Back to Journals » International Journal of Women's Health » Volume 17
Research Progress on the Relationship Between Serum Uric Acid Levels and Coagulation Dysfunction in Preeclampsia
Authors Zou M, Tang D, Liu F, Guan F
Received 31 July 2025
Accepted for publication 18 November 2025
Published 28 November 2025 Volume 2025:17 Pages 5007—5015
DOI https://doi.org/10.2147/IJWH.S557385
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
Mengjun Zou,1,2 Dongmei Tang,2 Fang Liu,2 Feng Guan2
1Zhongshan Clinical Medical College, Dalian University, Dalian, Liaoning, 116001, People’s Republic of China; 2Department of Obstetrics, Zhongshan Hospital Affiliated to Dalian University, Dalian, Liaoning, 116001, People’s Republic of China
Correspondence: Mengjun Zou, Email [email protected]
Abstract: Preeclampsia (PE) is a pregnancy-specific complication that typically occurs in the mid to late stages of gestation. Its main clinical features include gestational hypertension, proteinuria, and multiple organ dysfunction. In severe cases, it may progress to eclampsia, HELLP syndrome, and even pose life-threatening risks to both mother and fetus. Recent studies have found that serum uric acid (UA) levels are significantly elevated in patients with PE and closely correlated with disease severity, suggesting that UA may not only serve as a metabolic marker but also play an active role in the pathogenesis of PE. At the same time, coagulation dysfunction—an important pathological feature of PE—manifests as thrombocytopenia, consumption of coagulation factors, suppression of the fibrinolytic system, and microthrombus formation. These changes contribute significantly to organ damage and adverse pregnancy outcomes in PE. This review summarizes the dynamic changes in serum uric acid levels during PE and explores their relationship with coagulation abnormalities. Particular emphasis is placed on the potential mechanisms by which uric acid induces coagulation disorders, including endothelial cell injury, oxidative stress aggravation, and activation of inflammatory pathways. Additionally, the review discusses the clinical utility of various coagulation-related biomarkers (such as D-dimer, fibrinogen, PAI-1, and P-selectin) in the early prediction, severity assessment, and clinical management of PE. Current research indicates that combined monitoring of serum uric acid and coagulation markers—for instance, models integrating UA with the sFlt-1/PlGF ratio or with PAI-1, which have demonstrated high predictive accuracy (AUC > 0.90) for early-onset PE—may improve early detection and risk stratification. However, the current evidence remains primarily observational and is limited by heterogeneity in study designs. Future studies should prioritize well-designed prospective cohorts to clarify causal relationships and explore more sensitive and specific combined predictive models to provide a stronger theoretical and clinical foundation for improving maternal and fetal outcomes.
Keywords: preeclampsia, serum uric acid, coagulation dysfunction, endothelial injury, inflammatory response, hypercoagulable state, predictive model
Introduction
Preeclampsia (PE) is a pregnancy-specific syndrome that typically occurs after 20 weeks of gestation. It is mainly characterized by hypertension and proteinuria and, in severe cases, may involve critical organs such as the liver, kidneys, and brain, posing a threat to both maternal and fetal life.1–3 PE exhibits significant pathophysiological heterogeneity, broadly categorized into early-onset (before 34 weeks) and late-onset (at or after 34 weeks) subtypes, which may involve distinct placental and maternal vascular mechanisms and influence biomarker profiles.4,5 In China, the incidence of PE is approximately 2%–6%, a figure that is comparable to or even higher than rates observed in many other developing countries.6 Although the exact etiology remains unclear, factors such as insufficient placental perfusion, endothelial dysfunction, immune imbalance, and inflammatory responses are considered to play key roles in the pathogenesis of PE.7
In recent years, serum uric acid (UA), a byproduct of purine metabolism and a mediator of oxidative stress, has gained increasing attention.8 Multiple studies have shown that serum UA levels in PE patients are significantly higher than in normotensive pregnant women, suggesting a potential role in the onset and progression of the disease.9 However, due to variations in study design and inclusion criteria, the relationship between uric acid and PE remains controversial. The primary controversy centers on whether elevated serum UA is an active contributor to the pathogenesis of PE (eg, by promoting endothelial dysfunction, inflammation, and oxidative stress) or merely a secondary consequence of reduced renal clearance and/or increased tissue ischemia.10,11 Consequently, its clinical utility as a diagnostic or prognostic marker is still under debate.
On the other hand, coagulation dysfunction is also a key pathological feature of PE, often manifesting as a hypercoagulable state and even disseminated intravascular coagulation (DIC). Some researchers have pointed out that disruptions in the coagulation-fibrinolysis system may precede the appearance of clinical symptoms and contribute to early disease progression.12,13 Studies have shown that parameters such as platelet indices, prothrombin time, D-dimer levels, plasminogen activator inhibitor-1 (PAI-1), and P-selectin may have certain predictive value.14,15
Currently, it remains inconclusive whether there is an intrinsic link between elevated serum uric acid levels and coagulation dysfunction in PE, and the underlying mechanisms are not yet fully understood. Nevertheless, investigating their potential association is crucial, as converging pathways—such as endothelial cell activation, oxidative stress, and inflammatory responses—might connect hyperuricemia to the prothrombotic state observed in PE.16,17 Elucidating this interplay could provide deeper insights into the integrated pathophysiology of PE and identify novel therapeutic targets. Therefore, this review aims to summarize the research progress on changes in uric acid and coagulation abnormalities in PE, analyze their potential interaction mechanisms, specifically within the context of endothelial damage, oxidative stress, and inflammation, and explore their possible clinical value in disease prediction and management. To achieve this, the review will first outline the independent alterations in UA metabolism and the coagulation system in PE, then synthesize existing evidence for their interconnection, discuss proposed mechanistic links, and finally evaluate their combined potential as biomarkers and future research directions.
Overview of the Pathogenesis of Preeclampsia
The pathogenesis of preeclampsia remains incompletely understood, but it is widely recognized as a complex disorder involving the dysregulation of multiple physiological processes. One of the prevailing theories suggests that impaired trophoblast invasion in early pregnancy leads to defective remodeling of the uterine spiral arteries, resulting in insufficient placental perfusion. This induces local placental ischemia and hypoxia.18,19 These pathological changes further stimulate the synthesis and release of various pro-inflammatory cytokines, such as interleukin-2 (IL-2) and interleukin-6 (IL-6), into the maternal circulation, thereby damaging the vascular endothelium.20 The hypoxic placenta upregulates hypoxia-inducible factors (HIFs), which in turn promote the transcription and release of anti-angiogenic factors (like sFlt-1) and pro-inflammatory mediators, establishing a systemic inflammatory milieu.21
Elevated levels of inflammatory cytokines are particularly evident in patients with PE. IL-2 may inhibit normal trophoblast function and disrupt placental development, while IL-6 can enhance B lymphocyte activity and promote the formation and deposition of immune complexes.22 These immune complexes deposit on vascular walls and glomerular basement membranes, inducing upregulation of endothelial adhesion molecules and exacerbating endothelial dysfunction. Endothelial injury not only impairs the synthesis of vasodilators such as prostacyclin but also induces vasoconstriction, increased peripheral resistance, and microthrombus formation. Ultimately, these changes lead to a hypercoagulable state,2,6,14 as illustrated in Figure 1.
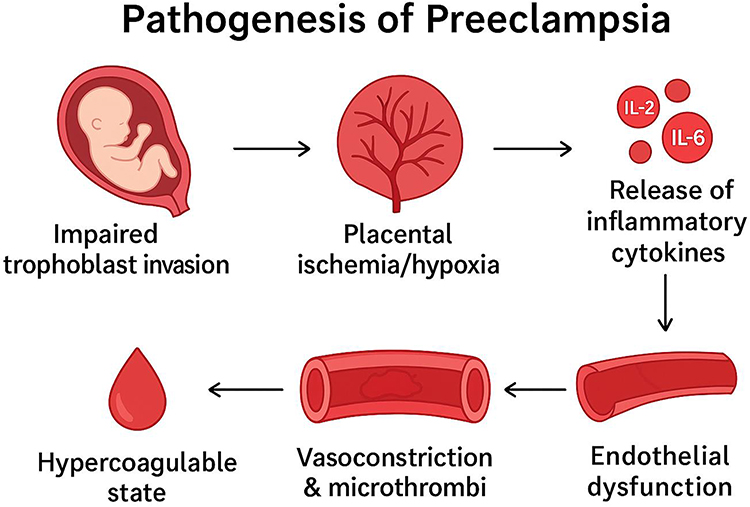 |
Figure 1 Pathogenesis of Preeclampsia, Schematic representation of the proposed pathophysiological mechanisms underlying preeclampsia. Impaired trophoblast invasion in early pregnancy results in inadequate remodeling of uterine spiral arteries, leading to placental ischemia and hypoxia. The hypoxic placenta releases inflammatory cytokines such as interleukin-2 (IL-2) and interleukin-6 (IL-6), which contribute to endothelial dysfunction. Endothelial injury induces vasoconstriction, increases peripheral vascular resistance, and promotes microthrombus formation, ultimately leading to a hypercoagulable state. |
Severe PE is often accompanied by widespread endothelial damage, activation of the coagulation system, and chronic disseminated intravascular coagulation (DIC), indicating that complex interactions may exist among coagulation, inflammation, and endothelial dysfunction.23,24 These mechanisms are thought to be present even in the early stages of PE, offering potential early diagnostic and therapeutic targets.
Changes and Significance of Serum Uric Acid in Preeclampsia
An increasing number of studies have shown that serum uric acid (UA) levels are closely associated with the development of hypertensive disorders of pregnancy (HDCP), particularly preeclampsia (PE).25 However, whether UA can serve as a sensitive early biomarker for predicting PE remains controversial. Some prospective and case-control studies have found that elevated UA levels in early or mid-pregnancy are positively correlated with the risk of developing PE. For instance, a follow-up study involving nearly one thousand pregnant women indicated that elevated UA levels increased the risk of HDCP, though its predictive value was not superior to traditional indicators such as proteinuria.26,27 Additionally, a cohort study by Mashak et al reported that elevated UA levels in early pregnancy significantly increased the incidence of PE, with an adjusted odds ratio (OR) of 7.1 (95% CI: 3.2–15.7). Receiver operating characteristic (ROC) curve analysis confirmed that UA had high predictive accuracy, with an area under the curve (AUC) of 0.955.28 Another study noted that when mid-pregnancy UA levels exceeded 213.24 μmol/L, the risk of developing PE increased by approximately 1.8 times.29
Nevertheless, not all studies support the independent predictive value of UA as an early indicator for PE. The comparability of these studies is often limited by heterogeneity in key factors, including the gestational age at which UA is measured, the classification of PE (eg, early- vs late-onset), and the baseline risk profiles of the study populations (eg, nulliparity, pre-existing hypertension, or obesity).30 This heterogeneity, combined with the fact that hyperuricemia in PE can arise from both reduced renal excretion and increased cellular turnover/ischemia, contributes to the ongoing controversy regarding its predictive utility. Some literature reviews suggest that although UA levels are often elevated in patients with PE, their accuracy and clinical utility in assessing disease severity or enabling early identification are still limited.31 As a result, serum UA is currently not recommended as a standalone marker for diagnosis or clinical decision-making. A potential reconciliation of these conflicting viewpoints is that UA may be a more robust biomarker within specific PE subtypes (such as early-onset PE with significant renal involvement) or when integrated into multi-marker prediction models, rather than as a universal, standalone test.32
On the other hand, elevated UA levels are also closely related to maternal and fetal outcomes in PE patients. Some studies have shown that the combined monitoring of serum UA and cystatin C (CysC) may help detect early signs of renal dysfunction, indicating its potential clinical value in disease management.33 Some researchers have suggested that when UA levels consistently exceed 400 μmol/L, there is an increased risk of adverse outcomes such as intrauterine fetal distress, fetal growth restriction (FGR), and perinatal mortality. In such cases, intensified monitoring and timely delivery should be considered when necessary.34 Additionally, mid-pregnancy combined testing of UA and blood lipid levels has been proposed as a supplementary approach to predicting adverse pregnancy outcomes.
In summary, although substantial evidence supports the important role of serum UA in the pathogenesis and progression of PE, there is still no unified standard or consensus regarding its specific application in early diagnosis, risk stratification, and maternal-fetal outcome prediction.35 At present, it is more appropriate to consider UA as part of a comprehensive assessment system, used in conjunction with other clinical indicators to improve predictive accuracy and guide individualized management strategies.
Coagulation Abnormalities in Preeclampsia
Pregnancy is a physiological state characterized by hypercoagulability, primarily marked by increased levels of coagulation factors (eg, Factors VII, VIII, and X) and fibrinogen (FIB), along with decreased concentrations of natural anticoagulants such as protein S. Additionally, fibrinolytic activity is enhanced, creating a pro-hemostatic environment that helps minimize blood loss during delivery. This hypercoagulable state becomes more pronounced as gestation progresses, especially in the third trimester, with coagulation parameters such as prothrombin time (PT), activated partial thromboplastin time (APTT), and thrombin time (TT) generally shortened. These changes are considered a physiological adaptation that facilitates hemostasis after placental separation and supports endometrial repair.36,37
However, in hypertensive disorders of pregnancy—particularly preeclampsia (PE)—this physiological hypercoagulability is further exaggerated and dysregulated, leading to pathological coagulation abnormalities. Studies have shown that PE patients often exhibit thrombocytopenia, consumptive decline in coagulation factors, suppression of fibrinolytic function, and a tendency toward microvascular thrombosis, indicating a disruption in the dynamic balance between coagulation and fibrinolysis.38,39 These pathological changes stem primarily from placental hypoperfusion and hypoxia-induced widespread endothelial injury. Hypoxia prompts placental trophoblasts to release anti-angiogenic factors such as soluble fms-like tyrosine kinase-1 (sFlt-1), further damaging the endothelial barrier and exacerbating the hypercoagulable state.
At the molecular level, damaged endothelial cells in PE express large amounts of tissue factor (TF), activating the extrinsic coagulation pathway. Simultaneously, exposed collagen and inflammatory mediators (eg, IL-6, TNF-α) trigger the intrinsic pathway, leading to excessive thrombin generation and subsequent platelet adhesion and aggregation.40 Studies have found significantly elevated levels of thromboxane B2 (TXB2) and reduced levels of prostacyclin I2 (PGI2) in the peripheral blood of patients with severe PE, contributing to vasoconstriction, elevated blood pressure, and further platelet activation.41
In terms of laboratory findings, PT, APTT, and TT are often prolonged in PE, particularly in severe cases. Meanwhile, FIB levels are reduced due to both increased consumption and impaired synthesis. A study involving 313 third-trimester pregnant women reported that FIB ≤ 2.87 g/L predicted PE with a sensitivity of 68%, specificity of 98%, and a positive predictive value of 97%.42 Notably, in predicting severe PE, this threshold yielded a sensitivity of 84% and an accuracy of 92.2%.
Von Willebrand factor (vWF), a glycoprotein synthesized by vascular endothelial cells, is a sensitive marker of endothelial damage and is significantly elevated in the plasma of PE patients. A prospective study found that vWF > 1.63 IU/mL predicted PE with a sensitivity of 68% and a specificity of 84.4%.43 vWF enhances platelet adhesion to damaged vessel walls, promoting platelet aggregation and thrombosis, making it a potential early biomarker for PE.
P-selectin is an adhesion molecule released from platelet alpha granules and activated endothelial cells. It facilitates platelet–endothelial interactions and participates in inflammatory and thrombotic processes. A study by Akolekar et al involving 8234 pregnant women found that peripheral blood P-selectin levels were significantly elevated at 11–13 weeks in those who later developed PE. When combined with uterine artery resistance index, the accuracy of predicting early-onset PE reached 90.3%.44 Thus, P-selectin may provide important supplemental information for early prediction and risk assessment of PE.
D-dimer (D-D), a fibrin degradation product released during fibrinolytic activation, is a sensitive marker of both hypercoagulability and secondary fibrinolysis. Studies have shown that D-D levels are significantly higher in PE patients than in normotensive pregnant women, particularly in cases of severe PE or HELLP syndrome. One study reported that D-D > 2170 ng/mL predicted HELLP syndrome with 91% sensitivity and 69% accuracy.45 Research by Pinheiro et al demonstrated that D-D could predict severe PE with an accuracy of 93.8%, highlighting its clinical value in assessing the severity of hypertensive disorders during pregnancy.
Plasminogen activator inhibitor-1 (PAI-1), a serine protease inhibitor synthesized by endothelial cells, primarily inhibits tissue-type plasminogen activator (t-PA), thereby suppressing fibrinolysis. In PE patients, hypoxia and inflammation synergistically upregulate PAI-1 expression, creating an antifibrinolytic state. A study found that PAI-1 > 77.3 ng/mL predicted PE with an accuracy of 75.3%, sensitivity of 84.6%, and specificity of 66.7%.46 These findings suggest that PAI-1 may play a role in the early identification of PE, although its independent predictive ability still requires validation alongside other markers. A summary of the key coagulation parameters altered in preeclampsia, their pathophysiological significance, and associated clinical values is provided in Table 1.
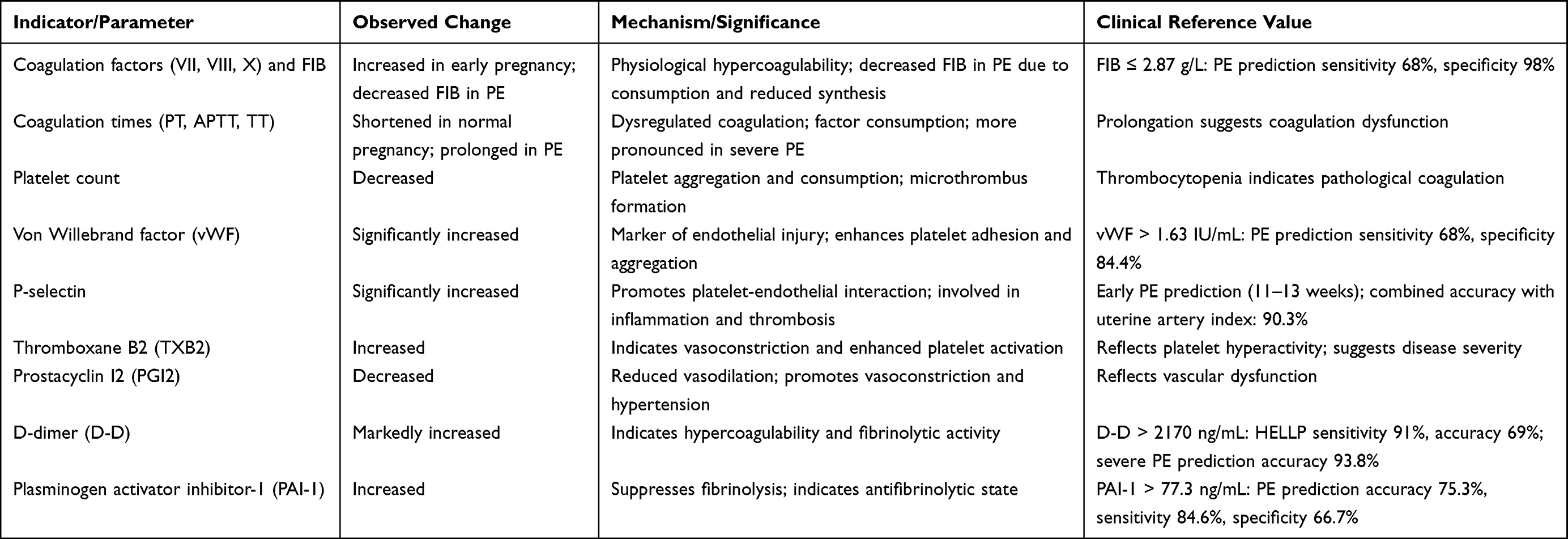 |
Table 1 Coagulation Abnormalities and Related Indicators in Preeclampsia |
Relationship Between Uric Acid and Coagulation Dysfunction
In recent years, increasing attention has been paid to whether elevated serum uric acid (UA) levels contribute to or exacerbate coagulation dysfunction in preeclampsia (PE). Both basic research and clinical observations suggest that UA is not merely a metabolic byproduct or an indirect indicator of renal function in PE, but may also actively participate in pathological processes such as inflammation, endothelial damage, and vascular dysfunction, ultimately affecting the coagulation–fibrinolysis balance.
Firstly, UA is believed to activate the nuclear factor-kappa B (NF-κB) pathway, promoting the release of pro-inflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), which in turn induce the expression of coagulation factors and activate platelets.47 Furthermore, UA can stimulate vascular endothelial cells to release tissue factor (TF), thereby initiating the extrinsic coagulation pathway. A study by Han et al48 on pregnant women with PE found a significant positive correlation between elevated serum UA levels and plasma TF concentrations. The increases in both were also associated with D-dimer and fibrinogen (FIB) levels, suggesting that UA may contribute to PE pathogenesis via coagulation system activation.
Secondly, UA-induced endothelial dysfunction is a major mechanism promoting a hypercoagulable state. High UA concentrations inhibit nitric oxide (NO) synthesis and impair endothelial function, increasing the expression of adhesion molecules such as ICAM-1 and VCAM-1.49 This promotes leukocyte adhesion and inflammatory infiltration, leading to endothelial activation and platelet aggregation. This process is closely related to elevated P-selectin and von Willebrand factor (vWF) levels, which further aggravate coagulation dysfunction.
Clinically, a study by Jin et al40 involving 98 PE patients demonstrated significant positive correlations between serum UA and both D-dimer and PAI-1 levels (r = 0.64 and 0.71, P < 0.01), along with associations between UA and prolonged PT and APTT. These findings indicate that elevated UA in PE may not only reflect disease severity but also act as a potential trigger of hypercoagulability and fibrinolytic suppression. Conversely, the potential for coagulation dysfunction to influence UA levels, while less studied, should be considered. Significant coagulation activation and microthrombus formation can lead to ischemic damage in organs such as the kidneys. This renal ischemia impairs uric acid excretion, potentially creating a secondary, compensatory elevation in serum UA levels. Therefore, the relationship may be bidirectional: UA can promote coagulation, and the resultant coagulopathy may exacerbate hyperuricemia through end-organ damage.33
In summary, UA may influence coagulation function in PE through multiple mechanisms, including procoagulant effects, antifibrinolytic activity, and exacerbation of endothelial injury. However, most existing studies are retrospective or observational, and a more critical evaluation of their design and limitations is warranted. Future large-scale prospective studies across diverse populations are needed to clarify causality and specific molecular pathways, which remain important areas for future research.
Clinical Significance and Research Prospects
The synergistic relationship between serum uric acid and coagulation dysfunction in preeclampsia highlights their potential clinical value in disease monitoring and management. Firstly, as an indicator of disease severity, elevated UA levels have been confirmed to correlate with severe PE, HELLP syndrome, placental abruption, and preterm birth.50 Meanwhile, coagulation parameters such as D-dimer, PAI-1, and vWF also play key roles in disease progression. Joint monitoring of UA and coagulation-related markers may improve the accuracy of PE classification and assist in identifying high-risk patients.
Secondly, early elevations of serum UA and certain coagulation markers provide new perspectives for early prediction and risk stratification of PE.51 Studies have shown that UA levels may rise before the onset of clinical symptoms, while markers like P-selectin and PAI-1 also show increasing trends weeks before PE onset. Combining these biomarkers in a unified monitoring strategy holds promise for developing highly sensitive and specific predictive models. For instance, a multifactorial model combining UA, the soluble fms-like tyrosine kinase-1 to placental growth factor ratio (sFlt-1/PlGF), and D-dimer has been shown to significantly enhance predictive power for early-onset PE. One study reported that such a combination achieved an area under the curve (AUC) of 0.92, with superior sensitivity and specificity compared to any single marker alone.52 Similarly, another predictive model that integrated maternal factors with uterine artery pulsatility index, mean arterial pressure, PAI-1, and P-selectin demonstrated an AUC of 0.90 for early-onset PE, underscoring the value of combinatorial approaches.53
Furthermore, in terms of clinical intervention, dynamic monitoring of UA and coagulation indicators may facilitate personalized treatment and surveillance strategies. For diagnosed PE patients, a sustained increase in UA accompanied by a rapid rise in D-dimer suggests ongoing coagulation system activation and possible disease progression, indicating the need to consider timely delivery to reduce maternal-fetal risks. For asymptomatic pregnant women with elevated UA, enhanced prenatal monitoring, shorter follow-up intervals, and dynamic evaluation may help delay or prevent the onset of PE.
Future studies should aim to clarify the molecular mechanisms by which UA regulates coagulation factor expression in PE, including whether it acts through oxidative stress or endothelial dysfunction to indirectly activate the coagulation cascade. Additionally, the development of multifactorial predictive models centered on UA and coagulation parameters, validated by multicenter, large-sample prospective cohort studies, is key to improving prediction accuracy and broad clinical applicability. It is also worth investigating whether interventions that reduce UA levels (eg, non-purine uric acid-lowering drugs) can improve coagulation abnormalities or delay the progression of PE, representing an important direction for future research.
Conclusion
Preeclampsia is a pregnancy-related disorder that poses a serious threat to maternal and fetal health. Its pathophysiological basis involves placental hypoperfusion, endothelial dysfunction, inflammation, and coagulation system disturbances. Serum uric acid, as a key product of oxidative stress and metabolic imbalance, has recently been identified as being closely associated with the development and progression of PE. At the same time, coagulation abnormalities are evident in the early stages of PE and are driven by endothelial injury and inflammatory responses, further exacerbating the disease process.54
Multiple studies suggest that elevated serum UA may affect coagulation function through mechanisms such as endothelial damage, tissue factor induction, and fibrinolysis inhibition, contributing to a mutually reinforcing cycle of hypercoagulability in PE.55,56 This review has synthesized evidence suggesting a potential bidirectional relationship, where UA promotes a prothrombotic state, and coagulation dysfunction may, in turn, exacerbate hyperuricemia through renal ischemic mechanisms. Clinically, the combined assessment of UA and coagulation biomarkers (such as D-dimer, PAI-1, vWF, and FIB) may enhance early prediction and severity assessment of PE, offering a theoretical basis for precision pregnancy management.
However, it is crucial to acknowledge the limitations of the current evidence base. The majority of studies elucidating the UA-coagulation relationship are observational or in vitro, which precludes definitive conclusions about causality. Furthermore, heterogeneity in PE definitions, study populations, and laboratory methods across studies complicates the comparison and consolidation of findings. Future research should, therefore, prioritize well-designed, large-scale prospective studies across diverse populations to validate these interactions and their clinical utility. The ultimate goal is to advance from “single-marker evaluation” to validated “multidimensional risk models”, integrating UA, coagulation parameters, angiogenic factors, and maternal characteristics to provide more scientific support for the early detection, diagnosis, and individualized treatment of preeclampsia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rosenberg EA, Seely EW. Update on preeclampsia and hypertensive disorders of pregnancy. Endocrinol Metab Clinics North Am. 2024;53(3):377–389. doi:10.1016/j.ecl.2024.05.012
2. Melchiorre K, Giorgione V, Thilaganathan B. The placenta and preeclampsia: villain or victim? Am J Clin Exp Obstet Gynecol. 2022;226(2s):S954–s962. doi:10.1016/j.ajog.2020.10.024
3. Jung E, Romero R, Yeo L, et al. The etiology of preeclampsia. Am J Clin Exp Obstet Gynecol. 2022;226(2s):S844–s866. doi:10.1016/j.ajog.2021.11.1356
4. Ziganshina MM, Muminova KT, Khasbiullina NR, et al. Characterization of vascular patterns associated with endothelial glycocalyx damage in early-and late-onset preeclampsia. Biomedicines. 2022;10(11):2790. doi:10.3390/biomedicines10112790
5. Panaschatenko A, Panova IA, Malyshkina AI, et al. Immunological and pathomorphological aspects of early and late preeclampsia. Медицинская иммунология. 2021;23(4):845–852.
6. MacDonald TM, Walker SP, Hannan NJ, Tong S, Kaitu’u-Lino TJ. Clinical tools and biomarkers to predict preeclampsia. EBioMedicine. 2022;75:103780. doi:10.1016/j.ebiom.2021.103780
7. Ives CW, Sinkey R, Rajapreyar I, Tita ATN, Oparil S. Preeclampsia-pathophysiology and clinical presentations: JACC state-of-the-art review. J Am Coll Cardiol. 2020;76(14):1690–1702. doi:10.1016/j.jacc.2020.08.014
8. Zhou Y, Xiao C, Yang Y. Pre-pregnancy body mass index combined with peripheral blood PLGF, DCN, LDH, and UA in a risk prediction model for pre-eclampsia. Front Endocrinol. 2023;14:1297731. doi:10.3389/fendo.2023.1297731
9. Yun L, Yu X, Xu R. Uric acid/superoxide dismutase can predict progression of gestational hypertension to preeclampsia. Front Cardiovasc Med. 2023;10:1148376. doi:10.3389/fcvm.2023.1148376
10. Xiong Y, Zheng P, Chen C, He C, Yang X, Cheng W. Association of maternal serum uric acid levels with LBW/SGA: a large retrospective cohort study. BMC Pregnancy Childbirth. 2024;24(1):160. doi:10.1186/s12884-024-06261-0
11. Suliman NA, Awadalla KE, Bakheit KH, Mohamed AO. Cancer antigen 125 and C-reactive protein inflammatory mediators and uric acid in association with preeclampsia in North Kordofan State, Western Sudan. PLoS One. 2023;18(1):e0280256. doi:10.1371/journal.pone.0280256
12. Nunes PR, Mattioli SV, Sandrim VCJC. NLRP3 activation and its relationship to endothelial dysfunction and oxidative stress: implications for preeclampsia and pharmacological interventions. Cells. 2021;10(11):2828.
13. Han C, et al. Oxidative Stress and Preeclampsia-Associated. Cell Oxid Stress. 2021;183.
14. Ramasamy S, Saravanan S, Rajendran J. Perspectives on the pathogenesis and complications of PE. 2023.
15. Kutllovci Hasani K, Ajeti N, Goswami NJMS. Understanding Preeclampsia: cardiovascular Pathophysiology. Histopathol Insights Mol Biomark. 2025;13(3):154.
16. Joy S, Venkatachalam K, Binesh A. Emerging perspectives on biomarker panels in deep vein thrombosis: the combined roles of D-dimer, P-selectin, and microparticles. Ann Vasc Surg2025.
17. Erez O, Othman M, Rabinovich A, et al. DIC in pregnancy–pathophysiology, clinical characteristics, diagnostic scores, and treatments. J Blood Med. 2022;13:21–44. doi:10.2147/JBM.S273047
18. Hauspurg A, Jeyabalan A. Postpartum preeclampsia or eclampsia: defining its place and management among the hypertensive disorders of pregnancy. Am J Clin Exp Obstet Gynecol. 2022;226(2s):S1211–s1221. doi:10.1016/j.ajog.2020.10.027
19. Alese MO, Moodley J, Naicker T. Preeclampsia and HELLP syndrome, the role of the liver. J Matern Fetal Neonatal Med. 2021;34(1):117–123. doi:10.1080/14767058.2019.1572737
20. Roberts JM, Rich-Edwards JW, McElrath TF, Garmire L, Myatt L. Subtypes of Preeclampsia: recognition and Determining Clinical Usefulness. Hypertension. 2021;77(5):1430–1441. doi:10.1161/HYPERTENSIONAHA.120.14781
21. Albogami SM, et al. Hypoxia-inducible factor 1 and preeclampsia: a new perspective. Curr Hypertens Rep. 2022;24(12):687–692.
22. Roberts JM. Preeclampsia epidemiology(ies) and pathophysiology(ies). Best Pract Res Clin Obstet Gynaecol. 2024;94:102480. doi:10.1016/j.bpobgyn.2024.102480
23. Ma’ayeh M, Costantine MM. Prevention of preeclampsia. Semin Fetal Neonatal Med. 2020;25(5):101123. doi:10.1016/j.siny.2020.101123
24. Yang Y, Le Ray I, Zhu J, Zhang J, Hua J, Reilly M. Preeclampsia prevalence, risk factors, and pregnancy outcomes in Sweden and China. JAMA Network Open. 2021;4(5):e218401. doi:10.1001/jamanetworkopen.2021.8401
25. Yagel S, Cohen SM, Admati I, et al. Expert review: preeclampsia type I and type II. Am J Obstet Gynecol MFM. 2023;5(12):101203. doi:10.1016/j.ajogmf.2023.101203
26. Shenhav S, Harel I, Solt I, et al. Fetoplacental unit involvement in uric acid production in women with severe preeclampsia: a prospective case control pilot study. J Matern Fetal Neonatal Med. 2024;37(1):2399304. doi:10.1080/14767058.2024.2399304
27. Püschl IC, Thaneswaran Vyramuthu M, Bonde L, et al. Is salivary uric acid, a putative biomarker of pre-eclampsia, of maternal, placental, or fetal origin? Eur J Obstet Gynecol Reprod Biol. 2024;295:34–41. doi:10.1016/j.ejogrb.2024.02.003
28. Mohamed RA, Ali IA. Role of neutrophil / lymphocyte ratio, uric acid / albumin ratio and uric acid / creatinine ratio as predictors to severity of preeclampsia. BMC Pregnancy Childbirth. 2023;23(1):763. doi:10.1186/s12884-023-06083-6
29. Mashak B, Bagheri RB, Noorani G, Soleimanifakhr S, Ataei M. Comparison of hemodynamic and biochemical factors and pregnancy complications in women with/without preeclampsia. Maedica. 2022;17(2):363–370. doi:10.26574/maedica.2022.17.2.363
30. Liu D, Li C, Huang P, et al. Serum levels of uric acid may have a potential role in the management of immediate delivery or prolongation of pregnancy in severe preeclampsia. Hypertens Pregnancy. 2020;39(3):260–266. doi:10.1080/10641955.2020.1761377
31. Neave ELA. Thrombotic microangiopathies in pregnancy: presentations, pathogenesis, challenges. 2025. UCL (University College London).
32. Lai Q, Zhang X. Predictive value of early pregnancy uric acid levels for adverse pregnancy outcomes. Afr J Reproduct Health. 2024;28(12):52–60. doi:10.29063/ajrh2024/v28i12.6
33. Dong L, Li W, Niu X, Luan L, Hui S. Correlation of uric acid and lipid levels with preeclampsia and final pregnancy outcome in late pregnancy. Am J Transl Res. 2025;17(4):2800–2808. doi:10.62347/HBLW4532
34. Chen Y, Ou W, Lin D, et al. Increased uric acid, gamma-glutamyl transpeptidase and alkaline phosphatase in early-pregnancy associated with the development of gestational hypertension and preeclampsia. Front Cardiovasc Med. 2021;8:756140. doi:10.3389/fcvm.2021.756140
35. Afrose D, Johansen MD, Nikolic V, et al. Evaluating oxidative stress targeting treatments in in vitro models of placental stress relevant to preeclampsia. Front Cell Develop Biol. 2025;13:1539496. doi:10.3389/fcell.2025.1539496
36. Xu C, Li Y, Zhang W, Wang Q. Analysis of perinatal coagulation function in preeclampsia. Medicine. 2021;100(26):e26482. doi:10.1097/MD.0000000000026482
37. Walsh SW, Strauss JF. 3rd: pregnancy-specific expression of protease-activated receptor 1: a therapeutic target for prevention and treatment of preeclampsia? Am J Clin Exp Obstet Gynecol. 2022;226(2s):S945–s953. doi:10.1016/j.ajog.2021.11.1367
38. Villalobos-Labra R, Liu R, Spaans F, et al. Placenta-derived extracellular vesicles from preeclamptic pregnancies impair vascular endothelial function via lectin-like oxidized LDL receptor-1. Hypertension. 2023;80(10):2226–2238. doi:10.1161/HYPERTENSIONAHA.123.21205
39. Ronnje L, Länsberg JK, Vikhareva O, Hansson SR, Herbst A, Zaigham M. Complicated COVID-19 in pregnancy: a case report with severe liver and coagulation dysfunction promptly improved by delivery. BMC Pregnancy Childbirth. 2020;20(1):511. doi:10.1186/s12884-020-03172-8
40. Peng J, Zhao Q, Pang W, Li Y, Dong X. Changes of coagulation function and platelet parameters in preeclampsia and their correlation with pregnancy outcomes. J Clin Hypertens. 2024;26(10):1181–1187. doi:10.1111/jch.14893
41. Palomo M, Youssef L, Ramos A, et al. Differences and similarities in endothelial and angiogenic profiles of preeclampsia and COVID-19 in pregnancy. Am J Clin Exp Obstet Gynecol. 2022;227(2):
42. Narkhede AM, Karnad DR. Preeclampsia and Related Problems. Indian J Crit Care Med. 2021;25(Suppl 3):S261–s266. doi:10.5005/jp-journals-10071-24032
43. Paidas MJ, Tita ATN, Macones GA, et al. Prospective, randomized, double-blind, placebo-controlled evaluation of the pharmacokinetics, safety and efficacy of recombinant antithrombin versus placebo in preterm preeclampsia. Am J Clin Exp Obstet Gynecol. 2020;223(5):
44. Martini C, Saeed Z, Simeone P, et al. Preeclampsia: insights into pathophysiological mechanisms and preventive strategies. Am J Prev Cardiol. 2025;23:101054. doi:10.1016/j.ajpc.2025.101054
45. Loskutova T, Donskay Y, Petulko A, Kryachkova N. Risk of placenta-associated complications at preeclampsia in pregnant women with thrombophilia. Wiadomosci lekarskie. 2022;75(12):2969–2973. doi:10.36740/WLek202212113
46. Liu Y, Zhou M, Cheng H, Du J. Effect of low-molecular-weight heparin calcium combined with magnesium sulfate and labetalol on coagulation, vascular endothelial function and pregnancy outcome in early-onset severe preeclampsia. Eur J Clin Pharmacol. 2024;80(10):1495–1501. doi:10.1007/s00228-024-03712-7
47. Xie RH, Ye XL, Tang CY, Wang YH, Zhong LX. Associated clinical factors for coagulation dysfunction due to trimeresurus stejnegeri: a retrospective observational study. J Toxicol. 2023;2023:8832355. doi:10.1155/2023/8832355
48. Han Q, Zheng W, Guo XD, et al. A new predicting model of preeclampsia based on peripheral blood test value. Eur Rev Med Pharmacol Sci. 2020;24(13):7222–7229. doi:10.26355/eurrev_202007_21874
49. Kovacheva VP, Venkatachalam S, Pfister C, Anwer T. Preeclampsia and eclampsia: enhanced detection and treatment for morbidity reduction. Best Pract Res Clin Anaesth. 2024;38(3):246–256. doi:10.1016/j.bpa.2024.11.001
50. Jin PP, Ding N, Dai J, Liu XY, Mao PM. Investigation of the relationship between changes in maternal coagulation profile in the first trimester and the risk of developing preeclampsia. Heliyon. 2023;9(7):e17983. doi:10.1016/j.heliyon.2023.e17983
51. El hamaoui D, Marchelli A, Gandrille S, et al. Thrombin cleaves membrane-bound endoglin potentially contributing to the heterogeneity of circulating endoglin in preeclampsia. Commun Biol. 2025;8(1):316. doi:10.1038/s42003-025-07751-3
52. Bucak M, Turan S, Turan OM. Stepwise risk stratification of early-onset preeclampsia: integrating mid-trimester uterine artery Doppler and maternal comorbidities. BMC Pregnancy Childbirth. 2025;25(1):758. doi:10.1186/s12884-025-07864-x
53. Garrido-Giménez C, Cruz-Lemini M, Álvarez FV, et al. Predictive model for preeclampsia combining sFlt-1, PlGF, NT-proBNP, and uric acid as biomarkers. J Clin Med. 2023;12(2):431. doi:10.3390/jcm12020431
54. Cui HX, Chen C, Jung YM, et al. Neutrophil-to-lymphocyte ratio (NLR) as a predictive index for liver and coagulation dysfunction in preeclampsia patients. BMC Pregnancy Childbirth. 2023;23(1):4. doi:10.1186/s12884-022-05335-1
55. Andersson M, Bengtsson P, Karlsson O, et al. Platelet aggregation and thromboelastometry monitoring in women with preeclampsia: a prospective observational study. Int J Obstet Anesth. 2025;61:104297. doi:10.1016/j.ijoa.2024.104297
56. Alemayehu E, Mohammed O, Belete MA, et al. Association of prothrombin time, thrombin time and activated partial thromboplastin time levels with preeclampsia: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2024;24(1):354. doi:10.1186/s12884-024-06543-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Factors for Fetal Growth Restriction in Patients with Preeclampsia: A Clinical Prediction Study
Yan M, Li F, Jun S, Li L, You W, Hu L
International Journal of General Medicine 2025, 18:2289-2301
Published Date: 28 April 2025
Exploring the Therapeutic Potential of FSGTC for Osteoarthritis: A Comprehensive Study Combining Nested Case Analysis, Network Pharmacology, and Experimental Validation
He M, Liu J, Gao W, Sun Y, Chen X, Fang Y
Drug Design, Development and Therapy 2025, 19:5123-5141
Published Date: 17 June 2025
Fatty Acid Transporter CD36 Promotes Ox-LDL-Induced Senescence of Vascular Endothelial Cells in Preeclampsia

Xiao Y, Tao M, Yu Y, Bai R, Zhuang Y, Huang Q, He J, Lin Z, Gao M, Li J, Wang Y, Xu Y, Shen X, Huang Z, Yao Y, Chen Z, Chen Q, Wang Z
Journal of Inflammation Research 2025, 18:12801-12816
Published Date: 16 September 2025