Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Research on the Association Between Periodontitis and COPD
Authors Xiong K, Yang P, Cui Y, Li J, Li Y, Tang B
Received 9 June 2023
Accepted for publication 28 August 2023
Published 1 September 2023 Volume 2023:18 Pages 1937—1948
DOI https://doi.org/10.2147/COPD.S425172
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Kaixin Xiong,1,* Peng Yang,2,* Yujia Cui,1 Jia Li,1 Yan Li,1 Boyu Tang1,3
1State Key Laboratory of Oral Diseases & National Center for Stomatology & National Clinical Center for Oral Diseases, West China Hospital of Stomatology, Sichuan University, Chengdu, People’s Republic of China; 2Department of Cardiovascular Surgery, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 3State Key Laboratory of Oral Diseases & National Center for Stomatology & National Clinical Center for Oral Diseases & Department of Conservation Dentistry and Endodontics, West China Hospital of Stomatology, Sichuan University, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Li, State Key Laboratory of Oral Diseases & National Center for Stomatology & National Clinical Center for Oral Diseases, West China Hospital of Stomatology, Sichuan University, Chengdu, People’s Republic of China, Email [email protected] Boyu Tang, Key Laboratory of Oral Diseases & National Center for Stomatology & National Clinical Center for Oral Diseases & Department of Conservation Dentistry and Endodontics, West China Hospital of Stomatology, Sichuan University, Chengdu, People’s Republic of China, Email [email protected]
Abstract: Periodontitis is a common chronic bacteria-initiated inflammatory disease that is closely associated with various systemic diseases, including chronic obstructive pulmonary disease (COPD). Periodontitis and COPD share similar risk factors, pathology and microorganisms. Epidemiological and clinical research have shown positive correlation between the two diseases. Individuals with severe periodontitis had a higher risk of developing COPD. Moreover, the relative risk of COPD in severe periodontitis was much higher compared to people without periodontal disease and patients with mild to moderate periodontitis. COPD patients with periodontitis had a higher frequency of COPD exacerbation and periodontal treatment demonstrated some control of COPD. However, the nature of periodontitis affecting COPD still needs further exploration. Periodontitis caused microbial and immune imbalances of the lung through several aspects: (I) under periodontitis status, periodontal pathogens directly caused the lung inflammatory reaction after inhalation and colonization on the lung, (II) periodontitis status promoted the oral colonization of pneumonia-associated pathogens, (III) periodontitis status affected the respiratory epithelium structure and (IV) periodontitis status caused imbalances in neutrophils, macrophages and inflammatory cytokines. In this review, we conclude the association between periodontitis and COPD through several aspects and further discuss the potential mechanism by which periodontitis affects COPD.
Plain Language Summary: Epidemiological and clinical research have shown positive correlation between periodontitis and COPD. Individuals with severe periodontitis had a higher risk of developing COPD. COPD patients with periodontitis had a higher frequency of COPD exacerbation. Meanwhile, periodontal treatment demonstrated some control of COPD. In this review, we concluded the association between periodontitis and further summarized that periodontitis caused microbial and immune imbalances of the lung through several aspects: (I) under periodontitis status, periodontal pathogens directly caused the lung inflammatory reaction after inhalation and colonization on the lung, (II) periodontitis status promoted the oral colonization of pneumonia-associated pathogens, (III) periodontitis status affected the respiratory epithelium structure and (IV) periodontitis status caused imbalances in neutrophils, macrophages and inflammatory cytokines.
Keywords: COPD, microorganism, immune, inflammation
Introduction
Periodontitis, also known as the destructive gum disease, is one of the six most prevalent non-communicable diseases worldwide.1,2 Periodontitis is a chronic inflammation of the periodontal supporting tissue caused mainly by polymicrobial infection.3 Microorganisms adhere to the tooth surface and cause aggressive immune response, eventually leading to tooth loosening and loss.3 The prevention of periodontitis is mainly achieved through daily self-performed oral hygiene, however, the incidence of periodontitis remains high and continues to increase, and is considered as the most common cause of tooth loss.4 In China, more than 90% of adults suffer from periodontal disease.2 Periodontitis not only causes tooth loss, but also adversely affects a variety of systemic diseases, such as cardiovascular disease, diabetes, rheumatoid arthritis, osteoporosis, chronic obstructive pulmonary disease (COPD), etc.
COPD is a chronic systemic inflammatory pulmonary disease characterized by incomplete and progressive airflow restriction, which is related to the abnormal inflammatory response of the lungs to harmful gases or particles.5,6 With repeated attacks and acute exacerbations of the disease, pulmonary function in COPD patients gradually decreases and shortness of breath occurs during daily activities and even at rest. COPD is a major cause of morbidity and disability, with a prevalence of around 10% in people over the age of 40.7 It is considered as the third leading cause of death globally,8 with approximately 90% of COPD related deaths occurring in Asia and Africa.8
Periodontitis has been shown to be closely associated with systemic diseases, including COPD. Periodontitis and COPD are common chronic diseases and both of the two diseases can significantly affect the quality of life. Both conditions have been linked to a range of risk factors, including smoking, microbial infection, environmental pollution, diabetes, poor socioeconomic status and poor dental habits. In recent years, there has been growing interest in the potential relationship between these two conditions, with research suggesting that they may be closely linked. However, the studies on the correlation between periodontitis and COPD are mainly limited to the condition that clinical cohort studies and meta-analysis have confirmed the positive correlation between them. While, the mechanisms of how periodontitis affects the progression of COPD remain unclear and require further study.
In this review, we conclude the association between periodontitis and COPD through epidemiological, clinical, pathological and microbial analysis, and further discuss the potential mechanisms by which periodontitis affects COPD.
Association Between Periodontitis and COPD
Periodontitis is a type of microbial infectious disease, closely related to systemic diseases. Recently, periodontitis was found to have a close relationship with respiratory system diseases, among which the association between periodontitis and COPD has become an area of intense interest. Here, we review the association between periodontitis and COPD through various aspects (Figure 1).
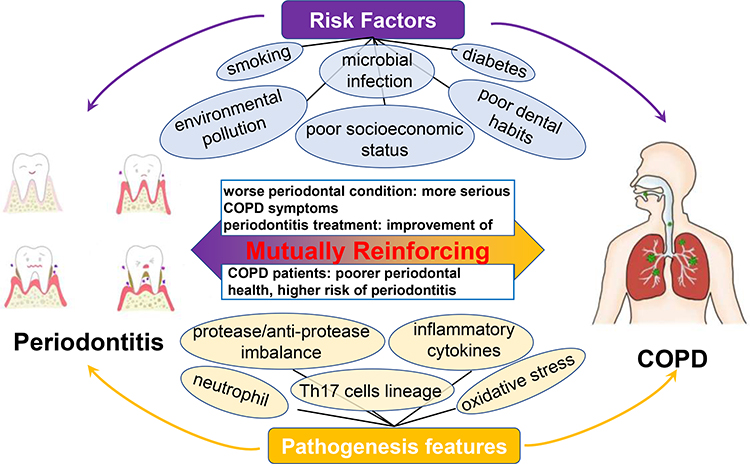 |
Figure 1 The association between periodontitis and COPD. Periodontitis and COPD share some associations through various aspects, including epidemiological and clinical phenotypes, risk factors and pathogenesis features. |
Epidemiological Association Between Periodontitis and COPD
In the 1990s, it was first hypothesized that there might be a correlation between periodontitis and COPD (the pulmonary emphysema sub-type).9 In the following years, increasing amounts of epidemiological data confirmed the correlation between the two chronic diseases. Scannapieco et al10 analyzed the first National Health and Nutrition Examination Survey (NHANES I) results in 1998 and indicated a correlation between periodontitis and chronic respiratory diseases. Three years later, Scannapieco et al11 conducted a follow-up study based on NHANES III and found that the periodontal attachment loss of patients with a history of COPD was significantly higher than that of patients without a history of COPD, with patients presenting a mean attachment loss ≥ 3.0 mm having a higher risk of COPD. Through the two studies, Scannapieco et al concluded that there’re some associations between periodontitis and COPD and further speculated that periodontitis might promote COPD progression.
In recent years, additional epidemiological investigations have confirmed these opinions. It was pointed that the worse periodontal condition, the more serious the COPD symptoms, and among all the periodontal indicators, plaque index was found to have the most significant correlation with COPD.12 Zhou et al and Javaheri et al confirmed that gingival index (GI), probing pocket depth (PD), bleeding on probing (BOP), and clinical attachment loss (CAL) are negatively correlated with forced expiratory volume in the first second/forced vital capacity (FEV1/FVC) and forced expiratory volume in the first second (FEV1), which indicated that poor periodontal health was associated with obstructive lung disease.13,14 Analysis of the data from NHANES III with machine learning and deep learning algorithms suggested that periodontitis could act as a crucial predictor of COPD.15 Similarly, it was found that patients with COPD had significantly poorer periodontal health, greater gingival inflammation, and deeper pockets or CALs compared to non-COPD controls.14,16 In a recent cohort study, Verma et al17 compared the periodontal status between 100 hospitalized non-tubercular respiratory ill patients (majority of the patients were diagnosed as lung cancer and COPD) containing group and 100 periodontal patients containing group and found that hospitalized patients with non-tubercular respiratory diseases had more severe pocket probing depth, plaque index and CAL, suggesting that there existed some associations between periodontitis and respiratory diseases (mainly lung cancer and COPD).
Moreover, some prospective studies and longitudinal studies also confirmed the positive correlation. Shen et al performed a large-scale population-based longitudinal cohort study, in which 22,332 patients with COPD, and two randomly selected matching individuals without COPD for each case, were included for evaluating the risk of periodontal diseases.18 11 years of observation indicated that the overall incidence of periodontal diseases was 1.19-fold greater in the COPD group.18 Takeuchi et al19 observed 900 community residents without COPD for 5 years and indicated that the relative risk of COPD in severe periodontitis group was much higher compared with the periodontally healthy group and the mild to moderate periodontitis group.
Clinical Association Between Periodontitis and COPD
Numerous epidemiological studies have confirmed the association between periodontitis and COPD, prompting researchers to investigate whether periodontal therapy can improve symptoms in patients with COPD. Interestingly, there exists evidence to suggest that treating periodontitis may improve lung function in people with COPD. Through reviewing the published literature of the last four decades, Gupta et al20 concluded that periodontal attachment loss had an impact on the risk of COPD occurrence and that periodontal treatment could reduce COPD exacerbations. Kucukcoskun et al21 equally divided 40 COPD patients with periodontitis into two groups, a control group without intervention and a treatment group with periodontal treatment. At the 1-year follow-up, the median frequency of acute episodes of COPD decreased from an average of 3 to 2 per person per year in the periodontal treatment group and increased from 2 to 3 in the control group. Similarly, Zhou et al22 divided 60 COPD patients with periodontitis into 3 groups, and treated with periodontal scaling and root planning (SRP), supragingival scaling, or oral hygiene instructions only with no periodontal treatment, respectively. Compared with the control group (without periodontal treatment), FEV1/FVC and FEV1 values in the treatment groups were significantly improved. The frequencies of COPD exacerbation were significantly decreased in the two treatment groups, while they increased in the control group, suggesting that periodontal treatment can control the acute exacerbations of COPD patients. Similarly, Sharma et al23 suggested that non-surgical periodontal therapy led to the improvement of lung function. These studies further indirectly confirmed that periodontitis promoted the aggravation of pulmonary symptoms in COPD patients to some extent.
Overall, the clinical association between periodontitis and COPD highlights the importance of maintaining good oral health to reduce the risk of developing respiratory diseases. Individuals with periodontitis or COPD should receive regular dental and medical check-ups and follow a comprehensive treatment plan to manage both conditions.
Shared Pathophysiological Process Between Periodontitis and COPD
It has been suggested that periodontitis and COPD are linked through a complex pathophysiological process. These two conditions share some pathological features, including T helper 17 (Th17) cells lineage, neutrophil, protease/anti-protease imbalance, oxidative stress and inflammatory cytokines.
Th17 and its associated inducing and secreting cytokines play important roles in both periodontitis and COPD pathological process.24 Th17 cells secrete proinflammatory cytokine Interleukin-17 (IL-17) to promote chronic inflammation, which act as the one of the main pathological features in both COPD and periodontitis. IL-17 promotes periodontal inflammation by stimulating primary gingival epithelial cells and periodontal ligament (PDL) cells to highly express proinflammatory cytokines, including Chemokine (C-X-C motif) ligand 1 (CXCL1), Chemokine (C-X-C motif) ligand 5 (CXCL5), Interleukin-1β (IL-1β), Interleukin-6 (IL-6), Interleukin-10 (IL-10), Interleukin-12 (IL-12), Tumor necrosis factor-alpha (TNF-α), stromelysin, Prostaglandin E2 (PGE2), etc.25 Similarly, IL-17 induces airway epithelial cells to secrete CXCL1, CXCL5, Chemokine (C-X-C motif) ligand 8 (CXCL8), Granulocyto-colony-Stimulating-Factor (G-CSF), and Granulocyte-macrophage colony stimulating factor (GM–CSF) to promote lung tissue inflammation and damage, aggravating the severity of COPD.26 In addition, by promoting the expression of Th17 cell differentiation-inducing cytokines, mainly including IL-1β, IL-6, IL-23, and Transforming growth factor-β (TGF-β), environmental stimulants like Porphyromonas gingivalis (P. gingivalis) or cigarette smoke could promote the production of Th17 and eventually cause periodontitis and COPD.27,28 In short, periodontitis and COPD share a similar Th17 lineage pathological process. In this process, IL-6, IL-1β, IL-23, and TGF-β induce Th17 differentiation and recruitment, followed by IL-17 secretion, which further promotes both periodontitis and COPD.
Both periodontitis and COPD share the characteristics of neutrophilic inflammation and neutrophil-mediated tissue damage. It’s shown that chemotaxis and extracellular proteolysis were significantly enhanced in neutrophils from COPD subjects, which indicated a stronger destructive potential.29,30 Moreover, it was observed that neutrophils of COPD moved with greater speed and formed fewer pseudopods during migration.29 Similarly, neutrophils also acted as the predominant inflammatory cells in gingivitis and neutrophil infiltration was also a characteristic of periodontitis.31 Abnormal neutrophil function was associated with increased prevalence of periodontitis.32 Hajishengallis et al found that neutrophils from patients with chronic periodontitis showed reduced speed, velocity, and accuracy,32 and that this abnormal behavior could be improved after periodontitis treatment.33 Therefore, neutrophils are a shared crucial pathology of both COPD and periodontitis.
The protease / anti-protease imbalance hypothesis has been widely accepted as the key pathological process mediating tissue destruction in COPD patients. Neutrophil elastase and α1-antitrypsin (AAT) are a common protease / anti-protease pairing. AAT deficiency is closely related with chronic respiratory diseases.34 Meanwhile, elastase was also found to induce emphysema.35 Bronchoalveolar lavage fluid detection from patients with COPD indicated a relationship between the elastase / anti-elastase imbalance and the extent of emphysema, in which elastase burden and anti-elastase capacity correlated directly and inversely with emphysema, respectively.36 Matrix metalloproteinases (MMPs) were also shown to induce the pathological destructive process of COPD, however these enzymes are controlled by specific tissue metalloproteinases inhibitors in healthy state.37 This imbalance hypothesis is relatively less well studied in periodontitis. However, it was found that the concentration of neutrophil elastase was significantly higher in the crevicular fluid of chronic gingivitis.38 A series of studies since then have also indicated that the AAT and neutrophil elastase imbalance is also associated with periodontitis.38–40 MMPs were also shown to be correlated with periodontal destruction, as in COPD.41
Oxidative stress acts as another shared feature of COPD and periodontitis, and is believed to be the important pathological process in COPD and periodontitis. Many oxidative stress associated signals including hydrogen peroxide level, oxidant-induced DNA damage marker, lipid peroxidation products, and superoxide dismutase 3 gene polymorphism, were significantly increased in patients with COPD, suggesting the crucial role of oxidant stress in this condition.42 Interestingly, some similar results were also observed in periodontitis. Stimulation with the periodontitis associated pathogen Fusobacterium nucleatum (F. nucleatum) led to a significant increase of intracellular reactive oxygen species (ROS) production in human gingival fibroblasts.43 This suggested that oxidative stress was also a key pathology in periodontitis.
Pro-inflammatory cytokines are a factor that directly promote inflammatory diseases, including COPD and periodontitis. Many pro-inflammatory cytokines are activated in periodontitis, and there exists a similar increase of some cytokines, including TNF-α, IL-6, C-reactive protein (CRP), IL-1β, etc. in COPD patients’ blood samples or lung secretions,44,45 indicating that, to some degree, periodontitis and COPD share a common inflammatory process.
Overall, the pathophysiological procedure between periodontitis and COPD is complex. Chronic inflammation and immune dysregulation play a key role in the development and progression of both conditions, and interventions targeting these mechanisms may have therapeutic potential for both periodontitis and COPD.
Shared Risk Factors Between Periodontitis and COPD
Both periodontitis and COPD are multi-risk factor chronic diseases. Interestingly, studies have suggested that periodontitis and COPD shared several common risk factors, including smoking, microbial infection, environmental pollution, diabetes, poor socioeconomic status and poor dental habits.
Smoking is a well-established risk factor for both periodontitis and COPD. Smoking damages the tissues of the oral cavity and respiratory tract, leading to chronic inflammation and increased risk of infection. Smoking is considered as the major risk factor for COPD. The prevalence of COPD in current smokers is twice of that in former smokers, and about 5.5 times of that in non-smokers.46 Smoking also acts as an important risk factor of periodontitis. The risk of periodontal diseases was significantly higher in smokers compared to that in nonsmokers.47 Tobacco smoke can cause inflammation and damage to the lungs, as well as the periodontal tissues in the mouth, leading to an increased risk of COPD and periodontal disease.
Microbial infection is another shared risk factor. Periodontitis is a bacterial infectious disease, and dental plaque biofilm is the main cause of its occurrence. Similarly, microbial infection is also a risk factor for COPD and bacterial infection is the most common cause of COPD exacerbation.48 Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis are the bacteria which are most frequently associated with acute exacerbations of COPD.49 Moreover, COPD can be further affected by oral microbial infections. Bacteria in the mouth can travel to the lungs and cause respiratory infections, potentially worsening COPD symptoms. In addition, chronic inflammation in the gums caused by periodontitis can lead to an increase in systemic inflammation, which can contribute to the development and progression of COPD.
Exposure to environmental pollutants such as particulate matter and air pollution can increase the risk of both periodontitis and COPD.50,51 Several air pollutants, including particulate matter of 10 μm (PM10), ozone and sulfur dioxide (SO2), were found to be associated with the occurrence of periodontitis, which suggested that air pollution might be a new modifiable risk indicator for periodontitis.50 Similarly, higher concentrations of PM2.5, PM10 and NO2 were significantly associated with the prevalence of COPD, resulting in lower lung function, and lower FEV1 and FVC.51 These pollutants can cause chronic inflammation and damage to respiratory and oral tissues.52,53
Diabetes is a risk factor for both periodontitis and COPD.54,55 High blood sugar levels can weaken the immune system and increase susceptibility to infections. Periodontitis and diabetes are linked by an established bidirectional relationship. In diabetes patients, the risk for periodontitis is two to three times higher than that in individuals without diabetes.56 Diabetes may increase periodontal inflammation through elevated inflammatory cytokines in the gingival crevicular fluid and exacerbate bone resorption through activation of osteoclasts via the Receptor activator of nuclear factor kappa-Β ligand (RANK-L) pathway.55 Similarly, it’s concluded that the diabetic state, including poor glycemic control and duration and level of severity, was associated with worsening of lung function, including decreased FVC and FEV1, and that after correction of hyperglycemia, these abnormalities could be mitigated.57
Poor socioeconomic status is also a shared common risk factor of COPD and periodontitis.58 COPD patients were less well educated and had lower income,59,60 meanwhile, it has been demonstrated that periodontal disease prevalence increased as educational level and monthly income decreased.60 Moreover, through Modified Kuppuswamy’s socioeconomic scale assessment, Verma et al17 demonstrated that low‑income individuals were at greater risk of periodontal infections than high‑income individuals. The findings of Lenk et al also indicated that patients with higher periodontitis indices were less well educated.61
In addition, poor dental habitat is another crucial shared risk factor of the two diseases. It is well known that poor dental habitat is closely related to periodontitis, however, relationship between poor dental habitat and COPD has not been frequently reported. Previous published reports suggested that COPD patients had significantly reduced brushing frequency, oral health knowledge scores, and were less likely to use dental floss and have regular dental visits.16,62
Overall, these studies indicate that COPD and periodontitis had some associations on the aspect of shared common risk factors. These shared risk factors suggest that individuals with periodontitis or COPD should take steps to reduce their risk of both diseases, including quitting smoking, maintaining a healthy diet, avoiding exposure to environmental pollutants, managing any underlying medical conditions such as diabetes, and maintaining good oral hygiene.
The Potential Mechanisms by Which Periodontitis Affects COPD
The pathophysiological connection between periodontitis and COPD involves changes in the microbial community, which leads to chronic inflammation and immune dysregulation in both the oral cavity and lungs. In addition, periodontitis also results in the release of pro-inflammatory cytokines and bacterial toxins into the bloodstream. These inflammatory mediators can subsequently reach the lungs, where they contribute to the development and progression of COPD (Figure 2).
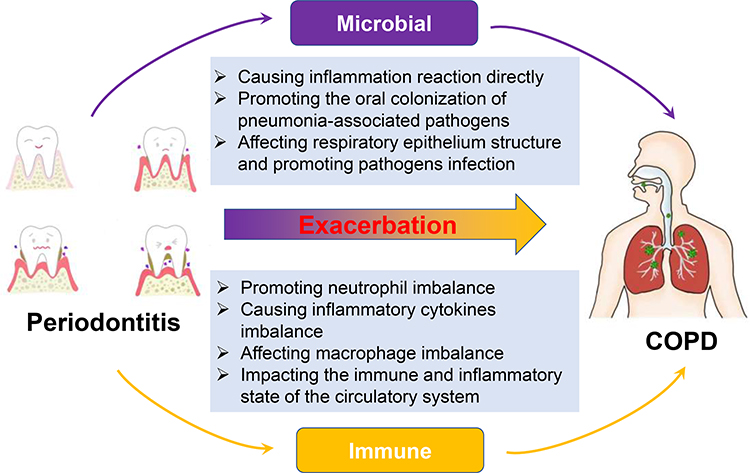 |
Figure 2 The potential mechanisms by which periodontitis affected COPD. Periodontitis promotes COPD progression mainly through causing imbalances in the microbial community and immune system. |
Periodontitis Promotes COPD Progression Through Microbial Interactions
Several microbial-infection associated mechanisms between periodontitis and respiratory diseases have been posited previously,63,64 including directly causing inflammation reaction, promoting the oral colonization of pneumonia-associated pathogens and affecting respiratory epithelium structure.
Oral Pathogens Could Be Aspirated into the Lung and Subsequently Cause Lung Inflammation
Numerous studies have confirmed that there exists microbial communication between periodontitis and COPD. Periodontal bacteria Aggregatibacter actinomycetemcomitans, Capnocytophaga sputigena, Porphyromonas gingivalis, Tannerella forsythia and Treponema denticola were detected in the tracheal aspirate of severe acute exacerbation COPD patients, suggesting that dental bacteria may contribute to the pathology of severe acute exacerbation of COPD.65 Moreover, it was reported that P. gingivalis, Treponema odontocera and Forsytanella detected in subgingival plaque and respiratory secretions of patients with acute exacerbation of COPD were homologous,66 suggesting that aspiration of periodontal pathogens into the lung promoted exacerbation of COPD symptoms. Tian et al67 indicated that the periodontal pathogen P. gingivalis could transfer to the lung tissue and subsequently promoted lung inflammation and decreased lung function. Moreover, elevated levels of inflammatory factors in lung tissue such as TNF-α, IL-17 and G-CSF were also detected, which further confirmed that periodontal pathogens could stimulate the secretion of inflammatory factors to induce lung injury after entering the lung. Parashar et al68 and Budden et al69 revealed that P. gingivalis induced lung injury by activating toll-like receptor-2 (TLR-2) and its downstream nuclear factor kappa-B (NF-κB) signaling pathway.
Periodontitis Promotes the Oral Colonization of Respiratory Pathogens, Which Then Travel to the Lung via Aspiration
The oral cavity is the closest reservoir for respiratory pathogens.70 Some respiratory pathogens can be inhaled through the mouth and upper respiratory tract before colonizing the lungs. During periodontitis, periodontal pathogens can enhance the oral colonization of respiratory pathogens, promoting the aspiration of more pathogens.70 In severe acute exacerbation COPD patients, lung pathogens such as Acinetobacter baumannii, Klebsiella pneumoniae, Pseudomonas aeruginosa and S. pneumoniae were detected in subgingival plaque biofilm.65 Tan et al71 found that P. gingivalis and several respiratory pathogens, including Klebsiella pneumoniae, Pseudomonas aeruginosa and Streptococcus pneumoniae in the subgingival plaque of COPD patients were higher than those of the non-COPD group and there was a significant negative correlation between P. gingivalis and FEV1/FVC in COPD patients.
Periodontitis-Associated Pathogens Could Damage Respiratory Epithelium and Promote Respiratory Pathogen Infection
Over production of mucin can lead to the further decrease of respiratory function in COPD patients.72 The periodontal pathogen P. gingivalis can significantly elevate the expression of a core mucin protein, Mucin 5AC (MUC5AC), in bronchial epithelial cells.73 Similarly, intratracheal administration of the periodontal pathogen F. nucleatum significantly elevated the number of Goblet cell metaplasia (associated with mucin hypersecretion) and expression of MUC5AC.74 Moreover, it has been suggested that F. nucleatum also exacerbates COPD through increased expression of MMP12 to promote alveolar wall destruction.74
Pneumonia-causing bacterial infection mediated by platelet-activating factor receptor (PAFR) is a crucial trigger for COPD exacerbation.72 The periodontal pathogen P. gingivalis promoted the expression of PAFR by alveolar epithelial cells, which led to increased adherence of pneumonia-causing pathogen S. pneumoniae.75
In short, aspiration of periodontal pathogens may damage the epithelium and simultaneously promote infection by pneumonia-causing pathogens, which would further promote COPD progression.
Periodontitis Promotes COPD Progression by Affecting the Immune Process
Immune imbalance plays an essential role in COPD progression. Periodontitis could affect the immune homeostasis in several ways, including causing neutrophil imbalance, inflammatory cytokines imbalance, macrophage imbalance and impacting the immune and inflammatory state of the circulatory system.
Periodontitis Affects COPD Progression Through Causing Imbalance of Neutrophil Number and Function
As discussed above, neutrophil-mediated inflammation is a shared pathogenic characteristic of both periodontitis and COPD. More importantly, previously studies demonstrated that periodontitis might affect lung inflammation by causing an imbalance of neutrophil number and function. It was shown that ligature together with P. gingivalis-induced periodontitis had the ability to induce pulmonary inflammation through the elevation of cytokines and neutrophils in lung tissue and blood.67 Moreover, in COPD patients, regardless of patient’s alpha-1 antitrypsin deficiency (AATD) status, with increasing severity of periodontitis, the migratory speed and accuracy of neutrophils declined.76 Therefore, an imbalance in neutrophil number and function plays an essential role in how periodontitis affects COPD.
Periodontitis Affects the Expression of Inflammatory Cytokines in Lung Tissue
Pro-inflammatory cytokines are the factors that directly promote inflammatory diseases, including COPD and periodontitis. Additionally, periodontitis could further promote the expression of inflammatory cytokines in lung tissue, which might act as one of the mechanisms by which periodontitis exacerbates COPD. Supernatants of the periodontal pathogen P. gingivalis elevated the expression of inflammatory cytokines, including TNF-α, Macrophage inflammatory protein 2 (MIP-2), IL-1β and IL-17, in the lung tissue of S. pneumoniae-infected mice, which further promoted the pneumonia inflammation.77 Extracellular vesicles of P. gingivalis-infected macrophages could induce the expression of TNF-α and IL-6 in lung epithelium cells, further inducing lung injury and inflammation.78 Moreover, it has been reported that F. nucleatum can trigger COPD by increasing the expression levels of IL-8 and IL-6 in several human respiratory epithelium cells and mouse lung tissue.79 In the F. nucleatum-exacerbated COPD mouse model, expressions of inflammatory cytokines were also significantly elevated in lung tissue, including expression of IL-6, CXCL-1, CXCL-5, Monocyte chemoattractant protein-2 (CCL-2), and CXCL-10.74 In short, periodontitis might exacerbate COPD by elevating the inflammatory cytokines in lung tissue.
Periodontitis Affects Macrophage Polarization in Lung Tissue
The functions of macrophages play important roles in the occurrence and progression of COPD. Macrophages are the most abundant immune cells in lung tissue and perform both pro-inflammatory and anti-inflammatory roles,80 and could exhibit various polarized phenotypes in order to respond and adapt to microenvironmental change. Macrophage polarization associated immune responses play important roles in COPD development. Macrophage polarization phenomenon and co-expression of M1 and M2 polarization are significantly elevated in COPD lung tissue.81
Periodontal pathogens can stimulate macrophage polarization, towards both M1 and M2.82 Moreover, periodontitis could affect systemic diseases by influencing the microphage polarization to some degree. Xu et al83 performed an in vivo study with obese rats and found that periodontitis promoted diabetic development by activating classical polarization of macrophages. Lyu et al also indicated that human β-defensin 3 could be therapeutic towards periodontitis associated systemic inflammation by modulating macrophage polarization.84 However, there are few published reports on the aspect of macrophage polarization between periodontitis and COPD. Several studies have shown that periodontitis could promote the expression of M1-related (such as the previously mentioned IL-1β, TNF-α, CXCL-1, CXCL-5 and CXCL-10) or M2-related (CCL-2, IL-17 and MMP-12) inflammatory factors in COPD lung tissue, therefore, we hypothesize that, like other systemic diseases, periodontitis may also influence COPD progression by affecting the polarization of local macrophages. However, the specific impacts require further study.
Periodontitis Affects COPD Progression by Influencing the Immune and Inflammatory State of the Circulatory System
In addition to local inflammation, periodontitis also results in the elevation of pro-inflammatory cytokines and bacterial toxins in the bloodstream. These inflammatory mediators in the circulatory system can also contribute to the progression of COPD.
Wang et al demonstrated that periodontitis could decrease lung function and exacerbate COPD via elevation of the inflammatory cytokines TNF-α, IL-1 and RANKL in serum, and that periodontitis treatment could decrease the level of inflammatory cytokines in serum, relieving their exacerbation on COPD.85 In the periodontal pathogen F. nucleatum-triggering COPD mouse model, the levels of KC (an IL-8 homologous neutrophil chemoattractant) and IL-6 were significantly increased.79 In the patients of periodontitis with acute exacerbation of COPD, the levels of IL-8 and IL-6 in the serum were evidently increased compared to those in periodontitis, acute exacerbation of COPD and healthy control groups.86 According to these results, it can be concluded that periodontitis could promote COPD progression by affecting the immune and inflammatory state of the circulatory system to some degree.
Conclusion
Periodontitis is closely associated with COPD. Both periodontitis and COPD share similar risk factors, microbial communication and pathology, as well as epidemiological and clinical features. Periodontitis could affect COPD progression through various aspects, including directly causing lung inflammatory reaction by periodontal pathogens, promoting oral colonization of pneumonia-associated pathogens, affecting the respiratory epithelium structure and causing imbalances in neutrophils, macrophages and inflammatory cytokines. Addressing oral health and inflammation are very important in reducing the risk of developing COPD and improving outcomes for those already afflicted by the disease. By recognizing the intricate relationship between periodontitis and COPD and implementing appropriate oral care measures, we can potentially alleviate the burden of COPD and enhance the overall quality of life for affected individuals. Therefore, reinforcing daily oral hygiene management and the control of periodontitis should be regarded as a crucial aspect of COPD management.
Acknowledgments
Kaixin Xiong and Peng Yang are co-first authors for this study. This work was supported by Key Projects of Sichuan Provincial Department of Science and Technology (2020YFSY0008), Research and Develop Program, West China Hospital of Stomatology Sichuan University (RD-02-202112), Natural Science Foundation of Sichuan Province (2022NSFSC1507, 2023NSFSC1503).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Chikte U, Pontes CC, Karangwa I, et al. Periodontal disease status among adults from South Africa—prevalence and effect of smoking. Int J Environ Res Public Health. 2019;16(19). doi:10.3390/ijerph16193662
2. Luo LS, Luan HH, Wu L, et al. Secular trends in severe periodontitis incidence, prevalence and disability-adjusted life years in five Asian countries: a comparative study from 1990 to 2017. J Clin Periodontol. 2021;48(5):627–637. doi:10.1111/jcpe.13447
3. Kinane DF, Stathopoulou PG, Papapanou PN. Periodontal diseases. Nat Rev Dis Primers. 2017;3:17038. doi:10.1038/nrdp.2017.38
4. Eke PI, Borgnakke WS, Genco RJ. Recent epidemiologic trends in periodontitis in the USA. Periodontol 2000. 2020;82(1):257–267. doi:10.1111/prd.12323
5. Soriano JB, Polverino F, Cosio BG. What is early COPD and why is it important? Eur Respir J. 2018;52(6). doi:10.1183/13993003.01448-2018
6. Yang W, Li F, Li C, Meng J, Wang Y. Focus on early COPD: definition and early lung development. Int J Chron Obstruct Pulmon Dis. 2021;16:3217–3228. doi:10.2147/copd.S338359
7. Scannapieco FA, Cantos A. Oral inflammation and infection, and chronic medical diseases: implications for the elderly. Periodontol 2000. 2016;72(1):153–175. doi:10.1111/prd.12129
8. Anees UR, Ahmad Hassali MA, Muhammad SA, et al. The economic burden of chronic obstructive pulmonary disease (COPD) in the USA, Europe, and Asia: results from a systematic review of the literature. Expert Rev Pharmacoecon Outcomes Res. 2020;20(6):661–672. doi:10.1080/14737167.2020.1678385
9. Travis J, Pike R, Imamura T, Potempa J. The role of proteolytic enzymes in the development of pulmonary emphysema and periodontal disease. Am J Respir Crit Care Med. 1994;150(6 Pt 2):S143–6. doi:10.1164/ajrccm/150.6_Pt_2.S143
10. Scannapieco FA, Papandonatos GD, Dunford RG. Associations between oral conditions and respiratory disease in a national sample survey population. Ann Periodontol. 1998;3(1):251–256. doi:10.1902/annals.1998.3.1.251
11. Scannapieco FA, Ho AW. Potential associations between chronic respiratory disease and periodontal disease: analysis of national health and nutrition examination survey III. J Periodontol. 2001;72(1):50–56. doi:10.1902/jop.2001.72.1.50
12. Chen H, Zhang X, Luo J, Dong X, Jiang X. The association between periodontitis and lung function: results from the national health and nutrition examination survey 2009 to 2012. J Periodontol. 2022;93(6):901–910. doi:10.1002/jper.21-0399
13. Javaheri N, Matin S, Naghizadeh-Baghi A, Bagheri A, Andreasian A, Ghobadi H. Periodontal status, its treatment needs, and its relationship with airflow limitation and quality of life in COPD patients. Eurasian J Med. 2020;52(3):259–264. doi:10.5152/eurasianjmed.2020.20002
14. Zhou X, Wang J, Liu W, et al. Periodontal status and microbiologic pathogens in patients with chronic obstructive pulmonary disease and periodontitis: a case–control study. Int J Chron Obstruct Pulmon Dis. 2020;15:2071–2079. doi:10.2147/copd.S266612
15. Vollmer A, Vollmer M, Lang G, et al. Associations between periodontitis and COPD: an artificial intelligence-based analysis of NHANES III. J Clin Med. 2022;11(23):7210. doi:10.3390/jcm11237210
16. Bhavsar NV, Dave BD, Brahmbhatt NA, Parekh R. Periodontal status and oral health behavior in hospitalized patients with chronic obstructive pulmonary disease. J Nat Sci Biol Med. 2015;6(Suppl 3):S93–7. doi:10.4103/0976-9668.166097
17. Verma AK, Pandey AK, Gupta A, et al. Periodontal status of patients with nontubercular respiratory diseases hospitalized in a tertiary care hospital. Natl J Maxillofac Surg. 2022;13(3):437–442. doi:10.4103/njms.njms_384_21
18. Shen TC, Chang PY, Lin CL, et al. Risk of periodontal diseases in patients with chronic obstructive pulmonary disease: a nationwide population-based cohort study. Medicine. 2015;94(46):e2047. doi:10.1097/md.0000000000002047
19. Takeuchi K, Matsumoto K, Furuta M, et al. Periodontitis is associated with chronic obstructive pulmonary disease. J Dent Res. 2019;98(5):534–540. doi:10.1177/0022034519833630
20. Gupta A, Verma UP, Verma AK, et al. Periodontal diseases: a covert focus of inflammation in pulmonary diseases. Indian J Respir Care. 2019;8:8–17.
21. Kucukcoskun M, Baser U, Oztekin G, Kiyan E, Yalcin F. Initial periodontal treatment for prevention of chronic obstructive pulmonary disease exacerbations. J Periodontol. 2013;84(7):863–870. doi:10.1902/jop.2012.120399
22. Zhou X, Han J, Liu Z, Song Y, Wang Z, Sun Z. Effects of periodontal treatment on lung function and exacerbation frequency in patients with chronic obstructive pulmonary disease and chronic periodontitis: a 2-year pilot randomized controlled trial. J Clin Periodontol. 2014;41(6):564–572. doi:10.1111/jcpe.12247
23. Sharma S, Gupta A, Verma AK, et al. Impact of non-surgical periodontal therapy on pulmonary functions, periodontal health and salivary matrix metalloproteinase-8 of COPD patients with chronic periodontitis: a clinico-biochemical study. Turk Thorac J. 2021;22(4):324–332. doi:10.5152/TurkThoracJ.2021.20096
24. Liu J, Ouyang Y, Zhang Z, et al. The role of Th17 cells: explanation of relationship between periodontitis and COPD? Inflamm Res. 2022;71(9):1011–1024. doi:10.1007/s00011-022-01602-1
25. Sun L, Girnary M, Wang L, et al. IL-10 dampens an IL-17-mediated periodontitis-associated inflammatory network. J Immunol. 2020;204(8):2177–2191. doi:10.4049/jimmunol.1900532
26. Ponce-Gallegos MA, Ramírez-Venegas A, Falfán-Valencia R. Th17 profile in COPD exacerbations. Int J Chron Obstruct Pulmon Dis. 2017;12:1857–1865. doi:10.2147/copd.S136592
27. Le Rouzic O, Koné B, Kluza J, et al. Cigarette smoke alters the ability of human dendritic cells to promote anti-Streptococcus pneumoniae Th17 response. Respir Res. 2016;17(1):94. doi:10.1186/s12931-016-0408-6
28. Moutsopoulos NM, Kling HM, Angelov N, et al. Porphyromonas gingivalis promotes Th17 inducing pathways in chronic periodontitis. J Autoimmun. 2012;39(4):294–303. doi:10.1016/j.jaut.2012.03.003
29. Jasper AE, McIver WJ, Sapey E, Walton GM. Understanding the role of neutrophils in chronic inflammatory airway disease. F1000Research. 2019;8. doi:10.12688/f1000research.18411.1
30. Burnett D, Chamba A, Hill SL, Stockley RA. Neutrophils from subjects with chronic obstructive lung disease show enhanced chemotaxis and extracellular proteolysis. Lancet. 1987;2(8567):1043–1046. doi:10.1016/s0140-6736(87)91476-0
31. Hajishengallis G. New developments in neutrophil biology and periodontitis. Periodontol 2000. 2020;82(1):78–92. doi:10.1111/prd.12313
32. Hajishengallis E, Hajishengallis G. Neutrophil homeostasis and periodontal health in children and adults. J Dent Res. 2014;93(3):231–237. doi:10.1177/0022034513507956
33. Kayar NA, Üstün K, Gözlü M, Haliloğlu S, Alptekin N. The effects of non-surgical periodontal therapy on neutrophil elastase and elastase alpha-1 proteinase inhibitor levels in GCF in periodontitis patients with or without acute coronary syndrome. Clin Oral Investig. 2021;25(5):3329–3338. doi:10.1007/s00784-021-03838-3
34. Cazzola M, Stolz D, Rogliani P, Matera MG. α(1)-Antitrypsin deficiency and chronic respiratory disorders. Eur Respir Rev. 2020;29(155). doi:10.1183/16000617.0073-2019
35. Serban KA, Petrache I. Mouse models of COPD. Methods Mol Biol. 2018;1809:379–394. doi:10.1007/978-1-4939-8570-8_25
36. Fujita J, Nelson NL, Daughton DM, et al. Evaluation of elastase and antielastase balance in patients with chronic bronchitis and pulmonary emphysema. Am Rev Respir Dis. 1990;142(1):57–62. doi:10.1164/ajrccm/142.1.57
37. Hao W, Li M, Zhang Y, Zhang C, Xue Y. Expressions of MMP-12, TIMP-4, and neutrophil elastase in PBMCs and exhaled breath condensate in patients with COPD and their relationships with disease severity and acute exacerbations. J Immunol Res. 2019;2019:7142438. doi:10.1155/2019/7142438
38. Aral CA, Ölçer SN, Aral K, Kapila Y. Oxidative stress, neutrophil elastase and IGFBP7 levels in patients with oropharyngeal cancer and chronic periodontitis. Oral Dis. 2020;26(7):1393–1401. doi:10.1111/odi.13370
39. Hiyoshi T, Domon H, Maekawa T, et al. Neutrophil elastase aggravates periodontitis by disrupting gingival epithelial barrier via cleaving cell adhesion molecules. Sci Rep. 2022;12(1):8159. doi:10.1038/s41598-022-12358-3
40. Fastovets OO, Masheiko IV, Lucash AY. Evaluation of bone resorptive potential in the treatment of generalized periodontitis. Wiad Lek. 2020;73(11):2396–2402.
41. Spiropoulou A, Zareifopoulos N, Bellou A, Spiropoulos K, Tsalikis L. Review of the association between periodontitis and chronic obstructive pulmonary disease in smokers. Monaldi Arch Chest Dis. 2019;89(1). doi:10.4081/monaldi.2019.1018
42. Taniguchi A, Tsuge M, Miyahara N, Tsukahara H. Reactive oxygen species and antioxidative defense in chronic obstructive pulmonary disease. Antioxidants. 2021;10(10). doi:10.3390/antiox10101537
43. Kang W, Jia Z, Tang D, et al. Fusobacterium nucleatum facilitates apoptosis, ROS generation, and inflammatory cytokine production by activating AKT/MAPK and NF-κB signaling pathways in human gingival fibroblasts. Oxid Med Cell Longev. 2019;2019:1681972. doi:10.1155/2019/1681972
44. Keddache S, Laheurte C, Boullerot L, et al. Inflammatory and immunological profile in COPD secondary to organic dust exposure. Clin Immunol. 2021;229:108798. doi:10.1016/j.clim.2021.108798
45. Guo P, Li R, Piao TH, Wang CL, Wu XL, Cai HY. Pathological mechanism and targeted drugs of COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:1565–1575. doi:10.2147/copd.S366126
46. Wheaton AG, Liu Y, Croft JB, et al. Chronic obstructive pulmonary disease and smoking status - United States, 2017. MMWR Morb Mortal Wkly Rep. 2019;68(24):533–538. doi:10.15585/mmwr.mm6824a1
47. Kouanda B, Sattar Z, Geraghty P. Periodontal diseases: major exacerbators of pulmonary diseases? Pulm Med. 2021;2021:4712406. doi:10.1155/2021/4712406
48. Hogea SP, Tudorache E, Fildan AP, Fira-Mladinescu O, Marc M, Oancea C. Risk factors of chronic obstructive pulmonary disease exacerbations. Clin Respir J. 2020;14(3):183–197. doi:10.1111/crj.13129
49. Soriano JB. An epidemiological overview of chronic obstructive pulmonary disease: what can real-life data tell us about disease management? Copd. 2017;14(sup1):S3–s7. doi:10.1080/15412555.2017.1286165
50. Marruganti C, Shin HS, Sim SJ, Grandini S, Laforí A, Romandini M. Air pollution as a risk indicator for periodontitis. Biomedicines. 2023;11(2). doi:10.3390/biomedicines11020443
51. Doiron D, de Hoogh K, Probst-Hensch N, et al. Air pollution, lung function and COPD: results from the population-based UK Biobank study. Eur Respir J. 2019;54(1). doi:10.1183/13993003.02140-2018
52. Glencross DA, Ho TR, Camiña N, Hawrylowicz CM, Pfeffer PE. Air pollution and its effects on the immune system. Free Radic Biol Med. 2020;151:56–68. doi:10.1016/j.freeradbiomed.2020.01.179
53. Ni K, Hua Y. Hydrogen sulfide exacerbated periodontal inflammation and induced autophagy in experimental periodontitis. Int Immunopharmacol. 2021;93:107399. doi:10.1016/j.intimp.2021.107399
54. Katsiki N, Steiropoulos P, Papanas N, Mikhailidis DP. Diabetes mellitus and chronic obstructive pulmonary disease: an overview. Exp Clin Endocrinol Diabetes. 2021;129(10):699–704. doi:10.1055/a-1038-3883
55. Luong A, Tawfik AN, Islamoglu H, et al. Periodontitis and diabetes mellitus co-morbidity: a molecular dialogue. J Oral Biosci. 2021;63(4):360–369. doi:10.1016/j.job.2021.10.006
56. Preshaw PM, Bissett SM. Periodontitis and diabetes. Br Dent J. 2019;227(7):577–584. doi:10.1038/s41415-019-0794-5
57. Park SS, Perez Perez JL, Perez Gandara B, et al. Mechanisms linking COPD to type 1 and 2 diabetes mellitus: is there a relationship between diabetes and COPD? Medicina. 2022;58(8). doi:10.3390/medicina58081030
58. Hobbins S, Chapple IL, Sapey E, Stockley RA. Is periodontitis a comorbidity of COPD or can associations be explained by shared risk factors/behaviors? Int J Chron Obstruct Pulmon Dis. 2017;12:1339–1349. doi:10.2147/copd.S127802
59. Jung ES, Lee KH, Choi YY. Association between oral health status and chronic obstructive pulmonary disease in Korean adults. Int Dent J. 2020;70(3):208–213. doi:10.1111/idj.12535
60. Lopez-de-andrés A, Vazquez-Vazquez L, Martinez-Huedo MA, et al. Is COPD associated with periodontal disease? A population-based study in Spain. Int J Chron Obstruct Pulmon Dis. 2018;13:3435–3445. doi:10.2147/copd.S174898
61. Lenk M, Noack B, Weidner K, Lorenz K. Psychopathologies and socioeconomic status as risk indicators for periodontitis: a survey-based investigation in German dental practices. Clin Oral Investig. 2022;26(3):2853–2862. doi:10.1007/s00784-021-04263-2
62. Gaeckle NT, Heyman B, Criner AJ, Criner GJ. Markers of dental health correlate with daily respiratory symptoms in COPD. Chron Obstruct Pulmon Dis. 2018;5(2):97–105. doi:10.15326/jcopdf.5.2.2017.0159
63. Muthu J, Muthanandam S, Mahendra J. Mouth the mirror of lungs: where does the connection lie? Front Med. 2016;10(4):405–409. doi:10.1007/s11684-016-0476-5
64. Scannapieco FA. Role of oral bacteria in respiratory infection. J Periodontol. 1999;70(7):793–802. doi:10.1902/jop.1999.70.7.793
65. Tan L, Wang H, Li C, Pan Y. 16S rDNA-based metagenomic analysis of dental plaque and lung bacteria in patients with severe acute exacerbations of chronic obstructive pulmonary disease. J Periodontal Res. 2014;49(6):760–769. doi:10.1111/jre.12159
66. Tan L, Pan C, Wang H, Zhao J, Zhao H, Pan Y. The homology analysis of Porphyromonas gingivalis, Treponema denticola and Tannerella forsythia in oral cavity and respiratory tract of COPD. Chin J Microecol. 2015;27(5). Chinese. doi:10.13381/j.cnki.cjm.201505010
67. Tian H, Zhang Z, Wang X, Liu W, Wang Z. Role of experimental periodontitis in inducing pulmonary inflammation in mice. Oral Dis. 2021. doi:10.1111/odi.13949
68. Parashar P, Parashar A, Saraswat N, Pani P, Pani N, Joshi S. Relationship between respiratory and periodontal health in adults: a case-control study. J Int Soc Prev Community Dent. 2018;8(6):560–564. doi:10.4103/jispcd.JISPCD_304_18
69. Budden KF, Shukla SD, Rehman SF, et al. Functional effects of the microbiota in chronic respiratory disease. Lancet Respir Med. 2019;7(10):907–920. doi:10.1016/s2213-2600(18)30510-1
70. Pathak JL, Yan Y, Zhang Q, Wang L, Ge L. The role of oral microbiome in respiratory health and diseases. Respir Med. 2021;185:106475. doi:10.1016/j.rmed.2021.106475
71. Tan L, Tang X, Pan C, Wang H, Pan Y. Relationship among clinical periodontal, microbiologic parameters and lung function in participants with chronic obstructive pulmonary disease. J Periodontol. 2019;90(2):134–140. doi:10.1002/jper.17-0705
72. Imai K, Iinuma T, Sato S. Relationship between the oral cavity and respiratory diseases: aspiration of oral bacteria possibly contributes to the progression of lower airway inflammation. Jpn Dent Sci Rev. 2021;57:224–230. doi:10.1016/j.jdsr.2021.10.003
73. Miya C, Cueno ME, Suzuki R, et al. Porphyromonas gingivalis gingipains potentially affect MUC5AC gene expression and protein levels in respiratory epithelial cells. FEBS Open Bio. 2021;11(2):446–455. doi:10.1002/2211-5463.13066
74. Suzuki R, Kamio N, Kaneko T, Yonehara Y, Imai K. Fusobacterium nucleatum exacerbates chronic obstructive pulmonary disease in elastase-induced emphysematous mice. FEBS Open Bio. 2022;12(3):638–648. doi:10.1002/2211-5463.13369
75. Kamio N, Hayata M, Tamura M, Tanaka H, Imai K. Porphyromonas gingivalis enhances pneumococcal adhesion to human alveolar epithelial cells by increasing expression of host platelet-activating factor receptor. FEBS Lett. 2021;595(11):1604–1612. doi:10.1002/1873-3468.14084
76. Sapey E, Yonel Z, Edgar R, et al. The clinical and inflammatory relationships between periodontitis and chronic obstructive pulmonary disease. J Clin Periodontol. 2020;47(9):1040–1052. doi:10.1111/jcpe.13334
77. Okabe T, Kamiya Y, Kikuchi T, et al. Porphyromonas gingivalis components/secretions synergistically enhance pneumonia caused by streptococcus pneumoniae in mice. Int J Mol Sci. 2021;22(23). doi:10.3390/ijms222312704
78. Yoshida K, Yoshida K, Fujiwara N, et al. Extracellular vesicles of P. gingivalis-infected macrophages induce lung injury. Biochim Biophys Acta Mol Basis Dis. 2021;1867(11):166236. doi:10.1016/j.bbadis.2021.166236
79. Hayata M, Watanabe N, Tamura M, et al. The periodontopathic bacterium Fusobacterium nucleatum induced proinflammatory cytokine production by human respiratory epithelial cell lines and in the lower respiratory organs in mice. Cell Physiol Biochem. 2019;53(1):49–61. doi:10.33594/000000120
80. Saradna A, Do DC, Kumar S, Fu QL, Gao P. Macrophage polarization and allergic asthma. Transl Res. 2018;191:1–14. doi:10.1016/j.trsl.2017.09.002
81. Bazzan E, Turato G, Tinè M, et al. Dual polarization of human alveolar macrophages progressively increases with smoking and COPD severity. Respir Res. 2017;18(1):40. doi:10.1186/s12931-017-0522-0
82. Yu T, Zhao L, Huang X, et al. Enhanced activity of the macrophage M1/M2 phenotypes and phenotypic switch to M1 in periodontal infection. J Periodontol. 2016;87(9):1092–1102. doi:10.1902/jop.2016.160081
83. Xu R, Zeng G, Wang S, et al. Periodontitis promotes the diabetic development of obese rat via miR-147 induced classical macrophage activation. Biomed Pharmacother. 2016;83:892–897. doi:10.1016/j.biopha.2016.07.030
84. Lyu J, Bian T, Chen B, et al. β-defensin 3 modulates macrophage activation and orientation during acute inflammatory response to Porphyromonas gingivalis lipopolysaccharide. Cytokine. 2017;92:48–54. doi:10.1016/j.cyto.2016.12.015
85. Han J, Cheng C, Zhu Z, et al. Vitamin D reduces the serum levels of inflammatory cytokines in rat models of periodontitis and chronic obstructive pulmonary disease. J Oral Sci. 2019;61(1):53–60. doi:10.2334/josnusd.17-0357
86. Yang Y, Li W, Wang ZM, Sun GY, Zhou P, Han XL. 慢性牙周炎与慢性阻塞性肺疾病急性加重患者血清白介素6和8水平及其与疾病关系初探[Clinical significance of interleukin-6 and −8 in patients with chronic periodontal disease and acute exacerbation of chronic obstructive pulmonary disease]. Chin J Stomatolol. 2018;53(5):312–317. Chinese. doi:10.3760/cma.j.issn.1002-0098.2018.05.005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Value of Serum Immune-Inflammatory Markers for Adverse Pregnancy Outcomes in Pregnant Women with Thrombophilia: A Retrospective Cohort Study
Zheng L, Ge R, Weng X, Lin L
Journal of Inflammation Research 2024, 17:6083-6091
Published Date: 5 September 2024
Age-Stratified Immune-Inflammatory Profiles and Prognostic Implications of Old Patients in the ICU: A Prospective Study
Lian H, Wang G, Zhang Q, Zhao H, Wang X
Journal of Inflammation Research 2025, 18:13727-13743
Published Date: 3 October 2025