")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Remote Diabetic Foot Temperature Monitoring for Early Detection of Diabetic Foot Ulcers: A Cost-Effectiveness Analysis
Authors Brooks E, Burns M , Ma R, Scholten HJ, Becker S
Received 2 June 2021
Accepted for publication 9 September 2021
Published 7 October 2021 Volume 2021:13 Pages 873—881
DOI https://doi.org/10.2147/CEOR.S322424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Elizabeth Brooks,1 Megan Burns,1 Ran Ma,2 Henk Jan Scholten,2 Shawn Becker3
1TTi Health Research and Economics, Westminster, MD, USA; 2Siren Care, Inc, San Francisco, CA, USA; 3Silvercat Advisors, LLC, Burlingame, CA, USA
Correspondence: Megan Burns
TTi Health Research and Economics, 1231 Tech Ct Suite 201, Westminster, MD, 21157, USA
Email [email protected]
Background: Foot temperature monitoring for the prevention and early detection of diabetic foot ulcers (DFU) is evidence-based and recommended in clinical practice. However, easy-to-use remote monitoring tools have been lacking, thereby preventing widespread adoption.
Objective: To evaluate the cost-effectiveness of remote foot temperature monitoring (RFTM) (Siren’s Neurofabric™ Diabetic socks) in addition to standard of care (SoC) versus SoC alone for early detection of DFU with diabetic neuropathy and a moderate to high risk of DFU.
Methods: A payer perspective decision-tree analysis was conducted to compare expected DFU occurrence and subsequent amputation rates and costs between treatment strategies over one year. Inputs in the model were sourced from publicly available literature and relevant health technology assessments. One-way sensitivity analyses were performed for each model variable.
Results: In the base-case scenario, RFTM plus SoC was a dominant strategy compared to SoC alone. RFTM plus SoC was associated with cost savings of $38,593 per additional ulcer avoided versus SoC alone, and $8027 per patient per year on average compared to SoC alone. These results were highly robust to one-way sensitivity analysis; all scenarios remained dominant if compliance was ≥ 13%.
Conclusion: RFTM is a cost-effective addition to SoC in patients with diabetic neuropathy at a moderate-to-high risk of DFU and subsequent amputation. Further, reduction in DFU and associated complications may result in improvements in the patient’s quality of life and mental health. Future studies are needed to evaluate the compliance and reduction of DFU occurrence in patients on RFTM.
Keywords: diabetes mellitus, diabetic foot, technology assessment, biomedical, cost-benefit analysis, cost savings, decision trees
A Letter to the Editor has been published for this article.
Introduction
Diabetes is a common and serious health issue in the United States (US), associated with a substantial clinical and economic burden. This burden is magnified when diabetes patients experience negative clinical consequences such as diabetic foot ulcers (DFU) and lower extremity amputation. As of 2015, 30 million US citizens had diabetes, accounting for 9% of the country’s population.1 Approximately 15–34% of people with diabetes are likely to experience DFU.2,3 DFU is an open sore or wound on the foot of a diabetic patient, most commonly located on the bottom of the foot.3 Diabetic patients at high risk for DFUs can include those with a history of DFUs, callus, or Charcot foot; such afflictions often lead to future ulceration.4 Many ulcers heal with additional intervention; however, 14–24% of diabetes patients require amputation. In total, 85% of diabetes-related amputations are due to DFUs.3
Patient outcomes and quality of life associated with both DFU and diabetes-related amputation are negative. Following a diabetes-related amputation, mortality exceeds 70% at 5 years for all patients.2 Outcomes are poor for patients experiencing DFU; a recent study demonstrated that 1-, 2-, and 5-year survival rates with DFU were 81%, 69%, and 29% respectively.5 Further, among those living with DFU, the incidence of concomitant depression is approximately 62%.6 Only 25% to 50% of patients with diabetes who experience depression are clinically diagnosed and appropriately treated.7 When such mental health issues go untreated, it can set off a cycle of worsening both the diabetic condition and the individual’s depression.7 Such issues may arise because worsened mental health may impact an individual’s ability to stay compliant with diabetic treatment plans.7
In addition, diabetes constitutes a substantial financial burden to the US healthcare system. In 2016, diabetes was found to be the third-highest cost in terms of US healthcare spending.8 Annual direct costs for diabetes care in the US are upwards of $176 billion, and as much as one-third of this cost (approximately $59 billion annually) is related to lower-extremity issues, including both DFU and diabetes-related amputations.2 According to the American Diabetes Association, in 2018, diagnosis and management of diabetic foot complications cost the US approximately $43 billion. On a per-patient basis, treating DFU costs approximately $2387 per month or $28,644 annually per diabetic patient.9,10 In 2013, it cost more to treat a DFU than the five costliest forms of cancer.11 In the event that an amputation occurs due to DFU, the amputation costs $83,326.12
Standard of care (SoC) treatments for DFU include “off-loading”, removing dead skin and tissue (“debridement”), applying medication and dressings to the DFU, managing blood glucose and other health problems, prevention of infection, and surgical measures.3 Although those methods are the current SoC, they still yield the aforementioned physical, mental, and financial hardships. Early detection is the key in the care of diabetic foot problems as studies have shown up to 75% of DFUs can be avoided if at-risk patients are identified early.13 Recently, additional guidance on the prevention of DFUs has come to include a role for temperature monitoring.14 Temperature monitoring measures the temperature differential between similar regions of each foot and an increase above a certain threshold is associated with inflammation.15 Inflammation anticipates the formation of a foot wound and temperature monitoring has been proven in multiple randomized clinical trials to identify ulcers early; this is important because many diabetes patients with neuropathy may not feel the pain associated with inflammation until the ulcer develops due to nerve damage associated with neuropathy.15 This is a prevalent issue because neuropathy affects roughly 50% of diabetes patients.16 Temperature monitoring allows the patient to potentially minimize poor outcomes associated with ulcer formation because it warns the diabetes patient of inflammation whether the patient feels it or not.15 Because of this, remote temperature monitoring can help improve outcomes for patients at risk of DFU.
While temperature monitoring is technically a SoC, there are no easy-to-use tools on the market. Temperature is considered one of the best diagnostics tests in determining whether or not a foot is likely to get an ulcer.17 However, temperature monitoring is not currently a routine in diabetic foot care, which could be because there is a lack of access to technology that measures foot temperature, because the cost-effectiveness of those technologies is not known, or because patients only perform simple monitoring of their condition at home.14 Clinical guidelines may not cite temperature monitoring as a useful diagnostic method if it has not been demonstrated as such.18 Remote foot temperature monitoring (RFTM) must be established as a simple and cost-effective diagnostic for DFU so that it can become more routine and recommended SoC.
Other studies have shown that temperature monitoring the foot of a diabetic patient can improve patient outcomes and reduce excess resource utilization. Lavery et al 2019 found that temperature monitoring a single foot predicted 91% of impending foot ulcers 41 days before their clinical presentation, on average.19 Banks et al 2020, a case series utilizing a temperature monitoring mat, found that outreach prompted by the mat led to medical intervention that may not have occurred if it were not time for a routine exam, and the outreach allowed for quicker healing with little complications for the diabetic feet.20 A systematic review done by Alahakoon et al 2020 found that patients who monitor their foot temperature at home are less likely to develop a DFU, and no amputations occurred in studies where amputation outcomes were recorded.21 Alone, self-monitoring of a foot by patients and healthcare professionals is limited due to the subtle warning signs of ulceration; however, the use of a temperature monitoring device can reduce foot ulceration.15 Overall, the literature supports the improved outcomes associated with RFTM for a diabetic foot.
If a temperature monitoring system could be introduced that offered a high likelihood of compliance through ease of use and reliable data, then it might be possible to significantly impact the outcomes and costs associated with diabetic foot complications. Here, we model the potential economic impact of adopting the utilization of RFTM. For the compliance and costs inputs, we used data specific to Siren’s Neurofabric™ Diabetic socks (Siren, San Francisco, CA), which is an RFTM that continuously tracks foot temperature and sends real-time information directly to physicians to enable tracing of issues related to temperature differentials that can indicate inflammation. The socks are equipped with sensors connected to a web and mobile application that monitor the temperature, which directly notifies the patient and his/her doctor if there is concerning information. The socks come in a lifetime supply and can be replaced when worn down without any maintenance costs. An observational study has shown that this RFTM device feels like normal socks, and reliably measure temperature.30 The results of the model, however, are not exclusive to a particular RFTM device. In addition to socks, other RFTM work similarly to the socks and can include mats, sticks, and insoles.
The objective of this study was to model the comparative and cost-effectiveness of the implementation of RFTM to reduce DFUs compared to the SoC.
Methodology
A decision-tree analysis was conducted to compare expected DFU occurrence rates and costs between SoC alone vs RFTM plus SoC for early detection of DFUs in patients with diabetic neuropathy at a moderate-to-high risk of DFU (ie, with a history of DFUs, calluses, or Charcot foot) (Figure 1). Further, the expected ulceration rate, cost-effectiveness, and incremental cost per additional ulcer avoided (ICER) were calculated at a yearly time horizon. Costs are reported in 2020 US dollars, and the model was developed from a US payer perspective.
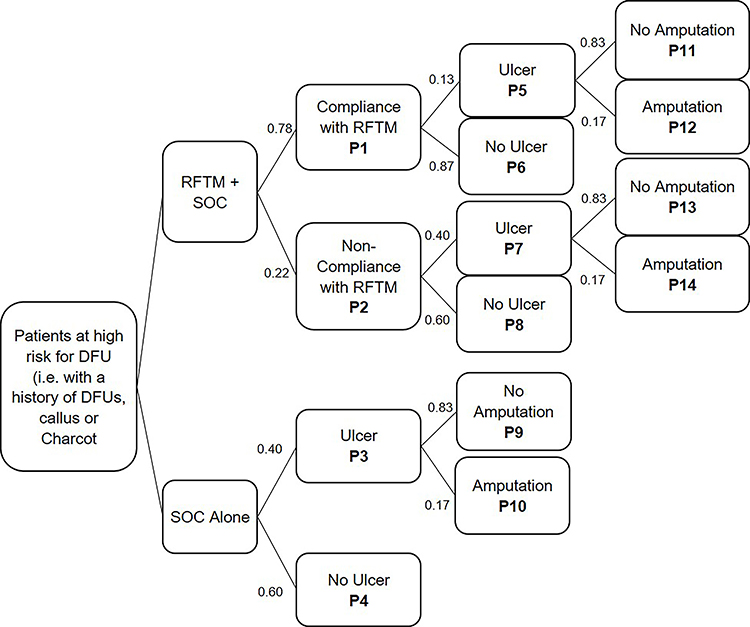 |
Figure 1 Decision-tree model structure. Abbreviations: DFU, diabetic foot ulcer; RFTM, remote foot temperature monitoring; SoC, standard of care. |
Clinical and cost inputs in the model were sourced from publicly available peer-reviewed literature and relevant health technology assessments. Inputs comprised the probability of developing DFU within 12 months, probability of amputation to resolve a foot ulcer, average healing time for a foot ulcer, average monthly cost of treatment of a foot ulcer, and average cost of amputation. No meta-analysis was undertaken. A weighted average was used if multiple sources were identified for the same outcome.
The model begins with patients who are at high risk for DFU, such as patients who have a history of DFUs, callus, or Charcot foot, who are assigned to RFTM with SoC or assigned to SoC alone. Patients assigned to the RFTM plus SoC group can be compliant (P1) or non-compliant (P2) with the RFTM usage. Compliance is measured as wearing the RFTM one hour a day for at least 16 days per month. From here, the model incorporates the probabilities of the patient developing an ulcer or not developing an ulcer based on their compliance status, represented as probabilities P5–P8. The model assumes one ulcer on one foot. For patients in both the compliant and non-compliant groups who develop an ulcer, the model predicts which of those ulcers will heal without amputation and those which will require amputation to heal (P11–P14). For patients only receiving SoC alone, compliance is not incorporated and therefore the model directs them to either develop an ulcer or not per probabilities P3 and P4. The model then calculates the probability that those with an ulcer will heal without amputation, or will require amputation (P9–P10).
A one-way sensitivity analysis was performed for each variable in the model. Ranges for the sensitivity analysis were determined for base case values. For compliance, the sensitivity analysis tested results from 10% to 100% compliance. For the likelihood that a patient will develop an ulcer in 12 months, the range was calculated as plus or minus 20% of the base case value for SoC Alone and Non-Compliant RFTM Users. For the probability an amputation is required in the event an ulcer occurs, the range was determined by the variability of outcomes in the vetted literature. The sensitivity analysis range for ulcer healing time was plus or minus 40% of the base case for SoC Alone and Compliant Users. A greater range was chosen for this variable due to the difference in healing time on a case-by-case basis. The average monthly cost of an ulcer and average cost of amputation had a range of plus or minus 20%. The cost range used in the model is between $1250 and $1500. The base case value remains $1500 to evaluate the cost-benefit with the higher cost of RFTM. The input for the reduction in the probability that a patient will develop an ulcer in 12 months for compliant patients is determined by a randomized controlled trial by Armstrong et al 2007 which states that those monitoring their foot temperature are 33% as likely to experience an ulcer.15
Published literature provided data on the likelihood that patients will develop ulcers within 12 months and require subsequent amputation, wound healing time, and the average cost of wound treatment and amputation. Model inputs are described in Table 1.2,3,9,10,12,15,22–24 Inputs for the SoC values are based on the search of publicly available literature. Costs were inflated to 2020 USD.
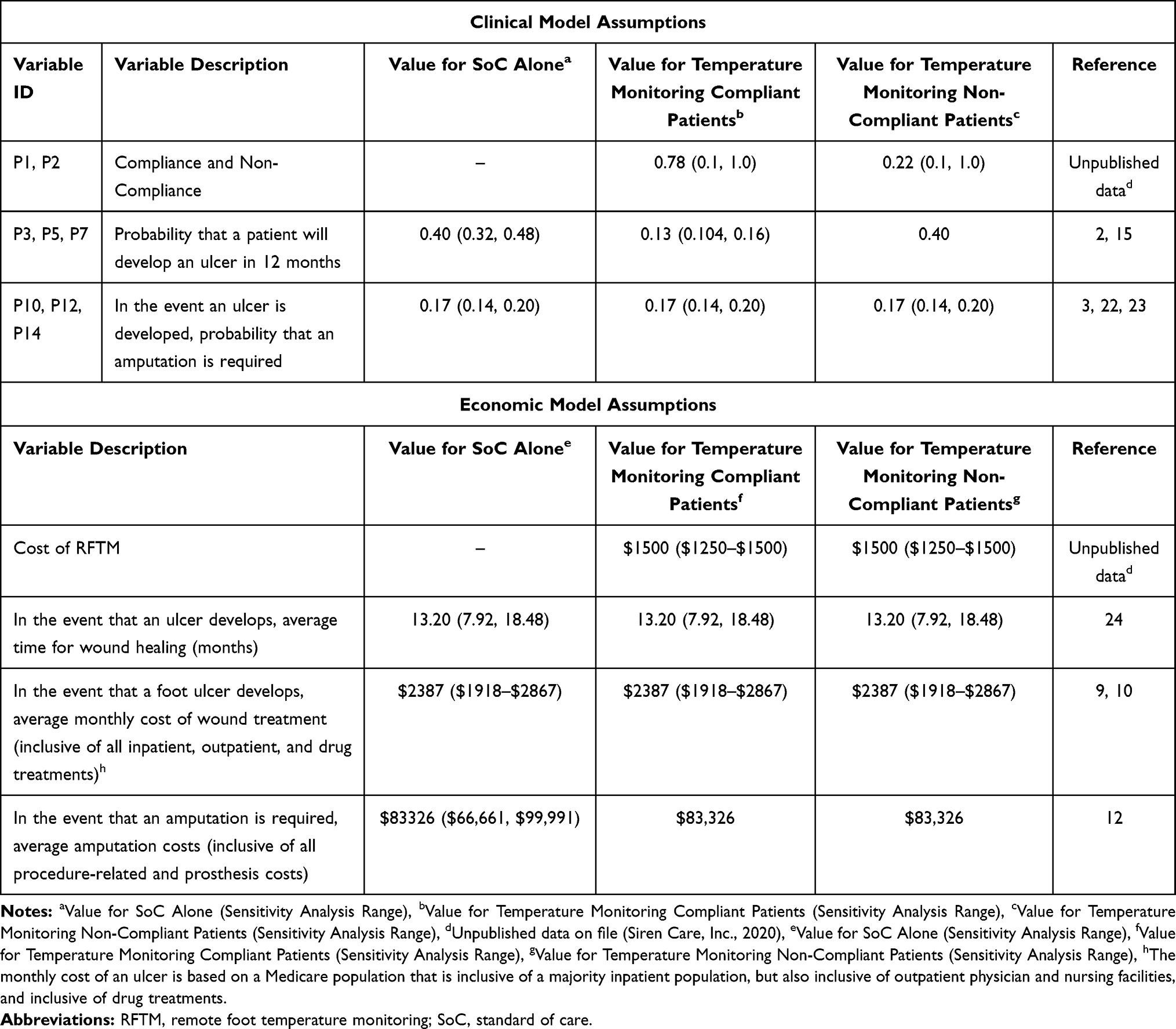 |
Table 1 Clinical and Economic Model Assumptions |
Results
Base Case Analysis
The RFTM in addition to SoC is the dominant and therefore more cost-effective method over the SoC alone (see Table 2). Table 2 shows that the remote temperature monitoring of the RFTM saves $38,593 per additional ulcer avoided. The mean annual cost per patient associated with DFU for RFTM plus SoC strategy is $10,303, while the mean annual per-patient costs associated with SoC alone are $18,330, resulting in mean per-patient payer savings of $8027 per year. The model included a sensitivity analysis (see –figure 4). When testing the results of the model with each of the variables’ ranges, RFTM was dominant 96% of the time in one-way sensitivity analyses.
 |
Table 2 One Year Cost-Effectiveness Results |
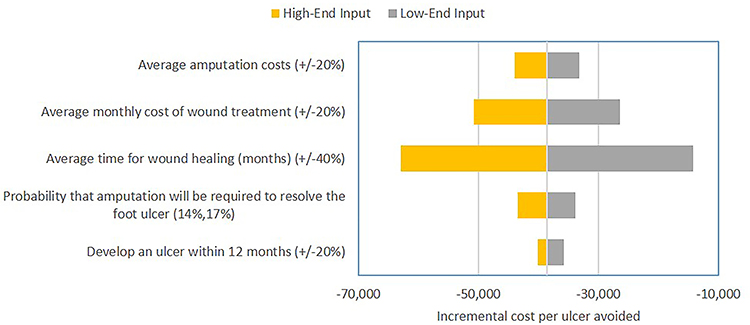 |
Figure 2 Sensitivity analysis for SoC alone. The points that fall below 0 favor RFTM, while points that are greater than 0 favor SoC alone. Abbreviations: RFTM, remote foot temperature monitoring; SoC, standard of care. |
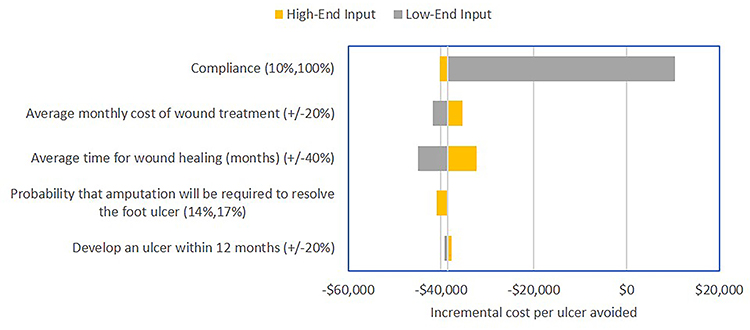 |
Figure 3 Sensitivity analysis for compliant RFTM users. The points that fall below 0 favor RFTM, while points that are greater than 0 favor SoC alone. Abbreviations: RFTM, remote foot temperature monitoring; SoC, standard of care. |
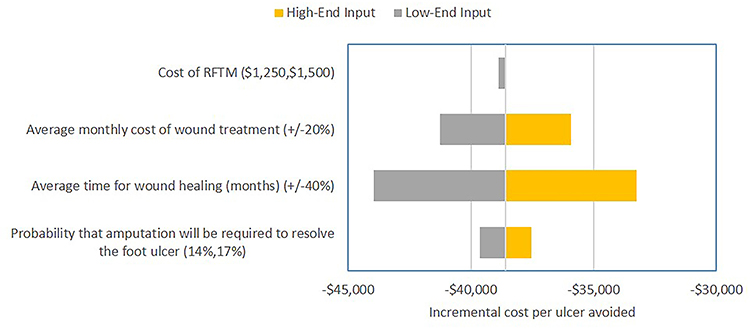 |
Figure 4 Sensitivity analysis for non-compliant RFTM users. The points that fall below 0 favor RFTM, while points that are greater than 0 favor SoC alone. Abbreviations: RFTM, remote foot temperature monitoring; SoC, standard of care. |
Sensitivity Analysis
A one-way sensitivity analysis was performed for each variable in the model (results shown in Figures 2–4). The points that fall below 0 favor RFTM, while points that are greater than 0 favor SoC alone.
The one-way sensitivity analysis for compliance demonstrated that RFTM is cost-effective at as low as 13% compliance (if all other base case values are unchanged). As a result, if at least 13% of patients are compliant with RFTM, it is still the dominant (less costly, more clinically effective) method over SoC alone; however, based on unpublished patient data describing experience with RFTM, patients are approximately 78% compliant with the service.
The highest level of variability in the model occurs when running the one-way sensitivity analysis in the SoC-only variables. When running the one-way sensitivity analysis for each patient group (SoC only, compliant RFTM users, and non-compliant RFTM users), the most variability occurs in the average monthly cost of treatment and the average time for wound healing. Assuming an average monthly cost of wound treatment in the SoC-only group of $1918 will save the facility $26,434 per ulcer avoided, whereas assuming an average monthly cost of $2876 would save the facility $50,753 per ulcer avoided. For the Compliant group, the same inputs result in cost savings of $41,755 and $35,432 per ulcer avoided, respectively. For the Non-Compliant group, the same inputs result in cost savings of $41,268 and $35,918 per ulcer avoided, respectively. When examining the average wound healing time (in months) in the SoC-only group of 8 months, the facility would expect to save $14,255 per ulcer avoided, whereas an average wound healing time of 18 months would result in savings of approximately $62,932 per ulcer avoided. Finally, wound healing time of 8 and 18 months results in cost savings of $44,921 and $32,265 per ulcer avoided, respectively, in the compliant group and cost savings of $43,948 and $33,239 per ulcer avoided in the non-compliant group, respectively.
Discussion
The model demonstrates that RFTM may improve patient outcomes with concomitant cost savings to healthcare payers; the expected ulceration rate with SoC alone is approximately 2.1 times greater than SoC with RFTM, and such ulceration rate is associated with greater expenses for both treatment and subsequent potential amputation. Further, early detection of DFU could lead to a reduction in amputation or shorter healing times which would improve the results of the model.25 There are, however, certain limitations associated with the model. The current model inputs are based on published literature; not direct outcomes data.
Temperature monitoring has been reported in the literature as a meaningful method of identifying issues and avoiding ulceration. However, compliance to previously existing foot temperature monitoring methods has been identified as a critical input into the value of monitoring in improving outcomes.26 This model is an effort to evaluate the potential impact of a temperature monitoring system that utilized new technology or methods to allow for greater compliance.
Additionally, patient-reported and quality of life metrics were excluded from the current analysis. Depression and quality of life, particularly following amputation, may increase overall costs of care for diabetic patients even beyond these results. Studies have reported that approximately 62% of people with a DFU experience depression, ranging from 28%-68%.6 Mental health is associated with the outcome of lower extremity wounds; those who have both diabetes and depression are more likely to need an amputation.27,28 In a pooled analysis from a systematic review, people with diabetes and depression have a 76% increased risk of lower extremity amputation.27 Once an amputation occurs, patients may experience additional feelings of anxiety, depression, and grief; sometimes serious enough to warrant a diagnosis of post-traumatic stress disorder.29 These issues may not only worsen the quality of life for the patient but can also incur expenses for payers.
Although the model does not use direct outcomes data or include quality of life metrics, it still shows massive cost savings. As such, if payers expected to see slightly different inputs in the model, they are still likely to experience cost savings, which is proved by the one-way sensitivity analysis. Further, extreme negative outcomes are currently associated with DFU, ie 14–24% of DFU patients requiring amputation, 5-year mortality after amputation exceeding 70%, and DFU complication costing the US $59 billion annually.2,3 The outcomes associated with DFU cannot get any worse than they currently are, but employing RFTM technology could help improve those outcomes.
Studies like this should continue to be conducted to establish RFTM as an easy-to-use and recommended tool in the clinical guidelines for DFU early detection and diagnosis. Such technology can be expanded upon to become even more useful. Continuous data collected by RFTM allow for machine learning, artificial intelligence, personalization, and more that could improve the experience of diabetes patients.
Conclusions
Remote foot temperature monitoring of a diabetic foot in patients who are at high risk for DFU such as those with a history of DFUs, callus, or Charcot foot may decrease the likelihood of DFU and subsequent amputation. This is accompanied by substantial cost savings for healthcare payers, with $38,593 annual incremental saving per ulcer avoided. Improvements in patient quality of life and mental health may increase these incremental benefits. Additional research is needed to quantify both compliance with and direct impact on DFU incidence associated with remote temperature monitoring devices.
Prior Presentation
This study has not been presented or submitted, in part or full, to any other journal or conference.
Data Sharing Statement
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.
Compliance with Ethics Guidelines
This study does not involve any human participants, human data, and/or human material. This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Author contributions
All authors had full access to all of the data in this study. All named authors meet the International Committee of Medical Journal Editors (ICJME) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given approval for this version to be published.
Funding
This study was sponsored by Siren Care. The article processing charges and open access fee for this publication were funded by Siren Care.
Disclosure
EB, MB, and SHB were paid consultants at Siren Care, Inc. for the duration of the project. RM and HJS are employees and share holders of Siren Care, Inc.
Ms Ran Ma has a patent US10638937B2: System and method for detecting inflammation in a foot issued to Siren Care, Inc., a patent US10480104B2: Smart yarn and method for manufacturing a yarn containing an electronic device issued to Siren Care, Inc., a patent US20190313913A1: Systems and methods for registration and activation of temperature-sensing garments pending to Siren Care, Inc., a patent US20200375470A1: Garment for monitoring a user and method for making the same pending to Siren Care, Inc. Mr Henk Jan Scholten has a patent US10638937B2: System and method for detecting inflammation in a foot issued to Siren Care, Inc., a patent US10480104B2: Smart yarn and method for manufacturing a yarn containing an electronic device issued to Siren Care, Inc., a patent US20190313913A1: Systems and methods for registration and activation of temperature-sensing garments pending to Siren Care, Inc., a patent US20200375470A1: Garment for monitoring a user and method for making the same pending to Siren Care, Inc. The authors report no other conflicts of interest in this work.
References
1. Center for Disease Control and Prevention. Diabetes growth rate steady, adding to health care burden; July 18, 2017. Available from: https://www.cdc.gov/media/releases/2017/p0718-diabetes-report.html#:~:text=More%20than%20100%20million%20U.S.,the%20U.S.%20population%20%E2%80%93have%20diabetes.
2. Armstrong D, Boulton A, Bus S. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367–2375. doi:10.1056/NEJMra1615439
3. American Podiatric Medical Association. Diabetic wound care. apma.org; 2020. Available from: https://www.apma.org/diabeticwoundcare.
4. Boulton A, Whitehouse R. The Diabetic Foot. Feingold K, Anawalt B, Boyce A, eds. MDText.com, Inc.; 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK409609/.
5. Brennan MB, Hess TM, Bartle B, et al. Diabetic foot ulcer severity predicts mortality among veterans with type 2 diabetes. J Diabetes Complications. 2016;31(3):556–561. doi:10.1016/j.jdiacomp.2016.11.020
6. Jiang F, Liu X, Yu H, Qian Y, Chen H. The incidence of depression in patients with diabetic foot ulcers: a systematic review and meta-analysis. Int J Low Extrem Wounds. 2020;153473462092989. doi:10.1177/1534734620929892
7. Center for Disease Control and Prevention. Diabetes and mental health. cdc.gov; August 6, 2018. Available from: https://www.cdc.gov/diabetes/managing/mental-health.html.
8. Dieleman JL, Cao J, Chapin A, et al. US health care spending by payer and health condition, 1996–2016. JAMA. 2020;323(9):863–884. doi:10.1001/jama.2020.0734
9. Barshes N, Saedi S, Wrobel J, Kougias P, Kundakcioglu O, Armstrong D. A model to estimate cost-savings in diabetic foot ulcer prevention efforts. J Diabetes Complications. 2017;31(4):700–707. doi:10.1016/j.jdiacomp.2016.12.017
10. Snyder R, Kirsner R, Warriner III R, Hanft J, Sheehan P. Consensus recommendations on advancing the standard of care for treating neuropathic foot ulcers in patients with diabetes. Ostomy Wound Manag. 2010;56(suppl 4):S1–S24.
11. Barshes N, Sigireddi M, Wrobel J, et al. The system of care for the diabetic foot: objectives, outcomes, and opportunities. Diabet Foot Ankle. 2013;4(1):21847. doi:10.3402/dfa.v4i0.21847
12. Margolis DJ, Malay S, Hoffstad OJ, et al. Economic burden of diabetic foot ulcers and amputations. Data Points #3. Vol 10. Agency for Healthcare Research and Quality; 2011. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65152/.
13. Boulton A, Armstrong D, Albert S, et al. Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American diabetes association, with endorsement by the American Association of clinical endocrinologists. Diabetes Care. 2008;31(8):1679–1685. doi:10.2337/dc08-9021
14. Bus S, Lavery L, Monteiro-Soares M, et al. IWGDF guideline on the prevention of foot ulcers in persons with diabetes; 2019. Available from: https://iwgdfguidelines.org/wp-content/uploads/2019/05/02-IWGDF-prevention-guideline-2019.pdf.
15. Armstrong D, Holtz-Neiderer K, Wendel C, Mohler J, Kimbriel H, Lavery L. Skin temperature monitoring reduces the risk for diabetic foot ulceration in high-risk patients. Am J Med. 2007;120(12):1042–1046. doi:10.1016/j.amjmed.2007.06.028
16. Hicks C, Selvin E. Epidemiology of peripheral neuropathy and lower extremity disease in diabetes. Curr Diab Rep. 2019;19(10):86. doi:10.1007/s11892-019-1212-8
17. Ibrahim A, Jude E, Langton K, et al. IDF Clinical practice recommendations on the diabetic foot: a guide for health care professionals. Diabetes Res Clin Pract. 2017;127:285–287. doi:10.1016/j.diabres.2017.04.013
18. Lipsky B, Senneville É, Abbas Z, et al. IWGDF guideline on the diagnosis and treatment of foot infection in persons with diabetes; 2019. Available from: https://iwgdfguidelines.org/wp-content/uploads/2019/05/05-IWGDF-infection-guideline-2019.pdf.
19. Lavery L, Petersen B, Linders D, Bloom J, Rothenberg G, Armstrong D. Unilateral remote temperature monitoring to predict future ulceration for the diabetic foot in remission. BMJ Open Diabetes Res Care. 2019;7(1):e000696. doi:10.1136/bmjdrc-2019-000696
20. Banks J, Petersen B, Rothenberg G, Jong A, Page J. Use of a remote temperature monitoring mat for the early identification of foot ulcers. Wounds. 2020;32(2):44–49.
21. Alahakoon C, Fernando M, Galappaththy C, et al. Meta‐analyses of randomized controlled trials reporting the effect of home foot temperature monitoring, patient education or offloading footwear on the incidence of diabetes‐related foot ulcers. Diabetic Med. 2020;37(8):1266–1279. doi:10.1111/dme.14323
22. Ferreira L, Carvalho A, Carvalho R. Short-term predictors of amputation in patients with diabetic foot ulcers. Diabetes Metab Syndr. 2018;12(6):875–879. doi:10.1016/j.dsx.2018.05.007
23. Guest J, Fuller G, Vowden P. Diabetic foot ulcer management in clinical practice in the UK: costs and outcomes. Int Wound J. 2018;15(1):43–52. doi:10.1111/iwj.12816
24. Shearer A, Gordois A, Scuffham P, Oglesby A. Predicted costs and outcomes from reduced vibration detection in people with diabetes in the US. Diabetes Care. 2003;26(8):2305–2310. doi:10.2337/diacare.26.8.2305
25. Frykberg R, Banks J. Management of diabetic foot ulcers: a review. Fed Pract. 2016;33(2):16–23.
26. van Netten J, Raspovic A, Lavery L, et al. Prevention of foot ulcers in the at‐risk patient with diabetes: a systematic review. Diabetes Metab Res Rev. 2020;36(S1):84–98. doi:10.1002/dmrr.3270
27. O’Neill S, Kabir Z, McNamara G, Buckley C. Comorbid depression and risk of lower extremity amputation in people with diabetes: systematic review and meta-analysis. BMJ Open Diabetes Res Care. 2017;5(1):e000366. doi:10.1136/bmjdrc-2016-000366
28. Williams L, Miller D, Fincke G, et al. Depression and incident lower limb amputations in veterans with diabetes. J Diabetes Complications. 2012;25(3):175–182. doi:10.1016/j.jdiacomp.2010.07.002
29. Bahari R. The psychological impact of diabetic limb problems. Int Med J Malays. 2015;14(2):3–8.
30. Reyzelman AM, Koelewyn K, Murphy M, et al. Continuous temperature-monitoring socks for home use in patients with diabetes: observational study. J Med Internet Res. 2018;20(12):e12460. doi:10.2196/12460
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.