Back to Journals » OncoTargets and Therapy » Volume 13
Response to Pyrotinib in a Chinese Patient with Bone-Metastatic Scrotal Paget’s Disease Harboring Triple Uncommon HER2 Mutation: A Case Report
Authors Guo JJ, Jiao XD, Wu Y, Qin BD, Liu K, Zang YS
Received 5 January 2020
Accepted for publication 26 February 2020
Published 30 June 2020 Volume 2020:13 Pages 6289—6293
DOI https://doi.org/10.2147/OTT.S244814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nicola Silvestris
Jin-Ju Guo,1,2,* Xiao-Dong Jiao,1,* Ying Wu,1,* Bao-Dong Qin,1 Ke Liu,1 Yuan-Sheng Zang1
1Department of Medical Oncology, Changzheng Hospital, Second Military Medical University, Shanghai 200072, People’s Republic of China; 2Department of Medical Oncology, People’s Hospital of Qianshan County, Jiangxi 334500, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuan-Sheng Zang
Department of Medical Oncology, Changzheng Hospital, Second Military Medical University, 64 Hetian Road, Shanghai 200072, People’s Republic of China
Tel/ Fax +86 21-66540109-8039
Email [email protected]
Background: Previous studies have suggested the efficacy of HER2 antibody (trastuzumab) in scrotal Paget’s disease with HER2 amplification or overexpression. However, no report about the effectiveness of HER2 inhibitor (pyrotinib) in those patients has been provided until now.
Case Presentation: We present a case of a Chinese patient with bone-metastatic scrotal Paget’s disease harboring triple uncommon HER2 mutations (R678Q/S310Y/S310F). Due to poor conditions (severe anemia, thrombocytopenia, ECOG PS3), this patient could not tolerate traditional chemotherapy and radiotherapy. Then, the patient participated in a registered clinical trial (NCT03239015) about basket trial for intractable cancer. The patient received pyrotinib (400 mg po qd) and achieved a partial response for 4.0 months.
Conclusion: This is the first report describing a patient with scrotal Paget’s disease harboring triple uncommon HER2 mutation who responds well to pyrotinib. This case suggested that HER2 mutation is also a potential biomarker for treatment in extramammary Paget’s disease and pyrotinib may be an ideal choice for these patients.
Keywords: Paget’s disease, extramammary Paget’s disease, HER2, pyrotinib
Extramammary Paget’s disease (EMPD) is a rare skin malignancy firstly reported in 1889, which usually occurs in the anus, genitals, or axillary skin, including primary EMPD and secondary EMPD.1,2 Because EMPD lesions may mimic various dermatoses such as eczema, contact dermatitis, initially it is difficult to diagnose EMPD correctly. It has been reported that the average delayed time from the symptoms to diagnosis is approximately 3 years.3 A biopsy of the lesion should be performed to confirm the specific diagnosis for a chronic, nonhealing skin wound. The diagnosis is confirmed by the presence of Paget’s cells on the histopathological examination of a tissue specimen. Histologically, the classic Paget’s cells appear as large, round with lightly stained cytoplasm such as vacuoles. In some cases, the cytoplasm of Paget’s cells is rich in mucus with the signet ring of nuclear deflection. The epidermal spinous layer is often thickened, and single, clustered or island-shaped basophilic Paget’s cells appear in the lower part of the spinal layer, which could reach the entire epidermis.4 Basal cells are sometimes squashed by the cancerous nest between the basement membrane band and Paget’s cells in a flat band shape. Immunohistochemically, the Paget’s cells frequently show positive reactivity to epithelial membrane antigen such as CK7, EMA, CEA, MUC1, CerB-2, GCDFP-15.5 Besides, previous studies reported that 20.7% of EMPD patients exhibited HER2 amplification and the probability of HER2 amplification was more notable in patients with metastatic EMPD.6,7
Extensive local excision of the skin and subcutaneous tissue with immediate reconstruction is the main method for the treatment of EMPD.8 Multidisciplinary comprehensive treatment may be a reasonable choice for invasive Paget’s disease. Adjuvant therapy such as radiotherapy or systemic chemotherapy may be necessary. Chemotherapy using 5-fluorouracil, mitomycin-C and paclitaxel has been proven effective in inadequately excised and advanced EMPD.5 Except for traditional chemotherapy, previous studies have reported HER2-targeted monoclonal antibody (trastuzumab) could yield significant clinical benefit in lymph node-metastatic penoscrotal EMPD patients with HER2 amplification.9 Pyrotinib is an oral irreversible tyrosine kinase inhibitor capable of inhibiting the HER1, HER2, and HER4. Until now, there has been no any report about the effectiveness of pyrotinib in those patients with HER2 gene alteration.
Here, we present a case of an advanced penoscrotal EMPD patient harboring triple uncommon HER2 mutations, namely, ERBB2 R678Q in exon 17, S310Y in exon 8 and S310F in exon 8, who responds well pyrotinib.
Case Report
A 66-year-old male presented to the local hospital with a 2-month history of edema of the right lower extremity in May 2019. B-ultrasound revealed that the right inguinal swollen lymph node was about 2.3 cm*1.0 cm in size. A computed tomography (CT) scan revealed multiple bone destruction of the bone, and ECT showed focal increased bone metabolic activity. PET-CT showed multiple osteolytic bone destruction with increased metabolism, pathological fracture of the right third rib (Figure 1A). The right inguinal lymphadenectomy biopsy showed carcinoma of unknown primary site with metastatic poorly differentiated adenocarcinoma. Immunohistochemistry demonstrated strong positivity for Glypican-3 and GATA, negativity for CK7, Napsin, TTF-1, CK20, CDX2, PSA.
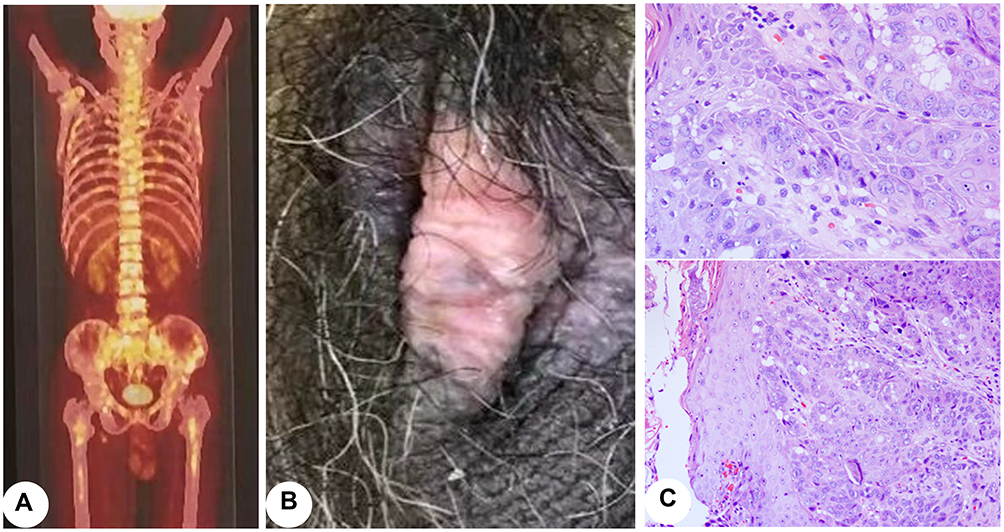 |
Figure 1 PET-CT showed multiple osteolytic bone destruction with increased metabolism, pathological fracture of the right third rib (A); eczema-like changes in the skin of the scrotum at the root of the penis (B); the epidermis was eroded partly, and scattered, nested Paget’s cells could be observed in the spinous layer with the dermal inflammatory cells infiltrated (C). |
After 1 month, the patient was hospitalized for cancer of unknown primary in our hospital. After a detailed medical history inquiry, the patient reported that there has been a rupture in the scrotum for approximately 4 years. Eczema-like change in the skin of the scrotum at the base of the penis was observed, with a size of 2.0x1.5 cm (Figure 1B). Then, the scrotal skin lesion biopsy was performed and pathological examination showed primary EMPD with Paget’s cells in the spinous layer (Figure 1C). Capture-based ultra-deep targeted sequencing was performed with a panel consisting of all exons and critical introns of 520 cancer-related genes. The next-generation sequencing assay showed that this patient had triple uncommon HER2 mutation, namely HER2 R678Q in exon 17, S310Y in exon 8 and S310F in exon 8 (Figure 2). Laboratory examination showed severe anemia (47g/L), thrombocytopenia (27*109/L), elevated CEA (17.8ng/mL), with ECOG PS 3 scores and pain NRS 6 scores.
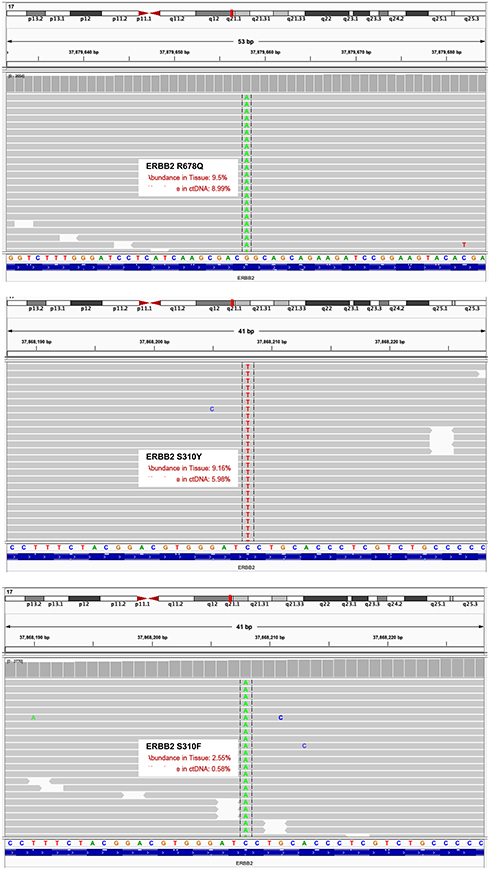 |
Figure 2 Next-generation sequencing (NGS) showed HER2 R678Q in exon 17, S310Y in exon 8 and S310F in exon 8; triple HER2 mutations could be observed in tissue and ctDNA. |
Due to poor conditions, the patient could not tolerate any traditional chemotherapy or radiotherapy. Then, the patient participated in a registered clinical trial (NCT03239015) in Shanghai Changzheng Hospital and received HER2 inhibitor pyrotinib (400 mg po qd). After pyrotinib treatment, the general pain and discomfort symptoms were significantly relieved, platelets and hemoglobin were increased (Figure 3). The Mefecon use dose for bone pain was also decreased to 1/3 of the original analgesic dose. After 2 months, CT scans revealed a significant decrease in tumor size of right inguinal lymph. According to the response evaluation criteria in solid tumor (version 1.1), the patient was considered to have a partial response to pyrotinib (Figure 3). The last CT scan showed that the right inguinal lymph node was stable (Figure 3). The follow-up is ongoing. Written informed consent has been provided by the patient to have the case details and any accompanying images published. Institutional approval was not required to publish the case details.
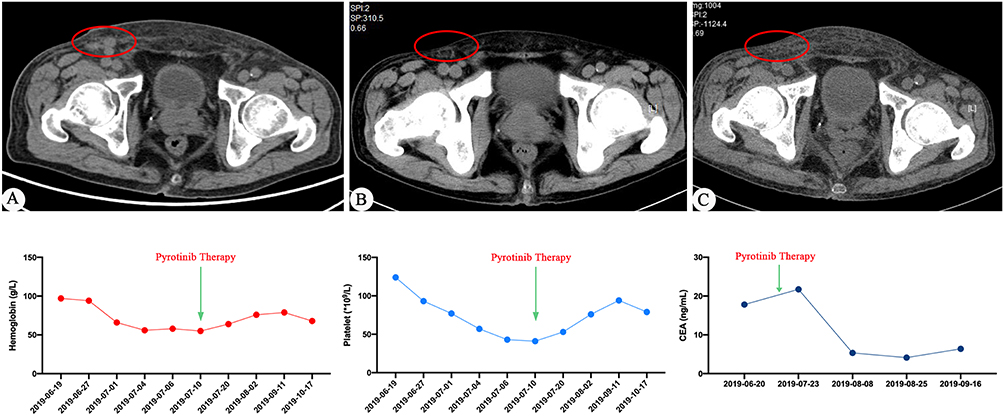 |
Figure 3 Computed tomography showed enlarged lymph nodes in the right groin area was shortened after pyrotinib treatment (A) before pyrotinib treatment and after (B) 2 months, (C) 3 months; hemoglobin and platelets counts were increased and CEA concentration was decreased. |
Discussion
The most common location of EMPD in males is the penoscrotal junction, followed in order by the scrotum and inguinal area.3 EMPD of the scrotum and penis is rare, which occurs predominantly in Asian males in the age group of 60–70 years.10 Inguinal lymph node metastases in patients with Scrotal Paget’s disease are more common, but distant metastasis is rare especially bone metastasis. There is no standard regimen for chemotherapy in patients with EMPD, some studies recommended the combined use of paclitaxel and other traditional chemotherapy drugs such as carboplatin.9 Except for chemotherapy, the previous study has suggested that local radiation therapy can also bring survival benefits.11
Due to a lack of standard of care treatment, EMPD could be classified into intractable cancer. In basket trials, genomic-guided therapy yields clinical benefits and provides novel insight into the optimal clinical management of this type of cancers.12 Histologically, EMPD is closely associated with Paget’s disease of the mammary gland. Previous studies reported that 15–60% of patients with EMPD harbor HER2 amplification or overexpression.7 And Her2-targeted trastuzumab monotherapy for EMPD patients has been described as clinical benefit with median progression-free survival (mPFS) from 6 to 12–17 months.13,14 However, the efficacy of HER2-targeted trastuzumab in advanced EMPD patients with HER2 mutation is limited, due to the therapeutic efficacy of trastuzumab is dependent on the HER2 overexpression and gene amplification of HER2.7 Therefore, trastuzumab combined with paclitaxel is effective, which has been recommended for those EMPD patients with HER2 amplification or overexpression.9
Pyrotinib is an oral irreversible tyrosine kinase inhibitor capable of inhibiting the HER1, HER2, and HER4 pathway.5 The previous Phase II clinical trial demonstrated that pyrotinib plus chemotherapy could yield an ORR of 78.5% with a PFS of 18.1 months for trastuzumab-resistant HER2-positive metastatic breast cancer patients.15 Therefore, pyrotinib has been recommended as a second-line medication for HER2-positive advanced breast cancer. In lung cancer patients, T-DM1 but not trastuzumab has been recommended for patients with HER2 mutation.16 However, the ideal choice for EMPD patients with HER2 mutation remains unknown. In 2019, Nordmann TM reported a case with EMPD harboring HER2 S310F mutation, who achieved near-complete response after treatment with trastuzumab and carboplatin.17 In the present study, we reported a novel HER2 gene alteration that these EMPD patients harbored triple uncommon HER2 mutations (R678Q/S310Y/S310F). Meanwhile, this patient showed a partial response to pyrotinib.
To our knowledge, this is the first report describing an advanced scrotal Paget’s disease patient harboring triple uncommon HER2 mutation who responds well to pyrotinib. This case contributes to the growing evidence of HER2 in the pathogenesis of metastatic EMPD and emphasizes the therapeutic efficacy of pyrotinib in these rare diseases.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hatta N. Prognostic factors of extramammary paget’s disease. Curr Treat Options Oncol. 2018;19(10):47. doi:10.1007/s11864-018-0567-4
2. Lam C, Funaro D. Extramammary Paget’s disease: summary of current knowledge. Dermatol Clin. 2010;28(4):807–826. doi:10.1016/j.det.2010.08.002
3. Yang WJ, Kim DS, Im YJ, et al. Extramammary Paget’s disease of penis and scrotum. Urology. 2005;65(5):972–975. doi:10.1016/j.urology.2004.12.010
4. Lopes Filho LL, Lopes IM, Lopes LR, Enokihara MM, Michalany AO, Matsunaga N. Mammary and extramammary Paget’s disease. An Bras Dermatol. 2015;90(2):225–231. doi:10.1590/abd1806-4841.20153189
5. Adashek JJ, Leonard A, Nealon SW, et al. Extramammary Paget’s disease: what do we know and how do we treat? Can J Urol. 2019;26(6):10012–10021.
6. Barth P, Dulaimi Al-Saleem E, Edwards KW, Millis SZ, Wong YN, Geynisman DM. Metastatic extramammary paget’s disease of scrotum responds completely to single agent trastuzumab in a hemodialysis patient: case report, molecular profiling and brief review of the literature. Case Rep Oncol Med. 2015;2015:895151.
7. Lu X, Zhang P, Zhu Y, Ye D. Human epidermal growth factor receptor 2 amplification as a biomarker for treatment in patients with lymph node-metastatic penoscrotal extramammary Paget’s disease. Oncol Lett. 2019;17(3):2677–2686. doi:10.3892/ol.2019.9930
8. Isrow D, Oregel KZ, Cortes J, et al. Advanced extramammary paget’s disease of the groin, penis, and scrotum. Clin Med Insights Oncol. 2014;8:87–90. doi:10.4137/CMO.S13107
9. Ichiyama T, Gomi D, Fukushima T, et al. Successful and long-term response to trastuzumab plus paclitaxel combination therapy in human epidermal growth factor receptor 2-positive extramammary Paget’s disease: a case report and review of the literature. Mol Clin Oncol. 2017;7(5):763–766. doi:10.3892/mco.2017.1422
10. Hsu L-N, Shen Y-C, Chen C-H, Sung M-T, Chiang P-H. Extramammary Paget’s disease with invasive adenocarcinoma of the penoscrotum: case report and systematic review. Urol Sci. 2013;24(1):30–33. doi:10.1016/j.urols.2013.01.003
11. Tagliaferri L, Casa C, Macchia G, et al. The role of radiotherapy in extramammary paget disease: a systematic review. Int J Gynecol Cancer. 2018;28(4):829–839. doi:10.1097/IGC.0000000000001237
12. Qin BD, Jiao XD, Liu K, et al. Basket trials for intractable cancer. Front Oncol. 2019;9:229. doi:10.3389/fonc.2019.00229
13. Wakabayashi S, Togawa Y, Yoneyama K, Suehiro K, Kambe N, Matsue H. Dramatic clinical response of relapsed metastatic extramammary paget’s disease to trastuzumab monotherapy. Case Rep Dermatol Med. 2012;2012:401362.
14. Watanabe S, Takeda M, Takahama T, et al. Successful human epidermal growth receptor 2-targeted therapy beyond disease progression for extramammary Paget’s disease. Invest New Drugs. 2016;34(3):394–396. doi:10.1007/s10637-016-0329-8
15. Ma F, Ouyang Q, Li W, et al. Pyrotinib or lapatinib combined with capecitabine in her2-positive metastatic breast cancer with prior taxanes, anthracyclines, and/or trastuzumab: a randomized, Phase II study. J Clin Oncol. 2019;37(29):2610–2619. doi:10.1200/JCO.19.00108
16. Li BT, Shen R, Buonocore D, et al. Ado-trastuzumab emtansine for patients with HER2-mutant lung cancers: results from a Phase II basket trial. J Clin Oncol. 2018;36(24):2532–2537. doi:10.1200/JCO.2018.77.9777
17. Nordmann TM, Messerli-Odermatt O, Meier L, et al. Sequential somatic mutations upon secondary anti-HER2 treatment resistance in metastatic ERBB2(S310F) mutated extramammary Paget’s disease. Oncotarget. 2019;10(62):6647–6650. doi:10.18632/oncotarget.27272
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.