Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Respiratory Interventions, Hospital Utilization, and Clinical Outcomes of Persons with COPD and COVID-19
Authors Elshafei AA ![]() , Flores SA, Kaur R
, Flores SA, Kaur R ![]() , Becker EA
, Becker EA ![]()
Received 16 September 2023
Accepted for publication 16 November 2023
Published 7 December 2023 Volume 2023:18 Pages 2925—2931
DOI https://doi.org/10.2147/COPD.S436228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Ahmad A Elshafei,1,2 Stephani A Flores,2 Ramandeep Kaur,3 Ellen A Becker3
1Department of Quality Operations & Population Health, Advocate Health, Green Bay, WI, USA; 2Department of Respiratory Care, Rush University Medical Center Chicago, IL, USA; 3Department of Cardiopulmonary Sciences, Rush University, Chicago, IL, USA
Correspondence: Ahmad A Elshafei, Department of Quality Operations & Population Health, Advocate Health, Green Bay, WI, USA, Email [email protected]
Purpose: Coronavirus disease 2019 (COVID-19) impacted outcomes of persons with chronic respiratory diseases such as chronic obstructive pulmonary disease (COPD). This study investigated the differences in respiratory interventions, hospital utilization, smoking status, and 30-day readmission in those with COPD and COVID-19 based on hospital survival status.
Methods: A retrospective cross-sectional study was conducted from February 2020 to October 2020 and included persons with COPD and COVID-19 infection. We examined respiratory interventions, hospital utilization and outcomes, and 30-day hospital readmission. Chi-square test analysis was used to assess categorical variables, and t-test or Mann–Whitney was used to analyze continuous data based on normality.
Results: Ninety persons were included in the study, 78 (87%) were survivors. The most common comorbidity was hypertension 71 (78.9%) (p = 0.003). Twenty-two (24%) persons were intubated, from whom 12 (15%) survived (p < 0.001). There were 25 (32.1%) and 12 (100%), (p < 0.001) persons who required an ICU admission from the survivor and non-survivor groups, respectively. Among the survivor group, fifteen (19%) persons required 30-day hospital readmission.
Conclusion: Persons with COPD and COVID-19 had a lower mortality rate (13%) compared to other studies in the early pandemic phase. Non-survivors had increased ICU utilization, endotracheal intubation, and more frequent application of volume control mode. Discharging survivors to long-term acute care facilities may reduce 30-day hospital readmissions.
Keywords: chronic obstructive pulmonary disease, COVID-19, COPD, respiratory interventions, hospital utilization, hospital readmission, comorbidities
Introduction
Coronavirus disease 2019 (COVID-19) is a respiratory infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Over 750 million persons have been infected with SARS-CoV-2 globally, of which more than six million died.1 Certain persons infected with COVID-19 had underlying respiratory diseases such as chronic obstructive pulmonary disease (COPD). COPD is a chronic inflammatory lung disease which causes defects in the airways and/or alveoli resulting in obstructed air flow and exhibits long-lasting respiratory symptoms.2 In 2015, the World Health Organization (WHO) estimated 65 million people were diagnosed with moderate-to-severe COPD and expected COPD to become the third leading cause of death worldwide by 2030.3 According to the Centers for Disease Control and Prevention (CDC), COPD is the foremost cause of death from lung disease, the sixth leading overall cause of death, and the third leading cause of hospital readmissions in the US.4 Although COPD primarily affects the lungs, significant systemic comorbidities may develop that worsen its severity.5 Persons who develop COPD exacerbations may require high needs for medical treatment and respiratory support leading to hospitalizations.6 There is no evidence demonstrating that having COPD creates a higher chance of contracting COVID-19, however evidence suggests that COPD could be associated with worse clinical outcomes in those with confounding COVID-19 pneumonia.7 Other risk factors for severe COVID-19 that are common in persons with COPD include older age, cardiovascular diseases, hypertension, and diabetes.8
Several studies explored how a COPD diagnosis affected COVID-19 outcomes. According to a meta-analysis, persons with COPD had a higher risk of low blood oxygen saturation if diagnosed with COVID-19.7 Moreover, those diagnosed with COPD and COVID-19 required advanced respiratory support compared with those without COPD. Examples of advanced respiratory support include high flow nasal cannula (HFNC), non-invasive positive pressure ventilation (NIPPV), and mechanical ventilation.6
Requiring advanced respiratory support because of acute respiratory failure often leads to an ICU admission and longer overall hospital length of stay.9 Those who recover from critical infections such as COVID-19 may also be at higher risk for additional hospital admissions. The severity of co-morbidities combined with (associated with) COVID-19 may also increase the risk of hospital readmission in the COPD population.10 In an Italian study, COPD was reported as a comorbidity in 16.4% of people who died and were infected with COVID-19.11 Although not specifically related to the COPD population, studies have reported hospital readmission data for persons infected with COVID-19. One study reported a 4.5% 30-day hospital readmission rate, while another study found a 19.9% 60-day readmission rate with 20% of the study sample dying during their readmission.12,13 Focusing on one-month and 6-month readmission, a recent study found 7.6% and 24% readmission rates, respectively.14
Along with COPD, smoking increases the severity of COVID-19.10,15 Two studies suggest that current smokers have impaired lung function making it more difficult to combat a COVID-19 infection.6,16 In a systematic review, persons with COVID-19 who had a 30-pack-year smoking history also had a 2.25 higher odds of requiring hospitalization.6 On the contrary, another study found that active smoking was not associated with severity of COPD. The increased risk for hospitalization could be related to higher comorbidity burden in the COPD population which may be further exacerbated by smoking. Moreover, current smokers and hospitalized patients who had COPD and COVID-19 were found to have a higher risk of severe respiratory symptoms (63%) and mortality (60%) compared to non-smokers.6 COPD was found to be an independent risk factor for death for those between 40 and 79 years of age who were hospitalized with COVID-19.17 Additionally, compared with those who have never smoked, the chances of dying in those who smoked more than 30-pack-years were 1.89 times higher after being infected with COVID-19.16
Pre-existing COPD worsens the prognosis from COVID-19. However, little is known about how COVID-19 impacts respiratory interventions and hospital utilization in persons with COPD. As a result, we aimed to investigate the differences in respiratory interventions, hospital utilization, smoking status, and 30-day readmission in persons with COPD and COVID-19 based on hospital survival status.
Methods
A retrospective observational cross-sectional study was conducted from February 1, 2020, to October 21, 2020, at a large Midwestern academic medical center in the US. Institutional review board approved the study protocol. Informed consent of persons to review their medical records was not required by the IRB as the study was classified as secondary research where no contact between investigators and study participants was allowed. The study is considered to be exempt from the Common Rule per section §46.104 of the Code of Federal Regulations. This study was conducted in accordance with the tenets of the Declaration of Helsinki. Participants’ data confidentiality was maintained throughout all study phases. Inclusion criteria were persons age >18 years old; COPD, emphysema, or chronic bronchitis diagnosis based on ICD-10 codes; and COVID-19 pneumonia. Primary study outcomes included identifying the types and frequency of respiratory interventions, hospital utilization, and outcomes in persons diagnosed with COPD and COVID-19 based on their hospital survival status. A secondary outcome included persons’ 30-day hospital readmission status.
Data collected from the electronic medical record system included demographic variables, respiratory interventions used, hospital utilization, therapies at discharge, mortality rates, and hospital readmission status. Variables included pre-admission pulmonary function tests (PFTs), age, comorbidities (hypertension, diabetes, obesity), gender, smoking status, and hospital readmission status. Respiratory interventions included pre-admission oxygen device (oxygen device interface and liter flow of oxygen) and the number of days persons required the following therapies: prone and self-prone sessions, short-acting beta agonist (SABA), and long-acting muscarinic antagonist (LAMA). Data on pre-intubation therapies included use of nasal cannula, high flow nasal cannula (HFNC), NIPPV, and high flow, high humidity oxygen therapy (HFHHOT). Assisted ventilation data included intubation, hours of mechanical ventilation, and ventilator mode(s) within the first 24 hours. Measures for hospital utilization were ICU length of stay and total hospital length of stay. Therapies needed at discharge were recorded for mechanical ventilation and oxygen therapy. Descriptive statistics were reported for all variables. Chi-square test compared hospital survival status for categorical variables, and t-test or Mann–Whitney analyzed continuous data based on normality. A p value threshold of 0.05 was used to determine statistical significance and data analysis was performed using SPSS 26.0 (SPSS Inc, Chicago, IL, USA)
Results
A total of 90 persons with COVID-19 and COPD diagnosis were included in the study, of which 17 (19%) persons had COPD confirmed by spirometry (see Table 1). There were 33 men and 57 women included, with an overall mean age of 70 years. Hypertension was the most common comorbidity. A total of 78 (87%) persons survived at hospital discharge. Smoking status did not differ between survivors and non-survivors.
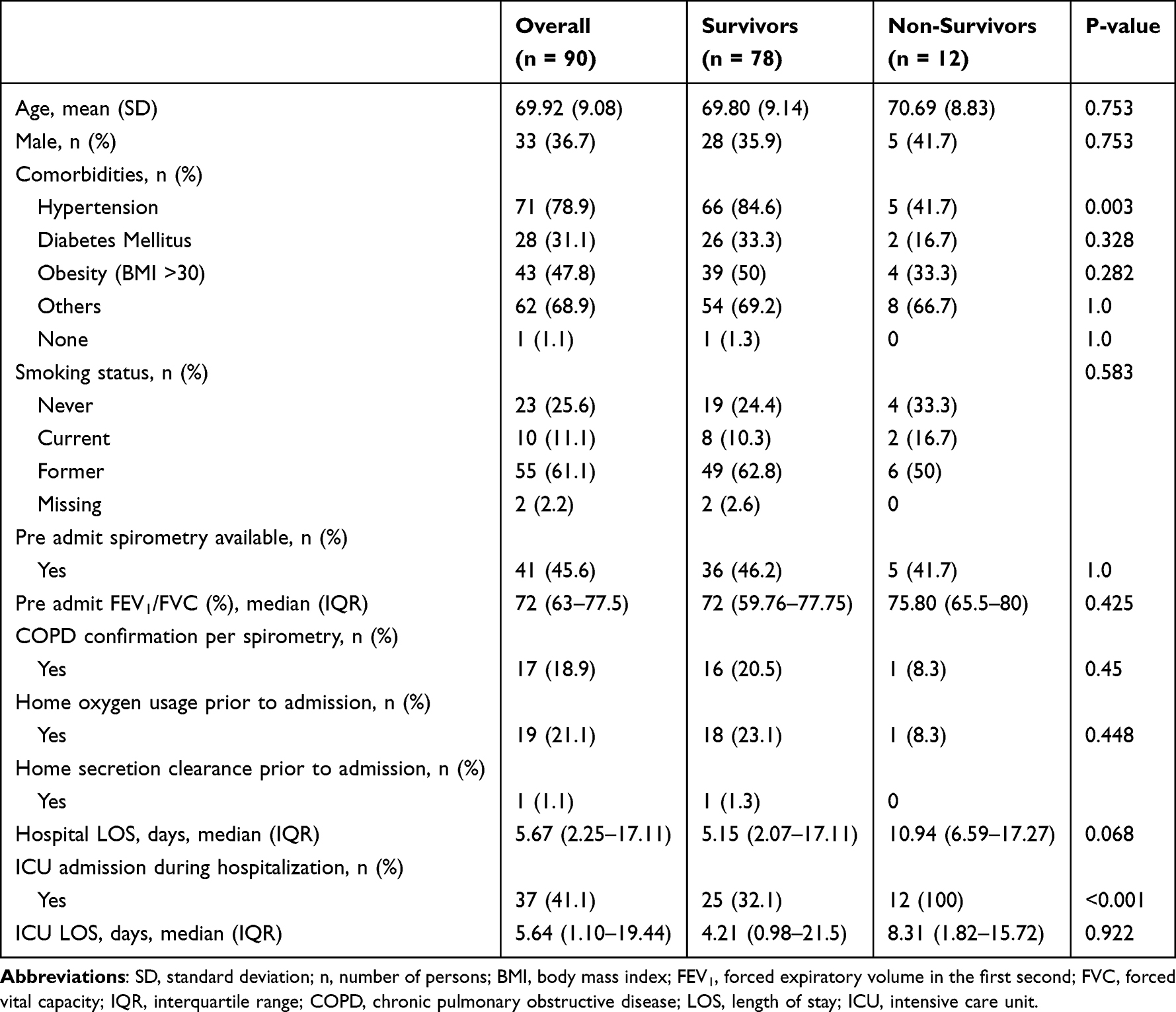 |
Table 1 Descriptive Statistics and Outcomes of Survivors versus Non-Survivors |
Overall, intubation was performed in 22 (24%) persons and non-survivor group had higher intubation rate when compared to the survivor group (83.3% vs 15.4%; p < 0.001). The non-survivor group had a higher use of the volume control mechanical ventilation mode when compared to the survivor group [4 (33.3%) vs 2 (2.6%), p = 0.002]. Other respiratory support did not affect survival status: 15 (17%) required pre-intubation HFNC 11 (12%) required manual prone therapy with a median of 2 prone sessions, while 8 (9%) underwent self-prone therapy (see Table 2). The non-survivor group had higher ICU admission rate when compared to the survivors (100% vs 32.1%; p < 0.001). Length of mechanical ventilation, ICU stay, or hospital stay did not significantly differ between the two study groups. Among the survivors, 15 (19.2%) persons had a 30-day hospital readmission during the study period. However, there were no significant differences in the use of respiratory interventions, hospital utilization, and patient outcomes among those who were readmitted compared to those without 30-day readmission (see Table 3).
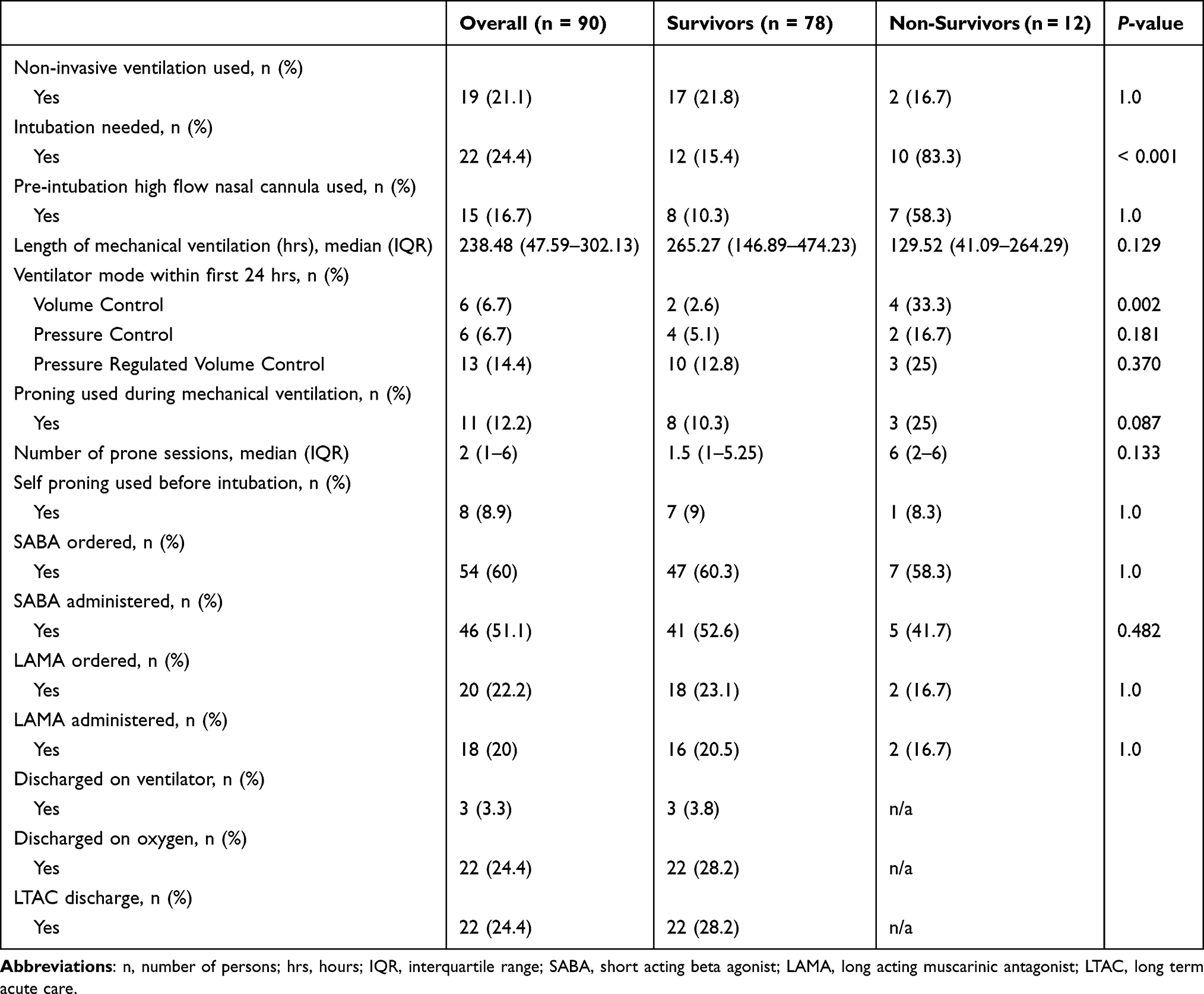 |
Table 2 Study Outcomes and Survival Status |
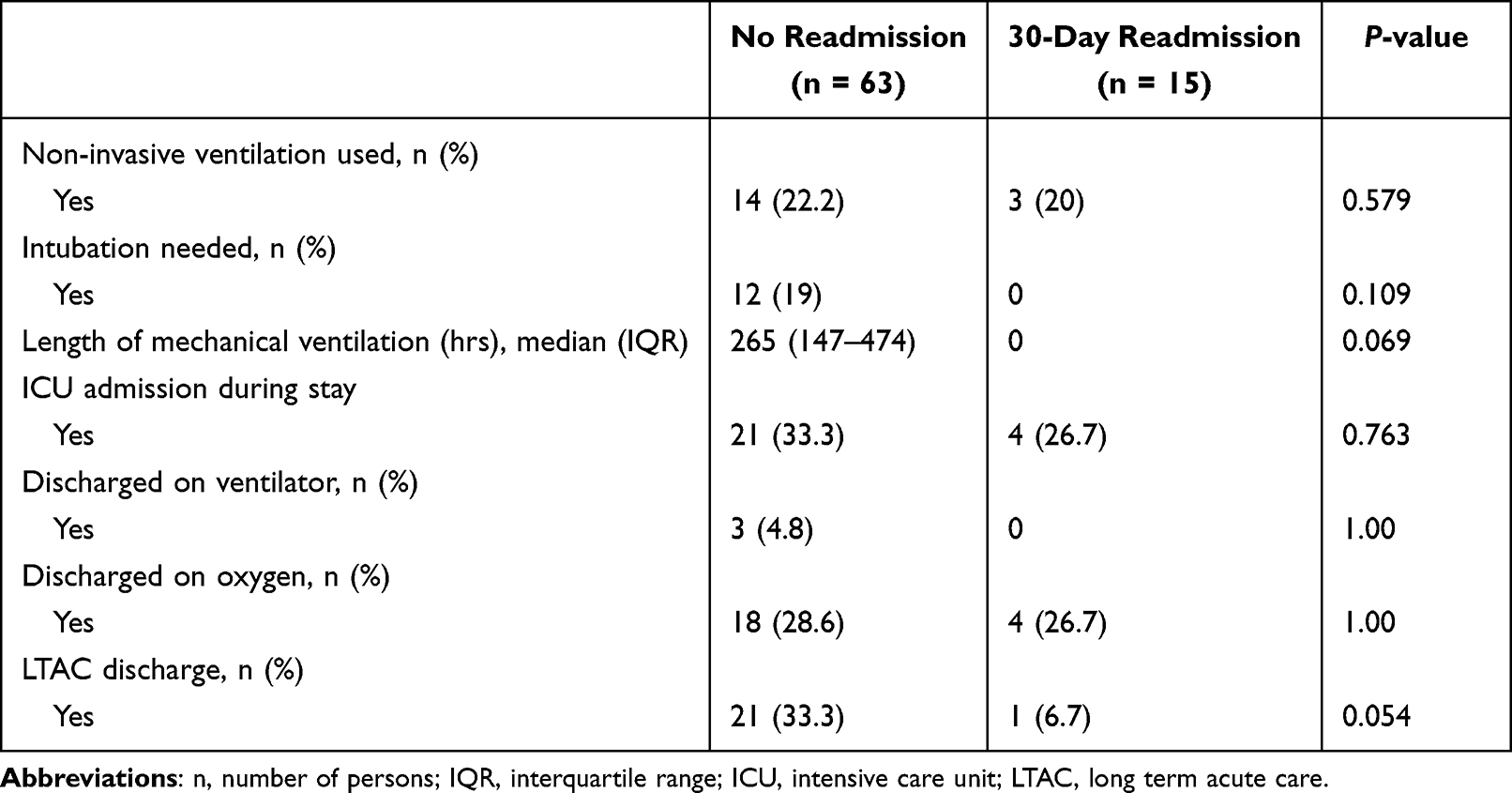 |
Table 3 Study Outcomes Based on 30-Day Readmission Status Amongst Survivors |
Discussion
This retrospective observational study of persons hospitalized with COVID-19 and pre-existing COPD found an 87% survival rate. The 13% mortality rate was similar to an Italian study that was conducted around the early phase of the pandemic which reported a 16.4% mortality rate.14 Hypertension was the most common comorbidity among our study sample with higher rate among the survivor group. This differed from other studies that found comorbid disease is associated with worse outcomes in persons with COVID-19; specifically,hypertension,diabetes,and heart disease have shown to increase the risk of hospitalization and death.14,18
All non-survivors required an ICU admission and the persons who were admitted to the ICU required higher levels of respiratory support. Similar studies reported ICU admission rates of 4% in Italy, 33% in Seattle, and 38% in Spain19, compared to our study’s ICU admission rate which was 41%.20,21 Moreover, 19% of the survivors in our study had a 30-day hospital readmission. This was consistent with the ranges for standalone COPD and COVID-19 related 30-day readmission rates. There is no literature examining 30-day hospital readmission status of persons with COPD and COVID-19. However, a systematic review and meta-analysis of nearly four million persons with COPD and without COVID-19 infection found a 30-day all-cause hospital readmission rate range of 9% to 26%.22 In the early phase of the COVID pandemic, Yeo et al reported a lower 30-day hospital readmission rate of 4.5% for persons with COVID-19 and 20% of their study sample died during their readmission.11 A systematic review included 13 studies with persons with COVID-19 found a 30-day hospital readmission range of 4.2% to 19.9%.23 COPD diagnosis and other comorbidity burden specifically hypertension, obesity, and smoking history are risk factors for hospital readmission. Several studies have reported unfavorable outcomes including readmission in persons with COPD who have comorbid diseases.24–26 To our knowledge, our study is the first to report 30-day hospital readmission data related to persons with COVID-19 and COPD.
Among survivors, higher intubation rate (19% vs 0%) and ICU admission (33.3% vs 26.7%) was noted in those who did not have 30-day readmission. One factor which may have affected these outcomes is that approximately 33% of those who did not have a 30-day readmission were discharged to a long-term acute care hospital which may have prevented this group from getting readmitted to the hospital. It is also understood that invasive mechanical ventilation has been associated with higher mortality in persons with COVID-19.27,28 It could also be that the persons in our study may have received rapid and earlier higher level of hospital care which led to preventing further clinical deterioration and a more favorable overall health outcome.
Prior home oxygen use was evident in the survivor group, and there is strong literature support demonstrating survival benefits in persons with COPD who utilized long-term oxygen therapy.29 The administration of short- and long-acting bronchodilator therapy during the hospital stay of the survivor and non-survivor groups did not have a significant impact on mortality rate and hospital respiratory utilization. This study’s findings were from the early phase of the pandemic in the US when there were variations in practices related to utilizing of high-level respiratory support such as invasive mechanical ventilation, NIPPV, and HFNC.14,28
Our study’s limitations include using retrospective data from a single academic center in the Midwestern US and a small sample size. A relatively small sample could have been due to pandemic-related infection control safety measures, such as social distancing and minimal crowd mixing as some persons with COPD had less exacerbations due to reduction of respiratory viral infections, avoided contracting COVID-19, or they were not diagnosed. Alqahtani et al (2021) reported a 50% reduction in admissions for COPD exacerbation during the pandemic period versus pre-pandemic.30 Another limitation is that only 19% of the study sample had a spirometry confirmed COPD diagnosis and the rest of the sample inclusion was based on physician ICD-10 diagnosis that is based on imaging results or other clinical factors. It is established that COPD may be inaccurately diagnosed in up to a third of hospitalized patients.31 Finally, it is possible that there was a confounding association of other risk factors for severe COVID-19 that are common in persons with COPD, such as older age, cardiovascular diseases, obesity, and diabetes that lead to increased hospital resource utilization, lower survival, and higher hospital readmission rates.8 Moreover, other vital social determinants of health such socioeconomic status and healthcare access were not considered in the study.
Conclusion
This study demonstrated that persons with COPD who were hospitalized with COVID-19 had a lower mortality rate compared to other studies conducted in the early phase of the pandemic. Non-survivors had increased ICU utilization and endotracheal intubation compared to survivors, therefore, allocating rapid and earlier hospital care could prevent clinical deterioration and the need for higher levels of care and perhaps. Moreover, non-survivors had more frequent application of volume control mode. Discharging survivors to LTACs may reduce 30-day readmissions. Further research into the effects of specific respiratory interventions and hospital utilization measures on improving the outcomes of persons with COPD in the setting of viral infections is warranted, especially in different demographic areas while enrolling larger samples with diverse COPD phenotypes.
Abbreviations
COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; COPD, chronic obstructive pulmonary disease; WHO, World Health Organization; CDC, Centers for Disease Control and Prevention; ICD, International classification of Diseases; PFT, pulmonary function tests; SABA, short-acting beta agonist; LAMA, long-acting muscarinic antagonist; HFNC, high flow nasal cannula; NIPPV, non-invasive positive pressure ventilation; ICU, Intensive care unit.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
None of the authors report any financial compensation, financial relationships, intellectual properties, or any other relationships that are relevant to this manuscript or that could have affected its composition.
References
1. World Health Organisation. COVID Data Tracker. WHO Coronavirus (COVID-19)Dashboard; 2022. Aailable from: https://covid19.who.int/.
2. 2023 GOLD Report Global Initiative for Chronic Obstructive Lung Disease - GOLD; 2022. Available fom: https://goldcopd.org/2023-gold-report-2/.
3. World Health Organization (WHO), COPD; 2015. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-copd.
4. FastStats. Centers for Disease Control and Prevention (2020); 2022. Available from: https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm.
5. Anzueto A. Impact of exacerbations on COPD. Eur Respir Rev. 2010;19(116):113–118. doi:10.1183/09059180.00002610
6. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Prevalence, severity and mortality associated with COPD and smoking in patients with covid-19: a rapid systematic review and meta-analysis. PLoS One. 2020;15(5):e0233147. doi:10.1371/journal.pone.0233147
7. Gerayeli FV, Milne S, Cheung C, et al. COPD and the risk of poor outcomes in COVID-19: a systematic review and meta-analysis. EClinicalMedicine. 2021;33:
8. Zaki N, Alashwal H, Ibrahim S. Association of Hypertension, diabetes, stroke, cancer, kidney disease, and high-cholesterol with covid-19 disease severity and fatality: a systematic review. Diabetes Metab Syndr. 2020;14(5):1133–1142. doi:10.1016/j.dsx.2020.07.005
9. Ouyang L, Yu M, Zhu Y, Gong J. Respiratory supports of COVID-19 patients in intensive care unit: a systematic review. Heliyon. 2021;7(4):e06813. doi:10.1016/j.heliyon.2021.e06813
10. Donnelly JP, Wang XQ, Iwashyna TJ, Prescott HC. Readmission and death after initial hospital discharge among patients with covid-19 in a large multihospital system. JAMA. 2021;325(3):304–306. doi:10.1001/jama.2020.21465
11. Yeo I, Baek S, Kim J, et al. Assessment of thirty-day readmission rate, timing, causes and predictors after hospitalization with COVID-19. J Intern Med. 2021;290(1):157–165. doi:10.1111/joim.13241
12. Guarin G, Lo KB, Bhargav R, et al. Factors associated with hospital readmissions among patients with COVID-19: a single-center experience. J Med Virol. 2021;93(9):5582–5587. doi:10.1002/jmv.27104
13. Nematshahi M, Soroosh D, Neamatshahi M, Attarian F, Rahimi F. Factors predicting readmission in patients with COVID-19. BMC Res Notes. 2021;14(1):374. doi:10.1186/s13104-021-05782-7
14. Marron RM, Zheng M, Fernandez Romero G, et al. Impact of chronic obstructive pulmonary disease and emphysema on outcomes of hospitalized patients with coronavirus disease 2019 pneumonia. J COPD Fdn. 2021;8(2):255–268. doi:10.15326/jcopdf.2020.0200
15. Zhao Q, Meng M, Kumar R, et al. The impact of COPD and smoking history on the severity of COVID‐19: a systemic review and meta‐analysis. J Med Virol. 2020;92(10):1915–1921. doi:10.1002/jmv.25889
16. Lowe KE, Zein J, Hatipoğlu U, Attaway A. Association of smoking and cumulative pack-year exposure with covid-19 outcomes in the Cleveland Clinic covid-19 registry. JAMA Intern Med. 2021;181(5):709–711. doi:10.1001/jamainternmed.2020.8360
17. Puebla Neira DA, Watts A, Seashore J, et al. Outcomes of patients with COPD hospitalized for coronavirus disease 2019. J COPD Fdn. 2021;8(4):517–527. doi:10.15326/jcopdf.2021.0245
18. Richardson S, Hirsch JS, Narasimhan M, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323(20):2052–2059. doi:10.1001/jama.2020.677
19. Leung JM, Niikura M, Yang CWT, Sin DD. COVID-19 and COPD. Eur Respir J. 2020;56(2):10.1183/13993003.02108–2020.
20. Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323(16). doi:10.1001/jama.2020.5394
21. Bhatraju PK, Ghassemieh BJ, Nichols M, et al. Covid-19 in critically ill patients in the Seattle region - case series. N Engl J Med 2020; 382:2012–2022.
22. Alqahtani JS, Njoku CM, Bereznicki B, et al. Risk factors for all-cause hospital readmission following exacerbation of COPD: a systematic review and meta-analysis. Eur Respir Rev. 2020;29(156):190166. doi:10.1183/16000617.0166-2019
23. Loo WK, Hasikin K, Suhaimi A, et al. Systematic review on covid-19 readmission and risk factors: future of machine learning in COVID-19 readmission studies. Front Public Health. 2022;10:898254. PMID: 35677770; PMCID: PMC9168237. doi:10.3389/fpubh.2022.898254
24. Bellou V, Belbasis L, Konstantinidis AK, Tzoulaki I, Evangelou E. Prognostic models for outcome prediction in patients with chronic obstructive pulmonary disease: systematic review and critical appraisal. BMJ. 2019;l5358. doi:10.1136/bmj.l5358
25. McFerrin C, Raza SJ, May A, Davaro F, Siddiqui S, Hamilton Z. Charlson comorbidity score is associated with readmission to the index operative hospital after radical cystectomy and correlates with 90-day mortality risk. Int Urol Nephrol. 2019;51(10):1755–1762. doi:10.1007/s11255-019-02247-6
26. Moore BJ, White S, Washington R, Coenen N, Elixhauser A. Identifying increased risk of readmission and in-hospital mortality using hospital administrative data: the AHRQ Elixhauser Comorbidity Index. Medical Care. 2017;55(7):698–705. doi:10.1097/MLR.0000000000000735
27. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single centered, retrospective, observational study. Lancet Respir Med. 2020;8(5):475–481. doi:10.1016/S2213-2600(20)30079-5
28. Tobin MJ, Laghi F, Jubran A. Caution about early intubation and mechanical ventilation in COVID-19. Ann Intensive Care. 2020;10(1):78. doi:10.1186/s13613-020-00692-6
29. Lacasse Y, Tan AM, Maltais F, Krishnan JA, Krishnan, J. A. Home oxygen in chronic obstructive pulmonary disease. American. J Respi Critic Care Med. 2018;197(10):1254–1264. doi:10.1164/rccm.201802-0382ci
30. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Reduction in hospitalised COPD exacerbations during COVID-19: a systematic review and meta-analysis. PLoS One. 2021;16(8):e0255659. doi:10.1371/journal.pone.0255659
31. Spero K, Khorfan F, Bayasi G, Spero K, Khorfan F, Bayasi G. The over diagnosis of COPD in hospitalized patients. Chest. 2016;150(4):921A. doi:10.1016/j.chest.2016.08.1021
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.