Back to Journals » Infection and Drug Resistance » Volume 16
Resistance Transition of Pseudomonas aeruginosa in SARS-CoV-2-Uninfected Hospitalized Patients in the Pandemic
Authors Xia J, Lu L, Zhao KL, Zeng QL ![]()
Received 28 May 2023
Accepted for publication 31 August 2023
Published 16 October 2023 Volume 2023:16 Pages 6717—6724
DOI https://doi.org/10.2147/IDR.S423167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Jin Xia,1 Lan Lu,2 Ke-Lei Zhao,2 Qiang-Lin Zeng1
1Department of Respiratory and Critical Care Medicine, Affiliated Hospital/Clinical College of Chengdu University, Chengdu, Sichuan, 610081, People’s Republic of China; 2Antibiotics Research and Re-Evaluation Key Laboratory of Sichuan Province, Chengdu University, Chengdu, Sichuan, 610106, People’s Republic of China
Correspondence: Ke-Lei Zhao, Antibiotics Research and Re-evaluation Key Laboratory of Sichuan Province, Chengdu University, Chengdu, Sichuan, 610106, People’s Republic of China, Tel +86 173 401 901 21, Email [email protected] Qiang-Lin Zeng, Department of Respiratory and Critical Care Medicine, Affiliated Hospital/Clinical college of Chengdu University, Chengdu, Sichuan, 610081, People’s Republic of China, Email [email protected]
Objective: To investigate the impact of coronavirus disease 2019 (COVID-19) specified preventive and control measures on the distribution and resistance transition of Pseudomonas aeruginosa (P. aeruginosa) in uninfected hospitalized patients during the pandemic.
Methods: This retrospective study retrieved data from 316 P. aeruginosa isolates in the year pre-COVID-19 (n=131) pandemic and the year under COVID-19 specified preventive and control (post-pandemic year, n=185), compared the general characteristics, laboratory results, and antimicrobial susceptibility tests of P. aeruginosa between the two groups.
Results: Compared with the pre-pandemic year, the isolation rate of P. aeruginosa (14.35% vs 22.31%, P< 0.001) increased, while the rate of drug resistant P. aeruginosa decreased significantly (29.77% vs 19.45%, P< 0.001) in the post-pandemic year; Prescription of β-Lactams (30.5% vs 50.0%, P< 0.01) also increased significantly. The resistance rates of P. aeruginosa isolates to ceftazidime (P< 0.01), ciprofloxacin (P< 0.01), and gentamicin (P< 0.001) increased, whereas the resistance rates to piperacillin/tazobactam (P< 0.01) and imipenem (P< 0.05) decreased significantly.
Conclusion: The COVID-19 specified preventive and control measures have influenced the distribution and resistance transition of P. aeruginosa, further verifications are needed in future research.
Keywords: COVID-19, Pseudomonas aeruginosa, isolation rate, drug resistance
Introduction
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has led to a significant global impact and is a major public health issue.1,2 The COVID-19 pandemic has caused a series of public health emergencies worldwide, and antimicrobial resistance (AMR) transition has become an unforeseen and unavoidable consequence.3 In the early stage of the pandemic, healthcare authorities in China managed to control the pandemic rapidly and effectively by adopting enhanced preventive measures, including designating specific hospitals to treat and manage patients with COVID-19 and guiding other ordinary hospitals to recruit systematic specified preventive and control measures (e.g. enhanced environmental cleaning and disinfection).4 However, these measures may also bring about changes in the hospital environment, including affecting the distribution of other pathogens and AMR from clinical isolates.
Pseudomonas aeruginosa (P. aeruginosa) is a ubiquitous gram-negative bacterium and a leading cause of chronic respiratory infections in immunocompromised patients, in the hospital environment, P. aeruginosa is a significant concern due to its ability to cause infections, particularly in vulnerable patients, and its propensity for antibiotic resistance.5 In China, the COVID-19 preventive measures, while primarily aimed at controlling the spread of the SARS-CoV-2 virus, could also presented challenges and considerations of antimicrobial resistance, including direct and indirect impacts on P. aeruginosa drug resistance.6 However, the evidence regarding the impact of these measures on the distribution and resistance transition of P. aeruginosa in uninfected hospitalized patients remains limited.7 This study examines the impact of COVID-19-specific preventive and control measures on the distribution and resistance patterns of P. aeruginosa in hospitalized patients who were not infected with COVID-19.
Materials and Methods
Study Design and Data Source
This retrospective study was performed in the Department of Respiratory and Critical Care Medicine, Affiliated Hospital of Chengdu University, a general teaching hospital in southwest China. The research period was from the year before the COVID-19 pandemic (pre pandemic year, January 2019-December 2019) and the first year of regular epidemic prevention and control (post pandemic year) from May 2020 to April 2021. The time breakpoint of outbreak and control was set as an announcement of measures for regular COVID-19 epidemic prevention and control by the healthcare authority in a meeting held on April 30, 2020.8
We included all P. aeruginosa positive patients, and excluded patients with P. aeruginosa negative cultures, non-bacterial cultures, and patients with incomplete information. The MicroScan Walkaway 40 automatic microbial analysis system was used for strain identification and antimicrobial susceptibility testing. Data were collected based on hospital laboratory microbiological data from the WHONET microbiology laboratory database, which compiles identification number, demographics, specimen type, and antibiotic susceptibility. The analysis was performed under the condition of one isolate per patient from the same hospitalization period. The quality control strain of P. aeruginosa was ATCC27853. The antimicrobial susceptibility test results were determined in accordance with the latest CLSI criteria (as applicable each year).
Measures of Variables
The following data were collected from the electronic medical record system: demographic variables: age and sex; clinical variables: smoking history, main diagnosis (respiratory diseases), main comorbidities (cardiovascular disease, liver disease, nervous diseases, kidney disease, diabetes mellitus, and cancers), proportion of patients prescribed antibiotic treatment (intravenous or oral administration) and joint antibiotic treatment (combined administration of at least two types of antibiotics via intravenous or oral administration), and proportion of patients administered short-term systemic corticosteroids (intravenous or oral administration) during hospitalization; laboratory variables: leukocyte count, hypersensitive C-reactive protein (hs-CRP) levels, and antimicrobial susceptibility tests of P. aeruginosa.
Definition
Definition of pre-pandemic and post-pandemic: The pre-pandemic year: the year before the COVID-19 pandemic, January 01, 2019-December 31, 2019); The post-pandemic year: the post-pandemic year was defined as the year of regular epidemic prevention and control, at May 01, 2020-April 30, 2021, this time breakpoint of outbreak and control was settled as an announcement of measures on regular COVID-19 epidemic prevention and control by the healthcare authority in a meeting held on April 30, 2020. In the post pandemic year, health management authorities adopted extensive, stringent, and thorough containment measures. The healthcare-associated infection control branch of the Chinese Preventive Medicine Association (CPMA) and healthcare-associated infection management committee of the Chinese Hospital Association (CHA) have offered expert consensus to prevent healthcare-associated SARS-COV-2 infection in health care workers.4 The hospital recruited systematic specified preventive and control measures under the guidance of such policies from various aspects of hospital patients, healthcare workers, equipment, material, and environment, which were obviously different from those in the pre-pandemic year. Regularly, routine cleaning and disinfection of touched surfaces are performed to ensure that all areas of the environment are regularly cleaned to a satisfactory standard for COVID-19 prevention.9
Definition of susceptible (S), intermediate (I) and resistant (R): Briefly, a threshold-based assessment of the degree of drug effectiveness was characterized as follows: S, susceptible; the P. aeruginosa strain is susceptible to a given antibiotic when it is inhibited in vitro by a concentration of this drug that is associated with a high likelihood of therapeutic success. I: intermediate: The P. aeruginosa response to a given antibiotic is intermediate when inhibited in vitro by a concentration of this drug that is associated with an uncertain therapeutic effect. R: resistant; the P. aeruginosa strain is resistant to a given antibiotic when inhibited in vitro by a concentration of this drug that is associated with a high likelihood of therapeutic failure.11
Data Analysis
Continuous variables were presented as means with standard deviations for normally distributed variables and as medians (interquartile range [IQR]) for non-normally distributed variables. For categorical variables, data are presented as percentages. Student’s t-test was used to compare continuous parametric variables, while the Mann–Whitney-U test was used to compare continuous non-parametric variables. The chi-square test and Fisher’s exact test were used to compare categorical data. Statistical significance was set at P < 0.05.
Results
General Characteristics
After removing repeated samples from the same patients during the same hospitalization period, 913 bacterial strains from 5386 valid samples were obtained, and 131 P. aeruginosa positive patients were included in the pre-pandemic period, 829 bacterial strains from 3622 valid samples were obtained, and 185 P. aeruginosa positive patients were included in the post-pandemic period. The distribution of specimens in valid samples is listed in Supplemental Table 1, as compared to the pre-pandemic year, the rate of blood samples significantly decreased (15.83% vs 11.68%, P=0.006), while that of urine samples increased significantly (3.88% vs 6.74%, P<0.001) in the post-pandemic year. The distribution of pathogens of bacterial strains is listed in Supplemental Table 2, the isolate rate of P. aeruginosa increased significantly during the post-pandemic period (14.35% vs 22.31%, P<0.001). Table 1 shows the demographics, main diagnosis of respiratory diseases, comorbidities, laboratories, clinical symptoms and signs, the following indicators were significantly different between patients from the pre-pandemic year and post-pandemic year: laboratories: leukocyte (P<0.001), eosinophils (P<0.001), neutrophils (P<0.001), and lymphocytes (P<0.001), basophils (P<0.001) and hs-CRP levels (P<0.01).
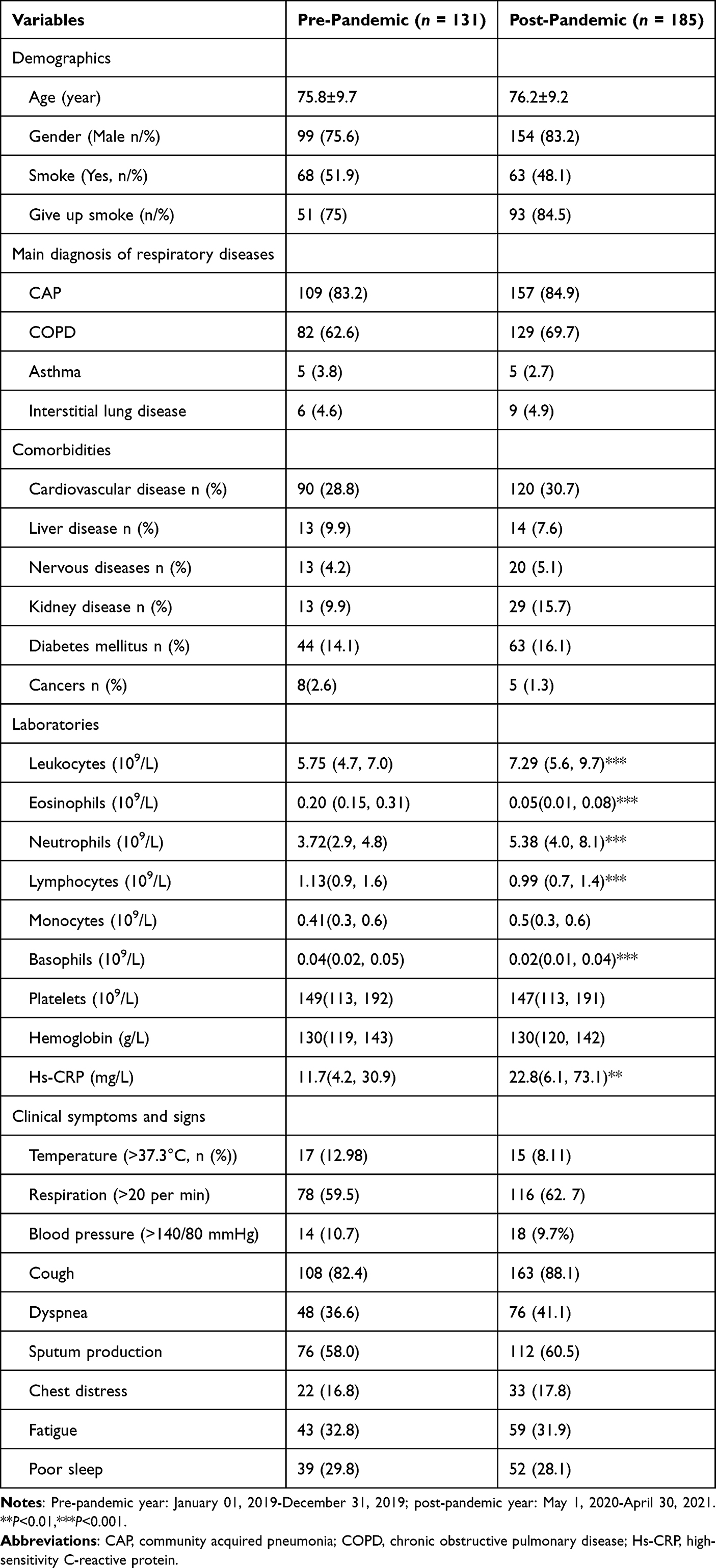 |
Table 1 Characteristics of P. aeruginosa Positive Patients in Pre- and Post-Pandemic Periods |
Resistance Transition of P. aeruginosa
According the summary of prescription of antibiotics by types, the prescription of β-Lactams (30.5% vs 50.0%, OR=2.275, 95% confidence interval: 1.421–3.463. P<0.01) increased significantly in the post-pandemic years (Table 2 and Figure 1). The distribution of specimens in P. aeruginosa isolates is listed in Supplemental Table 3, compared to the pre-pandemic period, the rate of drug resistant P. aeruginosa decreased significantly from (39 (29.77%) vs 36 (19.45%), P<0.001) in the post-pandemic period. The resistance of resistant P. aeruginosa profiles are shown in Table 3, the resistant rates of P. aeruginosa isolates to ceftazidime (P<0.01), ciprofloxacin (P<0.01), and gentamicin (P<0.001) increased, whereas the resistance rates to piperacillin/tazobactam (P<0.01) and imipenem (P<0.05) decreased significantly.
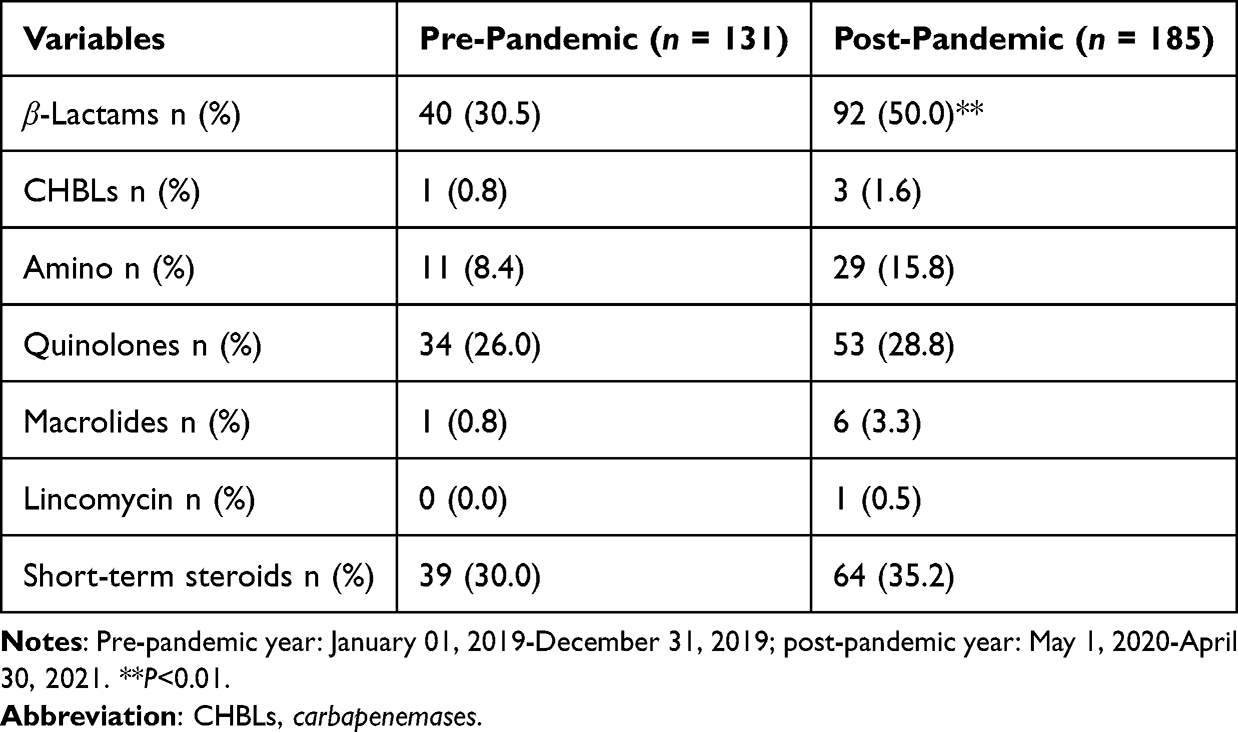 |
Table 2 Summary of Antimicrobic Administrations in P. aeruginosa Positive Patients |
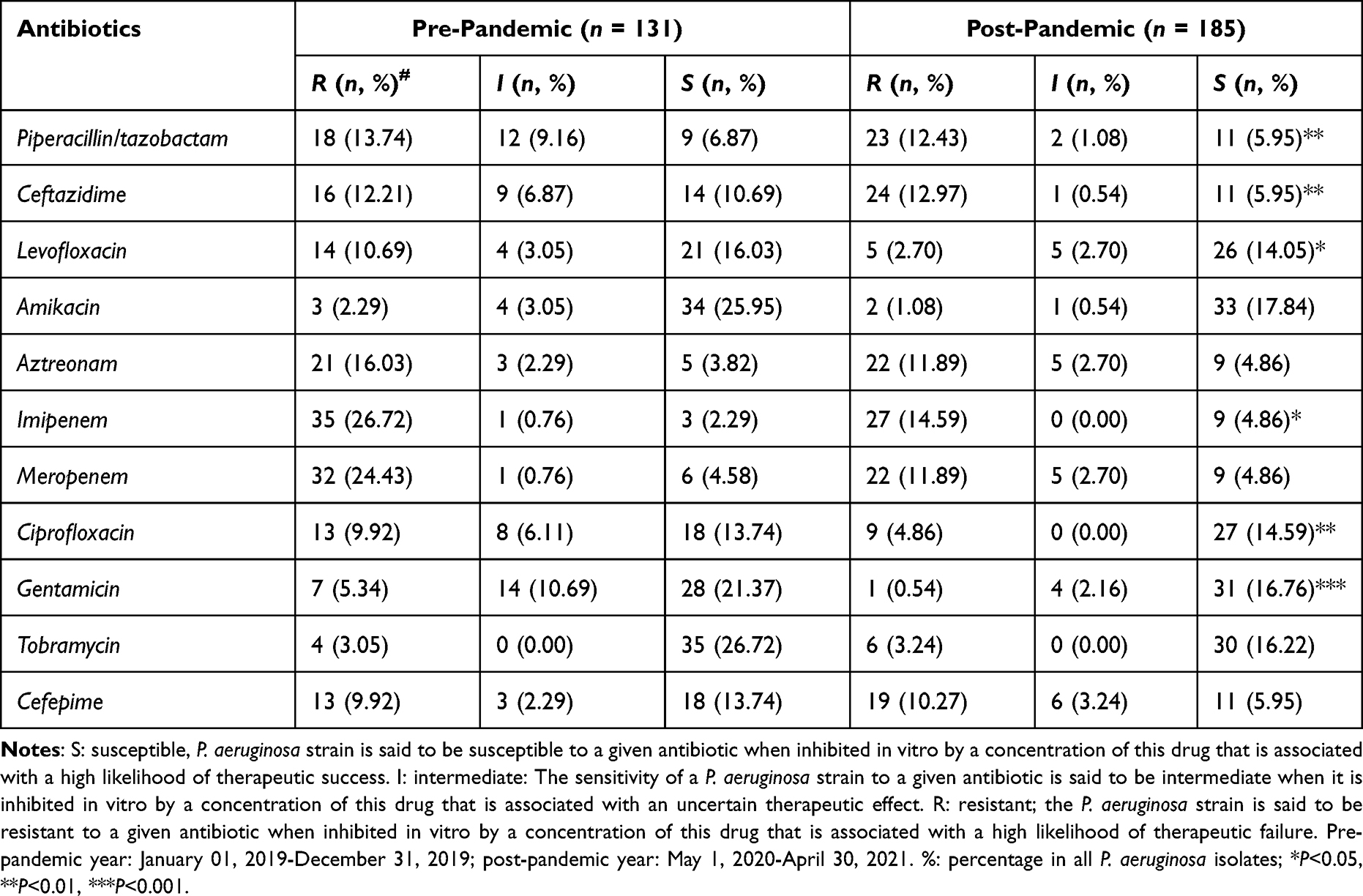 |
Table 3 Transition of Antimicrobial Resistance of P. aeruginosa |
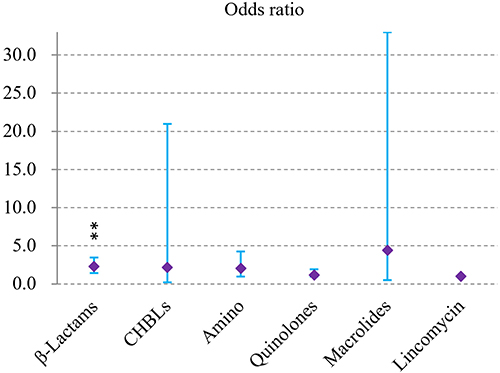 |
Figure 1 Odds ratio of a patient receive antimicrobial administration (by types) in the post-pandemic year (vs the pre-pandemic year); **P<0.01. Abbreviation: CHBLs, carbapenemases. |
Discussion
In recent years, the spread of P. aeruginosa worldwide has become a public health threat.12 By comparing clinical isolates during the pandemic year to the time before, this study examined the changes of isolation rate and resistance transition of P. aeruginosa in SARS-CoV-2-uninfected hospitalized patients in respiratory ward under COVID-19 specified preventive and control measures. P. aeruginosa is the secondary causative pathogen of infections in COVID-19 patients,13 and was ranked fourth in the strain distribution of major clinical isolates in 2020 in another study in China.14 In this study, the isolation rate of P. aeruginosa in uninfected patients, which ranked third (14.35% among 913 bacterial isolates) in the pre-pandemic year, was the leading pathogen among the 829 bacterial isolates (22.31%) in the post-pandemic year, consistent with a previous study, in that study, an increasing trend of P. aeruginosa isolates was observed.7
The pandemic has been reported to influence the use of antimicrobials and antimicrobial resistance in COVID patients co-infected with P. aeruginosa.14 In this study, the resistant rates of P. aeruginosa significantly increased to ceftazidime, ciprofloxacin, and gentamicin, in contrast, resistant rates decreased significantly to piperacillin/tazobactam and imipenem. As reported by Gysin et al,15 drug resistance in P. aeruginosa isolates was high for piperacillin/tazobactam, cefepime, ceftazidime and meropenem, since the evidence specifically examining changes in P. aeruginosa resistance among uninfected patients under these conditions are limited, the diversity of resistance to P. aeruginosa may varied in clinical settings, practice patterns, further research is warranted to quantify this phenomenon.
The COVID-19 pandemic has profound effects on the presentation of antibiotic prescription.16 A reported 72% of COVID-19 patients in hospitals received antimicrobial agents, even though only 8% had bacterial or fungal co-infections.17 In this study, the summary of antibiotic use showed an increasing trend in β-Lactams prescription (OR=2.275), which was in accordance with a previous study that reported an increased trend of resistance of P. aeruginosa to antibiotics due to inappropriate use of antibiotics.18
According to the WHO released list of antibiotic-resistant pathogens, P. aeruginosa was included in the “critical” category among a catalog of 12 families of “priority pathogens” that pose the greatest threat to human health.19 The change of isolation rate and transition of P. aeruginosa in this study showed that resistance might be associated with the change in hospitalization in the respiratory department forced by agency-regulated epidemic prevention and control measures in the post-pandemic period, these findings are important for understanding the current situation of resistance trends of uninfected patients, as well as for establishing better guidelines for preventing the dissemination of antimicrobial resistance. In addition, the implementation of infection prevention and control measures has the potential to become a double-edged sword with improper use of antibiotics, causing short-term changes in pathogens and drug resistance.20 These findings also advocate the need for adequate changes in antimicrobial stewardship implemented by health authorities, as well as appropriate prescription and optimal utilization of antimicrobials by physicians in future clinical practice.
This study has several limitations. First, this is a single-center retrospective study with limited data sources and small samples; thus, the analytical results need to be further verified by multicenter and large-scale research. Second, given the special situation in the pandemic, we collected information of P. aeruginosa isolates in two periods, besides the temporal changes caused by preventive and protective measures, resistance transition of P. aeruginosa may be influenced by other unknown factors such as different P. aeruginosa variants, patient-specified clinical interventions, varied public health dynamics. Third, given the retrospective nature, the high-risk clones can be found in hospitals but may not identified in this study, there is a need to expand the surveillance with whole genome analyses to investigate determinants and evolution of the pathogen.
Conclusion
The COVID-19 specified preventive and control measures have influenced the distribution and resistance transition of P. aeruginosa, further verifications are needed in future research.
Abbreviations
A. baumannii, Acinetobacter baumannii; AMR, antimicrobial resistance; CHA, Chinese Hospital Association; CLSI, Clinical and Laboratory Standards Institute; COVID-19, coronavirus disease 2019; CPMA, Chinese Preventive Medicine Association; E. coli, Escherichia coli; K. pneumoniae, Klebsiella pneumoniae; MIC, minimal inhibitory concentration; P. aeruginosa, Pseudomonas aeruginosa.
Data Sharing Statement
All the findings are available from the corresponding author upon request. All relevant data have been included in the manuscript.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki of the World Medical Congress and the Measures for Ethical Review of Biomedical Research Involving Human Beings issued by the National Health and Family Planning Commission of the People’s Republic of China. This study was approved by the Affiliated Hospital of Chengdu University (NO. PJ-2020-021-03 (2nd version updated at January 9, 2023)). The research only uses the previous medical record information and has removed the relevant personal information of the subject, which will not cause risks to the subject and will not have adverse effects on the rights and health of the subject, so the requirement for informed consent was waived owing to the retrospective nature of the study. We will make every effort to protect the privacy and personal information of the subject’s personal medical data within the scope permitted by law.
Acknowledgments
The authors gratefully acknowledge Dr. Yamei Zhang for her constructive comments and assistance during the review response process of this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Antibiotics Research and Re-evaluation Key Laboratory of Sichuan Province (ARRLKF21-06), the Research Project of Sichuan Medical Association (No. S21055), the Educational Reform Research Projects of Chengdu University (CDJGB2019088 and DJGB2019100), and the Innovation Foundation of The Affiliated Hospital of Chengdu University (No. CDFYCX202209).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Meskini M, Rezghi Rami M, Maroofi P, Ghosh S, Siadat SD, Sheikhpour M. An overview on the epidemiology and Immunology of COVID-19. J Infect Public Health. 2021;14(10):1284–1298. doi:10.1016/j.jiph.2021.07.021
2. Pollard CA, Morran MP, Nestor-Kalinoski AL. The COVID-19 pandemic: a global health crisis. Physiol Genomics. 2020;52(11):549–557. doi:10.1152/physiolgenomics.00089.2020
3. Lai CC, Chen SY, Ko WC, Hsueh PR. Increased antimicrobial resistance during the COVID-19 pandemic. Int J Antimicrob Agents. 2021;57(4):106324. doi:10.1016/j.ijantimicag.2021.106324
4. Li CH, Huang X, Cai M, Chen P. Expert consensus on personal protection in different regional posts of medical institutions during COVID-19 epidemic period. Chin J Infect Control. 2020;19(3):198–213.
5. Qin S, Xiao W, Zhou C, et al. Pseudomonas aeruginosa: pathogenesis, virulence factors, antibiotic resistance, interaction with host, technology advances and emerging therapeutics. Signal Transduct Target Ther. 2022;7(1):199. doi:10.1038/s41392-022-01056-1
6. Wang Z, Yu M, Lin L. The emerging antimicrobial resistance crisis during the COVID-19 surge in China. Lancet Microbe. 2023;4(5):e290–e291. doi:10.1016/S2666-5247(23)00038-1
7. Mesquita GP, Costa MCC, Silva MA, et al. Antimicrobial resistance of Pseudomonas aeruginosa isolated from patients with pneumonia during the COVID-19 pandemic and pre-pandemic periods in Northeast Brazil. Braz J Med Biol Res. 2023;56:e12726. doi:10.1590/1414-431x2023e12726
8. Chinese govt stresses regular epidemic control; 2020. Available from: http://english.www.gov.cn/premier/news/202004/30/content_WS5eaad5e8c6d0b3f0e9496ca2.html.
9. Bai YL, Liu YX, Feng D, Gao Y. Practical management of outpatient, emergency department and hospitalized patients in large scale general hospital during COVID-19 epidemic. Chin J Nosocomiol. 2020;30(8):1135–1140.
10. Rodloff A, Bauer T, Ewig S, Kujath P, Muller E. Susceptible, intermediate, and resistant - The intensity of antibiotic action. Dtsch Arztebl Int. 2008;105(39):657–662. doi:10.3238/arztebl.2008.0657
11. Subedi D, Vijay AK, Willcox M. Overview of mechanisms of antibiotic resistance in Pseudomonas aeruginosa: an ocular perspective. Clin Exp Optom. 2018;101(2):162–171. doi:10.1111/cxo.12621
12. Qu J, Cai Z, Liu Y, et al. Persistent bacterial coinfection of a COVID-19 patient caused by a genetically adapted pseudomonas aeruginosa chronic colonizer. Front Cell Infect Microbiol. 2021;11:641920. doi:10.3389/fcimb.2021.641920
13. Hu FP, Guo Y, Zhu DS, Wang F, Jiang XF, Xu YC. CHINET surveillance of bacterial resistance: results of 2020. Chin J Infect Chemother. 2021;21(4):377–387.
14. Kariyawasam RM, Julien DA, Jelinski DC, et al. Antimicrobial resistance (AMR) in COVID-19 patients: a systematic review and meta-analysis (November 2019-June 2021). Antimicrob Resist Infect Control. 2022;11(1):45. doi:10.1186/s13756-022-01085-z
15. Gysin M, Acevedo CT, Haldimann K, et al. Antimicrobial susceptibility patterns of respiratory Gram-negative bacterial isolates from COVID-19 patients in Switzerland. Ann Clin Microbiol Antimicrob. 2021;20(1):64. doi:10.1186/s12941-021-00468-1
16. van de Pol AC, Boeijen JA, Venekamp RP, et al. Impact of the COVID-19 pandemic on antibiotic prescribing for common infections in the Netherlands: a primary care-based observational cohort study. Antibiotics. 2021;10(2):196. doi:10.3390/antibiotics10020196
17. Getahun H, Smith I, Trivedi K, Paulin S, Balkhy HH. Tackling antimicrobial resistance in the COVID-19 pandemic. Bull World Health Organ. 2020;98(7):442. doi:10.2471/BLT.20.268573
18. Botelho J, Grosso F, Peixe L. Antibiotic resistance in Pseudomonas aeruginosa - Mechanisms, epidemiology and evolution. Drug Resist Updat. 2019;44:100640. doi:10.1016/j.drup.2019.07.002
19. Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318–327. doi:10.1016/S1473-3099(17)30753-3
20. Rawson TM, Ming D, Ahmad R, Moore LSP, Holmes AH. Antimicrobial use, drug-resistant infections and COVID-19. Nature Reviews Microbiology. 2020;18(8):409–410. doi:10.1038/s41579-020-0395-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Antimicrobial Resistance Pattern of Pseudomonas aeruginosa: An 11-Year Experience in a Tertiary Care Hospital in Makkah, Saudi Arabia
Momenah AM, Bakri RA, Jalal NA, Ashgar SS, Felemban RF, Bantun F, Hariri SH, Barhameen AA, Faidah H, AL-Said HM
Infection and Drug Resistance 2023, 16:4113-4122
Published Date: 26 June 2023
Microbial Keratitis Before, During and After the COVID-19 Pandemic, and the Role of Contact Lens Wear and Hand Hygiene
Randag AC, Wellens L, Kazemian N, Schimmer B, van Rooij J
Clinical Ophthalmology 2025, 19:1033-1043
Published Date: 21 March 2025