Back to Journals » Nature and Science of Sleep » Volume 18

Research on Large Endothelial Cell-Derived Extracellular Vesicles in Pediatric Obstructive Sleep Apnea Syndrome
Authors Lin W, Zhang H, Cao L, Wang S, Cui Y, Huang T, Wu T, Huang X, Lu Q, Yang Q ![]()
Received 9 February 2026
Accepted for publication 9 June 2026
Published 7 July 2026 Volume 2026:18 593831
DOI https://doi.org/10.2147/NSS.S593831
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Weinan Lin1,2,*, Hezi Zhang3,*, Lichao Cao3, Sihan Wang3, Yunfei Cui1, Ting Huang1,2, Tao Wu1,2, Xiao Huang1, Qinghua Lu1, Qin Yang1,2
1Department of Respiratory Medicine, Shenzhen Children’s Hospital, Shenzhen, Guangdong Province, People’s Republic of China; 2Shenzhen Pediatrics Institute of Shantou University Medical College, Shenzhen, Guangdong Province, People’s Republic of China; 3Department of Research and Development, Shenzhen Nucleus Gene Technology Co., Ltd, Shenzhen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qin Yang, Department of Respiratory Medicine, Shenzhen Children’s Hospital, Shenzhen, Guangdong Province, People’s Republic of China, Tel +86 18938690778, Email [email protected]
Purpose: To explore the association between clinical indicators of obstructive sleep apnea (OSA) and large endothelial cell-derived extracellular vesicles (large endothelial EVs) in children, and to explore their potential association with disease severity.
Patients and Methods: A total of 81 children with OSA were enrolled, including 29 cases of mild OSA and 52 cases of moderate-to-severe OSA. Receiver operating characteristic (ROC) curves evaluated the discriminatory ability of these EVs for severity groups. The correlation between large endothelial EVs and OSA clinical results, including sleep architecture and sleep-disordered breathing events, was evaluated using Spearman correlation analysis and multiple regression analysis.
Results: Levels of CD31+CD41- large endothelial EVs were significantly elevated in children with moderate-to-severe OSA compared to the mild OSA group (p< 0.05). While CD62E levels were nominally elevated in moderate-to-severe OSA (p<0.05), this association did not persist following false discovery rate correction, and the marker showed limited predictive utility in the validation cohort (AUC = 0.538). The ROC curve results indicated that the sensitivity and specificity of CD31+CD41- in distinguishing mild OSA from moderate-to-severe OSA were 82.8% and 75%, respectively, with an area under the curve of 0.848. CD31+CD41- large endothelial EVs in children with OSA showed significant positive correlations with the Obstructive Apnea-Hypopnea Index (OAHI), hypopnea index, and oxygen desaturation index (p<0.05). Multiple regression analysis revealed a logarithmic positive correlation between OAHI and CD31+CD41- large endothelial EVs (p<0.01). Sleep efficiency was negatively correlated with CD31+CD41- large endothelial EVs (p<0.05).
Conclusion: CD31+CD41- large endothelial EVs were closely associated with OAHI and sleep efficiency. These exploratory findings suggest their potential as a biomarker of OSA severity, but prospective validation is required before clinical application.
Keywords: obstructive sleep apnea, sleep architecture, large endothelial cell-derived extracellular vesicles, child
Introduction
Obstructive sleep apnea (OSA) is the most common form of sleep-disordered breathing in children. Recent epidemiological data indicate that the prevalence of childhood OSA is approximately 5.7%. Its main characteristics include recurrent partial or complete upper airway obstruction during sleep, leading to chronic intermittent hypoxia, hypercapnia, and sleep fragmentation.1,2 Previous studies have shown that OSA can cause neurocognitive deficits, cardiovascular complications, and metabolic disorders in children, seriously affecting their long-term health.3 Notably, OSA poses a significant threat to the cardiovascular health of children and adolescents, significantly increasing the risk of cardiovascular diseases such as hypertension, cardiac structural abnormalities, and heart failure.4 Among these, vascular endothelial injury is an early pathophysiological manifestation of OSA-related cardiovascular diseases.5 Chronic intermittent hypoxia and frequent sleep disruptions caused by OSA can induce systemic inflammatory responses and oxidative stress, resulting in damage to the structure and function of vascular endothelium.6
According to the Minimal Information for Studies of Extracellular Vesicles 2023 (MISEV2023) guidelines,7 endothelial microparticles (EMPs) are defined as large endothelial cell-derived extracellular vesicles (large endothelial EVs) that are released by direct budding from the plasma membrane of endothelial cells upon activation, injury, or apoptosis. Large endothelial EVs are vesicular membrane structures released by activated or apoptotic endothelial cells, with a diameter of approximately 0.1–1.0 μm, and carry endothelial-specific markers on their surface.8 Elevated large endothelial EV levels are positively correlated with the degree of endothelial injury. They are regarded as biomarkers of vascular endothelial damage.9–11 The surface markers of large endothelial EVs exhibit different phenotypic characteristics depending on the type of cardiovascular disease. CD62E is a classic marker of endothelial activation and is frequently upregulated under inflammatory conditions and in atherosclerotic cardiovascular disease.12 Adult studies have shown that CD62E large endothelial EVs are elevated in patients with pulmonary hypertension.13 The CD31+CD41− phenotype is considered a marker of endothelial cell apoptosis or damage and is elevated in conditions such as hyperlipidemia.14,15 CD31+CD42b− large endothelial EVs can specifically reflect the activation or apoptotic status of endothelial cells, and has been specifically associated with nocturnal hypoxia and disease severity in adult patients with OSA.5 Therefore, we selected these large endothelial EVs phenotypes to investigate endothelial activation, apoptosis/damage, and hypoxia‑related stress responses, aiming to better characterize the endothelial phenotype in pediatric OSA. Given that children have a lower chronic atherosclerotic burden, more pronounced adenotonsillar hypertrophy, and a shorter disease course than adults, the release profile of large endothelial EVs may differ from that observed in adults. However, few studies have investigated the relationship between large endothelial EVs and detailed sleep architecture parameters in children with OSA.
Therefore, this study not only evaluated the levels of large endothelial EVs in different OSA severity groups but also explored their specific associations with polysomnographic parameters, including respiratory events during sleep and sleep architecture, thereby providing new insights into the mechanisms underlying the link between large endothelial EVs and pediatric OSA. We hypothesized that children with moderate-to-severe OSA would have elevated large endothelial EV levels, and that these levels would be associated with specific sleep respiratory events and sleep architecture. The primary objectives were: (1) to compare the levels of large endothelial EVs (CD62E, CD31+CD41-, and CD31+CD42b-) across OSA severity groups; (2) to analyze correlations between these large endothelial EVs phenotypes and polysomnographic parameters; and (3) to assess their potential as biomarkers for stratifying OSA severity and indicating early vascular endothelial injury.
Materials and Methods
Study Subjects
Children (aged 4–14 years) who visited the sleep disorder clinic at our hospital for snoring and/or mouth breathing were recruited consecutively from December 2023 to April 2025. All parents and children signed the informed consent form (for children aged ≥8 years, signed jointly by the child and their parent/guardian; for children aged <8 years, signed by the parent/guardian on the child’s behalf). Inclusion criteria: children with snoring and/or mouth breathing during night sleep for more than 3 nights/week, and the Obstructive Apnea-Hypopnea Index (OAHI) in overnight polysomnography >1 time/hour.16 Exclusion criteria included: suffering from congenital heart disease, hereditary hypertension or taking antihypertensive drugs; having metabolic disorder-related diseases (such as diabetes, abnormal lipid metabolism); combined with craniofacial deformities, neuromuscular or hereditary diseases; having a history of premature birth or intrauterine growth restriction; being in the acute stage of various diseases; long-term use of anti-inflammatory or sympathomimetic drugs; having received previous OSA treatment (including drugs, surgery, non-invasive ventilation, oral appliances).
Since an OAHI ≥5 event/hour often necessitates the initiation of more aggressive therapeutic interventions (such as continuous positive airway pressure or surgery) rather than watchful waiting or pharmacotherapy alone,17 and this cutoff has been adopted in previous studies,18 moderate and severe OSA were combined into a single moderate-to-severe OSA group (OAHI >5) for the primary analysis in this study. Children with 1 < OAHI ≤5 event/hour were classified into the mild OSA group, and those with OAHI >5 event/hour into the moderate-to-severe OSA group.16 The study was approved by the Ethics Committee of Shenzhen Children’s Hospital (Approval No.: 202,309,102).
Flow Cytometric Analysis
On the morning after PSG monitoring (7:00–8:00), while the child is fasting, a nurse will collect 2.5 mL of venous blood and place it in an anticoagulant tube containing Ethylenediaminetetraacetic Acid, which will be immediately refrigerated and transported to the laboratory for testing within 24 hours. The blood samples were centrifuged at 160×g for 10 minutes to isolate platelet-rich plasma (PRP). Subsequently, the PRP was centrifuged at 1000×g for 6 minutes to obtain platelet-poor plasma (PPP), which was aliquoted into 500 μL portions and stored at −80°C. After thawing, the PPP samples were centrifuged at 16,000×g for 5 minutes at 4°C. A 450 μL aliquot of the supernatant was further centrifuged at 16,000×g for 60 minutes at 4°C, after which 250 μL of the resulting supernatant was discarded. Then, 100 μL of the enriched sample was mixed with 275 μL of dilution buffer (0.2% bovine serum albumin, PBS, 1% paraformaldehyde). The 0.2–1μm particle size gate was validated using the Flow Cytometry Sub-micron Particle Size Reference Kit (Cat. No. F13839, Thermo Fisher Scientific), including 0.2, 0.5, and 1.0 μm fluorescent microspheres. Fluorescence compensation was performed using single-stained controls for each fluorochrome. Fluorescence-minus-one (FMO) controls were used to define the quadrant boundaries for each marker, establishing the threshold for positive staining and eliminating background autofluorescence. The detector threshold was set based on baseline noise and particle signal intensity to exclude electronic noise. All samples were measured in triplicate. Intra-assay and inter-assay coefficients of variation (CV) were determined to ensure reproducibility. Sample processing, flow cytometric acquisition, and data analysis were performed in a blinded manner with respect to clinical group assignment. The mixture was stained with five μL each of APC-conjugated anti-human CD31 antibody (BioLegend, Cat. No. 303115), FITC-conjugated anti-human CD41 antibody (BioLegend, Cat. No. 303703), Brilliant Violet 421™-conjugated anti-human CD42b antibody (BioLegend, Cat. No. 303829), and PE-conjugated anti-human CD62E antibody (BioLegend, Cat. No. 336008). After incubation at 4°C for 45 minutes, the stained samples were filtered through a 200-mesh filter and analyzed using a flow cytometer (BD FACSAria™ III Cell Sorter, No. 95131, USA), with the particle size gate set at 0.2–1 μm. Data were processed using FlowJo v10.8.1 software, and results were presented as dot plots (for gating) and histograms.
Polysomnography (PSG)
Subjects underwent overnight PSG at the Sleep Center of Shenzhen Children’s Hospital from 8:00 PM to 7:00 AM the next day (using German SOMNOmedics V5 or American Philips Alice 6 equipment). PSG leads included the following channels: 6-channel electroencephalography (bilateral central, frontal, and occipital leads), electrooculography, submental electromyography, nasal airflow, thoracoabdominal movement, leg movement, and peripheral blood oxygen saturation. Recorded parameters included: 1. Sleep parameters: Total sleep time; Sleep efficiency; Duration and proportion of each sleep stage, including light sleep (Stage 1 Sleep + Stage 2 Sleep, S1S2), deep sleep (Stage 3 Sleep, S3), and rapid eye movement sleep (REM); 2. Sleep-disordered breathing events: Hypopnea Index (HI); Central Apnea Index (CAI); Obstructive Apnea Index (OAI); Obstructive Apnea-Hypopnea Index (OAHI); Apnea-Hypopnea Index (AHI); Oxygen Desaturation Index (ODI); Oxygen saturation (SpO2) during each sleep stage.
All sleep monitoring data were scored for sleep staging and breathing events by professionally trained technicians certified by the American Board of Registered Polysomnographic Technologists in accordance with the scoring manual.19
Statistical Analysis
Normally distributed data were expressed as “mean ± standard deviation (Mean ± SD)”; continuous variables were compared between groups using an independent-samples t-test, and categorical variables were compared using Chi-square tests. Non-normally distributed data were expressed as “median (P25, P75)” and compared between groups using the Mann–Whitney U-test; Spearman correlation analysis was used to assess the association between large endothelial EVs and various variables. Variables with statistical significance were included in multivariate linear regression analysis to determine the independent effects of age, gender, body mass index (BMI), breathing events, and sleep architecture on large endothelial EV levels. The correlation network heatmap and bubble diagram were visualized in the OmicShare platform (https://www.omicshare.com/tools/). Statistical analysis was performed using SPSS 29.0 (IBM Corp., USA), with statistical significance set at p<0.05. The OSA samples in this study were randomly divided into a training set and a validation set at a ratio of 7:3 (p<0.01), and receiver operating characteristic (ROC) analysis of large endothelial EVs was performed using the timeROC software (version 1.0.3). A model with an area under the ROC curve (AUC) >0.6 was considered to have reliable diagnostic value (Figure 1). To avoid unstable estimation and overfitting, we used 10-fold CV in the training set to optimize the model, followed by 100-iteration Bootstrap resampling to calculate AUC and 95% CIs for both sets separately. To avoid bias, sample processing, flow cytometric acquisition, and data analysis were performed in a blinded fashion without knowledge of the clinical group assignments.
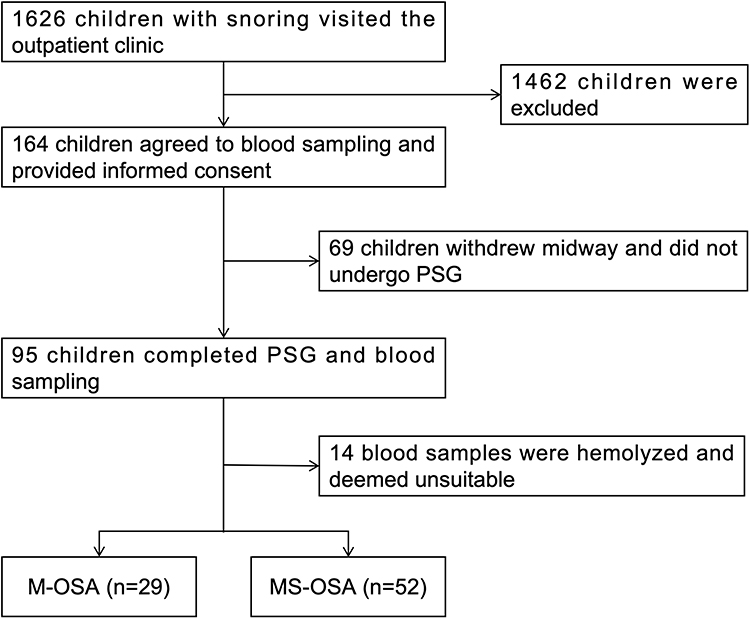 |
Figure 1 The selection process of participants in this study. The study commenced with 1626 snoring children visiting the outpatient clinic. After screening, exclusion of 1462 patients who did not meet the inclusion criteria, 164 children provided informed consent and agreed to participate in blood sampling. 69 children withdrew and did not undergo PSG. Ultimately, 95 children completed both PSG and blood sampling. Fourteen blood samples were excluded due to hemolysis, resulting in 81 children being included in the final analysis. Based on PSG results, participants were categorized into the mild OSA (n=29) and the moderate-to-severe OSA (n=52). |
Results
Study Population and Clinical Results
A total of 81 children aged 4–14 years were finally included in the study, including 53 males (65.4%) and 28 females (34.6%), with a mean age of 8.78±2.91 years; 29 cases (35.8%) in the mild OSA group and 52 cases (64.2%) in the moderate-to-severe OSA group; there were no statistically significant differences in gender, age, adenoid volume or body mass index (BMI) between the groups. The OAHI in the moderate-to-severe OSA group was significantly higher than that in the mild OSA group [8.36 (6.06, 17.70) vs. 2.31 (1.37, 3.09), p<0.001]. The ODI in the moderate-to-severe OSA was significantly higher than that in the mild OSA group [2.10 (1.10, 5.15) vs. 18.65 (8.90, 34.43), p<0.001], whereas the minimum oxygen saturation (minSpO2) in the moderate-to-severe OSA group was lower than that in the mild OSA group [86.00 (79.25, 89.00) vs. 91.00 (89.50, 93.00), p<0.001]. In terms of sleep architecture, the duration of rapid eye movement sleep (REM) in the moderate-to-severe OSA group was significantly shorter than that in the mild OSA group (15.24±4.47 vs. 12.76±5.40, p=0.009, Table 1).
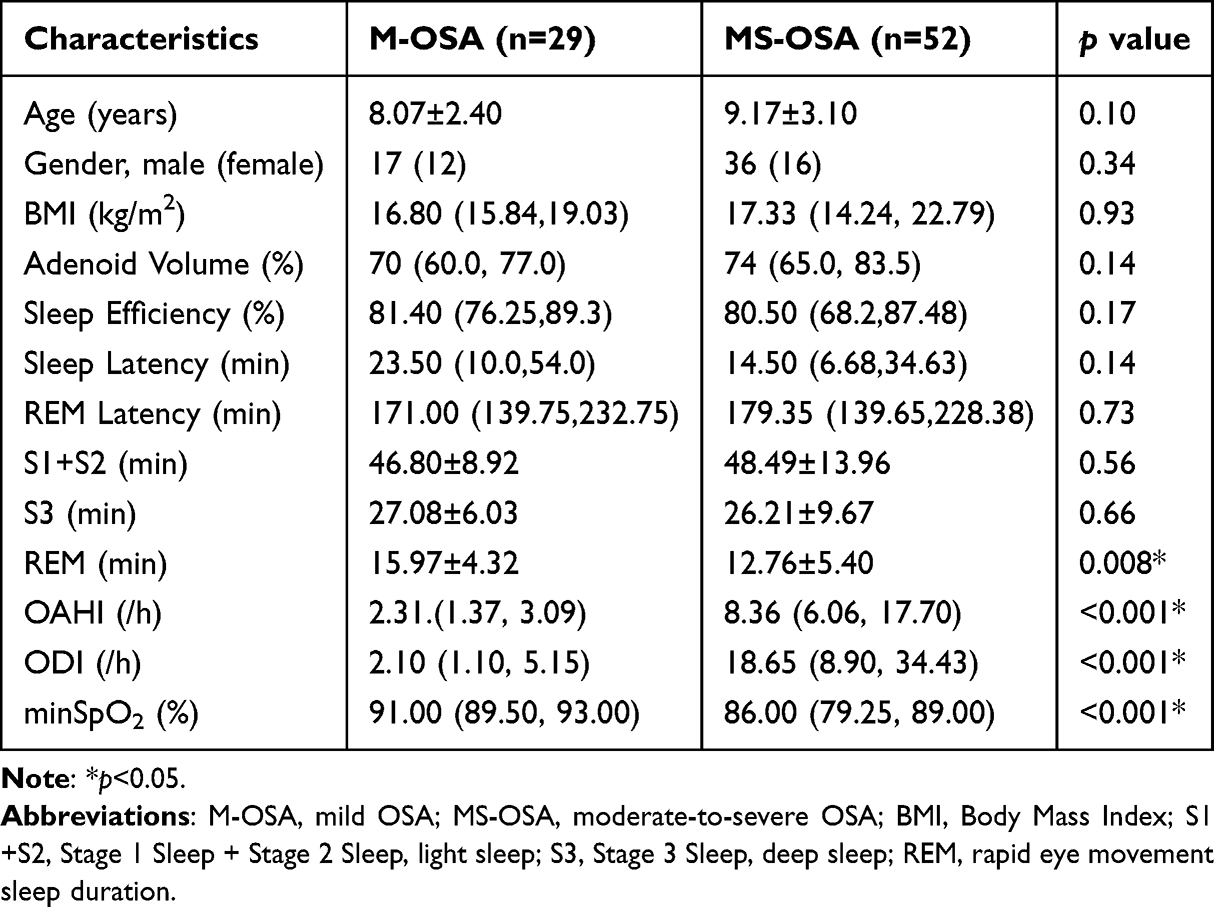 |
Table 1 General Characteristics and Sleep Architecture of Children with Mild OSA and Moderate-to-Severe OSA |
Large Endothelial EV Characteristics in Children with OSA
Compared with the mild OSA group, the levels of CD62E, CD31+CD41-, and CD31+CD42b- large endothelial EVs in the moderate-to-severe OSA group were all increased (Figure 2). In detail, the level of CD62E in the moderate-to-severe OSA group was significantly higher than that in the mild OSA group (182.20±46.87 MPs/μL vs. 150.84±38.43 MPs/μL, p<0.01, Figure 2B); CD31+CD41- large endothelial EVs in the moderate-to-severe OSA group were also significantly higher than those in the mild OSA group [(66 (53.13, 84.88) MPs/μL vs. 45.50 (39.75, 53.75) MPs/μL, p<0.01, Figure 2C)]; while the difference in CD31+CD42b- large endothelial EVs between the two groups was not statistically significant [(260 (173.75, 425.00) MPs/μL vs. 230.00 (125.00, 305.00) MPs/μL, p>0.05, Figure 2D].
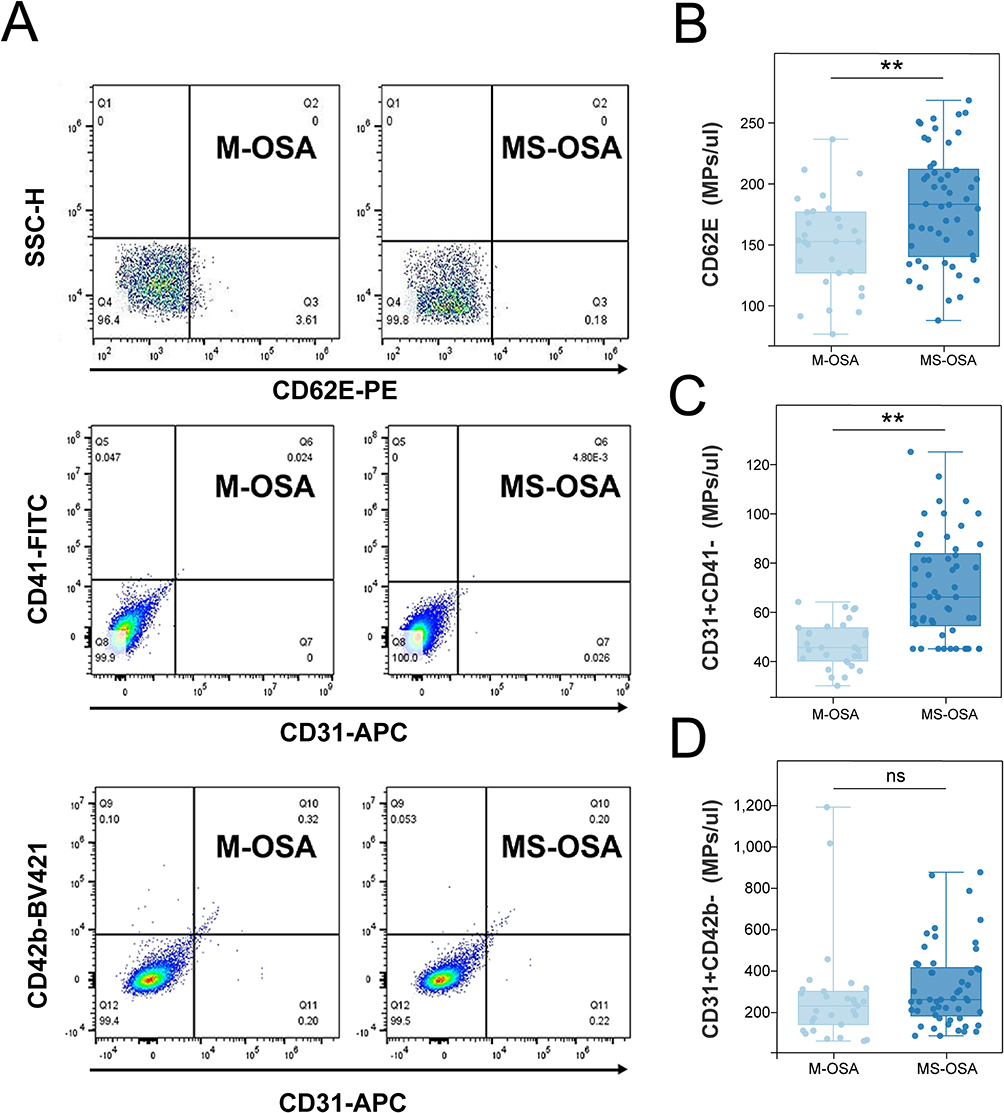 |
Figure 2 Flow Cytometry Analysis Profiles of Large Endothelial EVs in Children with OSA. The figure shows the results of flow cytometry analysis of large endothelial EVs in PPP samples from the mild OSA and moderate-to-severe OSA groups. Gating strategy was defined using fluorescence-minus-one (FMO) controls to determine quadrant boundaries and positive staining thresholds for each marker. (A) is a flow cytometry heatmap of CD62E+, CD31+CD41-, and CD31+CD42b- large endothelial EVs, where SSC-H stands for side scatter height; the levels of CD62E (B) and CD31+CD41- (C) large endothelial EVs in the moderate-to-severe OSA group were significantly higher than those in the mild OSA group (p<0.05, p<0.01). There was no statistically significant difference in CD31+CD42b- between the mild OSA and moderate-to-severe OSA groups (D, p>0.05). *p<0.05, **p<0.01. Abbreviations: M-OSA, Mild OSA; MS-OSA, Moderate-to-Severe OSA. |
ROC analyses were performed to evaluate the discriminative performance of CD62E, CD31+CD41-, and CD31+CD42b- in distinguishing the mild OSA group from the moderate-to-severe OSA group. CD31+CD41- showed the best overall performance [AUC, 95% confidence interval (CI): 0.848, 0.765–0.935]. The AUC of CD62E is 0.688 (95% CI 0.572–0.805), whereas CD31+CD42b- showed limited discrimination (AUC, 95% CI: 0.612, 0.482–0.742). Using the optimal cut-off values derived from the ROC curves, the best thresholds were 54.75 for CD31+CD41- (specificity 0.750, sensitivity 0.828), 180.245 for CD62E (specificity 0.538, sensitivity 0.828), and 372.5 for CD31+CD42b- (specificity 0.346, sensitivity 0.897, Figure 3A).
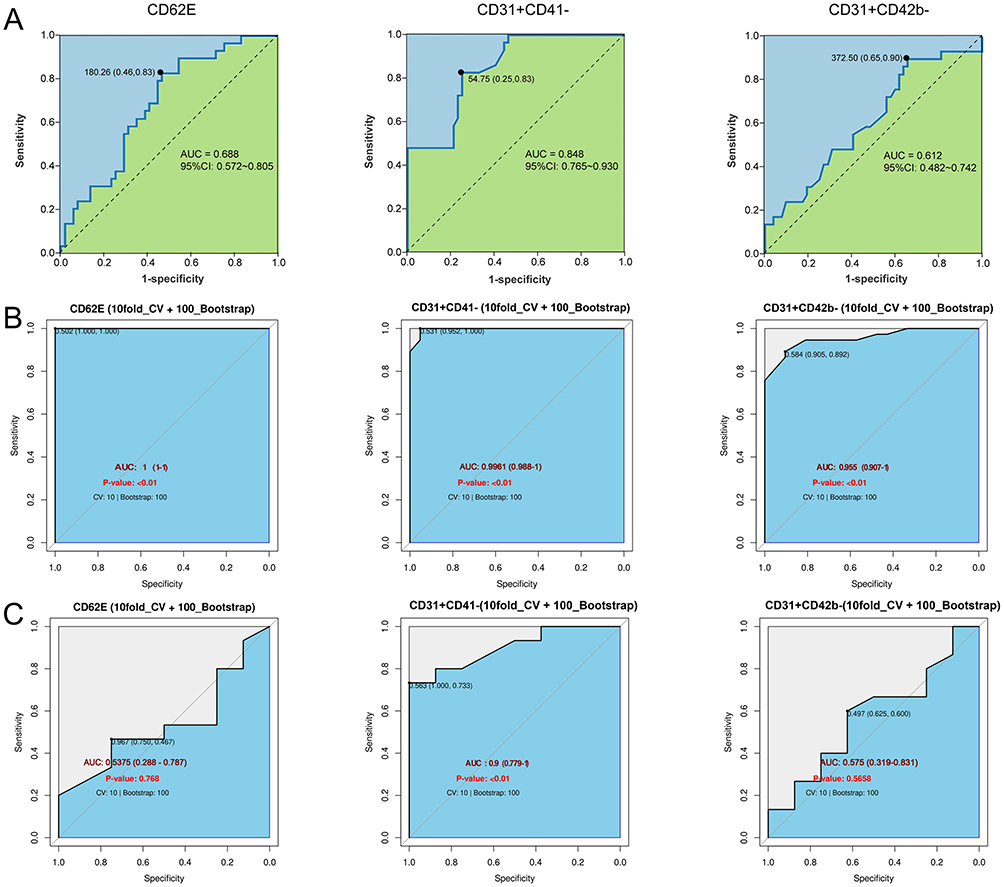 |
Figure 3 ROC Curve Analysis of Vascular Large Endothelial EVs in Distinguishing Mild from Moderate-to-Severe OSA. (A) ROC curves evaluating the discriminative performance of three biomarkers: CD62E (A, AUC=0.688, 95% CI: 0.572–0.805), CD31+CD41- (B, AUC=0.848, 95% CI: 0.765–0.930), and CD31+CD42b- (C, AUC=0.612, 95% CI: 0.482–0.742), for distinguishing between the mild OSA and moderate-to-severe OSA groups, with the diagonal dashed line in each panel representing the reference line of no discriminative value (AUC=0.5). (B) ROC curves with 10-fold cross-validation and 100 bootstrap iterations in the training set. (C) ROC curves with 10-fold cross-validation and 100 bootstrap iterations in the validation set. CD31+CD41− demonstrated superior diagnostic accuracy in both the training (AUC = 0.996, 95% CI: 0.988–1.000) and validation (AUC = 0.900, 95% CI: 0.779–1.000) sets, while CD62E and CD31+CD42b− exhibited reduced performance in the validation (AUCs ≤ 0.575). |
Furthermore, we conducted 10-fold cross-validation and Bootstrap validation on both the training and validation datasets to further verify the diagnostic efficacy of CD62E, CD31+CD41- and CD31+CD42b- in differentiating mild OSA from moderate-to-severe OSA. Notably, diagnostic performance derived from the training set tends to be optimistically biased; therefore, we primarily interpret diagnostic capacity based on validation-set results. In the training set (Figure 3B): CD31+CD41- (AUC 0.996, 95% CI 0.988–1.000), CD62E (AUC 1.000, 95% CI 1.000–1.000), CD31+CD42b- (AUC 0.955, 95% CI 0.907–1.000). In the validation set (Figure 3C): CD31+CD41- (AUC 0.900, 95% CI 0.779–1.000), CD62E (AUC 0.538, 95% CI 0.288–0.787), CD31+CD42b- (AUC 0.575, 95% CI 0.319–0.831).
Spearman Correlation Analysis Between Clinical Indicators and Large Endothelial EVs
Correlation analysis showed that there were significant associations between sleep architecture and specific large endothelial EV subsets (Figure 4). Briefly, sleep efficiency was significantly negatively correlated with CD31+CD41- microparticle levels (r=−0.223, p=0.045); REM latency was significantly positively correlated with CD62E microparticle levels (r=0.245, p=0.022). However, after False Discovery Rate (FDR) correction, no significant correlations were found between large endothelial EVs and sleep architecture (all p>0.05).
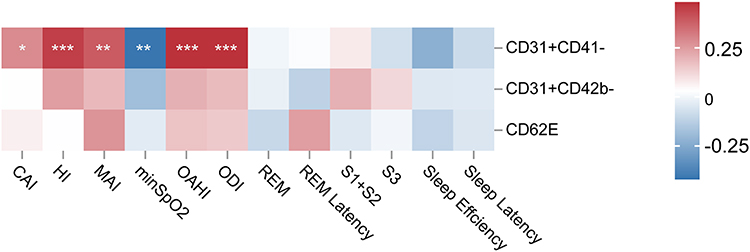 |
Figure 4 Correlation Analysis of Large Endothelial EVs with Sleep-Disordered Breathing Events and Sleep Architecture in Children with OSA Following FDR Correction. Red and blue colors indicate positive and negative correlations, respectively. The color intensity represents the magnitude of the correlation coefficient. CD31+CD41- EVs were significantly positively correlated with OAHI, CAI, MAI, HI, and ODI, and significantly negatively correlated with minSpO2, whereas CD31+CD42b- and CD62E showed no significant correlations with sleep parameters. * p < 0.05, ** p < 0.01, *** p < 0.001. |
CD31+CD41- large endothelial cell-derived extracellular vesicles were significantly positively correlated with OAHI, Central Apnea Index (CAI), Mixed Apnea Index (MAI), Hypopnea Index (HI), and Oxygen Desaturation Index (ODI) (r=0.492, r=0.297, r=0.401, r=0.463, r=0.492, p<0.05). They were significantly negatively correlated with Minimum Oxygen Saturation (minSpO2) (r=−0.413, p<0.01). CD31+CD42b- large endothelial EVs were only significantly positively correlated with HI (r=0.255, p=0.022), and CD62E large endothelial EVs were only positively correlated with MAI (r=0.271, p=0.010). After FDR correction, the correlations of CD31+CD41- with OAHI, CAI, MAI, HI, ODI, and minSpO2 remained significant, whereas the correlations of CD62E and CD31+CD42b- microparticles with sleep respiratory events were not significant. The above results indicate that CD31+CD41- large endothelial EVs are most closely associated with OSA-related sleep-disordered breathing events.
Data analysis showed that OAHI in children with OSA was logarithmically positively correlated with CD31+CD41- large endothelial EVs (R2=0.182, p<0.001). In children with OSA, as OAHI increased, the levels of CD31+CD41- large endothelial EVs first showed a rapid upward trend. The growth rate slowed and plateaued (Figure 5).
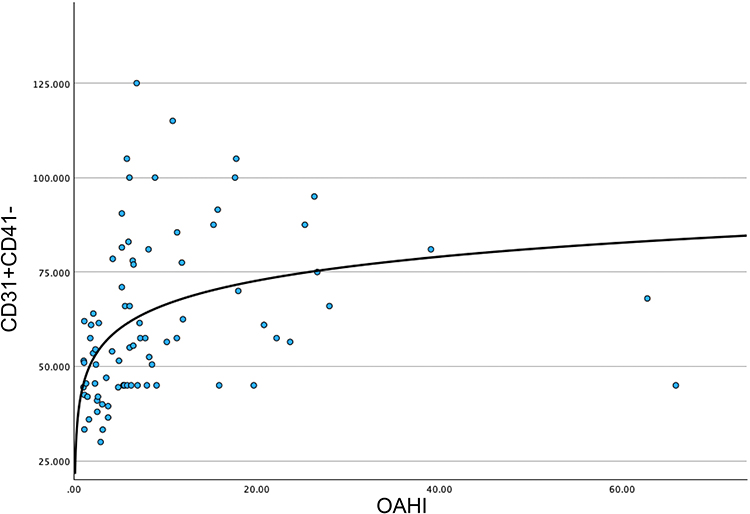 |
Figure 5 OAHI was positively correlated with CD31+CD41- in a logarithmic manner (R2=0.182, p<0.001). |
Multivariate Linear Regression Analysis Between Clinical Indicators and Large Endothelial EVs
Multivariate linear regression analysis was performed with CD31+CD41- large endothelial EVs levels as the dependent variable, logarithmic transformation of OAHI (lnOAHI) as the independent variable, REM sleep as a covariate, and confounding factors such as age, gender, adenoid volume, and BMI. The results showed that, after adjusting for the above confounding factors, lnOAHI was independently positively correlated with CD31+CD41- large endothelial EVs levels (Beta=0.478, p<0.001; Figure 6A), explaining 27.0% of the variation in CD31+CD41- levels (R2=0.270). Specifically, for each one logarithmic unit increase in OAHI, CD31+CD41- large endothelial EV levels increased by 0.478 standard deviations. No linear or curvilinear relationship was found between CD62E, CD31+CD42b- large endothelial EVs, and OAHI. Meanwhile, in this study, multivariate linear regression analysis was performed with sleep efficiency and REM latency as independent variables, REM sleep duration, OAHI, age, adenoid volume, and BMI as covariates, and each large endothelial EV as the dependent variable. The results showed that sleep efficiency was independently negatively correlated with CD31+CD41- levels (Beta=−0.290, p=0.032), explaining 17.3% of the variation in CD31+CD41- levels (R2=0.173), that is, the higher the sleep efficiency, the lower the CD31+CD41- microparticle levels; while CD62E and CD31+CD42b- large endothelial EVs showed no statistical significance (Figure 6B).
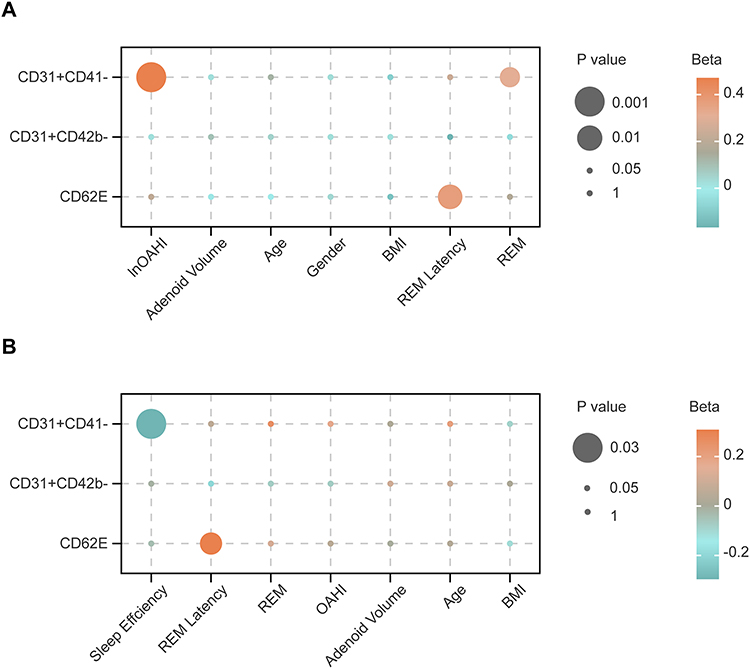 |
Figure 6 Bubble Plot of Multivariate Linear Regression Analysis of OAHI, Sleep Architecture, and Large Endothelial EVs. The bubble plot shows the results of a multivariate linear regression analysis; the size of the dots indicates statistical significance (p-value), and the color indicates the standardized coefficient (Beta; Orange for positive correlation, teal for negative correlation). (A) ln(OAHI) is independently positively correlated with CD31+CD41- levels (Beta=0.478, p<0.001). (B) Sleep efficiency is independently negatively correlated with CD31+CD41- levels (Beta=−0.290, p=0.032). |
Post-hoc power analysis showed that in the multiple linear regression with CD31+CD41- large endothelial extracellular vesicles as the outcome variable, the actual statistical power of the two predictors, ln(OAHI) and sleep efficiency, was 0.99975 and 0.99187, respectively, indicating that the current sample size had sufficient statistical power to detect the associations between CD31+CD41- large endothelial extracellular vesicles and key clinical variables.
Discussion
OSA can induce vascular endothelial injury and dysfunction, leading to the release of large endothelial EVs.20,21 Substantial evidence confirms that vascular large endothelial EVs serve as reliable biomarkers of endothelial damage.22,23 Given the limited research on large endothelial EVs in children, this study not only compared the levels and phenotypic characteristics of large endothelial EVs among children with different severities of OSA, but also performed detailed correlation analyses between large endothelial EVs and multiple polysomnographic parameters, thereby validating and extending previous findings: CD31+CD41- are not only closely associated with the severity of the OAHI, but also significantly correlated with key sleep quality indicators such as sleep efficiency, contributing to a more comprehensive understanding of their potential pathophysiological and biomarker roles.
Previous studies have demonstrated that CD31+CD41- and CD31+CD42b- large endothelial EVs are reliable indicators for assessing the extent of vascular endothelial injury.23,24 In adult patients with OSA, the levels of CD31+CD42b- large endothelial EVs increase progressively with disease severity.18 Additionally, studies have demonstrated that adult OSA patients have endothelial injury, as indicated by elevated CD62E levels, and its concentration is positively correlated with the severity of OSA.25 CD62E is released by activated endothelial cells and can serve as a marker of endothelial cell dysfunction;12 its elevated concentration promotes the adhesion of immune cells and platelets to the endothelium, thereby accelerating the progression of atherosclerosis.24,26–30 Mechanistically, OSA causes endothelial injury through multiple pathways, including nitric oxide (NO) depletion, oxidative stress, inflammatory responses, and endothelial cell apoptosis, and the interaction between endothelial cells and circulating inflammatory cells further exacerbate vascular damage.31,32
Therefore, this study selected CD31+CD41-, CD31+CD42b-, and CD62E large endothelial EVs as the primary observation targets. The results showed that the levels of CD62E and CD31+CD41- large endothelial EVs were significantly correlated with the severity of OSA in children with OSA. As the training-set ROC values present obvious optimistic bias, the diagnostic performance of these biomarkers was interpreted according to validation-set data. ROC curve analysis confirmed that the levels of CD31+CD41- large endothelial EVs differed significantly between children with mild OSA and those with moderate-to-severe OSA, consistent with findings from previous studies.23 CD31+CD42b- large endothelial EVs have been shown in adult OSA studies to be significantly positively correlated with OSA severity, endothelial dysfunction, and carotid intima-media thickness, and may serve as a reliable indicator for assessing OSA-related vascular endothelial dysfunction in adults.5 However, in the present study, no significant differences in levels of these EVs were observed between the mild OSA and moderate-to-severe OSA groups, nor were there any significant correlations with sleep parameters. These findings are not entirely consistent with those reported in adult studies, and this discrepancy may reflect age‑related characteristics in the mechanisms of endothelial injury. This difference may be attributed to the fact that adult OSA is often accompanied by multiple cardiometabolic risk factors, including obesity, hypertension, insulin resistance, and dyslipidemia, each of which can independently promote endothelial cell activation, apoptosis, and microparticle release.33 In contrast, the children enrolled in this study had a lower baseline burden of cardiometabolic risk, indirectly revealing the heterogeneity in endothelial microparticle release across different disease stages and clinical backgrounds. Future studies may further include healthy control children, track changes in CD31+CD42b- levels following therapeutic intervention in children with OSA, and explore the association between CD31+CD42b- and vascular endothelial function, to validate and elucidate the dynamic patterns and clinical significance of CD31+CD42b- in pediatric OSA.
Recent studies focusing on OSA and large endothelial EVs were summarized to describe the significant value of large endothelial EVs (Table 2).5,18,20,25,34–41 However, there are only 2 studies (20%) focusing on large endothelial EVs in childhood OSA, with only 18 cases in the moderate-to-severe OSA group. In contrast, 10 studies (80%) have addressed adult OSA, underscoring the need for research on large endothelial extracellular vesicles in pediatric OSA. 50% of the studies confirmed that large endothelial EV levels are elevated in patients with OSA and positively correlated with AHI, with significantly higher large endothelial EV levels in patients with severe OSA than in those with mild OSA; 3 studies reported that large endothelial EV levels decreased after Continuous Positive Airway Pressure (CPAP) treatment, and another study found that large endothelial EV levels increased after discontinuing CPAP treatment. In addition, 2 studies found that large endothelial EVs are negatively correlated with blood oxygen saturation; 1 study suggested that large endothelial EVs are positively correlated with carotid intima-media thickness; and 1 study found that large endothelial EVs are negatively correlated with vascular diastolic function. The above studies indicate that large endothelial EVs are associated with vascular endothelial function, that their levels increase with the severity of OSA, and that they can significantly decrease after CPAP treatment for OSA. Consistent with findings in adult studies, two pediatric studies on OSA, as well as our own study, have all found that levels of large endothelial EVs in children with OSA are closely associated with disease severity.
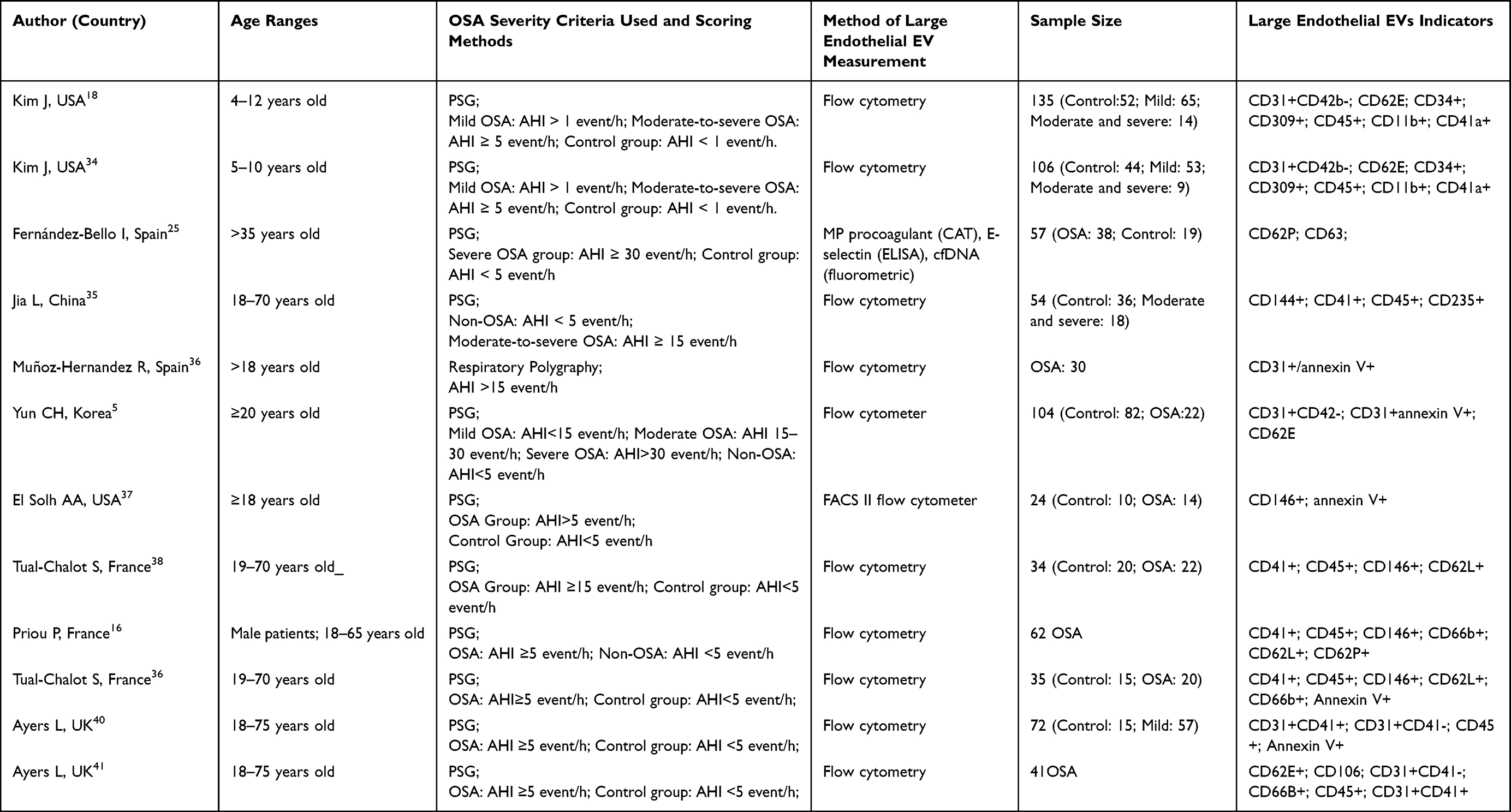 |
Table 2 Main Characteristics of Studies on Large Endothelial EVs in Patients with Obstructive Sleep Apnea |
Additionally, this study systematically compared the relationships between plasma levels of large endothelial EVs, sleep-disordered breathing events, and sleep architecture in children with OSA of varying severity. It was found that CD62E and CD31+CD41- large endothelial EVs were significantly higher in children with moderate-to-severe OSA than in those with mild OSA, and were positively correlated with OAHI, CAI, MAI, HI, and ODI indicators. Khalyfa et al reported that the miRNA content of circulating exosomes in children with OSA can induce alterations in endothelial function and structure,42 which is consistent with the findings of the present study, demonstrating that extracellular vesicles play a broader role in pediatric OSA, serving not only as biomarkers of endothelial injury but also as potential mediators of vascular dysfunction. The close association between large endothelial EVs and sleep architecture indicators in OSA varying severity further supports the link between endothelial activity and sleep disruption in OSA.
OAHI is an indicator reflecting the severity of sleep apnea in children.43,44 Multivariate regression analysis in this study showed that the OAHI index is an independent positive predictor of CD31+CD41- levels, and there is a logarithmic relationship between them: within the lower range of OAHI, CD31+CD41- increases rapidly with increasing OAHI, and the upward trend tends to plateau at higher OAHI levels. This relationship suggests that changes in endothelial-related microparticles may occur significantly in the early or mild-to-moderate stages of OSA, and then enter a relatively saturated state, indicating that vascular-related risks may begin to accumulate from lower OAHI levels, rather than only when OSA is severe.
Moreover, our study suggests that children with moderate-to-severe OSA have significantly shorter REM time and higher levels of large endothelial EVs than those with mild OSA. This result was consistent with previous studies. Recurrent upper airway obstruction in OSA patients is often accompanied by a decrease in blood oxygen saturation, which can cause repeated cortical arousal and lead to decreased REM sleep. The decrease of REM sleep is closely related to the occurrence of cardiovascular diseases.45–47 Recent animal experiments have shown that REM sleep deprivation can induce cardiac systolic function damage.48 This suggests that decreased REM sleep duration may be an important mediator of OSA-related early cardiovascular injury. Future prospective studies are warranted to explore this further. Sleep efficiency is a commonly used objective indicator to evaluate sleep quality. Insufficient sleep can enhance sympathetic nerve activity and inhibit parasympathetic nerve activity, resulting in increased blood pressure, impaired endothelial function, and increased inflammatory response.49–51 The multivariate linear regression analysis in this study revealed that, as sleep efficiency decreased in children with OSA, levels of CD31+CD41- increased. This suggests a statistical association between reduced sleep efficiency and elevated levels of large endothelial extracellular vesicles in children with OSA, potentially reflecting vascular endothelial injury associated with sleep architecture disruption. In light of the existing mechanistic literature and the cross-sectional data from this study, future longitudinal or interventional studies are warranted to explore the potential role of improving sleep architecture and sleep efficiency in mitigating vascular endothelial injury in children with OSA.
The main limitations of this study are as follows. First, its cross-sectional design precludes causal or prognostic inferences. Second, this study has a relatively small total sample size (n=81, 24 in the validation set), a single-center design, potential unmeasured confounding factors, and a reliance on a single 7:3 random split, though 10-fold CV and Bootstrap resampling were used to improve reliability, and future work will expand the sample size, conduct multi-center validation, and optimize the model with more clinical variables. Third, a healthy non-OSA control group was absent, restricting comparisons to mild versus moderate-to-severe OSA. Fourth, large endothelial EVs were measured only by flow cytometry; complementary methods (TEM/NTA) were not used, and platelet-derived vesicle overlap could not be fully excluded, consistent with MISEV limitations. Fifth, inflammatory and oxidative stress markers were not co-measured, preventing a complete mechanistic pathway from hypoxia to endothelial dysfunction. Sixth, although actual age was included as a continuous covariate in all multivariable models, pubertal status (Tanner stage) was not assessed, which can only partially reflect the hormonal and physiological changes associated with puberty. Finally, despite FDR correction, the borderline associations resulting from multiple statistical tests should still be regarded as exploratory findings.
Future studies will be required to verify these findings using multiple complementary approaches, in accordance with MISEV guidelines, to validate further the biological characteristics and functional roles of large endothelial EVs. Subsequent research will optimize the antibody panel to reduce interference from platelet-derived vesicles, expand the sample size, establish healthy control groups, and adopt a more detailed classification of OSA severity. Multi-technique combined detection will also be adopted to improve the accuracy and credibility of extracellular vesicle analysis. Combined detection of large endothelial EVs along with inflammatory and oxidative stress-related biomarkers; assessment of dynamic changes in large endothelial EVs before and after surgery or positive pressure ventilation therapy.
Conclusion
In this single-center cross-sectional study of children with obstructive sleep apnea (OSA), large endothelial extracellular vesicles (particularly the CD31+CD41- subtype) were significantly associated with both the obstructive apnea-hypopnea index and sleep efficiency. These findings provide new insights into the involvement of endothelial cells in the pathophysiology of pediatric OSA. However, further controlled, longitudinal, and mechanistic studies are needed to determine whether CD31+CD41- large endothelial EVs can serve as biomarkers for tracking disease progression or evaluating the effects of interventions.
Abbreviations
OSA, obstructive sleep apnea; large endothelial EVs, large endothelial cell-derived extracellular vesicles; OAHI, obstructive apnea-hypopnea index; CIH, chronic intermittent hypoxia; PSG, polysomnography; mild OSA, mild OSA group; MS-OSA, moderate-to-severe OSA group; EDTA, ethylenediaminetetraacetic acid; PRP, platelet-rich plasma; PPP, platelet-poor plasma; EEG, electroencephalography; EOG, electrooculography; EMG, electromyography; TST, total sleep time; CAI, central apnea index; OAI, obstructive apnea index; AHI, apnea-hypopnea index; ODI, oxygen desaturation index; AASM, American Academy of Sleep Medicine; BMI, body mass index; REM, rapid eye movement; MAI, mixed apnea index; ROC, receiver operating characteristic; NO, nitric oxide; NREM, non-rapid eye movement; CPAP, continuous positive airway pressure; FDR, False Discovery Rate.
Data Sharing Statement
The clinical data supporting the findings of this study are derived from hospital medical records. The experimental data on large endothelial cell-derived extracellular vesicles were generated by flow cytometry analysis conducted by the authors. Due to patient privacy and confidentiality agreements, and in compliance with institutional ethical regulations, the raw datasets are not publicly available. However, anonymized data supporting the key results of this study may be made available to qualified researchers upon reasonable request, subject to review and approval by the corresponding author and the relevant institutional ethics committee.
Ethics Approval and Informed Consent
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Shenzhen Children’s Hospital (Approval No. 202309102). All parents and children signed the informed consent form.
Acknowledgments
We would like to express our sincere gratitude to all individuals and organizations who supported and assisted us throughout this research. In particular, we extend our thanks to Dr. Kaiping Wu for contributions in patient recruitment; Dr. Yaxin Xiao and Dr. Hairui Li for assistance in sleep monitoring and data analysis; and Dr. Zhijiang Hou for support in statistical methodology.
Author Contributions
Weinan Lin: Investigation, Writing – Review & Editing. Hezi Zhang: Investigation, Writing – Review & Editing. Lichao Cao: Methodology, Formal analysis, Investigation, Writing – Original Draft. Sihan Wang: Methodology, Formal analysis, Investigation, Writing – Original Draft. Yunfei Cui: Investigation. Ting Huang: Investigation, Data Curation. Tao Wu: Investigation. Xiao Huang: Investigation, Data Curation. Qinghua Lu: Investigation, Data Curation. Qin Yang: Conceptualization, Supervision, Project Administration, Writing – Review & Editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Natural Science Foundation of China (82300030), Guangdong High-level Hospital Construction Fund Clinical Research Project of Shenzhen Children’s Hospital (LCYJ2022097).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Mannarino MR, Di Filippo F, Pirro M. Obstructive sleep apnea syndrome. Eur J Intern Med. 2012;23(7):586–15. doi:10.1016/j.ejim.2012.05.013
2. Marcus CL, Brooks LJ, Draper KA, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(3):576–584. doi:10.1542/peds.2012-1671
3. Wasilewska J, Kaczmarski M. Obstructive sleep apnea-hypopnea syndrome in children. Wiadomosci Lek Wars Pol 1960. 2010;63(3):201–212.
4. Baker-Smith CM, Isaiah A, Melendres MC, et al. Sleep-disordered breathing and cardiovascular disease in children and adolescents: a scientific statement from the American heart association. J Am Heart Assoc. 2021;10(18):e022427. doi:10.1161/JAHA.121.022427
5. Yun CH, Jung KH, Chu K, et al. Increased circulating endothelial microparticles and carotid atherosclerosis in obstructive sleep apnea. J Clin Neurol Seoul Korea. 2010;6(2):89–98. doi:10.3988/jcn.2010.6.2.89
6. Kohler M, Stradling JR. Mechanisms of vascular damage in obstructive sleep apnea. Nat Rev Cardiol. 2010;7(12):677–685. doi:10.1038/nrcardio.2010.145
7. Welsh JA, Goberdhan DCI, O’Driscoll L, et al. Minimal information for studies of extracellular vesicles (MISEV2023): from basic to advanced approaches. J Extracell Vesicles. 2024;13(2):e12404. doi:10.1002/jev2.12404
8. Helbing T, Olivier C, Bode C, Moser M, Diehl P. Role of microparticles in endothelial dysfunction and arterial hypertension. World J Cardiol. 2014;6(11):1135–1139. doi:10.4330/wjc.v6.i11.1135
9. Amabile N, Guérin AP, Leroyer A, et al. Circulating endothelial microparticles are associated with vascular dysfunction in patients with end-stage renal failure. J Am Soc Nephrol JASN. 2005;16(11):3381–3388. doi:10.1681/ASN.2005050535
10. Sun XD, Han L, Lan HT, et al. Endothelial microparticle-associated protein disulfide isomerase increases platelet activation in diabetic coronary heart disease. Aging. 2021;13(14):18718–18739. doi:10.18632/aging.203316
11. Dursun I, Poyrazoglu HM, Gunduz Z, et al. The relationship between circulating endothelial microparticles and arterial stiffness and atherosclerosis in children with chronic kidney disease. Nephrol Dial Transplant off Publ Eur Dial Transpl Assoc Eur Ren Assoc. 2009;24(8):2511–2518.
12. Leite AR, Borges-Canha M, Cardoso R, Neves JS, Castro-Ferreira R, Leite-Moreira A. Novel biomarkers for evaluation of endothelial dysfunction. Angiology. 2020;71(5):397–410. doi:10.1177/0003319720903586
13. Amabile N, Heiss C, Chang V, et al. Increased CD62e(+) endothelial microparticle levels predict poor outcome in pulmonary hypertension patients. J Heart Lung Transplant off Publ Int Soc Heart Transplant. 2009;28(10):1081–1086. doi:10.1016/j.healun.2009.06.005
14. Pimentel Mota IC, Souza LV, Parizotto GP, et al. Imbalance between the circulating endothelium-derived apoptotic microparticles and the endothelial colony-forming units of progenitor cells in patients undergoing diagnostic coronary angiography. Adv Med Sci. 2021;66(2):396–402. doi:10.1016/j.advms.2021.07.011
15. Amabile N, Cheng S, Renard JM, et al. Association of circulating endothelial microparticles with cardiometabolic risk factors in the Framingham heart study. Eur Heart J. 2014;35(42):2972–2979. doi:10.1093/eurheartj/ehu153
16. Ni X. Guidelines for diagnosis and treatment of obstructive sleep apnea in children in China (2020). Chin J Evidence-Based Med. 2020;20(8):883–900.
17. Ehsan Z, Ishman SL, Soghier I, et al. Management of persistent, post-adenotonsillectomy obstructive sleep apnea in children: an official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2024;209(3):248–261. doi:10.1164/rccm.202310-1857ST
18. Kim J, Bhattacharjee R, Kheirandish-Gozal L, Spruyt K, Gozal D. Circulating microparticles in children with sleep disordered breathing. Chest. 2011;140(2):408–417. doi:10.1378/chest.10-2161
19. Berry RB, Brooks R, Gamaldo C, et al. AASM scoring manual updates for 2017 (Version 2.4). J Clin Sleep Med JCSM off Publ Am Acad Sleep Med. 2017;13(5):665–666.
20. Priou P, Gagnadoux F, Tesse A, et al. Endothelial dysfunction and circulating microparticles from patients with obstructive sleep apnea. Am J Pathol. 2010;177(2):974–983. doi:10.2353/ajpath.2010.091252
21. Šmon J, Kočar E, Pintar T, Dolenc-Grošelj L, Rozman D. Is obstructive sleep apnea a circadian rhythm disorder? J Sleep Res. 2023;32(4):e13875. doi:10.1111/jsr.13875
22. Brodsky SV, Satoskar A, Nadasdy T. Endothelial microparticles in transplant patients - great potential but a long way to go. Front Biosci Elite Ed. 2012;4(3):876–888. doi:10.2741/e426
23. Li B, Huang Q, Lin C, et al. Increased circulating CD31+/CD42b-EMPs in Perthes disease and inhibit HUVECs angiogenesis via endothelial dysfunction. Life Sci. 2021;265:118749. doi:10.1016/j.lfs.2020.118749
24. Dursun I, Yel S, Unsur E. Dynamics of circulating microparticles in chronic kidney disease and transplantation: is it really reliable marker? World J Transplant. 2015;5(4):267–275. doi:10.5500/wjt.v5.i4.267
25. Fernández-Bello I, Monzón Manzano E, García Río F, et al. Procoagulant state of sleep apnea depends on systemic inflammation and endothelial damage. Arch Bronconeumol. 2022;58(2):117–124. doi:10.1016/j.arbres.2020.11.017
26. Roldán V, Marín F, Lip GYH, Blann AD. Soluble E-selectin in cardiovascular disease and its risk factors. A review of the literature. Thromb Haemost. 2003;90(6):1007–1020. doi:10.1160/TH02-09-0083
27. Liu L, Kubes P. Molecular mechanisms of leukocyte recruitment: organ-specific mechanisms of action. Thromb Haemost. 2003;89(2):213–220. doi:10.1055/s-0037-1613434
28. Sun H, Du Y, Zhang L, et al. Increasing circulating ESM-1 and adhesion molecules are associated with earlystage atherosclerosis in OSA patients: A cross-sectional study. SLEEP Med. 2022;98:114–120. doi:10.1016/j.sleep.2022.06.015
29. Zhang J, Zhang S, Xu S, et al. Oxidative stress induces E-selectin expression through repression of endothelial transcription factor ERG. J Immunol. 2023;211(12):1835–1843. doi:10.4049/jimmunol.2300043
30. Zhang L, Antabi MA, Mattar J, et al. Circulating cytokine levels and 5-year vascular recurrence after stroke: a multicenter prospective cohort study. Eur Stroke J;2025. 23969873251360145. doi:10.1177/23969873251360145
31. Feng J, Zhang D, Chen B. Endothelial mechanisms of endothelial dysfunction in patients with obstructive sleep apnea. Sleep Breath Schlaf Atm. 2012;16(2):283–294. doi:10.1007/s11325-011-0519-8
32. Kheirandish-Gozal L, Khalyfa A, Gozal D, Bhattacharjee R, Wang Y. Endothelial dysfunction in children with obstructive sleep apnea is associated with epigenetic changes in the eNOS gene. Chest. 2013;143(4):971–977. doi:10.1378/chest.12-2026
33. Santos B, Ramalho B, Relógio A, Cavadas C, Gaspar LS, Álvaro AR. Systematic review of changes in extracellular vesicles associated with obstructive sleep apnoea: implications for diagnosis and treatment. Eur Respir Rev Off J Eur Respir Soc. 2025;34(178):250073. doi:10.1183/16000617.0073-2025
34. Kim J, Gozal D, Bhattacharjee R, Kheirandish-Gozal L. TREM-1 and pentraxin-3 plasma levels and their association with obstructive sleep apnea, obesity, and endothelial function in children. Sleep. 2013;36(6):923–931. doi:10.5665/sleep.2726
35. Jia L, Fan J, Cui W, et al. Endothelial cell-derived microparticles from patients with obstructive sleep apnea hypoxia syndrome and coronary artery disease increase aortic endothelial cell dysfunction. Cell Physiol Biochem Int J Exp Cell Physiol Biochem Pharmacol. 2017;43(6):2562–2570. doi:10.1159/000484508
36. Muñoz-Hernandez R, Vallejo-Vaz AJ, Sanchez Armengol A, et al. Obstructive sleep apnoea syndrome, endothelial function and markers of endothelialization. Changes after CPAP. PLoS One. 2015;10(3):e0122091. doi:10.1371/journal.pone.0122091
37. El Solh AA, Akinnusi ME, Baddoura FH, Mankowski CR. Endothelial cell apoptosis in obstructive sleep apnea: a link to endothelial dysfunction. Am J Respir Crit Care Med. 2007;175(11):1186–1191. doi:10.1164/rccm.200611-1598OC
38. Tual-Chalot S, Fatoumata K, Priou P, et al. Circulating microparticles from patients with obstructive sleep apnea enhance vascular contraction: mandatory role of the endothelium. Am J Pathol. 2012;181(4):1473–1482. doi:10.1016/j.ajpath.2012.06.020
39. Tual-Chalot S, Gagnadoux F, Trzepizur W, Priou P, Andriantsitohaina R, Martinez MC. Circulating microparticles from obstructive sleep apnea syndrome patients induce endothelin-mediated angiogenesis. Biochim Biophys Acta. 2014;1842(2):202–207. doi:10.1016/j.bbadis.2013.11.017
40. Ayers L, Ferry B, Craig S, Nicoll D, Stradling JR, Kohler M. Circulating cell-derived microparticles in patients with minimally symptomatic obstructive sleep apnoea. Eur Respir J. 2009;33(3):574–580. doi:10.1183/09031936.00107408
41. Ayers L, Stoewhas AC, Ferry B, Stradling J, Kohler M. Elevated levels of endothelial cell-derived microparticles following short-term withdrawal of continuous positive airway pressure in patients with obstructive sleep apnea: data from a randomized controlled trial. Respir Int Rev Thorac Dis. 2013;85(6):478–485.
42. Khalyfa A, Kheirandish-Gozal L, Khalyfa AA, et al. Circulating plasma extracellular microvesicle MicroRNA cargo and endothelial dysfunction in children with obstructive sleep apnea. Am J Respir Crit Care Med. 2016;194(9):1116–1126. doi:10.1164/rccm.201602-0323OC
43. Cheng JX, Ren J, Qiu J, et al. Rapid eye movement sleep and slow wave sleep rebounded and related factors during positive airway pressure therapy. Sci Rep. 2021;11(1):7599. doi:10.1038/s41598-021-87149-3
44. Shahveisi K, Jalali A, Moloudi MR, Moradi S, Maroufi A, Khazaie H. Sleep architecture in patients with primary snoring and obstructive sleep apnea. Basic Clin Neurosci. 2018;9(2):147–156. doi:10.29252/nirp.bcn.9.2.147
45. Zhang J, Jin X, Li R, Gao Y, Li J, Wang G. Influence of rapid eye movement sleep on all-cause mortality: a community-based cohort study. Aging. 2019;11(5):1580–1588. doi:10.18632/aging.101858
46. Chen PH, Chung CC, Liu SH, Kao YH, Chen YJ. Lithium treatment improves cardiac dysfunction in rats deprived of rapid eye movement sleep. Int J Mol Sci. 2022;23(19):11226. doi:10.3390/ijms231911226
47. Ben-Israel N, Tarasiuk A, Zigel Y. Obstructive apnea hypopnea index estimation by analysis of nocturnal snoring signals in adults. Sleep. 2012;35(9):1299–1305C. doi:10.5665/sleep.2092
48. Tang H, Hu Y, Deng J. Extracellular vesicles and hypertension. Adv Exp Med Biol. 2023;1418:69–80.
49. Massar SAA, Liu JCJ, Mohammad NB, Chee MWL. Poor habitual sleep efficiency is associated with increased cardiovascular and cortisol stress reactivity in men. Psychoneuroendocrinology. 2017;81:151–156. doi:10.1016/j.psyneuen.2017.04.013
50. Saputro RE, Chou CC, Lin YY, Tarumi T, Liao YH. Exercise-mediated modulation of autonomic nervous system and inflammatory response in sleep-deprived individuals: a narrative reviews of implications for cardiovascular health. Auton Neurosci Basic Clin. 2025;259:103256. doi:10.1016/j.autneu.2025.103256
51. Javaheri S, Javaheri S. Update on persistent excessive daytime sleepiness in OSA. Chest. 2020;158(2):776–786. doi:10.1016/j.chest.2020.02.036
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Characteristics of the Attentional Network in Children with Sleep-Disordered Breathing
Wu Y, Wang Y, Wang C, Zhao F, Ma D, Xu Z, Ni X
Nature and Science of Sleep 2023, 15:719-727
Published Date: 20 September 2023