")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Research Hotspots and Trends of Deep Learning in Critical Care Medicine: A Bibliometric and Visualized Study
Authors Zhang K , Fan Y , Long K, Lan Y, Gao P
Received 9 May 2023
Accepted for publication 25 July 2023
Published 29 July 2023 Volume 2023:16 Pages 2155—2166
DOI https://doi.org/10.2147/JMDH.S420709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kaichen Zhang,* Yihua Fan,* Kunlan Long, Ying Lan, Peiyang Gao
Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peiyang Gao, Email [email protected]
Background: Interest in the application of deep learning (DL) in critical care medicine (CCM) is growing rapidly. However, comprehensive bibliometric research that analyze and measure the global literature is still lacking.
Objective: The present study aimed to systematically evaluate the research hotspots and trends of DL in CCM worldwide based on the output of publications, cooperative relationships of research, citations, and the co-occurrence of keywords.
Methods: A total of 1708 articles in all were obtained from Web of Science. Bibliometric analysis was performed by Bibliometrix package in R software (4.2.2), Microsoft Excel 2019, VOSviewer (1.6.18), and CiteSpace (5.8.R3).
Results: The annual publications increased steeply in the past five years, accounting for 95.67% (1634/1708) of all the included literature. China and USA contributed to approximately 71.66% (1244/1708) of all publications. Seven of the top ten most productive organizations rank in the top 100 universities globally. Hot spots in research on the application of DL in CCM have focused on classifying disease phenotypes, predicting early signs of clinical deterioration, and forecasting disease progression, prognosis, and death. Convolutional neural networks, long and short-term memory networks, recurrent neural networks, transformer models, and attention mechanisms were all commonly used DL technologies.
Conclusion: Hot spots in research on the application of DL in CCM have focused on classifying disease phenotypes, predicting early signs of clinical deterioration, and forecasting disease progression, prognosis, and death. Extensive collaborative research to improve the maturity and robustness of the model remains necessary to make DL-based model applications sufficiently compelling for conventional CCM practice.
Keywords: hotspots, trends, deep learning, critical care medicine
Introduction
Deep learning (DL) is a subset of machine learning (ML) that is created using complex algorithms that are inspired by the organization of the human brain with many discrete nodes or ‘neurons’ and can identify important patterns or features in a dataset.1 DL and ML refer to two different technologies, and DL is considered an advanced structure of ML. Convolutional neural networks, long and short-term memory networks, recurrent neural networks, transformer models, and attention mechanisms are all common u DL technologies.2 ML techniques are a collection of mathematical and statistical concepts such as support vector machine, random forest, and K-nearest neighbors.3 Whereas DL algorithms are specialized techniques that are a subset of ML.1 The most important difference between the two approaches is that ML requires a feature engineering process that eliminates unnecessary variables and pre-selects only those that will be used for learning.4 This process is disadvantaged by the requirement that experienced professionals pre-select critical variables. Conversely, DL algorithms overcomes this shortfall by a process in which have built-in mechanisms for assessing and addressing the root of any inaccuracies and do not require guidance.4 To “interpret” an image, for example, to deconstruct the image into specific features, such as brightness, curvature, sharpness, etc., the extraction process of the support vector machine, a ML technique, requires digital input into the computer algorithms to extract these image features.5 Whereas this feature extraction process is completely different in DL algorithms. By varying the weights of the given features, DL applies a series of convolutional filters to the image, and the DL algorithm can then be trained to recognize a specific type of image and ultimately achieve the extraction of features from the image.6
Patients in the critical care medicine (CCM) field usually have aggressive and complex conditions, complicated medical record data, and clear trends in personalized treatment, resulting in a huge need for automated and reliable health information processing and analysis.7 DL algorithms and models enable machines to mimic human activities such as seeing, hearing, and thinking, helping to solve many complex pattern recognition challenges, and such features seem to help bring breakthroughs to the CCM. In addition to its well-known use in image processing and analysis, DL is also widely used in the medical field for health-record analysis, clinical diagnosis, health monitoring, personalized medicine, and drug development.7 Managing most diseases in the field of CCM, such as sepsis, acute respiratory distress syndrome, and severe stroke, largely requires the application of DL technologies.8–10 Currently, various algorithms and models based on DL have been widely used in the management of common diseases in CCM (such as sepsis and acute respiratory distress syndrome), including early detection of diseases, severity score estimation, facilitating ICU liberation through early successful extubation, early mobility, and survival prediction.11–15 Accumulating evidence suggests that the application of DL technology promotes intelligence in CCM, not only effectively improving the quality of medical care, but also helping to increase the efficiency of clinicians.16
Publications on the application of DL in CCM have continued to grow in recent years. The continuous increase in publications is positive for the updating of knowledge, but it also poses a challenge for researchers, as the process of acquiring knowledge makes it difficult to avoid the heavy work of combing publications.17 As a quantitative research method used to analyze the scholarly characteristics of the literature in certain scientific fields, bibliometrics helps researchers to grasp research hotspots and trends in their fields of interest and to predict their prospects.18 Therefore, the present bibliometric and visualized study was performed to provide a comprehensive overview of current hotspots, future trends in the use of DL in CCM, to showcase the contributions of leading countries, authorities, and prominent scholars, and to provide clues to potential future collaborations and research directions.
Materials and Methods
Search Strategy
Data were obtained from the Web of Science on 15 March, 2023 using the followed strategy: TS=(critical care OR critically ill OR intensive care OR ICU OR high dependency) AND TS=(deep learning OR convolutional neural network). It should be noted that TS=Topic. The inclusion criteria were as follows: (a) literature published between 2012 and 2022; (b) articles as the type of literature; and (c) literature published in English. Duplicate publications were excluded. A manual check of the included literature was independently performed by two authors (clinicians).
Data Acquisition
Full records and cited references of the obtained publications were downloaded in BibTex or txt formats for further analysis. Information on the publications, including title, abstract, key words, country, author, institution, source, count of citations, cited references, and the 2021 IF of the top 10 core journals as well as the H-index of the top 10 most productive authors were recorded. Data extraction were conducted by two independent authors.
Bibliometric Analysis
Bibliometric analysis was performed by Bibliometrix package in R software (4.2.2), Microsoft Excel 2019, VOSviewer (1.6.18), and CiteSpace (5.8.R3). In the present study, publication trends in the literature were analyzed using Microsoft Excel 2019. A polynomial-fitting curve in Microsoft Excel 2019 was applied to predict the number of future publications. The National collaborative networks, author collaborative networks, institutional collaborative networks, and journal publication trends were constructed using Bibliometrix package. Furthermore, co-occurrence of keywords and co-citation relationship of references were analyzed using VOSviewer. Finally, using CiteSpace to analyze keyword bursts.
Results
Annual Growth Trend
A total of 1708 articles on DL in CCM were published in the past 11 years. Overall, there was an overall upward trend in the number of publications (Figure 1A), with 3 in 2012 to 651 in 2022. Notably, research activity peaked in 2017, where 95.67% (1634/1708) articles were published during the past six years.
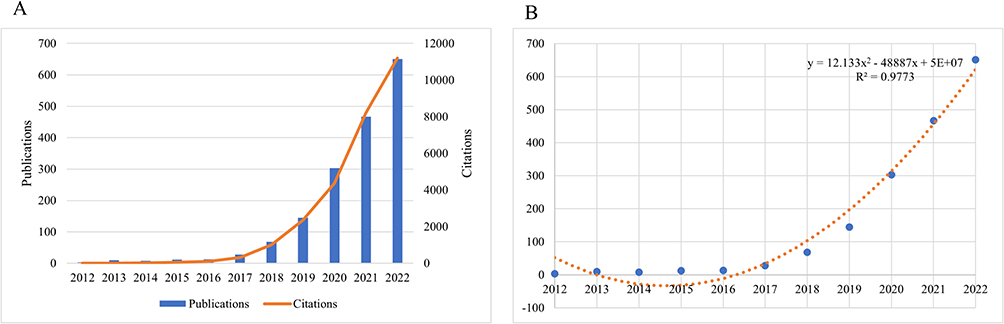 |
Figure 1 (A) The number of publications and annual citations over time. (B) Curve fitting of the e total annual growth trend of publications (R2 = 0.9773). |
Furthermore, the polynomial-fitting curve suggested that research in this area will continue to grow, with an R2 value of 0.9773 (Figure 1B).
Distribution of Countries/Regions
Publications on this topic were contributed by 62 different countries/regions. Table 1 shows the top ten most productive countries/regions. China ranked first with 804 publications, followed by the USA with 420 publications. USA had the highest number of total citations and average citations of all publications. Furthermore, China maintained close ties with USA, Korea, and France, whereas USA had strong cooperative bonds with China, England, and Australia (Figure 2).
 |
Table 1 The Top 10 Publishing Countries/Regions |
 |
Figure 2 The international collaboration between countries/regions. Notes: The different colors of arcs represent different countries/regions, and the larger the arc area, the wider the international cooperation of the country/region. Line thickness between countries/regions reflects the intensity of the closeness. |
Distribution of Affiliations
For the analysis of institutions, 2379 institutions made contributions to this field. The top ten most productive institutions were Chinese Academy of Sciences, Harvard University, University of Chinese, Academy of Sciences, University of California System, Wuhan University, Harvard Medical School, Tsinghua University, Centre National De La Recherche Scientifique CNRS, Shanghai Jiao Tong University, and Harbin Institute of Technology (Table 2). Notably, the top 10 institutions were from the China (n = 6), USA (n = 3), and France (n = 1). Furthermore, University of Chinese Academy of Sciences, Harvard University, and Tsinghua University have more connections to other affiliations (Figure 3).
 |
Table 2 The Top 10 Publishing Affiliations |
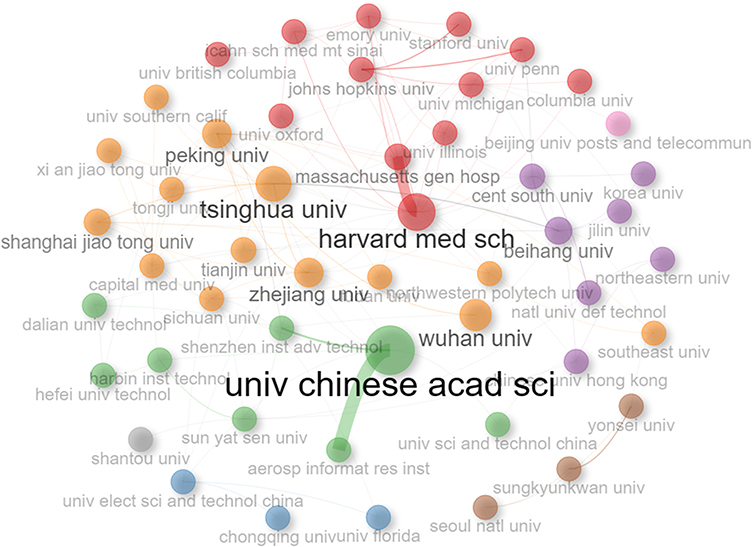 |
Figure 3 Collaboration between affiliations. Notes: Each circle represents an affiliation, and the larger the circle, the wider the cooperative relationship. Affiliations with frequent cooperative relationships are clustered into plates of the same color. Line thickness between affiliations reflects the intensity of the closeness. |
Analysis of Authors
Over the last ten years, a total of 6211 authors have made significant contributions to the field. Based on publication counts, Wang Y was the most productive author (n = 37), followed by Liu Y, Li Y, Wang J, Wang L, Zhang J, Zhang Y, Li L, Liu J, and Yang Y (Table 3). Furthermore, Zhang Y with the highest total citations and average citations, whereas Li Y has the highest H-index. Interestingly, the top ten most productive authors are all from China. These findings agree with the total productions for the nations mentioned above, showing that China is leading the way in this area. In addition, Wang Y, Wang X, Wang J and Zhang Y have more connections to other authors (Figure 4).
 |
Table 3 The Top 10 Publishing Authors |
 |
Figure 4 Collaboration between authors. Notes: Each circle represents an author, and the larger the circle, the wider the cooperative relationship. Authors with frequent cooperative relationships are clustered into plates of the same colour. Line thickness between authors reflects the intensity of the closeness. |
Analysis of Journals
A total of 260 journals have made contributions to this field. As shown in Table 4, IEEE Access, Scientific Reports, Remote Sensing were the top three. When it came to journal impact, IEEE Transactions on Geoscience and Remote Sensing ranked first, with an IF of 8.125, followed by Journal of Biomedical Informatics (IF = 8.000), and Computers in Biology and Medicine (IF = 6.698). These journals were therefore valuable resources for research in this field. Additionally, over the last five years, the top five most active journals have displayed a sharp rise in the number of annual publications (Figure 5).
 |
Table 4 The Top 10 Most Active Journals |
 |
Figure 5 Publications of the top 5 most active journals over time. |
Analysis of Co-Cited References
A total of 59,659 co-cited references were identified. After setting the minimum number of citations to 30, 52 of them were selected to form the cited reference network, which contained four clusters (Figure 6). Cluster 1 (in red) primarily centered on the model development and validation, cluster 2 (in green) primarily centered on the application of the models, cluster 3 (in blue) and cluster 4 (in yellow) primarily centered on the application of models in the medical field. These results suggest that DL-based model development and applications are the foundation of current research in this area. All literature included in Figure 6 is provided in Supplementary Material 1.
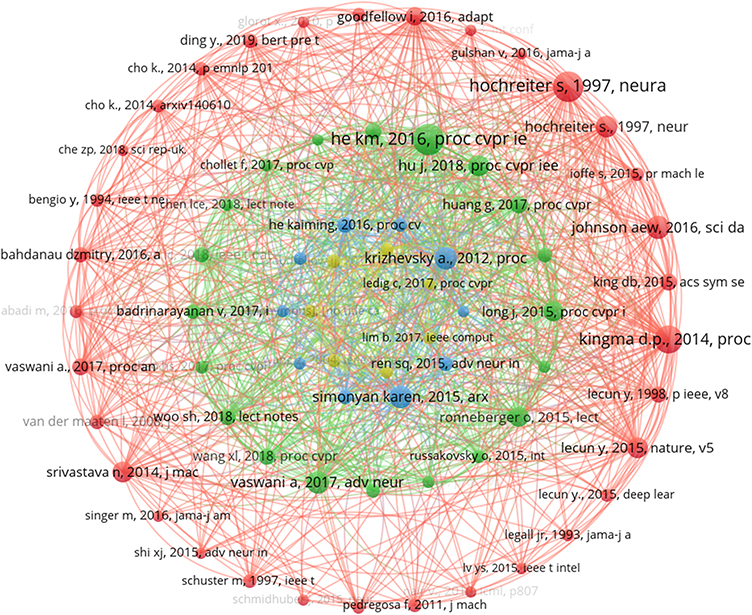 |
Figure 6 Network visualization map of co-citation references. Notes: Cluster 1 (in red), cluster 2 (in green), cluster 3 (in blue), cluster 4 (in yellow). The lines between the circles represent the co-citation relationship. The thickness and number of connections between the nodes indicate the strength of links between references. |
Analysis of Hotspots and Trends in Research
A total of 4864 keywords were identified. “Deep learning”, “machine learning”, and “feature extraction” were the keywords with the highest frequency (Figure 7A). After setting the minimum number of occurrences to ten, 84 of them were selected to form the keyword network, which contained six clusters (Figure 7A). Cluster 1 (in red) primarily centered on the model development and validation, cluster 2 (in green) and cluster 4 (in yellow) primarily centered on the extraction of clinical characteristics of critically ill patients, cluster 3 (in blue) primarily centered on the prognosis of critically ill patients, cluster 5 (in purple) primarily centered on monitoring changes in the condition of critically ill patients; and cluster 6 (in light blue) primarily centered on big data analysis in CCM. It was worth noting that “adaptation models”, “computed tomography”, and “electronic medical records” were recent emerging hot topics (Figure 7B). These topics offer potential research directions on DL in CCM for the future.
 |
Figure 7 (A) Network map of keywords on DL in CCM. (B) Visualization map of top 15 keywords with the strongest citation bursts. Notes: Cluster 1 (in red), cluster 2 (in green), cluster 3 (in blue), cluster 4, cluster 5 (in purple), cluster 6 (in light blue). The node size reflects the co-occurrence frequencies and the link indicates the co-occurrence relationship. The thickness of the link is proportional to the number of times two keywords co-occur. The blue bars indicate that the keywords have been published and the red bars indicate citation burstness. |
Discussion
The present study used a bibliometric approach to analyze publications of DL in CCM by exploring the expansion of research interest, publication output, top nations, international cooperation, top institutions, authoritative scholars, preferred journals, keywords, and citation analysis.
Publications on DL in CCM have grown steadily in recent years since the concept of DL was introduced in 2006.19 In 2018, there was a significant increase in interest in DL in CCM, which marked the turning point. Interest in DL in general medicine has been gradually increasing since 2012, but in the field of CCM, it was significantly delayed by six years.20 Indeed, the DL models are not commonly used in CCM daily practice. The reason is that few models have external validation, clinical interpretability and high predictability.21,22 Furthermore, most models are developed in a single institution and are do not perform well when applied to other institutions.23 There are also limited venues to incorporate the models. Ideally, they would be embedded in electronic health record systems, but this is challenging to implement due to the limitations of these systems and the corporate disincentives to do so.24,25 In addition, privacy issues are also one of the challenges faced by the adoption of artificial intelligence in the medical field.26 Based on the above evidence, we therefore believe that the safety and accountability of DL models applied to critically ill patients has not yet fully gained gain enough trust from the people. Since 2016, with the continuous development of DL technologies and the development of DL models that begin to pay attention to multi-center data sources and external validation, the accuracy and clinical adaptability of the models have been strengthened, which may help to establish patient confidence in the DL model.27,28 The emergence of new DL technologies, such as convolutional neural networks, long and short-term memory networks, recurrent neural networks, transformer models, and attention mechanisms, offers previously unheard-of possibilities for disease management, diagnosis, and prediction. In addition, MIMIC and eICU, two large public intensive care databases launched in 2016 and 2018, respectively, became available to researchers.29,30 Especially, the release of the MIMIC III database was a large contributing factor to the development of DL models in CCM. Types of DL models developed based on MIMIC III typically include diagnostic models, disease severity score models, real-time monitoring models, hospital length of stay prediction models, readmission prediction models, survival prediction models, and automated adverse drug reaction reporting models.12,15,31–35 Common conditions in the field of CCM that these DL models are applied to manage include sepsis, acute respiratory distress syndrome, acute kidney injury, and cardiovascular disease.31–35 The common variables used in these models can be divided into 4 categories: history information, admission information, vital signs, laboratory results, and arterial blood gas analysis.15 However, MIMIC-III is only an extensive single-center database spanning from 2001 to 2012 of electronic medical records of patients admitted to the ICU at Beth Israel Deaconess Medical Center, an academic teaching hospital of Harvard Medical School in Boston, USA.36 Therefore, the establishment of a continuously updated CCM database of multicenter admitted ICU patient data, or even electronic medical records of ICU patients admitted globally, would be more conducive to the promotion of the field of CCM as well as the application of DL models.
It was discovered that high-income nations predominate in DL research on CCM after analyzing the distribution of publications across nations. Notably, the top 30 countries in the world in terms of GDP include these ten most productive countries, suggesting that the number of publications is closely linked to the economic power of each country. This finding is consistent with the bibliometric findings of many other medical disciplines.37–39 Furthermore, over 70% of the publications came from the USA and China, indicating that these two nations are the main contributors to the DL in CCM research. Additionally, the highest citation rates are also found in these two nations, though China has a lower average citation rate per article than the USA. Analysis of collaborative networks showed that the USA and China are the countries with the most collaborative network relationships. A stable and adaptable policy is a prerequisite to ensure that international collaborations are successfully achieved. Adequate research funding, a wide range of research collaborators, as well as a significant proportion of visiting scholars all contribute to improved international partnerships. Furthermore, the top 100 universities in the world include seven of the top ten most productive institutions, indicating that the use of DL in CCM has gained the attention of leading universities. Researchers may be encouraged to consider conducting conjoint research or applying for educational programs or visiting scholars with these top institutions in the USA or China.
Notably, current articles on this topic are not in the top-tier clinical journals in this space, such as Critical Care Medicine, JAMA, or the New England Journal. It is likely due to the fact that there is still a gap between the DL models and clinical applicability. It needs to be acknowledged that DL has the advantage of responding to the challenges faced by CCM. DL algorithms and models enable machines to mimic human activities such as vision, hearing, and thinking and can automate and reliably process and analyze health information.7 Therefore, various algorithms and models based on DL have been widely used in the management of common diseases in CCM, including early detection of diseases, severity score estimation, facilitating ICU liberation through early successful extubation, early mobility, and survival prediction.11–15 Accumulating evidence suggests that the application of DL technology promotes intelligence in CCM, not only effectively improving the quality of medical care, but also helping to increase the efficiency of clinicians.16 DL implementation will support clinicians in the decision-making processes. Benefits comprehend earlier diagnoses, detection of subclinical deteriorations and generation of new medical knowledge.7 To improve the clinical utility of DL models in CCM, the following challenges need to be addressed. First, DL models that lack external validation automatically move away from clinical applicability. It should be advocated that researchers should develop external validation from a multidimensional perspective to continuously improve the scientific validity of the model and enhance the predictive performance, which in turn will promote the clinical interpretability and applicability of DL models in the CMM field.21 Models developed in a single institution are not always applicable to other institutions. Therefore, constructing models based on multicenter shared data should be advocated to increase the breadth of their applicability.23 If achievable, the creation of a global shared database of electronic medical records in the field of CCM is expected to bring a major breakthrough in this area.36 Furthermore, privacy protection through policies remains the cornerstone of health data, with the addition of special safeguards for personal health data addressed by the new innovative principles of the General Data Protection Regulation.40
Based on the authors keywords in the identified categories, CCM-related DL research mainly focused on the model development and validation, the extraction of clinical characteristics of critically ill patients, the prognosis of critically ill patients, monitoring changes in the condition of critically ill patients, and big data analysis in CCM. Furthermore, the primary disease domains addressed in CCM-related DL research were COVID-19, ARDS, sepsis, cardiac arrest, and acute kidney injury. The common targets of DL algorithms are these common diseases in CCM. It was worth noting that “adaptation models”, “computed tomography”, and “electronic medical records” were recent emerging hot topics. These topics offer potential research directions on DL in CCM for the future. DL has demonstrated potential applications in various areas of CCM. However, the development and implementation of DL in CCM remains challenging. Firstly, the absence of external validation and prospective assessment to confirm the repeatability of DL protocols both limit the utility of DL in clinical practice.41 Secondly, implementing artificial intelligence models in clinical practice may entail high initial costs, which is a significant barrier to implementing artificial intelligence (AI) in low- and middle-income countries.42 Furthermore, the World Health Organization released guidelines on the ethics and management of AI for health in 2021, emphasizing the key role of privacy, transparency, informed consent, and regulation of data protection frameworks.43 Thus, the legal protection of patient privacy also limits the current widespread use of AI in medicine.42
The application of AI is beneficial for the advancement of medicine.44,45 This study provides a systematic review of hot spots and trends in CCM-related DL research, highlights leading countries and institutions, reveals potential partnership networks, and provides insights into the direction of future research. However, limitations should be acknowledged. The COVID-19 pandemic has impacted various industries around the world, including the DL field and the CCM field. From the outset of the COVID-19 pandemic, it was clear that the greatest challenge was the unavailability of fully equipped and staffed ICU beds.46 With the expansion of the Internet, the amount of content on COVID-19 has exploded in the last three years. In addition to fact-based content, a large amount of COVID-19 content is being manipulated, and it leads to people spending more time online and getting more invested in this false content.47 Potentially preventing its spread by using DL to identify uninformative information early has also raised concerns.47 Therefore, the COVID-19 pandemic may introduce a publication bias to the publication trend of CCM-related DL research, which may lead to unstable research hotspots and trends identified in this study. Furthermore, given that our search strategy was constructed based on Topic, the search strategy used in the present study may have resulted in missing some relevant literature.
Conclusion
Hot spots in research on the application of DL in CCM have focused on classifying disease phenotypes, predicting early signs of clinical deterioration, and forecasting disease progression, prognosis, and death. Extensive collaborative research to improve the maturity and robustness of the model remains necessary to make DL-based model applications sufficiently compelling for conventional CCM practice.
Funding
This work was supported by Science and Technology Development Fund of Hospital of Chengdu University of Traditional Chinese Medicine (No.21ZL08).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Krizhevsky A, Sutskever I, Hinton GE. Imagenet classification with deep convolutional neural networks. Commun ACM. 2017;60:84–90. doi:10.1145/3065386
2. Girshick R, Donahue J, Darrell T, Malik J. Rich feature hierarchies for accurate object detection and semantic segmentation.
3. Goecks J, Jalili V, Heiser LM, Gray JW. How machine learning will transform biomedicine. Cell. 2020;181(1):92–101. doi:10.1016/j.cell.2020.03.022
4. Shinde P, Shah S. A review of machine learning and deep learning applications; 2019.
5. Irisson JO, Ayata SD, Lindsay DJ, Karp-Boss L, Stemmann L. Machine learning for the study of plankton and marine snow from images. Ann Rev Mar Sci. 2022;14:277–301. doi:10.1146/annurev-marine-041921-013023
6. Wang S, Yang DM, Rong R, Zhan X, Xiao G. Pathology image analysis using segmentation deep learning algorithms. Am J Pathol. 2019;189(9):1686–1698. doi:10.1016/j.ajpath.2019.05.007
7. Egger J, Gsaxner C, Pepe A, et al. Medical deep learning-A systematic meta-review. Comput Methods Programs Biomed. 2022;221:106874. doi:10.1016/j.cmpb.2022.106874
8. Zhang Z, Pan Q, Ge H, Xing L, Hong Y, Chen P. Deep learning-based clustering robustly identified two classes of sepsis with both prognostic and predictive values. EBioMedicine. 2020;62:103081. doi:10.1016/j.ebiom.2020.103081
9. Reamaroon N, Sjoding MW, Gryak J, Athey BD, Najarian K, Derksen H. Automated detection of acute respiratory distress syndrome from chest X-rays using directionality measure and deep learning features. Comput Biol Med. 2021;134:104463. doi:10.1016/j.compbiomed.2021.104463
10. Sharma N, Simmons LH, Jones PS, et al. Motor imagery after subcortical stroke: a functional magnetic resonance imaging study. Stroke. 2009;40(4):1315–1324. doi:10.1161/STROKEAHA.108.525766
11. Lauritsen SM, Kalør ME, Kongsgaard EL, et al. Early detection of sepsis utilizing deep learning on electronic health record event sequences. Artif Intell Med. 2020;104:101820. doi:10.1016/j.artmed.2020.101820
12. Aşuroğlu T, Oğul H. A deep learning approach for sepsis monitoring via severity score estimation. Comput Methods Programs Biomed. 2021;198:105816. doi:10.1016/j.cmpb.2020.105816
13. Jia Y, Kaul C, Lawton T, Murray-Smith R, Habli I. Prediction of weaning from mechanical ventilation using convolutional neural networks. Artif Intell Med. 2021;117:102087. doi:10.1016/j.artmed.2021.102087
14. Yeung S, Rinaldo F, Jopling J, et al. A computer vision system for deep learning-based detection of patient mobilization activities in the ICU. NPJ Digit Med. 2019;2:11. doi:10.1038/s41746-019-0087-z
15. Tang H, Jin Z, Deng J, et al. Development and validation of a deep learning model to predict the survival of patients in ICU. J Am Med Inform Assoc. 2022;29(9):1567–1576. doi:10.1093/jamia/ocac098
16. Datta R, Singh S. Artificial intelligence in critical care: its about time! Med J Armed Forces India. 2021;77(3):266–275. doi:10.1016/j.mjafi.2020.10.005
17. Danış F, Kudu E. The evolution of cardiopulmonary resuscitation: global productivity and publication trends. Am J Emerg Med. 2022;54:151–164. doi:10.1016/j.ajem.2022.01.071
18. Niu B, Hong S, Yuan J, Peng S, Wang Z, Zhang X. Global trends in sediment-related research in earth science during 1992–2011: a bibliometric analysis. Scientometrics. 2013;98(1):511–529. doi:10.1007/s11192-013-1065-x
19. LeCun Y, Bengio Y, Hinton G. Deep learning. Nature. 2015;521:436–444. doi:10.1038/nature14539
20. Guo Y, Hao Z, Zhao S, Gong J, Yang F. Artificial intelligence in health care: bibliometric analysis. J Med Internet Res. 2020;22(7):e18228. doi:10.2196/18228
21. Ozrazgat-Baslanti T, Loftus TJ, Ren Y, Ruppert MM, Bihorac A. Advances in artificial intelligence and deep learning systems in ICU-related acute kidney injury. Curr Opin Crit Care. 2021;27(6):560–572. doi:10.1097/MCC.0000000000000887
22. Ching T, Himmelstein DS, Beaulieu-Jones BK, et al. Opportunities and obstacles for deep learning in biology and medicine. J R Soc Interface. 2018;15(141):20170387.
23. Miotto R, Wang F, Wang S, Jiang X, Dudley JT. Deep learning for healthcare: review, opportunities and challenges. Brief Bioinform. 2018;19(6):1236–1246. doi:10.1093/bib/bbx044
24. Wang L, Tong L, Davis D, Arnold T, Esposito T. The application of unsupervised deep learning in predictive models using electronic health records. BMC Med Res Methodol. 2020;20(1):37. doi:10.1186/s12874-020-00923-1
25. Golas SB, Shibahara T, Agboola S, et al. A machine learning model to predict the risk of 30-day readmissions in patients with heart failure: a retrospective analysis of electronic medical records data. BMC Med Inform Decis Mak. 2018;18(1):44. doi:10.1186/s12911-018-0620-z
26. Harvey HB, Gowda V. Regulatory issues and challenges to artificial intelligence adoption. Radiol Clin North Am. 2021;59(6):1075–1083. doi:10.1016/j.rcl.2021.07.007
27. Zhong L, Dong D, Fang X, et al. A deep learning-based radiomic nomogram for prognosis and treatment decision in advanced nasopharyngeal carcinoma: a multicentre study. EBioMedicine. 2021;70:103522. doi:10.1016/j.ebiom.2021.103522
28. Hiremath A, Shiradkar R, Fu P, et al. An integrated nomogram combining deep learning, Prostate Imaging-Reporting and Data System (PI-RADS) scoring, and clinical variables for identification of clinically significant prostate cancer on biparametric MRI: a retrospective multicentre study. Lancet Digit Health. 2021;3(7):e445–e454. doi:10.1016/S2589-7500(21)00082-0
29. Pollard TJ, Johnson AE, Raffa JD, Celi LA, Mark RG, Badawi O. The eICU collaborative research database, a freely available multi-center database for critical care research. Sci Data. 2018;5:180178. doi:10.1038/sdata.2018.178
30. Johnson AE, Pollard TJ, Shen L, et al. MIMIC-III, a freely accessible critical care database. Sci Data. 2016;3:160035. doi:10.1038/sdata.2016.35
31. Guo F, Zhu X, Wu Z, Zhu L, Wu J, Zhang F. Clinical applications of machine learning in the survival prediction and classification of sepsis: coagulation and heparin usage matter. J Transl Med. 2022;20(1):265. doi:10.1186/s12967-022-03469-6
32. Alfieri F, Ancona A, Tripepi G, et al. External validation of a deep-learning model to predict severe acute kidney injury based on urine output changes in critically ill patients. J Nephrol. 2022;35(8):2047–2056. doi:10.1007/s40620-022-01335-8
33. Wu J, Lin Y, Li P, Hu Y, Zhang L, Kong G. Predicting Prolonged Length of ICU stay through machine learning. Diagnostics. 2021;11(12):2242. doi:10.3390/diagnostics11122242
34. Pishgar M, Theis J, Del Rios M, Ardati A, Anahideh H, Darabi H. Prediction of unplanned 30-day readmission for ICU patients with heart failure. BMC Med Inform Decis Mak. 2022;22(1):117. doi:10.1186/s12911-022-01857-y
35. McMaster C, Chan J, Liew DFL, et al. Developing a deep learning natural language processing algorithm for automated reporting of adverse drug reactions. J Biomed Inform. 2023;137:104265. doi:10.1016/j.jbi.2022.104265
36. Röösli E, Bozkurt S, Hernandez-Boussard T. Peeking into a black box, the fairness and generalizability of a MIMIC-III benchmarking model. Sci Data. 2022;9(1):24. doi:10.1038/s41597-021-01110-7
37. Qiang W, Xiao C, Li Z, et al. Impactful publications of critical care medicine research in China: a bibliometric analysis. Front Med. 2022;9:974025. doi:10.3389/fmed.2022.974025
38. Liu YX, Zhu C, Wu ZX, Lu LJ, Yu YT. A bibliometric analysis of the application of artificial intelligence to advance individualized diagnosis and treatment of critical illness. Ann Transl Med. 2022;10(16):854. doi:10.21037/atm-22-913
39. Cui X, Chang Y, Yang C, Cong Z, Wang B, Leng Y. Development and trends in artificial intelligence in critical care medicine: a bibliometric analysis of related research over the period of 2010–2021. J Pers Med. 2022;13(1):50. doi:10.3390/jpm13010050
40. Castelluccia Claude, le Me´tayer Daniel, European Parliament. European Parliamentary Research Service. Scientific foresight unit. Understanding algorithmic decision-making: opportunities and challenges; 2019. Available from: https://www.europarl.europa.eu/RegData/etudes/STUD/2019/624261/EPRS_STU.
41. Yoon JH, Pinsky MR, Clermont G. Artificial intelligence in critical care medicine. Crit Care. 2022;26(1):75. doi:10.1186/s13054-022-03915-3
42. Caruso PF, Greco M, Ebm C, Angelotti G, Cecconi M. Implementing artificial intelligence: assessing the cost and benefits of algorithmic decision-making in critical care. Crit Care Clin. 2023;6072(1):1–253.
43. Ethics and governance of artificial intelligence for health ethics and governance of artificial intelligence for health 2; 2021. Available from: http://apps.who.int/bookorders.
44. Wu Q, Liu S, Zhang R, et al. ACU&MOX-DATA: a platform for fusion analysis and visual display acupuncture multi-omics heterogeneous data. Acupunct Herbal Med. 2023;3(1):59–62. doi:10.1097/HM9.0000000000000051
45. Jiang C, Qu H. In-line spectroscopy combined with multivariate analysis methods for endpoint determination in column chromatographic adsorption processes for herbal medicine. Acupunct Herbal Med. 2022;2(4):253–260. doi:10.1097/HM9.0000000000000035
46. Arabi YM, Myatra SN, Lobo SM. Surging ICU during COVID-19 pandemic: an overview. Curr Opin Crit Care. 2022;28(6):638–644. doi:10.1097/MCC.0000000000001001
47. Machová K, Mach M, Porezaný M. Deep learning in the detection of disinformation about COVID-19 in online space. Sensors. 2022;22(23):9319. doi:10.3390/s22239319
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.