Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Reshaping Smart Pharmacy in TCM Hospitals via High-Reliability Organization Theory
Authors Cai T, Yao W, Yan X, Weng Y, Zhang J ![]() , Wang L, Wang W, Zhan W, Wang J, Jin J, Shi Z
, Wang L, Wang W, Zhan W, Wang J, Jin J, Shi Z
Received 6 January 2026
Accepted for publication 25 June 2026
Published 10 July 2026 Volume 2026:19 594106
DOI https://doi.org/10.2147/JMDH.S594106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Pavani Rangachari
Tiantian Cai, Wendong Yao, Xingxing Yan, Yayun Weng, Jianjun Zhang, Lanyu Wang, Weiling Wang, Weijiang Zhan, Jianping Wang, Juan Jin, Zheng Shi
Department of pharmacy, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, 310003, People’s Republic of China
Correspondence: Juan Jin, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), No. 54 Youdian Road, Shangcheng District, Hangzhou, 310003, People’s Republic of China, Email [email protected] Zheng Shi, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), No. 54 Youdian Road, Shangcheng District, Hangzhou, 310003, People’s Republic of China, Email [email protected]
Background: The advent of digital intelligence technologies has offered innovative solutions for drug data mining and efficacy prediction, facilitated the development of clinical pharmacy information systems, and enabled intelligent decision support for rational medication use. Nevertheless, current technological innovations and application studies have yet to establish a systematic framework for the comprehensive management and application of pharmaceutical services. In particular, pharmacy services in traditional Chinese medicine (TCM) hospitals remain relatively underdeveloped due to the distinctive characteristics of TCM.
Aim: Based on high-reliability organization theory, we construct an intelligent pharmaceutical service system with TCM characteristics to guarantee operational safety and reliability, and implement digital and intelligent management for pharmaceutical services.
Methods: The present study constructs a smart pharmaceutical service system with distinct TCM characteristics, grounded in HRO theory. Targeting the operational characteristics and service demands of clinical pharmacy in public hospitals, we established a digital intelligent pharmaceutical system with a “one center, two supports, six platforms” architecture under the guidance of high-reliability organization theory. Relevant evaluation indicators were compared pre- and post-implementation of the system, covering drug return rate, average approval turnaround time, clinician satisfaction, medical record compliance rate, PPI rational use rate, appeal review success rate of clinicians, proportion of ADR reports with proactive warnings, and monthly ADR reporting volume.
Results: Grounded in High Reliability Organization Theory, the smart pharmacy system integrates the functional modules of six major platforms and the unique strengths of traditional Chinese medicine. This system encompasses the entire spectrum of pharmaceutical service processes, including pre-event prevention, in-event intervention, and post-event evaluation, thereby forming a complete closed-loop quality management system. The Internet-based Hospital Quality Control Platform reduced the annual rates of refunds and drug returns. The Multidimensional Tiered Drug Scientific Management Platform shortened the average approval processing time and improved clinical physicians’ satisfaction. The Personalized Pharmacy Clinic Workstation enhanced the compliance rate of medical record quality control. The Homogenized Evaluation System increased the rational usage rate of proton pump inhibitors (PPIs) while reducing the success rate of clinical physicians’ appeals against evaluation results. The Adverse Drug Reaction (ADR) System raised the proportion of proactive monthly ADR reports as well as the total volume of ADR reporting.
Conclusion: By coordinating six major platforms, the smart-intelligent system achieves full-process and standardized management of pharmaceutical services. This framework not only enhances the quality and efficiency of pharmaceutical services in TCM (integrated) hospitals but also provides both theoretical underpinnings and practical pathways for the transformation of pharmaceutical service models.
Keywords: smart pharmaceutical services, high-reliability organization theory, traditional Chinese medicine hospitals, digital intelligence technology
Introduction
In 2021, six national departments, including the National Health Commission of China, jointly issued the Notice on Strengthening Pharmaceutical Management in Medical Institutions and Promoting Rational Drug Use.1 The document explicitly emphasized the need to strengthen the allocation of clinical pharmacists and develop specialized pharmaceutical services based on patient needs and the characteristics of clinical treatment and further noted thatclinical pharmacists should actively participate in clinical treatment, providing services such as prescription review for inpatients, involvement in treatment planning, medication monitoring and evaluation, as well as patient medication education.2 In addition, it advocated for the proactive and sustainable development of “Internet Plus Pharmaceutical Services.” With the deepening of healthcare reform in China, pharmaceutical services have increasingly centered on patient-oriented care, characterized by multidisciplinary collaboration among healthcare professionals and the adoption of modern technologies to improve service quality and efficiency.3 The transformation of pharmaceutical services, therefore, requires continuous innovation in technology, service models, and research methodologies.4 This transformation has become a key requirement for advancing the Healthy China strategy and for promoting pharmaceutical development within the framework of healthcare reform.5
In recent years, the rapid advancement of digital intelligence technologies has accelerated the integration of frontier fields such as artificial intelligence, big data, the Internet of Things, and cloud computing into hospital pharmaceutical services.6 These technologies have provided novel solutions for drug data mining and efficacy prediction, the development of clinical pharmacy information systems, and intelligent decision support for rational medication use.7 Nonetheless, most technological innovations and application studies have concentrated on enhancing pharmaceutical services in general hospitals, while the unique characteristics of Traditional Chinese Medicine (TCM) hospitals have rendered their pharmaceutical services relatively underdeveloped in this domain.8 The particularity of TCM pharmaceutical services is reflected in multiple dimensions.9 First, they demand highly specialized supporting facilities. However, many hospitals face challenges such as incomplete infrastructure for decoction rooms and preparation laboratories, irrational functional layouts, outdated or missing equipment, and quality deficiencies.10 Second, in clinical practice, the application of TCM often involves the use of multiple formulae, with prescriptions that are inherently complex and highly variable. The processing of Chinese medicinal materials involves intricate techniques such as paozhi (traditional preparatory methods), while the selection, compatibility, and potential interactions of Chinese medicines add further layers of complexity. At the same time, the integration of Western medicine with TCM has become increasingly widespread and diverse. These characteristics significantly increase the challenges associated with pharmaceutical services in TCM hospitals. Clinical pharmacy services must therefore incorporate both Western and Chinese pharmacy practices, and should not be considered in isolation.11 Over the past few years, with the growing global influence of TCM and the rapid expansion of the TCM industry, the clinical workload related to TCM has steadily increased in hospitals. However, many institutions still lack modernized, integrated information management systems that operate across both desktop and mobile platforms. This deficiency poses risks and challenges to the timeliness and standardization of pharmaceutical service quality control, thereby limiting the ability to provide a robust scientific basis for clinical decision-making.12
High-Reliability Organization (HRO) theory originates from the study of organizations—such as nuclear power plants and aircraft carriers—that maintain exceptionally high levels of safety despite operating in high-risk environments.13 The High-Reliability Organization theory offers a critical leadership and governance framework for managing complexity and risk within healthcare systems. In highly dynamic, potentially hazardous, and multidisciplinary fields such as pharmaceutical services, effective leadership extends beyond routine operational management to encompass the cultivation of an organizational culture that continuously identifies risks, adapts to change, and ensures safety. The five principles of HRO-preoccupation with failure, reluctance to simplify interpretations, sensitivity to operations, commitment to resilience, and deference to expertise—serve as concrete expressions of such leadership. Together, they form a systematic governance mechanism that enables healthcare organizations to maintain both safety and efficiency under conditions of uncertainty. Nevertheless, existing research on HRO applications in healthcare has largely focused on implementing individual principles or technical tools, with limited integration of the five principles into an actionable and replicable leadership framework.14,15 Such a framework is urgently needed to guide systematic risk management practices, particularly amid the ongoing digital transformation. This gap in knowledge constitutes the central problem that the present study seeks to address. The theory emphasizes reducing error rates through effective management and early-warning mechanisms in complex and high-stakes settings, thereby ensuring operational safety and reliability.16 In the past several years, HRO theory has been widely applied in hospitals, demonstrating positive outcomes in diverse areas such as anesthesia,17 surgery, nursing,15 pediatrics,18 and medical record quality control.14 In the context of hospital pharmaceutical management, the rising public enthusiasm for TCM, the increasing integration of Chinese and Western medicine, and the generally higher educational level of the population—which translates into greater expectations for healthcare services—place new demands on clinical pharmacists. They are now required to rapidly and accurately assess complex drug interactions within shorter timeframes and to ensure comprehensive, full-cycle management of pharmaceutical services. This includes everything from prescription review and medication education to drug management and adverse reaction monitoring, forming a closed-loop system. The application of HRO theory is particularly appropriate in this context, as its core principles—namely error prevention, process consistency, and continuous learning—are closely aligned with the fundamental priorities of pharmaceutical service management. Consequently, the establishment of a new paradigm of smart pharmaceutical services grounded in HRO theory is both feasible and of critical significance.19
Material and Methods
Based on this framework, this study operationalizes the five principles of HRO as a leadership framework. It addresses key dimensions of pharmaceutical service governance, including error prevention in internet-based medicine, reengineering of complex medication management processes, coordinated safety control of Chinese and Western medicines, clinical pharmacy decision support, standardization of professional services, and optimization of data monitoring.20 Aligning these dimensions with the practical needs of clinical pharmaceutical services in public hospitals, this study leverages information technology to develop a digital and intelligent pharmacy system structured around “one center, two supports, and six platforms.” With patient safety and rational drug use as the core governance objectives, the system relies on two enabling platforms—Chinese and Western medicine knowledge graph technology and digital intelligence technology.21 On this basis, it establishes six functional platforms: internet hospital quality control management, multi-dimensional and hierarchical medication scientific management and control, personalized pharmacy clinics, specialized clinical pharmacist workstations, standardized prescription review, and real-time adverse drug reaction reporting.22 Through this architecture, the study translates HRO leadership principles into a feasible governance structure and technical pathway, thereby transforming pharmaceutical service models from passive response to active prevention and control, and from experience-driven to data-driven practice.23
Its technical architecture is divided into four layers. The first is the infrastructure layer, which comprises the cloud computing platform, network facilities, and Internet of Things (IoT) devices. The second is the data layer, consisting of a knowledge base for Chinese and Western medicines, a rule base for rational drug use, and a patient information database. The third is the application layer, which incorporates the six functional modules. The fourth is the presentation layer, which provides different user interfaces for pharmacists, physicians, and administrators. The system adopts a microservices architecture to ensure that each module can be independently developed and deployed while maintaining overall integration (Figure 1).
 |
Figure 1 Construction framework of the smart pharmaceutical service system in public hospitals: Drawing on the characteristics and practical needs of clinical pharmacy services in public hospitals, we propose a smart-intelligent pharmaceutical service framework based on HRO theory, which is structured as “one center, two supports, and six platforms”. Specifically, patient safety and rational drug use form the central focus; the TCM-Western medicine knowledge graph and digital intelligence technologies serve as dual support platforms. On this basis, six integrated platforms are established: the Internet hospital quality-control management platform, the multidimensional hierarchical drug management and control platform, the personalized pharmacy outpatient workstation, the specialized clinical pharmacist workstation, the standardized prescription review system, and the real-time adverse drug reaction reporting system. Together, these platforms enable a full-process, intelligent, and standardized model of pharmaceutical services tailored to the unique requirements of TCM (integrated) hospitals. |
The functional module design of the six platforms (Table 1), together with the distinctive strengths of TCM (Table 2), supports the construction of a highly executable and standardized system. This system encompasses the entire process of pharmaceutical services, including pre-event prevention, intra-event intervention, and post-event evaluation, thereby forming a complete quality management closed loop.
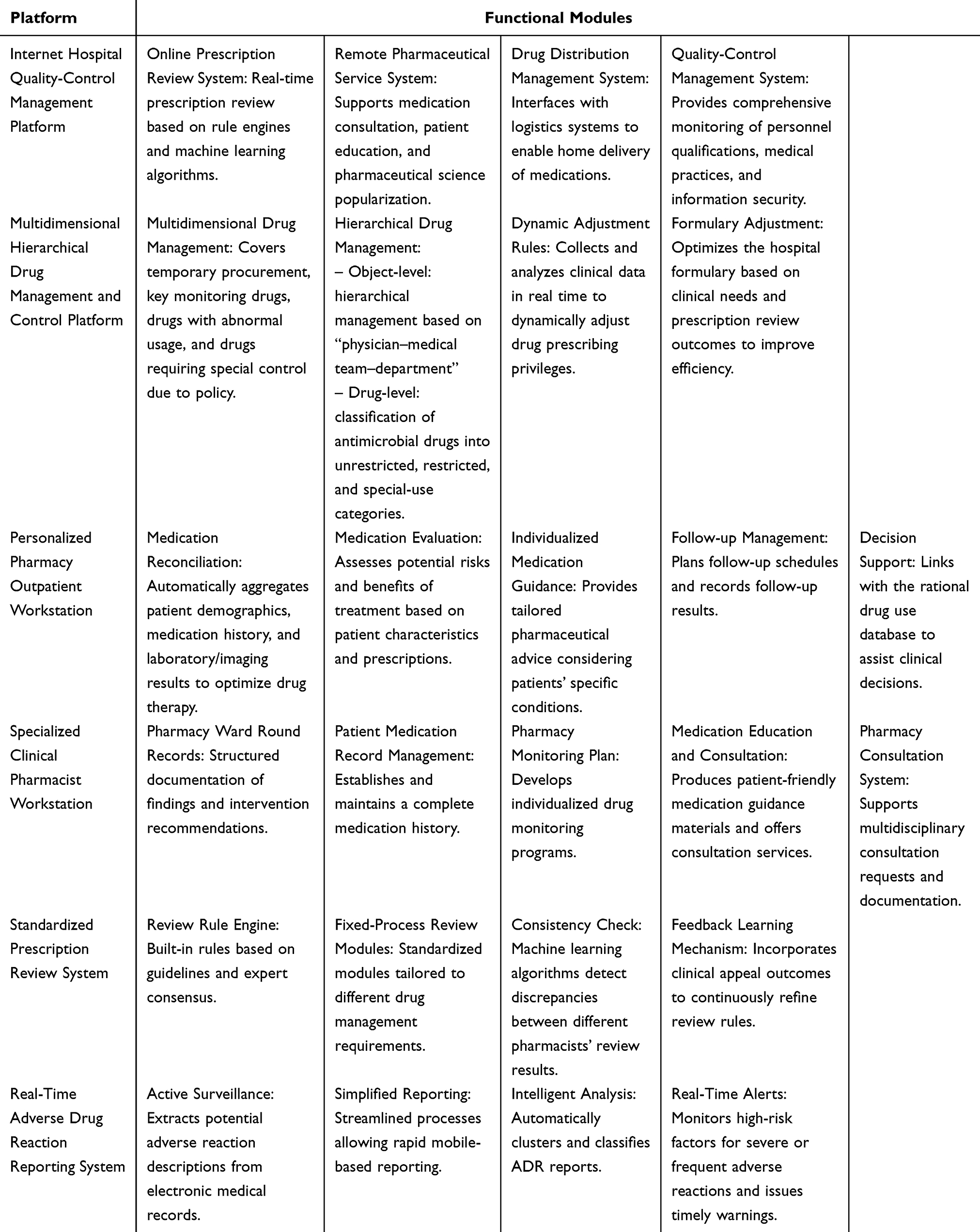 |
Table 1 Functional Module Design of the Platforms |
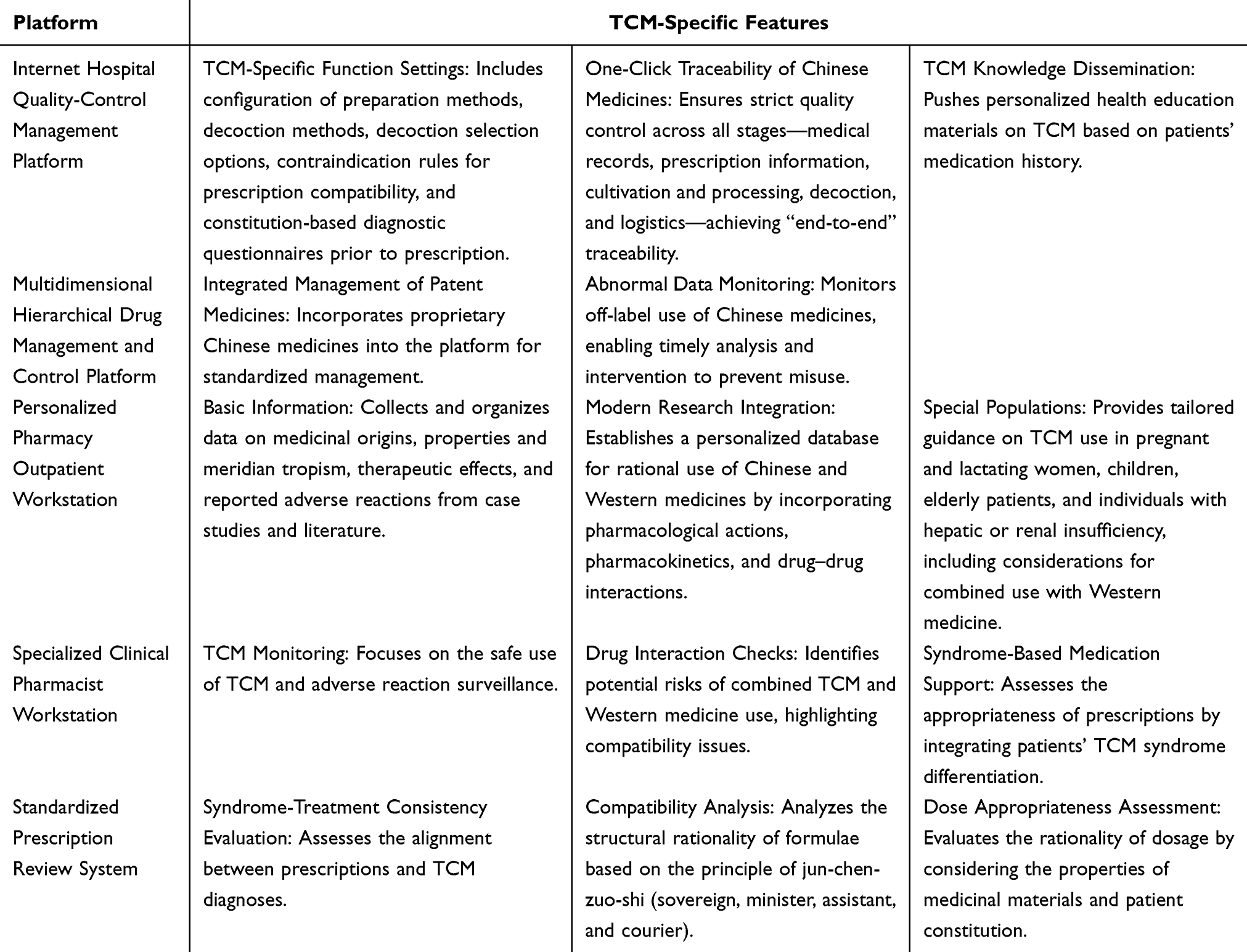 |
Table 2 TCM-Specific Features of the Platform Functions |
Results
The smart pharmaceutical service system proposed in this study fully integrates the characteristics of TCM.24 By leveraging the TCM safety knowledge base and digital-intelligence technologies, it achieves comprehensive, full-process management of pharmaceutical services.25 The five core principles of HRO theory also play a pivotal role in the construction of this system.
Since the end of 2022, the Internet Hospital has launched a convenient TCM prescription dispensing channel, with the average daily number of prescriptions increasing from fewer than 100 initially to over 30,000 at present. The quality control platform of the Internet hospital fundamentally addressed the issue of “refunds for fees and medications due to improper medical orders occurring after patient payment and drug collection” through process redesign—specifically, by replacing the “post-dispensing reviewer” model with a “real-time reviewer at the point of order entry” approach. As shown in Table 3, this intervention resulted in an absolute reduction of 2.64% in the rate of refunds and medication returns, and a relative reduction of as high as 86.56%. This decline empirically supports the effectiveness of optimizing the real-time prescription review process. The improvement not only reduces patient time burden and psychological frustration associated with refund procedures but also lowers friction costs in hospital operations, thereby achieving a dual enhancement in patient experience and operational efficiency. It should be noted, however, that patient refunds and medication returns are attributable to multiple factors; therefore, the observed changes can only partially account for the overall effectiveness of this intervention. The concurrent increase in average daily dosage (a proxy for service attractiveness) and the steep reduction in refund rates (a proxy for service reliability) collectively delineate a coherent service upgrading pathway for Internet hospitals. This pathway is characterized by technological innovation (eg., real-time prescription review systems) as the foundational enabler and process redesign (advancing risk control nodes to pre-prescription stages) as the operational engine. Such an approach drives the transition of TCM dispensing services from a growth-oriented, volume-based model to a quality and efficiency centered paradigm, ultimately delivering a more streamlined and safer patient care experience.
 |
Table 3 Annual Rate of Prescription Refunds/Returns Before and After Implementation of the Internet Hospital Quality-Control Platform |
The Multidimensional Hierarchical Drug Management and Control Platform enables refined classification management of drugs with varying regulatory requirements, such as temporary procurement drugs, key monitoring drugs, drugs with abnormal consumption patterns, and those requiring special control due to policy factors.26 This platform has transformed the previous extensive and loosely controlled management model into one of precision management.27 It not only strengthens supervision but also safeguards the legitimate and rational clinical demand for essential medicines, while simultaneously realizing multi-level precision management across physicians, medical teams, and clinical departments (Table 4). Through the integration of information technology and refined management, the multi-dimensional graded drug scientific control platform has delivered a marked enhancement in both approval efficiency and clinical satisfaction—two core metrics of pharmaceutical service quality. In the pre-implementation period, the average approval cycle for drug requests was 72 hours, posing a substantial risk of treatment delay under time-sensitive conditions such as emergency medication or temporary procurement. Post-implementation, the cycle has been compressed to ≤ 2 hours (Table 4), yielding an at least 36 fold acceleration in approval speed. This transformative improvement resolves the inefficiencies of the prior extensive management approach, robustly supports necessary and rational medication needs in daily clinical practice, and guarantees timely patient access to prescribed therapies. Clinician feedback represents the “gold standard” for assessing the effectiveness of pharmaceutical management interventions. The 12.2% increase in satisfaction scores demonstrates that, following platform implementation, physicians are no longer burdened by protracted approval procedures, and their legitimate demands for rational drug use are reliably met. As a result, they demonstrate strong endorsement of the hospital’s managerial efficiency. Collectively, these findings indicate that the multi-dimensional graded drug scientific control platform has successfully harmonized strict regulatory control with agile service delivery, and the empirical evidence confirms a paradigm shift from extensive, process oriented management toward a refined, data driven, and scientifically grounded governance model.
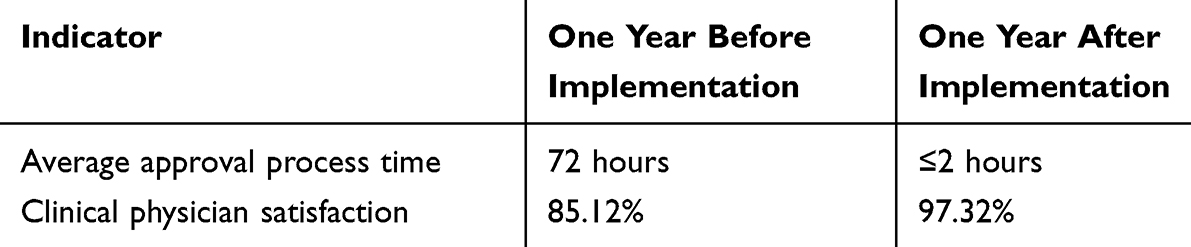 |
Table 4 Comparison of Performance Before and After Implementation of the Multidimensional Hierarchical Drug Management and Control Platform |
To address the diverse needs of specialized outpatient clinics—such as the pharmacy clinic for chronic diseases, the pharmacy clinic for medication use in lactating women, and the PCCM (Pulmonary and Critical Care Medicine) clinic for cough and asthma—a personalized pharmacy outpatient workstation was developed. This was achieved by constructing an integrated knowledge base combining Chinese and Western medicine and by incorporating the intelligent quality-control–based 930 medical record internal quality-control system to ensure rigorous quality oversight of outpatient pharmacy records. The 8.14% increase in the medical record quality control pass rate (Table 5) provides intuitive evidence of a marked enhancement in the standardization of pharmaceutical outpatient medical record documentation. This improvement suggests that the overwhelming majority of medical records now meet standards of both standardization and normalization, substantially mitigating legal risks and closing management loopholes inherent in medical documentation practices.
 |
Table 5 Quality-Control Pass Rate of Pharmacy Outpatient Medical Records Before and After Implementation |
With the expansion of clinical pharmacy teams and the growing need for homogenized management across multiple hospital campuses, the scientific rigor and accuracy of rational drug-use interventions have attracted increasing attention. The development of a standardized prescription review system is characterized by the establishment of a mature and reproducible model for rational drug-use evaluation. This includes the formulation of usage specifications, the creation of a point-based evaluation system, the development of modular review tools, and the establishment of feedback mechanisms. Table 6 presents a compelling before-and-after comparison. In the pre-implementation year, the rational use rate of proton pump inhibitors (PPIs) stood at 85.11%, and the success rate of physician appeals against automated review decisions was notably high at 78.93%. One year post-implementation, the rational use rate increased sharply to 99.96%—a gain of 14.85 percentage points—indicating near-universal adherence to rational prescribing standards. In parallel, the appeal success rate fell to 58.13%, a decline of 20.8%. This bidirectional shift demonstrates two interrelated effects. First, prescribing behavior has been effectively disciplined through targeted interventions, including the establishment of standardized usage protocols and the development of modular clinical decision support tools. Second, the “real-time point-based evaluation + results feedback” mechanism has fostered greater consensus between clinicians and the pharmacy governance system. As a result, irrational medication use has been substantially curbed, while unproductive management friction has been significantly reduced. Collectively, these outcomes reflect a dual gain in medication safety and communication efficiency within a harmonized, multi-hospital quality management framework.
 |
Table 6 Comparison of Performance Before and After Implementation of the PPI Standardized Prescription Review System |
The Adverse Drug Reaction (ADR) system consists of two modules: real-time reporting and early-warning monitoring. In addition to digitizing the existing ADR reporting system, an ADR early-warning monitoring module was developed. This module integrates natural language processing (NLP) techniques to automatically extract drug-related adverse reaction keywords (eg., “rash,” “nausea”) from electronic medical records based on patients’ medication orders. A non-punitive reporting mechanism was also established to encourage clinical pharmacists to actively monitor ADR risks and proactively identify potential medication hazards, rather than relying solely on retrospective reporting. Indicators such as the proportion of proactively reported ADRs among the total monthly ADR reports and the overall number of ADR reports showed significant improvement (Table 7). Through the integration of natural language processing technology and a non-punitive reporting culture, the adverse drug reaction (ADR) monitoring system has transitioned from a passive, retrospective reporting model to an active, prospective early-warning system. Table 7 provides robust evidence of this transformation. In the year prior to implementation, the proportion of monthly ADR reports originating from active early warnings was 0%; in the year following implementation, this proportion reached 10–15%. This shift signifies the hospital’s new ability to automatically capture potential medication risks. By scanning electronic medical records for pre-specified risk-related keywords, the system autonomously identifies hidden threats, addressing a long-standing blind spot in conventional manual surveillance. Over the same period, the total annual ADR report count increased steadily from 433 to 478, a net gain of 45 reports. This increase is jointly attributable to the motivating effect of the incentive-based reporting system on clinical staff and the additional detection capacity afforded by the new technology. Taken together, the adoption of an active early-warning mechanism expands the breadth of pharmacovigilance, relocates drug safety control earlier in the healthcare pathway, and—when coupled with the overall rise in reporting volume, collectively reinforces a more rigorous and forward-looking patient safety defense framework.
 |
Table 7 Comparison of ADR Reporting Before and After Implementation of the ADR System |
Discussion
A cross-sectional study covering 199 hospitals across 30 provincial-level administrative regions in China revealed that although 63.82% of medical institutions have initiated smart-pharmacy programs—particularly in prescription review, prescription evaluation, and Internet-based hospital services. However, the overall coverage of pharmaceutical services across the entire process remains suboptimal.28 Problems such as uneven development across different stages, insufficient full-process integration, and regional disparities persist.29 These challenges are particularly pronounced in public hospitals and are reflected in the following aspects: 1. Complex drug management: TCMs encompass a wide variety of categories and specifications, often requiring unique storage conditions, which significantly increases the difficulty of management. 2. Lack of scientific basis for clinical medication decisions: Data on TCM drug–drug interactions remain incomplete, and intelligent decision-support systems are lacking. 3. Inadequate monitoring and evaluation of medication use: Systems for adverse drug reaction monitoring are underdeveloped, with insufficient mechanisms for real-time reporting and analysis. 4. Low level of informatization: Information silos persist, and the efficiency of data collection, management, and analysis is poor. 5. Traditional service models: Services remain primarily focused on drug dispensing, while clinical pharmacy services are underutilized and insufficiently developed.
Moreover, research on the informatization of TCM faces several unique challenges. First, the degree of data standardization is low: TCM terminology lacks unified standards, prescriptions are highly complex in composition, and dosage descriptions are expressed in diverse ways.30 Second, the knowledge system is intricate: classical TCM theories—such as properties and meridian tropism (xingwei guijing) and the principle of sovereign, minister, assistant, and courier (jun-chen-zuo-shi)—are difficult to represent in structured data formats.31 Third, clinical evidence is insufficient: many Chinese medicines lack high-quality evidence from evidence-based medicine.32 Finally, specialized management requirements exist: aspects such as quality control of decoction pieces, decoction processes, and compatibility contraindications demand dedicated management systems.33 In response to these difficulties, scholars have begun exploring new research directions, including the construction of TCM knowledge graphs, data mining of adverse drug reactions associated with Chinese medicines. And the development of prescription recommendation systems. However, these efforts remain at an early stage of development overall.34
Against this backdrop, a key challenge for intelligent pharmacy lies in determining how to leverage digital and information technologies to build a clinical pharmacy system with distinct TCM characteristics. Furthermore, given the multiple complexities inherent in TCM pharmaceutical services, it is essential to establish mechanisms that can effectively address emergencies while ensuring rigorous quality control throughout the pharmaceutical service process.35
HRO are complex systems in which a large amount of personnel work within dynamic and potentially hazardous environments. Effectively managing unexpected events in HRO theory while maintaining safety and efficiency is an arduous task.36 The theory is grounded in five core principles, which, when applied to the construction of a smart pharmacy system, can be embodied as follows: (1) Preoccupation with failure: establishing a non-punitive adverse event reporting system that encourages proactive identification and reporting of potential risks; (2) Reluctance to simplify interpretations: acknowledging the inherent complexity of TCM usage and avoiding excessive simplification in clinical practice; (3) Sensitivity to operations: maintaining real-time monitoring to ensure continuous awareness of system performance; (4) Commitment to resilience: developing rapid response mechanisms to guarantee that problems are promptly addressed and resolved; (5) Deference to expertise: preserving clinical pharmacists’ decision-making authority within the system design to ensure professional judgment is respected.
Based on HRO theory, the construction of the smart pharmaceutical service system has achieved closed-loop management of pharmaceutical services, encompassing the entire process from prescription review and medication education to drug management and adverse drug reaction monitoring. The standardized prescription review software, with its built-in rule engine and intelligent allocation system, has addressed inconsistencies in pharmacists’ review standards, thereby improving the scientific rigor and consistency of review outcomes.37 The personalized pharmacy outpatient workstation integrates multidimensional patient information and establishes a collaborative knowledge base for rational drug use involving both TCM and Western medicine (Figure 2), enabling precise medication recommendations for special populations and embodying the patient-centered service concept.
 |
Figure 2 Information system framework for rational medication use of Chinese medicines during pregnancy and lactation. |
Furthermore, the Internet Hospital Quality-Control Platform has incorporated TCM standardized formula management and decoction guidance functions, while the refined drug management platform has established a classification system for proprietary Chinese medicines based on TCM theory.38 These designs have significantly enhanced the standardization and safety of TCM pharmaceutical services.
In addition, through the establishment of a incentive-based reporting system, real-time monitoring mechanisms, and rapid response processes, the framework has effectively reduced the risk of medication errors and improved the reliability of pharmaceutical services.39 In particular, the real-time ADR reporting system, integrated with natural language processing technology, enables proactive monitoring and intelligent analysis of adverse reactions, thereby providing strong support for clinical medication safety.40
Nevertheless, this study has certain limitations. On the one hand, the relatively low degree of standardization and structuring of TCM data may affect the accuracy and generalizability of the system.41 On the other hand, the implementation of a smart pharmacy system requires sustained investments in technology, personnel, and funding, which may pose challenges to hospital operations. Future research will further explore the application of artificial intelligence in constructing integrated TCM–Western medicine knowledge graphs and clinical decision-support tools,42 promote the development of standardized datasets, and optimize the usability and scalability of the system.43
Conclusion
This study responds to the dual imperatives of promoting high-quality development in TCM and transforming hospital-based pharmaceutical services. Using HRO theory as an overarching leadership and governance framework, the study addresses key structural challenges inherent in TCM hospital pharmaceutical services—namely, the complexity of polyherbal prescription combinations, the extensive co-administration of Chinese and Western medicines, and the need for specialized support management. In response, a novel smart pharmacy system was developed. Centered on the core goals of patient safety and rational medication use, the system integrates TCM and Western medicine knowledge graphs with advanced digital intelligence technologies. Through the synergistic operation of six major platforms, the system enables full-process, standardized pharmaceutical service management across multiple care settings. The resulting governance architecture not only streamlines clinical workflows and improves service efficiency but also significantly reinforces the organization’s capacity for proactive risk prevention and professional clinical decision support (Figures 1 and 2).
The empirical findings of this study suggest that effective healthcare leadership transcends the mere integration of technological tools. Instead, it fundamentally rests on the cultivation of an organizational culture capable of continuously detecting hazards, adapting to dynamic conditions, and preserving safety. In the system developed herein, the five principles of HRO theory have been translated into actionable governance mechanisms. Exemplary mechanisms include a reward-based ADR reporting system that encourages voluntary hazard identification, real-time monitoring systems that sustain operational awareness, and structural provisions that preserve clinical pharmacists’ professional discretion. Together, these mechanisms constitute a governance ecosystem defined by three core attributes: safety-centric priority setting, empirical (data-driven) decision-making, and professional empowerment. Such an ecosystem enables healthcare organizations to sustain reliable, stable performance in highly dynamic and potentially hazardous operational environments.
For healthcare managers, this study yields three actionable lessons for healthcare leaders and policymakers. First, the success of digital and intelligent transformation is not determined by the technical sophistication of the tools themselves, but by the presence of a well-aligned leadership framework that actively channels technological applications toward the core goals of patient safety and care quality. Second, governance structure design must uphold professional judgment as a core asset, avoiding the reduction of inherently complex pharmaceutical decisions into simplistic algorithmic outputs. Failure to do so risks eroding the professional identity and clinical accountability of pharmacists. Third, achieving service homogenization across multiple hospital campuses and diverse clinical scenarios necessitates unified governance standards and interoperable data platforms, rather than overreliance on administrative flat or fragmented local pilots.
This study makes two primary contributions. First, it enriches the application scenarios of High Reliability Organization theory within the domain of TCM management. Second, it provides a replicable governance pathway for the digital transformation of public hospitals, especially TCM hospitals. At the same time, the study reveals persistent practical challenges, notably the lack of structured TCM data and the urgent need for enhanced investments in digital infrastructure and clinical informatics talent. To address these gaps, future research and practice should further integrate artificial intelligence and big data analytics to advance the integrated Chinese and Western medicine knowledge graph, promote the standardization of clinical datasets, and iteratively refine system functions and user adaptability. These efforts will drive the vertical evolution of pharmaceutical services toward greater precision, intelligence, homogenization, and end-to-end process integration, ultimately providing solid support for the high-quality development of TCM and pharmacy under the Healthy China strategy.
Acknowledgments
We thank Home for Researchers editorial team (www.home-for-researchers.com) for language editing service.
Funding
This study was financially supported by the Zhejiang Medical Doctors Association Clinical Rational Drug Use Special Committee Clinical Research Fund Program (Grant No. YS2024-2-002), Special Research Project on Promoting High-quality Development of Public Hospitals through High-Reliability Organization Construction of the Zhejiang Provincial Hospital Association (2025-4), High-quality development and modernization capacity improvement project for public hospitals (202522), Hospital Pharmacy Scientific Research Project of Zhejiang Pharmaceutical Association (2019ZYYG05, 2022ZYY25), Hospital Pharmaceutical High Quality Development and Medical Community Pharmaceutical Management Special Research Funding Project of Zhejiang Pharmaceutical Association (2025ZGYY06), Hospital Prescription Analysis Project of Zhejiang Pharmaceutical Association (2B12401).
Disclosure
The authors declare that there are no conflicts of interests.
References
1. Shi JN, Yang J, Zheng Y, Wong PHH, Hu H, Ung COL. The clinical quality management system of advanced therapy medicinal products in the hospital setting: a scoping review. Mol Ther Methods Clin Dev. 2025;33(2):22. doi:10.1016/j.omtm.2025.101485
2. Wang X, Gu M, Gao XQ, et al. Application of information-intelligence technologies in pharmacy intravenous admixture services in a Chinese third-class a hospital. BMC Health Serv Res. 2022;22(1):14. doi:10.1186/s12913-022-08580-4
3. Mi X, Su XL, Jin ZY, et al. Economic evaluations of clinical pharmacy services in China: a systematic review. BMJ Open. 2020;10(1):13. doi:10.1136/bmjopen-2019-034862
4. Paolinelli JP, de Alencar T, Rocha KS, et al. Implementation of clinical pharmacy services in primary health care: a scoping review. J. Eval. Clin. Pract. 2025;31(6). doi:10.1111/jep.70285.
5. Liao J, Hua XL, Cai XF, Su YY, Yu LX. Practice and Discussion on the Management Mode of Comprehensive Pharmacy under the Strategy of Healthy China. J Healthc Eng. 2022;2022:5. doi:10.1155/2022/5477995
6. Bu F, Sun H, Li L, et al. Artificial intelligence-based internet hospital pharmacy services in China: perspective based on a case study. Front Pharmacol. 2022;13.
7. Deng JZ, Chen Y, Zhang XY, Zhou YH, Xiong B. Intelligent supervision of PIVAS drug dispensing based on image recognition technology. PLoS One. 2024;19(4):22.
8. Huang XR, Estau D, Liu XN, Yu Y, Qin JG, Li ZJ. Evaluating the performance of ChatGPT in clinical pharmacy: a comparative study of ChatGPT and clinical pharmacists. Br J Clin Pharmacol. 2024;90(1):232–13. doi:10.1111/bcp.15896
9. Du M, Luo JW, Wang SP, Liu S. Genetic algorithm combined with BP neural network in hospital drug inventory management system. Neural Comput Appl. 2020;32(7):1981–1994. doi:10.1007/s00521-019-04379-3
10. Penm J, Moles R, Wang H, Li Y, Chaar B. Factors affecting the implementation of clinical pharmacy services in China. Qualitative Health Research. 2014;24(3):345–356. doi:10.1177/1049732314523680
11. Zhuang Y, Yu L, Jiang N, Ge Y. TCM-KLLaMA: intelligent generation model for Traditional Chinese Medicine Prescriptions based on knowledge graph and large language model. Comput. Biol. Med. 2025;189:109887. doi:10.1016/j.compbiomed.2025.109887
12. Xuebing H, Mingna S, Tungalag B, et al. Application of artificial intelligence in the development of traditional chinese medicine. Basic Clin Pharmacol Toxicol. 2025:137(1).
13. Merchant NB, O’Neal J, Dealino-Perez C, Xiang J, Montoya A Jr, Murray JS. A high-reliability organization mindset. Am J Med Qual. 2022;37(6):504–510. doi:10.1097/JMQ.0000000000000086
14. Auschra C, Asaad E, Sydow J, Hinkelmann J. Interventions into reliability-seeking health care organizations: a systematic review of their goals and measuring methods. J Patient Saf. 2022;18(8):e1211–e1218. doi:10.1097/PTS.0000000000001059
15. Almutairi AS, Said FM. Development and delphi validation of a comprehensive high reliability program to improve nursing work environment and patient safety. Cureus. 2026;18(4):e107677. doi:10.7759/cureus.107677
16. Pozzobon LD, Lam J, Chimonides E, Perkins-Meingast B, Luk W-S. Adopting high reliability organization principles to lead a large scale clinical transformation. Healthc. Manag. Forum. 2023;36(4):241–245. doi:10.1177/08404704231162785
17. Sutcliffe KM. Building cultures of high reliability: lessons from the high reliability organization paradigm. Anesthesiol. Clin. 2023;41(4):707–717. doi:10.1016/j.anclin.2023.03.012
18. Cartland J, Green M, Kamm D, Halfer D, Brisk MA, Wheeler D. Measuring psychological safety and local learning to enable high reliability organisational change. BMJ Open Quality. 2022;11(4):e001757. doi:10.1136/bmjoq-2021-001757
19. Lindaas NA, Anthun KS, Magnussen J. New Public Management and hospital efficiency: the case of Norwegian public hospital trusts. BMC Health Serv Res. 2024;24(1):11. doi:10.1186/s12913-023-10479-7
20. Pan QH, Liu Y, Wei SF. Design of a multi-category drug information integration platform for intelligent pharmacy management: a needs analysis study. Medicine. 2024;103(15):9.
21. He J, Guo Y, Lam LK, et al. OpenTCM: a GraphRAG-Empowered LLM-based System for Traditional Chinese Medicine Knowledge Retrieval and Diagnosis. Arxiv. 2025.
22. Lv LS, Yao Y, Zhang MW, Xin CW. Impact of implementing the lean management on internal errors at an outpatient hospital pharmacy in China. Patient Prefer Adherence. 2025;19:139–147. doi:10.2147/PPA.S486478
23. Mi DZ, Li Y, Zhang KY, Huang CN, Shan WJ, Zhang JB. Exploring intelligent hospital management mode based on artificial intelligence. Front Public Health. 2023;11:8. doi:10.3389/fpubh.2023.1182329
24. Y-y D, P-r L, T-t H, S-x L, Ye S, Z-w Y. Application and Development of Intelligent Medicine in Traditional Chinese Medicine. Curr Med Sci. 2021;41(6):1116–1122. doi:10.1007/s11596-021-2483-2
25. Haoyu T, Kuo Y, Xin D, et al. TCMLLM-PR: evaluation of large language models for prescription recommendation in traditional Chinese medicine. Digital Chin Med. 2024;7(4):343–355. doi:10.1016/j.dcmed.2025.01.007
26. Xiang S, Lin H, Cai F, Jiang Z. Integrating knowledge graphs with ancient Chinese medicine classics: challenges and future prospects of multi-agent system convergence. ChinMed. 2025;20(1). doi:10.1186/s13020-025-01226-7
27. Yang X, Luo H, Nie XY, Kong XTR. Tacit knowledge-informed approximate dynamic programming for last-mile delivery operations in online-to-offline pharmacies. Ind Manage Data Syst. 2025;125(3):1078–1109. doi:10.1108/IMDS-09-2024-0874
28. Song Z, Yan Y, Yang L, Zhao R. Current status of intelligent pharmaceutical care services in China: a cross-sectional study. Chin J Hospital Pharm. 2023;43(12):
29. Chen L, Mao Y, Zhou X. Construction and application of pharmaceutical service model of traditional Chinese medicine combined outpatient in the first affiliated hospital of Suzhou university. Tradit. Chin. Med. 2019;41(11):1161–1164.
30. Hua H, Tang J-Y, Zhao J-N, et al. From traditional medicine to modern medicine: the importance of TCM regulatory science (TCMRS) as an emerging discipline. ChinMed. 2025;20(1). doi:10.1186/s13020-025-01152-8.
31. Jin Z, Zhang Y, Miao J, Yang Y, Zhuang Y, Pan Y. A knowledge-guided and traditional Chinese medicine informed approach for herb recommendation. Front Inf Technol Electron Eng. 2023;24(10):1416–1429. doi:10.1631/FITEE.2200662
32. Liu D-H, He X-L, Ni S-H, et al. Pharmaceutical changes and countermeasures for transformation of traditional Chinese medicine preparations in medical institutions into new drugs based on human use experience. Zhongguo Zhong Yao Za Zhi. 2024;49(2):565–568. doi:10.19540/j.cnki.cjcmm.20231113.302
33. Jia XD, Zhang W, Si FY, et al. Qualitative study on the problems and potential solution strategies for part-time clinical pharmacists’ clinical services work in a tertiary hospital in China. BMJ Open. 2024;14(6):8. doi:10.1136/bmjopen-2024-083956
34. Huang M, Yang F-W, Zhang J-H, Zhang B-L. Inheritance, innovation and development of traditional Chinese medicine in new era call for scientific supervision. Zhongguo Zhong Yao Za Zhi. 2023;48(1):1–4. doi:10.19540/j.cnki.cjcmm.20221021.601
35. de Oliveira KB, de Oliveira OJ. Making hospitals sustainable: towards greener, fairer and more prosperous services. Sustainability. 2022;14(15):21.
36. Sculli GL, Pendley-Louis R, Neily J, et al. A high-reliability organization framework for health care: a multiyear implementation strategy and associated outcomes. J. Patient Saf. 2022;18(1):64–70. doi:10.1097/PTS.0000000000000788
37. Zhu XM, Hu H, Yao DN. Exploring community pharmacy manager/ pharmacist perceptions and responses to China’s dual-channel policy for improving access and rational use of innovative drugs: a qualitative study. Int J Clin Phar. 2025;10.
38. Xiaoen C, Chuanbiao W, Qiang X, Yuanzhang H, Xiaohui Z. Development demand of artificial intelligence based on traditional chinese medicine to study on the typical of the big data of traditional chinese medicine. Modern. Tradit. Chin. Med Materia Medica-World Sci Technol. 2020;22(4):1243–1248.
39. Yao L, Zhang Y, Wei B, Zhang W, Jin Z. A topic modeling approach for traditional chinese medicine prescriptions. IEEE Trans Knowledge Data Eng. 2018;30(6):1007–1021. doi:10.1109/TKDE.2017.2787158
40. Yao Z, Guo YF, Li M. Analysis of the role of Informatization, based on data analyses, in hospitals to improve hospital management. Altern Ther Health Med. 2023;29(3):172–185.
41. Zhao JH, Wu X, Chen Y, et al. What Makes a Hospital Excellent? A Qualitative Study on the Organization and Management of Five Leading Public Hospitals in China. Risk Manag Healthc Policy. 2023;16:1915–1927. doi:10.2147/RMHP.S424711
42. Zhi LH, Yin P, Ren JJ, et al. Running an internet hospital in china: perspective based on a case study. J Med Internet Res. 2021;23(9):9. doi:10.2196/18307
43. Zhang GW, Gong MC, Li HJ, Wang S, Gong DX. The “Trinity” smart hospital construction policy promotes the development of hospitals and health management in China. Front Public Health. 2023;11:4.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.