Back to Journals » Infection and Drug Resistance » Volume 16
Responding to Higher-Than-Expected Infant Mortality Rates from Respiratory Syncytial Virus (RSV): Improving Treatment and Reporting Strategies
Authors Dvorkin J, De Luca J ![]() , Alvarez-Paggi D
, Alvarez-Paggi D ![]() , Caballero MT
, Caballero MT ![]()
Received 1 October 2022
Accepted for publication 16 January 2023
Published 27 January 2023 Volume 2023:16 Pages 595—605
DOI https://doi.org/10.2147/IDR.S373584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Julia Dvorkin,1,2 Julián De Luca,1 Damian Alvarez-Paggi,1,2 Mauricio T Caballero1,2
1Fundación INFANT, Buenos Aires, Argentina; 2Consejo Nacional de Investigaciones Científicas y Técnicas (CONICET), Buenos Aires, Argentina
Correspondence: Mauricio T Caballero, Fundación INFANT, Gavilán 94, Buenos Aires, Argentina, Email [email protected]
Abstract: Respiratory syncytial virus (RSV) has a major role in respiratory infections in young infants around the world. However, substantial progress has been made in recent years in the field of RSV. A wide variety of observational studies and clinical trials published in the past decade provide a thorough idea of the health and economic burden of RSV disease in the developing world. In this review, we discuss the impact of RSV burden of disease, major gaps in disease estimations, and challenges in generating new therapeutic options and an immune response against the virus, and briefly describe next generation technologies that are being evaluated.
Keywords: respiratory syncytial virus, vaccines, prevention, antivirals, therapeutics
Burden of RSV-Related Acute Lower Respiratory Tract Infection
Human respiratory syncytial virus (RSV) represents one of the most important threats to young infants’ health in the world.1 RSV is currently the most common cause of acute lower respiratory tract infection (LRTI), responsible for over 33 million episodes in young children worldwide and constituting the leading disease diagnosed in hospital admissions, with 3.2 million episodes per year during 2019.2–4 In addition, RSV-LRTI is one of the most important causes of post-neonatal mortality,3,5 with more than 99% of RSV-related childhood deaths occurring in low- and middle-income countries (LMICs).2,3
The enormous impact of RSV disease among young children is evident when considering both the global health burden and the economic burden. It is estimated that RSV produces 1.2 million discounted disability-adjusted life-years (DALYs), and a global economic burden on children under 5 of approximately US$4.82 billion.6 An alarming 65% of this burden comes from LMICs, with almost 55% of global costs stemming from LRTIs that require hospitalization.7 Besides, in 5–10% of the hospitalized infants, the disease can require an admission to the pediatric intensive care unit (PICU), which leads to a considerable increase in costs for the health services.8,9 Specific treatment of RSV infections is a considerable challenge. However, an effective intervention against RSV severe disease might reduce the hospital costs of illness as it may diminish hospital stay and PICU requirements by preventing progression to severe disease once infection has occurred. Therefore, multiple antivirals are being explored, but investment in development may be limited because of an underestimation of the burden of disease and limited access to a point-of-care detection method for RSV in children across all age groups.10
In this sense, there is an urgent need to implement preventive strategies. It is estimated that in a maternal vaccination and immunoprophylaxis scenario, more than 104,000 hospitalizations and 3000 deaths may be prevented yearly, while also potentially averting 98–137 discounted DALYs per 1000 person-years.6 Considering all these aspects, the World Health Organization (WHO) has set as a priority the development of safe, effective, and affordable preventive strategies for RSV disease.11
Therefore, a detailed quantification of RSV-related deaths is key for decision making and prioritization of next generation therapeutic and preemptive strategies based on maternal immunization, immunoprophylaxis, and effective allocation of health resources.1,12 Likewise, an assessment of accurate rates of RSV disease can be beneficial to track the progress towards a reduction in RSV-related mortality after the implementation of preventive interventions.13
Despite the similar hospitalization rates for children in the age range 0–60 months in both LMICs and high-income countries (HICs), there is a divergence in these rates in the 0–6 month subgroup.3 In young infants, the admission rate was 5.2 per thousand hospitalizations in LMICs and 8.2 per thousand in HICs in 2019.3 This variation in hospitalization rates in the first months of life, when RSV-LRTI is more hazardous, can also correspond to the discrepancy in the case fatality rates observed between countries in the same age range (1.1% in LMICs vs <0.05% in HICs).3,14 As a matter of fact, lower admission rates in young infants from poor settings can represent not only a lower level of access to healthcare but also a higher rate of home mortality due to this pathogen, as recently described in studies from LMICs.15–20 Indeed, for every in-hospital infant death due to RSV-LRTI, three deaths occurred at the community level in LMICs.3,9,14,16,19 This gap in the mortality burden due to RSV is shown to be substantially increased in some rural areas with extremely poor access to healthcare facilities, where reports showed that 13 children died outside the health facilities for every single death at hospital.3,12,19 Despite consistent progress in understanding the impact of RSV disease in the developing world, there are still major discrepancies in the estimated mortality burden.12
Major Gaps in Estimating RSV Disease Burden
Precise determination of the global mortality burden of RSV is challenging for several reasons.12,21 First, there is no affordable, sensitive, and specific diagnostic test available for countries with limited economic resources.12,21,22 Gold standard diagnostic tests are based on real-time polymerase chain reaction (RT-PCR), which requires qualified human resources and highly expensive equipment and supplies.22 Second, diagnostic accuracy based on vital statistics, verbal autopsies, or medical records is low, especially in poor settings, where mortality rates can be excessively high.23–26 Lastly, methods based on complete autopsies, necropsies, or minimally invasive tissue sampling, which can be considered gold standards, are not commonly performed in LMICs owing to technical and economic inequity, in addition to cultural, political, and religious reasons.27–29
Estimates of the total burden of LRTIs, in general and specifically due to RSV, generated by different research groups present discrepancies that can be difficult to reconcile.13,30 In this sense, the paucity of diagnostic methods and registries based on active surveillance studies in constrained settings obstacles for accuracy.12 For these reasons, different groups have established a diversity of mathematical and statistical methods to determine the full picture of the total burden of RSV disease.3,13,30
Although different statistical models show disparities in global etiologic fractions of RSV deaths, variations in the data source and modeling also impact the estimation of the burden of other LRTI causes (Table 1). In 2010, the relative difference between Child Health Epidemiology Reference Group (CHERG) and Global Burden of Disease (GBD) in global mortality due to LRTI in children under 5 was 49%, with 1,396,000 and 847,000 total deaths calculated, respectively.13,31,32 GBD estimations from 2010 showed that the total mortality burden due to RSV was calculated as 234,000 deaths, while Nair et al showed 66,000 deaths in 2005 (71% less).8,31 Mortality estimates due to RSV in 2016 were lower than in previous years (Table 1); however, the relative difference between GBD and Respiratory Virus Global Epidemiology Network (RSV GEN) groups was −37%.2,30 More recently, the RSV GEN consortium has published the global RSV disease burden estimates for 2019. For this calculation, the group expanded the information obtained previously, adding data from primary studies that determined the community mortality burden in 11 LMICs, which allowed them to improve the overall estimation.3
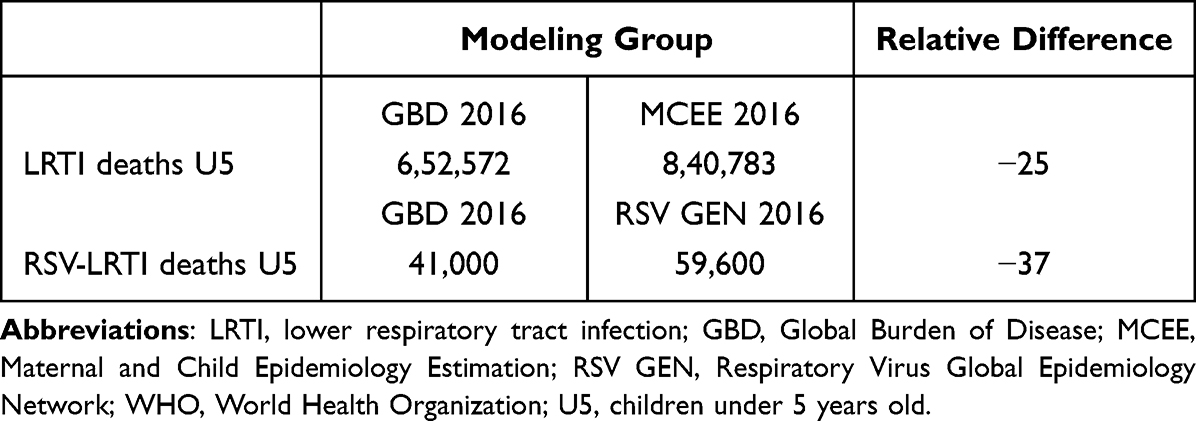 |
Table 1 Estimates of the Global Burden Due to All Causes of LRTI and RSV-LRTI in Children Under Five in 2016 |
Next Steps to Improve RSV Burden Estimates
It remains crucial to establish clear epidemiological surveillance strategies for interventions in the future. In this sense, it is fundamental that decision makers from LMICs recognize the relevance of RSV as a cause of morbidity and mortality in young children. The planning of robust and cost-effective surveillance systems, leveraging existing resources and capacities, is key.33 However, some caveats must be considered before establishing an active epidemiological surveillance program.
The criteria for RSV case definition for surveillance and viral detection can be problematic. In contrast to severe acute respiratory infection (SARI) or influenza-like illness (ILI), patients with RSV-ARI usually do not have the same signs and symptoms during the disease.34 For this reason, both SARI and ILI, which are usually used for influenza surveillance worldwide, can underestimate RSV incidence by 50–80%.35 Therefore, an extension of clinical signs for the screening of infants is necessary to increase RSV detection. The WHO recommends extending clinical diagnosis criteria to patients without fever, or with apnea or sepsis.33 Even though the WHO recommendation can be sensitive for RSV diagnosis,36 it may be incomplete. From this perspective, severe RSV-LRTI usually presents with hypoxemia, wheezing, or subcostal indrawing, which are not included in SARI or ILI case definitions (Table 2).36,37
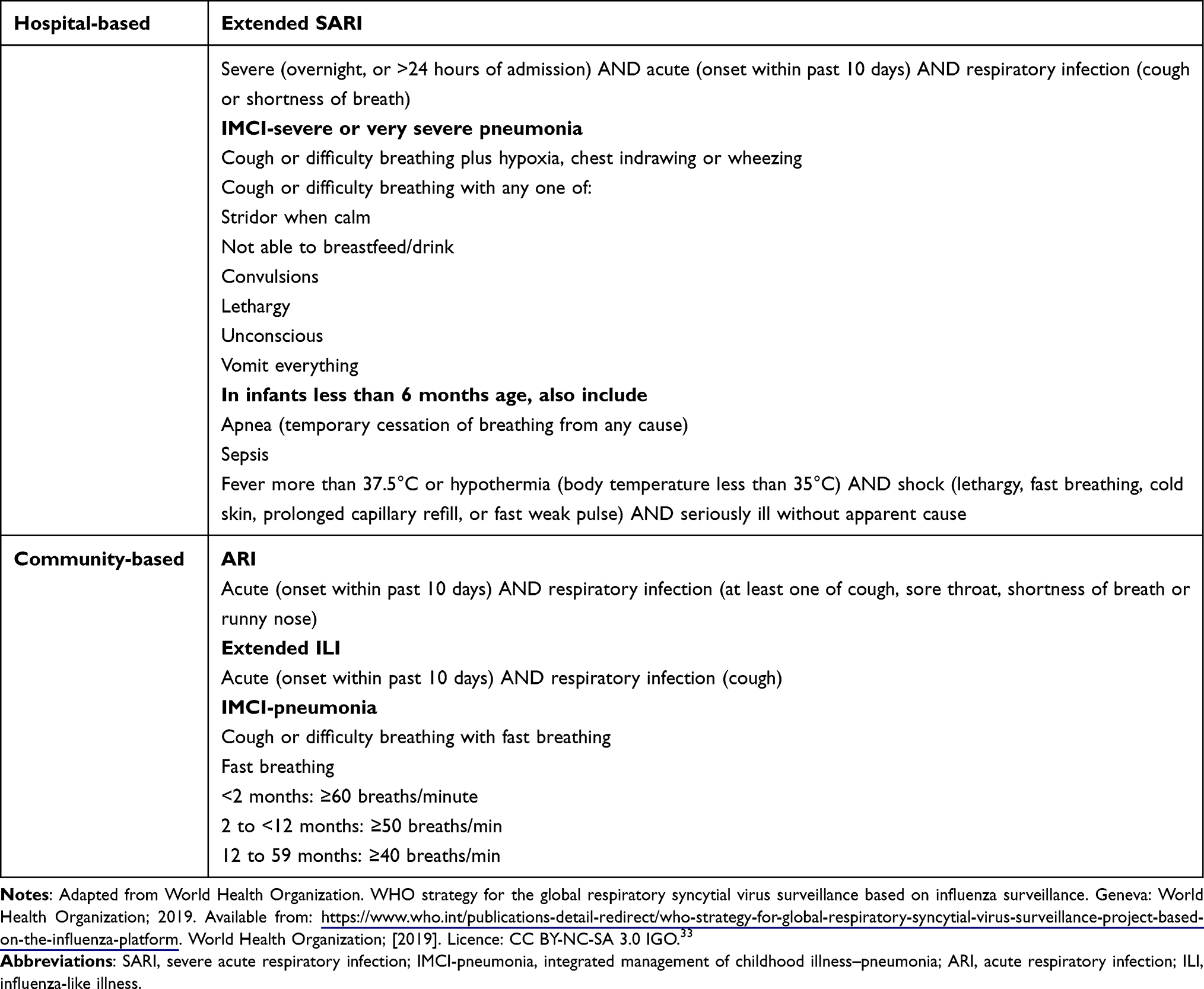 |
Table 2 Case Definition for RSV Surveillance |
The recent determination of RSV community mortality surveillance in LMICs was key to understanding the role of viruses in silent deaths that occur outside facilities.1 However, diagnostic approaches and results may vary depending on the method used to attribute deaths to RSV. In this sense, the advent of minimally invasive tissue sampling (MITS) and expert panel revision of cases may be considered a new diagnostic gold standard.1,4,12,17 Studies conducting MITS procedures for RSV surveillance can provide valuable information for improving statistical models. Attribution rates based on different scenarios of sampling methods or diagnostic tests can provide information to enable adjustments to be made based on more reliable methods.
Challenges in Generating Natural or Artificial Immunity Against RSV
RSV infection and the subsequently elicited immune response present multiple exceptional characteristics. Although virtually all children by the age of 3 years old have been infected, RSV infection repeats continuously throughout life with low variations in antigenicity, apparently by inducing immunological amnesia,38 a phenomenon that has been described in detail for other pathogens, such as measles.39 Moreover, inappropriate or dysregulated responses can be pathogenic: enhanced RSV disease (ERD) is a prime example of a vaccine-associated enhanced disease; such diseases consist of modified clinical manifestations and outcomes in individuals exposed to a wild-type pathogen following prior vaccination for that same pathogen, and constitute a much-studied phenomenon.40,41 Thus, both natural infection and vaccination introduce several challenges in eliciting a safe and effective immunological response.
The Complex Network of Host–Pathogen Interactions Involving RSV
Multiple crosstalk points between RSV and the host’s immune system have been described. During the early stages of infection, the viral non-structural (NS) 1 and NS2 proteins are expressed. These two proteins cooperate to downregulate the production and signaling of both type I and type III interferon (IFN) levels, despite strong viral replication, dampening innate immune responses and ultimately affecting the strength of the adaptive response.42 RSV G glycoprotein, which is one of the predominant viral surface proteins (in addition to F glycoprotein), has been postulated to exert multiple functions.43 Existing both as a membrane protein in the viral particle and as a secreted form from infected cells, apart from viral attachment, G glycoprotein has been ascribed a plethora of immunomodulatory functions. G has been postulated: to act as a virokine by interaction with CX3C.R1, disrupting leukocyte chemotaxis;44 to exert a decoy function for neutralizing antibodies;45 and even to downregulate the activation of dendritic cells (DCs) by interaction with DC-SIGN and L-SIGN.46
In addition, RSV has been reported to infect and affect the function of multiple immune cells, such as DCs,47 natural killer (NK) cells,48 regulatory B lymphocytes (BRegs),49 CD4+ cells,50 CD8+ cells,51 and even macrophages, in a persistent fashion by altering patterns of gene expression.52 Moreover, RSV has been shown to induce the depletion of regulatory T cells (TRegs) and hinder the activation of T cells by inhibiting the immunological synapse assembly among these DCs and T cells.53 Altogether, such complexity in the host–pathogen interactions, encompassing both immunomodulatory effects and infection of immune cells with concomitant alteration of function, is likely to underlie the mechanistic bases for the immunological amnesia that results in the commonly observed multiple repeated infections during a person’s lifetime.
Challenges in RSV Vaccine Development
Additional challenges in generating effective preventive strategies stem from the history of failed attempts at producing a safe vaccine candidate. In 1966, a formalin-inactivated RSV (FIRSV) vaccine was tested in infants and young children in the United States. FIRSV primed for ERD, resulting in hospitalization rates of up to 80% and two deaths in immunized infants upon viral infection.54,55 These events hampered RSV vaccine development for decades, and clinical immunopathological and transcriptional footprints of ERD in humans have only recently been uncovered.56 ERD is characterized by an exuberant inflammatory response, severe alveolar injury, eosinophil infiltration and degranulation, and suppressed surfactant proteins and type I IFN. The molecular bases of ERD have been ascribed to the production of low-avidity, non-protective anamnestic antibodies during infection of wild-type RSV (wtRSV) post-immunization, triggering complement-mediated injury.57,58 Moreover, a Th2 polarization of the immune response has been described in animal models59 and recently confirmed in humans,56 with Th2 cytokines enhancing pulmonary pathology, mucus secretion, and airway resistance.40,41 The mechanistic description of ERD has not been fully uncovered, although a strong case has been built around the possibility of original antigenic sin (OAS) lying at the root of this phenomenon.60 The OAS theory considers that exposure to similar (but not identical) antigens conditions the response to subsequent exposure to the WT antigen, as in the case of immunization with an inactivated vaccine or a recombinantly produced immunogen followed by natural infection. Thus, past exposure may impact negatively on the memory response to challenge, and, in particular, on vaccine safety and efficacy. Consequently, it is imperative to carefully design and test novel antigens in the quest to generate a safe, effective vaccine.56
Preventive Strategies Under Development
At present, 34 candidates for RSV disease prevention are being tested, eight of them aimed at the pediatric population and another three for pregnant women.61 In the vaccine development field, four different approaches are being evaluated: live attenuated or chimeric vaccines, protein-based (inactivated, particle, or subunit) vaccines, recombinant vectors, and nucleic acid vaccines.61 For immunoprophylaxis, three monoclonal antibodies (mAbs) are in the preclinical stage, one is in phase 1 and two are in phase 3 clinical trials.61
Recent results from phase 2 and 3 clinical trials of candidate vaccines and long-lived mAbs set the hallmark for an upcoming new era in RSV prevention. The allocation of preventive strategies to specific subgroups of individuals is fundamental for future immunization strategies. In this sense, there are several challenges and concerns to be addressed.
Preemptive interventions should generate a robust immune response in the first 3–6 months of life. In this sense, maternal immunization seemed to be the best approach to confer protection in the first months of life. Nevertheless, the benefits of the vaccination against RSV for pregnant women can be controversial because it is not clear how this virus affects this specific population.62,63 In addition, the vaccination window during pregnancy may affect vaccine efficacy in preterm neonates and infants with prenatal growth restrictions.64
The immunization plan for older infants could emulate the influenza vaccination strategy. However, there are some challenges regarding the vaccination timeline, duration of immunity, and role of other respiratory viruses that can occupy the RSV viral niche.
Immunoprophylaxis based on long-lived mAbs may be a reasonable intervention in preterm babies or infants with severe comorbidities. Nonetheless, exhaustive cost-effectiveness analysis should be carried out to determine the capacity of LMICs to afford this type of prophylaxis. To date, the only preventive strategy approved for use in humans is Palivizumab®, a mAb, restricted only to premature infants born with less than 29 weeks of gestational age or less than 32 weeks when associated with severe cardiac or respiratory comorbidities.65 The requirement of administering more than five doses to achieve an efficacy close to 55% (owing to its low half-life) is the main disadvantage of this intervention.66
In the next section, we will briefly describe the most advanced candidates in development for RSV disease prevention, by their target population.
Pediatric Immunization
Live-attenuated vaccines (LAVs) are specifically designed to generate a potent immune response, eliciting local mucosal humoral and cellular adaptive immunity, by mimicking natural infection while diminishing its virulence for reduced pathogenesis.
- MV-012-968 (Meissa Vaccines): this investigational recombinant RSV LAV, inoculated as an intranasal spray, is being tested in parallel in both adults and children. First, a randomized, placebo-controlled, double-blind phase 2a human challenge study, run in healthy adults prescreened for low RSV immunogenicity, has already been completed and official results are expected to be revealed soon (NCT04690335). Second, a dose-escalation phase 1c trial testing the vaccine in 63 seronegative children between 6 and 36 months of age started in June 2021. The study aims to evaluate the safety and immunogenicity of administering three different concentrations of the candidate vaccine, inoculated in either one or two doses (NCT04909021).
- Sanofi’s VAD00001 intranasal LAV phase 2 trial for infants and toddlers (6–18 months) started in September 2020. This study aims to assess the safety profile of each dose of the study product and to characterize the RSV-A serum neutralizing antibody response. Its mechanism of action is based on NS2 or NS1 deletion, which bolsters the innate response (NCT04491877).
Subunit vaccines are protein-based candidates that primarily induce a CD4 T-cell response.41 New protein-based vaccines are in development that implement non-F viral antigens, circumventing previous ERD risks.
Recombinant vectors: vector-based vaccines use an innovative replication-incompetent carrier vector to deliver RSV antigens and induce an immune response against them, ideally without generating any response against the carrier.
Janssen developed the Ad26.RSV.preF vaccine for both the elderly and pediatric population, based on the human Adenovirus strain 26 vector expressing the F protein stabilized in the pre-fusion conformation. Remarkable results were found in a phase 2 trial in adults, which demonstrated protection from RSV infection in a human challenge model: following intranasal viral challenge, the primary endpoint (rtPCR-determined RSV) was significantly lower in volunteers who received Ad26.RSV.preF compared to placebo.67 The vector-based active was also found to be safe and well tolerated in a phase 1/2b trial tested in seropositive infants aged 12–24 months, while also eliciting a substantial humoral and cellular immune response (NCT03303625, NCT03606512, and NCT04908683).
Maternal Immunization
Subunit vaccines based on F subunits are under development exclusively for pregnant women and older people who have already been previously exposed to RSV and are therefore not at risk of developing enhanced respiratory disease.5
- Pfizer’s RSVpreF vaccine’s phase 2b trial was conducted in healthy women who were pregnant from 24 to 36 weeks of gestation, with the concomitant evaluation of their newborn infants. RSVpreF vaccine elicited high neutralizing titers in maternal sera obtained at the time of delivery, with none of the adverse events reported in infants considered by the investigators to be related to maternal vaccination. In an interim analysis performed during the 2020 RSV season, estimated vaccine efficacy in infants for any medically attended RSV-associated LRTI was 84.7% (95% CI 21.6 to 97.6) and for medically attended severe RSV-associated LRTI, 91.5% (95% CI −5.6 to 99.8).68 A phase 3 clinical efficacy trial involving infants born to women who received 120 μg of RSVpreF vaccine without aluminum hydroxide (owing to its local adverse events) during pregnancy is under way to evaluate its safety and efficacy against medically attended LRTI (MA-LRTI) and medically attended severe LRTI in infants through 180 days of life and during the first year of life (NCT04424316).
- GlaxoSmithKline: in phase 1 and 2b studies, the pre-F subunit vaccine RSVpreF3, for maternal immunization to protect infants, showed a 14-fold increase in RSV A and B neutralizing antibody titers 1 week after vaccination, and maintained a six-fold increase or more after 91 days in healthy women who were not pregnant.69 A phase 3 clinical trial designed to evaluate its effect on MA-LRTI due to RSV in infants up to 6 months of age was halted on February 18, 2022 (NCT04605159).
Immunoprophylaxis
One of the most important aspects to consider in the development of next generation mAbs is affordability, which can be achieved by investing in higher efficiency of production, increased duration of effect, and the development of biosimilars. It is vital for new mAbs in development to become more accessible in order to shift to a cost-effective strategy that can bridge between the areas where future vaccines may not be able to generate an efficient immune response, such as in extremely premature infants and immunocompromised children.
Next generation RSV antibodies have been engineered with Fc mutations to extend their half-life and enable protection for an entire RSV season.5 The leading candidate is Nirsevimab (Astra Zeneca, Sanofi), a mAb targeting the RSV fusion protein which, in a phase 3 RCT, was demonstrated to have efficacy of 74.5% (95% CI 49.6–87.1; P<0.001) in the reduction of MA-RSV-associated LRTI in healthy preterm infants (born at a gestational age of 29 to <35 weeks) through 150 days after injection.70
Clesrovimab (MK-1654) is another mAb, binding to site IV of the F glycoprotein, under development, with an extended half-life. This mAb is in phase 2b/3 trials (NCT04767373) and phase 3 trials (NCT04938830) in infants and children at increased risk for severe RSV disease, with an estimated completion date of April 2026. Trial simulations predict that a single dose of Clesrovimab may provide ≥75% efficacy for the prevention of RSV LRTI, lasting for at least 150 days.71
Treatment Strategies
Treatment for RSV infection is currently limited to supportive care and involves maintaining good hydration and oxygen therapy if necessary. Pharmacological agents such as bronchodilators or corticosteroids are often used to relieve RSV symptoms in infants, but their efficacy has not been proven during randomized controlled trials.72
Ribavirin, a nucleoside analog able to suppress RSV replication, is, to date, the only antiviral approved for RSV infection. However, the use of this drug is controversial as severe adverse effects have been reported.73,74 A recent meta-analysis showed no differences in mortality (risk ratio 0.63; 95% CI: 0.28–1.42) in all subjects treated with aerosol/oral ribavirin compared to supportive care.75 It only showed efficacy in subjects with hematological malignancy or stem cell transplants.75
Multiple antiviral agents are being explored to attenuate the severity of infection. The development of an effective therapeutic against RSV may have an impact not only in acute disease but also in the reduction of long-term wheezing, an outcome that should be evaluated when feasible. The most advanced antiviral agents under development target the F protein to inhibit the entry of the virus (Presatovir, JNJ-53718678, Ziresovir, and RV521 – Sisunatovir) or act by blocking RSV replication (EDP-938).76 Lumicitabine, an oral nucleoside analog pro-drug which inhibits RSV polymerase activity, has been suspended owing to toxicity concerns in infants.77
Presatovir (GS-5806) is an oral fusion inhibitor that blocks pre-fusion protein conformational change.78 In a trial in healthy human adults, patients challenged with RSV and treated with GS-5806 had reduced viral loads and lower symptom scores.79 The most recent phase 2 studies to evaluate this antiviral agent in high-risk patients, such as lung transplant patients80 and hematopoietic cell transplant recipients,81 did not show reductions in viral loads or improvement in clinical outcomes.
JNJ-53718678 (JNJ-8678) is an RSV-specific fusion inhibitor. In a placebo-controlled study, healthy adults challenged with RSV treated with this antiviral showed reduced viral loads and clinical disease severity.82 In a phase 1b trial in children aged 1–24 months, treatment with JNJ-8678 administered for 7 days was well tolerated and there was a greater reduction in viral load with JNJ-8678 than with placebo.83 Larger studies are needed to assess the effects on clinical outcomes. Safety and efficacy are currently being studied in a phase 2 trial (NCT03656510) in children aged ≥28 days to ≤3 years with RSV infection.
Ziresovor (AK0529), another oral F-protein inhibitor, in a phase 2 study, VICTOR (NCT02654171), demonstrated no severe adverse effects and early suggestions of clinical efficacy against RSV. In a phase 3 trial developed in infants aged 1–24 months hospitalized with RSV infection in China (AirFLO, NCT04231968), Ziresovir demonstrated a rapid onset of clinical effects after 2 days of treatment, with more pronounced benefits in infants aged <6 months, and a significant antiviral effect (77% viral load reduction compared with placebo).
Sisunatovir (RV521) is an orally available, small molecule inhibitor of RSV F protein. In a randomized, double-blind, placebo-controlled trial (NCT03258502), healthy adults were challenged with RSV. Positive results regarding viral loads and clinical outcomes were obtained, and there was no evidence of viral resistance.84 This drug is currently in phase 2 clinical development in infants (REVIRAL 1, NCT04225897).
EDP-938 is a nonfusion replication inhibitor of RSV that acts by modulating the viral nucleoprotein (N protein). In a phase 2a, randomized, double-blind, placebo-controlled, human virus challenge trial (NCT03691623), all EDP-938 regimens were shown to be superior to placebo with regard to the lowering of viral load, total symptom scores, and mucus weight.85 Intervention with EDP-938 after only a short symptom window of up to 48 hours in adults with upper respiratory tract infection is currently being evaluated in an ongoing clinical study (NCT04196101). There is also an ongoing phase 2, randomized, double-blind, placebo-controlled, trial to evaluate EDP-938 regimens in infants (aged 28 days to 36 months) infected with RSV (start date April 2022, NCT04816721).
Conclusions
RSV is the most important cause of hospitalizations and a leading cause of child mortality globally. It is responsible for significant resource utilization and costs for healthcare systems, patients, and their families. Although estimating the total burden of disease is challenging, several improvements have been achieved in the past few years. In the scope of new treatments in development and promising clinical vaccine trials, it is mandatory to conduct cost-effectiveness analyses to guide public health decision making. To achieve this aim, it is crucial to establish epidemiological surveillance strategies to capture not only inpatient cases and deaths, but also the community burden of disease and mortality. Moreover, RSV infection surveillance through high-sensitivity and high-specificity point-of-care tests may be needed to monitor the effectiveness of new antivirals and vaccines in the community, mostly in low-income settings.
Disclosure
Dr Mauricio T Caballero has received grant support from the Bill & Melinda Gates Foundation. The authors report no other conflicts of interest in this work.
References
1. Srikantiah P, Vora P, Klugman KP. Assessing the full burden of respiratory syncytial virus in young infants in low- and middle-income countries: the importance of community mortality studies. Clin Infect Dis. 2021;73(Supplement_3):S177–9. doi:10.1093/cid/ciab486
2. Shi T, McAllister DA, O’Brien KL, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390(10098):946–958.
3. Li Y, Wang X, Blau DM, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. 2022;399(10340):2047–2064.
4. Li Y, Johnson EK, Shi T, et al. National burden estimates of hospitalisations for acute lower respiratory infections due to respiratory syncytial virus in young children in 2019 among 58 countries: a modelling study. Lancet Respir Med. 2021;9(2):175–185.
5. Mazur NI, Terstappen J, Baral R, et al. Respiratory syncytial virus prevention within reach: the vaccine and monoclonal antibody landscape. Lancet Infect Dis. 2022;2022:1.
6. Li X, Willem L, Antillon M, Bilcke J, Jit M, Beutels P. Health and economic burden of respiratory syncytial virus (RSV) disease and the cost-effectiveness of potential interventions against RSV among children under 5 years in 72 Gavi-eligible countries. BMC Med. 2020;18(1):82.
7. Zhang S, Akmar LZ, Bailey F, et al. Cost of Respiratory Syncytial Virus-Associated Acute Lower Respiratory Infection Management in Young Children at the Regional and Global Level: a Systematic Review and Meta-Analysis. J Infect Dis. 2020;222(Supplement_7):S680–7.
8. Nair H, Nokes DJ, Gessner BD, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet. 2010;375(9725):1545–1555.
9. Geoghegan S, Erviti A, Caballero MT, et al. Mortality due to respiratory syncytial virus. burden and risk factors. Am J Respir Crit Care Med. 2017;195(1):96–103.
10. Simões EAF, DeVincenzo JP, Boeckh M, et al. Challenges and opportunities in developing respiratory syncytial virus therapeutics. J Infect Dis. 2015;211(suppl_1):S1–20.
11. WHO preferred product characteristics for respiratory syncytial virus (RSV) vaccines; 2022. Available from: https://www.who.int/publications-detail-redirect/WHO-IVB-17.11.
12. Caballero MT, Satav A, Gill CJ, et al. Challenges of assessing community mortality due to respiratory viruses in children aged less than 5 years. Clin Infect Dis. 2021;73(Supplement_3):S248–54.
13. Kovacs SD, Mullholland K, Bosch J, et al. Deconstructing the differences: a comparison of GBD 2010 and CHERG’s approach to estimating the mortality burden of diarrhea, pneumonia, and their etiologies. BMC Infect Dis. 2015;15(1):1.
14. Mazur NI, Löwensteyn YN, Willemsen JE, et al. Global respiratory syncytial virus–related infant community deaths. Clin Infect Dis. 2021;73(Supplement_3):S229–37.
15. Caballero MT, Bianchi AM, Nuño A, et al. Mortality associated with acute respiratory infections among children at home. J Infect Dis. 2019;219(3):358–364.
16. Caballero MT, Bianchi AM, Grigaites SD, et al. Community mortality due to respiratory syncytial virus in Argentina: population-based surveillance study. Clin Infect Dis. 2021;73(Supplement_3):S210–7.
17. Blau DM, Baillie VL, Els T, et al. Deaths attributed to respiratory syncytial virus in young children in high–mortality rate settings: report from Child Health And Mortality Prevention Surveillance (CHAMPS). Clin Infect Dis. 2021;73(Supplement_3):S218–28.
18. Gill CJ, Mwananyanda L, MacLeod WB, et al. Infant deaths from respiratory syncytial virus in Lusaka, Zambia from the ZPRIME study: a 3-year, systematic, post-mortem surveillance project. Lancet Glob Health. 2022;10(2):e269–77.
19. Simões EAF, Dani V, Potdar V, et al. mortality from respiratory syncytial virus in children under 2 years of age: a prospective community cohort study in Rural Maharashtra, India. Clin Infect Dis. 2021;73(Supplement_3):S193–202.
20. Kazi AM, Aguolu OG, Mughis W, et al. Respiratory syncytial virus–associated mortality among young infants in Karachi, Pakistan: a prospective postmortem surveillance study. Clin Infect Dis. 2021;73(Supplement_3):S203–9.
21. Zanone SM, Krause LK, Madhi SA, et al. Challenges in estimating RSV-associated mortality rates. Lancet Respir Med. 2016;4(5):345–347.
22. Butt SA, Maceira VP, McCallen ME, Stellrecht KA. Comparison of three commercial RT-PCR systems for the detection of respiratory viruses. J Clin Virol. 2014;61(3):406–410.
23. Menéndez C, Quintó L, Castillo P, et al. Limitations to current methods to estimate cause of death: a validation study of a verbal autopsy model. Gates Open Res. 2021;4:55.
24. Gupta N, Bharti B, Singhi S, Kumar P, Thakur JS. Errors in filling WHO death certificate in children: lessons from 1251 death certificates. J Trop Pediatr. 2014;60(1):74–78.
25. Mathers CD, Fat DM, Inoue M, Rao C, Lopez AD. Counting the dead and what they died from: an assessment of the global status of cause of death data. Bull World Health Organ. 2005;83(3):171–177.
26. Ordi J, Ismail MR, Carrilho C, et al. Clinico-pathological discrepancies in the diagnosis of causes of maternal death in sub-saharan Africa: retrospective analysis. PLoS Med. 2009;6(2):e1000036.
27. Cox JA, Lukande RL, Kateregga A, Mayanja-Kizza H, Manabe YC, Colebunders R. Autopsy acceptance rate and reasons for decline in Mulago Hospital, Kampala, Uganda. Trop Med Int Health. 2011;16(8):1015–1018.
28. Oluwasola OA, Fawole OI, Otegbayo AJ, Ogun GO, Adebamowo CA, Bamigboye AE. The autopsy: knowledge, attitude, and perceptions of doctors and relatives of the deceased. Arch Pathol Lab Med. 2009;133(1):78–82.
29. Tan GC, Hayati AR, Khong TY. Low perinatal autopsy rate in Malaysia: time for a change. Pediatr Dev Pathol. 2010;13(5):362–368.
30. Troeger C, Blacker B, Khalil IA, et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Infect Dis. 2018;18(11):1191–1210.
31. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128.
32. Liu L, Johnson HL, Cousens S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379(9832):2151–2161.
33. World Health Organization. WHO strategy for the global respiratory syncytial virus surveillance based on influenza surveillance. Geneva: World Health Organization; 2019. Available from: https://www.who.int/publications-detail-redirect/who-strategy-for-global-respiratory-syncytial-virus-surveillance-project-based-on-the-influenza-platform.
34. Pebody R, Moyes J, Hirve S, et al. Approaches to use the WHO respiratory syncytial virus surveillance platform to estimate disease burden. Influenza Other Respi Viruses. 2020;14(6):615–621.
35. Saha S, Pandey BG, Choudekar A, et al. Evaluation of case definitions for estimation of respiratory syncytial virus associated hospitalizations among children in a rural community of northern India. J Glob Health. 2015;5(2):010419.
36. Nyawanda BO, Mott JA, Njuguna HN, et al. Evaluation of case definitions to detect respiratory syncytial virus infection in hospitalized children below 5 years in Rural Western Kenya, 2009–2013. BMC Infect Dis. 2016;16(1):218.
37. Atwell JE, Geoghegan S, Karron RA, Polack FP. Clinical predictors of critical lower respiratory tract illness due to respiratory syncytial virus in infants and children: data to inform case definitions for efficacy trials. J Infect Dis. 2016;214(11):1712–1716.
38. Openshaw PJM, Chiu C, Culley FJ, Johansson C. Protective and Harmful Immunity to RSV Infection. Annu Rev Immunol. 2017;35:501–532.
39. Mina MJ, Kula T, Leng Y, et al. Measles virus infection diminishes preexisting antibodies that offer protection from other pathogens. Science. 2019;366(6465):599–606.
40. Munoz FM, Cramer JP, Dekker CL, et al. Vaccine-associated enhanced disease: case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. 2021;39(22):3053–3066.
41. Acosta PL, Caballero MT, Polack FP. Brief history and characterization of enhanced respiratory syncytial virus disease. Clin Vaccine Immunol. 2016;23(3):189–195.
42. Sedeyn K, Schepens B, Saelens X. Respiratory syncytial virus nonstructural proteins 1 and 2: exceptional disrupters of innate immune responses. PLoS Pathog. 2019;15(10):e1007984.
43. McLellan JS, Ray WC, Peeples ME. Structure and function of respiratory syncytial virus surface glycoproteins. Curr Top Microbiol Immunol. 2013;372:83–104.
44. Tripp RA, Jones LP, Haynes LM, Zheng H, Murphy PM, Anderson LJ. CX3C chemokine mimicry by respiratory syncytial virus G glycoprotein. Nat Immunol. 2001;2(8):732–738.
45. Bukreyev A, Yang L, Fricke J, et al. The secreted form of respiratory syncytial virus G glycoprotein helps the virus evade antibody-mediated restriction of replication by acting as an antigen decoy and through effects on Fc receptor-bearing leukocytes. J Virol. 2008;82(24):12191–12204.
46. Johnson TR, McLellan JS, Graham BS. Respiratory syncytial virus Glycoprotein G interacts with DC-SIGN and L-SIGN to activate ERK1 and ERK2. J Virol. 2012;86(3):1339–1347.
47. Tognarelli EI, Bueno SM, González PA. Immune-modulation by the human respiratory syncytial virus: focus on dendritic cells. Front Immunol. 2019;10:5.
48. van Erp EA, Feyaerts D, Duijst M, et al. Respiratory syncytial virus infects primary neonatal and adult natural killer cells and affects their antiviral effector function. J Infect Dis. 2019;219(5):723–733.
49. Zhivaki D, Lemoine S, Lim A, et al. Respiratory syncytial virus infects regulatory B cells in human neonates via chemokine receptor CX3CR1 and promotes lung disease severity. Immunity. 2017;46(2):301–314.
50. Raiden S, Sananez I, Remes-Lenicov F, et al. Respiratory syncytial virus (RSV) Infects CD4+ T cells: frequency of circulating CD4+ RSV+ T cells as a marker of disease severity in young children. J Infect Dis. 2017;215(7):1049–1058.
51. Jozwik A, Habibi MS, Paras A, et al. RSV-specific airway resident memory CD8+ T cells and differential disease severity after experimental human infection. Nat Commun. 2015;6(1):10224.
52. Rivera-Toledo E, Gómez B. Respiratory syncytial virus persistence in macrophages alters the profile of cellular gene expression. Viruses. 2012;4(12):3270–3280.
53. González PA, Prado CE, Leiva ED, et al. Respiratory syncytial virus impairs T cell activation by preventing synapse assembly with dendritic cells. Proc Nat Acad Sci. 2008;105(39):14999–15004.
54. Blanco JCG, Boukhvalova MS, Morrison TG, Vogel SN. A multifaceted approach to RSV vaccination. Hum Vaccin Immunother. 2018;14(7):1734–1745.
55. Chin J, Magoffin RL, Shearer LA, Schieble JH, Lennette EH. Field evaluation of a respiratory syncytial virus vaccine and a trivalent parainfluenza virus vaccine in a pediatric population. Am J Epidemiol. 1969;89(4):449–463.
56. Polack FP, Alvarez-Paggi D, Libster R, et al. Fatal enhanced respiratory syncytial virus disease in toddlers. Sci Transl Med. 2021;13(616):eabj7843.
57. Delgado MF, Coviello S, Monsalvo AC, et al. Lack of antibody affinity maturation due to poor Toll-like receptor stimulation leads to enhanced respiratory syncytial virus disease. Nat Med. 2009;15(1):34–41.
58. Polack FP, Teng MN, Collins L, et al. A role for immune complexes in enhanced respiratory syncytial virus disease. J Exp Med. 2002;196(6):859–865.
59. Graham BS, Henderson GS, Tang YW, Lu X, Neuzil KM, Colley DG. Priming immunization determines T helper cytokine mRNA expression patterns in lungs of mice challenged with respiratory syncytial virus. J Immunol. 1993;151(4):2032–2040.
60. Tripp RA, Power UF. Original antigenic sin and respiratory syncytial virus vaccines. Vaccines. 2019;7(3):107.
61. RSV vaccine and mAb snapshot; 2022. Available from: https://www.path.org/resources/rsv-vaccine-and-mab-snapshot/.
62. Wheeler SM, Dotters-Katz S, Heine RP, Grotegut CA, Swamy GK. Maternal effects of respiratory syncytial virus infection during pregnancy. Emerg Infect Dis. 2015;21(11):1951–1955.
63. Aranda SS, Polack FP. Prevention of pediatric respiratory syncytial virus lower respiratory tract illness: perspectives for the next decade. Front Immunol. 2019;10:3.
64. Steinhoff MC, Omer SB, Roy E, et al. Neonatal outcomes after influenza immunization during pregnancy: a randomized controlled trial. CMAJ. 2012;184(6):645–653.
65. Brady MT, Byington CL; Committee On Infectious Diseases And Bronchiolitis Guidelines Committee. Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection. Pediatrics. 2014;134(2):415–420.
66. Ofman G, Pradarelli B, Caballero MT, et al. Respiratory failure and death in vulnerable premature children with lower respiratory tract illness. J Infect Dis. 2020;2020:5.
67. Sadoff J, De Paepe E, DeVincenzo J, et al. Prevention of respiratory syncytial virus infection in healthy adults by a single immunization of Ad26.RSV.preF in a human challenge study. J Infect Dis. 2022;226(3):396–406.
68. Simões EAF, Center KJ, Tita ATN, et al. Prefusion F protein–based respiratory syncytial virus immunization in pregnancy. N Eng J Med. 2022;386(17):1615–1626.
69. GSK. GSK presents positive clinical data on maternal and older adults RSV candidate vaccines; 2022. Available from: https://www.gsk.com/en-gb/media/press-releases/gsk-presents-positive-clinical-data-on-maternal-and-older-adults-rsv-candidate-vaccines/.
70. Hammitt LL, Dagan R, Yuan Y, et al. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N Eng J Med. 2022;386(9):837–846.
71. Maas BM, Lommerse J, Plock N, et al. Forward and reverse translational approaches to predict efficacy of neutralizing respiratory syncytial virus (RSV) antibody prophylaxis. eBioMedicine. 2021;73:6.
72. Thornhill EM, Salpor J, Verhoeven D. Respiratory syntycial virus: current treatment strategies and vaccine approaches. Antivir Chem Chemother. 2020;28:2040206620947303.
73. Kalergis AM, Soto JA, Gálvez NMS, et al. Pharmacological management of human respiratory syncytial virus infection. Expert Opin Pharmacother. 2020;21(18):2293–2303.
74. Chiou H-E, Liu C-L, Buttrey MJ, et al. Adverse effects of ribavirin and outcome in severe acute respiratory syndrome: experience in two medical centers. Chest. 2005;128(1):263–272.
75. Tejada S, Martinez-Reviejo R, Karakoc HN, Peña-López Y, Manuel O, Rello J. Ribavirin for treatment of subjects with respiratory syncytial virus-related infection: a systematic review and meta-analysis. Adv Ther. 2022;39(9):4037–4051.
76. Shang Z, Tan S, Ma D. Respiratory syncytial virus: from pathogenesis to potential therapeutic strategies. Int J Biol Sci. 2021;17(14):4073–4091.
77. Beigel JH, Nam HH, Adams PL, et al. Advances in respiratory virus therapeutics – a meeting report from the 6th isirv Antiviral group conference. Antiviral Res. 2019;167:45–67.
78. Bergeron HC, Tripp RA. Emerging small and large molecule therapeutics for respiratory syncytial virus. Expert Opin Investig Drugs. 2020;29(3):285–294.
79. DeVincenzo JP, Whitley RJ, Mackman RL, et al. Oral GS-5806 activity in a respiratory syncytial virus challenge study. N Engl J Med. 2014;371(8):711–722.
80. Gottlieb J, Torres F, Haddad T, et al. A phase 2b randomized controlled trial of presatovir, an Oral RSV fusion inhibitor, for the treatment of Respiratory Syncytial Virus (RSV) in lung transplant (LT) recipients. J Heart Lung Transplant. 2018;37(4):S155.
81. Chemaly RF, Dadwal SS, Bergeron A, et al. A phase 2, randomized, double-blind, placebo-controlled trial of presatovir for the treatment of respiratory syncytial virus upper respiratory tract infection in hematopoietic-cell transplant recipients. Clin Infect Dis. 2020;71(11):2777–2786.
82. Stevens M, Rusch S, DeVincenzo J, et al. Antiviral activity of oral JNJ-53718678 in healthy adult volunteers challenged with respiratory syncytial virus: a placebo-controlled study. J Infect Dis. 2018;218(5):748–756.
83. Martinón-Torres F, Rusch S, Huntjens D, et al. Pharmacokinetics, safety, and antiviral effects of multiple doses of the Respiratory Syncytial Virus (RSV) fusion protein inhibitor, JNJ-53718678, in infants hospitalized with RSV infection: a randomized phase 1b study. Clin Infect Dis. 2020;71(10):e594–603.
84. DeVincenzo J, Tait D, Efthimiou J, et al. A randomized, placebo-controlled, respiratory syncytial virus human challenge study of the antiviral efficacy, safety, and pharmacokinetics of RV521, an inhibitor of the RSV-F Protein. Antimicrob Agents Chemother. 2020;64(2):e01884–19.
85. Ahmad A, Eze K, Noulin N, et al. EDP-938, a respiratory syncytial virus inhibitor, in a human virus challenge. N Eng J Med. 2022;386(7):655–666.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.