Back to Journals » Drug Design, Development and Therapy » Volume 20
Efimosfermin for the Treatment of Metabolic Dysfunction-Associated Steatohepatitis (MASH): Mechanism of Action, Clinical Development and Emerging Therapeutic Potential
Authors Alamgir M ![]() , Sohal A
, Sohal A ![]() , Kowdley KV
, Kowdley KV
Received 6 January 2026
Accepted for publication 19 March 2026
Published 31 March 2026 Volume 2026:20 560039
DOI https://doi.org/10.2147/DDDT.S560039
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Mariam Alamgir,1 Aalam Sohal,1,2 Kris V Kowdley1,3
1Department of Hepatology, Liver Institute Northwest, Seattle, WA, USA; 2Department of Gastroenterology and Hepatology, Creighton University, Phoenix, AZ, USA; 3Elson S. Floyd College of Medicine, Washington State University, Spokane, WA, USA
Correspondence: Kris V Kowdley, Liver Institute Northwest, 3216 NE 45th Pl, Suite 100, Seattle, WA, 98105, USA, Email [email protected]
Abstract: Metabolic dysfunction-associated steatotic liver disease (MASLD), the hepatic manifestation of metabolic syndrome, has emerged as the leading cause of chronic liver disease worldwide. Its global prevalence estimated at 38% between 2016– 2019, representing a nearly 50% increase compared with 1990– 2006. A subset of patients with MASLD will develop Metabolic dysfunction-associated steatohepatitis (MASH), which can progress to cirrhosis and require transplantation. Until 2024, no therapy was available for the treatment of MASH. In 2024, resmetirom became the first drug approved for the treatment of MASH. The approval of semaglutide, a GLP-1 agonist for the treatment of MASH, followed this development. Besides these two drugs, multiple other pharmacologic therapies targeting metabolic and inflammatory pathways currently under active development. Fibroblast growth factor-21 (FGF-21) has emerged as a key endocrine regulator with physiological effects on glucose and lipid metabolism. Efimosfermin, a long-acting once-monthly FGF-21 analogue, is currently under development and represents a promising therapeutic option for MASLD, with the added advance of long-term adherence. Phase 2 clinical trials have reported efimosfermin to be beneficial in MASH resolution and fibrosis regression in patients with MASH and F2/F3 fibrosis. This review summarizes the biologic rationale, clinical development and emerging therapeutic role of efimosfermin in the treatment landscape of MASH.
Keywords: MASH, efimosfermin, FGF-21, advanced fibrosis, cirrhosis, GLP-1, resmetirom
Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD) is now the most common chronic liver disease worldwide, with an estimated prevalence of MASLD reported to be at 38%, suggesting that 1 in 3 people has MASLD.1 MASLD is not only a leading cause of liver disease but has also been associated with a higher risk of cardiovascular mortality.2 In approximately 20% of patients, MASLD can progress to metabolic dysfunction-associated steatohepatitis (MASH), characterised by inflammation and ballooning degeneration of hepatocytes, which can progress to cirrhosis and hepatocellular carcinoma (HCC).1 The burden of MASH continues to rise, and it is now the leading cause of transplantation among women in the United States.3
Until early 2024, there were no approved pharmacologic therapies, and lifestyle modification remained the cornerstone of management. This paradigm shifted in March 2024, when resmetirom became the first drug approved for patients with MASH.4 Subsequently, semaglutide, a GLP-1 agonist was approved for patients with MASH. Both therapies have been reported to have meaningful anti-fibrotic effects in randomized placebo-controlled Phase III clinical trials., with improvement of >1 fibrosis stage in 25.9%-29.9% of patients receiving resmetirom (vs 9.7% in the placebo group) and 36.8% of patients receiving semaglutide (vs 22.4% in the placebo group).5 Fibrosis regression is a key regulatory endpoint, as multiple studies have reported that advanced fibrosis stage is associated with hepatic adverse events, including liver transplantation and decompensation.6
Several additional therapies are currently being studied as anti-fibrotic therapy among patients with MASH. Among these, fibroblast growth factor-21 (FGF-21) analogues are of significant interest. FGF-21 is a key metabolic hormone that regulates lipid oxidation, glucose homeostasis, and hepatic inflammation.7 FGF-21 signalling is a key regulator of multiple pathogenic pathways of MASH, including steatosis, inflammation, and fibrosis.7 While resmetirom and semaglutide exert their anti-fibrotic effects primarily through metabolic improvements, FGF-21 analogues offer a dual mechanism, combining metabolic improvements with a direct anti-fibrotic effect via hepatic stellate cells (HSC)/macrophage pathways.8 Multiple phase 2/3 clinical studies have reported significant improvement in fibrosis stage among patients receiving FGF-21 analogues. Efimosfermin, an FGF-21 analogue was recently studied in a phase 2a clinical trial and reported promising results.9 This review aims to summarize the current literature on the mechanism of action, clinical trials, and future directions for efimosfermin.
The Role of FGF-21
FGF-21 is a member of the FGF superfamily and is closely related to FGF-19 and FGF-23.10 FGF-21 binds to coreceptor β-klotho (KLB), which enables it to escape the interstitial environment and enter the systemic circulation to act as an endocrine hormone.11 The major organs regulated by this hormone include the liver, pancreas, adipose tissue, small intestine, and muscle.12 During human evolution, there was a survival advantage to consuming large amounts of energy quickly, especially fructose.13 Fructose metabolism rapidly depletes ATP, resulting in substantial stress on the liver.13 In response to stress, hepatocytes upregulate FGF-21 expression.14 FGF-21 acts via endocrine, autocrine, and paracrine pathways to reduce metabolic stress and protect hepatocytes from injury.
Endocrine Effects
There is a strong correlation between FGF-21 levels and macronutrient levels.14–16 During a low-protein, high-fructose, or carbohydrate diet, the levels of FGF-21 increase.14–16 FGF-21 levels have also been reported to reduce the desire to eat sweet-tasting foods.17–19 FGF-21 also plays a role in insulin sensitivity. By increasing insulin sensitivity during positive caloric balance, FGF-21 redirects energy from the liver to the peripheral adipose tissue and skeletal muscles. Furthermore, due to enhanced insulin sensitivity, FGF-21 reduces the release of free fatty acids into the circulation, thereby limiting their hepatic uptake.20 Due to increased sensitivity, insulin promotes the uptake of chylomicrons from the gastrointestinal tract and very low-density lipoprotein (VLDL) secreted by the hepatocytes.21 These properties have resulted in development of FGF-21 analogues as treatments for MASLD/MASH.
Autocrine Effects
FGF-21 protects against endoplasmic reticulum stress and increases the anti-oxidative capacity of hepatocytes by activating the transcription factor Nrf2.22–24 FGF-21 also increases autophagy of misfolded proteins and suppresses pro-apoptotic pathways and increasing the expression of transcription factor HNF-4α (hepatocyte nuclear factor-4α), a regulator of the functional capacity of hepatocytes, including albumin synthesis, gluconeogenesis, lipid metabolism, and cytochrome P450-mediated oxidative pathways.25–27 Among patients with MASH, HNF-4α expression is reduced, providing a rationale for the efficacy of FGF-21 analogues for treatment of this disease.27
Paracrine Effects
FGF-21, released by stressed hepatocytes, modulates the activity and phenotype of Kupffer cells and HSC.28,29 FGF-21 shifts the phenotype of macrophages from an inflammatory to a repair phenotype.28 In vitro studies have reported that FGF-21 suppresses HSC differentiation into myofibroblasts.29 In vivo studies have reported that FGF-21 loss accelerates fibrosis progression in the lungs, pancreas, liver, kidney, and heart.30–33 Studies have also reported that loss-of-function mutations in FGF-21 pathways increase the risk of liver fibrosis.34,35
Sympathetic Effects
FGF-21 exerts central nervous system effects that complement its peripheral metabolic action via the ability to cross the blood-brain receptor and act on receptors that express β-klotho (KLB).36,37 Recently, Rose et al used dietary models of MASH to demonstrate that the weight-loss effects of FGF-21 are secondary to signalling from KLB-expressing cells in both the central nervous system and adipose tissue.36 Their study suggested that cholesterol metabolism is governed primarily by neuronal activation. It also reported that FGF-21 increases hepatic sympathetic activity. They also reported that both the central and peripheral nervous systems are required for FGF-21’s hepatic effects.36 Owen et al using a mice model reported FGF-21 promotes weight loss by activating sympathetic nervous activity to the brown adipose tissue.37 However, the relevance of this mechanism in humans remains unclear because human adipose brown tissue is limited and heterogeneous.38
Crosstalk with Other Hormones
Besides Insulin, FGF-21 modulates the activity of other hormones that regulate metabolism. FGF-21 has been reported to increase glucagon receptor expression in the liver, as well as potentiate thyroid hormone receptor signalling in the liver by upregulating thyroid hormone receptor β (THR-β).39,40 These changes result in increased fatty acid oxidation and triglyceride synthesis in the liver.40
FGF-21 results in increased secretion of adiponectin from the adipose tissue.41 This may contribute to its role as a mediator of metabolism, inflammation, and fibrosis.42–44 Among patients with MASH, lower adiponectin levels are associated with insulin resistance, steatosis, and liver inflammation.43–45 Increased levels of adiponectin are associated with increased insulin sensitivity.45 In the liver, adiponectin promotes fatty acid oxidation and inhibits de novo lipogenesis.46 Adiponectin also suppresses Kupffer cell activation.47 Adiponectin has also been shown to shift differentiation of monocytes from anti-inflammatory phenotype of M2-like macrophages and suppress pro-inflammatory macrophages.48 Adiponectin also inhibits HSC activation by leptin, thereby preventing fibrosis.47,48 Figure 1 shows the effect of FGF-21 on various organs.
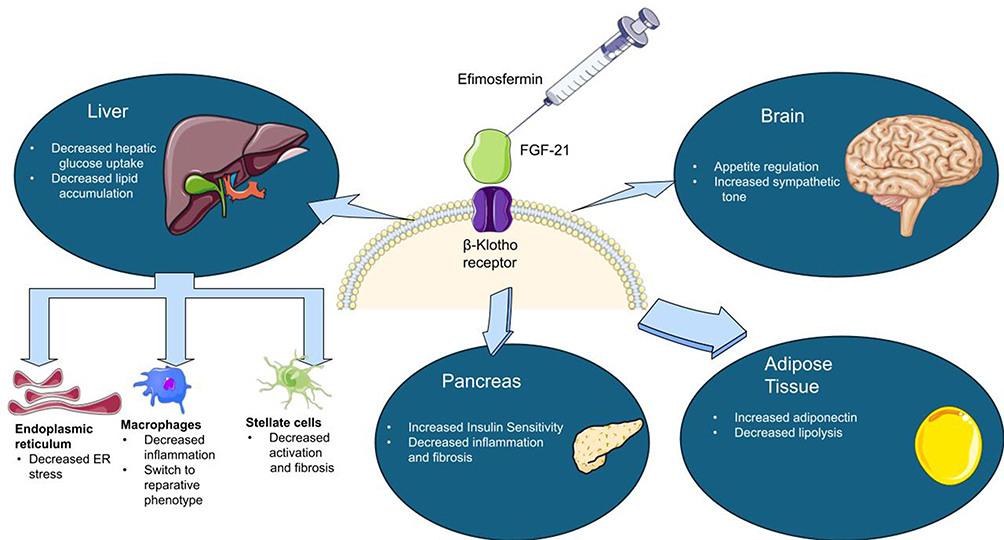 |
Figure 1 The effect of efimosfermin on various organs.40,45,47,48 |
FGF-21 Analogues
As mentioned above, FGF-21 has many beneficial effects, but the main limitation is the short circulating half-life (30 minutes to 2 hours).49 This is primarily due to inactivation and renal clearance. FGF-21 is cleaved by endopeptidase FAP (fibroblast activating protein), which reduces its binding capacity to KLB.50,51 Studies have reported that the FAP is highly expressed in the liver of MASH patients with fibrosis.52 Thus, FGF-21 analogues were engineered to have a longer plasma half-life. Three FGF-21 analogues, efruxifermin, efimosfermin, and pegozafermin, are currently in phase 2/3 clinical trials.53–55 (Table 1). All these therapies have been reported to have a longer half-life than native FGF-21 and are presently being studied with subcutaneous weekly/monthly dosing.
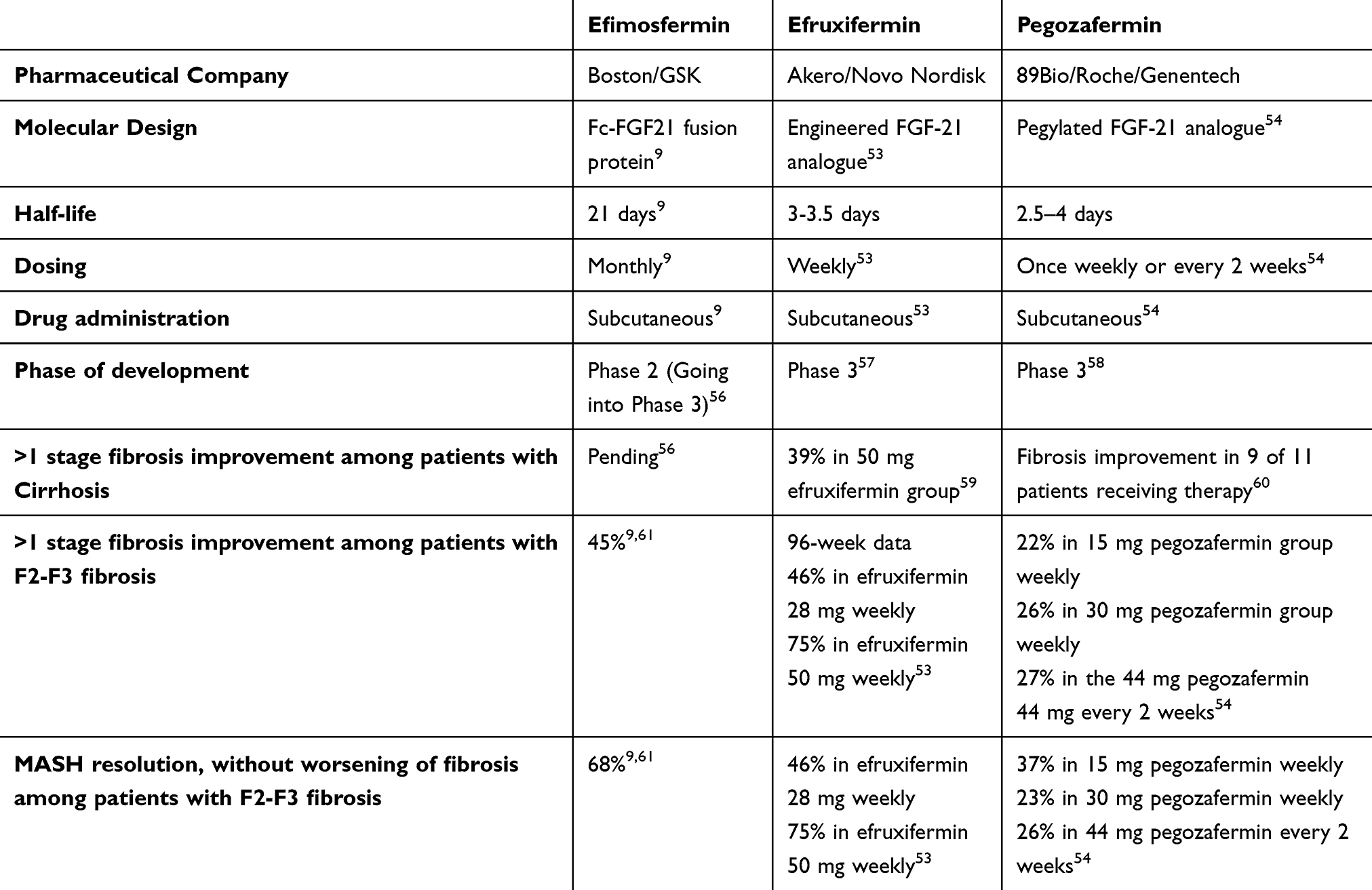 |
Table 1 Comparison of Various FGF-21 Analogues Being Developed for MASH. Phase 2 Study Involving Patients with MASH and F2/F3 Fibrosis |
Efimosfermin
Efimosfermin is a long-acting genetically engineered variant of human FGF-21, stabilized by amino acid substitutions, and fused to the N-terminus of the human IgG Fc domain (Fc-FGF-21).55 This fusion increases thermodynamic stability, reduces proteolytic degradation, and prolongs systemic exposure.55 The half-life of this analogue has been reported to be 21 days.61 While pegozafermin and efruxifermin are being studied for weekly/q2 weeks dosing, the long half-life supports once-a-month dosing for efimosfermin.53–55
Phase 1 Study Involving Hypertriglyceridemia and Obesity
Efimosfermin was initially studied among patients with obesity and hypertriglyceridemia.62 In a phase 1 randomized controlled trial involving 64 participants, the use of efimosfermin was associated with reductions in triglycerides (54%), total cholesterol (7%), and low-density lipoprotein cholesterol (12%), and an increase in high-density lipoprotein cholesterol (36%).62 The study also reported an increase in adiponectin levels.62 An improvement in markers of insulin resistance, including insulin, C-peptide, and the homeostatic model of insulin resistance (HOMA-IR), was also noted.61 Hepatic fat fraction among patients receiving efimosfermin decreased by 56% compared to placebo.62 An improvement in the alanine transaminase (ALT), aspartate transaminase (AST), alkaline phosphatase (ALP), as well as in the non-invasive markers of fibrosis, such as the Enhanced liver fibrosis (ELF) score and N-terminal type III collagen propeptide, was noted.62 This study suggested the potential role of efimosfermin among patients with MASLD, and thus it was studied in phase 2 trials.
Phase 2 Multiple-Dose Study Involving Patients with Obesity and MASH
In this 12-week study, individuals with MASH, aged 18–75 years and BMI>30, were randomly assigned to one of the five cohorts: 75 mg every 4 weeks, 75 mg every 2 weeks, 150 mg every 4 weeks, 150 mg once every 2 weeks, or 300 mg every 4 weeks.55 Of 102 patients, 65 received efimosfermin. At week 12, 47 of 53 patients (89%) receiving efimosfermin had a 30% reduction in the hepatic fat fraction. All 11 patients who received 300 mg q4 weeks had >30% reduction in the fat content. This supported the use of once-a-month dosing and was then assessed in a subsequent study.55
Efimosfermin was assessed in a phase 2a multiple-dose study involving 84 participants with biopsy-confirmed MASH and F2 and F3 fibrosis. Of the 84 participants, 67 patients completed the 24-week biopsy. Patients on efimosfermin therapy had a statistically significant higher rate of MASH resolution without worsening of fibrosis (68% vs 29%, p<0.01), as well as fibrosis improvement without worsening of MASH (45% vs 21%, p<0.01.9 Fibrosis improvement as well as MASH resolution was noted in 39% of the participants, compared to 18% of the patients on placebo (p-0.066).9 Efimosfermin use also resulted in a statistically significant reduction in both the absolute and relative hepatic fat fraction compared to placebo, with 32% of patients on efimosfermin therapy achieving liver fat normalization.9 The open-label extension of this study included 33 participants. Among patients in the open-label extension, 45.5% had >1 stage of fibrosis improvement without worsening of MASH, and 63.4% achieved MASH resolution without worsening of fibrosis.63 A phase 3 trial is currently underway to assess the safety and efficacy of efimosfermin, as once-a-month therapy for patients with MASH.56
Phase 2 Study Among Patients with MASH and Compensated Cirrhosis
A phase 2 randomized, double-blind, placebo-controlled study assessing the safety, efficacy, tolerability, and pharmacokinetics of efimosfermin among patients with MASH and compensated cirrhosis is currently underway, with results pending.59 Efruxifermin, another FGF-21 analogue, was studied in a phase 2b clinical trial involving 181 patients with compensated cirrhosis. The study reported that 29–39% of patients in the efruxifermin group had cirrhosis reversal compared to 14% in the placebo group.60 In another study, use of pegozafermin among patients with cirrhosis was associated with a decrease in fibrosis in 45% of the participants receiving pegozafermin therapy, compared to 0% in the placebo group.64
Safety Data
The most common adverse events reported in the efimosfermin trials are gastrointestinal adverse events and injection-site reactions.55,62,63 In the 12-week phase 2a trial, the most common adverse event noted were gastrointestinal adverse events such as nausea, vomiting, or diarrhea;55 40% of patients receiving efimosfermin therapy experienced gastrointestinal side effects. No treatment-related deaths were recorded. Efimosfermin is administered by subcutaneous injection, and trials have reported injection-site reactions as a common adverse event. In the 24-week phase 2 trial, of the 31 patients receiving efimosfermin, one patient experienced a serious adverse event (biliary colic). Two patients discontinued therapy due to gastrointestinal side effects.9 No cardiovascular or hepatotoxic adverse events were reported in the clinical trials.55,62,63
Considerations for Combination Therapy and Drug Interactions
Gastrointestinal adverse events are common in both currently approved and investigational therapies for MASH. As more therapies, including FGF-21 analogues are approved, the question of combination or sequential therapy is likely to emerge in clinical practice. The timing and sequencing of the agents may be essential to minimize GI intolerance. The phase 2a trial of efimosfermin excluded patients on GLP-1 agonists. Phase 3 studies will include patients who have been on stable GLP-1 therapy for 6 months and results will be important in understanding the role of combination therapy.56
Currently, there is limited data on drug interactions between FGF-21 analogues and other drugs approved for MASLD. As FGF-21 analogues undergo protein degradation and are not metabolized by the cytochrome p450 system (CYP), there is a low likelihood of interactions with drugs that undergo CYP metabolism.50,51 Attention should be paid to patients with MASLD and diabetes, as efimosfermin has been shown to improve glycemic markers, and its concomitant use with anti-diabetic medications carries the theoretical risk of hypoglycemia.63 It is reassuring that the current phase 2 trials did not report hypoglycemia as a side effect. Among patients with hyperlipidemia on statins, the use of FGF-21 analogues will likely result in a significant reduction in low density lipoprotein (LDL) cholesterol and triglycerides, potentially requiring de-escalation of lipid-lowering therapy.61,62 The phase 2a trial included patients on concomitant stable statin therapy for 12 weeks, and no adverse effects have been reported.55
Effect on Cardiovascular Health
One of the significant causes of mortality among patients with MASLD is cardiovascular-related adverse events.6 Thus, it is pertinent to understand the role of efimosfermin on cardiovascular health. By improving insulin sensitivity, hyperlipidemia, and adiponectin levels, efimosfermin may improve cardiovascular outcomes in patients with MASLD.41,45,65 A meta-analysis of randomized controlled trials reported FGF-21 analogues reduce triglycerides and LDL cholesterol, while increasing HDL cholesterol and adiponectin levels.65 FGF-21 may also play have a protective effect on the heart by reducing myocardial cell apoptosis, oxidative stress and fibrosis.66 A study by He et al did not report a correlation between a single-nucleotide polymorphism associated with the gain of FGF-21 mutation and the risk of coronary artery disease and heart failure.67
Phase 2 studies have not reported an adverse cardiovascular safety signal. Studies have reported that patients receiving efimosfermin did not experience adverse changes in blood pressure or heart rate in the trials.55,62,63 To date, no studies have assessed the impact of FGF-21 analogues on major adverse cardiovascular events. Long-term studies evaluating the effect of FGF-21 on major adverse clinical events (MACE) will be beneficial in the future.
Effect on Bone Health
Pre-clinical studies have raised concerns regarding the effect of FGF-21 signalling on bone metabolism.68–70 In an animal model, FGF-21 treatment was shown to inhibit osteoblastogenesis and stimulate adipogenesis in bone marrow, potentially leading to increased bone loss.68 However, another murine model did not report these changes.69 FGF-21 has also been reported to inhibit growth hormone-induced secretion of insulin-like growth factor (IGF-1), another putative mechanism that may result in bone resorption.70
Clinical trials of pegozafermin and efruxifermin, have not shown meaningful change in bone mineral density by dual-energy X-ray absorptiometry (DEXA) (53.54). Currently, the overall clinical evidence is limited, and the phase 2 study of efimosfermin excluded patients with osteoporosis. Given that patients with MASLD are at increased risk of osteoporosis due to metabolic comorbidities, low testosterone levels, and cirrhosis-related bone disease, data on bone safety should remain an essential consideration as longer-duration trials emerge.71 It is possible that DEXA scan may be a recommended part of routine screening among patients receiving FGF-21 analogues, although this will be more clear as these therapies undergo regulatory review. Although efimosfermin has demonstrated a favorable short-term safety profile in early-phase trials, the available data are limited by small sample sizes and short follow-up durations. Longer-term studies are required to completely characterize the bone and cardiovascular safety, as well as the durability of long-term administration. Ongoing Phase 3 trials and post-approval surveillance will be essential to assess the long-term safety profile of efimosfermin across MASH populations.
Combination Therapy
As more drugs are approved for MASH, combination therapy is likely to become an integral component of clinical management for optimal therapeutic benefit, especially with therapies with non-overlapping mechanisms of action. Resmetirom was the first drug approved for this indication, and it acts by selectively targeting hepatic THR-β.4 THR-β signalling regulates bile acid, triglyceride, and cholesterol synthesis, reducing liver fat content.72 Studies have reported that thyroid hormone regulates FGF-21 expression in the liver.72 THR-β activation induces secretion of FGF-21.72 Thus, combining resmetirom with FGF-21 analogues may yield synergistic effects, leading to increased insulin sensitivity, increased adipocyte glucose uptake, and decreased lipolysis and release.
Semaglutide, a GLP-1 agonist is now FDA approved for patients with MASH.5 Thus, combining GLP-1 agonist, with an FGF-21 analogue, may offer complementary benefits. An animal model noted that the absence of liver FGF-21 expression was associated with resistance to liraglutide-induced weight loss.73 The Phase 2 study of efimosfermin did not include patients on concomitant GLP-1 therapy.9 The phase 3 study is currently underway and will include patients who have been on a stable dose of GLP-1 for at least 6 months. This will be beneficial in improving our understanding of combination therapy. A study evaluating the safety and efficacy of efruxifermin as an add-on therapy to GLP-1 agonist reported a similar tolerability profile.74 Albeit a small study, 88% of patients receiving combination therapy had normalization of liver fat content, measured by MRI-PDFF.74 More data are needed to assess the efficacy of this combination.
Future Directions
Efimosfermin has reported promising phase 2 data, meeting liver histology endpoints, while demonstrating a favorable tolerability profile among patients with MASH and F2/F3 fibrosis.9,63 These findings support continued development and further investigation through phase 2 and 3 trials. The current data on efimosfermin comes from clinical trials among patients with F2/F3 fibrosis.9,51 A phase 2 trial assessing the safety and efficacy of the treatment in patients with cirrhosis is currently underway, and the results are awaited to confirm its potential role in cirrhosis.59 Resmetirom is presently being studied in patients with cirrhosis.75 In a phase 2 trial assessing the effect of semaglutide on fibrosis regression in patients with cirrhosis, semaglutide did not significantly improve fibrosis regression, compared to placebo.76 Thus, the phase 2 trial evaluating the efficacy of efimosfermin in patients with cirrhosis will be essential to define its role as a potential antifibrotic agent.59
A Phase 3 trial assessing the impact of efimosfermin in patients with MASH and F2/F3 fibrosis is currently underway.56 If efimosfermin meets the histological endpoints of MASH resolution and fibrosis improvement in subsequent trials with acceptable safety and tolerability it may be receive conditional approval as was achieved for resmetirom and semaglutide. However, to obtain full approval, this medication will need to demonstrate improvement in the clinical outcomes such as liver transplant-free survival, reduction in decompensations, and complications of portal hypertension. Phase 3 trials of efimosfermin and the other FGF-21 analogues are currently ongoing, and the results will inform whether these therapies receive conditional approval, while the clinical outcomes are ongoing.56–58
Efimosfermin and other FGF-21 analogues, if approved, will represent a novel therapeutic option for MASH with significant fibrosis that targets both metabolic improvement and direct anti-fibrotic effect. This drug will be suitable for patients in whom fibrosis regression is the primary therapeutic objective, in patients who are intolerant to weight loss therapy or have not achieved the therapeutic goal of MASH resolution and fibrosis improvement with incretin-based therapies, and in those with lean-MASH. The option of once-a-month therapy may be attractive, if adequate efficacy is demonstrated. Efimosfermin may also be used either in combination or following initial metabolic optimization with GLP-1 agonists. Studies aimed at head-to-head comparisons and combination regimens will be critical for refining patient selection and defining their role within personalised treatment algorithms for MASH. The proposed positioning strategies will remain hypothetical until more data is available.
Regarding the monitoring of efimosfermin effects, non-invasive tests are increasingly used for monitoring patients on therapy. We expect that recommendations regarding monitoring of treatment response with FGF-21 analogues may be similar to the recent expert consensus on monitoring of response among patients with resmetirom.77
Disclosure
Kris V. Kowdley declares grants and/or contracts from Altimmune, Akero therapeutics, Astra Zeneca, Boehringer Ingelheim, Boston Pharmaceuticals, Corcept, 89Bio, Gilead, GlaxoSmithKline, Hanmi, HighTide, Inventiva, Kowa, Madrigal, Mirum and Zydus; royalties/licenses from UpToDate; consulting fees from 89Bio, Akero therapeutics, Boehringer Ingelheim, Corcept, Gilead, GlaxoSmithKline, Inipharm, Ipsen, Kowa, Madrigal, Mirum, Novo Nordisk and Zydus; payment/honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from, Gilead, Ipsen, Madrigal, and Novo Nordisk; stock or stock options for Inipharm. The authors report no other conflicts of interest in this work.
References
1. Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77(4):1335–10. doi:10.1097/HEP.0000000000000004
2. Suresh MG, Mohamed S, Geetha HS, et al. Cardiovascular implications in metabolic dysfunction-associated steatotic liver disease (MASLD): a state-of-the-art review. Korean Circ J. 2025;56:103–130. doi:10.4070/kcj.2025.0212
3. Noureddin M, Vipani A, Bresee C, et al. NASH leading cause of liver transplant in women: updated analysis of indications for liver transplant and ethnic and gender variances. Am J Gastroenterol. 2018;113(11):1649–1659. doi:10.1038/s41395-018-0088-6.
4. Harrison SA, Bedossa P, Guy CD, et al. MAESTRO-NASH investigators. A phase 3, randomized, controlled trial of resmetirom in NASH with liver fibrosis. N Engl J Med. 2024;390(6):497–509. doi:10.1056/NEJMoa2309000.
5. Sanyal AJ, Newsome PN, Kliers I, et al; ESSENCE Study Group. Phase 3 trial of semaglutide in metabolic dysfunction–associated steatohepatitis. N Engl J Med. 2025;392(21):2089–2099. doi:10.1056/NEJMoa2413258.
6. Sanyal AJ, Van Natta ML, Clark J, et al. NASH clinical research network (CRN). Prospective study of outcomes in adults with nonalcoholic fatty liver disease. N Engl J Med. 2021;385(17):1559–1569. doi:10.1056/NEJMoa2029349.
7. Xie T, Leung PS. Fibroblast growth factor 21: a regulator of metabolic disease and health span. Am J Physiol Endocrinol Metab. 2017;313(3):E292–E302. doi:10.1152/ajpendo.00101.2017.
8. Schwabe RF, Tacke F, Sugimoto A, Friedman SL. Antifibrotic therapies for metabolic dysfunction-associated steatotic liver disease. JHEP Rep. 2025;7(8):101421. doi:10.1016/j.jhepr.2025.101421.
9. Danpanichkul P, Aboona MB, Sukphutanan B, et al. Incidence of liver cancer in young adults according to the Global Burden of Disease database 2019. Hepatology. 2024;80(Suppl 4):828–843. [Abstract 5017. Presented at the American Association for the Study of Liver Diseases (AASLD) Liver Meeting; November 2024; San Diego, CA.Ornitz DM, Itoh N]. doi:10.1097/HEP.0000000000000872
10. Ornitz DM, Itoh N. The fibroblast growth factor signaling pathway. Wiley Interdiscip Rev Dev Biol. 2015;4(3):215–266. doi:10.1002/wdev.176.
11. Wu X, Ge H, Lemon B, et al. Separating mitogenic and metabolic activities of fibroblast growth factor 19 (FGF19). Proc Natl Acad Sci U S A. 2010;107(32):14158–14163. doi:10.1073/pnas.1009427107.
12. The human protein atlas. Available from:https://www.proteinatlas.org/ENSG00000134962-KLB/tissue.
13. Johnson RJ, Stenvinkel P, Andrews P, et al. Fructose metabolism as a common evolutionary pathway of survival associated with climate change, food shortage and droughts. J Intern Med. 2020;287(3):252–262. doi:10.1111/joim.12993.
14. Dushay JR, Toschi E, Mitten EK, Fisher FM, Herman MA, Maratos-Flier E. Fructose ingestion acutely stimulates circulating FGF21 levels in humans. Mol Metab. 2015;4(1):51–57. doi:10.1016/j.molmet.2014.09.008.
15. Laeger T, Henagan TM, Albarado DC, et al. FGF21 is an endocrine signal of protein restriction. J Clin Invest. 2014;124(9):3913–3922. doi:10.1172/JCI74915.
16. Harris L-ALS, Smith GI, Patterson BW, et al. Alterations in 3-hydroxyisobutyrate and FGF21 metabolism are associated with protein ingestion–induced insulin resistance. Diabetes. 2017;66(7):1871–1878. doi:10.2337/db16-1475.
17. Jensen-Cody SO, Flippo KH, Claflin KE, et al. FGF21 signals to glutamatergic neurons in the ventromedial hypothalamus to suppress carbohydrate intake. Cell Metab. 2020;32(2):273–286.e6. doi:10.1016/j.cmet.2020.06.008.
18. Søberg S, Sandholt CH, Jespersen NZ, et al. FGF21 is a sugar-induced hormone associated with sweet intake and preference in humans. Cell Metab. 2017;25(5):1045–1053.e6. doi:10.1016/j.cmet.2017.04.009.
19. von Holstein-Rathlou S, BonDurant LD, Peltekian L, et al. FGF21 mediates endocrine control of simple sugar intake and sweet taste preference by the liver. Cell Metab. 2016;23(2):335–343. doi:10.1016/j.cmet.2015.12.003.
20. Kang P, Zhang Y, Zeng D, et al. Fibroblast growth factor 21 levels are associated with perception and neural responses to sweetness in type 2 diabetes mellitus. Diabetes Metab J. 2025;49(4):893–905. doi:10.4093/dmj.2024.0390
21. Pavlic M, Xiao C, Szeto L, Patterson BW, Lewis GF. Insulin acutely inhibits intestinal lipoprotein secretion in humans in part by suppressing plasma free fatty acids. Diabetes. 2010;59(3):580–587. doi:10.2337/db09-1297.
22. Tanaka N, Takahashi S, Zhang Y, et al. Role of fibroblast growth factor 21 in the early stage of NASH induced by methionine- and choline-deficient diet. Biochim Biophys Acta. 2015;1852(7):1242–1252. doi:10.1016/j.bbadis.2015.02.012.
23. Wu L, Pan Q, Wu G, et al. Diverse changes of circulating fibroblast growth factor 21 levels in hepatitis B virus-related diseases. Sci Rep. 2017;7(1):16482. doi:10.1038/s41598-017-16312-6.
24. Ye D, Wang Y, Li H, et al. Fibroblast growth factor 21 protects against Acetaminophen-induced hepatotoxicity by potentiating peroxisome proliferator-activated receptor coactivator protein-1α-mediated antioxidant capacity in mice. Hepatology. 2014;60(3):977–989. doi:10.1002/hep.27060.
25. Chen L, Wang K, Long A, et al. Fasting-induced hormonal regulation of lysosomal function. Cell Res. 2017;27(6):748–763. doi:10.1038/cr.2017.45.
26. Rupérez C, Lerin C, Ferrer-Curriu G, et al. Autophagic control of cardiac steatosis through FGF21 in obesity-associated cardiomyopathy. Int J Cardiol. 2018;260:163–170. doi:10.1016/j.ijcard.2018.02.109
27. Bolotin E, Liao H, Ta TC, et al. Integrated approach for the identification of human hepatocyte nuclear factor 4α target genes using protein binding microarrays. Hepatology. 2010;51(2):642–653. doi:10.1002/hep.23357.
28. Yu Y, He J, Li S, et al. Fibroblast growth factor 21 (FGF21) inhibits macrophage-mediated inflammation by activating Nrf2 and suppressing the NF-κB signaling pathway. Int Immunopharmacol. 2016;38:144–152. doi:10.1016/j.intimp.2016.05.026
29. Le CT, Nguyen G, Park SY, Choi DH, Cho E-H, Mukhopadhyay P. LY2405319, an analog of fibroblast growth factor 21 ameliorates α-smooth muscle actin production through inhibition of the succinate—G-protein couple receptor 91 (GPR91) pathway in mice. PLoS One. 2018;13(2):e0192146. doi:10.1371/journal.pone.0192146.
30. Desai BN, Singhal G, Watanabe M, et al. Fibroblast growth factor 21 (FGF21) is robustly induced by ethanol and has a protective role in ethanol associated liver injury. Mol Metab. 2017;6(11):1395–1406. doi:10.1016/j.molmet.2017.08.004.
31. Opoku YK, Liu Z, Afrifa J, et al. Fibroblast growth factor-21 ameliorates hepatic encephalopathy by activating the STAT3-SOCS3 pathway to inhibit activated hepatic stellate cells. EXCLI J. 2020;19:567–581. doi:10.17179/excli2020-1287
32. Zhang S, Yu D, Wang M, et al. FGF21 attenuates pulmonary fibrogenesis through ameliorating oxidative stress in vivo and in vitro. Biomed Pharmacother. 2018;103:1516–1525. doi:10.1016/j.biopha.2018.03.100
33. Giontella A, Zagkos L, Geybels M, et al. Renoprotective effects of genetically proxied fibroblast growth factor 21: mendelian randomization, proteome-wide and metabolome-wide association study. Metabolism. 2023;145:155616. doi:10.1016/j.metabol.2023.155616
34. Panera N, Meroni M, Longo M, et al. The KLB rs17618244 gene variant is associated with fibrosing MAFLD by promoting hepatic stellate cell activation. EBioMedicine. 2021;65:103249. doi:10.1016/j.ebiom.2021.103249
35. Larsson SC, Michaëlsson K, Mola-Caminal M, Höijer J, Mantzoros CS. Corrigendum to “Genome-wide association and Mendelian randomization study of fibroblast growth factor 21 reveals causal associations with hyperlipidemia and possibly NASH” [Metab Volume 137, December 2022, 155329]. Metabolism. 2023;143:155555. doi:10.1016/j.metabol.2023.155555
36. Rose JP, Morgan DA, Sullivan AI, et al. FGF21 reverses MASH through coordinated actions on the CNS and liver. Cell Metab. 2025;37(7):1515–1529.e6. doi:10.1016/j.cmet.2025.04.014.
37. Owen BM, Ding X, Morgan DA, et al. FGF21 acts centrally to induce sympathetic nerve activity, energy expenditure, and weight loss. Cell Metab. 2014;20(4):670–677. doi:10.1016/j.cmet.2014.07.012.
38. Ruan H-B, Liu F. Developmental and functional heterogeneity of thermogenic adipose tissue. J Mol Cell Biol. 2020;12(10):775–784. doi:10.1093/jmcb/mjaa029
39. Habegger KM, Stemmer K, Cheng C, et al. Fibroblast growth factor 21 mediates specific glucagon actions. Diabetes. 2013;62(5):1453–1463. doi:10.2337/db12-1116
40. Bruinstroop E, van der Spek AH, Boelen A. Role of hepatic deiodinases in thyroid hormone homeostasis and liver metabolism, inflammation, and fibrosis. Eur Thyroid J. 2023;12(3):e220211. doi:10.1530/ETJ-22-0211.
41. Holland WL, Adams AC, Brozinick JT, et al. An FGF21-adiponectin-ceramide axis controls energy expenditure and insulin action in mice. Cell Metab. 2013;17(5):790–797. doi:10.1016/j.cmet.2013.03.019
42. Marangoni RG, Masui Y, Fang F, et al. Adiponectin is an endogenous anti-fibrotic mediator and therapeutic target. Sci Rep. 2017;7(1):4397. doi:10.1038/s41598-017-04162-1
43. Zhao K, Zhang H, Ding W, et al. Adipokines regulate the development and progression of MASLD through organellar oxidative stress. Hepatol Commun. 2025;9(2):e0639. doi:10.1097/HC9.0000000000000639.
44. Pezzino S, Puleo S, Luca T, Castorina M, Castorina S. Adipokine and hepatokines in metabolic dysfunction-associated steatotic liver disease (MASLD): current and developing trends. Biomedicines. 2025;13(8):1854. doi:10.3390/biomedicines13081854.
45. Lin Z, Tian H, Lam KL, et al. Adiponectin mediates the metabolic effects of FGF21 on glucose homeostasis and insulin sensitivity in mice. Cell Metab. 2013;17(5):779–789. doi:10.1016/j.cmet.2013.04.005.
46. Gamberi T, Magherini F, Modesti A, Fiaschi T. Adiponectin signaling pathways in liver diseases. Biomedicines. 2018;6(2):52. doi:10.3390/biomedicines6020052.
47. Luo Y, Liu M. Adiponectin: a versatile player of innate immunity. J Mol Cell Biol. 2016;8(2):120–128. doi:10.1093/jmcb/mjw012.
48. Handy JA, Fu PP, Kumar P, et al. Adiponectin inhibits leptin signalling via multiple mechanisms to exert protective effects against hepatic fibrosis. Biochem J. 2011;440(3):385–395. doi:10.1042/BJ20102148.
49. Geng L, Lam KSL, Xu A. The therapeutic potential of FGF21 in metabolic diseases: from bench to clinic. Nat Rev Endocrinol. 2020;16(11):654–667. doi:10.1038/s41574-020-0386-0.
50. Dunshee DR, Bainbridge TW, Kljavin NM, et al. Fibroblast activation protein cleaves and inactivates fibroblast growth factor 21. J Biol Chem. 2016;291(11):5986–5996. doi:10.1074/jbc.M115.710582.
51. Lee S, Choi J, Mohanty J, et al. Structures of β-klotho reveal a ‘zip code’-like mechanism for endocrine FGF signalling. Nature. 2018;553(7689):501–505. doi:10.1038/nature25010.
52. Zhang J, Li Y. Fibroblast growth factor 21 analogs for treating metabolic disorders. Front Endocrinol. 2015;6:168. doi:10.3389/fendo.2015.00168
53. Noureddin M, Frias JP, Neff GW, et al. Safety and efficacy of once-weekly efruxifermin versus placebo in metabolic dysfunction-associated steatohepatitis (HARMONY): 96-week results from a multicentre, randomised, double-blind, placebo-controlled, phase 2b trial. Lancet. 2025;406(10504):719–730. doi:10.1016/S0140-6736(25)01073-6.
54. Loomba R, Sanyal AJ, Kowdley KV, et al. Randomized, controlled trial of the FGF21 analogue pegozafermin in NASH. N Engl J Med. 2023;389(11):998–1008. doi:10.1056/NEJMoa2304286.
55. Loomba R, Kowdley KV, Rodriguez J, et al. Efimosfermin alfa (BOS-580), a long-acting FGF21 analogue, in participants with phenotypic metabolic dysfunction-associated steatohepatitis: a multicentre, randomised, double-blind, placebo-controlled, phase 2a trial. Lancet Gastroenterol Hepatol. 2025;10(8):734–745. doi:10.1016/S2468-1253(25)00067-6.
56. Available from: https://clinicaltrials.gov/study/NCT07221227.
57. Available from: https://clinicaltrials.gov/study/NCT06215716.
58. Available from: https://clinicaltrials.gov/study/NCT06318169.
59. Available from: https://clinicaltrials.gov/study/NCT06920043.
60. Noureddin M, Rinella ME, Chalasani N, et al. GS-012 Efruxifermin improves fibrosis in participants with compensated cirrhosis due to MASH: results of a 96-week, randomized, doubleblind, placebo-controlled, phase 2b trial (SYMMETRY). Journal of Hepatology. 2025;82(Suppl 1):S8. doi:10.1016/S0168-8278(25)00309-5
61. Once-monthly efimosfermin alfa (BOS-580) in metabolic dysfunction-associated steatohepatitis With F2/F3 fibrosis: results from a 24-week, randomized, double-blind, placebo-controlled, phase 2 trial. Gastroenterol Hepatol. 2024;20(12 Suppl 11):15–16.
62. Rader DJ, Maratos-Flier E, Nguyen A, et al. CLLF580X2102 study team. LLF580, an FGF21 analog, reduces triglycerides and hepatic fat in obese adults with modest hypertriglyceridemia. J Clin Endocrinol Metab. 2022;107(1):e57–e70. doi:10.1210/clinem/dgab624.
63. Noureddin M, Kowdley K, Kutch K, Jeglinski B, Koziel MJ, Loomba R. Once-monthly efimosfermin alfa for up to 48 weeks in metabolic dysfunction-associated steatohepatitis with F2/F3 fibrosis: results from a phase 2 open-label extension study.
64. Loomba R, Sanyal AJ, Kowdley KV, et al. Fibrosis improvement with pegozafermin treatment in MASH patients with F4 fibrosis: analysis from a 24-week randomized, double-blind, placebo-controlled Phase 2 trial (ENLIVEN).
65. Nie Z, Xu J, Liu Y, et al. Effects and safety of FGF21 analogs on glycemic parameters, lipid profiles, and adiponectin in overweight and obese adults: a meta-analysis of randomized controlled trials. Int J Endocrinol. 2025;2025(1):9943228. doi:10.1155/ije/9943228.
66. Zhao Z, Cui X, Liao Z. Mechanism of fibroblast growth factor 21 in cardiac remodeling. Front Cardiovasc Med. 2023;10:1202730. doi:10.3389/fcvm.2023.1202730
67. He Q, Li Y, Yu R, Lin M. Association of FGF21 with metabolic and cardiovascular diseases: a mendelian randomization analysis. Exp Clin Endocrinol Diabetes. 2025;133(5):259–267. doi:10.1055/a-2549-6889.
68. Wei W, Dutchak PA, Wang X, et al. Fibroblast growth factor 21 promotes bone loss by potentiating the effects of peroxisome proliferator-activated receptor γ. Proc Natl Acad Sci U S A. 2012;109(8):3143–3148. doi:10.1073/pnas.1200797109.
69. Li X, Stanislaus S, Asuncion F, et al. FGF21 is not a major mediator for bone homeostasis or metabolic actions of PPARα and PPARγ agonists. J Bone Miner Res. 2017;32(4):834–845. doi:10.1002/jbmr.2936.
70. Inagaki T, Lin VY, Goetz R, Mohammadi M, Mangelsdorf DJ, Kliewer SA. Inhibition of growth hormone signaling by the fasting-induced hormone FGF21. Cell Metab. 2008;8(1):77–83. doi:10.1016/j.cmet.2008.05.006.
71. Khanmohammadi S, Kuchay MS. Effects of metabolic dysfunction-associated steatotic liver disease on bone density and fragility fractures: associations and mechanisms. J Obes Metab Syndr. 2024;33(2):108–120. doi:10.7570/jomes24004.
72. Adams AC, Astapova I, Fisher FM, et al. Thyroid hormone regulates hepatic expression of fibroblast growth factor 21 in a PPARα-dependent manner. J Biol Chem. 285(19):14078–14082. 10.1074/jbc.C110.107375.
73. Le TDV, Fathi P, Watters AB, et al. Fibroblast growth factor-21 is required for weight loss induced by the glucagon-like peptide-1 receptor agonist liraglutide in male mice fed high carbohydrate diets. Mol Metab. 2023;72:101718. doi:10.1016/j.molmet.2023.101718
74. Harrison SA, Frias JP, Lucas KJ, et al. Safety and efficacy of efruxifermin in combination with a GLP-1 receptor agonist in patients with NASH/MASH and type 2 diabetes in a randomized phase 2 study. Clin Gastroenterol Hepatol. 2025;23(1):103–113. doi:10.1016/j.cgh.2024.02.022.
75. Available from: https://clinicaltrials.gov/study/NCT05500222.
76. Loomba R, Abdelmalek MF, Armstrong MJ, et al. Semaglutide 2·4 mg once weekly in patients with non-alcoholic steatohepatitis-related cirrhosis: a randomised, placebo-controlled phase 2 trial. Lancet Gastroenterol Hepatol. 2023;8(6):511–522. doi:10.1016/S2468-1253(23)00068-7
77. Noureddin M, Charlton MR, Harrison SA, et al. Expert panel recommendations: practical clinical applications for initiating and monitoring resmetirom in patients with MASH/NASH and moderate to noncirrhotic advanced fibrosis. Clin Gastroenterol Hepatol. 2024;22(12):2367–2377. doi:10.1016/j.cgh.2024.07.003.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Performance of APRI and FIB-4 Scores Compared to FibroScan: A Cross-Sectional Study in a Black Sub-Saharan African Population
Nsumbu JB, Makulo JR, Mutombo Tshiswaka T, Kisoka Lusunsi C, Nlombi Mbendi C
Hepatic Medicine: Evidence and Research 2025, 17:27-37
Published Date: 15 July 2025
Resmetirom: An Update on Therapy for Metabolic Dysfunction-Associated Steatohepatitis (MASH)
Van Kleef LA, Michel M, Alkhouri N, Brouwer WP, Schattenberg JM
Drug Design, Development and Therapy 2026, 20:559331
Published Date: 17 March 2026