")
Back to Journals » Infection and Drug Resistance » Volume 16
Requiring Reconsideration of Differences of Aeromonas Infections Between Extra-Intestinal and Intestinal in Hospitalized Patients
Authors Zhang D , Li W, Hu X, Huang H, Zhang X
Received 13 October 2022
Accepted for publication 16 January 2023
Published 25 January 2023 Volume 2023:16 Pages 487—497
DOI https://doi.org/10.2147/IDR.S393347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Daiqin Zhang,* Wenting Li,* Xin Hu, Hongyu Huang, Xiaobing Zhang
Department of Laboratory Medicine, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaobing Zhang, Department of Laboratory Medicine, The First Affiliated Hospital of Chongqing Medical University, No. 1 Youyi Road, Yuzhong District, Chongqing, 400016, People’s Republic of China, Tel +86-15123967161, Fax +86-23-89012742, Email [email protected]
Purpose: The purpose of this study is to examine the variations between extra-intestinal and intestinal infections of Aeromonas in terms of strain types, risk factors, drug susceptibility results, and the distribution of drug resistance and virulence genes.
Patients and Methods: A total of 188 Aeromonas strains were identified to the species level using housekeeping genes (rpoD, gyrB, and gyrA). The risk factors for Aeromonas extra-intestinal and intestinal infection, as well as mortality, were retrospectively examined in this study. The broth microdilution method was used to investigate the antimicrobial susceptibility profiles. Touchdown polymerase chain reaction (PCR) assays and DNA sequencing were employed to confirm virulence and the presence of drug resistance genes.
Results: The housekeeping genes identified 188 strains into 7 species. Extra-intestinal isolates generally contained A. caviae and A. hydrophila, while intestinal were A. veronii (p=0.0001). Extra-intestinal infections (158/188) were the main type and accounted for 24/27 of all fatalities. Malignant tumors, hepatobiliary diseases, anemia, and hypoproteinemia were linked to infections. Poor results were associated with septic shock. Using the broth microdilution method, over 80% isolates were susceptible to most antimicrobials, except for ceftazidime (79.8%) and ceftriaxone (69.7%). Except for imipenem, intestinal strains were more susceptible to other medications than extra-intestinal. Using touch-down polymerase chain reaction testing and DNA sequencing, 6 strains, 31 strains, and a strain only had blaTEM, blaCphA, and blaVIM, respectively. Two Aeromonas hydrophila each possessed blaCphA+ blaCTXM-M-9, and blaCphA + blaCTX-M-1 + blaCTX-M-15-like + blaTEM; two Aeromonas caviae each possessed blaNDM + blaCTX-M-1 +blaCTX-M-15-like + blaTEM, and blaNDM + blaTEM. Thirty-four of the 42 strains mentioned above were isolated from extra-intestinal. Act, aexT, and ascF-G, were in intestinal more frequently, but alt, hlyA, ela, and lip were in extra-intestinal more frequently.
Conclusion: Aeromonas inside and outside intestinal differed in their clinical characteristics, drug susceptibility, drug resistance and virulence genes.
Keywords: intestinal and extra-intestinal infections, Aeromonas, risk factor, virulence
Introduction
Aeromonas is a gram-negative, facultative anaerobic oxidase positive bacillus that ranges in size from 0.3 to 1.0 µm.1 Intestinal infection is the most common type of infectious disease caused by Aeromonas,2 but it can also result in infections of wound, liver and gallbladder, necrotizing fasciitis, sepsis, and other infectious diseases.3 However, it is important to be aware that there have been more instances of extra-intestinal infections in recent years.4 As an opportunistic pathogen, Aeromonas is more likely to infect and kill patients with low immunity, including those with malignant tumors, hematological tumors, cirrhosis, diabetes, and other diseases.5–7 In 1986, Aeromonas separated from the vibrio family,8 which it had previously been a part of it. Since then, the group of bacteria known as Aeromonas has expanded. However, our capacity to identify them has been constrained by the use of common clinical microbe identification methods, including the VITEK2 Compact system, the VITEK MALDI-TOF system, and even 16S rRNA.2,9,10 For precise identification, housekeeping genes like rpoD and gyrB can be sequenced.11,12 It is also possible to use multilocus phylogenetic analysis (MLPA).3 Drug resistance in Aeromonas has been steadily rising in recent years as a result of the expanding use of antibiotics in both aquaculture and human healthcare.13
Exotoxin, extracellular protease, adhesion factor, and secretion system are the key components of Aeromonas’ virulence factors.14 This makes the harmful elements of this organism complicated and varied. Aeromonas is able to thwart the host’s immune system and spread infection thanks to a range of virulence factors.15
In this work, the characteristics of Aeromonas infection and mortality were examined. Comparing the virulence gene and drug susceptibility of intestinal isolates versus extra-intestinal isolates. A preliminary assessment of Aeromonas’ drug resistance mechanism was made.
Materials and Methods
Material
In the clinical microbiology database of the First Affiliated Hospital of Chongqing Medical University, a 3200-bed facility in southwest China, 188 strains of Aeromonas were gathered between January 2013 and September 2020. A total of 158 strains were obtained from patients with parenteral infection (39 strains in skin wound secretion, 28 strains in bile, 25 strains in pleural and peritoneal fluid, 24 strains in blood, 22 strains in urine, and 20 strains in others), while 30 strains were identified from patients with intestinal infection. The VITEK MALDI-TOF technology (bioMerieux, Marcy I ‘Etoile, France) was utilized by the microbiology lab to identify microorganisms. And 188 Aeromonas strains were kept at 80 °C in 15% glycerol.
Identification of Bacterial Strains
Housekeeping genes (rpoD, gyrB, and gyrA) sequencing were used to confirm the identity of all isolates. Primers were taken from prior publications.16–18 The primers used for amplification and sequencing of the housekeeping genes are listed in Table 1.
 |
Table 1 The Primers of Target Genes and PCR Conditions |
Data Collection and Definition
In this study, a retrospective analysis was conducted. Only the first episode was considered in patients with more than one positive Aeromonas culture. The electronic medical records mainly covered the following contents: characteristics of infection, diagnosis and treatment, auxiliary examination, and prognosis. Sepsis with persistent hypotension needing vasopressors to keep MAP 65 mm Hg and having a blood lactate level >2 mmol/L (18 mg/dL) despite sufficient volume resuscitation are clinical indicators of patients with septic shock.19 Hemoglobin below 13 g/dL in adult males and 12 g/dL in adult females was considered anemia.20 Serum albumin components were below 35 g, indicating hypoproteinemia.21 Serum potassium level <3.5 mmol/L was hypokalemia. Systemic steroid use was defined as oral or intravenous administration of at least 20 mg/day of a steroid (prednisone, hydrocortisone, methylprednisolone, or dexamethasone) within 1 month of infection.22 The result was death. The inappropriate antimicrobial therapy used improper drugs that are not susceptible to pathogens.
Drug Sensitivity Test
The microbroth dilution method was used to determine the antimicrobial susceptibility pattern of all isolates to some commonly used antimicrobial agents, including ciprofloxacin, levofloxacin, cefuroxime, ceftazidime, ceftriaxone, cefepime, aztreonam, imipenem, and meropenem. The breakpoints were interpreted according to the Clinical and Laboratory Standards Institute (CLSI) guidelines.23 Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as quality controls for antibiotic susceptibility tests.
Polymerase Chain Reaction (PCR) Amplification of Drug Resistance and Virulence Genes
Touchdown PCR assays and sequencing were used to validate the presence of the carbapenemase genes (blaCphA, blaKPC, blaIMP, blaVIM, blaNDM, and blaOXA-48-like), extended-spectrum beta-lactamase (ESBL) genes (blaCTX-M-1, blaCTX-M-9, blaCTX-M-15-like, blaSHV, and blaTEM), and Ampc (blaACC and blaFOX).24 A total of 12 virulence factor-encoding genes were also found using PCR, including act, ast, alt, aerA, hlyA, ela, gcaT, lip, lafA, fla, aexT, and ascF-G.25–27 The amplification primer sequences are listed in Table 1.
Statistical Analysis
The data were analyzed using SPSS statistical software (version 25.0, IBM). Pearson’s chi-square test or Fisher’s exact test was used to analyze the categorical variables. Student’s t-test or Mann–Whitney U-test was utilized for continuous variables. To assess independent risk factors for Aeromonas mortality, univariate analysis was used to evaluate the putative variables, and multivariate logistic regression analysis was carried out for statistically significant variables in univariate analysis. Odds ratios (OR) were calculated with 95% confidence interval (CI). P<0.05 was deemed to statistically significant. The positive PCR amplicons were sequenced by Sangon Biotech (Shanghai) Co., Ltd. (Shanghai, China). Using Seqman (DNAStar), the sequences were assembled, and the data were compared in the NCBI (http://www.ncbi.nlm.nih.gov) using BLAST.
Results
Identification of Bacteria
A total of 188 Aeromonas isolates were divided into 7 species based on the results of housekeeping genes. Aeromonas caviae (28.7%), Aeromonas hydrophila (26.1%), Aeromonas veronii (25%), and Aeromonas dhakensis (18.1%) were the four species of Aeromonas that were most common. Additionally, 2 isolates of Aeromonas jandaei, 1 isolate each of Aeromonas sobria and Aeromonas media were identified. Figure 1 depicts the spread of Aeromonas isolated from infections of the extra-intestinal and intestinal. Overall, intestinal isolates typically contained A. veronii (p=0.0001); and extra-intestinal isolates were mainly contained A. caviae and A. hydrophila (p=0.0001).
 |
Figure 1 Distribution of various Aeromonas that have been isolated in and outside of the intestinal. |
Characteristics of Infected Patients
A total of 188 patients with Aeromonas infection were found between 2013 and 2020. The patients were on average 53.9 years old, with a male-to-female ratio of 1.5 (114/74). Malignant neoplasms (solid tumors and hematologic malignancies), hepatobiliary diseases (posthepatitic cirrhosis and cholelithiasis), anemia, and hypoproteinemia were the most prevalent underlying illnesses among infected people (Table 2). Different comorbidities were seen in patients with infections both inside and outside the intestinal. Patients with age >80, hematological malignancies, and gastrointestinal diseases were more likely to have an intestine infection with Aeromonas.
 |
Table 2 Clinical Characteristics of Patients with Aeromonas Infection |
Twenty-seven individuals (14.4%) died from Aeromonas infection, 24 of whom had extra-intestinal infection. Hematological malignancies (P=0.006), cholelithiasis (P=0.028), septic shock (P=0.002), and surgical history within 6 months (P=0.011), were all risk factors for the nosocomial death of Aeromonas, according to a univariate analysis. Septic shock was the only independent risk factor for Aeromonas death (P=0.020), according to the multivariate logistic regression model’s results, which are displayed in Table 3. A connection between intestinal infection and death was not discovered. Most patients with intestinal infections had hematological malignancies, cholelithiasis, septic shock, chemoradiotherapy, systemic steroid use, and surgical history within 6 months (Table 4).
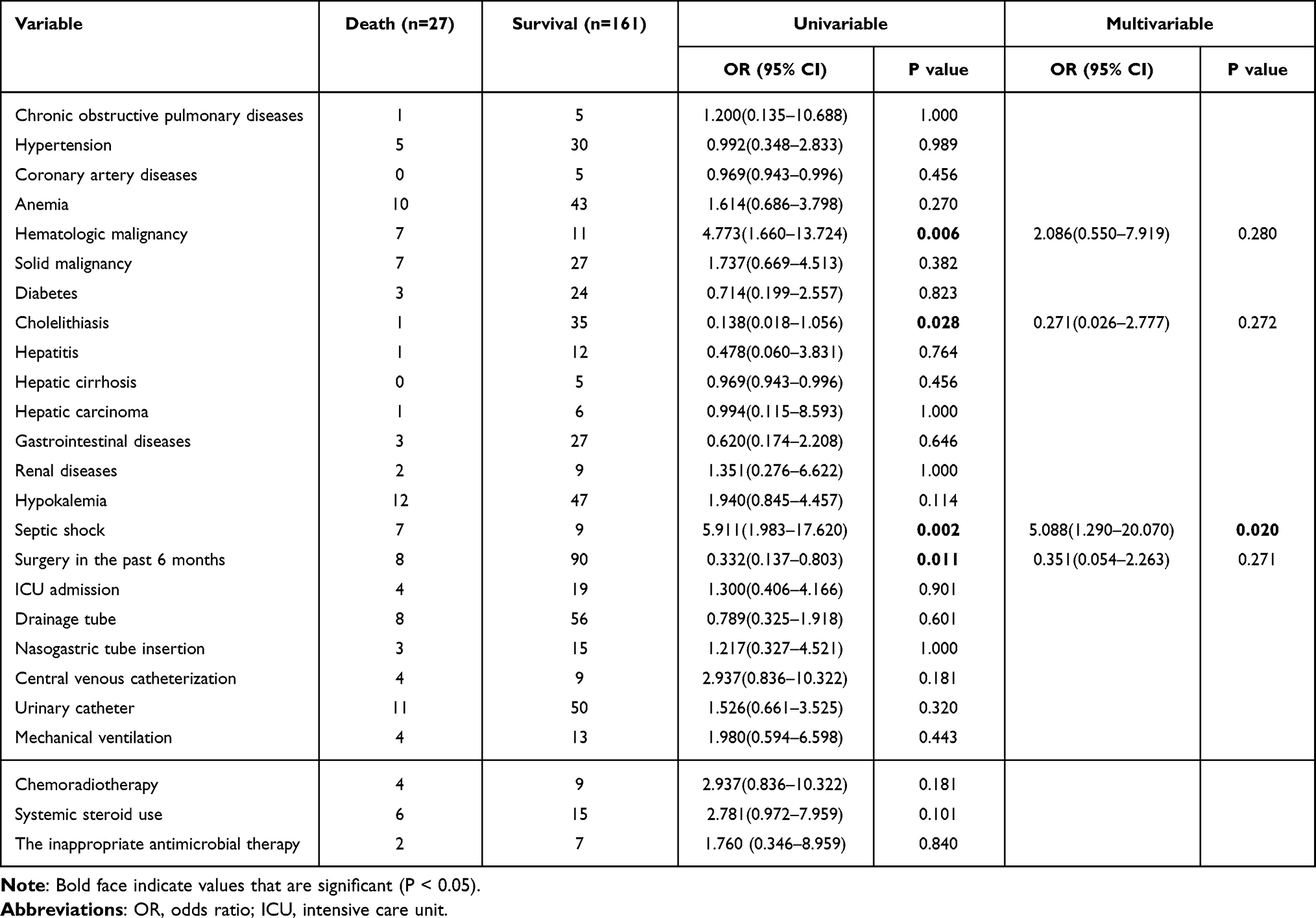 |
Table 3 Analysis of Risk Factors Associated with Hospital Death Caused by Aeromonas Infection |
 |
Table 4 Analysis of Risk Factors for Death from Intestinal and Extra-Intestinal Aeromonas Infection |
Drug Sensitivity
According to Table 5, which summarizes the results of the antimicrobial susceptibility tests, more than 83% of the bacterial strains were susceptible to ciprofloxacin (83.5%), levofloxacin (89.4%), cefepime (87.2%), aztreonam (86.2%), imipenem (87.2%), and meropenem (93.6%). Ceftazidime and ceftriaxone each had a 79.8% and a 69.7% sensitivity rate for Aeromonas, respectively.
 |
Table 5 Antimicrobial Susceptibilities of Aeromonas Isolates Determined by the Broth Microdilution Method and Aeromonas Isolates from Inside and Outside the Intestinal Were Compared for Drug Sensitivity |
With the exception of imipenem, intestinal infection strains were more susceptible to other medications than extra-intestinal infection strains, and ceftazidime, ceftriaxone, and ciprofloxacin all demonstrated statistically significant sensitivity. However, compared to intestinal strains, extra-intestinal strains had a considerably higher susceptibility to imipenem (Table 5).
Drug Resistance and Virulence Genes
By using PCR, it was discovered that 42 Aeromonas strains solely carried the ESBLs and carbapenemase genes: 6 strains only carried blaTEM; 31 strains only carried blaCphA, including A. dhakensis, A. veronii, A. hydrophila and A. jandaei; and one A. caviae with blaVIM. The remaining four Aeromonas strains possessed the following combinations of drug resistance genes: two A. hydrophila each had blaCphA + blaCTXM-M-9, and blaCphA + blaCTX-M-1 + blaCTX-M-15-like + blaTEM; two A. caviae each carried blaNDM + blaCTX-M-1 + blaCTX-M-15-like + blaTEM, and blaNDM + blaTEM. All of them were generated from extra-intestinal isolates, except for 7 strains with blaCphA, and one with blaVIM. 21 strains (63.64%) of the 33 strains with a positive CphA gene were discovered to be incompatible with the drug sensitivity of carbapenems. The ratios of act, ast, alt, aerA, hlyA, ela, lip, and gcaT were found to be 39.4%, 25.5%, 76.1%, 58%, 48.4%, 66%, 71.3%, and 88.3% respectively. Fla, lafA, aexT, and ascF-G were found in ratios of 72.3%, 21.8%, 20.2%, and 18.6%. The virulence genes act, aexT, and ascF-G were found in intestinal infection more frequently than extra-intestinal. Additionally, the detection rate of the virulence genes alt, hlyA, ela, and lip from extra-intestinal infection was considerably higher than that from intestinal infection (Table 6).
 |
Table 6 Intestinal and Extra-Intestinal Infections Caused by Aeromonas Were Compared in Terms of Their Virulence Genes |
Discussion
Aeromonas are easy to isolate; however, because of its heterogeneous phenotypic characteristics, species identification is difficult. In contrast to the use of the 16S rRNA gene and the VITEK MALDI-TOF method, nucleotide sequencing of housekeeping genes, such as rpoD and gyrB,6,28 or multilocus phylogenetic analysis (MLPA),3 can enable a more precise identification of the species.
Despite the fact that Aeromonas infections are primarily intestinal infections,29 there have been an increasing number of reports in recent years of extra-intestinal infections with Aeromonas.30,31 While Qu et al32 found that Aeromonas extra-intestinal infection primarily came from blood, Fu et al4 reported that skin and soft tissue infection was the primary cause of Aeromonas extra-intestinal infection. In this study, extra-intestinal infection was the primary type of Aeromonas infection, while skin wound infection was the primary extra-intestinal infection type. There were statistically different Aeromonas species isolated from different infection sites. A. veronii was the most prevalent species of intestinal infection in the paper, despite earlier research32 suggesting that A. dhakensis was most frequently found in patients with intestinal infection. This study and that of Chen et al33 are identical. In both cases, the extra-intestinal infections were mainly caused by A. caviae and A. hydrophila.
Similar to the findings of earlier studies,2,6 the work revealed that men made up the majority of those infected with Aeromonas, and it was noted that people in their middle and later years made up the majority of those infected, which may be related to their pre-existing illnesses and lowered immune systems.7 According to this study, the majority of patients with Aeromonas infection also had underlying illnesses like malignancies (solid tumors, hematological malignancies), hepatobiliary diseases (posthepatitic cirrhosis, cholelithiasis), anemia and hypoproteinemia. Su et al6 reported that patients with liver cirrhosis have significant morbidity and mortality from Aeromonas infection, which may be caused by abnormal performance of the mononuclear macrophage system in patients with liver cirrhosis, and a decrease in the body’s immune defense mechanism.
In contrast to the 14.9% to 63% described in the literature,5,34 the mortality rate with an Aeromonas infection (14.4%) was relatively low. According to Ji et al,5 the use of appropriate antimicrobial medicines, metastatic cancer and shock were linked to Aeromonas mortality (P<0.05). In the study, the following conditions increased the probability of death in patients with Aeromonas infection: hematological malignancy, cholelithiasis, septic shock, recent surgery, and transfusion. Immunosuppressive medications and intensive chemotherapy accelerate the immune system’s degeneration in hematological malignancy patients, making them more vulnerable to infection.35 In a clinical study by Xu et al,35 42 people with leukemia complicated by an Aeromonas infection took part. Most Aeromonas infections were found to occur in leukemia patients who were experiencing granulocyte shortage, and granulocyte insufficiency lasting longer than 7 days was associated with patient mortality.
The 188 strains had higher susceptibility rates to ciprofloxacin, levofloxacin, cefepime, amtraenem, imipenem and meropenem, both of which were over 83%, similar to those reported in other regions.6,29 And then, there are differences in the drug resistance rates of Aeromonas in different infection sites, and the drug resistance rate of strains with extra-intestinal infection is significantly higher than that of strains with intestinal infection, which is in line with the study results of Zhou et al.29 However, intestinal infection strains were much less susceptible to imipenem than extra-intestinal strains, with a susceptibility rate of only 76.7%. Imipenem susceptibility ranged from 89.8% to 95% in earlier reports29,36 using intestinal isolates. In order to do future research, we must increase the sample size.
The three primary lactamases found in Aeromonas are Ambler C cephalosporin enzymes, D penicillinases, and B metallic lactamases (MBLs).2 The metalloenzyme CphA gene mainly exists in A. hydrophila, A. veronii, and A. jandaei, but not in A. caviae.37 This experiment’s discovery of the CphA gene in A. dhakensis, A. veronii, A. hydrophila, and A. jandaei supported this assertion. In addition, imipenem and meropenem sensitivity was discovered in 22 of 33 CphA-positive Aeromonas strains. According to earlier research, the genotype and drug sensitivity phenotype of CphA were discordant because gene mutation altered the gene expression of the protein.38 The research team will continue to look into what specific mechanism triggered this outcome. Two Aeromonas strains harboring the CphA gene and ESBLs were identified in this study, and the findings of the drug sensitivity tests were in line with the genotype expression. We need to pay more attention to the combined drug resistance of the CphA gene and the Aeromonas ESBLs, which has not yet been extensively explored. Additionally, two strains with both NDM and ESBLs were found, and NDM frequently co-existed with other drug resistance genes, which were transferred horizontally through plasmids and integrons in strains,39 leading to its spread in different strains, which presented serious challenges to the prudent use of antibiotics.
The diversity and complexity of Aeromonas’s harmful nature were caused by a wide range of virulence factors. When relevant virulence factors were screened, it was discovered that 188 Aeromonas strains had detection rates of alt, aerA, ela, lip, gcaT and fla that were higher than 58%, comparable to those documented in the literature.40 Extracellular proteases have the ability to break down different types of proteins, supply amino acids to bacteria, and directly cause significant tissue damage. This is a key pathogenic mechanism used by infected bacteria to get past the host’s defenses and propagate throughout the body.2,41 In the study, it has been discovered that the extracellular protease detection rate of strains isolated from the intestinal was higher than that from the extra-intestinal, indicating a difference in pathogenicity between strains infected from the intestinal and those infected from the extra-intestinal.
Conclusion
In a word, Aeromonas in this region was mainly infected by extra-intestinal. Compared with intestinal strains, it was found that there were differences in species distribution, drug susceptibility, drug resistance and virulence gene distribution between the two types of infection.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. The collection of culture isolates and collation of anonymous clinical data was in accordance with the approved clinical practice guidelines. Approval was granted by the Institutional Review Board and Ethics Committee of Chongqing Medical University approved this study (approval number: KY2021-557).
Acknowledgments
The authors would like to thank all participants and data collectors.
Funding
This work was supported by the Natural Science Foundation of Chongqing (No. cstc2019jcyj-msxmX0253). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Martin-Carnahan A, Joseph SW. Bergey’s Manual of Systematic Bacteriology. Philadelphia, Boston, MA: Springer; 2005:556–578.
2. Janda JM, Abbott SL. The genus Aeromonas: taxonomy, pathogenicity and infection. Clin Microbiol Rev. 2010;23:35–73. doi:10.1128/CMR.00039-09
3. Goncalves PR, de Oliveira WF, Marques DSC, et al. The genus Aeromonas: a general approach. Microb Pathog. 2019;130:81–94. doi:10.1016/j.micpath.2019.02.036
4. Fu MQ, Rao DP, Wu FF. Epidemic characteristics and drug resistance analysis of Aeromonas from clinical inpatients. J Baotou Med Coll. 2020;32:307–309.
5. Ji YR, Dong SJ, Kyong RP. Clinical and therapeutic implications of Aeromonas bacteremia:14 years nation-wide experiences in Korea. Infect Chemother. 2016;48:274–284. doi:10.3947/ic.2016.48.4.274
6. Sun Y, Zhao Y, Xu W, et al. Taxonomy, virulence determinants and antimicrobial susceptibility of Aeromonas spp. isolated from bacteremia in southeastern China. Antimicrob Resist Infect Control. 2021;10:43. doi:10.1186/s13756-021-00911-0
7. Kitagawa H, Ohge H, Yu LS, et al. Aeromonas dhakensis is not a rare cause of Aeromonas bacteremia in Hiroshima, Japan. J Infect Chemother. 2020;26:316–320. doi:10.1016/j.jiac.2019.08.020
8. Hänninen ML, Siitonen A. Distribution of Aeromonas phenospecies and genospecies among strains isolated from water, foods or from human clinical samples. Epidemiol Infect. 1995;115:39–50. doi:10.1017/S0950268800058106
9. Beaz HR, Alperi A, Buján N, et al. Comparison of phenotypical and genetic identification of Aeromonas strains isolated from diseased fish. Syst Appl Microbiol. 2010;33:149–153. doi:10.1016/j.syapm.2010.02.002
10. Fan X, Xiao M, Xu ZP. Evaluation of matrix-assisted laser desorption ionization time-of-flight mass spectrometry systemClin-TOF- II MS in identification of gram negative bacteria. Chin J Lab Med. 2017;40:41–45.
11. Soler L, Yáñez MA, Chacon MR, et al. Phylogenetic analysis of the genus Aeromonas based on two housekeeping genes. Int J Syst Evol Microbiol. 2004;54:1511–1519. doi:10.1099/ijs.0.03048-0
12. He TF, Li Y, Chen X, et al. Genetically classification of Aeromonas strains identified by gyrB and rpoD gene. Chin J Clin Lab Sci. 2015;33:569–572.
13. Anandan S, Gopi R, Ragupathi NKD, et al. First report of bla OXA-181-mediated carbapenem resistance in Aeromonas caviae in association with pKP3-A: threat for rapid dissemination. J Glob Antimicrob Resist. 2017;10:310–314. doi:10.1016/j.jgar.2017.07.006
14. Lay CJ, Zhuang HJ, Ho YH, et al. Different clinical characteristics between polymicrobial and monomicrobial Aeromonas bacteremia -a study of 216 cases. Intern Med. 2010;49:2415–2421. doi:10.2169/internalmedicine.49.4117
15. Tomás JM. The Main Aeromonas Pathogenic Factors. ISRN Microbiol. 2012;2012:1–22. doi:10.5402/2012/256261
16. Bożena K, Henrik C, Stefan E, et al. Phylogeny of the family Pasteurellaceae based on rpoB sequences. Int J Syst Evol Microbiol. 2004;54:1393–1399. doi:10.1099/ijs.0.03043-0
17. Zhang XJ, Qin GM, Bing XW, et al. Molecular and phenotypic characterization of Vibrio aestuarianus, a pathogen of the cultured tongue sole, Cynoglossus semilaevis Gunther. J Fish Dis. 2011;34:57–64. doi:10.1111/j.1365-2761.2010.01212.x
18. Martinez-Murcia AJ, Monera A, Saavedra MJ, et al. Multilocus phylogenetic analysis of the genus Aeromonas. Syst Appl Microbiol. 2011;34:189–199. doi:10.1016/j.syapm.2010.11.014
19. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:801–810. doi:10.1001/jama.2016.0287
20. Horwich TB, Fonarow GC, Hamilton MA, et al. Anemia is associated with worse symptoms, greater impairment in functional capacity and a significant increase in mortality in patients with advanced heart failure. J Am Coll Cardiol. 2002;39:1780–1786. doi:10.1016/S0735-1097(02)01854-5
21. Finfer S, Bellomo R, McEvoy S, et al. Effect of baseline serum albumin concentration on outcome of resuscitation with albumin or saline in patients in in- tensive care units: analysis of data from the saline versus albumin fluid evaluation (SAFE) study. BMJ. 2006;333:1044–1045.
22. Chang YB, Zhang DQ, Niu SQ, et al. MBLs, rather than efflux pumps, led to carbapenem resistance in fosfomycin and aztreonam/avibactam resistant Elizabethkingia anophelis. Infect Drug Resist. 2021;14:315–327. doi:10.2147/IDR.S294149
23. Clinical and Laboratory Standards Institute. Methods for antimicrobial dilution and disk susceptibility testing of infrequently isolated or fastidious bacteria. In: CLSI Guideline M45.
24. Wang Q, Wang X, Wang J, et al. Phenotypic and genotypic characterization of CarbapenemresistantEnterobacteriaceae: data from a longitudinal large-scale CRE study in China (2012–2016). Clin Infect Dis. 2018;67:196–205. doi:10.1093/cid/ciy660
25. Sun JJ, Zhang XJ, Gao XJ, et al. Characterization of virulence properties of Aeromonas veronii isolated from diseased Gibel Carp (Carassius gibelio). Int J Mol Sci. 2016;17:496. doi:10.3390/ijms17040496
26. Pablos M, Rodriguez-Calleja JM, Santos JA, et al. Occurrence of motile Aeromonas in municipal drinking water and distribution of genes encoding virulence factors. Int J Food Microbiol. 2009;135:158–164. doi:10.1016/j.ijfoodmicro.2009.08.020
27. Sreedharan K, Philip R, Singh IS. Characterization and virulence potential of phenotypically diverse Aeromonas veronii isolates recovered from moribund freshwater ornamental fishes of Kerala, India. Antonie Van Leeuwenhoek. 2013;103:53–67. doi:10.1007/s10482-012-9786-z
28. Wu CJ, Wang HC, Chen PL, et al. AQU-1, a chromosomal class C beta-lactamase, among clinical Aeromonas dhakensis isolates: distribution and clinical significance. Int J Antimicrob Agents. 2013;42:456–461. doi:10.1016/j.ijantimicag.2013.08.002
29. Zhou YY, Yu L, Nan Z, et al. Taxonomy, virulence genes and antimicrobial resistance of Aeromonas isolated from extra-intestinal and intestinal infections. BMC Infect Dis. 2019;19:158. doi:10.1186/s12879-019-3766-0
30. Meng GP, Yu QQ, Ma Q, et al. Analysis of clinical distribution characteristics and drug sensitivity of 41 patients with Aeromonas caviae infection. J Henan Med Coll. 2020;32:307–309.
31. Sinclair HA, Heney C, Sidjabat HE, et al. Sidjabat Genotypic and phenotypic identification of Aeromonas species and CphA-mediated carbapenem resistance in Queensland, Australia. Diagn Microbiol Infect Dis. 2016;85:98–101. doi:10.1016/j.diagmicrobio.2016.02.005
32. Qu F, Bao CM, Eb C, et al. Prevalence and antimicrobial resistance of different Aeromonas species. Chin J Infect Chemother. 2004;4:302–305.
33. Chen YW, Su SL, Li CW, et al. Pancreaticobiliary cancers and Aeromonas isolates carrying type secretion system genes ascF-ascG are associated with increased mortality: an analysis of 164 Aeromonas infection episodes in Southern Taiwan. Front Cell Infect Microbiol. 2021;11:749269. doi:10.3389/fcimb.2021.749269
34. Funada H, Matsuda T. Aeromonas bacteremia in patients with hematologic diseases. Intern Med. 1997;36:171–174. doi:10.2169/internalmedicine.36.171
35. Xu CH, Lin QS, Lyu YX, et al. Clinical features and laboratory data analysis of Aeromonas bacteremia with hematological diseases. Chin J Hematol. 2019;40:1035–1039.
36. Wu LF, Han JY, Dong YF, et al. Virulence gene determination and drug resistance analysis of diarrhea associated Aeromonas. Genom Appl Biol. 2020;39:312–328.
37. Balsalobre LC, Dropa M, Lincopan N, Mamizuka EM, Matté GR, Matté MH. Detection of metallo-β-lactamases-encoding genes in environmental isolates of Aeromonas hydrophila and Aeromonas jandaei. Lett Appl Microbiol. 2009;49:142–145. doi:10.1111/j.1472-765X.2009.02625.x
38. Rossolini GM, Zanchi A, Chiesurin A, et al. Distribution of cphA or related carbape-nemase-encoding genes and production of carbapenemase activity in members of the genus Aeromonas. Antimicrob Agents Chemother. 1995;39:346–349. doi:10.1128/AAC.39.2.346
39. Zhang TY, Lin YF, Li PH, et al. Characterization of plasmid co-harboring NDM-1 and SHV-12 from a multidrug-resistant Citrobacter freundii strain ZT01-0079 in China. Infect Drug Resist. 2021;9:947–952. doi:10.2147/IDR.S301736
40. Zhang DX, Kang YH, Song MF, et al. Identity and virulence properties of Aeromonas isolates from healthy Northern snakehead (Channa argus) in China. Lett Appl Microbiol. 2019;69:100–109. doi:10.1111/lam.13172
41. Abbott SL, Cheung WK, Janda JM. The genus Aeromonas: biochemical characteristics, atypical reactions, and phenotypic identification schemes. J Clin Mierobi. 2003;41:2348–2357. doi:10.1128/JCM.41.6.2348-2357.2003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.