Back to Journals » Cancer Management and Research » Volume 18

Research Progress of HER2 in Cervical Carcinoma
Authors Yang X ![]() , Tang Y, Liu G, Hui H, Guo L
, Tang Y, Liu G, Hui H, Guo L ![]() , Li N, Zhou Y
, Li N, Zhou Y
Received 31 March 2026
Accepted for publication 6 June 2026
Published 26 June 2026 Volume 2026:18 613300
DOI https://doi.org/10.2147/CMAR.S613300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Yong Teng
Xinru Yang,1,* Yi Tang,1,* Genyun Liu,2 Hui Hui,2 Lin Guo,2 Na Li,2 Yun Zhou2
1The Affiliated Xuzhou Clinical College of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Department of Radiation Oncology, Southeast University Affiliated Xuzhou Central Hospital, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yun Zhou, Department of Radiation Oncology, Southeast University Affiliated Xuzhou Central Hospital, Xuzhou, Jiangsu, 220005, People’s Republic of China, Tel +86 18952172811, Email [email protected]
Abstract: Cervical cancer (CC) remains a major gynecological malignancy worldwide, and patients with recurrent, metastatic, or treatment-resistant disease continue to have limited therapeutic options. Human epidermal growth factor receptor 2 (HER2) is a proto-oncogenic receptor tyrosine kinase involved in tumorigenesis and progression through gene amplification, activating mutation, and protein overexpression. Although HER2 has been extensively studied and successfully targeted in breast and gastric cancers, its biological and therapeutic significance in CC remains less clearly defined and appears to vary according to histological subtype and molecular context. Current evidence suggests that HER2 alterations are relatively uncommon in unselected CC populations but may be enriched in selected adenocarcinoma subgroups, including gastric-type and other human papillomavirus (HPV)-independent variants. This review synthesizes current evidence regarding the structure, function, expression patterns, prognostic implications, testing criteria, and therapeutic relevance of HER2 in CC. Particular attention is given to HER2-directed antibody-drug conjugates, especially trastuzumab deruxtecan (T-DXd), which have emerged as an important recent therapeutic advance and have renewed interest in HER2 as an actionable target in selected patients with HER2-expressing cervical carcinoma. This review further highlights the need for biomarker-driven patient selection, standardized HER2 assessment, and rational integration of HER2-directed strategies into precision treatment for CC.
Keywords: cervical cancer, HER2, cervical adenocarcinoma, targeted therapy
Introduction
Cervical cancer (CC) remains one of the most common gynecological malignancies worldwide. According to Global Cancer Statistics, cervical cancer ranked as the fourth most common cancer among women globally in 2022, with approximately 660,000 new cases and 350,000 deaths.1 Although screening and human papillomavirus (HPV) vaccination have reduced the overall disease burden in many regions, patients with recurrent, metastatic, or treatment-resistant cervical cancer continue to have limited therapeutic options and poor clinical outcomes.2
Cervical cancer consists of biologically and clinically distinct histological subtypes. Squamous cell carcinoma (SCC) accounts for the majority of cases and has shown a declining incidence in many populations. In contrast, cervical adenocarcinoma represents approximately 15% to 20% of cervical cancer cases and has increased in relative frequency over recent decades.3,4 Compared with SCC, adenocarcinoma is often associated with less favorable clinical behavior and poorer treatment outcomes.5 According to the International Endocervical Adenocarcinoma Criteria and Classification (IECC), cervical adenocarcinoma can be divided into HPV-associated adenocarcinoma, HPV-independent adenocarcinoma, and adenocarcinoma not otherwise specified when tumors cannot be further classified.3,6 Among HPV-independent tumors, gastric-type adenocarcinoma (GAC) is particularly aggressive and is frequently characterized by advanced-stage presentation, high recurrence risk, and reduced sensitivity to standard platinum-based chemotherapy.3,6,7 These features underscore the urgent need for biomarker-driven therapeutic strategies in clinically high-risk cervical cancer subtypes.
Human epidermal growth factor receptor 2 is a well-established oncogenic driver and therapeutic target in several malignancies. HER2 overexpression, gene amplification, and activating mutations have been successfully targeted in breast and gastric cancers, where HER2-targeted agents have substantially improved treatment outcomes.8–11 This therapeutic success provides an important biological and clinical foundation for evaluating HER2 as a potential actionable target in cervical cancer. However, HER2 alterations in cervical cancer are less common and more dependent on histological subtype than in classical HER2-driven tumors. HER2 amplification is relatively rare in SCC and in unselected cervical cancer populations, whereas HER2 overexpression, amplification, or mutation appears to be enriched in selected adenocarcinoma subtypes, including GAC and other HPV-independent variants.7,12–14 This subtype-specific enrichment may provide a unique window of opportunity for biomarker-guided precision treatment.
Recent clinical evidence has further strengthened the relevance of HER2 in cervical cancer. In particular, the DESTINY-PanTumor02 trial demonstrated encouraging antitumor activity of trastuzumab deruxtecan, a HER2-targeted antibody-drug conjugate, across HER2-expressing solid tumors, including cervical cancer.15 The observed activity of trastuzumab deruxtecan has expanded the therapeutic potential of HER2 beyond traditional HER2-driven cancers and has renewed interest in HER2 testing and patient selection in cervical cancer.2,16 Together with emerging data on HER2 mutations and pan-HER tyrosine kinase inhibitors (TKIs), these findings suggest that HER2 should be considered not merely as a prognostic marker but as a clinically actionable biomarker in selected patients with recurrent, metastatic, or treatment-resistant cervical cancer.13,17,18
Despite this progress, several important issues remain unresolved, including the true prevalence of HER2 alterations across histological subtypes, their prognostic versus predictive significance, the optimal testing strategy for HER2 positivity, and the appropriate integration of HER2-targeted therapies into clinical practice.19,20 Therefore, this review aims to synthesize current evidence regarding the structure, function, expression patterns, clinical significance, targeted therapeutic strategies, and evolving interpretation criteria of HER2 in cervical cancer, with particular emphasis on its role in biomarker-guided precision treatment.
Structure and Function of HER2
The HER2 gene, located on human chromosome 17q21, is a proto-oncogene belonging to the epidermal growth factor receptor (EGFR) family. The HER2 protein is a 185 kDa transmembrane receptor tyrosine kinase (RTK) composed of 1255 amino acids. Its structure comprises three domains: an extracellular ligand-binding domain, a single-pass transmembrane domain, and an intracellular protein tyrosine kinase domain. The kinase domain spans approximately amino acid residues 720–987.
The HER2 protein possesses intrinsic tyrosine kinase activity. As no ligand that binds directly to HER2 has been identified, it primarily functions by forming heterodimers with other EGFR family members—namely EGFR (HER1), HER3, and HER4. Upon heterodimerization and binding to their respective ligands, HER2 activates downstream signaling pathways, such as the Ras/Raf/mitogen-activated protein kinase (MAPK) and phosphatidylinositol 3-kinase (PI3K)/Akt pathways, thereby promoting cell proliferation and tumorigenesis.21 HER2 is the preferred dimerization partner within the family, and heterodimers containing HER2 exhibit stronger signaling activity than those without it.9
Expression of HER2 in Cervical Cancer
In 1987, Slamon et al first identified an association between HER2 and the pathogenesis of breast cancer,10 an observation that subsequently laid the foundation for decades of translational and clinical investigation. Since that time, HER2 gene amplification has been firmly established as a key oncogenic driver in several malignancies, most notably breast, gastric, and colorectal cancers. Within gynecological oncology, approximately one-third of uterine serous carcinomas (USC) demonstrate HER2 protein overexpression and/or gene amplification.22 By contrast, data regarding HER2 expression in other gynecological malignancies, including CC, remain comparatively limited and heterogeneous.
In CC, reported HER2 positivity rates vary widely across studies. A meta-analysis documented a range from 0% to 87%.12 The reported incidence of HER2 overexpression in CC differs markedly according to the assessment criteria used: studies adhering to American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) standards report an overall rate of 5.7%, compared with 27.0% in non-adherent studies (P < 0.001). Other reports describe HER2 overexpression rates in CC ranging from 1% to 21%,23 and HER2 expression appears to be increased in recurrent CC. Similarly, the reported incidence of HER2 gene amplification is 1.2% in studies following ASCO/CAP guidelines versus 24.9% in those that do not (P = 0.004).24 These marked discrepancies indicate that the reported prevalence of HER2 alterations in CC should be interpreted cautiously and cannot be attributed to biological variation alone.
Several methodological factors may contribute to this variability. First, study populations differ substantially in histological composition. Cohorts enriched for cervical adenocarcinoma, GAC, or other HPV-independent variants are more likely to report higher HER2 alteration rates than cohorts dominated by SCC.7,12,20 Second, HER2 immunohistochemistry (IHC) scoring systems have not been applied consistently across studies. Earlier studies often used non-standardized criteria, different thresholds for IHC positivity, or variable definitions of incomplete, basolateral, lateral, and circumferential membranous staining.11 This issue is particularly relevant in cervical glandular lesions, in which HER2 staining patterns may resemble gastroesophageal adenocarcinoma more closely than breast cancer.7,11 Third, technical differences, including antibody clone, staining platform, antigen retrieval, fixation quality, and laboratory workflow, may influence staining intensity and reproducibility.12,22 Fourth, pathological interpretation remains an important source of variation, especially when weak or heterogeneous staining, cytoplasmic staining, or equivocal IHC 2+ cases are interpreted differently.12 Finally, some studies relied on IHC alone, whereas others incorporated confirmatory fluorescence in situ hybridization (FISH) or next-generation sequencing (NGS), making direct comparison across cohorts difficult.7,11 These limitations suggest that the wide range of reported HER2 positivity in CC reflects both biological heterogeneity and methodological inconsistency. Future studies should therefore use harmonized IHC scoring criteria, clearly report antibody clones and testing platforms, apply reflex FISH or validated molecular testing for equivocal cases, and analyze HER2 prevalence separately according to histological subtype.
HER2 mutations have also been documented in CC, with reported mutation rates ranging from 4% to 6%.13 In a cohort of 1,015 patients with operable CC, non-synonymous HER2 mutations were identified in 3.15% of cases, with S310F representing the most frequent mutation site.25 Notably, no concurrent HER2 mutation with HER2 overexpression or amplification was detected in that study, suggesting that these alterations may define distinct molecular subsets. Although certain analyses have not identified statistically significant differences in HER2 overexpression between squamous and non-squamous cancers (NSC), multiple studies have demonstrated that HER2 amplification and point mutations vary significantly according to histological subtype.5,13,14,25 Specifically, amplification and mutation of HER2 occur more frequently in NSC than in SCC. This distinction carries clinical implications, as patients with NSC generally exhibit less favorable post-treatment prognosis.19 In cervical adenocarcinoma, alterations involving erb-b2 receptor tyrosine kinase 2 (ERBB2) and erb-b2 receptor tyrosine kinase 3 (ERBB3) often co-occur. A pronounced tendency toward simultaneous ERBB2 and ERBB3 alterations has been reported, implying that aberrant HER3-mediated signaling may arise through interaction between mutated HER3 and activated HER2.26 Enrichment of ERBB2 amplification and oncogenic missense mutations has been observed at rates of 28% in usual-type endocervical adenocarcinoma (UEA), 14% in GAC, and 9% in SCC.14 These data support the notion that cervical adenocarcinoma, particularly specific histological variants, harbors a comparatively higher burden of biologically relevant HER2 alterations, thereby warranting focused evaluation.
A study including 209 cases of cervical adenocarcinoma classified according to International Endocervical Adenocarcinoma Criteria and Classification further investigated HER2 expression and amplification.7 HER2 protein expression was identified in 57.4% of adenocarcinomas, whereas HER2 amplification was confirmed in 6.2%. Amplification appeared more frequent in GAC (14.7%) and unspecified mucinous adenocarcinoma (10%), although precise estimates remain subject to methodological limitations. These findings suggest that anti-HER2-targeted therapy may be particularly applicable to selected patients with cervical adenocarcinoma, especially those with GAC, and that refined pathological subtyping may enhance therapeutic stratification. Most studies have not demonstrated consistent associations between HER2 alterations (overexpression, amplification, or mutation) and conventional clinicopathological parameters. Patients infected with Human Papillomavirus-18 (HPV-18) tend to exhibit higher rates of ERBB2 mutations than those infected with Human Papillomavirus-16 (HPV-16), although this difference has not reached statistical significance.13
In routine clinical practice, immunohistochemistry (IHC) is employed to evaluate HER2 protein expression, FISH to assess gene amplification, and NGS to detect gene amplification and point mutations. Given that gene expression is a regulated biological process, HER2 gene amplification or point mutations do not invariably translate into HER2 protein overexpression. For specimens with borderline or equivocal findings, repeat testing or confirmatory analysis using complementary methodologies is advisable to ensure accurate classification.
Taken together, the most recent evidence indicates that, under harmonized ASCO/CAP scoring criteria and integrated IHC/FISH assessment, the proportion of CC exhibiting true HER2 amplification or high-level protein overexpression remains relatively low, typically within the single-digit range. Nevertheless, HER2 alterations are disproportionately enriched in cervical adenocarcinomas—particularly GAC and other HPV-independent variants—and are also observed in a small subset of biologically aggressive, advanced-stage SCC. Tumors within this HER2-enriched subgroup frequently present with more advanced International Federation of Gynecology and Obstetrics Staging (FIGO stage), higher rates of nodal metastasis, and increased risk of recurrence, thereby defining a population most likely to benefit from HER2-directed ADCs. Accordingly, precise characterization of HER2 expression and ERBB2 gene amplification status has become an essential component of contemporary pathological assessment and individualized treatment planning in CC.8
Clinical Significance of HER2 Positive Expression in Cervical Cancer
The prognostic implications of ERBB2 alterations in CC remain incompletely defined and, in many instances, statistically inconclusive. One study reported that patients harboring ERBB2 mutations exhibited a two-year disease-free survival (DFS) rate of 78.1% and a five-year DFS rate of 71.4%; however, survival analysis did not demonstrate a significant association between ERBB2 mutation status and DFS.13 In a separate cohort, ERBB2 mutations appeared more frequently in metastatic tumors, yet the observed differences failed to reach statistical significance. Moreover, when sequencing results were compared between patients with stage I–IVA disease and those with stage IVB disease, the carcinogenic mutation rate of ERBB2 was found to be consistent across stages, suggesting that mutation occurrence alone does not account for disease progression.
Although earlier genomic analyses did not consistently establish ERBB2 mutations as independent prognostic determinants in unselected cervical cancer populations, their predictive value for targeted therapy has become increasingly evident. In the final analysis of the Phase II SUMMIT basket study, treatment with neratinib achieved an objective response rate (ORR) of approximately 18% and a clinical benefit rate (CBR) approaching 45% in patients with HER2-mutant recurrent or metastatic cervical cancer. Median progression-free survival (PFS) was 5.1 months, and median duration of response (DoR) was 7.6 months, with all responses observed in endocervical adenocarcinomas. On the basis of these findings, the 2024 revision of the National Comprehensive Cancer Network (NCCN) guidelines incorporated neratinib as a category 2A option for HER2-mutated recurrent or metastatic cervical cancer, thereby underscoring the clinical importance of routine ERBB2 mutation testing in advanced disease.18 Despite these individual study findings, HER2 alterations in CC have not been consistently statistically linked to prognosis. In comparison, the poorer prognosis of cervical adenocarcinoma and metastatic/recurrent CC with more significant HER2 alterations suggests that HER2 still plays a role in the development of CC. Some studies indicate that patients with invasive cervical cancer (ICC) harboring ERBB2 mutations have a worse prognosis compared to those with wild-type ERBB2 or Phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA) mutations, but a better prognosis compared with those carrying Kirsten rat sarcoma viral oncogene homolog (KRAS) mutations.13 The study noted that among patients carrying ERBB2 mutations, 12.5% also carried KRAS mutations, and 6.25% carried PIK3CA mutations. Among patients with ERBB2 amplification, 58% had concurrent PIK3CA mutations. A high incidence of PI3K pathway genomic alterations was observed in ERBB2-amplified patients, regardless of tumor site.25 Notably, Friedman et al pointed out that ERBB2 and KRAS alterations are mutually exclusive in histological subtypes of CC,14 suggesting that the co-alteration status of HER2 with other genes may influence patient prognosis.
This interplay appears particularly relevant in cervical adenocarcinoma. Ueda et al demonstrated that 46% of adenocarcinomas (including both HPV-related and HPV-independent tumors) were positive for both HER2 (IHC 2+ or 3+ using a 10% cutoff) and EGFR.20 Co-expression was significantly associated with lymph node metastasis, advanced tumor stage, and shorter recurrence-free survival, suggesting that concurrent activation of HER2 and EGFR signaling confers a more aggressive biological phenotype. Additional evidence indicates that, in cervical adenocarcinoma, HER2 amplification is more frequently observed in tumors with advanced FIGO stage (III/IV), GAC subtype, perineural invasion (PNI), and ovarian spread, whereas HER2 overexpression correlates with lymphovascular invasion (LVI) and ovarian involvement. Both LVI and PNI occur at higher rates in GAC than in non-GAC tumors.7 More recent data further refine the prognostic landscape. A 2025 retrospective study involving 179 cases reported that approximately 44% of tumors exhibited some degree of HER2 immunoreactivity (IHC 1+–3+), whereas only about 5% met criteria for true HER2 positivity when IHC findings were integrated with FISH confirmation. Elevated HER2 expression correlated strongly with adverse pathological features, including higher FIGO stage, lymph node metastasis, LVI, PNI, and increased serum cancer antigen 125 (CA125) levels. Moreover, HER2 expression independently predicted reduced PFS, with the HER2-positive subset demonstrating the most pronounced survival disadvantage.19 Although survival analysis revealed only a modest downward trend in overall survival (OS) among patients with HER2 amplification—and this did not achieve statistical significance—amplification was significantly associated with recognized high-risk features, including advanced FIGO stage, PNI, and ovarian involvement. Given the established efficacy of HER2-targeted therapy in gastric cancer,6 the enrichment of ERBB2 alterations in GAC and the identification of GAC as a strong independent predictor of disease-specific survival and tumor recurrence underscore the importance of clarifying HER2 status in gastric-type cervical adenocarcinoma. In this context, HER2 assessment may carry both biological and therapeutic implications.
In summary, current evidence does not support HER2 alterations as robust or independent prognostic biomarkers across unselected cervical cancer populations. Although HER2 abnormalities frequently coincide with aggressive clinicopathological characteristics—particularly in cervical adenocarcinoma and GAC—their direct impact on survival outcomes remains heterogeneous and context-dependent. These observations suggest that the clinical significance of HER2 in CC resides less in conventional prognostic stratification and more in its function as a predictive biomarker guiding targeted therapeutic decision-making. Consequently, research efforts have increasingly focused on defining the therapeutic utility of HER2-directed strategies in recurrent or metastatic disease, a topic addressed in the subsequent section.
Targeted Therapy for HER2 Positive Expression
Consistent with its evolving role as a predictive rather than purely prognostic biomarker, HER2 has emerged as a clinically actionable target in selected subsets of cervical cancer.12,13,15,18 However, HER2-targeted therapy in cervical cancer should not be interpreted as a single therapeutic category. Based on current evidence, HER2-directed therapeutics can be broadly grouped into trastuzumab-based monoclonal antibody therapy, HER2-targeted ADCs, and pan-HER TKIs.2,8 This classification is clinically important because different therapeutic classes correspond to different HER2 alteration patterns, including protein overexpression, gene amplification, and activating ERBB2/HER2 mutations.13,14,18,23
The therapeutic success of HER2-directed agents in other malignancies provides the conceptual and translational foundation for their application in cervical cancer. In tumors characterized by HER2 amplification or overexpression, most prominently breast and gastric cancers, HER2-targeted strategies have demonstrated durable clinical benefit.2,10,11 This paradigm has prompted investigation into whether analogous molecular subsets of cervical cancer may derive similar therapeutic advantage.7,13 A meta-analysis evaluating HER2-targeted therapy in HER2-altered cancers reported clinically meaningful antitumor activity, suggesting that although the overall response rate remains modest in unselected populations, a clinically meaningful subgroup may benefit from targeted intervention.8,24
Trastuzumab-based therapy provides proof of concept that HER2 blockade may be clinically beneficial in selected HER2-positive cervical cancer, particularly when combined with platinum-based chemotherapy.2,8 The available cervical cancer-specific evidence remains limited, but it supports the feasibility of translating HER2 blockade into biomarker-selected cervical cancer populations.12,13 Because trastuzumab primarily targets HER2 protein overexpression and gene amplification, its clinical value depends heavily on accurate HER2 assessment by IHC, FISH, or molecular testing.7,11 Therefore, trastuzumab-based regimens should currently be viewed as biologically rational and potentially useful in selected patients, rather than as broadly applicable therapy for all cervical cancer populations.8
Pan-HER TKIs represent a distinct therapeutic approach, particularly for tumors driven by activating ERBB2/HER2 mutations rather than HER2 protein overexpression or gene amplification.23 The SUMMIT trial (NCT01953926), a multi-cohort basket study, demonstrated antitumor activity of neratinib in patients with HER2-mutant recurrent or metastatic cervical cancer.17,18 These findings support ERBB2/HER2 mutation as a potentially actionable alteration in cervical cancer, although responses appear to be confined to molecularly selected subgroups.13,18 Larger cervical cancer-specific studies are still needed to define the optimal role, sequencing, and combination strategies of pan-HER inhibitors.
Among recent therapeutic advances, HER2-targeted ADCs have generated the greatest clinical interest. Trastuzumab deruxtecan (T-DXd) combines HER2-targeted antibody recognition with delivery of a topoisomerase I (TOP1) inhibitor payload and has demonstrated clinically meaningful activity across HER2-expressing solid tumors, including cervical cancer.8,16 In the DESTINY-PanTumor02 trial, T-DXd showed encouraging activity in the cervical cancer cohort, with an ORR of 50.0%.15 Subgroup analysis showed that patients with HER2 IHC 3+ tumors derived the greatest benefit, with an ORR of 75.0%. Patients who had received no more than one prior line of therapy had an ORR of 66.7%, suggesting that earlier integration of HER2-targeted therapy may improve therapeutic yield. Patients previously treated with TOP1 inhibitors also showed a numerically higher ORR than those without prior exposure, while programmed death-ligand 1 (PD-L1)-negative tumors showed a numerically higher response rate than PD-L1-positive tumors. Although these subgroup findings should be interpreted cautiously, they suggest that HER2 expression level, prior treatment exposure, and tumor immune context may influence response to ADC-based therapy.15
Subsequent gynecologic subgroup analyses further clarified this therapeutic gradient. Patients with HER2 IHC 3+ cervical cancer derived the most substantial clinical benefit from T-DXd therapy, whereas those categorized as HER2-low, defined as IHC 1+ or IHC 2+ with negative FISH, also demonstrated measurable but comparatively attenuated antitumor activity.15,27 These findings suggest that HER2 expression in cervical cancer may exist along a biologically continuous therapeutic spectrum rather than a simple positive or negative classification, with response probability correlating with expression intensity.12,15 The emergence of HER2-targeted ADCs has therefore strengthened the rationale for HER2 testing and biomarker-driven patient selection in recurrent, metastatic, or treatment-resistant cervical cancer.
Reflecting the accumulating clinical evidence, the NCCN cervical cancer guidelines have incorporated T-DXd as a treatment option in the second-line setting and beyond for appropriately selected patients.28 This incorporation underscores the growing clinical relevance of HER2-directed therapy, but routine implementation in cervical cancer remains evolving and depends on accurate HER2 assessment, molecular stratification, and further prospective validation.12,18 The ongoing or recently completed clinical trials evaluating HER2-targeted agents with relevance to cervical carcinoma are summarized in Table 1.
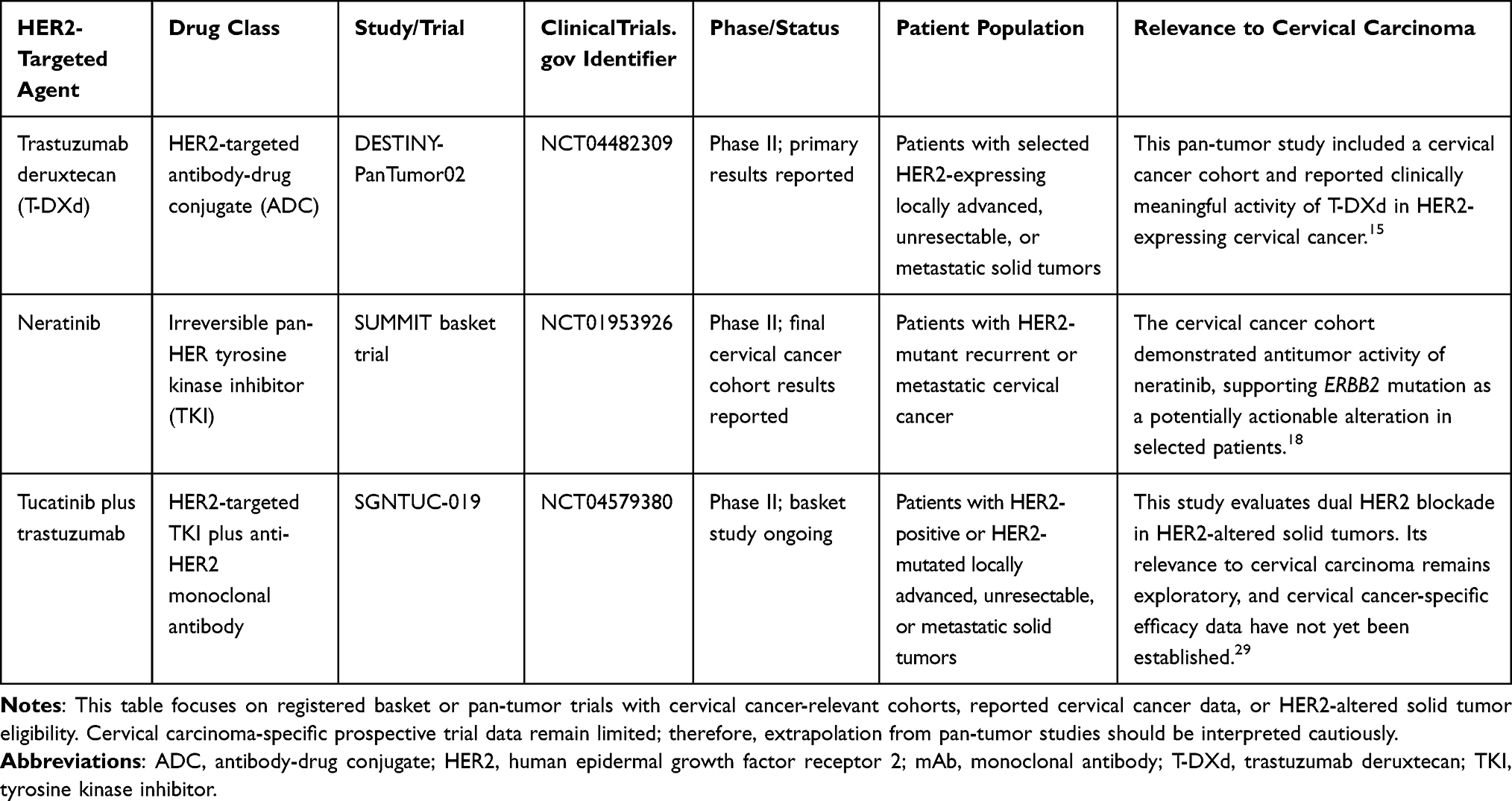 |
Table 1 Registered Basket or Pan-Tumor Trials of HER2-Targeted Agents with Relevance to Cervical Carcinoma |
In summary, HER2-targeted therapy should be regarded as an evolving biomarker-driven strategy for molecularly defined subsets of cervical cancer rather than as a broadly applicable treatment for unselected patients.18 Trastuzumab-based therapy supports the feasibility of HER2 blockade in selected HER2-positive tumors, T-DXd and other HER2-targeted ADCs represent a promising therapeutic strategy for HER2-expressing cervical cancer, and pan-HER inhibitors are most relevant to ERBB2/HER2-mutant recurrent or metastatic disease. Future clinical trials should prioritize refined molecular stratification, particularly in cervical adenocarcinoma and gastric-type variants, and explore earlier-line integration and rational combination strategies.13 Accurate identification of patients most likely to benefit remains essential to maximizing clinical efficacy while avoiding unnecessary treatment exposure.
HER2 Positive Criteria
Accurate determination of HER2 expression status is fundamental to appropriate patient selection for HER2-targeted therapy. In CC, however, standardized and disease-specific criteria for HER2 assessment have not yet been formally established. Historically, in the absence of dedicated guidelines for CC, investigators have relied on the detailed frameworks developed by the ASCO and CAP for breast and gastric cancers. These guidelines, which define HER2 protein expression and gene amplification thresholds, have undergone periodic revision—most notably in breast cancer—to improve diagnostic consistency and clinical applicability.11 Given this lack of CC-specific standards, the HER2 positive criteria adopted across studies have varied substantially. Consequently, many clinical investigations have referenced the established ASCO/CAP criteria for breast or gastroesophageal cancers. For example, the DESTINY-PanTumor02 trial, which enrolled patients with gynecological malignancies, applied the gastric cancer HER2 testing criteria.15 This approach is supported by pathological observations indicating that the HER2 staining pattern in cervical adenocarcinoma more closely resembles that of gastric or gastroesophageal adenocarcinoma than that observed in breast cancer. Accordingly, the application of ASCO/CAP guidelines formulated for gastroesophageal adenocarcinoma to cervical cancer has been proposed as a more biologically congruent strategy.7 Under this framework, an IHC score of 3+ is considered sufficient to classify a tumor as HER2 positive. IHC 0 and IHC 1+ are defined as HER2 negative. An IHC score of 2+ is regarded as equivocal and necessitates reflex testing by FISH to determine HER2 gene amplification status. If FISH confirms gene amplification, the tumor is categorized as HER2 positive; if amplification is absent, the tumor is classified as HER2 negative. Representative HER2 immunohistochemical staining patterns corresponding to the current four scoring categories in cervical cancer are shown in Figure 1.
 |
Figure 1 HER2 immunohistochemistry showing the current 4 immunohistochemical categories in cervical cancer. (A) HER2 immunohistochemical staining showing a score of 0 (400×). (B) HER2 immunohistochemical staining showing a score of 1+ (400×). (C) HER2 immunohistochemical staining showing a score of 2+ (400×). (D) HER2 immunohistochemical staining showing a score of 3+ (400×). All images are original and provided by the authors. |
Because therapies such as trastuzumab are primarily directed against tumors with HER2 gene amplification, a dual-modality testing strategy—comprising initial IHC assessment followed by reflex FISH in IHC 2+ cases—is particularly important in cervical adenocarcinoma.
To date, no consensus guidelines specific to cervical cancer or gynecological tract malignancies have been issued to standardize HER2 testing in this setting.12 As a result, HER2 interpretation in CC is still largely extrapolated from established breast cancer and gastroesophageal adenocarcinoma criteria.11 Although application of the ASCO/CAP criteria for gastroesophageal adenocarcinoma to CC has demonstrated favorable inter-observer reproducibility and high concordance between IHC and FISH results, this approach remains imperfect because HER2 staining patterns, histological context, tumor heterogeneity, and therapeutic implications may differ across tumor types.
Several unresolved issues therefore merit attention. First, testing algorithms should be optimized according to histological subtype, particularly for cervical adenocarcinoma and GAC.7 Second, clearer criteria are needed for IHC 2+ equivocal cases, reflex FISH testing, and the interpretation of HER2-low disease in the context of emerging ADC-based therapy. Third, technical procedures, scoring thresholds, and quality control should be further harmonized across pathology laboratories to improve diagnostic reproducibility.15 Given these unresolved issues and the variability in HER2 assessment across studies, the commonly used HER2 scoring systems and their main characteristics are summarized in Table 2.
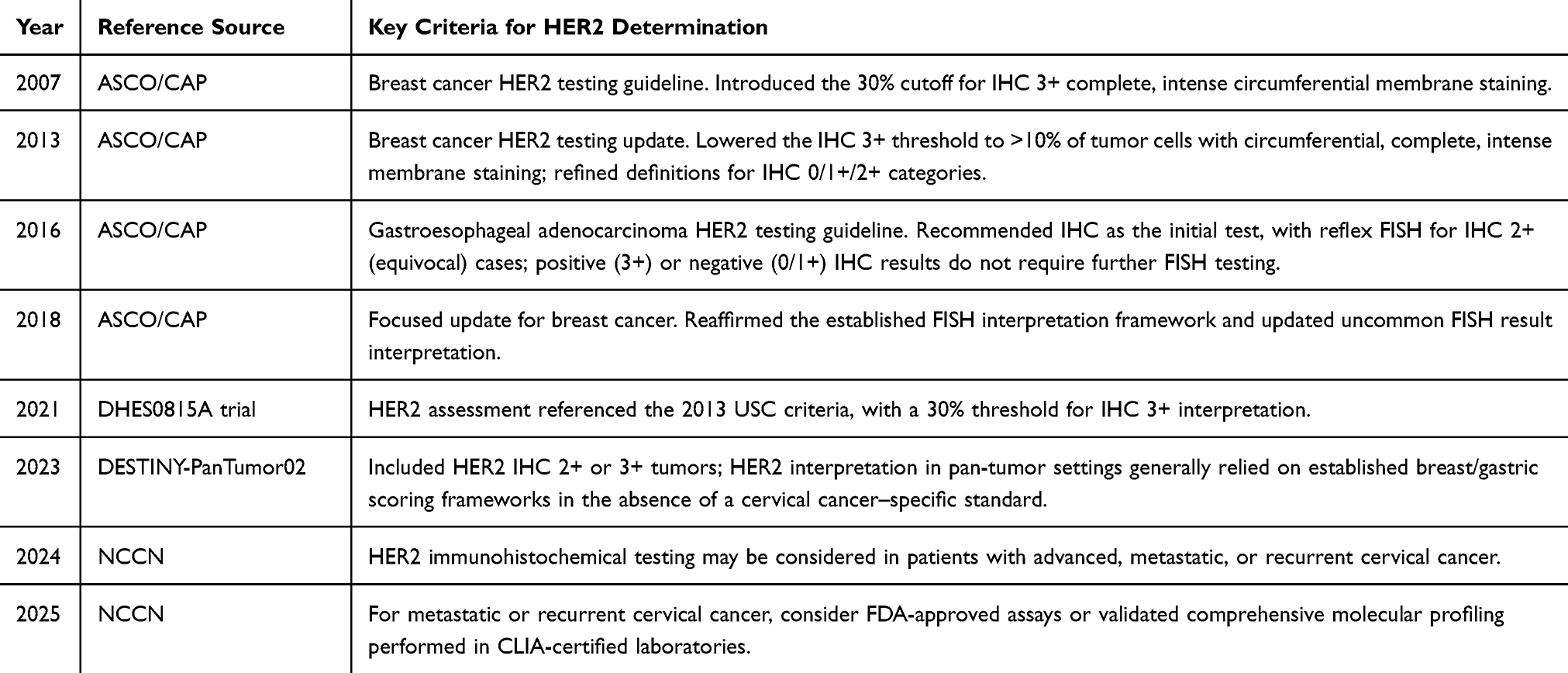 |
Table 2 Comparison of Key Updates in HER2 IHC Scoring Systems |
Establishing a harmonized and evidence-based HER2 testing framework for cervical cancer and other gynecological tract malignancies is therefore essential.7,22 Such standardization would support accurate patient triage, improve consistency across clinical trials, facilitate biomarker-driven patient selection, and ultimately maximize the therapeutic benefit derived from HER2-targeted strategies in CC.
Limitations and Unresolved Challenges
Several limitations and unresolved challenges should be acknowledged. First, most available evidence regarding HER2 in cervical cancer is derived from retrospective cohorts, small subgroup analyses, or basket trials, and prospective cervical cancer-specific data remain limited.15,18 Therefore, the therapeutic relevance of HER2 should be interpreted cautiously and within biomarker-selected populations. Second, reported HER2 positivity rates vary substantially across studies because of differences in histological composition, IHC scoring criteria, antibody clones, staining platforms, pathological interpretation, and the inconsistent use of confirmatory FISH or molecular testing.12 This methodological heterogeneity limits direct comparison across studies and underscores the need for standardized HER2 assessment criteria specific to cervical cancer and other gynecological tract malignancies. Third, the optimal predictive biomarkers for HER2-targeted therapy remain incompletely defined. Although HER2 overexpression, amplification, and activating ERBB2 mutations are clinically relevant, validated biomarkers beyond HER2 status itself are lacking.13,23 The clinical significance of HER2-low disease, co-alterations in pathways such as PI3K or MAPK, and immune or tumor microenvironment (TME) features requires further investigation.15 Finally, acquired resistance to HER2-targeted therapy remains an anticipated challenge. Future studies should clarify resistance mechanisms, define rational sequencing strategies, and evaluate combination approaches, including HER2-targeted agents with immune checkpoint inhibitors or other targeted therapies.8
Conclusion
Taken together, the clinical importance of HER2 in cervical cancer lies less in its value as a universal prognostic marker and more in its potential to guide precision treatment in highly selected molecular and histological subsets. Current evidence does not support the broad application of HER2-targeted therapy to unselected cervical cancer populations. Instead, meaningful clinical benefit appears to be concentrated in patients with defined HER2 alterations, including HER2 overexpression, HER2 amplification, or activating ERBB2/HER2 mutations. Although HER2 alterations are relatively uncommon in unselected cervical cancer populations, they are enriched in certain adenocarcinoma subtypes, especially GAC and other HPV-independent variants. These subgroups are frequently associated with aggressive clinical behavior, limited sensitivity to standard platinum-based chemotherapy, and poor outcomes after recurrence or metastasis. Therefore, HER2 assessment should be considered not as a routine marker for all patients in the same manner, but as part of a biomarker-driven strategy for identifying patients most likely to benefit from targeted therapy.
A major barrier to clinical progress is the lack of standardized HER2 testing criteria specific to cervical cancer and other gynecological tract malignancies. Current practice still relies largely on scoring systems developed for breast cancer or gastroesophageal adenocarcinoma. Although these frameworks provide useful references, they may not fully account for the unique morphology, staining patterns, and biological behavior of cervical glandular lesions. Future guidelines should establish gynecological tract-specific IHC and FISH scoring criteria, clarify the interpretation of equivocal and HER2-low cases, and define appropriate reflex testing algorithms. Such standardization is essential for improving diagnostic reproducibility, clinical trial comparability, and biomarker-driven patient selection.
Among emerging therapeutic strategies, next-generation HER2-targeted antibody-drug conjugates, particularly trastuzumab deruxtecan, currently represent one of the most promising directions for HER2-positive cervical cancer. Compared with conventional HER2 blockade, ADCs combine target recognition with cytotoxic payload delivery and may partly overcome intratumoral heterogeneity through the bystander effect. This feature is particularly relevant in solid tumors such as cervical cancer, where HER2 expression may be heterogeneous and conventional binary definitions of HER2 positivity may fail to capture the full therapeutic spectrum. Future trials should therefore refine HER2 expression thresholds, evaluate the clinical relevance of HER2-low disease, and determine the optimal timing of ADC integration in recurrent, metastatic, or treatment-resistant cervical cancer.
Future research should also prioritize HPV-independent cervical cancer variants, particularly GAC. These tumors are not directly prevented by HPV vaccination strategies and often show aggressive biology and limited responsiveness to standard treatment. For this population, HER2-targeted strategies may become an important therapeutic avenue if reliable biomarkers and testing algorithms can be established. However, validated predictive biomarkers beyond HER2 status itself remain insufficiently established. It remains unclear which patients with HER2-low disease are most likely to benefit from ADC-based therapy, which molecular co-alterations influence response or resistance, and whether immune or TME features can predict benefit from combinations of HER2-targeted agents with PD-1 or PD-L1 inhibitors. Clarifying these predictive factors will be essential for refining patient selection, avoiding unnecessary treatment exposure, and improving the durability of clinical benefit.
In parallel, the interaction between HER2 signaling and the TME deserves further investigation. Rational combinations of HER2-targeted agents with immune checkpoint inhibitors may help improve response durability in selected patients, but require prospective validation. Finally, identifying the molecular mechanisms of acquired resistance to HER2-targeted therapy will be essential for developing sequential treatment strategies and rational combination regimens.
In conclusion, HER2 is emerging as a clinically actionable biomarker in selected subsets of cervical cancer rather than a broadly applicable prognostic marker or universal therapeutic target. The next stage of progress will depend on standardized HER2 testing, rigorous molecular stratification, focused investigation of HPV-independent adenocarcinoma subtypes, rational integration of next-generation ADCs, and mechanistic studies of resistance and combination therapy. Through these efforts, HER2-directed strategies may become an increasingly important component of precision treatment for appropriately selected patients with cervical cancer.
Abbreviations
ADCs, antibody-drug conjugates; ASCO/CAP, American Society of Clinical Oncology/College of American Pathologists; CA125, cancer antigen 125; CBR, clinical benefit rate; CC, cervical cancer; CLIA, Clinical Laboratory Improvement Amendments; DFS, disease-free survival; DoR, duration of response; EGFR, epidermal growth factor receptor; ERBB2, erb-b2 receptor tyrosine kinase 2; ERBB3, erb-b2 receptor tyrosine kinase 3; FDA, Food and Drug Administration; FIGO, International Federation of Gynecology and Obstetrics; FISH, fluorescence in situ hybridization; GLOBOCAN, Global Cancer Observatory; HER2, human epidermal growth factor receptor 2; HER3-DXd, patritumab deruxtecan; HPV, human papillomavirus; HPV-18, human papillomavirus type-18; ICC, invasive cervical cancer; IECC, International Endocervical Adenocarcinoma Criteria and Classification; IHC, immunohistochemistry; KRAS, Kirsten rat sarcoma viral oncogene homolog; LVI, lymphovascular invasion; MAPK, mitogen-activated protein kinase; NCCN, National Comprehensive Cancer Network; NGS, next-generation sequencing; NSC, non-squamous cancer; ORR, objective response rate; OS, overall survival; PD-L1, programmed death-ligand 1; PFS, progression-free survival; PI3K, phosphatidylinositol 3-kinase; PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha; PNI, perineural invasion; RTK, receptor tyrosine kinase; SCC, squamous cell carcinoma; T-DXd, trastuzumab deruxtecan; TOP1, topoisomerase I; UEA, usual-type endocervical adenocarcinoma; USC, uterine serous carcinoma; WHO, World Health Organization.
Acknowledgments
The authors would like to thank all individuals who provided support and assistance during the preparation of this manuscript.
Funding
This work was supported by the New Round of Xuzhou “Pengcheng Talent Program”–High-level Healthcare Talent Recruitment and Development Project (Project Number: 2-2025TD08).
Disclosure
Xinru Yang reports Support for the manuscript from Xuzhou Municipal Health Commission, during the conduct of the study, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–11. doi:10.3322/caac.21834
2. Oh DY, Bang YJ. HER2-targeted therapies: a role beyond breast cancer. Nat Rev Clin Oncol. 2020;17(1):33–48. doi:10.1038/s41571-019-0268-3
3. Stolnicu S, Barsan I, Hoang L, et al. International endocervical adenocarcinoma criteria and classification (IECC): a new pathogenetic classification for invasive adenocarcinomas of the endocervix. Am J Surg Pathol. 2018;42(2):214–226. doi:10.1097/PAS.0000000000000986
4. Höhn AK, Brambs CE, Hiller GGR, May D, Schmoeckel E, Horn LC. WHO classification of female genital tumors. Geburtshilfe Frauenheilkd. 2021;81(10):1145–1153. doi:10.1055/a-1545-4279
5. Li J, Xue X, Zhang Y, et al. The differences in immune features and genomic profiling between squamous cell carcinoma and adenocarcinoma: a multi-center study in Chinese patients with uterine cervical cancer. Gynecol Oncol. 2023;175:133–141. doi:10.1016/j.ygyno.2023.05.071
6. Stolnicu S, Barsan I, Hoang L, et al. Diagnostic algorithmic proposal based on comprehensive immunohistochemical evaluation of 297 invasive endocervical adenocarcinomas. Am J Surg Pathol. 2018;42(8):989–1000. doi:10.1097/PAS.0000000000001090
7. Shi H, Shao Y, Lu W, Lu B. An analysis of HER2 amplification in cervical adenocarcinoma: correlation with clinical outcomes and the international endocervical adenocarcinoma criteria and classification. J Pathol Clin Res. 2021;7(1):86–95. doi:10.1002/cjp2.184
8. Zhu K, Yang X, Tai H, Zhong X, Luo T, Zheng H. HER2-targeted therapies in cancer: a systematic review. Biomarker Res. 2024;12(1):16–32. doi:10.1186/s40364-024-00565-1
9. Moasser MM. The oncogene HER2: its signaling and transforming functions and its role in human cancer pathogenesis. Oncogene. 2007;26(45):6469–6487. doi:10.1038/sj.onc.1210477
10. Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235(4785):177–182. doi:10.1126/science.3798106
11. Bartley AN, Washington MK, Ventura CB, et al. HER2 testing and clinical decision making in gastroesophageal adenocarcinoma: guideline from the college of American pathologists, American society for clinical pathology, and American society of clinical oncology. Am J Clin Pathol. 2016;146(6):647–669. doi:10.1093/ajcp/aqw206
12. Itkin B, Garcia A, Straminsky S, et al. Prevalence of HER2 overexpression and amplification in cervical cancer: a systematic review and meta-analysis. PLoS One. 2021;16(9):e0257976. doi:10.1371/journal.pone.0257976
13. Xiang L, Jiang W, Ye S, et al. ERBB2 mutation: a promising target in non-squamous cervical cancer. Gynecol Oncol. 2018;148(2):311–316. doi:10.1016/j.ygyno.2017.12.023
14. Friedman CF, Ravichandran V, Miller K, et al. Assessing the genomic landscape of cervical cancers: clinical opportunities and therapeutic targets. Clin Cancer Res. 2023;29(22):4660–4668. doi:10.1158/1078-0432.CCR-23-1078
15. Meric-Bernstam F, Makker V, Oaknin A, et al. Efficacy and safety of trastuzumab deruxtecan in patients with HER2-expressing solid tumors: primary results from the DESTINY-PanTumor02 phase II trial. J Clin Oncol. 2024;42(1):47–58. doi:10.1200/JCO.23.02005
16. Perez J, Garrigós L, Gion M, et al. Trastuzumab deruxtecan in HER2-positive metastatic breast cancer and beyond. Expert Opin Biol Ther. 2021;21(7):811–824. doi:10.1080/14712598.2021.1890710
17. Oaknin A, Friedman CF, Roman LD, et al. Neratinib in patients with HER2-mutant, metastatic cervical cancer: findings from the Phase 2 SUMMIT basket trial. Gynecol Oncol. 2020;159(1):150–156. doi:10.1016/j.ygyno.2020.07.025
18. Friedman CF, D’Souza A, Bello Roufai D, et al. Targeting HER2-mutant metastatic cervical cancer with neratinib: final results from the phase 2 SUMMIT basket trial. Gynecol Oncol. 2024;181:162–169. doi:10.1016/j.ygyno.2023.12.004
19. Xu Q, Yin Z, Li Y, Zhu X, Lou H, Ni J. Prognostic value of HER2 expression in cervical adenocarcinoma: a retrospective cohort study. Oncol Lett. 2025;29(5):1–11. doi:10.3892/ol.2024.14747
20. Ueda A, Takasawa A, Akimoto T, et al. Prognostic significance of the co-expression of EGFR and HER2 in adenocarcinoma of the uterine cervix. PLoS One. 2017;12(8):e0184123. doi:10.1371/journal.pone.0184123
21. Ligorio F, Zambelli L, Fucà G, et al. Prognostic impact of body mass index (BMI) in HER2+ breast cancer treated with anti-HER2 therapies: from preclinical rationale to clinical implications. Ther Adv Med Oncol. 2022;14:17588359221079123. doi:10.1177/17588359221079123
22. Buza N, English DP, Santin AD, Hui P. Toward standard HER2 testing of endometrial serous carcinoma: 4-year experience at a large academic center and recommendations for clinical practice. Mod Pathol. 2013;26(12):1605–1612. doi:10.1038/modpathol.2013.113
23. Yan M, Parker BA, Schwab R, Kurzrock R. HER2 aberrations in cancer: implications for therapy. Cancer Treat Rev. 2014;40(6):770–780. doi:10.1016/j.ctrv.2014.02.008
24. Zheng Y, Shen G, Zhang C, et al. Efficacy of anti-HER2 drugs in the treatment of patients with HER2-mutated cancers: a systematic review and meta-analysis. Clin Exp Med. 2023;23(7):3205–3216. doi:10.1007/s10238-023-01072-7
25. Nasioudis D, Gysler S, Latif N, et al. Molecular landscape of ERBB2/HER2 gene amplification among patients with gynecologic malignancies; clinical implications and future directions. Gynecol Oncol. 2024;180:1–5. doi:10.1016/j.ygyno.2023.11.021
26. The Cancer Genome Atlas Research Network. Integrated genomic and molecular characterization of cervical cancer. Nature. 2017;543(7645):378–384. doi:10.1038/nature21386
27. Pistilli B, Mosele F, Corcos N, et al. Patritumab deruxtecan in HR+HER2− advanced breast cancer: a phase 2 trial. Nat Med. 2025;31(10):3492–3503. doi:10.1038/s41591-025-03885-3
28. Abu-Rustum NR, Yashar CM, Arend R, et al. NCCN Guidelines® insights: cervical cancer, version 1.2024: featured updates to the NCCN Guidelines. J Natl Compr Canc Netw. 2023;21(12):1224–1233. doi:10.6004/jnccn.2023.0062
29. Monk B, Jin F, Ramos J, Tan Q, O’Malley D. A phase 2 basket study of tucatinib and trastuzumab in solid tumors with human epidermal growth factor receptor 2 alterations: uterine and cervical cancer cohorts (SGNTUC-019, trial in progress) (1261). Gynecol Oncol. 2023;176:S165–S166. doi:10.1016/j.ygyno.2023.06.170
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exploration of Traditional Chinese Medicine Comprehensive Treatment of Triple Negative Breast Cancer Based on Molecular Pathological Mechanism
Zhu M, Liu Y, Wen Z, Tan H, Li S, Yu X, Luo H, Li D, Wang J, Qin F
Breast Cancer: Targets and Therapy 2025, 17:289-304
Published Date: 10 April 2025