Back to Journals » International Medical Case Reports Journal » Volume 19
Resistant Facial Verruca Plana Treated with a Single-Dose Intramuscular Hepatitis B Vaccine as Immunotherapy in a Child
Authors Aden AI ![]() , Mohamed MM
, Mohamed MM ![]() , Hassan MY
, Hassan MY ![]() , Ali AI
, Ali AI ![]()
Received 1 February 2026
Accepted for publication 11 April 2026
Published 16 April 2026 Volume 2026:19 600078
DOI https://doi.org/10.2147/IMCRJ.S600078
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Abdisalam Ibrahim Aden,1 Mohamed Mukhtar Mohamed,2,3 Mohamed Yaqub Hassan,4 Ahmed Isse Ali1
1Department of Dermatology and Venerology, Mogadishu Somali Turkiye Training and Research Hospital, Mogadishu, Somalia; 2Department of Emergency Medicine, Mogadishu Somali-Turkey Training and Research Hospital, Mogadishu, Somalia; 3Faculty of Medicine and Surgery, Jazeera University, Mogadishu, Somalia; 4Department of Pediatrics, Mogadishu Somali-Turkey Training and Research Hospital, Mogadishu, Somalia
Correspondence: Mohamed Mukhtar Mohamed, Department of Emergency Medicine, Mogadishu Somali Turkey Research and Training Hospital, Jaalle Siyad Street, Mogadishu, Somalia, Tel +252-618810800, Email [email protected]
Background: Facial Verruca plana is a common manifestation of human papillomavirus infection that frequently affects the face of children and adolescents and may be resistant to conventional therapies. Management is particularly challenging in pediatric patients due to lesion persistence, recurrence, and cosmetic concerns that limit the use of destructive modalities. Immunotherapy has emerged as a promising alternative; however, evidence for its use in facial verruca plana remains limited.
Case Presentation: A 9-year-old girl presented with a more than two-year history of multiple facial verruca plana refractory to standard treatments, including topical tretinoin, salicylic acid, and imiquimod. She had no underlying systemic or immunological disease. Clinical examination revealed numerous flat-topped, skin-colored to slightly erythematous papules diffusely involving the face. Laboratory investigations were unremarkable. Following pediatric consultation and informed consent, a single intramuscular hepatitis B vaccine booster was administered as an off-label immunotherapeutic intervention. Clinical improvement was observed within three weeks, with complete resolution of all lesions by six weeks. No adverse effects were reported, and no recurrence was observed during 10 months of follow-up, with sustained remission at 18 months.
Discussion: Immunotherapeutic approaches promote wart clearance through enhancement of cell-mediated immunity. Previous studies of hepatitis B vaccine immunotherapy have largely focused on common and plantar warts and often required repeated or intralesional administration. In contrast, this case demonstrates complete and sustained resolution of facial verruca plana in a pediatric patient following a single intramuscular dose, suggesting a systemic immunomodulatory effect.
Conclusion: Intramuscular hepatitis B vaccination may represent a safe and effective immunotherapeutic option for selected pediatric patients with recalcitrant facial verruca plana. Further controlled studies are required to confirm its efficacy and clinical applicability.
Keywords: verruca plana, hepatitis B vaccine, immunotherapy, pediatric dermatology, human papillomavirus
Introduction
Verruca plana is a benign cutaneous manifestation of human papillomavirus (HPV), most commonly associated with HPV types 3 and 10, and frequently affects the face and extremities of children and adolescents. Clinically, it presents as multiple flat-topped, skin-colored to slightly erythematous papules. Although spontaneous resolution may occur, lesions often persist for prolonged periods and demonstrate a tendency toward recurrence, particularly in pediatric populations.1,2
The management of verruca plana remains challenging. Topical keratolytics, retinoids, cryotherapy, and topical immunomodulators are examples of conventional therapeutic modalities that are frequently used; however, these treatments are frequently linked to incomplete clearance, frequent recurrence, and treatment-related side effects. These difficulties are particularly noticeable in facial lesions, where the use of destructive treatment methods is restricted due to the possibility of scarring and dyspigmentation. As a result, it is still challenging to provide pediatric patients with effective and aesthetically pleasing results.1,2
In recent times, immunotherapy has been investigated as an alternative method for treating stubborn warts, with the goal of boosting the body’s cell-mediated immune response and aiding in the elimination of the virus. Notably, the hepatitis B virus (HBV) vaccine has been identified as a promising immunotherapeutic candidate. It is believed to work by activating systemic immune responses that help remove HPV-infected keratinocytes. Clinical research has shown its efficacy in treating resistant warts when delivered through intralesional or intramuscular injections, highlighting its potential as an immune-modulating treatment.3,4
However, evidence regarding the use of hepatitis B vaccination in facial verruca plana, particularly in pediatric patients, remains limited. Therefore, we report a case of long-standing, treatment-resistant facial verruca plana in a child that showed rapid and complete resolution following a single-dose intramuscular hepatitis B vaccine administered as immunotherapy.
Case Presentation
A 9-year-old girl presented to the Department of dermatology and venerology Mogadishu Somali Turkiye Recep Tayyip Erdogan Training and Research Hospital with persistent plane warts involving multiple areas of the face for more than two years. The lesions were asymptomatic but caused significant cosmetic concern.
She had no history of chronic disease, autoimmune conditions, allergies, or immunodeficiency, and no relevant personal or family history of dermatologic or systemic illness. The patient was otherwise healthy.
Priorly the patient was given treatments included topical tretinoin, salicylic acid preparations (cream and solution), and imiquimod, all used for adequate durations with good adherence without clinical improvement.
On physical examination, the patient was found to have Fitzpatrick skin type V, Multiple flat-topped, skin-colored to slightly erythematous papules diffusely involving the face, more prominent on the left upper facial region as shown in (Figure 1). There were no signs of inflammation, ulceration, or secondary infection. The clinical assessment and clinical findings were consistent with verruca plana.
 |
Figure 1 Multiple flat-topped, skin-colored papules involving the face before treatment. The eye region is covered with a rectangular mask to preserve patient anonymity. |
Given the long duration, facial distribution, and refractoriness to standard therapy, further evaluation was performed. Complete blood count; serum electrolytes, urea, creatinine, and fasting glucose; liver and thyroid function tests; and HIV screening were all within normal limits. Serologic testing demonstrated positive hepatitis B surface antibodies, consistent with prior routine immunization.
Following consultation with a pediatrician and discussion with the patient’s family regarding off-label use, a single intramuscular hepatitis B vaccine booster was administered as an immunotherapeutic intervention.
At three weeks, the patient demonstrated noticeable clinical improvement. By six weeks, there was complete resolution of all facial lesions as shown in (Figure 2).
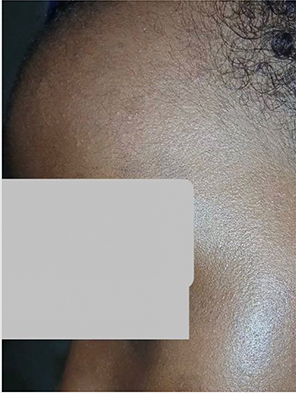 |
Figure 2 Complete resolution of lesions six weeks after intramuscular hepatitis B vaccine booster, with restoration of normal skin texture. The eye region is covered with a rectangular mask to preserve patient anonymity. |
No additional treatments were used during follow-up. The patient was monitored for 10 months, during which no recurrence or adverse local or systemic effects were observed. Extended follow-up confirmed continued remission, with no warts present 18 months after vaccination.
Discussion
Recalcitrant verruca plana, particularly in pediatric patients with facial involvement, represents a distinct clinical challenge compared with common and plantar warts. Although the majority of available literature focuses on these more prevalent wart subtypes, verruca plana is often more resistant to conventional therapies and poses additional management difficulties due to its predilection for cosmetically sensitive areas such as the face. In children, treatment is further complicated by concerns regarding tolerability, safety, and the risk of scarring or dyspigmentation.1,2
Immunotherapy has emerged as an important modality in the management of resistant warts, particularly when conventional therapies fail or are poorly tolerated. Unlike destructive approaches, immunotherapeutic strategies enhance host cell-mediated immunity against human papillomavirus (HPV)-infected keratinocytes, thereby promoting viral clearance. A broad spectrum of immunotherapeutic agents has been investigated, including measles–mumps–rubella (MMR) vaccine, tuberculin purified protein derivative (PPD), and other antigen-based therapies, which act by inducing a delayed-type hypersensitivity response and stimulating systemic immune activation. These approaches have demonstrated the ability to achieve clearance of both treated and distant lesions, reflecting their systemic therapeutic effect.5–7 In addition, systemic immunotherapy has been shown to enhance T-helper-1–mediated immune responses, which are essential for effective viral eradication and sustained remission.1,2
Among emerging immunotherapeutic approaches, the hepatitis B virus (HBV) vaccine has gained increasing attention as a potential treatment for recalcitrant warts. Nofal et al demonstrated that intramuscular administration of the HBV vaccine resulted in higher clearance rates compared with intralesional injection, suggesting a systemic immune-mediated mechanism.3 Similarly, Gharib et al reported that intralesional HBV vaccine is effective and safe in the treatment of resistant plantar warts, supporting its role as an immune-modulating therapy.4
Despite these advances, most available studies have focused on common and plantar warts, with limited data addressing verruca plana, particularly in pediatric populations. This gap is clinically important, as facial verruca plana is often more resistant to treatment and requires approaches that minimize cosmetic sequelae.
Comparison with Previous Studies
Most previous studies evaluating hepatitis B virus (HBV) vaccine therapy have focused on common and plantar warts and have typically required repeated treatment sessions or intralesional administration as shown in Table 1.3,4
 |
Table 1 Reported Use of Hepatitis B Vaccine in Cutaneous Warts |
In contrast, the present case achieved complete resolution with a single intramuscular dose in a pediatric patient with facial verruca plana, indicating a potentially simpler and more patient-friendly therapeutic approach.
The present case highlights several important points. It involves facial verruca plana in a pediatric patient, a subgroup that is underrepresented in current literature. In addition, complete and sustained clearance was achieved following a single intramuscular HBV vaccine booster.
Limitations
This report is limited by its single-case design, which restricts generalizability. Immunological parameters were not assessed. Although spontaneous resolution cannot be entirely excluded, it is unlikely given the prolonged disease duration of more than two years without remission and lack of response to multiple prior therapies.
Conclusion
This case demonstrates complete and sustained resolution of recalcitrant facial verruca plana in a child following a single intramuscular hepatitis B vaccine booster. The findings support the potential role of hepatitis B vaccination as a systemic immunotherapeutic option in selected cases of resistant warts, particularly in pediatric patients with cosmetically sensitive lesions. However, given the limited evidence and the nature of a single case report, further controlled studies are required to confirm efficacy, determine optimal treatment protocols, and establish its role in clinical practice.
Data Sharing Statement
All relevant data of this manuscript and supporting findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval
In our institution, case reports do not need institutional review board (IRB) approval.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Acknowledgment
The authors would like to express their gratitude to Dr Mohamud Mohamed Abdulkadir for his expert clinical insights and valuable contributions during the assessment and management of this case. His guidance greatly assisted in the Case Assessment and the clinical decision-making process. The authors also acknowledge the support of the Department of dermatology and venerology team of Mogadishu Somali Turkiye Recep Tayyip Erdogan Training and Research Hospital for their dedication to patient care.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any funding.
Disclosure
The authors declare no competing interests in this work.
References
1. Mohammed GF, Al-Dhubaibi MS, Bahaj SS, Elneam AIA. Systemic immunotherapy for the treatment of warts: a literature review. J Cosmet Dermatol. 2022;21(11):5532–5. doi:10.1111/jocd.15330
2. Thappa DM, Chiramel MJ. Evolving role of immunotherapy in the treatment of refractory warts. Indian Dermatol Online J. 2016;7(5):364–370. doi:10.4103/2229-5178.190487
3. Nofal A, Elaraby A, Elkholy BM. Intralesional versus intramuscular hepatitis B virus vaccine in the treatment of multiple common warts. Dermatol Surg. 2022;48(11):1178–1184. doi:10.1097/DSS.0000000000003595
4. Gharib K, Taha A, Elradi M. Intralesional Acyclovir versus intralesional Hepatitis-B vaccine in treatment of resistant plantar warts: a randomized controlled trial. Arch Dermatol Res. 2024;316(6):325. doi:10.1007/s00403-024-03001-4
5. Mohta A, Kushwaha RK, Gautam U, Sharma P, Nyati A, Jain SK. A comparative study of the efficacy and safety of intralesional measles, mumps, and rubella vaccine versus intralesional vitamin D3 for the treatment of warts in children. Pediatr Dermatol. 2020;37(5):853–859. doi:10.1111/pde.14280
6. Shaheen MA, Salem SA, Fouad DA, El-Fatah AA. Intralesional tuberculin (PPD) versus measles, mumps, rubella (MMR) vaccine in treatment of multiple warts: a comparative clinical and immunological study. Dermatol Ther. 2015;28(4):194–200. doi:10.1111/dth.12230
7. Chauhan PS, Mahajan VK, Mehta KS, Rawat R, Sharma V. The efficacy and safety of intralesional immunotherapy with measles, mumps, rubella virus vaccine for the treatment of common warts in adults. Indian Dermatol Online J. 2019;10(1):19–26. doi:10.4103/idoj.IDOJ_142_18
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Case of Genital and Extragenital Warts Unresponsive to Immunotherapy Using Measles, Mumps, Rubella Vaccine
Achdiat PA, Yunitasari, Usman HA, Maharani RH
International Medical Case Reports Journal 2023, 16:739-746
Published Date: 15 November 2023
Efficacy and Safety Profile of Tuberculin Protein Purified Derivative Injection As Immunotherapy For the Treatment of Cutaneous and Anogenital Warts: A Review Article
Achdiat PA, Suwarsa O, Hidayat YM, Shafiee MN, Dwiyana RF, Hindritiani R, Sutedja E, Pudjiati SR, Hilmanto D, Dhamayanti M, Parwati I, Maharani RH, Sutedja EK, Avriyanti E, Yunitasari
ImmunoTargets and Therapy 2024, 13:123-150
Published Date: 5 March 2024