphia: Lippincot Williams & Wilkins; 2005:556–565.
36. Sun XG, Hansen JE, Garatachea N, Storer TW, Wasserman K. Ventilatory efficiency during exercise in healthy subjects. Am J Respir Crit Care Med. 2002;166(11):1443–1448. doi:10.1164/rccm.2202033
37. Young AL, Bragman FJS, Rangelov B, et al. Disease progression modelling in chronic obstructive pulmonary disease (COPD). Am J Respir Crit Care Med. 2020;201(3):294–302. doi:10.1164/rccm.201908-1600OC
38. Kitahara Y, Hattori N, Yokoyama A, et al. Cigarette smoking decreases dynamic inspiratory capacity during maximal exercise in patients with type 2 diabetes. Hiroshima J Med Sci. 2012;61(2):29–36.
39. Gläser S, Ittermann T, Koch B, et al. Influence of smoking and obesity on alveolar-arterial gas pressure differences and dead space ventilation at rest and peak exercise in healthy men and women. Respir Med. 2013;107(6):919–926. doi:10.1016/j.rmed.2013.02.013
40. Pinto-Plata VM, Celli-Cruz RA, Vassaux C, et al. Differences in cardiopulmonary exercise test results by american thoracic society/european respiratory society-global initiative for chronic obstructive lung disease stage categories and gender. Chest. 2007;132(4):1204–1211. doi:10.1378/chest.07-0593
41. Celli BR, Locantore N, Tal-Singer R, et al. Emphysema and extrapulmonary tissue loss in COPD: a multi-organ loss of tissue phenotype. Eur Respir J. 2018;51(2):
42. Lewis DA, Sietsema KE, Casaburi R, Sue DY. Inaccuracy of noninvasive estimates of VD/VT in clinical exercise testing. Chest. 1994;106(5):1476–1480. doi:10.1378/chest.106.5.1476
43. Liu Z, Vargas F, Stansbury D, Sasse SA, Light RW. Comparison of the end-tidal arterial PCO2 gradient during exercise in normal subjects and in patients with severe COPD. Chest. 1995;107(5):1218–1224. doi:10.1378/chest.107.5.1218
44. Sridhar MK, Carter R, Moran F, Banham SW. Use of a combined oxygen and carbon dioxide transcutaneous electrode in the estimation of gas exchange during exercise. Thorax. 1993;48(6):643–647. doi:10.1136/thx.48.6.643
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.