Back to Journals » Nature and Science of Sleep » Volume 17

Respiratory Arousal Threshold in Patients with Epilepsy and Obstructive Sleep Apnea
Authors Liao TW ![]() , Chang CW, Cheng MY, Wu T, Chen NH, Lin SW
, Chang CW, Cheng MY, Wu T, Chen NH, Lin SW ![]() , Chuang LP
, Chuang LP ![]()
Received 22 April 2025
Accepted for publication 26 July 2025
Published 8 August 2025 Volume 2025:17 Pages 1825—1836
DOI https://doi.org/10.2147/NSS.S535940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Ting-Wei Liao,1 Chun-Wei Chang,2 Mei-Yun Cheng,2,3 Tony Wu,1,4 Ning-Hung Chen,5– 7 Shih-Wei Lin,5,6 Li-Pang Chuang5,6,8
1Department of Neurology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan; 2Section of Epilepsy, Department of Neurology, Chang Gung Memorial Hospital Linkou Medical Center, and Chang Gung University College of Medicine, Taoyuan, Taiwan; 3Department of Medical Science, National Tsing Hua University, Hsinchu, Taiwan; 4Department of Neurology, New Taipei Municipal Tucheng Hospital, New Taipei City, Taiwan; 5Department of Pulmonary and Critical Care Medicine, Sleep Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan; 6Department of Respiratory Therapy, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan; 7School of Traditional Chinese Medicine, Chang Gung University, Taoyuan, Taiwan; 8School of Medicine, Chang Gung University, Taoyuan, Taiwan
Correspondence: Li-Pang Chuang, Sleep Center, Department of Pulmonary and Critical Care Medicine, Chang Gung Memorial Hospital, Linkou Medical Center, No. 5, Fusing St., Guishan Dist., Taoyuan, 333, Taiwan, Tel +886-3-3196200 EXT 2680, Email [email protected]
Background: Patients with epilepsy (PWE) have a higher likelihood of developing obstructive sleep apnea (OSA). However, limited literature investigates the phenotypes of OSA in this population. This study aimed to evaluate the respiratory arousal threshold (rAT) in PWE with concurrent OSA.
Methods: Patients were recruited from the Sleep and Epilepsy Center at Chang Gung Memorial Hospital between January 2010 and June 2022. We included adult patients who underwent overnight in-laboratory polysomnography after the onset of epilepsy. Additionally, age-, sex-, and apnea-hypopnea index (AHI)-matched patients with OSA only were included as controls. Low rAT was defined using predictive models based on polysomnography criteria.
Results: We enrolled 48 PWE, of whom 36 (75%) had concurrent OSA (PWE+OSA), and 108 patients with OSA only. PWE+OSA were older upon PSG examination and had a later epilepsy onset compared to PWE only. PWE had more concomitant antiseizure medications and hypnotics compared to patients with OSA only. Among those with OSA, 19 (52.8%) with PWE+OSA and 68 (63.0%) with OSA only were predicted to have a low rAT. Continuous positive airway pressure compliance was significantly lower in the low rAT subgroup compared to the high rAT subgroup (p = 0.021) within the OSA-only group, whereas no significant difference was observed between rAT subgroups in the PWE+OSA group.
Conclusion: Our study provides insights into the presence of a low rAT in PWE+OSA, with no significant difference in its ratio compared to OSA controls. However, since rAT was estimated using a predictive model rather than direct measurement, this limitation may affect the interpretation of our findings. Further studies using gold-standard methods are needed to clarify the underlying mechanisms contributing to the higher OSA prevalence in PWE.
Keywords: epilepsy, obstructive sleep apnea, respiratory arousal threshold, continuous positive airway pressure, CPAP compliance
Introduction
Obstructive sleep apnea (OSA) frequently coexists as a comorbidity in patients with epilepsy (PWE). According to a meta-analysis, the prevalence of OSA in PWE was estimated to be 33.4%, with moderate-to-severe OSA, defined as an apnea-hypopnea index (AHI) of ≥15, observed in 9.7% of PWE.1 Several risk factors have been identified for the concurrent occurrence of OSA in PWE, including older age, male gender, and higher seizure frequency.2
The occurrence of apnea-associated arousal or hypoxemia in OSA can result in sleep fragmentation and chronic sleep loss, which may have a detrimental impact on seizure frequency.3 There is an association between OSA and refractory epilepsy, particularly concerning oxygen desaturation during sleep.4 PWE who have comorbid OSA are more prone to experiencing seizures during sleep.5 Additionally, the emergence of OSA symptoms often coincides with an increase in seizure frequency or the onset of status epilepticus.6 Managing OSA can also contribute to the control of epilepsy, as continuous positive airway pressure (CPAP) therapy has been shown to reduce interictal epileptiform discharges in adults with epilepsy and OSA.7 PWE with OSA who receive CPAP treatment may exhibit improved seizure control compared to those who remain untreated.1 PWE with OSA who demonstrated good compliance with CPAP therapy also experienced a reduction in seizure frequency.8 Moreover, the higher risk of OSA in PWE is associated with poorer cognitive function and an elevated predicted risk of sudden unexpected death in epilepsy.9,10
In recent years, advancements in understanding the pathogenesis of OSA through upper airway and respiratory phenotyping techniques have revealed four primary causes of OSA.11 These phenotypes encompass 1. impaired anatomy, 2. impaired dilator muscle function asleep, 3. respiratory control instability (high loop gain), and 4. low respiratory arousal threshold (rAT).
Approximately 30% to 50% of OSA patients fall into the category of low rAT, meaning they awaken in response to small changes (> −15 cmH2O) in negative intrathoracic pressure.11 Several factors have been identified in relation to the low rAT, including a negative association with increasing body mass index (BMI) and the use of antihypertensive medications, while increasing age and antidepressant use have shown a positive association.12 A low rAT is also linked to reduced compliance with CPAP treatment over time.13 Consequently, in addition to standard CPAP therapy, targeted non-CPAP interventions aimed at addressing the impairments associated with each phenotypic trait are crucial.11 For instance, the use of non-myorelaxant hypnotics may be beneficial for patients with a low rAT.14–16
Because recognizing phenotypes in patients with OSA is gaining importance and the standard measurement of these phenotypic traits is not easily performed in clinical practice, point-of-care tools based on routine clinical sleep study metrics have been developed to estimate these OSA traits.17,18 For example, Edwards et al demonstrated that a simple clinical score can predict a low rAT using standard polysomnography (PSG) parameters.17 Points are assigned for each of the following criteria: an AHI score of <30 events per hour, nadir oxygen saturation measured by pulse oximetry > 82.5%, and the fraction of hypopneas (percentage of all respiratory events that were hypopneas) > 58.3%. A score of 2 or above predicted a low arousal threshold with a sensitivity of 80.4% and a specificity of 88.0%.
Sleep disturbances are a common occurrence in PWE, often characterized by sleep fragmentation and interruptions in sleep continuity.19,20 Studies have shown that individuals with generalized or focal epilepsy exhibit significantly higher indices of sleep stage transitions and arousal when compared to controls.20 Unlike patients with OSA, whose arousals are typically linked to mechanoreceptor and chemoreceptor activation due to airway narrowing, hypoxia, or hypercapnia, PWE may experience cortical arousals associated with both ictal and interictal epileptic activity.19 These frequent arousals can hinder the attainment of deeper and more stable sleep stages, limit the accumulation of respiratory stimuli required to activate the pharyngeal dilators, and perpetuate respiratory control instability through an excessive ventilatory response.11
Nonetheless, there is a paucity of literature investigating the distinct phenotypes of OSA in PWE. The potential synergistic negative impact on the arousal system in individuals coping with both epilepsy and OSA remains shrouded in uncertainty. As the exact cause of the increased prevalence of OSA in PWE remains unclear, we propose that disruptions in the arousal system, driven by both epileptic activity and disordered breathing, may play a critical role in the development of OSA in this population. Consequently, we have devised this retrospective study with two primary objectives: 1. To evaluate the clinical implications of OSA on PWE. 2. To predict the rAT in PWE and concurrent OSA.
Methods
Institutional Review
The study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (ethical license No: 202201433B0). The requirement for written informed consent was waived because all cases involved retrospective review of medical records related to routine clinical care, with no direct patient contact or intervention. All patient data were de-identified to ensure confidentiality, and the study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Patients
The participants for this study were recruited from the Sleep Center and Epilepsy Center at Chang Gung Memorial Hospital. The Sleep Center registry included patients who underwent various sleep studies (such as PSG, CPAP titration, or multiple sleep latency tests) at Chang Gung Memorial Hospital, specifically at the Taoyuan, Linkou or Taipei branch. The available data spanned from January 2010 to June 2022. The Epilepsy Center registry, on the other hand, consisted of patients diagnosed with epilepsy who received follow-up care at our institutes in Chang Gung Memorial Hospital, across the Taoyuan, Linkou, or Taipei branches. The data from this registry covered the period from November 2009 to August 2022. Our study included patients who were present in both registries and were aged 18 years or above. The medical charts were meticulously reviewed by an epileptologist (TW Liao), and the diagnosis was confirmed based on the definition of epilepsy established by the International League Against Epilepsy (ILAE).21
For the PSG data to be eligible for further analysis, it had to adhere to our standardized overnight in-laboratory PSG protocol, as described previously,22 and excluded studies conducted before epilepsy onset or after OSA-related surgery. In cases where a patient had undergone multiple PSG examinations, we selected the first eligible PSG study for further evaluation. The diagnosis of OSA was defined as an AHI of ≥5, categorized into mild OSA (AHI ≥ 5 to <15 events per hour of sleep), moderate OSA (AHI ≥ 15 to <30 events per hour), or severe OSA (AHI ≥ 30 events per hour).23 To predict the low rAT in patients with OSA, we utilized criteria from a previous study, requiring the presence of at least two of the following: AHI < 30/hour, nadir peripheral capillary oxygen saturation (SpO2) > 82.5%, or fraction of hypopneas > 30%.17
In summary, our inclusion criteria were as follows: (1) adult patients who met the diagnosis of epilepsy, and (2) had undergone an overnight in-laboratory PSG after the onset of epilepsy. Patients were excluded if (1) the diagnosis of epilepsy could not be confirmed, or (2) their PSG data did not meet the eligibility criteria for further analysis. The flow chart depicting patient inclusion is illustrated in Figure 1. Additionally, we enrolled age, sex, and AHI-matched patients with OSA only as controls, with a ratio of 1:3, for comparison with patients who have both epilepsy and OSA (PWE+OSA).
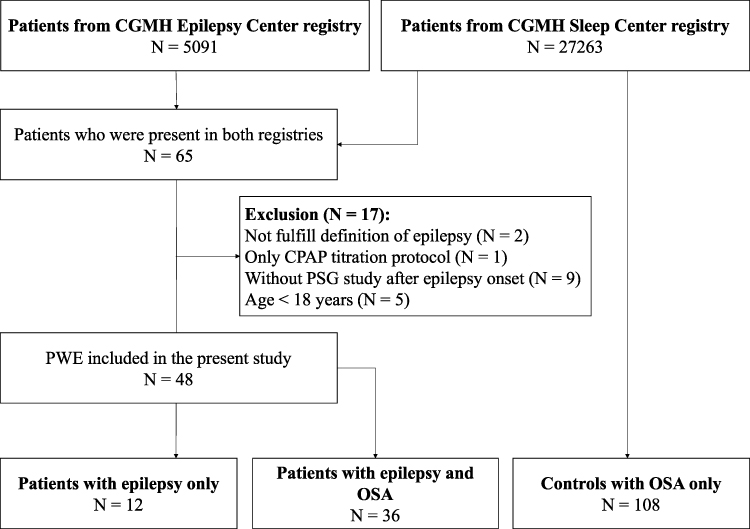 |
Figure 1 The flow chart depicting patient inclusion. Abbreviations: CGMH, Chang Gung Memorial Hospital; CPAP, continuous positive airway pressure; PSG, polysomnography; OSA, obstructive sleep apnea. |
We gathered essential demographic and clinical information, including the age at PSG examination, sex, body weight, BMI, neck circumference (NC), Epworth Sleepiness Scale (ESS) score,24 age of epilepsy onset, duration of epilepsy, epilepsy classification, etiology of epilepsy, seizure types, concomitant antiseizure medication (ASM), and concomitant use of hypnotics. Drug-resistant epilepsy was defined as the failure of adequate trials of two tolerated and appropriately chosen and used ASM regimens (either as monotherapy or in combination) to achieve sustained seizure freedom, in accordance with the criteria set by the ILAE.25 Active epilepsy was defined as ongoing treatment with ASMs and/or the occurrence of at least one seizure within the past year.26
Polysomnography
All patients underwent an overnight in-laboratory PSG following a standardized protocol.27 Sleep stages and associated events were scored based on the guidelines established by the American Academy of Sleep Medicine (AASM).27,28 Several parameters were recorded for further analysis and comparisons, including the AHI, AHI during the rapid eye movement (REM) sleep stage (AHI in R), apnea index (AI), desaturation index, sleep efficiency, sleep latency, REM sleep latency, arousal index, periodic leg movement during sleep (PLMS) index, snore index (SI), times of the longest apnea, mean SpO2, lowest SpO2, and duration of time with SpO2 below 85%.
No seizures were observed during the PSG recordings in any of the participants, and therefore no data were excluded on this basis.
Continuous Positive Airway Pressure Therapy
We retrieved automatic CPAP treatment data for the subjects from the Sleep Center registry. To ensure the validity of our analysis, we prioritized the initial CPAP treatment record following each eligible PSG study when available. The collected data encompassed CPAP compliance, the percentage of days with CPAP usage, the average number of hours used per day, and residual AHI. CPAP compliance was defined as the percentage of days in which CPAP was used for a minimum of four hours.29
Statistics
The statistical analysis was conducted using IBM SPSS Statistics, version 26 (IBM Corp., Armonk, NY, USA).
We compared demographic and clinical data among the PWE-only, PWE+OSA, and OSA-only groups. Additionally, we compared demographic and clinical data between low and high rAT subgroups within the PWE+OSA and OSA-only groups. PSG parameters were compared among five groups: PWE-only, PWE+OSA with low or high rAT, and OSA-only with low or high rAT. CPAP-related data were compared between low and high rAT subgroups within both the PWE+OSA and OSA-only groups. All key parameters necessary for grouping (eg, AHI, respiratory event classification, and CPAP compliance) were complete for all included patients. For other variables, cases with missing data were excluded from specific subgroup or correlation analyses without imputation.
Nominal variables, such as the male-to-female ratio, epilepsy classification, etiology of epilepsy, active seizure status, and drug-resistant epilepsy at the last visit, were assessed using Fisher’s exact test. Parametric variables, such as age at PSG examination, body weight, BMI, NC, ESS score, age of epilepsy onset, duration of epilepsy, and CPAP-related variables, were assessed using Student’s t-test (for two groups) or analysis of variance (ANOVA) (for multiple groups). Post hoc analysis following ANOVA was conducted using the Bonferroni correction.
Nonparametric variables, such as the number of concomitant ASMs, the number of concomitant hypnotics, and PSG parameters, were assessed using the Mann–Whitney U-test (for 2 groups) or the Kruskal–Wallis test (for multiple groups). Post hoc analysis following Kruskal–Wallis test was performed using the Bonferroni adjustment.
The threshold for statistical significance was set at p < 0.05 or adjusted p < 0.05 for all tests. Additionally, a post hoc power analysis was conducted for the comparison of the proportion of low rAT between the PWE+OSA group and the OSA-only group, using Fisher’s exact test.
Results
Table 1 presents a summary of the demographic and clinical data for the patients in our study. A total of 48 PWE and 108 patients with OSA only were included in this study. Among the PWE, 36 patients (75%) had concurrent OSA (PWE+OSA) (male/female: 30/6). PWE-only group were significantly younger at the time of PSG examination compared to PWE+OSA (adjusted p = 0.002) or OSA-only (adjusted p = 0.001) group. Compared to PWE-only group, PWE+OSA had an older age of epilepsy onset (32.2 ± 16.5 vs 16.3 ± 7.9, p < 0.001). OSA-only group had a lower number of concomitant ASMs, a lower number of concomitant hypnotics, and a lower total number of concomitant ASMs and hypnotics compared to PWE+OSA or PWE-only group.
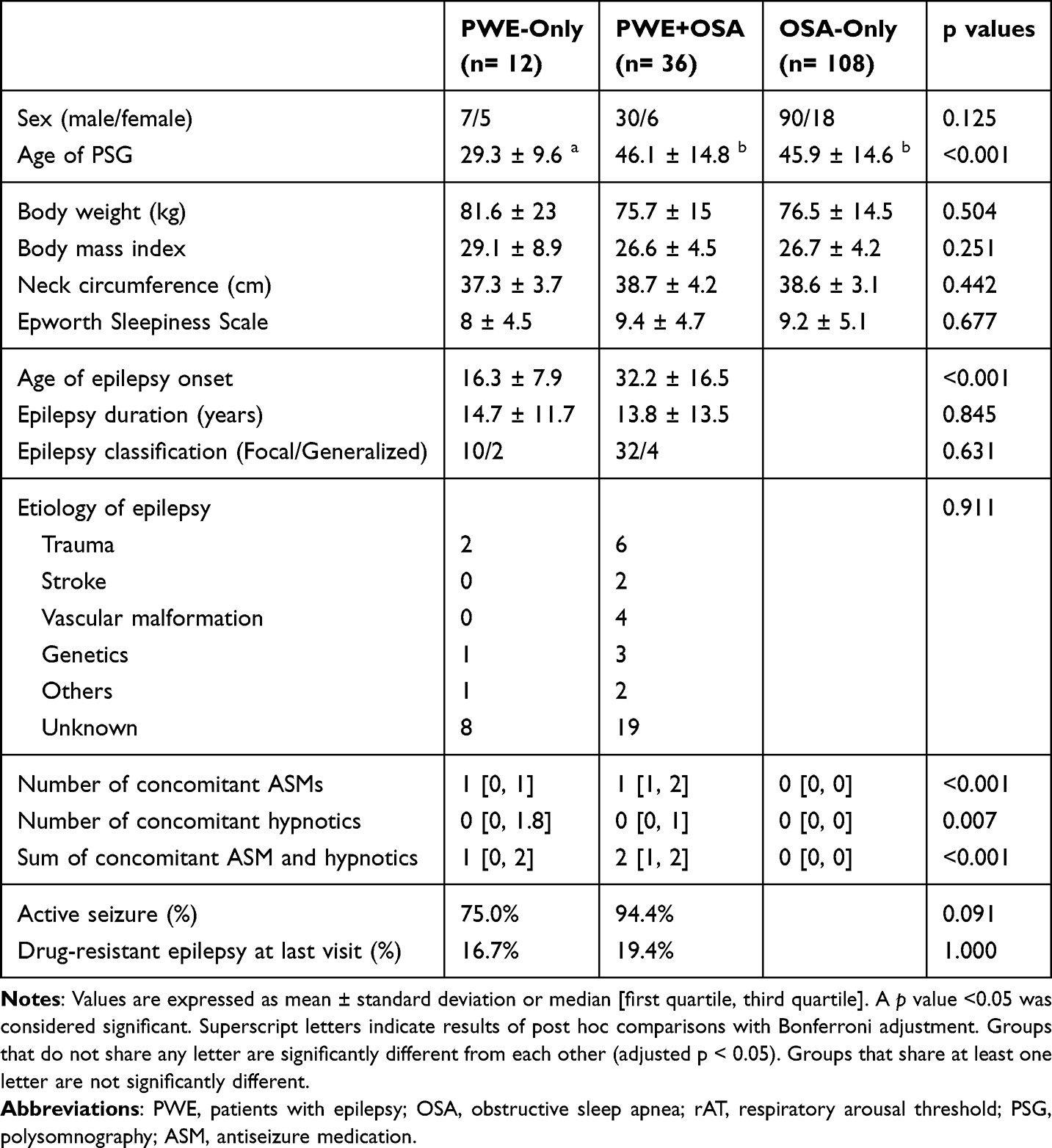 |
Table 1 Demographic and Clinical Data of the Enrolled Patients |
Table 2 presents a summary of the demographic and clinical data for the patients with OSA, categorized by predicted rAT status. Among the PWE+OSA group, 19 (52.8%) were predicted to have a low rAT. Among OSA-only group, 68 (63.0%) were predicted to have a low rAT. The ratio of low rAT did not differ significantly between these two groups (p = 0.327). Among OSA-only group, the low rAT subgroup had lower body weight (p = 0.005), lower BMI (p < 0.001), and lower NC (p = 0.005) compared to the high rAT subgroup. Among the PWE+OSA group, the low rAT subgroup showed a trend toward lower body weight (p = 0.255), lower BMI (p = 0.256), and lower NC (p = 0.124) compared to the high rAT subgroup, although these differences did not reach statistical significance. Compared to their OSA-only counterparts, both the low rAT and high rAT subgroups of PWE+OSA had significantly higher number of concomitant ASMs, a higher number of concomitant hypnotics, and a higher total number of concomitant ASMs and hypnotics.
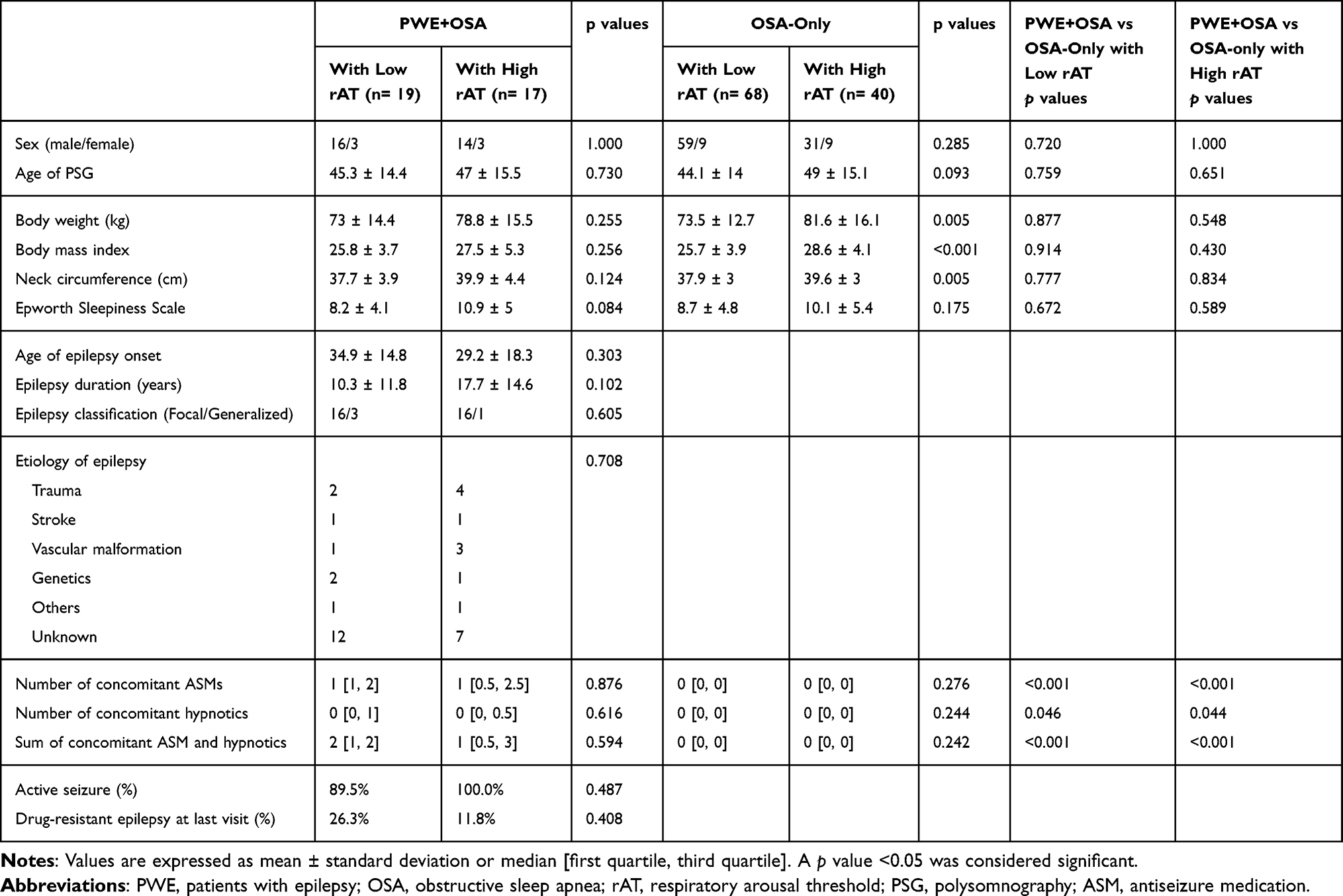 |
Table 2 Demographic and Clinical Data of the Patients with OSA |
Table 3 provides an overview of the PSG data across the five study groups: PWE-only, PWE+OSA with low rAT, PWE+OSA with high rAT, OSA-only with low rAT, and OSA-only with high rAT. Significant post hoc differences are indicated using superscript letters. The full set of Bonferroni-adjusted p-values for all pairwise comparisons is provided in Supplementary Table 1.
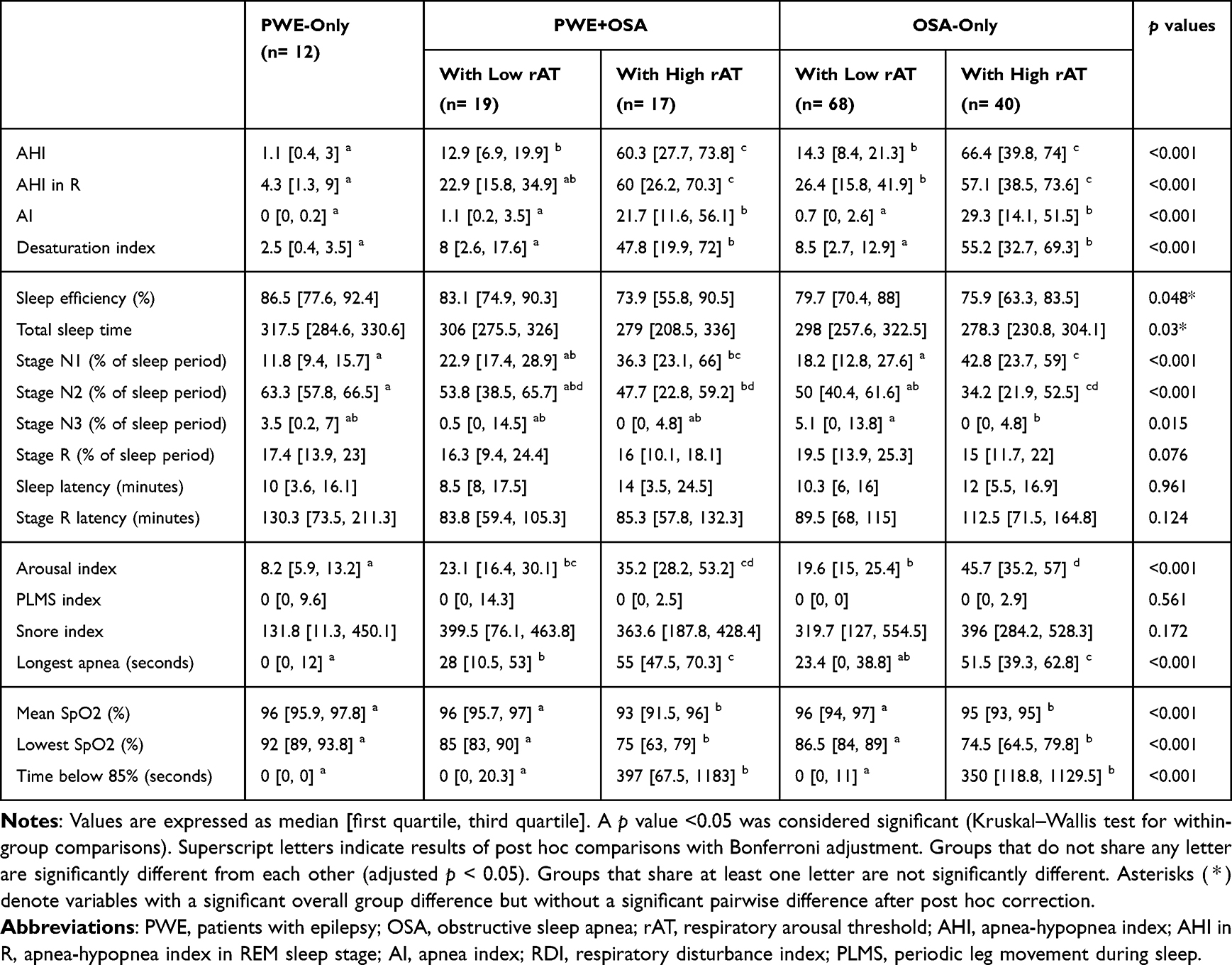 |
Table 3 Polysomnography Data of the Enrolled Patients |
Compared to all four OSA groups, the PWE-only group showed significantly lower AHI and arousal index. Additionally, the PWE-only group had a lower fraction of stage N1 sleep, a higher fraction of stage N2 sleep, shorter longest apnea time, higher mean SpO2 level, and less time with SpO2 below 85%, particularly when compared to those with high rAT subgroups within both the PWE+OSA and OSA-only groups.
Among both PWE+OSA and OSA-only groups, low rAT subgroups had significantly lower AHI, lower AI, lower desaturation index, shorter longest apnea time, higher mean and lowest SpO2 levels, and spent less time with SpO2 below 85% compared to their high rAT counterparts. Among the OSA-only group, the low rAT subgroup also had a lower fraction of stage N1 sleep (adjusted p < 0.001), a higher fraction of stage N2 sleep (adjusted p = 0.002), a higher fraction of stage N3 sleep (adjusted p = 0.017), and a lower arousal index (adjusted p < 0.001) compared to the high rAT subgroup.
In inter-group comparisons, there were no significant differences in PSG parameters between PWE+OSA and OSA-only groups when matched for rAT phenotype (ie, comparisons within the low-rAT and high-rAT categories).
Table 4 presents the CPAP treatment outcomes for the 12 PWE with a total of 15 CPAP treatment records, along with 19 CPAP treatment records from OSA-only control group. Among the OSA-only group, CPAP compliance was significantly lower in the low rAT subgroup compared to the high rAT subgroup (p= 0.021). Although the differences were not statistically significant, the low rAT subgroup within the PWE+OSA group showed numerically lower CPAP compliance (53.4%), a lower percentage of days used (63.1%), and a lower average number of hours used per day (4.0 hours) compared to the high rAT subgroup from PWE+OSA (65.6%, 91.6%, and 5.5 hours respectively).
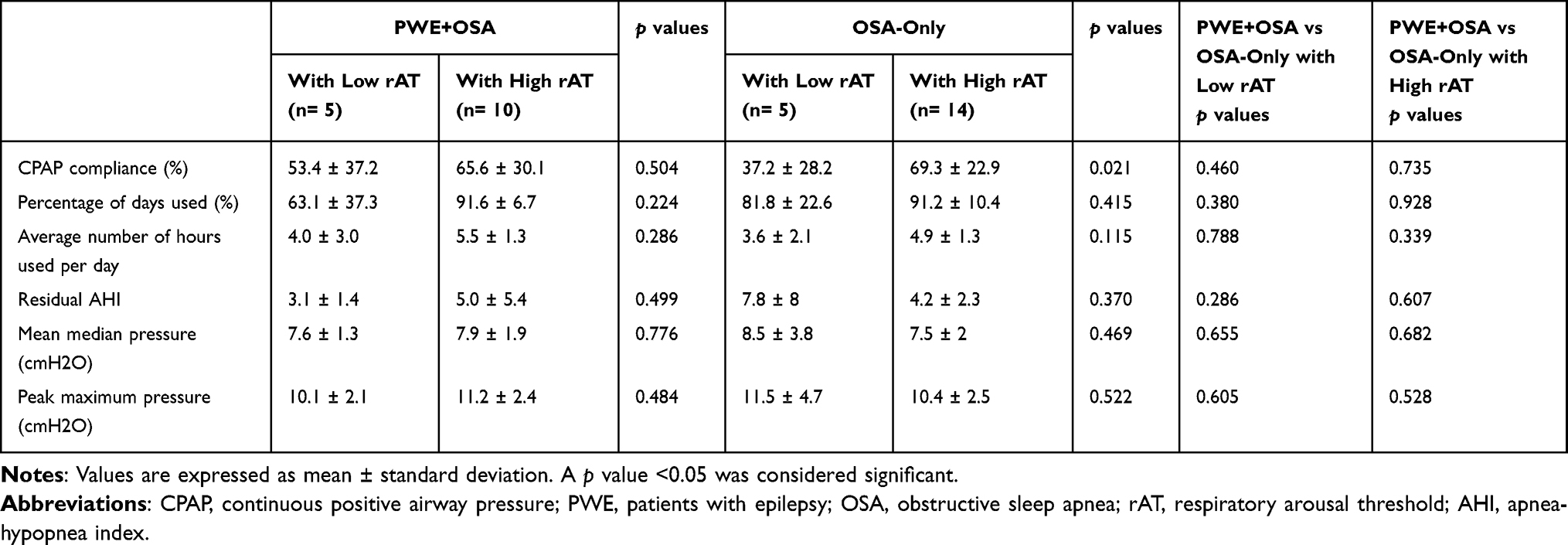 |
Table 4 CPAP Treatment Responses in Patients with Epilepsy and Concurrent OSA |
Post hoc power analysis indicated that, given the observed proportions of low rAT in the PWE+OSA (52.8%) and OSA-only (63.0%) groups, the effect size (Cohen’s w) was 0.081. With the available sample sizes (n = 36 and n = 108, respectively), the estimated statistical power to detect a significant difference was only 16.2%.
Discussion
In this study, we included a total of 48 PWE, of which 36 patients (75%) had concurrent OSA, and 108 patients with OSA only who underwent in-laboratory PSG. The PWE+OSA group were notably older at the time of PSG examination and had a later onset of epilepsy compared to PWE-only group. The OSA-only group were taking fewer concomitant ASMs and hypnotics compared to PWE+OSA and PWE-only groups. Among those with OSA, 19 (52.8%) in the PWE+OSA group and 68 (63.0%) in the OSA-only group were predicted to have a low rAT. The ratio of low rAT did not differ significantly between the two groups. These patients with a predicted low rAT exhibited significantly lower AHI, lower AI, lower desaturation index, higher mean SpO2 levels, higher lowest SpO2 levels, and less time with SpO2 below 85%. Among the OSA-only group, CPAP compliance was significantly lower in the low rAT subgroup compared to the high rAT subgroup. In the PWE+OSA group, although CPAP compliance, the percentage of used days, and the average hours of CPAP usage were numerically lower in the low rAT subgroup, these differences did not reach statistical significance.
The relationship between an increased age of epilepsy onset and the risk of OSA remains unclear. A study found that older adult patients with late-onset or worsening seizures had a higher AHI on PSG compared to patients who were seizure-free or experienced seizure improvement.30 Sleep apnea and low oxygen saturation levels during sleep are linked to late-onset epilepsy.31 Late-onset epilepsy may be more commonly caused by structural issues, such as cerebrovascular disease, brain tumors, and neurodegenerative disorders.32 One possible explanation for this association is that patients with etiologies for late-onset epilepsy, especially cerebrovascular disease, have a higher prevalence of OSA. Previous literature found that the prevalence of mild OSA and severe OSA was 71% and 30% in post-stroke patients, respectively.33 Brainstem infarction, more extensive hemispheric strokes, and bilateral lesions were reported to be associated with post-stroke OSA or OSA severity.34–36 Weakness of pharyngeal muscles and disturbance of central respiratory control are believed to be the pathogenesis of post-stroke OSA.37
In our study, there were no significant differences in the proportions of etiologies between PWE+OSA and PWE-only groups. However, we did not evaluate the detailed neurological manifestations and locations of brain lesions in our PWE with structural etiologies, which may have varying degrees of association with OSA occurrence. Future studies could further investigate and clarify the association between an increased age of epilepsy onset and the risk of OSA.
We found that PWE were taking not only more ASMs but also more hypnotics compared to patients in OSA-only group, suggesting this group experiences more sleep disturbances. A meta-analysis showed that PWE have worse sleep quality compared to controls.38 Poor sleep quality and insomnia are associated with poor seizure control and a lower quality of life.39,40 The causes of sleep disturbances in PWE are usually multifactorial. In addition to sleep interruptions associated with epileptic activity, circadian misalignment and psychiatric comorbidities such as depression or anxiety also play a role.41,42
We also observed a trend of higher numbers of concomitant ASMs in PWE+OSA compared to PWE-only group, although this difference was not significant after Bonferroni correction. The trend of higher ASM use suggests that seizures might be more challenging to control in this population. Moreover, the use of certain ASMs may exacerbate existing OSA symptoms. Benzodiazepines, for instance, can intensify drowsiness and lead to relaxation of the pharyngeal muscles.43 Additionally, specific ASMs like sodium valproate have been linked to weight gain and metabolic syndrome, which can increase the risk of OSA.44
Prior studies have shown that the prevalence of predictive low rAT in Asians with OSA falls within the range of approximately 28.4% to 50.2%.45,46 Hang et al conducted a retrospective analysis of 3718 OSA patients at a prominent sleep center in central Taiwan and reported a predicted low rAT prevalence of about 50.2% among Taiwanese OSA patients, using the same predictive model.46 In our study population with OSA, low rAT was predicted in 52.8% of the PWE+OSA group and in 63.0% of the OSA-only group. The slightly higher prevalence of low rAT in our study may be related to selection bias due to the lower BMI in both OSA groups compared to the mean BMI in Hang et al’s study.
Interestingly, the lack of a significant difference in rAT phenotype between the PWE+OSA and OSA-only groups was unexpected. We had initially hypothesized that the PWE+OSA group would exhibit a more disrupted arousal system and, consequently, a higher proportion of low rAT, contributing to their increased risk of OSA. Although the slightly lower prevalence of low rAT in the PWE+OSA group might be partially attributed to the sedative effects of ASMs and hypnotics—which are known to elevate arousal thresholds11—this marginal difference does not sufficiently explain the substantially higher prevalence of OSA observed in people with epilepsy. These findings suggest that factors beyond arousal threshold may contribute to the elevated risk of OSA in people with epilepsy. Potential mechanisms include additional effects of ASMs—such as reduced upper airway muscle tone or changes in body weight—as well as altered central ventilatory control.11,44 These hypotheses warrant further exploration in future mechanistic studies.
Notably, the PWE-only group demonstrated more favorable PSG findings compared to both low rAT subgroups (PWE+OSA and OSA-only). Although arousal system alterations are possible in epilepsy, they likely differ from the low rAT trait that contributes to obstructive events in OSA. Moreover, the well-controlled epilepsy status in most of our PWE-only participants may have contributed to more stable nocturnal respiration. In contrast, the rAT prediction model remained applicable to both PWE+OSA and OSA-only groups, as their low rAT subgroups shared similar clinical and PSG features. These findings suggest that the rAT phenotype retains its relevance in PWE+OSA group, while the absence of OSA-related arousal instability in PWE-only may account for their more favorable respiratory parameters.
Finally, the impact of low rAT on CPAP compliance is believed to be significant, and a similar trend was observed in our cohort.13 In the PWE+OSA group, the concurrent use of ASMs or hypnotics may have attenuated the differences in CPAP adherence between the low and high rAT subgroups, unlike the more pronounced difference seen in the OSA-only group. These findings suggest that stratifying PWE by rAT status could help tailor OSA management. Although this association was less distinct in the PWE+OSA group, rAT status may still influence treatment outcomes. Identifying this physiological trait may offer a path toward optimizing both OSA and epilepsy care.
However, due to the relatively small number of CPAP users in our study, these findings should be considered hypothesis-generating rather than conclusive. Additionally, disease severity may have confounded CPAP adherence, as the low rAT subgroup had a lower mean AHI compared to the high rAT group.29 We anticipate that future studies with larger sample sizes will be able to validate and further investigate this association.
The current study has several limitations that need to be acknowledged. Firstly, the sample size was small, and the study design was retrospective, which may introduce selection bias and limit the generalizability of the findings. Post hoc power analysis indicated that the study was underpowered to detect small differences in rAT distribution between the PWE+OSA and OSA-only groups (Cohen’s w = 0.081; power = 16.2%). Therefore, the absence of a statistically significant difference should be interpreted with caution. Secondly, our study involved extensive group comparisons. Although statistical adjustments (eg, Bonferroni correction) were applied for multiple comparisons, the risk of Type I errors may still be present.
Thirdly, the definition of low rAT in patients with OSA was based on a predictive model derived from PSG criteria rather than direct intrathoracic pressure measurements. The gold standard methods, such as epiglottic or esophageal pressure monitoring, were not used in this study.11 This limitation may affect the interpretation of our results, particularly since the predictive model has not been specifically validated in the PWE+OSA population.
Fourthly, the severity of epilepsy among our studied patients tended to be mild, and most of the patients were managed with a single ASM. As a result, the hypothesized negative impact of epileptic activity on the arousal system may not have been evident in this relatively mild population. Fifthly, potential confounding variables were not fully controlled in our group comparisons. For example, the PWE-only group tended to be younger, while the OSA-only group used fewer ASMs or hypnotics. These differences may introduce bias, particularly since many ASMs have sedative properties that could elevate the rAT.11 To better understand these complex interactions, future studies should consider focusing on patients with poorly controlled epilepsy, including those during medication-free periods, to more clearly isolate the effects on rAT.
Lastly, the results for PWE-only group might be influenced by potential confounding factors, including their younger age at the time of PSG examination and the reasons for undergoing PSG. It is possible that this group of patients, despite not having OSA, might have other sleep disorders or be potential patients with OSA.
Conclusions
In summary, our study provides insights into the presence and implications of low rAT in PWE+OSA. We found no significant difference in the prevalence of low rAT between the PWE+OSA group and the OSA-only control group, based on a PSG-based prediction model. Additionally, demographic and PSG characteristics were similar between low rAT subgroups in both populations. Notably, CPAP compliance was significantly lower in the low rAT subgroup within the OSA-only group, while this trend was attenuated in the PWE+OSA group.
These findings suggest that although low rAT may be a common feature in both groups, it may not fully explain the increased prevalence of OSA in PWE. Alternative mechanisms may contribute to this elevated risk. Further studies using gold-standard methods to directly measure rAT, and involving more heterogeneous epilepsy populations, are needed to clarify these complex interactions and guide more personalized OSA management in PWE.
Data Sharing Statement
The data that support the findings of this study are not publicly available due to privacy considerations but are available from the corresponding author upon reasonable request.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work the author used ChatGPT in order to revise sentences and proofread. After using this tool/service, the author reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Acknowledgments
This work was supported by Sleep Center and Epilepsy Center in Chang Gung Memorial Hospital. We thank all participants for their contributions to this study.
This manuscript has not been previously published in a peer-reviewed journal. However, part of the work was presented as a conference abstract at the 21st Annual Meeting of the Taiwan Society of Sleep Medicine (TSSM) in 2023, where preliminary findings were shared. Only the abstract was published in the conference proceedings; no full-text article has been published elsewhere. URL: https://tssm.org.tw/upload/ckeditor/1697270000.pdf.
Author Contributions
Li-Pang Chuang: methodology, validation, investigation, resources, writing—review and editing, supervision, project administration. Ting-Wei Liao: Conceptualization, software, formal analysis, data curation, writing—original draft preparation, visualization. Chun-Wei Chang: Conceptualization, methodology, resources, writing—review and editing. Mei-Yun Cheng, Tony Wu: Methodology, investigation, resources, writing—review and editing. Ning-Hung Chen: Investigation, resources, writing—review and editing, supervision. Shih-Wei Lin: Formal analysis, resources, writing—review and editing. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Lin Z, Si Q, Xiaoyi Z. Obstructive sleep apnoea in patients with epilepsy: a meta-analysis. Sleep Breath. 2017;21(2):263–270. doi:10.1007/s11325-016-1391-3
2. Li P, Ghadersohi S, Jafari B, Teter B, Sazgar M. Characteristics of refractory vs. medically controlled epilepsy patients with obstructive sleep apnea and their response to CPAP treatment. Seizure. 2012;21(9):717–721. doi:10.1016/j.seizure.2012.07.016
3. Latreille V, St Louis EK, Pavlova M. Co-morbid sleep disorders and epilepsy: a narrative review and case examples. Epilepsy Res. 2018;145:185–197. doi:10.1016/j.eplepsyres.2018.07.005
4. Rashed HR, Tork MA, El-Nabil LM, et al. Refractory epilepsy and obstructive sleep apnea: is there an association? Egypt J Neurol Psychiatry Neurosurg. 2019;55(1):1–6. doi:10.1186/s41983-019-0072-0
5. Malow BA, Levy K, Maturen K, Bowes R. Obstructive sleep apnea is common in medically refractory epilepsy patients. Neurology. 2000;55(7):1002–1007. doi:10.1212/WNL.55.7.1002
6. Hollinger P, Khatami R, Gugger M, Hess CW, Bassetti CL. Epilepsy and obstructive sleep apnea. Eur Neurol. 2006;55(2):74–79. doi:10.1159/000092306
7. Pornsriniyom D, Shinlapawittayatorn K, Fong J, Andrews ND, Foldvary-Schaefer N. Continuous positive airway pressure therapy for obstructive sleep apnea reduces interictal epileptiform discharges in adults with epilepsy. Epilepsy Behav. 2014;37:171–174. doi:10.1016/j.yebeh.2014.06.025
8. Jo H, Choi S, Kim D, Joo E. Effects of obstructive sleep apnea on epilepsy, and continuous positive airway pressure as a treatment option. J Clin Med. 2022;11(7):2063. doi:10.3390/jcm11072063
9. Piperidou C, Karlovasitou A, Triantafyllou N, et al. Influence of sleep disturbance on quality of life of patients with epilepsy. Seizure. 2008;17(7):588–594. doi:10.1016/j.seizure.2008.02.005
10. McCarter AR, Timm PC, Shepard PW, et al. Obstructive sleep apnea in refractory epilepsy: a pilot study investigating frequency, clinical features, and association with risk of sudden unexpected death in epilepsy. Epilepsia. 2018;59(10):1973–1981. doi:10.1111/epi.14548
11. Eckert DJ. Phenotypic approaches to obstructive sleep apnoea - new pathways for targeted therapy. Sleep Med Rev. 2018;37:45–59. doi:10.1016/j.smrv.2016.12.003
12. Zinchuk A, Edwards BA, Jeon S, et al. Prevalence, associated clinical features, and impact on continuous positive airway pressure use of a low respiratory arousal threshold among male United States veterans with obstructive sleep apnea. J Clin Sleep Med. 2018;14(5):809–817. doi:10.5664/jcsm.7112
13. Wu H, Fang F, Wu C, Zhan X, Wei Y. Low arousal threshold is associated with unfavorable shift of PAP compliance over time in patients with OSA. Sleep Breath. 2021;25(2):887–895. doi:10.1007/s11325-020-02197-9
14. Eckert DJ, Owens RL, Kehlmann GB, et al. Eszopiclone increases the respiratory arousal threshold and lowers the apnoea/hypopnoea index in obstructive sleep apnoea patients with a low arousal threshold. Clin Sci. 2011;120(12):505–514. doi:10.1042/CS20100588
15. Eckert DJ, Malhotra A, Wellman A, White DP. Trazodone increases the respiratory arousal threshold in patients with obstructive sleep apnea and a low arousal threshold. Sleep. 2014;37(4):811–819. doi:10.5665/sleep.3596
16. Carter SG, Berger MS, Carberry JC, et al. Zopiclone increases the arousal threshold without impairing genioglossus activity in obstructive sleep apnea. Sleep. 2016;39(4):757–766. doi:10.5665/sleep.5622
17. Edwards BA, Eckert DJ, McSharry DG, et al. Clinical predictors of the respiratory arousal threshold in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 2014;190(11):1293–1300. doi:10.1164/rccm.201404-0718OC
18. Chu Y, Zinchuk A. The present and future of the clinical use of physiological traits for the treatment of patients with OSA: a narrative review. J Clin Med. 2024;13(6):1636. doi:10.3390/jcm13061636
19. Peter-Derex L, Klimes P, Latreille V, Bouhadoun S, Dubeau F, Frauscher B. Sleep disruption in epilepsy: ictal and interictal epileptic activity matter. Ann Neurol. 2020;88(5):907–920. doi:10.1002/ana.25884
20. Calvello C, Fernandes M, Lupo C, et al. Sleep architecture in drug-naive adult patients with epilepsy: comparison between focal and generalized epilepsy. Epilepsia Open. 2023;8(1):165–172. doi:10.1002/epi4.12687
21. Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55(4):475–482. doi:10.1111/epi.12550
22. Chuang LP, Chen NH, Li HY, et al. Dynamic upper airway changes during sleep in patients with obstructive sleep apnea syndrome. Acta Otolaryngol. 2009;129(12):1474–1479. doi:10.3109/00016480902780242
23. Epstein LJ, Kristo D, Strollo PJ, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263–276.
24. Chen NH, Johns MW, Li HY, et al. Validation of a Chinese version of the Epworth sleepiness scale. Qual Life Res. 2002;11(8):817–821. doi:10.1023/a:1020818417949
25. Kwan P, Arzimanoglou A, Berg AT, et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc task force of the ILAE commission on therapeutic strategies. Epilepsia. 2010;51(6):1069–1077. doi:10.1111/j.1528-1167.2009.02397.x
26. Zack MM, Kobau R. National and state estimates of the numbers of adults and children with active epilepsy - United States, 2015. MMWR Morb Mortal Wkly Rep. 2017;66(31):821–825. doi:10.15585/mmwr.mm6631a1
27. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. deliberations of the sleep apnea definitions task force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
28. Iber C. The AASM manual for the scoring of sleep and associated events: rules. Terminol Technical Specification. 2007.
29. Sawyer AM, Gooneratne NS, Marcus CL, Ofer D, Richards KC, Weaver TE. A systematic review of CPAP adherence across age groups: clinical and empiric insights for developing CPAP adherence interventions. Sleep Med Rev. 2011;15(6):343–356. doi:10.1016/j.smrv.2011.01.003
30. Chihorek AM, Abou-Khalil B, Malow BA. Obstructive sleep apnea is associated with seizure occurrence in older adults with epilepsy. Neurology. 2007;69(19):1823–1827. doi:10.1212/01.wnl.0000279334.78298.d5
31. Grigg-Damberger M, Foldvary-Schaefer N. Hypoxia not AHI in adults with sleep apnea midlife markedly increases risk of late onset epilepsy carosella CM et al sleep apnea, hypoxia, and late-onset epilepsy: the atherosclerosis risk in communities study SLEEP-2023-0175.R1. Sleep. 2023. doi:10.1093/sleep/zsad252
32. DiFrancesco JC, Labate A, Romoli M, et al. Clinical and instrumental characterization of patients with late-onset epilepsy. Front Neurol. 2022;13:851897. doi:10.3389/fneur.2022.851897
33. Seiler A, Camilo M, Korostovtseva L, et al. Prevalence of sleep-disordered breathing after stroke and TIA: a meta-analysis. Neurology. 2019;92(7):e648–e654. doi:10.1212/WNL.0000000000006904
34. Siccoli MM, Valko PO, Hermann DM, Bassetti CL. Central periodic breathing during sleep in 74 patients with acute ischemic stroke - neurogenic and cardiogenic factors. J Neurol. 2008;255(11):1687–1692. doi:10.1007/s00415-008-0981-9
35. Ahn SH, Kim JH, Kim DU, Choo IS, Lee HJ, Kim HW. Interaction between sleep-disordered breathing and acute ischemic stroke. J Clin Neurol. 2013;9(1):9–13. doi:10.3988/jcn.2013.9.1.9
36. Brown DL, McDermott M, Mowla A, et al. Brainstem infarction and sleep-disordered breathing in the BASIC sleep apnea study. Sleep Med. 2014;15(8):887–891. doi:10.1016/j.sleep.2014.04.003
37. Stevens D, Martins RT, Mukherjee S, Vakulin A. Post-stroke sleep-disordered breathing-pathophysiology and therapy options. Front Surg. 2018;5:9. doi:10.3389/fsurg.2018.00009
38. Bergmann M, Tschiderer L, Stefani A, Heidbreder A, Willeit P, Hogl B. Sleep quality and daytime sleepiness in epilepsy: systematic review and meta-analysis of 25 studies including 8,196 individuals. Sleep Med Rev. 2021;57:101466. doi:10.1016/j.smrv.2021.101466
39. Quigg M, Gharai S, Ruland J, et al. Insomnia in epilepsy is associated with continuing seizures and worse quality of life. Epilepsy Res. 2016;122:91–96. doi:10.1016/j.eplepsyres.2016.02.014
40. Lin CY, Wu T, Chang CW, et al. Reduced sleep quality is related to poor quality of life in patients with Juvenile myoclonic epilepsy, a case-control study. Life. 2022;12(3):434. doi:10.3390/life12030434
41. Quigg M, Bazil CW, Boly M, et al. Proceedings of the sleep and epilepsy workshop: section 1 decreasing seizures-improving sleep and seizures, themes for future research. Epilepsy Curr. 2021;21(3):15357597211004566. doi:10.1177/15357597211004566
42. Quigg M, Pavlova MK, Buchanan GF, Epilepsy W. Proceedings of the sleep and epilepsy workshop: introduction. Epilepsy Curr. 2021;21(3):15357597211004551. doi:10.1177/15357597211004551
43. Hsu TW, Chen HM, Chen TY, Chu CS, Pan CC. The association between use of benzodiazepine receptor agonists and the risk of obstructive sleep apnea: a nationwide population-based nested case-control study. Int J Environ Res Public Health. 2021;18(18):9720. doi:10.3390/ijerph18189720
44. Soylemez E, Ozturk O, Baslo SA, Balcik ZE, Atakli D. Metabolic syndrome and obstructive sleep apnea syndrome among patients with epilepsy on monotherapy. Epilepsy Behav. 2020;111:107296. doi:10.1016/j.yebeh.2020.107296
45. Lee RWW, Sutherland K, Sands SA, et al. Differences in respiratory arousal threshold in Caucasian and Chinese patients with obstructive sleep apnoea. Respirology. 2017;22(5):1015–1021. doi:10.1111/resp.13022
46. Hang LW, Huang CS, Cheng WJ. Clinical characteristics of Asian patients with sleep apnea with low arousal threshold and sleep structure change with continuous positive airway pressure. Sleep Breath. 2021;25(3):1309–1317. doi:10.1007/s11325-020-02235-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.