Back to Journals » Drug Design, Development and Therapy » Volume 20
Resmetirom: An Update on Therapy for Metabolic Dysfunction-Associated Steatohepatitis (MASH)
Authors Van Kleef LA ![]() , Michel M, Alkhouri N, Brouwer WP
, Michel M, Alkhouri N, Brouwer WP ![]() , Schattenberg JM
, Schattenberg JM ![]()
Received 8 December 2025
Accepted for publication 24 February 2026
Published 17 March 2026 Volume 2026:20 559331
DOI https://doi.org/10.2147/DDDT.S559331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Anastasios Lymperopoulos
Laurens A Van Kleef,1,* Maurice Michel,2,3,* Naim Alkhouri,4 Willem Pieter Brouwer,1 Jörn M Schattenberg2,3
1Department of Gastroenterology and Hepatology, Erasmus MC University Medical Center, Rotterdam, the Netherlands; 2Department of Internal Medicine II, University Medical Center Saarland, Homburg, Germany; 3Medical Faculty, Saarland University, Saarbrücken, Germany; 4Department of Hepatology, Arizona Liver Health, Chandler, AZ, USA
*These authors contributed equally to this work
Correspondence: Jörn M Schattenberg, Department of Internal Medicine II, University Medical Center Saarland, Kirrberger Str. 100, Homburg, 66421, Germany, Tel +49 6841 1615027, Email [email protected]
Abstract: Metabolic dysfunction associated steatotic liver disease (MASLD) affects nearly one-third of adults worldwide, particularly among individuals with obesity or type 2 diabetes, and in 10– 30% progresses to metabolic dysfunction associated steatohepatitis (MASH) or fibrosis. Resmetirom, a selective thyroid hormone receptor-β (THR-β) agonist, became the first therapy to demonstrate both MASH resolution and fibrosis improvement, leading to accelerated food and drug administration (FDA) approval in 2024 and conditional European Medicine Agency (EMA) approval in 2025 in the treatment of fibrotic MASH. Resmetirom is a liver-specific drug that simulates the effect of T3 and thereby reduces intrahepatic fat. It is safe and generally well tolerated. Current clinical guidance recommends treating patients with non-cirrhotic fibrotic MASH (typically those with LSM-VCTE 10– 20 kPa or MRE 3.1– 4.4 kPa), while excluding patients with cirrhosis, active liver disease, significant alcohol use, or untreated thyroid disorders. Treatment monitoring focuses on hepatic safety, thyroid function in selected patients, and assessment of response using non-invasive tests and ALT after 6– 12 months. Real-world data indicate rapid adoption of non-invasive eligibility assessments, early improvements in liver stiffness, and frequent concomitant GLP-1 receptor agonist use, with treatment response appearing independent of weight-loss therapy. As semaglutide has now also gained regulatory approval for fibrotic MASH, optimal positioning of resmetirom within treatment algorithms, combination strategies with GLP-1 receptor agonists, and the long-term impact on liver-related and cardiometabolic outcomes remain key priorities. This review discusses the evidence supporting conditional approval of resmetirom, outlines current clinical recommendations, early real-world experiences, and highlights ongoing challenges and future directions in the management of fibrotic MASH.
Keywords: resmetirom, MASLD, MASH, fibrosis, pharmaceutical treatment
Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD) is the most prevalent liver disease, affecting approximately one in three adults worldwide.1 Among individuals with MASLD, around 30% progress to steatohepatitis and 10–30% develop clinically significant fibrosis, with substantially higher rates observed in those with type 2 diabetes mellitus (T2DM) or obesity.2–5 Approximately 3% of patients progress to cirrhosis over a period of 20 years.6 Cirrhosis is strongly associated with morbidity and mortality and is largely irreversible while hence it should ideally be prevented and targeted screening is widely recommended.7,8 The progressive and multifactorial nature of MASLD, combined with the limited effectiveness and adherence challenges of lifestyle interventions, underscores the urgent need for pharmacological therapies to halt disease progression and improve clinical outcomes.9
Several agents for MASH, including selonsertib (ASK1 inhibitor), elafibranor (PPAR-α/δ agonist), obeticholic acid (FXR agonist), and cenicriviroc (CCR2/CCR5 antagonist), were evaluated in Phase 3 trials but failed to gain FDA approval due to insufficient efficacy or safety concerns.10–13 Conditional approval can currently be obtained by demonstrating efficacy in this setting requires meeting the following key endpoints: (1) fibrosis improvement without worsening of MASH, and/or (2) MASH resolution without worsening of fibrosis. The challenging path toward the first approved therapy underscores the complexity of treating fibrotic MASH and highlights the critical importance of appropriate patient selection.14
Amid this background, the MAESTRO-NASH phase 3 trial evaluated Resmetirom, a selective thyroid hormone receptor-β (THR-β) agonist, in precirrhotic MASH (F1b – F3) and met the regulatory endpoints.15 The trial recruited participants with MASH and the histological stages F1b to F3 and required participants to have three metabolic risk factors. The preplanned interim analysis at 52 weeks demonstrated both fibrosis regression and resolution of MASH, making resmetirom (which improves intrahepatic lipid metabolism and modulates fibrosis) the first therapeutic agent to meet both regulatory endpoints required for food and drug administration (FDA) approval.
This review summarizes the pathway and evidence that led to accelerated FDA and conditional European medicine agency (EMA) approval for resmetirom, discusses current treatment recommendations and highlights current challenges and remaining knowledge gaps.
Drug Development of Resmetirom
Figure 1 summarizes the path towards conditional approval of resmetirom (MGL-3196), which was initially developed as a lipid-lowering agent, based on evidence that agonism of thyroid hormone receptor beta (THR-β) improves atherogenic lipids and lipoproteins associated with cardiovascular outcomes.16 However, the lipid-lowering potency was inferior to statins. Yet due to its hepatic mechanisms of action, its potential in treating patients with metabolic dysfunction-associated steatohepatitis (MASH) and fibrosis was proposed by Becky Taub.16 The selective binding of resmetirom, to THR-β, which is highly expressed in the liver and involved in several lipid oxidation and metabolic pathways made the compound a strong candidate for development in the relatively new indication of MASH.17 Moreover, its mechanism of action may counteract hepatic hypothyroidism, a frequent feature of both overt and subclinical hypothyroidism in patients with MASLD/MASH.18 Resmetirom can restore the relative intrahepatic triiodothyronine (T3) deficiency and stimulate hepatic metabolism.19 The secondary effects on lipid profiles underscore their value in patients with MASH, who are frequently present with a high metabolic burden.
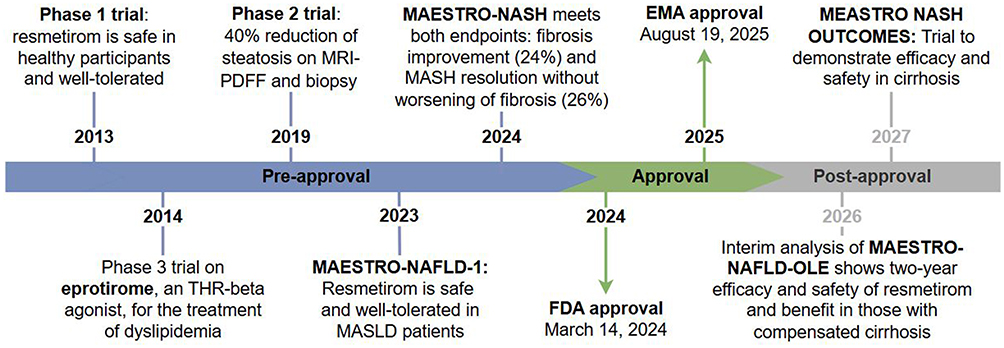 |
Figure 1 Timeline towards approval of resmetirom and anticipated trials. Key studies leading to the conditional approval of resmetirom in the treatment of fibrotic MASH as well as the anticipated future trials of which the preliminary results of the MEASTRO-NAFLD-OLE trial as presented during the EASL and AASLD 2025 already have been incorporated. |
The potential hepatic effects of resmetirom were demonstrated in preclinical animal studies, showing reductions in hepatic triglycerides, steatosis, inflammatory and fibrosis markers. A Phase 1 safety study in healthy participants receiving increasing doses of resmetirom demonstrated excellent tolerability and only mild adverse events unrelated to the study medication.16 A Phase 2 trial was then conducted in adults with biopsy-confirmed MASH (fibrosis stages F1–F3) and a hepatic fat fraction of at least 10% at baseline, assessed by MRI-proton density fat fraction (MRI-PDFF).20 In this phase 2 study, resmetirom achieved its primary endpoint and led to a significant reduction in hepatic fat fraction compared to placebo after 12 weeks (−32.9% vs −10.4%; p<0.0001) and 36 weeks (−37.3% vs −8.5%; p<0.0001) (Figure 2). In line with its mechanism of action, resmetirom also significantly reduced atherogenic lipids and lipoproteins. A second liver biopsy performed after 36 weeks of treatment showed histological improvements in markers of MASH. The most common adverse events reported were gastrointestinal, including diarrhea and nausea.
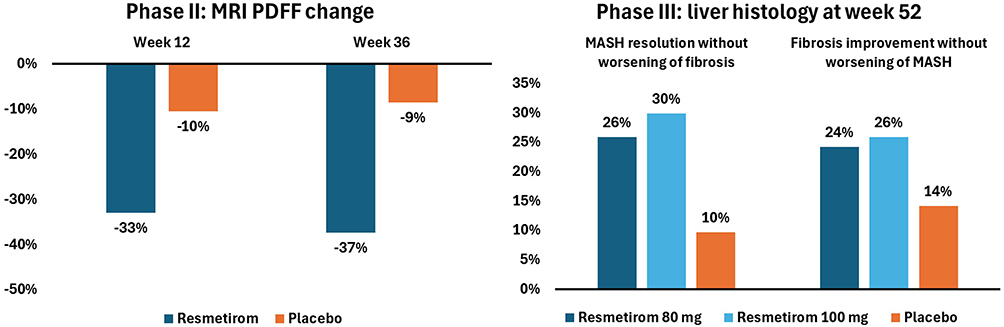 |
Figure 2 Primary endpoints from the Phase II and phase III resmetirom trials. The phase II study reports on the relative MRI PDFF change for resmetirom compared to placebo in 123 patients living with MASLD having an average fat percentage of 16.2%. The phase III study reports on (1) MASH resolution without worsening of fibrosis and (2) at least one stage of fibrosis improvement without worsening of MASH in 966 patients with significant differences between treatment arms and placebo arm (p < 0.001). |
Based on the positive phase 2 findings, the phase 3 trial (MAESTRO-NASH) was initiated in March 2019 evaluating two doses of resmetirom (80 mg and 100 mg) in patients with biopsy-confirmed MASH and fibrosis (F1B–F3).15 Both histologically defined primary endpoints were met at week 52: MASH resolution without worsening of fibrosis (80 mg, 25.9%; 100 mg, 29.9% vs placebo, 9.7%; p<0.001 for both comparisons) and fibrosis improvement by at least one stage (80 mg, 24.2%; 100 mg, 25.9% vs placebo, 14.2%; p<0.001 for both comparisons) (Figure 2). An improvement in lipid profiles was seen as early as 24 weeks of treatment: LDL cholesterol levels decreased by −13.6% (80 mg) and −16.3% (100 mg) vs 0.1% with placebo (p<0.001 for both comparisons), and interestingly, lipoprotein (a) levels were also significantly reduced in both treatment arms compared to placebo. Overall, no changes in body weight or glycemic control (HbA1c) were seen, which themselves have strong associations with LSM-VCTE.21 In line with the histological improvements, non-invasive tests (NITs) also improved with resmetirom compared to placebo. The safety profile was consistent with previous trials, with gastrointestinal side effects being the most common in the resmetirom arms. The observed loose stools occurred early, and they were reported less frequently after week 12, suggesting that adaptations can occur. The trial remains ongoing for up to 54 months to assess long-term outcomes as per FDA regulatory guidance.22
The MAESTRO-NASH trial is part of a broader clinical program comprising a total of four complementary phase 3 trials designed to evaluate the overall efficacy and safety of resmetirom in MASH.23 Although the majority of these trials (MAESTRO-NASH, MAESTRO-NAFLD-1 and MAESTRO-NAFLD-OLE) include patients with non-cirrhotic MASH, the MAESTRO-NAFLD-1 and MAESTRO-NAFLD-OLE also involve patients with well-compensated MASH-cirrhosis in a smaller subset. In turn, the MEASTRO-NASH-Outcomes trial only includes patients with well-compensated MASH cirrhosis. The MAESTRO-NAFLD-1 and MAESTRO-NAFLD-OLE trials were designed to assess the safety and tolerability of resmetirom (80 and 100 mg) compared to placebo in patients with presumed MASH, diagnosed using NITs rather than biopsy. Of note, parts of the MAESTRO-NAFLD-1 trial also included patients with phenotypic MASLD defined as steatosis (CAP ≥ 280 dB/m) and a VCTE range between ≥5.5 kPa and <8.5 kPa.24 The MAESTRO-NAFLD-1 contained three double-blind treatment arms that continued into the open-label extension study (MAESTRO-NAFLD-OLE). The treatment arms included randomized patients receiving 80 mg or 100 mg of resmetirom versus placebo, while open-label arms included patients on 100 mg resmetirom and those starting at 80 mg with well-compensated MASH cirrhosis.
The primary endpoint of MAESTRO-NAFLD-1 was safety assessed by the incidence of treatment-emergent adverse events (TEAEs) at week 52.24 In the primary analysis no differences in TEAE incidence among treatment arms: 86.5% (open-label 100 mg), 86.1% (100 mg), 88.4% (80 mg) vs 81.8% (placebo) were observed. As seen in earlier trials, gastrointestinal side effects occurred more frequently in the resmetirom groups. Key secondary endpoints were also met, with relevant reductions in atherogenic lipid profiles, including amongst others LDL cholesterol, apoliprotein B, triglycerides and lipoprotein(a), and liver fat content in resmetirom-treated patients. Similar aspects were also observed after the open-label switch from placebo (MAESTRO-NAFLD-1) to 100 mg resmetirom (MAESTRO-NAFLD-OLE). Results of the MAESTRO-NAFLD-OLE, presented at AASLD 2025, show sustained improvements in lipids and NITs over a total of 2 years with resmetirom treatment throughout MAESTRO-NAFLD-1 and subsequently MAESTRO-NAFLD-OLE and without new safety concerns.25 In the open-label cohort of MAESTRO-NAFLD-OLE with well-compensated MASH cirrhosis, sustained reductions in liver stiffness measurement (LSM-VCTE) were observed after two years of treatment.26 Notably, 35% of patients showed a potential conversion from F4 to F3 fibrosis based on NITs (LSM-VCTE <15 kPa and ≥25% decrease from baseline). Additionally, the proportion of patients with signs of clinically significant portal hypertension (CSPH, defined as VCTE >25 kPa) decreased from 35% at baseline to 15% after two years of resmetirom treatment.
Pharmacodynamics, Pharmacokinetics and Safety
Pharmacokinetics and Pharmacodynamics
Resmetirom is an orally administered thyroid hormone receptor beta (THR-β) agonist that binds selectively to THR-β. This high selectivity helps minimize systemic off-target effects, particularly those related to THR-α activation in the heart, bone, and thyroid gland. Early studies showed that, unlike other thyromimetics such as eprotirome and MB07811, resmetirom has no detectable THR-α activity.16 Even at a dose of 200 mg no adverse effects on vital signs, ECG parameters, heart rate, or blood pressure were observed.16 No data is available on safety at higher dosages.
Resmetirom acts mainly by stimulating THR-β-mediated gene transcription in the nucleus, especially genes involved in lipid metabolism.27 Through this mechanism, it enhances cholesterol breakdown and reduces de novo lipogenesis.28 Activation of THR-β by resmetirom also increases hepatic iodothyronine deiodinase 1 (DIO1) activity, which promotes the conversion of thyroxine (T4) to the active hormone triiodothyronine (T3) or to reverse T3.16,29
In the phase 1 trial, reductions in free T4 were observed at higher doses of resmetirom at 100 mg and 200 mg consistent with THR-β activation.16,30 However, there were no dose-dependent effects on free T3 or thyroid-stimulating hormone (TSH), indicating no impact on the central thyroid axis.16 The phase 3 MAESTRO-NASH trial reported similar findings: both resmetirom treatment arms showed reduced fT4 levels compared with placebo, while T3 and TSH remained largely unchanged.15 Although the prevalence of hypothyroidism and thyroxine replacement therapy was between 12% and 14% across the placebo and both treatment arms, the aforementioned effects were independent of thyroxine-replacement status, and no clinical symptoms related to lower fT4 levels were observed.15 In the MAESTRO NASH study patients with active hyperthyroidism, untreated hypothyroidism or doses of thyroxin exceeding 200 micrograms were excluded from the MAESTRO-NASH trial. According to the AASLD practice guidelines, abnormal thyroid function should be addressed before initiating therapy, with assessment of TSH levels at baseline or within six months prior to treatment, followed by regular monitoring during therapy.31
Resmetirom also increased levels of sex hormone–binding globulin (SHBG), a THR-β–regulated gene product that helps stabilize circulating sex hormones. At week 52, SHBG concentrations increased by 145% with 80 mg and by 205% with 100 mg, compared with a - 0.4% change in the placebo group.15 In the phase 1 trial, a trend toward higher testosterone levels was seen in males, with no changes in follicle-stimulating hormone (FSH) or luteinizing hormone (LH).16 Similarly, in the phase 3 study, sex hormone levels showed minimal changes from baseline.15 Notably, a 120% increase in SHBG levels observed in the phase 3 trial was associated with histologic response, suggesting that SHBG may serve as a potential biomarker of treatment response, although further investigation is warranted. No adverse clinical effects related to increased SHBG have been reported to date.
Safety Considerations
The most common adverse events associated with resmetirom were mild-to-moderate gastrointestinal symptoms, such as diarrhea and nausea which typically occur after drug initiation and cease after week 12. Importantly, there was no evidence of drug-induced liver injury or cartilage toxicity, in contrast to other THR-β-agonists (including eprotirome), for which further development was discontinued due to safety.15–17 Pruritus occurred slightly more frequently in both treatment arms compared with placebo.
Among more than 1300 patients who received resmetirom at doses of 80 or 100 mg/day for up to one year, two cases of liver injury were considered possibly related to the drug. The observed toxicity was predominantly hepatocellular, with ALT levels of 236 and 578 U/L, accompanied by low alkaline phosphatase and bilirubin levels.32 Liver injury developed within three months of treatment initiation and resolved completely within two months after discontinuation.32 One additional case of severe hepatotoxicity was reported, which upon repeated liver biopsy was found to represent interface hepatitis consistent with autoimmune hepatitis.31 In one patient, reintroduction of resmetirom led to recurrent liver injury, and the drug was subsequently permanently discontinued.32 Consistent with these findings, the AASLD recommends regular monitoring of liver enzymes during therapy to detect rare hepatotoxicity and advises discontinuation of treatment if significant liver injury occurs.31
Resmetirom is primarily metabolized by the cytochrome P450 enzyme CYP2C8 and may therefore interact with drugs that are CYP2C8 inhibitors, such as clopidogrel and gemfibrozil, or substrates, such as pioglitazone. These interactions have important clinical implications. Co-administration with clopidogrel, a moderate CYP2C8 inhibitor, does require dose adjustment of resmetirom, while the concomitant use of gemfibrozil, a strong CYP2C8 inhibitor, is not recommended. Pioglitazone, a CYP2C8 substrate, may have increased plasma concentrations when used with resmetirom; however, no dose adjustment is necessary, and clinical monitoring is advised. Furthermore, resmetirom is a substrate of OATP1B1, OATP1B3, and BCRP transporters and may interact with inhibitors such as cyclosporine.
Similar considerations apply to the use of statins, as resmetirom can increase plasma concentrations of several statins.33 Therefore, lipid profiles should be monitored to achieve the desired cardiovascular risk reduction. According to the manufacturer’s guidance, the maximum recommended daily dosages are 20 mg for rosuvastatin and simvastatin and 40 mg for atorvastatin and pravastatin.
Regarding treatment discontinuation, data from clinical trials indicate low drop-out rates. In the MAESTRO-NAFLD trial, discontinuation rates were 1.5% and 1.2% for the 100 mg and 80 mg doses, respectively, compared with 0.9% for placebo after one year of treatment. In the MAESTRO-NASH trial, discontinuation rates were slightly higher, at 6.8% and 2.2% for the 100 mg and 80 mg groups, respectively, compared with 2.2% in the placebo group. In the MAESTRO-NASH OUTCOMES trial, preliminary data presented at the EASL reported a drop-out rate of approximately 8% at the time of the interim analysis.26
Regulatory Approval and Clinical Recommendations
Conditional Approval
Resmetirom received accelerated approval from the FDA in March 2024 for adults with fibrotic MASH owing the high unmet need for a drug to treat MASH. The EMA granted conditional approval in August 2025, and the drug has entered the European market since October 2025, starting in Germany. Following these regulatory milestones, four key guidance documents have been published to support the clinical implementation of resmetirom. First, an expert panel released practical recommendations for the initiation and monitoring of resmetirom in Clinical Gastroenterology and Hepatology.33 Second, the AASLD issued an update to its practice guidance.31 Third, a global consensus statement on MASLD and MASH was published in Gastroenterology, which includes a dedicated section on resmetirom.34 Finally, the German S2K-MASLD guideline has been amended to incorporate recommendations for resmetirom use.35
Who to Treat
Not all MASLD patients are eligible for treatment; in fact, only a minority with evidence of the presence of MASH. Fortunately, treatment recommendations are based on non-invasive test with no need of liver histology. LSM (either MRE or VCTE) is generally divided into two categories: “treatment recommended” and “consider treatment”, summarized in Figure 3. The AASLD guidance primarily targets patients with LSM-VCTE between 8–15 kPa or by LMS-MRE between 3.1–4.4 kPa. Additionally, treatment may be considered in those with higher LSM-VCTE values of 15–20 kPa or LSM-MRE 4.4–5.0 kPa. Other elastography procedures that have been validated in MASH can be used interchangeably. Next to imaging, other NITs suggestive F2-F3 fibrosis (as outlined in the NILDA guidelines) can be used for treatment decisions, with sufficient data available for the ELF test and potentially PRO-C3 ADAPT in the future.31,36 The expert panel recommendations propose slightly higher thresholds. Specifically, it does not recommend treatment for patients with LSM-VCTE between 8–10 kPa or by LSM-MRE between 3.1–3.3 kPa, implying greater caution in patients with borderline stiffness values to avoid overtreatment. LSM-based tests such as FAST, MAST and MEFIB are listed as alternatives for LSM.33 The global consensus statement takes an LSM-VCTE-driven approach and does not explicitly address MRE or cT1. Yet, similar to AASLD, it supports consideration of treatment for patients with LSM-VCTE between 8 kPa and 20 kPa, but notes that individuals with 8–10 kPa should undergo an additional non-invasive test to suggest F2–F3 fibrosis before treatment initiation.34 In the German health care system, the LSM-VCTE cut-offs are between 10 and 19.9 kPa, highlighting that overtreatment of patients in the stage F1 is not a desired goal. In this group, active management and repeated testing are recommended.35 In summary, the current recommendations focus primarily on patients with an LSM-VCTE between 10–20 kPa when measured with LSM-VCTE or between 3.1–4.4 kPa when measured with MRE.
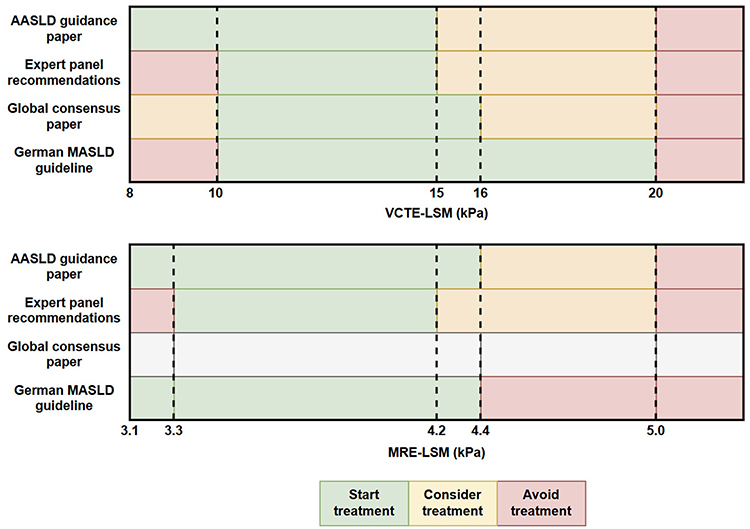 |
Figure 3 Comparison of resmetirom treatment eligibility across guidelines for LSM. An overview of the differences in treatment eligibility for the different recommendations. Green indicates eligible for treatment, yellow indicates consider treatment but typically requires more careful ruling out of cirrhosis, and red indicates do not consider treatment. The dotted line is placed at common thresholds for change in recommendation to ease interpretation. |
Who Not to Treat
All guidelines emphasize the need to rule out cirrhosis before initiating treatment with resmetirom, as efficacy and safety have not been formally demonstrated in this group.31,33–35 Recommendations are to rule-out cirrhosis in accordance with the exclusion criteria of the MAESTRO-NASH trial (1) F4 fibrosis on biopsy at any time; (2) imaging suggestive of portal hypertension defined as ascites, portosystemic venous collaterals or varices; (3) clinical manifestation of hepatic decompensation; and (4) clinical signs or laboratory data suggestive of portal hypertension including impaired liver function. The corresponding NIT cut-offs have been defined at LSM-VCTE ≥20 kPa and LSM-MRE ≥5 kPa, platelets <140/nl, ELF > 11.3, hepatic nodularity on imaging; elevated INR, low albumin or elevated bilirubin not related to liver dysfunction or caused by Gilberts syndrome.15,31,33–35 In addition, the global consensus statement explicitly highlights that for patients with LSM-VCTE ≥16 kPa, a second NIT other than LSM-VCTE should rule out cirrhosis.34
In addition, the following contraindications are defined: uncontrolled concomitant liver disease, excess alcohol use and untreated thyroid disease. It is important to exclude individuals from treatment when alcoholic liver disease is present with amounts of alcohol exceeding >20 grams/day in females or >30 grams per day in males, whereas the German recommendation allows up to 50 grams/day in females and 60 grams/day in males.31,33,35 Figure 4 illustrates a summary of the indications and contraindications across the guidelines.
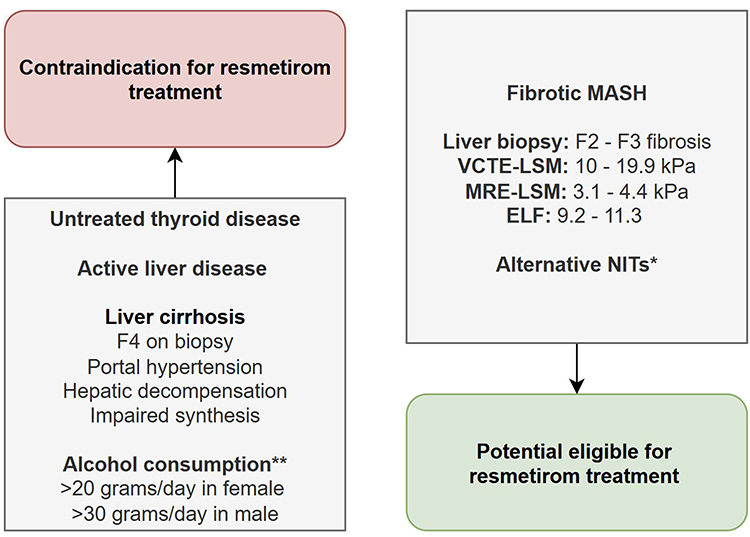 |
Figure 4 Overview of the indications and contraindications across the guidelines. Contraindications for resmetirom treatment summarising the available guidance papers. *Alternative NITs that were mentioned are in line with the NILDA guidelines, indicating F2-F3. **In Germany, the threshold is higher at >60 grams per day in males and >50 grams per day in females, and thereby includes MetALD patients as well. The treatment eligibility differs more across guidelines as illustrated in Figure 3 and discussed previously. |
How to Monitor Safety in Patients on Resmetirom
Monitoring of hepatic function is recommended after the initiation of resmetirom treatment. Current recommendations include safety assessment every 3 months, which can be extended to every 6 months after 6 months of treatment. Hepatotoxicity must be assessed in patients experiencing AST or ALT elevations exceeding 5 times the ULN or impaired liver function and treatment should be discontinued in case of hepatotoxicity.31
Additional attention is required for patients with uncontrolled thyroid disease, as free T4 levels decreased up to 24% in patients receiving levothyroxine alongside resmetirom, while free T3 levels remained unchanged. The routine monitoring of thyroid function including TSH and free T4 is recommended for patients living with pre-existing thyroid disease.31,33 Additionally, when concomitant statin therapy was adapted according to the label, lipid profile should be re-assessed as part of the safety monitoring.31,33 In the recent German Guidelines monitoring of thyroid function and lipid profiles was recommended regardless of medical history, owing to the conditional approval status by EMA.35
How to Evaluate Treatment Response
Evaluation of the treatment response is important to identify patients without benefit from therapy. All four guidance papers recommend the evaluation of treatment response after a year of therapy, using the same modalities as used when treatment eligibility was assessed. The global consensus statement and expert panel paper also mention that early evaluation of treatment response may be considered at month six based on LSM-VCTE, together with ALT, which is also included in the regular safety assessment.33,34 Owing to the variability of LSM, guidelines offer slightly different cut-offs defining improvement. Improvement under resmetirom treatment should exceed 20–30% on LSM-VCTE and 25–30% on LSM-MRE, accompanied by a reduction in ALT levels if elevated at baseline.31,33–35 Improvement is considered a treatment response and resmetirom treatment should be continued.
If NITs remain unchanged or a suboptimal improvement is seen after 12 months, treatment can be continued based on an individual consideration, since it is suggestive of stable or halted disease. In this case, the treatment strategy should be re-evaluated and can be continued after risk-benefit assessment.31,33–35 The expert panel recommendations also include MRI-PDFF in their treatment monitoring, which might be particularly relevant in patients who do not have an improvement in ALT or NITs, since ≥30% reduction in MRI-PDFF was one of the best predictors of histological response.15,33 These rules are of importance, considering that the long-term benefit of resmetirom treatment is currently evaluated in the ongoing MAESTRO-NASH trail.28
Treatment futility is defined as a significant worsening (similar thresholds as for the improvement) of the non-invasive parameters or a consistent increase in ALT. The global consensus statement specifically states that the lack of ALT response after 1 year of treatment with resmetirom should not be used as the sole criterion for discontinuing treatment.31,33–35 In case of treatment futility, resmetirom treatment should be discontinued.
Clinical Impact Beyond the Liver
MASLD is a multisystem disorder and is generally considered the hepatic manifestation of the metabolic syndrome.5,37 Resmetirom, however, appears to act primarily within the liver, targeting intrahepatic fat metabolism. Aligning with this concept, resmetirom has not demonstrated meaningful effects on fasting glucose, HbA1c, or body mass index.15 However, aligning with the mechanism of action, resmetirom significantly reduces atherogenic lipid profiles in patients with biopsy-proven fibrotic MASH, with reductions of up to 20% over 24–52 weeks.15,38,39 Importantly, patients enrolled in the MAESTRO-trials were managed according to current standard of care in terms of the cardiovascular risk profile, and thus resmetirom brought added benefits to existing lipid lowering strategies. However, the effects on cardiovascular events and MACE remain to be shown. For this, it is important to realize that the MAESTRO-NASH trial specifically excluded the patients with relevant CVD and the study was also not powered to detect any differences in CVD events.40,41 Consequently, the long-term impact of THR-β agonists on cardiovascular risk has not been established, and the AASLD notes that further data are required to determine their effect on cardiovascular disease outcomes.28,31 This might be particularly difficult to study as CVD has previously been linked to higher LSM most likely due to venous congestion, interfering with the non-invasive treatment eligibility criteria, which could result in individuals with CVD more easily be selected for treatment with resmetirom in the absence of fibrotic MASH.42,43
Whilst there is a clear improvement in lipid profiles, lipid-lowering treatment should be continued after initiating resmetirom as the LDL-reduction with statins or PCSK-9 inhibitors is more substantial and these drugs have been associated with improved long-term cardiovascular outcomes.44,45 Statins may even have hepatoprotective properties as in patients with cirrhosis, there were lower rates of hepatocellular carcinoma and hepatic decompensation and on a population level there may also be lower rates of fibrosis.46–48 This further underscores the need for a holistic treatment approach covering every aspect of metabolic dysfunction rather than siloed disease management of patients with fibrotic MASH.
Real-World Data
Now that resmetirom has been conditionally approved for the treatment of fibrotic MASH in both the US and Europe, more granular real-world data are expected to emerge soon. Such data will be essential for guiding clinicians on optimal patient selection, timing of initiation, and monitoring strategies, as well as for assessing hard clinical endpoints and cost-effectiveness. At the time of writing this review, however, available information remains limited to two peer-reviewed manuscripts and preliminary reports from international conferences and needs to be interpreted with caution, awaiting further validation with preferably longer follow-up.
Across two cohorts with a combined 250 patients on resmetirom, gastrointestinal symptoms and pruritus were the most common side effects, with discontinuation rates ranging from 9% to 16%, though no drug-induced liver injury was observed, and liver enzymes improved over 3 months. Streamlined prescription pathways and closer follow-up may further reduce discontinuation and improve timely access to therapy.49,50
At the EASL International Liver Congress in June 2025, two abstracts were presented encompassing a total of 460 patients who had recently initiated resmetirom treatment in the United States.51,52 In these studies, approximately 80% of patients began therapy without histological (biopsy) confirmation, relying solely on non-invasive tests for diagnosis and monitoring. After three months of treatment, about 50% of patients demonstrated a ≥25% reduction in LSM-VCTE, while no substantial changes were observed in BMI, HbA1c, or liver enzyme levels. In real-world practice, resmetirom is frequently prescribed alongside GLP-1 receptor agonists, used by nearly 20% of patients in these cohorts. However, concomitant GLP-1RA use was not associated with differences in treatment response.
During the 2025 AASLD The Liver Meeting, new real-world data on resmetirom were presented across eight abstracts, encompassing a combined 4125 patients, with likely overlap between datasets. In a TriNetX claims-based analysis (n = 1438), 27% of patients were also prescribed semaglutide and 15% tirzepatide. A modest rise in ALT and AST was observed within the first 90 days after treatment initiation, followed by significant improvement beyond 90 days.53 An independent propensity-matched analysis of the same registry showed that concomitant semaglutide use was associated with lower fibrosis progression (25% vs 39%) at a median of 130 days compared with resmetirom monotherapy.54 In an electronic medical record-based cohort of 848 patients (347 with ≥6 months of follow-up), concomitant GLP-1 receptor agonist use was common (23%, including 11% on semaglutide). After six months, FIB-4 scores declined modestly (1.8 to 1.6), aligning with reductions in ALT and AST, while platelet counts remained unchanged.55 Another multicenter cohort (n = 148) reported a 17% discontinuation rate, primarily due to non-specified adverse effects.56 In contrast, the Optum Market Clarity claims dataset (n = 341) found that only 12 patients discontinued, all of whom later restarted therapy, although the dispensed medication covered approximately 75% of the expected doses at six months (with high variability based on the SD of 30%).57 Finally, a registry-based matched-cohort analysis (n = 1304) demonstrated early improvements in mortality (0.7% vs 2.0%), major adverse liver outcomes (1.0% vs 2.2%), and cardio-renal outcomes (0.9% vs 2.9%) compared with non-resmetirom users, yet needs further validation.58
Collectively, these studies highlight the growing adoption of non-invasive eligibility assessments for resmetirom initiation, consistent biochemical improvements (even when preceded by transient worsening), encouraging early clinical responses, and good overall treatment persistence. Notably, the concomitant use of GLP-1 receptor agonists was common, yet treatment response to resmetirom appeared independent of these weight-loss interventions, while still contributing to improvements in liver health. Current data should be interpreted with caution, as it has very limited follow-up and is prone to selection bias and confounding by indication. Additional studies with longer follow-up are needed to confirm sustained hepatic and extra-hepatic benefits in real-world practice.
Implementation Challenges and Future Outlook
Positioning in Treatment Algorithms
Currently, two treatment options for the indication fibrotic, non-cirrhotic MASH have received FDA approval: resmetirom and semaglutide. No head-to-head comparison has been conducted, and the choice of drug is based on individual clinical decision. A recent network meta-analysis compared the relative efficacy of various compounds investigated in phase 2b and phase 3 trials.59 In contrast to the ESSENCE III and MEASTRO NASH trial, this meta-analysis showed that semaglutide and resmetirom exhibited similar potency for fibrosis regression, whereas resmetirom demonstrated greater efficacy for MASH resolution.15,59,60 Additional agents are currently under investigation and will likely be added to the treatment options but are beyond the scope of this review.59 Resmetirom seems to be a valuable addition in patients receiving a stable dose of GLP-1 exhibiting residual liver disease.61,62 When a patient is initiated on a GLP-1 RA in the indication of T2D or even obesity, a benefit for the liver phenotype should be reassessed at month 6 before the addition of a second liver-directed agent is considered. Since THR-β agonists are lacking weight-loss properties, a combination with GLP-1 seems appealing to potentiate treatment response, yet awaits evaluation in future studies.15,63 In addition, individuals with dyslipidaemia-related phenotype, THR-β agonist will exert additional extrahepatic effects through LDL cholesterol and lipoprotein(a) lowering effects.64
Combination Therapies
Semaglutide, a GLP-1 receptor agonist, primarily addresses systemic metabolic dysfunction by reducing weight. However, emerging evidence suggests that newer anti-obesity agents may also exert weight–loss–independent metabolic effects.65,66 Given the widespread use of GLP-1 RAs in the management of obesity and T2DM, in the MAESTRO-NASH trial, 16.8% and 12.7% of participants were receiving GLP-1 receptor agonists in the 80 mg and 100 mg treatment arms, respectively.15 In the MAESTRO-NAFLD trial, between 7.6% and 11.7% of the participants were on GLP-1 receptor agonists across treatment groups.24 Subgroup analyses indicated that the efficacy and safety of resmetirom were consistent irrespective of baseline GLP-1 use.15 Madrigal’s recent acquisition of an oral GLP-1 analogue underscores the growing interest in a synergistic therapeutic strategy combining systemic metabolic improvement with direct liver-targeted mechanisms.67
Several other agents for fibrotic MASH are being studied in phase 2 and 3 trials. Hence, future therapy may include combination regimens incorporating fibroblast growth factor 21 (FGF21) analogues, pan–peroxisome proliferator-activated receptor (pan-PPAR) agonists, or dual incretin agonists targeting both GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptors.2,9 Collectively, these emerging strategies highlight the potential use of a multimodal therapy addressing both hepatic and systemic components of metabolic dysfunction, moving the field closer to personalized treatment of fibrotic MASH, nonetheless further data is required before individualized recommendations can be provided. A holistic approach is important in choosing the right (combination of) drugs with lifestyle and exercise, as long as formal recommendations based on evidence are lacking.
Duration of Therapy
In case of a favorable response, the current guidelines recommend continuing treatment. At this point, there is no evidence on the safety of stopping treatment or on the recurrence rates of steatosis, steatohepatitis, and fibrosis. Future studies should evaluate whether patients could discontinue treatment upon reaching treatment goals.
Conclusion
The approval of resmetirom changed the reality of care for patients with MASLD. The ongoing clinical trials will be crucial for determining whether the observed histological improvements translate into a durable reduction in liver-related events and mortality. Today, treatment decisions are guided by recent advances in non-invasive testing, and while no options for patients with compensated cirrhosis are available yet, the future in MASH treatment looks bright. Moving forward, the therapeutic landscape will likely evolve toward combination regimens, which may enhance efficacy and target multiple pathogenic pathways. Early identification of responders and non-responders will be crucial to provide cost-effective and individualized care. Ultimately, an integrative comprehensive metabolic health concept for patients with MASLD is required and supported by drugs like resmetirom.
Abbreviations
AASLD, American Association for the Study of Liver Diseases; AIH, Autoimmune hepatitis; ALT, Alanine aminotransferase; BMI, Body mass index; CAP, Controlled attenuation parameter; CCR2/CCR5, C-C chemokine receptor types 2 and 5; CSPH, Clinically significant portal hypertension; CV, Cardiovascular; DIO1, Iodothyronine deiodinase type 1; ELF, Enhanced liver fibrosis test; EMA, European Medicine Agency; FDA, US Food and Drug Administration; fT3, Free triiodothyronine; fT4, Free thyroxine; FXR, Farnesoid X receptor; GLP-1, Glucagon-like peptide-1; GLP-1 RA, GLP-1 receptor agonist; HbA1c, Hemoglobin A1c; INR, International normalized ratio; LDL, Low-density lipoprotein; LH, Luteinizing hormone; LSM, Liver stiffness measurement; LSM-MRE, LSM measured by magnetic resonance elastography; LSM-VCTE, LSM measured by vibration-controlled transient elastography; MACE, Major adverse cardiovascular events; MASH, Metabolic dysfunction-associated steatohepatitis; MASLD, Metabolic dysfunction-associated steatotic liver disease; MRE, Magnetic resonance elastography; MRI-PDFF, MRI-proton density fat fraction; NILDA, Non-Invasive Liver Disease Assessment; NIT, Non-invasive test; OATP1B1/OATP1B3, Organic anion transporting polypeptides 1B1 and 1B3; OLE, Open-label extension; PDFF, Proton density fat fraction; PEth, Phosphatidylethanol; PPAR-α/δ, Peroxisome proliferator-activated receptor alpha/delta; SHBG, Sex hormone-binding globulin; T2DM, Type 2 diabetes mellitus; TEAE, Treatment-emergent adverse event; THR-β, Thyroid hormone receptor beta; T3, Triiodothyronine; T4, Thyroxine; TSH, Thyroid-stimulating hormone; ULN, Upper limit of normal (reference range); VCTE, Vibration-controlled transient elastography.
Acknowledgments
ChatGPT-5 has been used to check for style and grammar upon finalizing the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Financial support was provided by the Foundation for Liver and Gastrointestinal Research, Rotterdam, the Netherlands. The funding source did not influence the writing of the report and the decision to submit for publication.
Disclosure
LvK Travel expenses from EASL and Falk Foundation. MM declares consultant honorary from Boehringer Ingelheim, Ipsen, Madrigal Pharmaceuticals; Speaker honorarium from AbbVie, AstraZeneca, Daiichi Sankyo, Gilead Sciences, GSK, Ipsen and NovoNordisk; Travel support: Abbvie, Boehringer Ingelheim, Gilead Sciences, Ipsen, Mirum and NovoNordisk. NA has received grant/research support from 89bio, Akero Therapeutics, Arbutus Biopharma, AstraZeneca, BioAge, Boehringer Ingelheim, Bristol Myers Squibb, Corcept Therapeutics, Galectin Therapeutics, Genentech, Gilead Sciences, Hepagene Therapeutics, Intercept Pharmaceuticals, Inventiva Pharma, Ionis Pharmaceuticals, Ipsen, Lilly, Madrigal Pharmaceuticals, Merck, NGM Biopharmaceuticals, NorthSea Therapeutics, Novo Nordisk, Perspectum, Pfizer, PharmaIN, Poxel, Regeneron, Viking Therapeutics, and Zydus Pharmaceuticals; reports speaker’s fees from AbbVie, AstraZeneca, Echosens, Gilead Sciences, Ipsen, Madrigal Pharmaceuticals, Novo Nordisk, and Perspectum; and reports consulting for 89bio, AbbVie, Akero, Boehringer Ingelheim, Echosens, Fibronostics, Gilead Sciences, HistoIndex, Intercept Pharmaceuticals, Ipsen, LiverRight, Madrigal Pharmaceuticals, NorthSea Therapeutics, Novo Nordisk, Perspectum, Pfizer, Regeneron, and Sonicy Incytes. JMS declares consultant honorary from Akero, Alentis, Alexion, Altimmune, Astra Zeneca, 89Bio, Bionorica, Boehringer Ingelheim, Gilead Sciences, GSK, HistoIndex, Ipsen, Inventiva Pharma, Madrigal Pharmaceuticals, Kríya Therapeutics, Lilly, eTherapeutics, Merck, MSD Sharp & Dohme GmbH, Nordic Bioscience, Northsea Therapeutics, Novartis, Novo Nordisk, Pfizer, Roche, Sanofi, Siemens Healthineers, Summit Clinical, and Vantage Biosciences Research; speaker honorarium from AbbVie, Boehringer Ingelheim, Gilead Sciences, Ipsen Novo Nordisk, Madrigal Pharmaceuticals, Worldwide Clinical Trials, Stockholder options: Hepta Bio. WPB received speakers fees for Eli Lilly, is part of the advisory board of Novo Nordisk and participates in trials of 89BIO, Boehringer Ingelheim, Novo Nordisk, and Inventiva Pharma. The authors report no other conflicts of interest in this work.
References
1. Younossi ZM, Golabi P, Paik JM, et al. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77(4):1335–14. doi:10.1097/HEP.0000000000000004
2. Targher G, Valenti L, Byrne Christopher D. Metabolic dysfunction–associated steatotic liver disease. N Engl J Med. 2025;393(7):683–698. doi:10.1056/NEJMra2412865
3. Hagström H, Shang Y, Hegmar H, et al. Natural history and progression of metabolic dysfunction-associated steatotic liver disease. Lancet Gastroenterol Hepatol. 2024;9(10):944–956. doi:10.1016/S2468-1253(24)00193-6
4. Michel M, Doll M, Albert N, et al. Obesity and harmful alcohol consumption are predictors for advanced liver disease in the disease management program for type 2 diabetes. United Eur Gastroenterol J. 2024;12(1):11–21. doi:10.1002/ueg2.12511
5. Pustjens J, van Kleef LA, Janssen HLA, et al. Differential prevalence and prognostic value of metabolic syndrome components among patients with MASLD. JHEP Rep. 2024;6(12):101193. doi:10.1016/j.jhepr.2024.101193
6. Owrangi S, Paik JM, Golabi P, et al. Meta-analysis: global prevalence and mortality of cirrhosis in metabolic dysfunction-associated steatotic liver disease. Aliment Pharmacol Ther. 2024;61(3):433–443.
7. Premkumar M, Kamath PS, Reiberger T, et al. Recompensation in decompensated cirrhosis. Lancet Gastroenterol Hepatol. 2025;10(11):1028–1040. doi:10.1016/S2468-1253(25)00095-0
8. Pustjens J, Brouwer WP, Ayada I, et al. Considerations and clinical utility of referral pathways for early detection of liver disease in at-risk populations. World J Gastroenterol. 2025;31(37):107665. doi:10.3748/wjg.v31.i37.107665
9. Newsome PN, Loomba R. Therapeutic horizons in metabolic dysfunction-associated steatohepatitis. J Clin Invest. 2025;135(13). doi:10.1172/JCI186425
10. Harrison SA, Wong VW, Okanoue T, et al. Selonsertib for patients with bridging fibrosis or compensated cirrhosis due to NASH: results from randomized Phase III STELLAR trials. J Hepatol. 2020;73(1):26–39. doi:10.1016/j.jhep.2020.02.027
11. Sanyal AJ, Ratziu V, Loomba R, et al. Results from a new efficacy and safety analysis of the REGENERATE trial of obeticholic acid for treatment of pre-cirrhotic fibrosis due to non-alcoholic steatohepatitis. J Hepatol. 2023;79(5):1110–1120. doi:10.1016/j.jhep.2023.07.014
12. Anstee QM, Neuschwander-Tetri BA, Wai-Sun Wong V, et al. Cenicriviroc lacked efficacy to treat liver fibrosis in nonalcoholic steatohepatitis: aurora phase III randomized study. Clin Gastroenterol Hepatol. 2024;22(1):124–134.e1. doi:10.1016/j.cgh.2023.04.003
13. Harrison S, Ratziu V, Bedossa P, et al. RESOLVE-IT Phase 3 trial of elafibranor in NASH: final results of the week 72 interim surrogate efficacy analysis. 2020.
14. Drenth JPH, Schattenberg JM. The nonalcoholic steatohepatitis (NASH) drug development graveyard: established hurdles and planning for future success. Expert Opin Investig Drugs. 2020;29(12):1365–1375. doi:10.1080/13543784.2020.1839888
15. Harrison Stephen A, Bedossa P, Guy Cynthia D, et al. A phase 3, randomized, controlled trial of resmetirom in NASH with liver fibrosis. N Engl J Med. 2024;390(6):497–509. doi:10.1056/NEJMoa2309000
16. Taub R, Chiang E, Chabot-Blanchet M, et al. Lipid lowering in healthy volunteers treated with multiple doses of MGL-3196, a liver-targeted thyroid hormone receptor-β agonist. Atherosclerosis. 2013;230(2):373–380. doi:10.1016/j.atherosclerosis.2013.07.056
17. Kelly MJ, Pietranico-Cole S, Larigan JD, et al. Discovery of 2-[3,5-dichloro-4-(5-isopropyl-6-oxo-1,6-dihydropyridazin-3-yloxy)phenyl]-3,5-dioxo-2,3,4,5-tetrahydro[1,2,4]triazine-6-carbonitrile (MGL-3196), a Highly Selective Thyroid Hormone Receptor β agonist in clinical trials for the treatment of dyslipidemia. J Med Chem. 2014;57(10):3912–3923. doi:10.1021/jm4019299
18. Sinha RA, Singh BK, Yen PM. Thyroid hormone regulation of hepatic lipid and carbohydrate metabolism. Trends Endocrinol Metab. 2014;25(10):538–545. doi:10.1016/j.tem.2014.07.001
19. Ratziu V, Scanlan TS, Bruinstroop E. Thyroid hormone receptor-β analogues for the treatment of metabolic dysfunction-associated steatohepatitis (MASH). J Hepatol. 2025;82(2):375–387. doi:10.1016/j.jhep.2024.10.018
20. Harrison SA, Bashir MR, Guy CD, et al. Resmetirom (MGL-3196) for the treatment of non-alcoholic steatohepatitis: a multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet. 2019;394(10213):2012–2024. doi:10.1016/S0140-6736(19)32517-6
21. van Kleef LA, Savas M, Michel M, et al. Weight change is associated with metabolic liver health in a general population extending beyond weight loss targets of international guidelines. Gastro Hep Adv. 2026;5(2):100831. doi:10.1016/j.gastha.2025.100831
22. Harvey BE. NASH: regulatory considerations for clinical drug development and U.S. FDA approval. Acta Pharmacol Sin. 2022;43(5):1210–1214. doi:10.1038/s41401-021-00832-z
23. Harrison SA, Ratziu V, Anstee QM, et al. Design of the phase 3 MAESTRO clinical program to evaluate resmetirom for the treatment of nonalcoholic steatohepatitis. Aliment Pharmacol Ther. 2024;59(1):51–63. doi:10.1111/apt.17734
24. Harrison SA, Taub R, Neff GW, et al. Resmetirom for nonalcoholic fatty liver disease: a randomized, double-blind, placebo-controlled phase 3 trial. Nat Med. 2023;29(11):2919–2928. doi:10.1038/s41591-023-02603-1
25. Alkhouri N, Taub R, Lu X, et al. 4003: Durability of resmetirom response in MASLD patients after two years of treatment in MAESTRO-NAFLDOL. Hepatology. 2025;S1–S2308.
26. Alkhouri N, Taub R, Lu X, et al. LBO-002 Treatment with resmetirom for up to two years led to improvement in liver stiffness, fibrosis biomarkers, fibrosis scores and portal hypertension risk in 122 patients with compensated MASH cirrhosis. J Hepatol. 2025;82:S9–S10. doi:10.1016/S0168-8278(25)00311-3
27. Brennan PN, Kopka CJ, Agirre-Garrido L, et al. Reviewing MAESTRO-NASH and the implications for hepatology and health systems in implementation/accessibility of resmetirom. Npj Gut Liver. 2025;2(1):3. doi:10.1038/s44355-024-00017-5
28. Arvanitakis K, Koufakis T, Cholongitas E, et al. Insights into the results of resmetirom trials: can a thyroid hormone receptor agonist be the holy grail of MASH therapy? Pharmacol Ther. 2025;268:108811. doi:10.1016/j.pharmthera.2025.108811
29. Kelly GS. Peripheral metabolism of thyroid hormones: a review. Altern Med Rev. 2000;5(4):306–333.
30. Bochukova E, Schoenmakers N, Agostini M, et al. A mutation in the thyroid hormone receptor alpha gene. N Engl J Med. 2012;366(3):243–249. doi:10.1056/NEJMoa1110296
31. Chen VL, Morgan TR, Rotman Y, et al. Resmetirom therapy for metabolic dysfunction-associated steatotic liver disease: october 2024 updates to AASLD practice guidance. Hepatology. 2025;81(1):312–320. doi:10.1097/HEP.0000000000001112
32. Resmetirom. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012.
33. Noureddin M, Charlton MR, Harrison SA, et al. Expert panel recommendations: practical clinical applications for initiating and monitoring resmetirom in patients with MASH/NASH and moderate to noncirrhotic advanced fibrosis. Clin Gastroenterol Hepatol. 2024;22(12):2367–2377. doi:10.1016/j.cgh.2024.07.003
34. Younossi ZM, Zelber-Sagi S, Lazarus JV, et al. Global consensus recommendations for metabolic dysfunction-associated steatotic liver disease and steatohepatitis. Gastroenterology. 2025;169(5):1017–1032.e2. doi:10.1053/j.gastro.2025.02.044
35. Roeb E, Canbay A, Bantel H, et al. Amendment Resmetirom “zur S2k‑Leitlinie Metabolische Lebererkrankungen” (vormals Nicht‑alkoholische Fettlebererkrankung v. 2.0/April 2022) der Deutschen Gesellschaft für Gastroenterologie, Verdauungs‑ und Stoffwechselkrankheiten (DGVS) (Version 2.3). Deutsche Gesellschaft für Gastroenterologie, Verdauungs‑ und Stoffwechselkrankheiten (DGVS) Leitlinie. 2025.
36. Sterling RK, Duarte-Rojo A, Patel K, et al. AASLD practice guideline on imaging-based noninvasive liver disease assessment of hepatic fibrosis and steatosis. Hepatology. 2025;81(2):672–724. doi:10.1097/HEP.0000000000000843
37. van Kleef LA, Ayada I, Alferink LJM, et al. Metabolic dysfunction associated fatty liver disease improves detection of high liver stiffness: the Rotterdam study. Hepatology. 2022;75(2):419–429. doi:10.1002/hep.32131
38. Suvarna R, Shetty S, Pappachan JM. Efficacy and safety of resmetirom, a selective thyroid hormone receptor-β agonist, in the treatment of metabolic dysfunction-associated steatotic liver disease (MASLD): a systematic review and meta-analysis. Sci Rep. 2024;14(1):19790. doi:10.1038/s41598-024-70242-8
39. Harrison SA, Bashir M, Moussa SE, et al. Effects of resmetirom on noninvasive endpoints in a 36-week phase 2 active treatment extension study in patients with NASH. Hepatol Commun. 2021;5(4):573–588. doi:10.1002/hep4.1657
40. Sjouke B, Langslet G, Ceska R, et al. Eprotirome in patients with familial hypercholesterolaemia (the AKKA trial): a randomised, double-blind, placebo-controlled phase 3 study. Lancet Diabetes Endocrinol. 2014;2(6):455–463. doi:10.1016/S2213-8587(14)70006-3
41. Angelin B, Kristensen JD, Eriksson M, et al. Reductions in serum levels of LDL cholesterol, apolipoprotein B, triglycerides and lipoprotein(a) in hypercholesterolaemic patients treated with the liver-selective thyroid hormone receptor agonist eprotirome. J Intern Med. 2015;277(3):331–342. doi:10.1111/joim.12261
42. van Kleef LA, Lu Z, Ikram MA, et al. Liver stiffness not fatty liver disease is associated with atrial fibrillation: the Rotterdam study. J Hepatol. 2022;77(4):931–938. doi:10.1016/j.jhep.2022.05.030
43. Dajti E, Huber AT, Ferraioli G, et al. Advances in imaging–Elastography. Hepatology. 2025;10–1097.
44. Chou R, Cantor A, Dana T, et al. Statin use for the primary prevention of cardiovascular disease in adults: updated evidence report and systematic review for the US preventive services task force. JAMA. 2022;328(8):754–771. doi:10.1001/jama.2022.12138
45. Khan SU, Yedlapati SH, Lone AN, et al. PCSK9 inhibitors and ezetimibe with or without statin therapy for cardiovascular risk reduction: a systematic review and network meta-analysis. BMJ. 2022;377:e069116. doi:10.1136/bmj-2021-069116
46. Ayada I, van Kleef LA, Zhang H, et al. Dissecting the multifaceted impact of statin use on fatty liver disease: a multidimensional study. EBioMedicine. 2023;87:104392. doi:10.1016/j.ebiom.2022.104392
47. Choi J, Nguyen VH, Przybyszewski E, et al. Statin use and risk of hepatocellular carcinoma and liver fibrosis in chronic liver disease. JAMA Intern Med. 2025;185(5):522–530. doi:10.1001/jamainternmed.2025.0115
48. Sharma R, Simon TG, Hagström H, et al. Statins are associated with a decreased risk of severe liver disease in individuals with noncirrhotic chronic liver disease. Clin Gastroenterol Hepatol. 2024;22(4):749–759.e19. doi:10.1016/j.cgh.2023.04.017
49. Ravela N, Shackelford P, Blessing N, et al. Early experience with resmetirom to treat metabolic dysfunction-associated steatohepatitis with fibrosis in a real-world setting. Hepatol Commun. 2025;9(4). doi:10.1097/HC9.0000000000000670
50. Shuaibi S, Tobal I, Gore J, et al. A real-world experience with resmetirom: tolerability and access. Gastro Hep Adv. 2025;4(9):100709. doi:10.1016/j.gastha.2025.100709
51. Saggese A, Buckholz A, Schwartz R, et al. SAT-407-YI Assessing early changes and responses to resmetirom therapy using real world single center data. J Hepatol. 2025;82:S624. doi:10.1016/S0168-8278(25)01674-5
52. Dunn W, Singal A, Asaad I, et al. OS-097 Evaluating noninvasive diagnostic pathways for identifying MASH patients eligible for Resmetirom therapy: a real-world cohort analysis. J Hepatol. 2025;82:S66. doi:10.1016/S0168-8278(25)00412-X
53. Jahagirdar V, Rama K, Asgharpour A, et al. 4069: prescribing patterns and clinical characteristics of resmetirom recipients: real-world insights. Hepatology. 2025;S1–S2308.
54. Solpari K, Saggese A, Yang S, et al. 4084: combination therapy with resmetirom and GLP-1 receptor agonists demonstrates superior efficacy in reducing liver fibrosis in patients with metabolic dysfunction-associated steatohepatitis: a real-world multicohort analysis. Hepatology. 2025;S1–S2308.
55. Kim Y, O’Donnell J, Fakhraei R, et al. 4073: evaluating the early real-world impact of resmetirom in patients with metabolic dysfunction-associated steatohepatitis (MASH): a United States cohort study using electronic medical records. Hepatology. 2025;S1–S2308.
56. Blessing N, Robinson B, Shackelford P, et al. 4051 real world resmetirom 6-month follow up data. Hepatology. 2025;S1–S2308.
57. Bansal M, Rava A, Gutierrez C, et al. 4067: patient characteristics and treatment patterns among patients using resmetirom in the real-world setting. Hepatology. 2025;S1–S2308.
58. Jahagirdar V, Parmar K, Shah N, et al. 4052: resmetirom improves mortality, liver and cardiorenal-metabolic (CRM) outcomes in individuals with metabolic dysfunction-associated steatotic liver disease in routine clinical practice. Hepatology. 2025;S1–S2308.
59. Souza M, Al-Sharif L, Antunes VLJ, et al. Comparison of pharmacological therapies in metabolic dysfunction-associated steatohepatitis for fibrosis regression and MASH resolution: systematic review and network meta-analysis. Hepatology. 2025;82(6):1523–1533. doi:10.1097/HEP.0000000000001254
60. Newsome PN, Sanyal AJ, Engebretsen KA, et al. Semaglutide 2.4 mg in participants with metabolic dysfunction-associated steatohepatitis: baseline characteristics and design of the phase 3 ESSENCE trial. Aliment Pharmacol Ther. 2024;60(11–12):1525–1533. doi:10.1111/apt.18331
61. Raverdy V, Tavaglione F, Chatelain E, et al. Data-driven cluster analysis identifies distinct types of metabolic dysfunction-associated steatotic liver disease. Nat Med. 2024;30(12):3624–3633. doi:10.1038/s41591-024-03283-1
62. Zhou X-D, Song SJ, Guo CY, et al. Validation of a data-driven clustering model for MASLD: evidence from three large-scale asian cohorts. JHEP Rep;2026;8(1):101645.
63. Michel M, Schattenberg JM. Semaglutide targets MASH molecular pathways beyond weight loss. Nat Med. 2025;31(9):2865–2866. doi:10.1038/s41591-025-03927-w
64. Kushner RF, Almandoz JP, Rubino DM. Managing adverse effects of incretin-based medications for obesity. JAMA. 2025;334(9):822–823. doi:10.1001/jama.2025.11153
65. Michel M, Schattenberg JM. Targeting fibrosis and steatohepatitis through the metabolism - results from the ESSENCE trial. JHEP Rep. 2025;7(9):101492. doi:10.1016/j.jhepr.2025.101492
66. Caussy C, Cusi K, Rosenstock J, et al. Relationship between metabolic and histological responses in people with metabolic dysfunction-associated steatohepatitis with and without type 2 diabetes: participant-level exploratory analysis of the SYNERGY-NASH trial with tirzepatide. Diabetes Care. 2025;dc251306.
67. Madrigal. Madrigal pharmaceuticals enters into exclusive global license agreement for oral GLP-1 receptor agonist with CSPC pharmaceutical group limited. Volume 2025. Madrigal; 2025. Available from: https://ir.madrigalpharma.com/news-releases/news-release-details/madrigal-pharmaceuticals-enters-exclusive-global-license.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efimosfermin for the Treatment of Metabolic Dysfunction-Associated Steatohepatitis (MASH): Mechanism of Action, Clinical Development and Emerging Therapeutic Potential
Alamgir M, Sohal A, Kowdley KV
Drug Design, Development and Therapy 2026, 20:560039
Published Date: 31 March 2026
Fibroblast Growth Factor 21: Mechanisms, Therapeutic Potential, and Clinical Translation in Metabolic Dysfunction
Rama K, Jahagirdar V, Sanyal AJ
Drug Design, Development and Therapy 2026, 20:560034
Published Date: 28 April 2026